
Abstract
Background:
Men’s lacrosse has been one of the fastest growing team sports in the United States, at both the collegiate and high school levels. Uniquely, it combines both continuous overhead and contact activity. Thus, an understanding of its injury epidemiology and mechanisms is vital. Shoulder injuries have been shown to be common in the sport, but thus far there has been no dedicated analysis of these injuries with which to better inform injury prevention strategies.
Study Design:
Descriptive epidemiology study.
Methods:
All athlete exposures (AEs) and shoulder injuries reported to the National Collegiate Athletic Association (NCAA) Injury Surveillance System for intercollegiate men’s lacrosse athletes from 2004-2005 through 2008-2009 were collected. Type of injury was documented and the injury incidence per 1000 AEs was calculated. Event type, injury mechanism, specific injury, outcome, and time lost were recorded. Statistical analysis was performed using 95% CIs, calculated based on a normal approximation to Poisson distribution.
Results:
There were a total of 124 observed shoulder injuries during 229,591 monitored AEs. With weights, this estimates 1707 shoulder injuries over 2,873,973 AEs, for an incidence of 0.59 per 1000 AEs (95% CI, 0.56-0.62). The incidence of shoulder injury during competition was 1.89 per 1000 AEs (95% CI, 1.76-2.02), compared with 0.35 per 1000 AEs (95% CI, 0.33-0.38) during practice. Acromioclavicular joint injuries were most common (0.29 per 1000 AEs; 95% CI, 0.27-0.31). Labral injuries and instability events were also frequent (0.11 per 1000 AEs; 95% CI, 0.10-0.13). Player-to-player contact caused 57% of all shoulder injuries, with 25% due to contact with the playing surface. The average time lost was 11.0 days, with 41.9% of all shoulder injuries requiring ≥10 days. Clavicle fractures and posterior shoulder dislocation were particularly severe, with no athletes returning to play during the same season.
Conclusion:
Shoulder injuries are common in NCAA men’s lacrosse and are an important source of lost playing time. Acromioclavicular injuries were the most frequent injury in this series, but labral and instability injuries were also common. In this increasingly popular contact sport, an understanding of the epidemiology and mechanism of shoulder injuries may be used to improve protective equipment and develop injury prevention.
The first men’s lacrosse National Collegiate Athletic Association (NCAA) championship game was played in 1971. Since then, the popularity of and access to the sport has grown substantially. In 1988-1989, there were 150 schools sponsoring varsity men’s lacrosse teams with 4805 participants. By 2013-2014, the number increased to 391 with 13,857 participants, 2 making lacrosse one of the fastest growing sports in the United States. Players are involved at a younger age, and the sport has been made more popular throughout the country and around the world.
The rapidly increasing popularity of this unique overhead, contact sport mandates an understanding of the injury profile of men’s lacrosse. Thus far, data have been reported on eye injuries, 15 anterior cruciate ligament injuries, 17 overall epidemiology,7,10,11,23 and concussion3-5,9; however, no epidemiologic study has been reported specifically on shoulder injuries. Notably, shoulder injuries account for 6.5% of reported injuries at the high school level. 23 Professional men’s lacrosse shows a similar trend, with 14% of all injuries affecting the shoulder (J. Parsons and P. Stull, unpublished data, 2015). To better inform injury prevention measures, it is important to understand these common injuries and their mechanisms. The purpose of the current study was to describe the incidence and mechanism of shoulder injuries in the game of men’s collegiate lacrosse.
Methods
Institutional review board approval (exemption) was obtained for this study. Approval of methods and to conduct the study was also received from the NCAA.
Data Collection
Data for this study were collected by the NCAA via its Injury Surveillance System (ISS). The data were obtained from Datalys, the nonprofit organization responsible for the collection, organization, and maintenance of the database. The data were obtained for the most recent 5-year period available, 2004-2005 through 2008-2009, to reflect the current state of the game. The details of the system have been well described previously by Dick et al 6 and Kerr et al. 13 It is a “convenience sample” in which volunteer certified athletic trainers from NCAA-sponsored institutions submit information related to the type of injury, body part injured, measures of injury severity (time loss and the need for surgery), and sport-specific details related to the mechanism of injury and player position via a web-based system. The NCAA ISS has repeatedly been used for the purposes of calculating incidence and describing the epidemiology of injury in American collegiate athletics.1,7,8,19,20
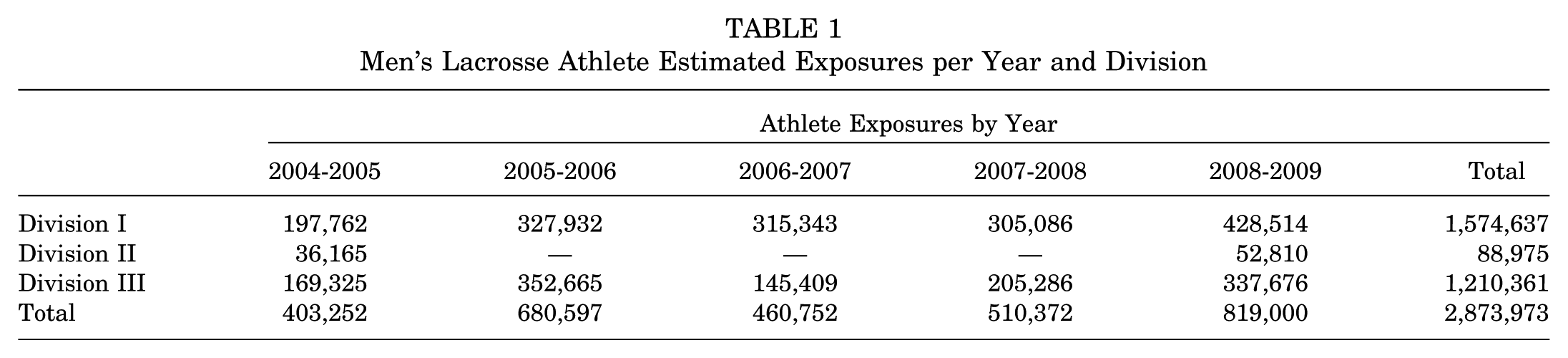
With the provided data for the sport code “Men’s Lacrosse,” an exposure data set was extracted from the 5-year period from 2004-2005 through 2008-2009 (Table 1). One athlete exposure is defined as 1 student-athlete participating in 1 game or practice, no matter the duration. Using the sport code “Men’s Lacrosse” and the body part code “Shoulder,” an injury data set was extracted for these years. A reportable injury is “one that (1) occurred as a result of participation in an intercollegiate practice or competition and (2) required medical attention by an athletic trainer or physician and (3) resulted in restriction of participation or performance for one or more calendar days beyond the day of injury.” 6 The exported data set passes through an automated verification process, and any data flagged for invalid values are addressed by the athletic trainers and data quality assurance staff.
Men’s Lacrosse Athlete Estimated Exposures per Year and Division
Statistical Methods
For each athlete exposure (AE) and injury reported in the data set, the NCAA has provided a sampling weight to allow extrapolation of the data from the small convenience sample to the entire NCAA population. These sampling weights have been included in all analyses.
The incidence of injury was calculated as the number of injuries divided by the number of AEs. This is reported per 1000 AEs to allow comparison with previously reported data.7,10,23 The 95% CIs were calculated for the incidence rates based on assumptions of a normal approximation to Poisson distribution.
Within the provided data, there is no descriptive information regarding injury severity. For each injury, however, the time lost, defined as the duration from the initial index injury to return to play, from activity was reported. This was used as a surrogate for severity of injury. Here, injuries with ≥10 days lost, including season-ending injuries, are considered particularly severe. 7
Further analysis described the mechanism of injury and evaluated for factors affecting the incidence of injury, such as the event type or activity during which the injury occurred.
Results
A total of 7087 events were recorded, each with between 4 and 55 athletes participating, yielding a total of 229,591 observed AEs. Data collection each year began on the first day of preseason and ran through the final day of competition, including any postseason games or practices if applicable. Of the 2,873,973 estimated AEs, 2,417,650 were practice AEs and 456,323 were game AEs. There were no participating Division II schools from 2005-2006 through 2007-2008.
These results represent the incidence of injuries. This allows the results of the sampled population to be better extrapolated to all NCAA men’s lacrosse participants during the 2004-2005 through 2008-2009 seasons.
There were a total of 124 observed injuries during the collection period. When weighted to an estimated 2,873,973 AEs, there were an estimated 1707 shoulder injuries, yielding an incidence of 0.59 per 1000 AEs (95% CI, 0.56-0.62). When evaluated according to event type, the incidence of shoulder injuries during practice was 0.35 per 1000 AEs (95% CI, 0.33-0.38) and during competition, 1.89 per 1000 AEs (95% CI, 1.76-2.02).
Table 2 presents the weighted incidence of each specific shoulder injury during the collection period. Acromioclavicular (AC) joint injuries were the most common, accounting for 50.0% of all shoulder injuries. Labral injuries (including anterior, posterior, superior labral anterior and posterior [SLAP] tears) and those associated with anterior/posterior instability events combine to account for over 20% of all shoulder injuries (21.8%). The incidence of posterior dislocation/subluxation was rare (0.01 per 1000 AEs; 95% CI, 0.01-0.02). The rate of fracture about the shoulder, including the clavicle and scapula, was 0.02 per 1000 AEs (95% CI, 0.01-0.02).
Specific Injury Incidence a
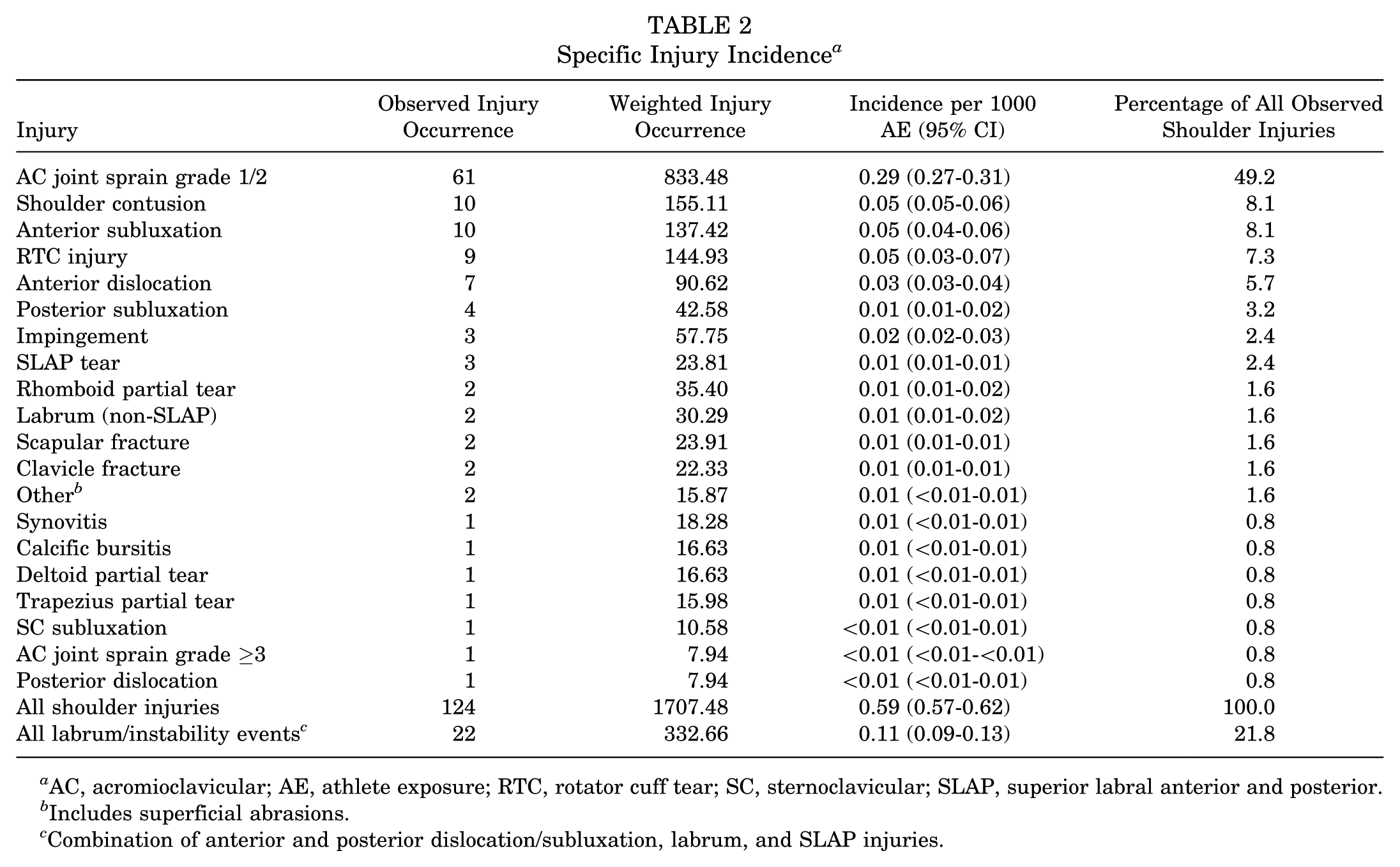
AC, acromioclavicular; AE, athlete exposure; RTC, rotator cuff tear; SC, sternoclavicular; SLAP, superior labral anterior and posterior.
Includes superficial abrasions.
Combination of anterior and posterior dislocation/subluxation, labrum, and SLAP injuries.
Most shoulder injuries occurred by player-player contact (57%). Contact with the playing surface caused 25% of the injuries. The balance comprised acute noncontact injury (8.7%), contact with apparatus (4.6%), and overuse injuries (4.6%).
For those athletes able to return to play that season, the average time loss for shoulder injuries in this cohort was 11.0 days. Not surprisingly, fractures were severe injuries, with all athletes with clavicle fracture remaining out for the remainder of the season and those with scapular fractures missing an average of 42.5 days (Table 3). Grade 1 or 2 AC joint injuries resulted in significant loss of time (10.5 days), with the number rising significantly (26.0 days) for grade ≥3 injuries and 1 season-ending injury. Anterior subluxation/dislocation events also resulted in extended loss of time (16.8 days) and 2 season-ending injuries. Posterior subluxations and dislocations led to fewer missed days (7.2 days) but also resulted in 1 season-ending injury. Other injuries that led to ≥10 days of time lost include SLAP tears (13.7 days) and presumed non-SLAP labral tears (12 days). Overall, 41.9% of all shoulder injuries reported resulted in ≥10 days lost.
Season-Ending Shoulder Injuries With Average Time Loss of ≥10 Days a
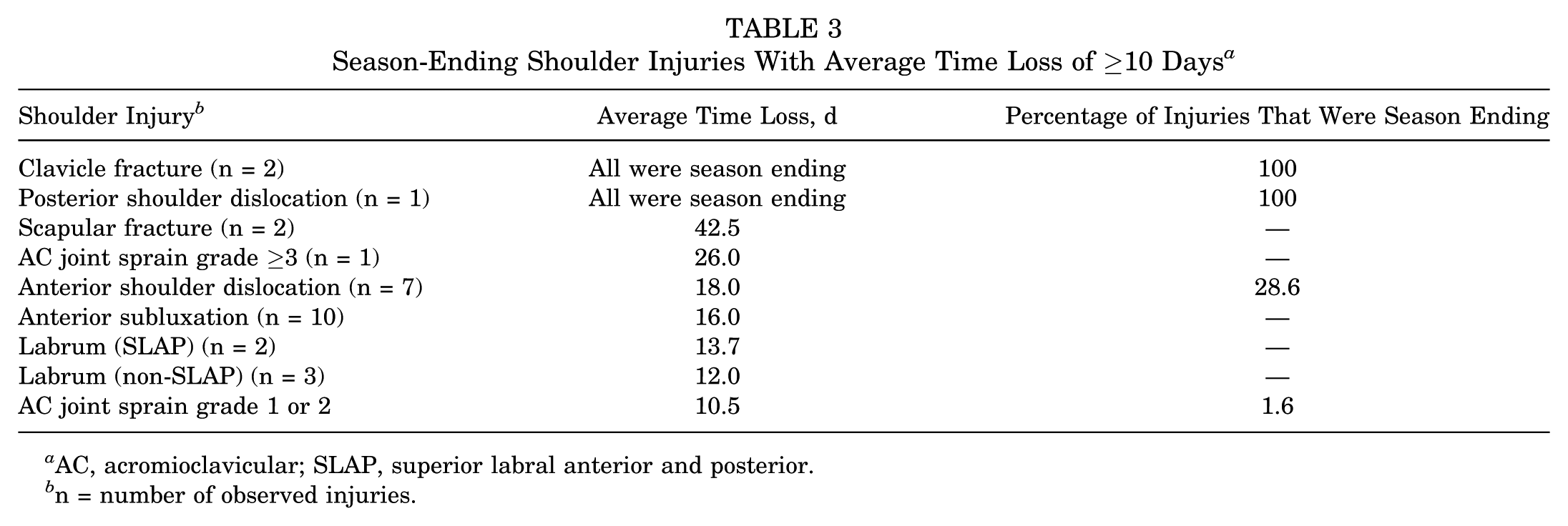
AC, acromioclavicular; SLAP, superior labral anterior and posterior.
n = number of observed injuries.
Several specific injuries were further analyzed to better understand their mechanism. Injuries to the AC joint represented the largest subset of shoulder injuries; almost all (99%) were partial sprains. Injuries to the AC joint were primarily related to player-to-player contact (67.7%) and player-to-surface contact (28.9%). Most players sustaining AC joint injuries returned to play within 1 week (44.5%) or 2 weeks (24.4%). Still, 9.5% of players had not returned to play after 4 weeks, and 2.0% of players sustained season-ending injuries (all grade 1 or 2 injuries).
Labral injuries (anterior, posterior, SLAP) and those associated with instability events accounted for 20% of all shoulder injuries. The primary injury mechanism for these injuries was player contact (44.3%), with contact with the playing surface accounting for most other injuries (37.8%). The average time lost for these athletes was 16.9 days.
Discussion
For more than a decade, lacrosse has been one of the fastest growing team sports in the United States. According to the US Lacrosse 2013 Participation Survey, 21 nearly 750,000 players participated in lacrosse on organized teams at some level in 2013, an increase of nearly 25,000 players from just 1 year prior. At the collegiate level, the growth is particularly astounding. In this era of downsizing of college athletics, lacrosse has defied the odds, with 60 new college programs beginning play in 2013, with 39 more starting in 2014. 21
The men’s game is unique in that it is an overhead contact sport more similar to American football than to sports using sticks such as ice hockey. This exposes the athlete to the typical injuries encountered in overhead sports, collision sports, and sports using handheld equipment (sticks or crosses).
Common maneuvers that occur in men’s lacrosse may lead to unique mechanisms of injury. Body contact, or checking, is permissible if the contact is above the waist and below the shoulder of the opponent, and the opponent is in possession of or within 5 yards of the ball. It is similar to ice hockey and typically involves a collision at the shoulder level with both hands on the stick. If a player falls or is driven into the ground, a direct blow to the top of the shoulder may occur. If the fall occurs with the arm in an abducted and externally rotated position, the shoulder may dislocate in an anterior-inferior direction. Finally, during a face-off, rotational force in the shoulder, combined with a posteriorly directed shearing force, may lead to labral injury.
The NCAA mandates that all players, except the designated goalkeeper, wear shoulder and arm pads. 18 Although shoulder pads have become more robust in recent years, they remain significantly thinner and lightweight than those used in ice hockey or football. Lacrosse shoulder pads have a noncantilever design, sitting directly on top of the shoulder. With the purpose of not restricting motion, these pads offer less protection.
In a limited report of the NCAA ISS, 12 men’s lacrosse had the fifth-highest overall game injury rate (15.7 injuries per 1000 AEs) among men’s sports, falling below football (39.1 per 1000 AEs), wrestling (23.8 per 1000 AEs), soccer (19.1 per 1000 AEs), and ice hockey (17.7 per 1000 AEs) during the 2004-2005 season. In this same report, the shoulder was the most commonly injured body part during a game during the 2003-2004 season.
Hinton et al 10 conducted a 3-year prospective study of high school lacrosse players in Fairfax County, Virginia, reporting the types, mechanisms, and circumstances of lacrosse injuries in this population. The overall injury rate was 2.89 per 1000 AEs. Shoulder injuries accounted for 8.5% of all injuries (0.24 per 1000 AEs).
Similarly, Xiang et al 23 used the High School Reporting Information Online (RIO) database to describe the epidemiology of high school boys’ lacrosse from 2008-2009 through 2011-2012. They found an overall injury incidence rate of 2.26 per 1000 AEs. Shoulder injury accounted for 6.5% of all injuries and ranked seventh of 10 body sites for frequency of injury.
Dick et al 7 reported on the epidemiology of all men’s lacrosse injuries at the collegiate level, using data from the NCAA ISS from 1988-1989 through 2003-2004. With an incidence of 1.56 injuries per 1000 AEs, the shoulder was the second most commonly injured body part during a game. The practice shoulder injury incidence was reported to be 0.23, making it the fourth most common practice injury in their series.
In the present study, the overall incidence of shoulder injury in intercollegiate men’s lacrosse players was found to be 0.59 per 1000 AEs (95% CI, 0.56-0.62). The incidence of shoulder injuries during practice was 0.35 per 1000 AEs (95% CI, 0.33-0.38) and 1.89 per 1000 AEs (95% CI, 1.76-2.02) during competition, comparable although slightly increased compared with the rates in the series by Dick et al. 7 These data indicate that with the increased participation in men’s lacrosse, the rates of shoulder injuries have increased modestly (from 1.56 to 1.89 per 1000 AEs). Both our data and that of the prior NCAA study report an increased rate of shoulder injury in the collegiate population compared with that of high school players. This may be explained by the increased physicality of play in the older age group. The fact that in this cohort 86.7% of shoulder injuries were due to contact (player contact, contact with playing surface, and contact with apparatus) supports this conjecture.
These data also provide important information on the specific types of shoulder injuries that occur in men’s lacrosse. Of the 21 specific types of injuries coded (Table 2), the most common injury was to the AC joint (50.0%), and the second most common injury was to the labrum (21.8%). This high incidence of labral injuries in men’s lacrosse has not been previously reported and is an important consideration in diagnosing and treating these injuries.
AC Joint Injuries
With an incidence of 0.29 per 1000 AEs (95% CI, 0.27-0.31), AC joint injuries are the most common shoulder injury in intercollegiate men’s lacrosse. In the report by Dick et al 7 of NCAA men’s lacrosse players from 1988-1989 through 2003-2004, the incidence of AC joint injuries during games was 0.64 per 1000 AEs, and the incidence of the same injuries during practices was 0.06, 10-fold less. In our updated group, a similar trend holds true, but the incidence has increased to 1.14 per 1000 AEs (95% CI, 1.05-1.24) and 0.13 per 1000 AEs (95% CI, 0.11-0.13) for games and practices, respectively.
The most common mechanism of AC joint injury in our group was contact with another player (body checking), accounting for 67.7% of injuries. In the typical body check, the player lowers and drives the top of the shoulder into the other player’s body. This forces the shoulder girdle downward and away from the clavicle, leading to potential injury to the acromioclavicular and/or coracoclavicular ligaments. Contact with the playing surface was responsible for nearly all of the remaining AC joint injuries (28.9%). A similar mechanism occurs when a player falls and is driven into the ground, leading to a direct blow to the top of the shoulder and separation of the AC joint.
Less than half of all players who sustained an AC joint injury were able to return to play within 1 week (44.5%), with 30.2% out for at least 2 weeks. Of athletes with AC joint injuries, 49% would meet the study definition by Dick et al 7 of 10+ days lost as a marker of a severe injury, attesting to the morbidity of the injury.
As previously mentioned, the required shoulder pads in men’s lacrosse are noncantilevered and rest on top of the shoulder. The above data suggest that their design does not adequately protect the shoulder. This may be due to their mobility or insufficient padding. Further attention to their design, including a better padded and less mobile structure, may help to decrease the incidence of these injuries.
Labral Injuries (Superior, Posterior, Anterior) and Instability Events (Subluxations and Dislocations)
Particularly notable in this report and previously underrecognized is the high incidence of shoulder labral injuries and instability events. In aggregate, they account for 21.8% of all shoulder injuries in NCAA men’s lacrosse, occurring with an incidence of 0.11 per 1000 AEs (95% CI, 0.09-0.13).
Some typical maneuvers that occur in men’s lacrosse lead to unique mechanisms of labral injury. Body checking typically involves contact at the shoulder level with both hands on the stick, followed by pushing forward of both arms, extending the elbows, flexing the shoulders, and protracting the scapula. This constellation of forces, like blocking by football linemen, leads to a net posterior force on the shoulder and, as in football, may lead to posterior labral injury. The face-off is another unique event that may also be associated with labral injury. The face-off player crouches with both hands on the stick, which is positioned flat on the ground. The player then pushes both arms forward to clamp the ball, while twisting the stick to gain possession. This maneuver leads to both a rotational force in the shoulder and a posteriorly directed force; this shearing may also lead to labral injury.
Posterior shoulder injury has previously been reported in athletes who subject their shoulders to repeated posteriorly directed shear forces. Mair et al 16 described posterior labral injuries in a series of 9 contact athletes, a group composed of 8 football linemen and 1 lacrosse player. In the Mair et al 16 series, the lacrosse athlete recalled the moment of injury to have occurred when holding his stick in front of his body. He then suffered a posteriorly directed blow with the shoulder forward-flexed and the elbow locked in extension. At surgery, he, along with all of the football linemen, had posterior labral detachment. 22
The current study found that posterior shoulder subluxation/dislocation was a rare event, with an incidence of 0.02 per 1000 AEs (95% CI, 0.01-0.02). In accordance with that proposed by Mair et al, 16 the most common mechanism of posterior instability was contact with another player, accounting for 47.1% of these injuries. Contact with the playing surface and shooting were the cause of the remaining injuries. Most players with a posterior shoulder injury were able to return to play within 1 week (52.9%). However, 31.4% required more than 2 weeks; of these, 15.7% did not return to play during that season. This attests to the potential severity of these injuries.
The mechanism of anterior-inferior labral tear with shoulder subluxation/dislocation occurs in most collision sports and has been well described. An anteriorly directed force with the arm in abduction and external rotation leads to tearing/avulsion of the anterior-inferior glenohumeral ligament and capsulolabral complex. If a player is checked and makes contact with the ground with the arm in an abducted and externally rotated position, the shoulder may dislocate in an anterior-inferior direction, leading to anterior and inferior labral injury. In our population, anterior labral injuries (dislocation, subluxation, and labral tear) had a combined incidence of 0.09 per 1000 AEs (95% CI, 0.08-0.10). These results are similar to the overall incidence of instability events occurring in collegiate sports, reported by Owens et al. 19 In their series, a total of 4080 glenohumeral instability events were documented, resulting in an incidence rate of 0.12 injuries per 1000 AEs.
Fractures
In its classification of shoulder injuries, the NCAA includes fracture of the scapula, proximal humerus, and clavicle. Of note, it is unknown whether the scapular fractures are those of the body or glenoid fractures associated with an instability event (bony Bankart). In our cohort, there were no reported humerus fractures. The incidence of each scapular and clavicle fracture was 0.01 per 1000 AEs (95% CI, <0.01-0.01) in this population. Hinton et al 10 reported the incidence of all fractures in boys’ high school lacrosse to be 0.27 per 1000 AEs, but they did not classify them according to the site of the fracture. Similarly, Xiang et al 23 reported the incidence of any fracture in boys’ high school lacrosse to be 0.25 per 1000 AEs.
The mechanism of injury for these injuries in our study was similar to that seen with AC joint injuries. Most were due to contact with another player, whereas the remainder were due to contact with the playing surface. As with AC joint injuries, clavicle fractures are due to a direct blow to an area protected by shoulder pads. Thus, it is likely that improvements to shoulder pads could help to decrease this injury rate. Neither of the athletes who suffered a clavicle fracture was able to return to play during that season. Both players with scapular fractures returned to play; however, it was after 20 and 65 days, respectively.
Game Versus Practice
Dick et al 7 found that, overall, athletes were 4 times more likely to have an injury during a game than in a practice (12.58 vs 3.24 injuries per 1000 AEs for games and practice exposures, respectively). Similarly, in the high school population, Hinton et al 10 found the overall rate of injury to be 4.44 per 1000 AEs, whereas the rate of injury during practice was 1.40 per 1000 AEs. In the series of collegiate athletes reported by Owens et al, 19 athletes sustained more glenohumeral instability events during games than practices (incidence rate ratio [IRR], 3.50; 95% CI, 3.29-3.73).
Similar to prior reports, we found that shoulder injuries were 5 times more common during games than in practices. Dick et al 7 hypothesized that this finding was to be expected, due to the sustained elevated intensity of game play. Athlete exposure during practice likely involves periods of instruction, conditioning, and noncontact drills, in addition to drills and scrimmages that are similar to game play. This is substantiated by the findings of an NCAA ISS report of all men’s lacrosse injuries reported during the 2005-2006 season, which found that in a practice environment, a noncontact mechanism was responsible for 49% of all reported injuries, whereas contact with another player was causative in 25%. 12 However, during competition, noncontact injuries accounted for only 25% of those reported, while contact with another athlete was the listed mechanism for 52%.
Mechanism of Injury
In his study of high school boys’ lacrosse, Xiang et al 23 found that 40.9% of all injuries were due to contact with another player. Dick et al 7 reported that 45.9% of all game injuries resulted from player contact. Owens et al 19 also found that male collegiate athletes were more likely to sustain a glenohumeral instability event from player contact (IRR, 2.74; 95% CI, 2.31-3.25) than other mechanisms. Our findings corroborate these studies, with 57.5% of all shoulder injuries caused by contact with another player. Nearly 25% of the remaining shoulder injuries were reported to be due to contact with the playing surface. Whether a change in playing surface could potentially affect the incidence of shoulder injury is unknown and deserves further study.
Time Loss
Due to limitations in the data collected, neither the NCAA ISS nor other similar injury databases have specific details regarding the severity of injuries. As such, it is necessary to use surrogate markers. Time loss has been previously used for this purpose.7,10 A threshold of ≥10 days of time loss was chosen to allow for comparison with prior studies.7,19
In our study, 41.9% of all injuries necessitated ≥10 days of recovery prior to return to play. This is comparable with that reported by Owens et al, 19 in which time lost to sport (>10 days) occurred in 45% of glenohumeral instability events. Shoulder injuries are particularly limiting in men’s lacrosse, since shoulder braces are poorly tolerated and may restrict motion in a sport where overhead activity is necessary. Table 3 lists the shoulder injuries for which the average time loss was ≥10 days. This information is useful to help advise players, coaches, and medical professionals when handling these injuries during the season.
Only 3.7% of all shoulder injuries in this series were season ending. Table 3 includes the percentage of each specific injury that was season ending. This, too, is very useful in counseling athletes regarding their likelihood of returning to play.
Limitations
While it has been consistently used as a source of quality epidemiologic data for American collegiate athletics, the NCAA ISS does have limitations. While they collect data from a “convenience sample” of institutions sponsoring intercollegiate men’s lacrosse and assign weights to injuries and exposures to allow extrapolation to the entire NCAA population, many sponsoring schools are not sampled. This introduces the possibility for either overestimation or underestimation of the incidence of injury. In a validation study, Kucera et al 14 found that the NCAA ISS captured 88.2% of all time-loss injuries in men’s and women’s soccer. Division II schools are particularly underrepresented in this population, with no data collected for 3 of the 5 years studied. This could raise concerns about the applicability of these data to that specific population.
Another limitation of a database study such as this is that all injury data are reported by athletic trainers and are not further validated by a sports medicine physician. The athletic trainers are also limited to the confines of the designed system. For example, when reporting AC joint injuries, there are only 2 categories: partial (Rockwood 1 or 2) and complete (Rockwood ≥3). This is a simplified system, with no allowance for free text comments. As such, some of the details of specific injuries may be lost. Furthermore, clinical follow-up and treatment decision making are not captured in this database. This limits our ability to judge injury severity, beyond time loss. The use of time loss as a surrogate for injury severity is also limited, as this is subject to great variability at the hands of different medical providers. In addition, the use of “season ending” also does not provide specific information regarding the timing of the injury within the season. Thus, season ending could mean any number of actual days lost. Despite these limitations listed above, this method of data collection has been previously validated in epidemiologic studies of American collegiate athletics. Therefore, we believe that this method allows the most current and representative presentation of shoulder injuries within the sport of American intercollegiate men’s lacrosse.
Areas of Future Research
Similar to prior reports of men’s collegiate lacrosse injuries, 7 we found injuries to the AC joint to be common and an important area of future research. The efficacy of current shoulder pads has not been investigated and may reveal the potential for significant injury prevention. In our study, we also found a high incidence of labral injuries in men’s lacrosse. This is an area that has not been emphasized previously and deserves further study.
Conclusion
Men’s lacrosse is one of the fastest growing sports in the United States, including at the intercollegiate level. It is a unique sport, with injury risks factors commonly associated with both contact and overhead sports. As such, it is essential to understand the epidemiology of men’s lacrosse shoulder injuries.
We found that AC joint injuries continue to be particularly common, despite shoulder pads, which are meant to protect this area. For the first time, we demonstrated the high incidence of labral and instability injuries in men’s lacrosse. Finally, this study emphasizes the potentially serious nature of shoulder injuries in men’s lacrosse, with 41.9% of all shoulder injuries necessitating at least 10 days of time loss. This information will also help to guide future injury prevention programs, including alterations to equipment and rules, to protect the athletes.
Footnotes
Acknowledgements
The authors thank the many athletic trainers who have volunteered their time and efforts to submit data to the NCAA Injury Surveillance Program. Their efforts are greatly appreciated and have a tremendously positive effect on the safety of collegiate athletes.
The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official view of the Datalys Center or the National College Athletic Association.
One or more of the authors has declared the following potential conflict of interest or source of funding: The NCAA Injury Surveillance Program data were provided by the Datalys Center for Sports Injury Research and Prevention. The Injury Surveillance Program was funded by the National College Athletic Association (NCAA).