
Abstract
Background:
Subchondral bone overgrowth has been described with variable frequency after microfracture, but little systematic information is available about the clinical incidence, risk factors, or clinical relevance of this phenomenon.
Hypothesis:
Subchondral overgrowth (1) occurs with high incidence and various degrees after microfracture, (2) is associated with risk factors, and (3) affects clinical outcome score and failure rate.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 84 patients undergoing microfracture in the knee were prospectively followed up to 6 years postoperatively through use of cartilage-sensitive magnetic resonance imaging to detect the incidence of subchondral bone overgrowth. The quantity of the overgrowth was graded systematically and was then correlated to patient and lesion characteristics, surgical technique, validated functional outcome scores, and failure rate.
Results:
Subchondral bone overgrowth was observed in 62% of patients at a mean of 22 months after surgery. Most bone overgrowth (64%) was low grade and developed during the first 12 months after microfracture. Risk factors for bone overgrowth included high body mass index, defects on the lateral femoral condyle, and aggressive debridement of the calcified cartilage layer. Knee injury and Osteoarthritis Outcome Score results were not significantly different between patients with or without subchondral bone overgrowth. However, 93% of patients who failed microfracture demonstrated osseous overgrowth, and patients with osseous overgrowth showed a significantly higher failure rate (25%) than patients without overgrowth (3.1%; P < .01).
Conclusion:
Subchondral bone overgrowth is frequently observed after microfracture surgery but is mostly of low grade. Several risk factors were identified that can affect the incidence of this phenomenon. Importantly, subchondral overgrowth is associated with an increased rate of postoperative failure after microfracture.
Focal defects of articular cartilage remain a frequent cause of pain and functional limitation, often resulting in surgical intervention. Several different treatments have been proposed and studied. 15 As early as 1959, Pridie 16 proposed drilling of the defect as a method to promote bleeding and recruit bone marrow elements to reconstitute cartilage in the lesion. In the 1990s Steadman introduced microfracture, which remains the most commonly performed cartilage repair technique because of its technical simplicity, limited patient morbidity, and satisfactory overall results.1,3,11-15,17,23 Using the principle of marrow stimulation, the microfracture technique includes debridement of the defect, removal of the calcified cartilage, and penetration of the subchondral bone with specifically designed awls. To date, microfracture is still the gold standard technique against which new cartilage repair technologies are compared. However, it is well recognized that microfracture is not a panacea, as the repair cartilage formed is biomechanically and histologically different than normal hyaline articular cartilage. The limited quality of the fibrohyaline repair cartilage has been suggested as one factor responsible for the functional deterioration seen in some patients after initial improvement after microfracture. In addition to the quality of cartilage repair tissue, changes to the subchondral bone plate including cysts, edema, and more recently subchondral osseous overgrowth have been described and are considered as potential risk factors for the observed functional deterioration after microfracture. 4 The phenomenon of bony overgrowth, also referred to as intralesional osteophyte or elevation of subchondral bone plate, is being identified in an increasing number of studies, with a reported incidence of 10% to 99%.4,5,7,10,14,15,19,21 It has been suggested that subchondral overgrowth results in a thinning of the overlying repair cartilage layer with alterations in cartilage biomechanics and that this process may play an important role in the outcome after microfracture. However, little systematic information is available about the causes, risk factors, and clinical relevance of subchondral overgrowth. Therefore, the purpose of this study was to prospectively identify the incidence of subchondral overgrowth after microfracture, provide a quantitative measure and grading, define associated risk factors, and evaluate the clinical relevance of subchondral overgrowth.
Methods
All patients who underwent microfracture for symptomatic articular cartilage lesions in the knee by a single surgeon between 2005 and 2011 were prospectively included in the study with the specific purpose of evaluating subchondral bone changes after microfracture. Appropriate approval of the institutional review board was obtained for this study. Besides patient demographics, body mass index (BMI) and lesion characteristics such as number of lesions, lesion size, and location were recorded. Associated meniscal and ligamentous injuries and their treatment were also recorded. Intraoperative surgical data included the type of microfracture instrumentation (awl), number of holes placed per square centimeter, and depth of calcified cartilage layer debridement. Postoperative evaluation included magnetic resonance imaging (MRI) using a previously described cartilage-sensitive MRI sequencing protocol.4,15 MRI was performed in a 1.5-T magnet (Signa Horizon LX; General Electric Medical Systems) with use of either a linear receive-only knee extremity coil or a transmit-and-receive phased-array coil. Fast-spin-echo images were acquired in 3 planes through use of a repetition time of 3500 to 5000 ms, an echo time of 34 ms (effective), a field of view of 13 to 16 cm2, and a matrix of 512 × 256 to 354, providing a maximum in-plane resolution of 254 μm in the frequency direction by 406 μm in the phase direction by a slice resolution of 3 to 3.5 mm with no gap. MRI was performed for study purposes and not on the basis of clinical symptoms; serial MRI was conducted at predefined postoperative intervals set at 6, 12, 24, 36, and 48 months after microfracture. MRI results were evaluated by a blinded musculoskeletal specialist for evidence of osseous overgrowth. Since grading of osseous overgrowth has not previously been described, a grading system was developed based on the amount of bone overgrowth in relation to the fill of the defect similar to a grading system previously described for quantifying the amount of repair cartilage tissue fill after cartilage repair. 4 Grades were defined as 0 to 3, with grade 0 presenting no overgrowth; grade 1 showing overgrowth filling 1% to 33% of the depth of the defect; grade 2 presenting overgrowth of 34% to 66%, and grade 3 presenting with greater than 67% of the defect filled by bony overgrowth (Figure 1). The degrees of overgrowth were blindly assigned in 2 independent assessments for each MRI and demonstrated intraobserver reliability of greater than 90%. The final degree of overgrowth seen on serial MRI was used for statistical calculations.
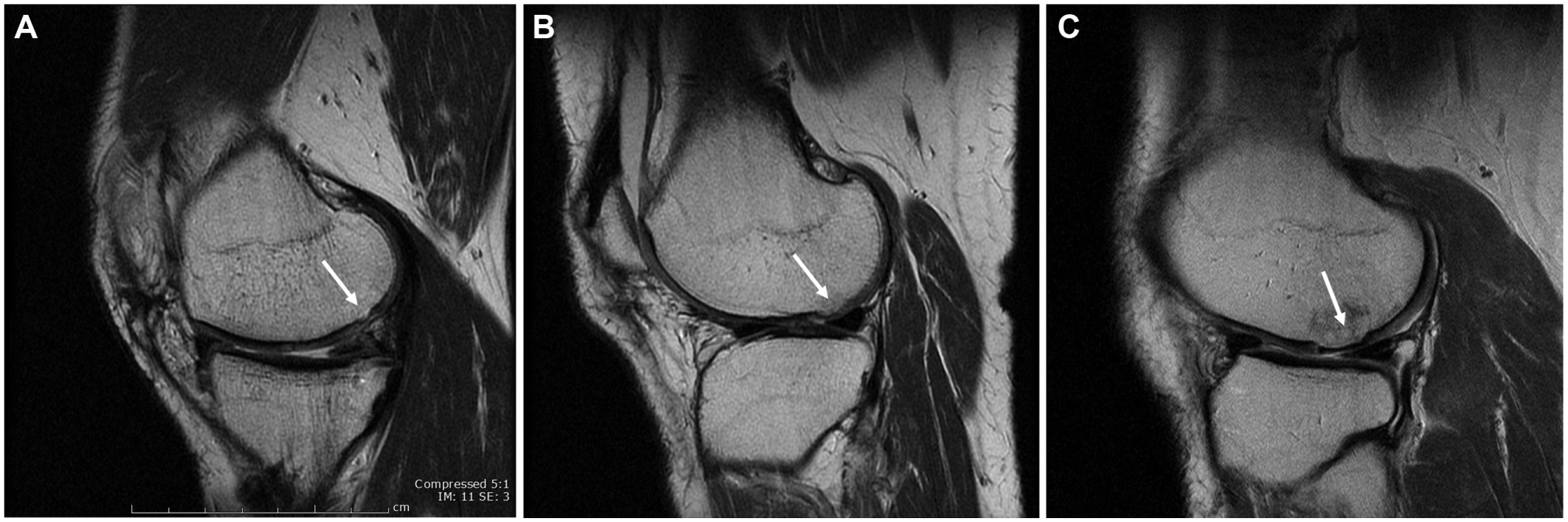
Magnetic resonance images demonstrating the grades of subchondral overgrowth after microfracture (arrows): (A) grade 1, (B) grade 2, and (C) grade 3.
Postoperative clinical outcome evaluation was performed with the Knee injury and Osteoarthritis Outcome Score (KOOS), an outcome score validated for cartilage repair, as well as the incidence of clinical failure after microfracture. Patients were defined as clinical failure if they had persistent severe joint symptoms and dysfunction requiring additional surgical treatment of the cartilage defect after the index microfracture.
Instrumentation used for microfracture in this study included 2 different types of awls with diameters of 3.81 mm (Conmed-Linvatec) and 5.1 mm (Arthrex). Calcified cartilage debridement was performed with a previously described technique that entailed a ring curette. Calcified cartilage debridement was defined as aggressive or deep if it resulted in any visible bleeding from the underlying subchondral bone indicating deep debridement into the cancellous portion of the subchondral bone.
Postoperative rehabilitation was standardized by use of a previously described protocol and entailed the same progression of postoperative weightbearing for all patients with isolated cartilage lesions and patients with concomitant adjuvant procedures such as ligament reconstruction.4,15 In patients with femoral condylar lesions, weightbearing was avoided for 2 weeks and then increased by 25% of body weight per week. Patients with trochlear lesions were allowed to bear weight as tolerated with a hinged knee brace at full extension. Continuous passive motion was started after 24 hours at 0° to 40° and was continued for 6 hours per day for 6 weeks. Range of motion was advanced as tolerated under supervision by a therapist.
Statistical analysis was performed with Microsoft Excel and SAS software (version 9.3; SAS Institute Inc). Study patients were divided into groups based on the presence or absence of osseous overgrowth as well as the grade of overgrowth. Logistic regression analysis was used to compare groups and evaluate for risk factors based on odds ratio (OR) and 95% confidence interval (CI). All patient and surgical variables were included in the analysis regardless of their univariate association. After the initial analysis, multiple regression analysis was performed through use of stepwise variable selection to control for any confounding factors. The Wilcoxon rank sum test was used to evaluate KOOS scores between groups. Nominal data (yes/no) were analyzed with the Fisher exact test. Bonferroni correction was used for multiple comparisons. P < .05 was considered significant.
Results
A total of 84 patients (94 lesions) underwent microfracture between 2005 and 2011. The mean age of patients was 46.2 years. Patient demographics, lesion characteristics, and procedure information are detailed in Table 1. Overall clinical follow-up was conducted for a mean of 23.9 months (range, 6-81 months) with a mean MRI follow-up of 22.3 months (range, 6-72 months). MRI at a mean of 12 months demonstrated evidence of subchondral osseous overgrowth in 39 patients (46.4%). After an initial negative MRI, 13 additional patients developed overgrowth on subsequent MRI, resulting in a total of 52 patients (62%) with osseous overgrowth at a mean of 22 months after microfracture. The mean length of follow-up was longer in patients with overgrowth compared with those without overgrowth (26.2 vs 17.1 months: OR, 1.045; 95% CI, 1.01-1.08). Of the 52 patients with overgrowth, 33 (63.5%) demonstrated grade 1 overgrowth, 15 (28.8%) demonstrated grade 2 overgrowth, and 4 (7.6%) demonstrated grade 3 overgrowth (Figure 2).
Patient Characteristics, Risk Factors for Overgrowth, and Related Outcomes a
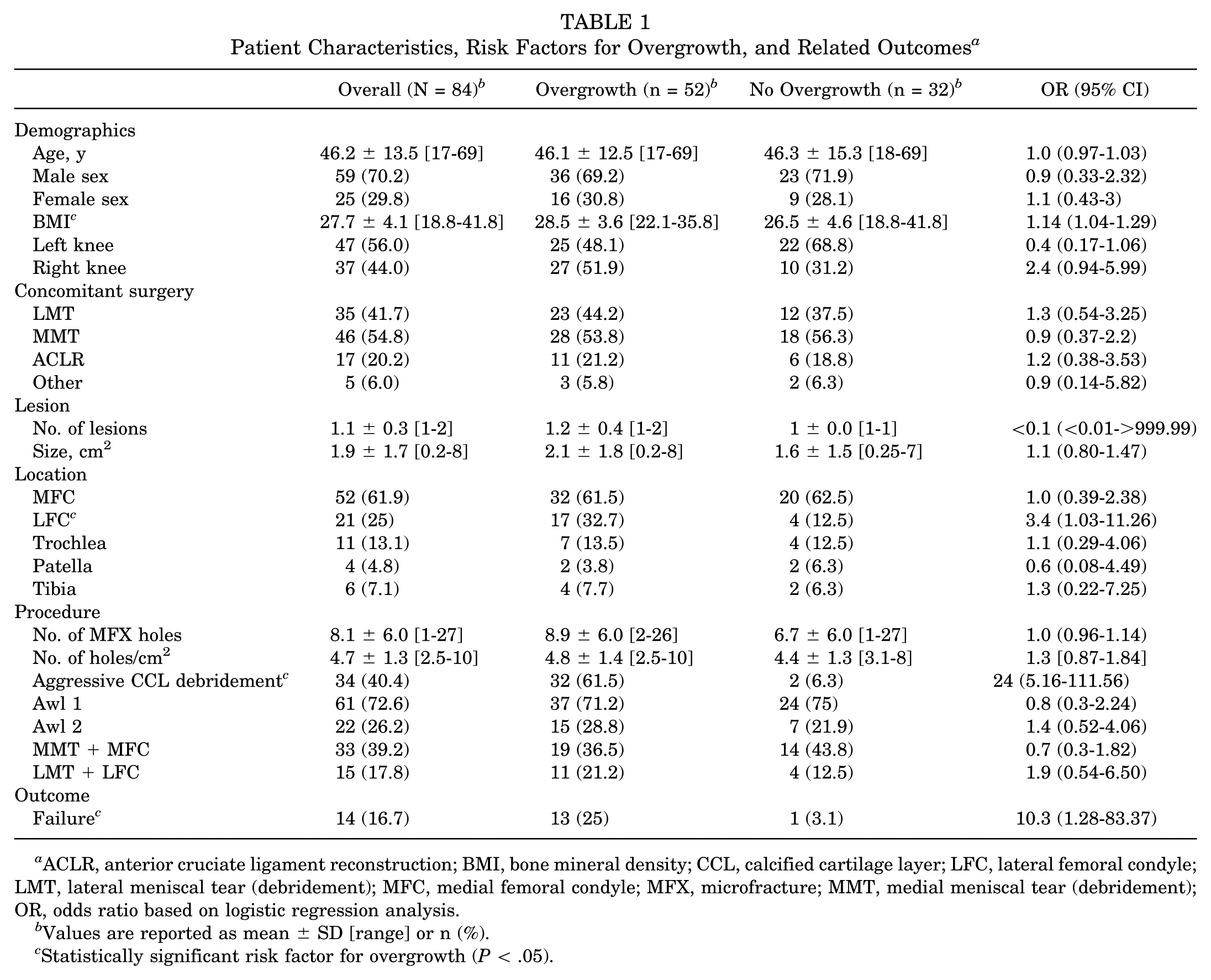
ACLR, anterior cruciate ligament reconstruction; BMI, bone mineral density; CCL, calcified cartilage layer; LFC, lateral femoral condyle; LMT, lateral meniscal tear (debridement); MFC, medial femoral condyle; MFX, microfracture; MMT, medial meniscal tear (debridement); OR, odds ratio based on logistic regression analysis.
Values are reported as mean ± SD [range] or n (%).
Statistically significant risk factor for overgrowth (P < .05).
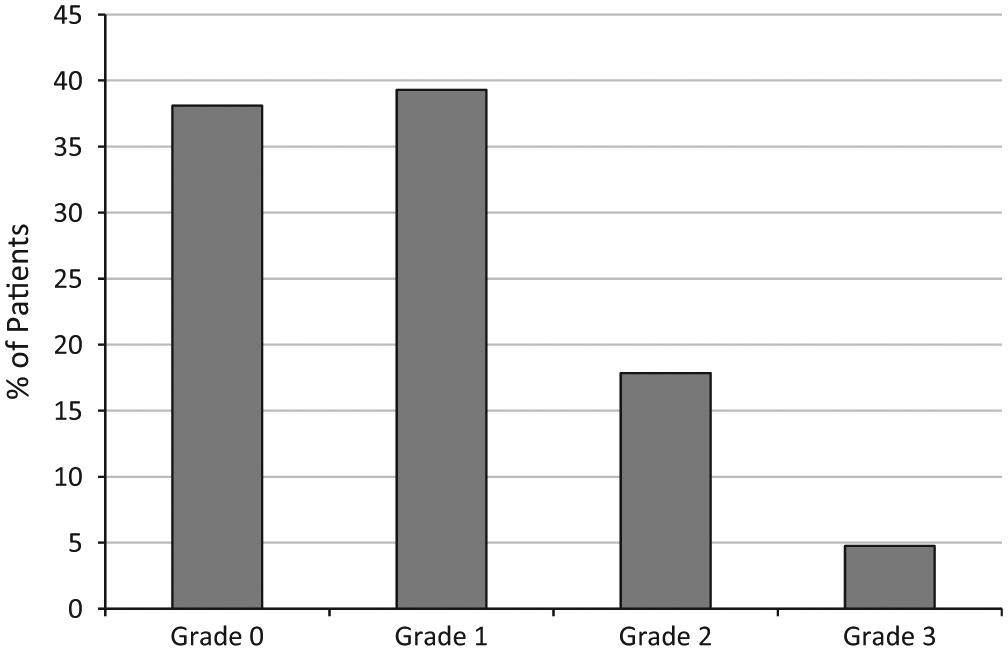
Incidence of individual grades of subchondral bone overgrowth after microfracture in all patients (N = 84).
Comparative analysis of patients with and without overgrowth is shown in Table 1. Statistically significant risk factors for bony overgrowth found on logistic regression analysis included BMI (OR, 1.14; 95% CI, 1.04-1.29), lesion location on the lateral femoral condyle (OR, 3.4; 95% CI, 1.03-11.16), and aggressive, deep removal of the calcified cartilage layer (OR, 24; 95% CI, 5.16-111.56). Age, sex, side, meniscal tears in the same compartment, concomitant procedures, defect number, defect size, and microfracture hole diameter (awl size) were not found to correlate with overgrowth incidence or grade. Although a trend was noted for a higher number of holes per surface area in lesions with subchondral overgrowth (8.9 vs 6.7 holes per square centimeter), this did not reach statistical significance. Multiple logistic regression analysis for improved control of statistical variables confirmed that aggressive removal of the calcified cartilage layer was the most significant risk factor for subchondral bone overgrowth after microfracture.
Overall KOOS scores for patients with overgrowth were not significantly different than scores of patients without overgrowth (median 81 and 83 points, respectively). Similarly, subscore analysis for pain, symptoms, activities of daily living (ADL), sports and recreation, and quality of life (QoL) demonstrated no significant effect of subchondral overgrowth (Figure 3). Comparison of KOOS scores based on grade of osseous overgrowth demonstrated no significant effect of overgrowth grade on knee function after microfracture (Figure 4). Accordingly, individual component subscores for symptoms, pain, ADL, sports and recreation, and QoL did not show differences between the degrees of overgrowth. Median KOOS scores were significantly lower in patients for whom treatment failed (68.8 vs 84.2; P = .01).
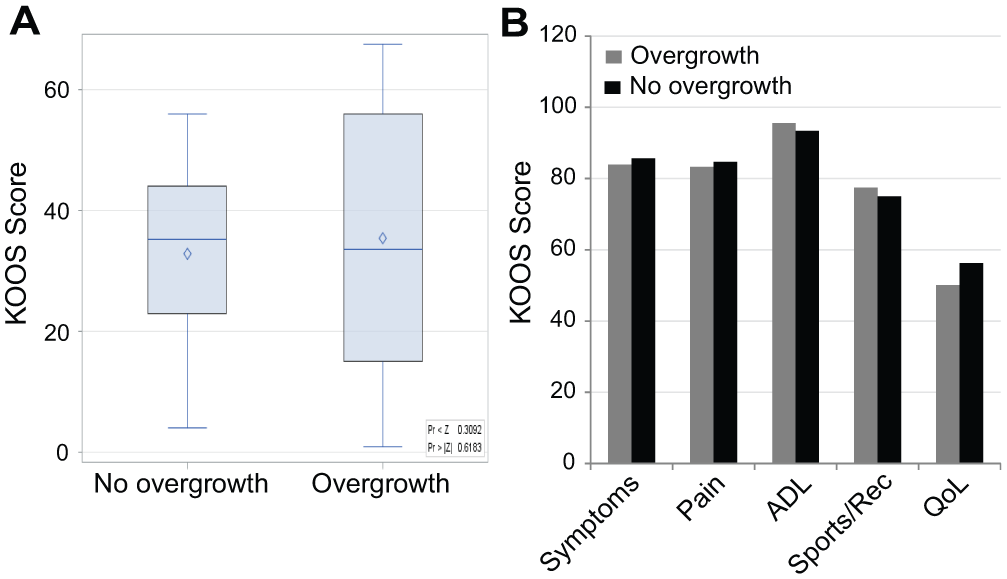
(A) Overall scores and (B) subscores on the Knee injury and Osteoarthritis Outcome Score (KOOS) after microfracture of the knee in patients with and without subchondral overgrowth. ADL, activities of daily living; QoL, quality of life; Sports/Rec, sports and recreation.
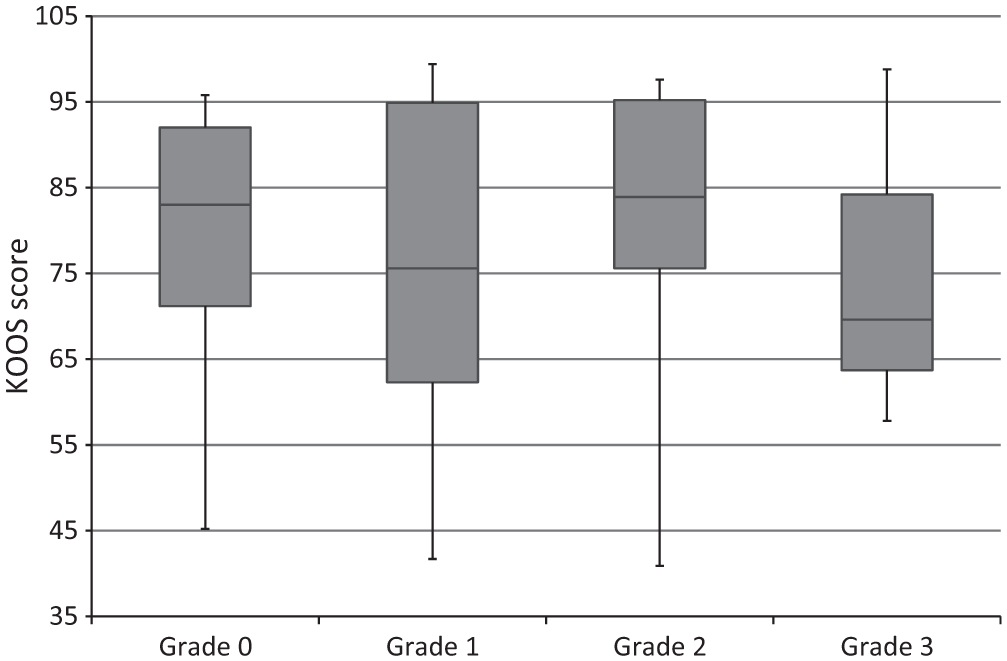
Comparison of Knee injury and Osteoarthritis Outcome Score (KOOS) results based on grade of subchondral bone overgrowth.
Fourteen (16.7%) patients went on to clinical failure after their microfracture procedure. Mean time to failure was 30.3 ± 17.9 months. Thirteen of 14 patients (93%) who experienced failed microfracture demonstrated evidence of overgrowth (OR, 10.3; 95% CI, 1.3-83.4). The failure rate in the overgrowth group was 25% (13/52) and was significantly higher than the failure rate of 3.1% (1/32) seen among patients without overgrowth (P < .01) (Figure 5). The failure rate was 27.3% (9/33) in patients with grade 1 overgrowth, 20% (3/15) in patients with grade 2, and 25% (1/4) in patients with grade 3. One failure occurred in a patient without overgrowth. Patient and lesion characteristics, meniscal status in the involved compartment, concomitant procedures, number of microfracture penetrations per surface area, and microfracture hole diameter did not have a significant effect on failure.
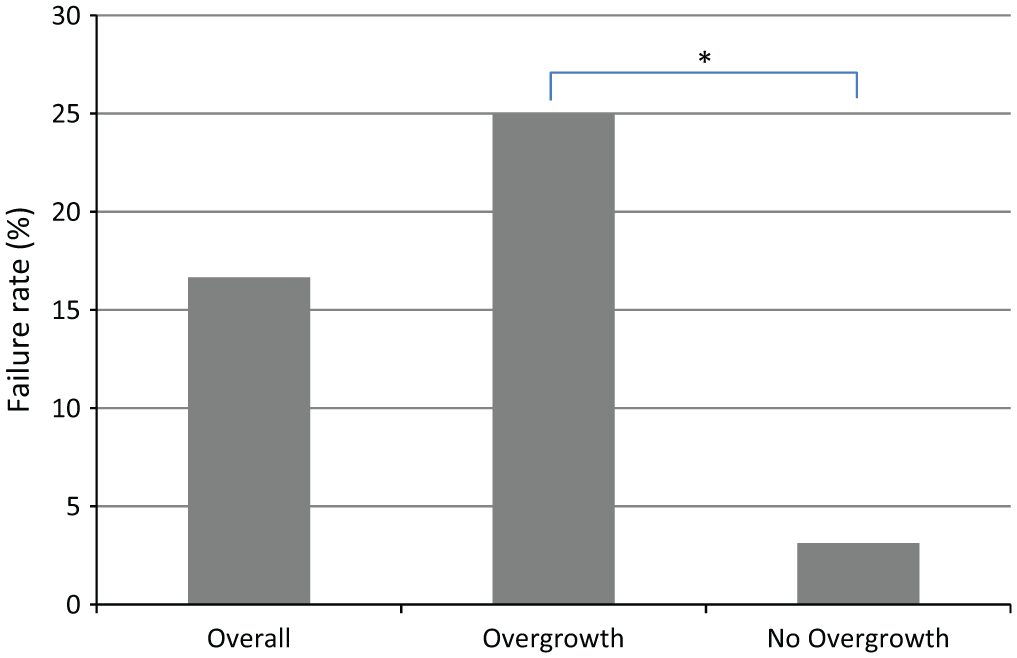
Comparison of the failure rates after microfracture overall and with and without subchondral bone overgrowth (*P < .05).
Discussion
The phenomenon of osseous overgrowth in cartilage defects treated with microfracture has been increasingly recognized but still is not well understood.4,5,7,10,14,15,19,21 This study was designed to improve the clinical understanding of bone overgrowth by systematically investigating the incidence and extent of osseous overgrowth after microfracture but also by identifying the risk factors and, most important, defining the relevance of osseous overgrowth for clinical outcome. Osseous overgrowth in our study was observed in 62% of patients, which falls within the reported incidence of 10% to 99% described in previous studies.4,5,7,10,14,15,19,21 Recent literature demonstrates a trend toward increasing reported incidence of osseous overgrowth, which likely reflects the improved sensitivity of MRI with higher resolution and improved sequencing over time. This is consistent with a recent study using sophisticated 3-dimensional quantitative software analysis of MRI that demonstrated overgrowth in virtually all cases. However, that study found highly variable volume of the osseous overgrowth, ranging from <10% to 80% of the involved defect, with most overgrowth described as spotty and minor. 21 This finding is consistent with our study, which demonstrated that the majority of osseous overgrowth after microfracture was of low grade.
Our study demonstrated that the incidence of overgrowth increased over time from 46% at 12 months after microfracture to 62% at final follow-up. Similarly, Cole et al 7 observed an increase from 54% to 70% during the observation period after microfracture. Saris and coworkers 19 observed increasing overgrowth over time after microfracture in a randomized comparison with chondrocyte transplantation. Their findings, as well as ours, suggest that most osseous overgrowth after microfracture occurs between 6 and 12 months postoperatively, but further long-term study is required to completely evaluate the timeline of development of osseous overgrowth.
The current study used a grading system of osseous overgrowth to allow for a more subtle characterization of this phenomenon and to improve evaluation of its clinical presentation and relevance. We devised a system of overgrowth grades from 0 to 3 based on the amount of fill of the repaired cartilage lesion by bony overgrowth. A similar grading system was previously described to classify the amount of repair cartilage fill in articular cartilage defects after cartilage repair and demonstrated that fill grade correlated with functional outcome after cartilage repair.4,15 Since increasing fill of the cartilage defect by osseous overgrowth decreases the volume of repair cartilage tissue in the repaired articular cartilage defect, it was hypothesized that the amount of osseous overgrowth may increasingly affect the biomechanics of the repair cartilage and outcome after microfracture. However, our study did not show a significant effect of the degree of overgrowth on functional outcome scores or failure rate. The lack of effect of overgrowth grade on outcome may have resulted from the relatively lower number of patients with high-grade overgrowth in our study. A similar distribution of the severity of osseous overgrowth with a predominance of low-grade overgrowth was seen in one other recent study. 21 However, our study suggests that even low amounts of osseous overgrowth can be associated with clinical failure after microfracture. While our data are helpful in defining and identifying the incidence of the variable degrees of bony overgrowth after microfracture, further study is needed to better systematically investigate this aspect.
The cause of the subchondral osseous overgrowth is not clearly understood. Previous studies have theorized that overgrowth may be inherent to the process of microfracture itself, as the procedure involves disrupting the subchondral bone plate and creating vascular and marrow access to recruit pluripotent mesenchymal stem cells that can undergo both osteogenic and chondrogenic differentiation.2,5 Additional influence from mechanical loading and the physiological environment has been suggested. 8 Besides the lack of information about the pathophysiological process of bony overgrowth, little or no information is available in the literature about the factors that affect development of bony overgrowth after cartilage repair with microfracture. Our data show that BMI and lesion location on the lateral femoral condyle presented significant risk factors for bone overgrowth after microfracture. Both BMI and lesion location have been shown to affect cartilage repair after microfracture, 15 and the stimulatory effect of increased load resulting from higher BMI and the focal loading biomechanics in the lateral compartment on the subchondral bone may explain this finding.
Recent studies have suggested that technical aspects of microfracture may be relevant since penetrating the subchondral bone with a conical awl was shown to significantly affect subchondral bone morphologic characteristics. 6 Our study provides important additional technical information as it shows that neither the diameter of the awl tips nor the penetrations per surface area of the defect had a significant effect on the incidence of subchondral bone overgrowth. Importantly, however, the technique of calcified cartilage removal had a significant effect on the incidence of subchondral overgrowth. Previous authors have pointed out the importance of removing the calcified cartilage layer for adhesion of the clot as well as subsequent diffusion of nutrients from subchondral bone to overlying neocartilage.1,2 An equine study on microfracture with and without removal showed evidence of poorer macroscopic and microscopic cartilage repair when the calcified cartilage layer was not debrided. 9 The exact technique of calcified cartilage removal has not been described in detail, but our results suggest that aggressive, deep removal of the calcified cartilage layer that penetrates significantly into the subchondral bone with resultant bleeding in the area presents a significant risk factor for overgrowth. The stimulatory effect of the bone marrow contents as well as associated local accumulation of stimulatory growth factors from bone marrow and blood cells could explain the focal subchondral bone reaction. This theory could also explain why subchondral overgrowth is observed in other cartilage repair techniques, for example, in up to 64% of chondrocyte transplantations, since curettage of the base of the cartilage defect in this technique can sometimes be associated with focal punctuate bleeding as well.4,6,7,14,19,24 Our study suggests that gentle, superficial debridement that avoids bleeding is preferable to aggressive debridement. 3 The calcified cartilage removal technique has not been standardized, making this part of the microfracture procedure difficult to perform correctly even for the experienced surgeon. Gentle debridement of the defect bed during microfracture seems to be a critical step to avoid subchondral overgrowth and may help to reduce failure rate from this commonly used cartilage repair technique.
Interestingly, our study demonstrated that subchondral osseous overgrowth did not seem to statistically affect knee function, as KOOS scores and subscores were not significantly affected by subchondral overgrowth. Only one other study has assessed the clinical effect of subchondral bone overgrowth after microfracture. A recent study by Shive et al 21 also demonstrated no significant difference in KOOS scores at follow-up of 12 months. The lack of effect on clinical function scores in their study and ours may be the result of the predominance of a low grade of osseous overgrowth in both studies.
Importantly, our study demonstrated the clinical failure rate to be significantly higher in patients with osseous overgrowth compared with those without. In fact, patients who demonstrated osseous overgrowth were 10 times more likely to experience failed microfracture surgery in our study, and more than 90% of patients whose microfracture failed had osseous overgrowth. Our overall failure rate of 16.7% after microfracture was similar to the rates described in other studies.2,4,14,18,22 No other studies have investigated failure rate related to osseous overgrowth. Our finding of increased failure associated with overgrowth confirms speculations in previous studies that bony abnormalities and thinning of the cartilage layer over areas of overgrowth may affect long-term durability and outcome of repair cartilage.1,14,15,20
Whether the grading of the defect did affect failure rate cannot be conclusively determined from our study since the majority of cases showed grade 1 overgrowth with only occasional grade 3 overgrowth. However, the fact that several cases with only grade 1 overgrowth went on to fail microfracture suggests that this phenomenon even at low grade may affect the biomechanics and durability of the repair cartilage tissue. This is important since a subgroup of patients after microfracture demonstrate decreasing joint function after initial functional improvement with an associated increase in clinical failure and need for surgical revision. The observed effect of subchondral bone overgrowth in our study offers a potential explanation for the functional deterioration and failure after initial improvement after microfracture in this subpopulation. It can be speculated that reducing the risk for subchondral overgrowth may also reduce the rate of failure after microfracture. Further systematic study is warranted to evaluate this assumption.
The present study provides new information; however, several limitations should be considered while interpreting the data. The prospective nonrandomized design of this study introduces the possibility of selection bias for patients receiving microfracture. We attempted to limit such bias by including only consecutive patients who fit the previously described indication criteria for microfracture. 15 The limited patient numbers, especially in some of the subgroup analyses, might have generated type II error. A further limitation may be related to the difference in follow-up between our patients with and without osseous overgrowth. This was addressed by using multiple regression analysis of the available data, but inherently some level of error remains. Strengths of this study include the length of follow-up compared with previous studies discussing subchondral overgrowth after microfracture as well as our unique assessment of risk factors and failure rate, which have not previously been studied. The uniformity of the operative approach by a single surgeon and consistent postoperative rehabilitation presents another strength of the present study.
In summary, our study demonstrates a high incidence of osseous overgrowth after microfracture surgery. This overgrowth can be classified based on the amount of bone formation, but insufficient data prevent a definitive conclusion on the effect of the overgrowth grade on outcome. The finding that patients with overgrowth have a 10-fold higher failure rate after microfracture is the most clinically relevant finding of this study. Besides BMI and lesion location in the lateral compartment, aggressive deep debridement of the calcified cartilage layer within a lesion presents the most significant risk factor for osseous overgrowth. This suggests that careful attention to this technical step is important to optimize outcomes after microfracture. Further systematic research is required to better delineate the details of the biomechanical and clinical effect of subchondral bone overgrowth and its relevance not only for microfracture but also for second-generation microfracture-based cartilage repair technologies.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.