
Abstract
Background:
Hip arthroscopic surgery has emerged as a successful procedure to manage acetabular labral tears and concurrent hip injuries, which if left untreated, may contribute to hip osteoarthritis (OA). Therefore, it is essential to analyze the economic impact of this treatment option.
Purpose:
To investigate the cost-effectiveness of hip arthroscopic surgery versus structured rehabilitation alone for acetabular labral tears, to examine the effects of age on cost-effectiveness, and to estimate the rate of symptomatic OA and total hip arthroplasty (THA) in both treatment arms over a lifetime horizon.
Study Design:
Economic and decision analysis; Level of evidence, 2.
Methods:
A cost-effectiveness analysis of hip arthroscopic surgery compared with structured rehabilitation for symptomatic labral tears was performed using a Markov decision model constructed over a lifetime horizon. It was assumed that patients did not have OA. Direct costs (in 2014 United States dollars), utilities of health states (in quality-adjusted life years [QALYs] gained), and probabilities of transitioning between health states were estimated from a comprehensive literature review. Costs were estimated using national averages of Medicare reimbursements, adjusted for all payers in the United States from a societal perspective. Utilities were estimated from the Harris Hip Score. Cost-effectiveness was assessed using the incremental cost-effectiveness ratio (ICER). One-way and probabilistic sensitivity analyses were performed to determine the effect of uncertainty on the model outcomes.
Results:
For a cohort representative of patients undergoing hip arthroscopic surgery at our facility, arthroscopic surgery was more costly (additional $2653) but generated more utility (additional 3.94 QALYs) compared with rehabilitation over a lifetime. The mean ICER was $754/QALY, well below the conventional willingness to pay of $50,000/QALY. Arthroscopic surgery was cost-effective for 94.5% of patients. Although arthroscopic surgery decreased in cost-effectiveness with increasing age, arthroscopic surgery remained more cost-effective than rehabilitation for patients in the second to seventh decades of life. The lifetime incidence of symptomatic hip OA was over twice as high for patients treated with rehabilitation compared with arthroscopic surgery. The preferred treatment was sensitive to the utility after successful hip arthroscopic surgery, although the utility at which arthroscopic surgery becomes less cost-effective than rehabilitation is far below our best estimate. For older patients, the lifetime cost of arthroscopic surgery was greater, while the lifetime utility of arthroscopic surgery was less, approaching that of the rehabilitation arm.
Conclusion:
Hip arthroscopic surgery is more cost-effective and results in a considerably lower incidence of symptomatic OA than structured rehabilitation alone in treating symptomatic labral tears of patients in the second to seventh decades of life without pre-existing OA.
Keywords
Hip arthroscopic surgery was first attempted in 1931 by Burman. 9 However, it was not until 1957 that Paterson 34 published the first report of acetabular labral tears while describing 2 cases of irreducible posterior hip dislocations. Suzuki et al 41 described the arthroscopic appearance of acetabular labral tears in 1986. Since then, advances in imaging and arthroscopic surgery have greatly increased the recognition of this diagnosis. The prevalence of labral tears has been estimated to be 22% to 55% in patients with hip or groin pain. 19 More importantly, the association of labral tears with pathological conditions of the hip such as femoroacetabular impingement (FAI), acetabular dysplasia, hypermobility, and trauma has increased focus on its optimal management in patients presenting with these conditions.19,23,35,44 Furthermore, through arthroscopic and anatomic observations, McCarthy et al 28 suggested a contribution to early degenerative hip disease.
Hip osteoarthritis (OA) profoundly affects quality of life in the United States (US), with estimated costs as high as $42.3 billion from 904,900 hip and knee replacements in 2009. 29 With the lifetime risk of symptomatic hip OA estimated at 25.3%, 30 it is paramount to address conditions that can precipitate this state to reduce the quality of life lost, caused by disability and functional limitations, and their corresponding economic impact. Hip arthroscopic surgery has emerged as an efficacious tool to address labral tears and FAI, both of which are intricately involved in the potential origin of OA.17,23,28 Despite this, few studies have examined the economic impact of hip arthroscopic surgery in treating labral tears. 37 If hip arthroscopic surgery presents an opportunity for a surgeon to curtail OA in patients with symptomatic labral tears, the societal impact (both financial and health related) of this practice needs to be vigorously evaluated to minimize opportunity costs of not offering this treatment and continuing with nonsurgical care.
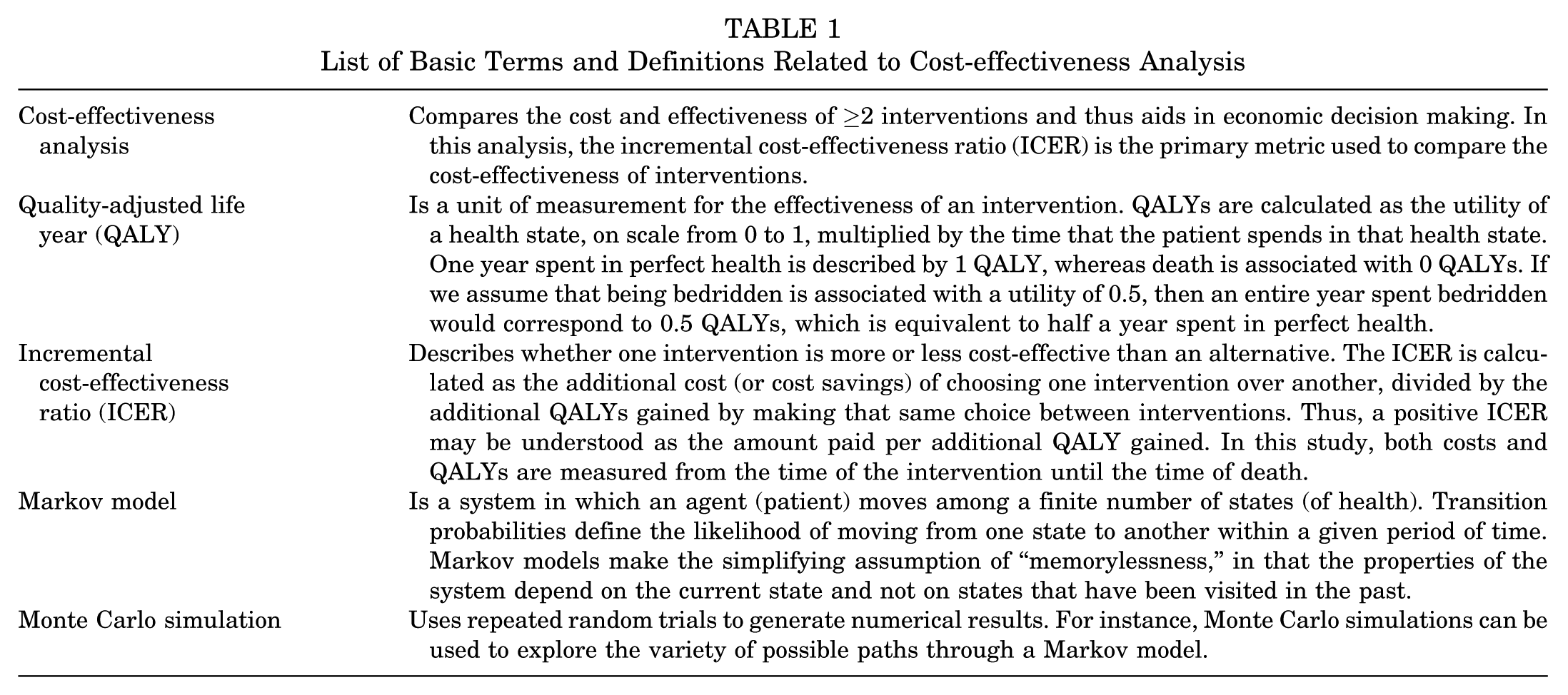
A cost-effectiveness analysis (CEA) compares the health outcomes and costs of different interventions. 36 We used this method to compare the societal economic impact of the operative and nonoperative management of labral tears. There were 3 purposes of this study: (1) to investigate the cost-effectiveness of hip arthroscopic surgery versus structured rehabilitation alone for acetabular labral tears in patients without OA, (2) to examine the effects of age on cost-effectiveness, and (3) to estimate the rate of symptomatic OA and total hip arthroplasty (THA) in both treatment arms over a lifetime horizon. Table 1 provides the definition of basic terms used in a CEA.
List of Basic Terms and Definitions Related to Cost-effectiveness Analysis
Methods
We investigated the cost-effectiveness of hip arthroscopic surgery versus structured rehabilitation for acetabular labral tears using recommendations by the Panel on Cost-Effectiveness in Health and Medicine.36,38,43 Using TreeAge Pro 2014 (TreeAge Software), we constructed a Markov decision model with a cycle length of 1 year and a lifetime horizon to simulate health trajectories from the initial treatment to death. Cumulative costs and quality of life over potential health trajectories were assessed for a representative patient cohort and analyzed to determine the relative cost-effectiveness of the 2 strategies. Model parameters were obtained from a comprehensive literature review (Table 2). Cost-effectiveness was estimated from the societal perspective.
List of Model Parameters, With Base Values, Ranges for 1-way Sensitivity Analysis, and Literature Sources a
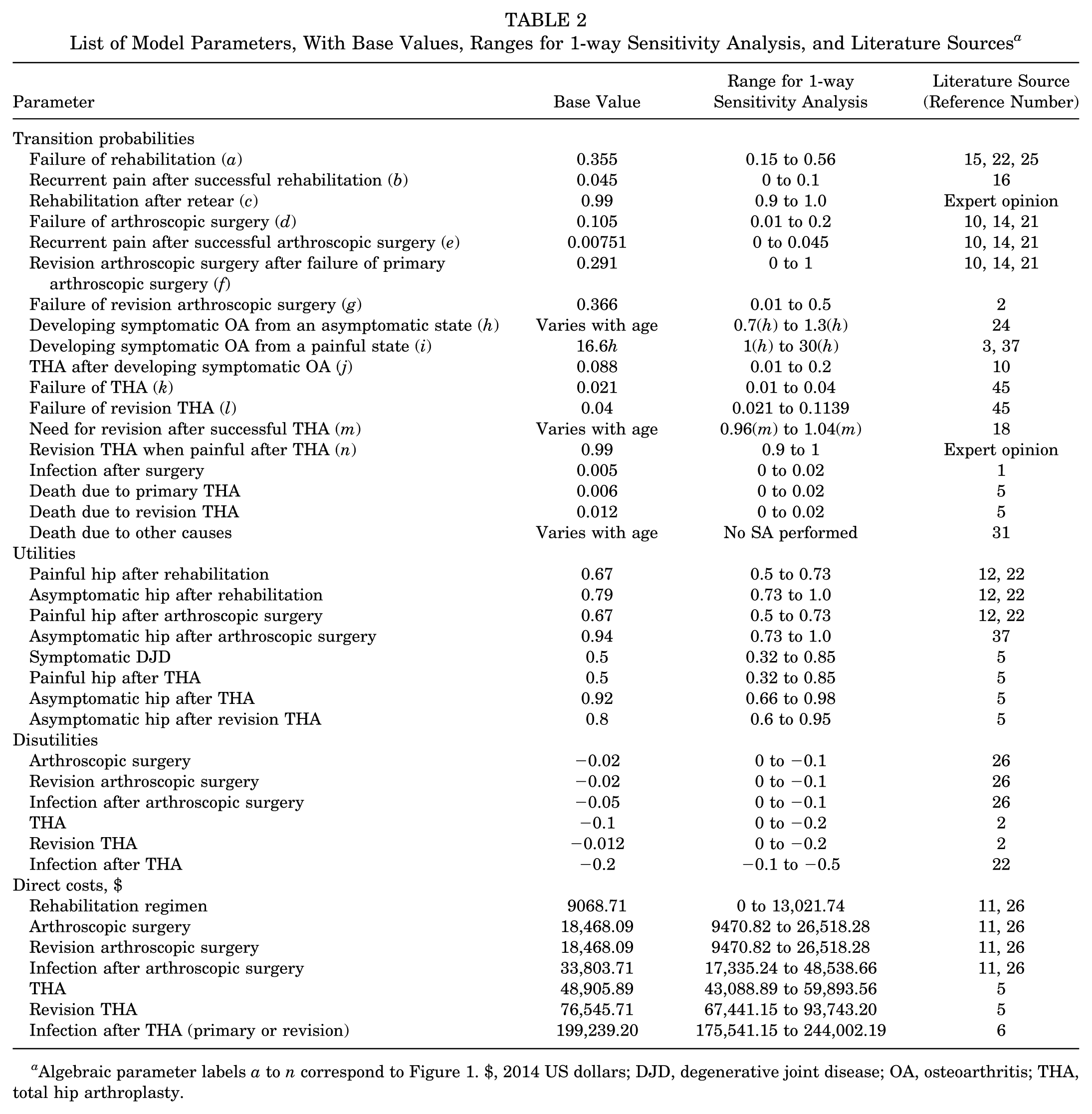
Algebraic parameter labels a to n correspond to Figure 1. $, 2014 US dollars; DJD, degenerative joint disease; OA, osteoarthritis; THA, total hip arthroplasty.
Markov Model Structure
In a decision analysis, a Markov model combines multiple sources of evidence to simulate the recursive and chronic progression of a condition over a defined time interval (or horizon). 40 Our model consisted of a decision tree with 2 main treatment arms: hip arthroscopic surgery and structured rehabilitation (Figure 1). Patients entered both treatment arms after the diagnosis of an acetabular labral tear. Costs, recovery, and complications of treatment were simulated in the year after the treatment. After the initial treatment, all patients entered 1 of 4 health states: asymptomatic, painful hip, symptomatic OA, and death. Patients in the hip arthroscopic surgery arm could undergo revision hip arthroscopic surgery; however, patients in the rehabilitation arm were not allowed to cross over to the operative arm. Patients with symptomatic OA could undergo THA and subsequently transition to 1 of 3 states: asymptomatic, painful hip, and death. Patients with a painful hip after primary THA could undergo revision THA, unless it was contraindicated (estimated rate of 1% based on expert opinion). After revision THA, the patient transitioned to 1 of the 3 health states available after primary THA.
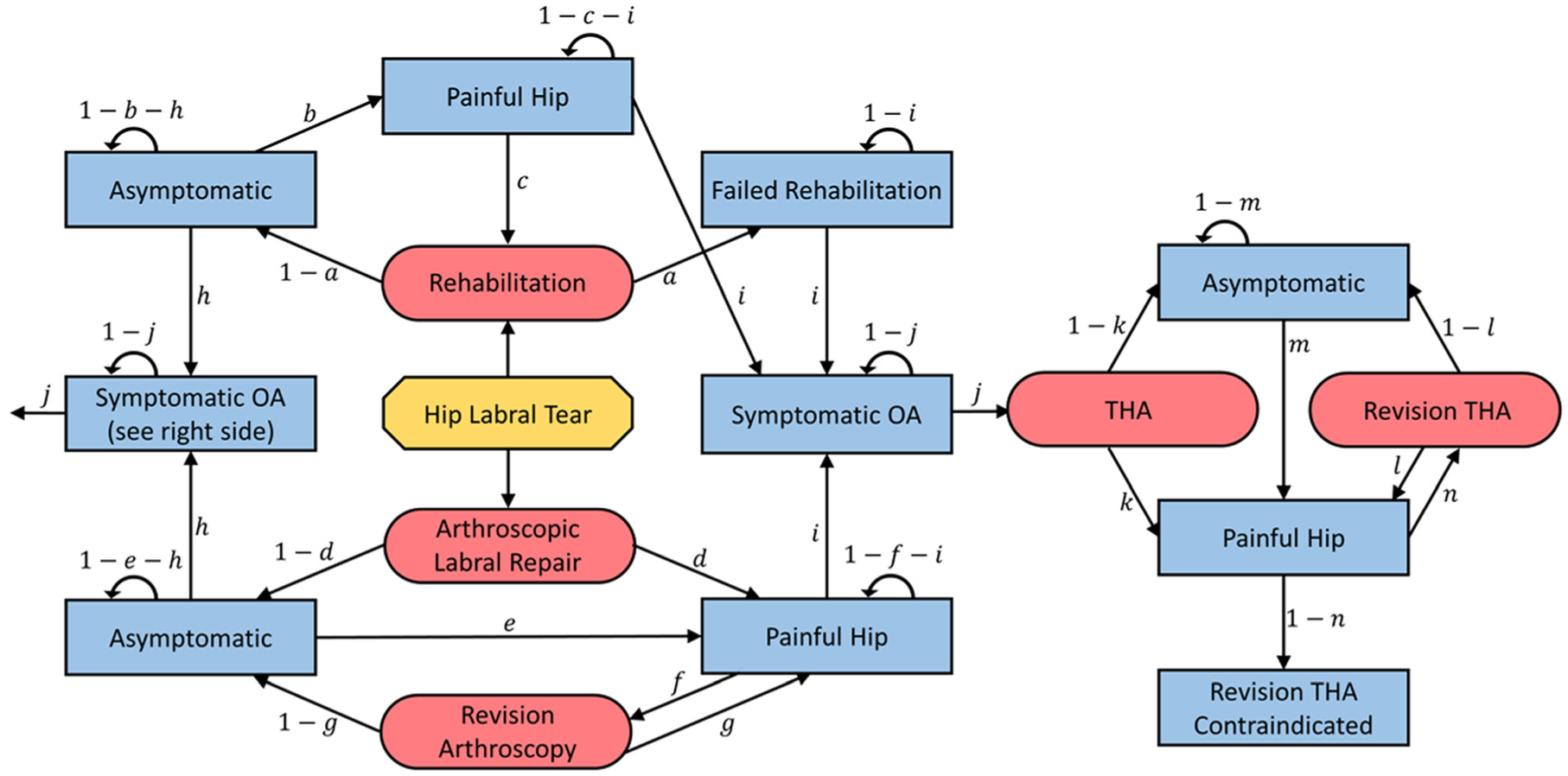
Markov model. The octagon represents the starting state, the rectangles represent health states, and the rounded rectangles represent procedures. Transition probabilities a to n are listed in Table 2 and online Appendix Table A1. Transitions to death and complications of surgery are not shown in this illustration but are fully incorporated into the model. OA, osteoarthritis; THA, total hip arthroplasty.
Transition Probabilities
Success or failure rates of treatments and rates of revision hip arthroscopic surgery were derived from the literature.2,10,14,15,21,22,25 Weighted averages based on patient populations were used when multiple studies provided relevant values. Patients who experienced success after arthroscopic surgery or rehabilitation (and entered the “asymptomatic” state) developed symptomatic OA at rates consistent with the general population. 24 Patients who experienced failure after arthroscopic surgery or rehabilitation (and entered the “painful hip” state) developed symptomatic OA at higher rates, estimated from a study by Bardakos and Villar 3 based on 2 assumptions: (1) patients with labral tears and patients with FAI have similar rates of developing symptomatic OA, and (2) patients who have failed the treatment of labral tears or FAI have similar rates of developing symptomatic OA as patients with the same pathological condition left untreated. Probabilities of developing hip pain after primary or revision THA were calculated using the Swedish Hip Arthroplasty Register. 18
Population and Mortality Rates
In this model, individual patients had different ages at the time of initial treatment. For the base case, the ages of the 2039 patients who underwent hip arthroscopic surgery for labral tears at our institution between February 2008 and June 2014 (mean [±SD] age, 36.7 ± 13.9 years) were compiled and used to generate a probability distribution from which the ages of patients in our model cohort were obtained. Institutional review board approval was obtained before the use of these data. We also considered additional model cohorts in which the patients’ ages were representative of the general US population and in which patients’ ages were selected from uniform distributions representing each decade of life from the second to seventh decades (with age uniformly distributed in each decade). Simulated patients did not have OA at the time of initial treatment. All-cause mortality was derived from the US Centers for Disease Control and Prevention life tables. 31 Mortality rates after primary and revision THA were 0.6% and 1.2%, respectively. 5
Utilities and Costs
Utilities, expressed in quality-adjusted life years (QALYs), are measures of health-related quality of life on a scale from 0 (death) to 1 (perfect health). 7 Previous CEAs used patient-reported outcome (PRO) scores to derive a preference-based measure of health.8,12,42 Chang et al 12 described a relationship between the Harris Hip Score (HHS) and utility. Shearer et al 37 used this relationship, with linear interpolation, to estimate the utilities of health states after hip arthroscopic surgery from previously published PRO scores. We employed this method to estimate the utilities of the painful and asymptomatic states after rehabilitation using the HHS reported by Hunt et al. 22 All health states relating to symptomatic OA and THA were assigned utilities published by Bozic et al. 5
Total societal costs of hip arthroscopic surgery and rehabilitation were based on national average Medicare reimbursements in 2014 US dollars. We used previously described adjustments to reflect all payer reimbursements (including private insurance, self-pay, and Medicaid).26,27 Costs of primary THA and revision THA were obtained from the literature.4,5 A discount rate (used to weigh future gains and losses less heavily than those in the present) of 3% was applied to reflect the present value of utilities and costs. 39
Cost-effectiveness Analysis
The primary outcome for determining the preferred treatment strategy was the incremental cost-effectiveness ratio (ICER), defined as the difference in costs of the 2 treatment strategies divided by their difference in utilities. 37 Willingness to pay (WTP) is a threshold ICER, defined such that ICERs less than the WTP indicate that arthroscopic surgery is cost-effective while the ICER greater than the WTP indicates that rehabilitation is cost-effective. We selected a WTP of $50,000/QALY. 20 Neumann et al 32 have suggested higher WTP values ranging from $100,000/QALY to $150,000/QALY. However, we chose the value of $50,000/QALY to provide a more conservative assessment of the cost-effectiveness of arthroscopic surgery versus rehabilitation.
We performed 1-way sensitivity analyses on all model parameters to determine their effect on cost, utility, and ICER. The model was assessed as each parameter was individually varied within a reasonable range around its base value. These ranges were based on the literature or the authors’ expert opinion when literature values were unavailable (Table 2; see the Appendix, available online at http://ajsm.sagepub.com/supplemental). A parameter was considered sensitive if variations within its specified range resulted in a change in the preferred treatment strategy. A parameter was considered robust if a change in the preferred treatment was not detected. We performed a probabilistic sensitivity analysis (PSA) to evaluate the model’s outcomes when multiple parameters were drawn from probability distributions and thereby allowed to vary from their base values. We selected a variable for inclusion in the PSA if it was sensitive in terms of cost, utility, or cost-effectiveness or if the 1-way sensitivity analysis showed variations in the ICER exceeding $2000/QALY.
Results
Over an average patient’s lifetime, choosing arthroscopic surgery over structured rehabilitation alone for the treatment of a labral tear generated $2653 in additional costs but provided 3.94 QALYs in additional utility. The mean ICER was $754/QALY, well below the WTP of $50,000/QALY. Although the ICER increased with age, confirming that arthroscopic surgery provides less utility per cost for older patients, the ICER remained less than the WTP, indicating that arthroscopic surgery was preferred over rehabilitation for all age groups assessed. Arthroscopic surgery was more costly but provided greater utility than rehabilitation for all age groups (Table 3).
Results of Base Case for Representative Cohorts and Patients in the Second to Seventh Decades of Life a
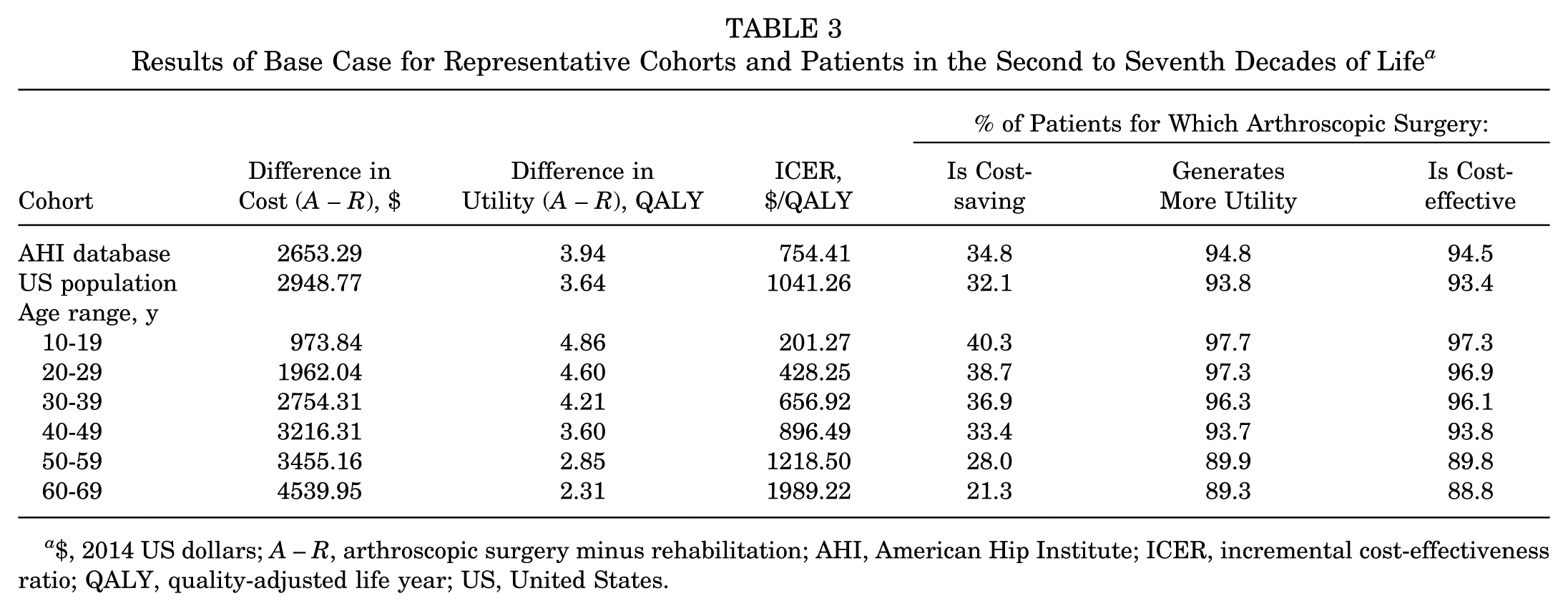
$, 2014 US dollars; A – R, arthroscopic surgery minus rehabilitation; AHI, American Hip Institute; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life year; US, United States.
Probabilistic Sensitivity Analysis
The mean lifetime costs of hip arthroscopic surgery and rehabilitation were $26,070 ± $7983 and $23,529 ± $5222, respectively, while the median costs were $24,676 and $23,068, respectively. The mean utilities for arthroscopic surgery and rehabilitation were 21.78 ± 4.81 and 17.74 ± 3.16 QALYs, respectively, while the median utilities were 22.35 and 18.10 QALYs, respectively. Compared with rehabilitation, arthroscopic surgery provided cost savings in 40.3% of the cohort and greater utility in 92.1% of the cohort. On the basis of the ICER, 94.8% of the cohort demonstrated a preference for arthroscopic surgery (Table 4).
Results of Probabilistic Sensitivity Analysis With 1 Million Trials a
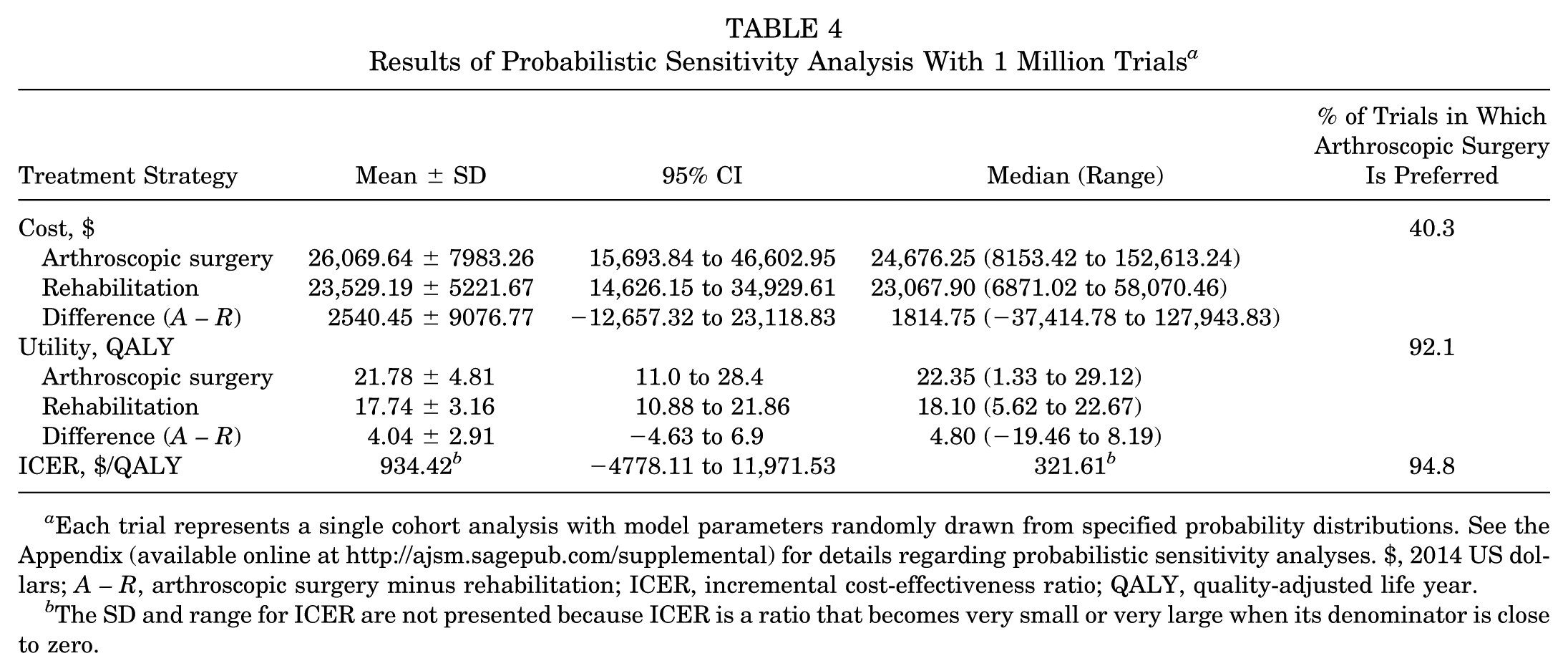
Each trial represents a single cohort analysis with model parameters randomly drawn from specified probability distributions. See the Appendix (available online at http://ajsm.sagepub.com/supplemental) for details regarding probabilistic sensitivity analyses. $, 2014 US dollars; A – R, arthroscopic surgery minus rehabilitation; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life year.
The SD and range for ICER are not presented because ICER is a ratio that becomes very small or very large when its denominator is close to zero.
Microsimulations for Assessment of Patient Variability
Microsimulations were performed to assess the variability in treatments and outcomes among individual patients within a cohort. Base values of parameters were used, excluding the initial age of the patient, which was drawn from a distribution representative of patients who underwent hip arthroscopic surgery at our institution (as previously described). Overall, arthroscopic surgery was cost-effective for 94.5% of patients (Figure 2). The percentage of patients for which arthroscopic surgery was cost-effective decreased with age, from 97% in patients between 10 and 29 years old to 89% in patients ≥60 years old (Table 3).
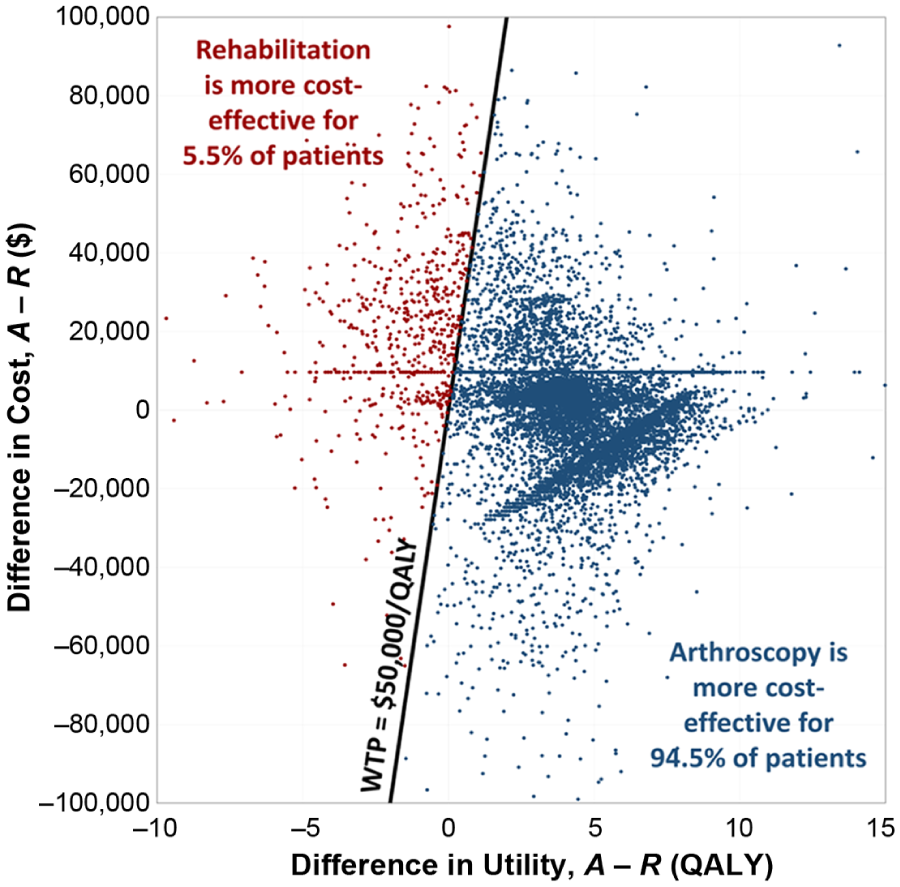
Distribution of microsimulations showing individual patient variability in outcomes of hip arthroscopic surgery and rehabilitation in a cohort representative of patients undergoing hip arthroscopic surgery at our institution. Base values of model parameters are used. $, 2014 US dollars; A – R, arthroscopic surgery minus rehabilitation; QALY, quality-adjusted life year; WTP, willingness to pay.
The lifetime prevalence of symptomatic OA and subsequent THA in patients undergoing arthroscopic surgery (28.5% and 18.7%, respectively) was less than half that of patients undergoing rehabilitation (62.0% and 45.9%, respectively) (Table 5). Primary THA alone accounted for additional costs of $3893, on average, per patient in the rehabilitation arm.
Results of 1-way Sensitivity Analyses a
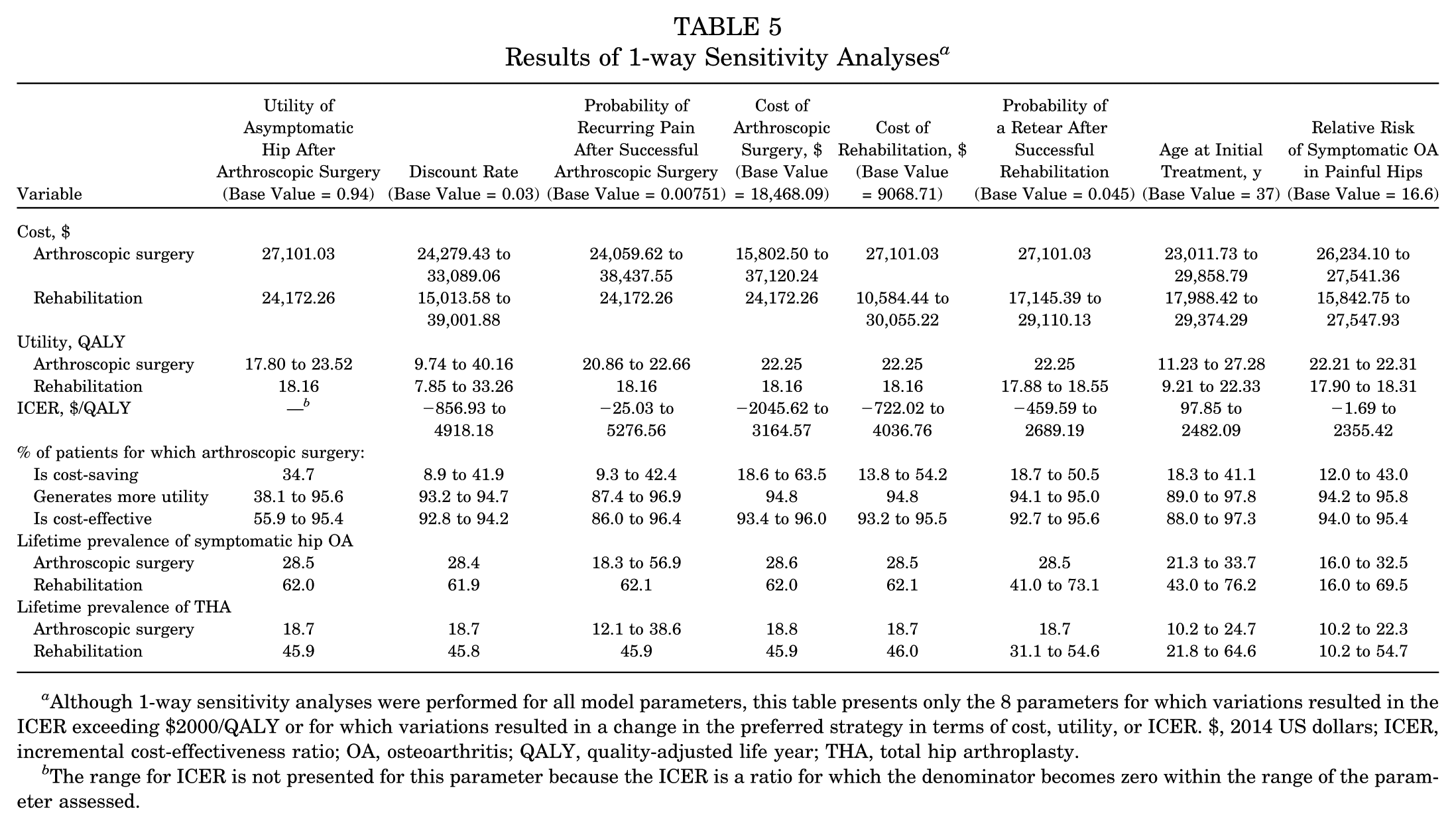
Although 1-way sensitivity analyses were performed for all model parameters, this table presents only the 8 parameters for which variations resulted in the ICER exceeding $2000/QALY or for which variations resulted in a change in the preferred strategy in terms of cost, utility, or ICER. $, 2014 US dollars; ICER, incremental cost-effectiveness ratio; OA, osteoarthritis; QALY, quality-adjusted life year; THA, total hip arthroplasty.
The range for ICER is not presented for this parameter because the ICER is a ratio for which the denominator becomes zero within the range of the parameter assessed.
1-way Sensitivity Analysis
Model parameters were individually varied within clinically sensible ranges based on the literature or on the authors’ expert opinion if the literature was inadequate. We report the effect of varying model parameters on cost, utility, ICER, and lifetime prevalence of symptomatic OA and THA (Figure 3 and Table 5). Furthermore, we report threshold values of model parameters at which the preferred treatment strategy, in terms of cost, utility, or ICER, changes from the base case (Table 6).
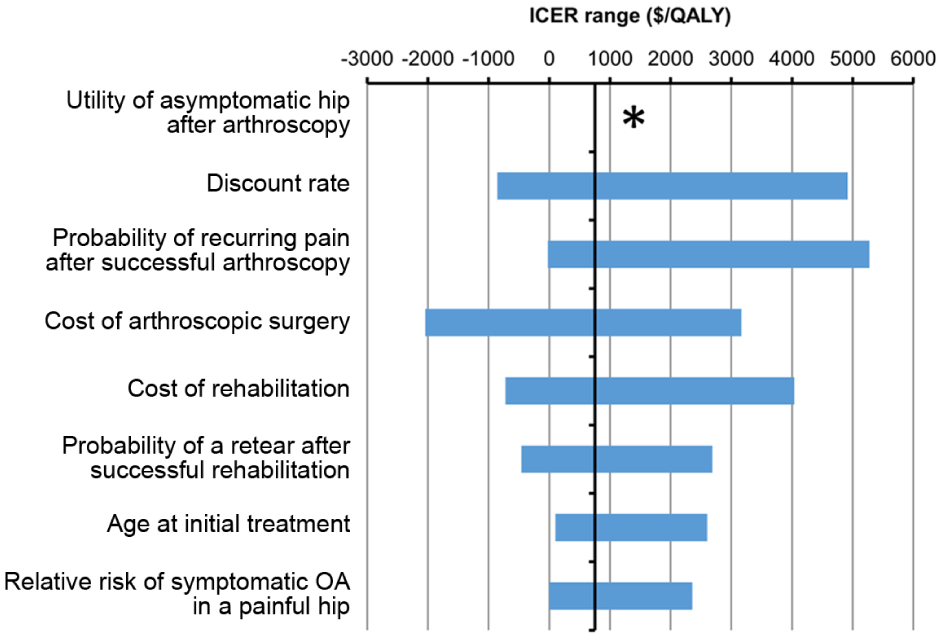
Tornado diagram showing incremental cost-effectiveness ratio (ICER) ranges resulting from 1-way sensitivity analyses in which individual model parameters are varied within reasonable ranges. Although 1-way sensitivity analyses were performed for all model parameters, this table presents only the 8 parameters for which variations resulted in the ICER exceeding $2000 per quality-adjusted life year (QALY) or for which variations resulted in a change in the preferred strategy in terms of cost, utility, or ICER (Table 6). The center line represents the base-case ICER of $754/QALY. *The ICER range is not presented for this parameter because the ICER is a ratio for which the denominator becomes zero within the range of the parameter assessed. $, 2014 US dollars; OA, osteoarthritis.
Results of Threshold Analyses a
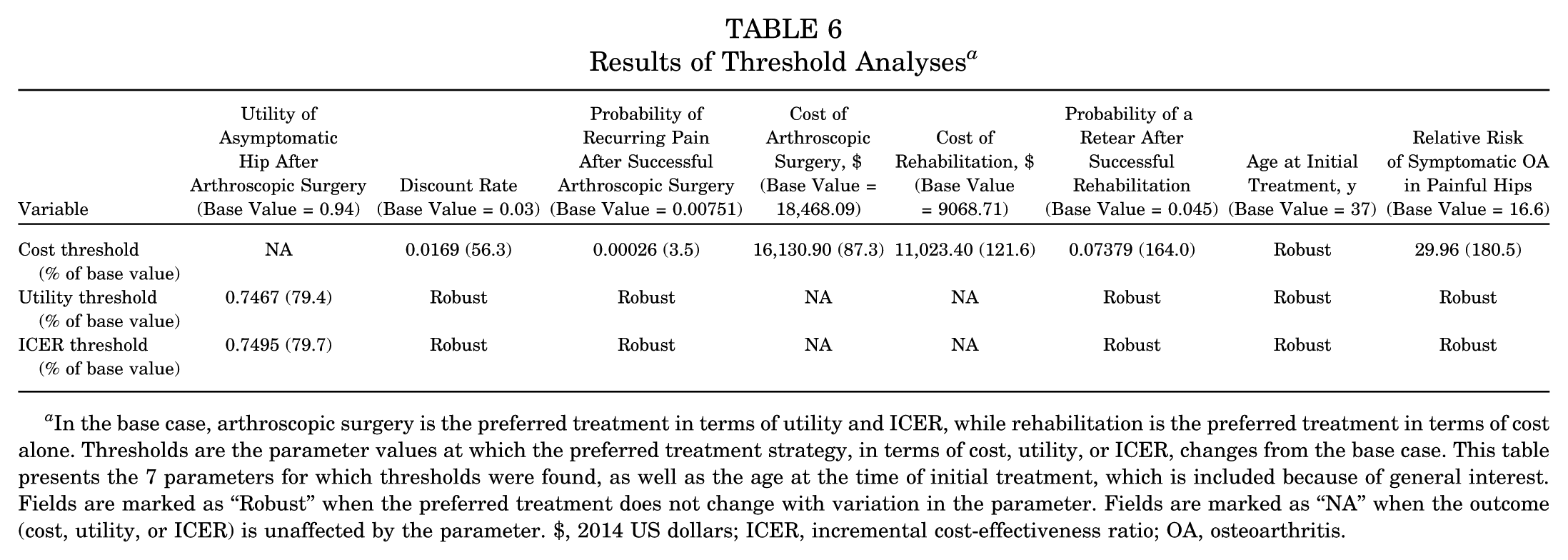
In the base case, arthroscopic surgery is the preferred treatment in terms of utility and ICER, while rehabilitation is the preferred treatment in terms of cost alone. Thresholds are the parameter values at which the preferred treatment strategy, in terms of cost, utility, or ICER, changes from the base case. This table presents the 7 parameters for which thresholds were found, as well as the age at the time of initial treatment, which is included because of general interest. Fields are marked as “Robust” when the preferred treatment does not change with variation in the parameter. Fields are marked as “NA” when the outcome (cost, utility, or ICER) is unaffected by the parameter. $, 2014 US dollars; ICER, incremental cost-effectiveness ratio; OA, osteoarthritis.
The preferred treatment in terms of the ICER (arthroscopic surgery in the base case) was sensitive only to a single parameter: the utility of an asymptomatic hip after arthroscopic surgery. The mean ICER indicated that rehabilitation was more cost-effective than arthroscopic surgery when the utility of an asymptomatic patient after arthroscopic surgery was less than 0.75 (Table 6). Arthroscopic surgery was more cost-effective than rehabilitation in 59% of patients in this limiting case.
Interestingly, arthroscopic surgery remained the preferred treatment in terms of the ICER, even when the probability of failing rehabilitation and/or the utility of an asymptomatic hip after rehabilitation were varied within substantial exploratory ranges. The probability of failing rehabilitation was assessed from 0.15 to 0.56, approximately 40% to 160% of the base value of 0.355.15,22,25 The utility of an asymptomatic hip after rehabilitation was assessed from 0.73 to 1.0, approximately 0.92% to 127% of the base value of 0.79.12,22 For detailed discussions of parameter values and ranges for sensitivity analyses, see Appendix Tables A1 to A4 (available online).
The preferred treatment based on cost alone (rehabilitation in the base case) was sensitive to 6 parameters (Table 6). Sensitivity analyses identified threshold values for these parameters, beyond which arthroscopic surgery was cost-saving compared with rehabilitation. Therefore, there are reasonable sets of parameter values for which arthroscopic surgery costs less and provides more utility than rehabilitation (termed “dominant”). For instance, hip arthroscopic surgery was dominant over rehabilitation when the cost of arthroscopic surgery was less than 87.3% of the base value or when the cost of a rehabilitation regimen was greater than 121.6% of the base value (Table 6).
Although the preferred treatment in terms of either cost-effectiveness or cost alone was not sensitive to the patient’s initial age, varying the initial age from 10 to 69 years resulted in a considerable ICER of $2384/QALY (Table 5 and Figure 4). For older patients, the lifetime cost of arthroscopic surgery was greater, while the lifetime utility of arthroscopic surgery was less, approaching that of the rehabilitation arm (Figure 4).
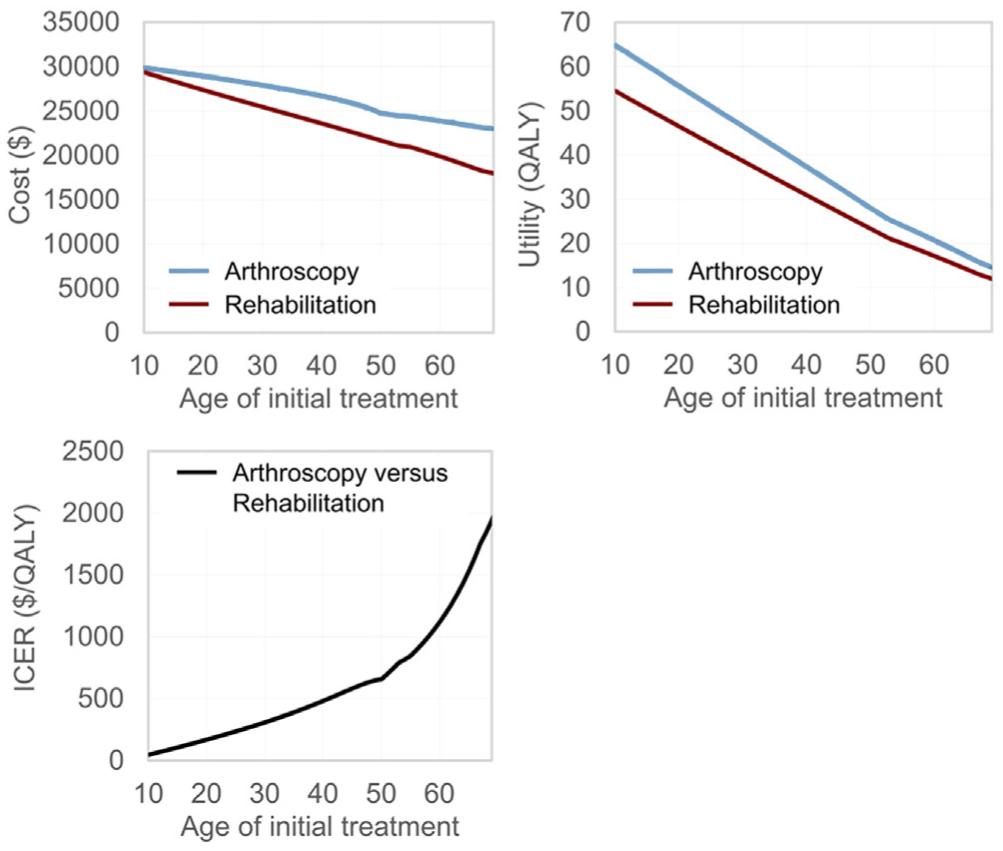
Results of 1-way sensitivity analysis for the patient’s age at the time of initial treatment. As the initial age increases, the lifetime cost of arthroscopic surgery increases, while the utility of arthroscopic surgery approaches that of rehabilitation. The increase in the incremental cost-effectiveness ratio (ICER) with age is the combined result of these changes. QALY, quality-adjusted life year.
Discussion
The current model estimated that the treatment of a labral tear via arthroscopic surgery costs $2653 more and generates 3.94 QALYs more than rehabilitation over an average patient’s lifetime. The mean trade-off (ICER) was $754/QALY, far below the conventional WTP of $50,000/QALY. This indicates that arthroscopic surgery is considerably more cost-effective than rehabilitation, on average. Within a typical cohort, arthroscopic surgery was more cost-effective than rehabilitation for 94.5% of patients. Arthroscopic surgery decreased in cost-effectiveness with age but remained more cost-effective than rehabilitation for patients from the second to seventh decades of life. Patients treated with arthroscopic surgery were less than twice as likely to develop symptomatic OA and require THA compared with patients treated with rehabilitation. This was because of the lower success rate of rehabilitation and the higher likelihood of developing symptomatic OA in a patient with a painful hip.
Sensitivity analyses are necessary for understanding the conditions in which one treatment is preferred over another. The cost-effectiveness of arthroscopic surgery compared with rehabilitation was sensitive to only 1 parameter: the patient’s utility after successful hip arthroscopic surgery. If this utility were lower than 0.75, then rehabilitation would be more cost-effective than arthroscopic surgery, on average. We note that arthroscopic surgery remained cost-effective for 59% of patients even in this limiting case. For comparison, our best estimate for the utility after successful hip arthroscopic surgery was 0.94, based on an earlier CEA by Shearer et al 37 that evaluated several studies reporting the mean HHS or modified HHS after hip arthroscopic surgery. Of the studies evaluated, the lowest mean score was 81, which corresponds to a utility of 0.82 (based on the relationship between the HHS and utility established by Chang et al 12 ). However, if a value of 0.82 were assigned to this parameter (or an even lower value of 0.79, equal to the utility after successful rehabilitation), arthroscopic surgery would remain more cost-effective than rehabilitation. Therefore, arthroscopic surgery is expected to be more cost-effective than rehabilitation, on average, unless the current literature drastically overestimates the outcomes of hip arthroscopic surgery.
Nwachukwu et al 33 recently performed a systematic review of CEAs in sports medicine, demonstrating their paucity in the literature. Among the few studies identified was an analysis of hip arthroscopic surgery by Shearer et al. 37 The authors compared hip arthroscopic surgery to observation over a lifetime horizon in a 36-year-old patient population with FAI, assuming that arthroscopic surgery provided symptomatic relief for 3 years and that hip arthroscopic surgery did not otherwise affect the rate of OA progression. Using a Markov model that accounted for OA and subsequent THA, they estimated ICERs of $21,700/QALY and $79,500/QALY for patients without and with preoperative OA, respectively. Using a threshold of $50,000/QALY, the authors concluded that hip arthroscopic surgery for FAI might be cost-effective in the absence of preoperative OA. In contrast, our study compared hip arthroscopic surgery to structured rehabilitation in labral tears in the absence of OA without limiting the duration of the asymptomatic state and accounting for different rates of progression to symptomatic OA for patients with asymptomatic and painful hips. Our analysis yielded an ICER of $754/QALY, suggesting that hip arthroscopic surgery provides much greater cost-effectiveness over a patient’s lifetime compared with structured rehabilitation alone.
There are multiple limitations to consider. First, because there are disproportionately fewer articles in the literature reporting on the nonoperative treatment of labral tears, the estimated success rate after rehabilitation may be inaccurate. However, a sensitivity analysis of this parameter did not change the preferred strategy. Second, patients in the rehabilitation arm were not allowed to undergo hip arthroscopic surgery. This restriction was necessary to compare surgical candidates with and without access to operative management. In reality, patients certainly have the liberty to opt out of rehabilitation alone and pursue operative management along with rehabilitation. This can potentially change their health state. This model would not be applicable to those patients as the frequency of changing management either as a choice of the patient or by recommendation of the health care provider is not known and cannot be speculated. Furthermore, the effect of arthroscopic surgery could vary depending on when a patient would change treatment arms and his/her health state at that particular time. Third, there is insufficient literature on the extent of symptomatic relief after hip arthroscopic surgery, with most studies reporting outcomes after 2 years. While the extrapolation of these results over a lifetime adds uncertainty to our model, sensitivity analyses did not alter our treatment strategy. Fourth, this study examined direct costs only. Dall et al 13 have underscored the societal implications of indirect costs such as employment, income, missed work, and disability payments. These estimates, while generalizable for musculoskeletal disorders, are unavailable in the literature. An association between labral tears and functional limitation is needed to infer indirect costs.
This study reports the outcomes of a rigorous CEA on the treatment of labral tears. By allowing different rates of progression to symptomatic OA in asymptomatic patients and those with painful hips, and by accounting for the potential need for revision THA, we created a sophisticated model that simulated the societal impact of disease progression after a labral tear. Because hip arthroscopic surgery is cost-effective compared with rehabilitation alone, it has an important role in improving quality of life in patients failing nonoperative management. Further studies should focus on identifying the patient population that most benefits from the operative treatment of labral tears.
Conclusion
We estimate that hip arthroscopic surgery is more cost-effective than rehabilitation alone in the treatment of symptomatic labral tears for the majority of patients without OA in the second to seventh decades of life, although arthroscopic surgery decreases in cost-effectiveness with age. The lifetime risk of developing hip OA and undergoing THA is less than half in patients treated with arthroscopic surgery compared with rehabilitation alone. Considering these findings, patients with symptomatic labral tears who have failed nonoperative management and who do not have evidence of OA may be offered hip arthroscopic surgery as a viable treatment option.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G.D. reports personal fees and other from Arthrex Inc, personal fees and other from MAKO Surgical Corp, other from Breg, other from ATI, personal fees and other from Pacira, personal fees from Stryker, personal fees from Orthomerica, personal fees from DJO Global, and personal fees from Amplitude, outside the submitted work. B.G.D. is also a board member of the American Hip Institute, which funds research and is the institute where this study was performed.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.