
Abstract
Background:
Low-intensity pulsed ultrasound stimulation (LIPUS) has been proven to be a beneficial biophysical therapy for tendon-bone (T-B) healing. However, the optimal time to initiate LIPUS treatment has not been determined yet. LIPUS initiated at different stages of the inflammatory phase may profoundly affect T-B healing.
Purpose:
An established rabbit model was used to preliminarily investigate the effect of LIPUS initiation timing on T-B healing.
Study Design:
Controlled laboratory study.
Methods:
A total of 112 mature rabbits that underwent partial patellectomy were randomly assigned to 4 groups: daily mock sonication (control group) and daily ultrasonication started immediately postoperatively (immediate group), on postoperative day 7 (7-day delayed group), or on postoperative day 14 (14-day delayed group). Peripheral leukocyte counts at the inflammatory phase were used to assess postoperative inflammation. The rabbits were sacrificed at 8 or 16 weeks postoperatively for microarchitectural, histological, and mechanical evaluations of the patella–patellar tendon (PPT) junction.
Results:
The biomechanical properties of the PPT junction were significantly improved in the LIPUS-treated groups. Significantly higher ultimate strength and stiffness were seen in the 7-day delayed group compared with the other groups at 8 weeks postoperatively (P < .05 for all). Newly formed bone expansion from the remaining patella in the ultrasonic treatment groups was significantly increased and remodeled compared with the control group. Micro–computed tomography analysis showed that the 7-day delayed group had significantly more bone volume and bone mineral content at the interface as compared with the other groups at 8 weeks postoperatively (P < .05 for all). Histologically, the ultrasonic treatment groups exhibited a significantly better PPT junction, as shown by more formation and remodeling of the fibrocartilage layer and newly formed bone. Additionally, peripheral leukocyte counts displayed a significant increase from postoperative day 1 to day 3 in the immediate group as compared with the other groups. Furthermore, postoperative hydrarthrosis was more likely in the immediate group.
Conclusion:
LIPUS started at postoperative day 7 had a more prominent effect on T-B healing compared with the other treatment regimens in this study.
Clinical Relevance:
The findings of the study may help optimize the initiation timing of LIPUS for T-B healing.
Keywords
A tendon integrates with bone through an ordered transitional interface, which is composed of a complex mixture of hard, bony, and soft connective tissues.2,3,11 This multitissue interface, known as the bone-tendon junction (BTJ), is morphologically categorized into 4 distinct yet continuous tissue zones: tendon, uncalcified fibrocartilage, calcified fibrocartilage, and bone.3,14,20,46 This highly specialized and organized interface is beneficial for mediating the load transfer and minimizing concentrated stress between the tendon and bone.4,14,23 Unfortunately, the BTJ is easily injured in sports activities involving jumping, cutting, and pivoting, while its healing is a slow process.9,29,31,41,46 The reason for its complicated healing is not only because tendon-bone (T-B) healing takes place between soft tendinous tissue and hard bony tissue but also more importantly because the junctional fibrocartilage layer is regenerated slowly and incompletely at the healing interface.17,31 Thus, how to functionally and biologically restore BTJ injuries has become an important research question in sports medicine.
Generally, T-B healing is characterized by a series of sequential phases, including inflammation, renewal, and remodeling.15,20,44,47 These healing phases mainly involve inflammation, angiogenesis, chondrogenesis, and osteogenesis at the healing interface.2,18,23,48 The initial inflammatory phase plays a critical role in T-B healing, which initiates the regenerative healing process and creates an accelerating effect for the following healing process.1,24,28,45 Therefore, various types of biophysical interventions were applied in the initial inflammatory phase to augment T-B healing, such as ultrasonic therapy and magnetic therapy.11,21,46 Low-intensity pulsed ultrasound stimulation (LIPUS), an effective, noninvasive, nonoperative, inexpensive, and safe ultrasonic therapy, has been experimentally confirmed to be beneficial for T-B healing when initially applied at postoperative day 3, 7, or 14 in a rabbit model.19-21,37,47 Moreover, in vivo and in vitro studies have suggested that the effects of LIPUS on T-B healing may be attributed to its enhanced angiogenic, chondrogenic, and osteogenic activity as well as regulated inflammation on the reparative processes.20,34,37 Although the efficacy and mechanisms of LIPUS on T-B healing have been experimentally proven in several studies, the optimal treatment protocols for T-B healing, especially the timing for initiating ultrasonication, remain unclear. Because the postoperative inflammatory phase of a rabbit lasts 2 weeks,15,19,20 it is possible that the effect of LIPUS on T-B healing will vary with the initiation timing of treatment. In the current study, we picked 3 representative and practicable time points to preliminarily optimize the initiation timing of LIPUS on T-B healing.
To answer this clinical question, this study was designed to preliminarily optimize the initiation timing of LIPUS on T-B healing, with respect to the inflammatory response and micro–computed tomography (micro-CT), histomorphology, and biomechanical properties using an established rabbit model.
Methods
Animal Model and Surgery
The Animal Ethics Committee of Central South University approved the protocol of this study (Permit No. 2012-06-14). A total of 112 mature male New Zealand White rabbits (weight, 3.1 ± 0.2 kg) underwent standard partial patellectomy in the right hindlimb according to a previous protocol.15,36 Briefly, the rabbit was anesthetized with 3% sodium pentobarbital (0.8 mL/kg intravenous injection; Sigma), and then an anterolateral skin incision was longitudinally made on the right hindlimb knee. After the patella, patellar tendon, and tibial tuberosity were exposed, transverse osteotomy was performed between the proximal two-thirds and the distal one-third of the patella using a diamond wire saw (Mc01 0701; Mytec). The distal third of the patella and its fibrocartilage layer were removed, and 2 evenly spaced tunnels (0.8-mm diameter) were drilled longitudinally through the remaining patella. The remaining proximal patella and patellar tendon were tightly reattached together through the 2 predrilled tunnels with No. 3-0 nonabsorbable PDS II suture (Ethicon). The suture was tied at the superior pole of the patella, and then a figure-of-8 tension band wire was additionally applied around the superior pole of the patella to the tibial tuberosity to prevent separation of the junction reattachment before closing the surgical incision (Figure 1A). Cast immobilization with an open window for LIPUS treatment was performed at the resting position of the knee for the first 4 weeks (Figure 1B). A painkiller (tramadol; Grunenthal GmbH) was given for 3 days after surgery (1.5 mg/kg intravenous injection every 12 hours). Rabbits were allowed free cage activities after surgery.
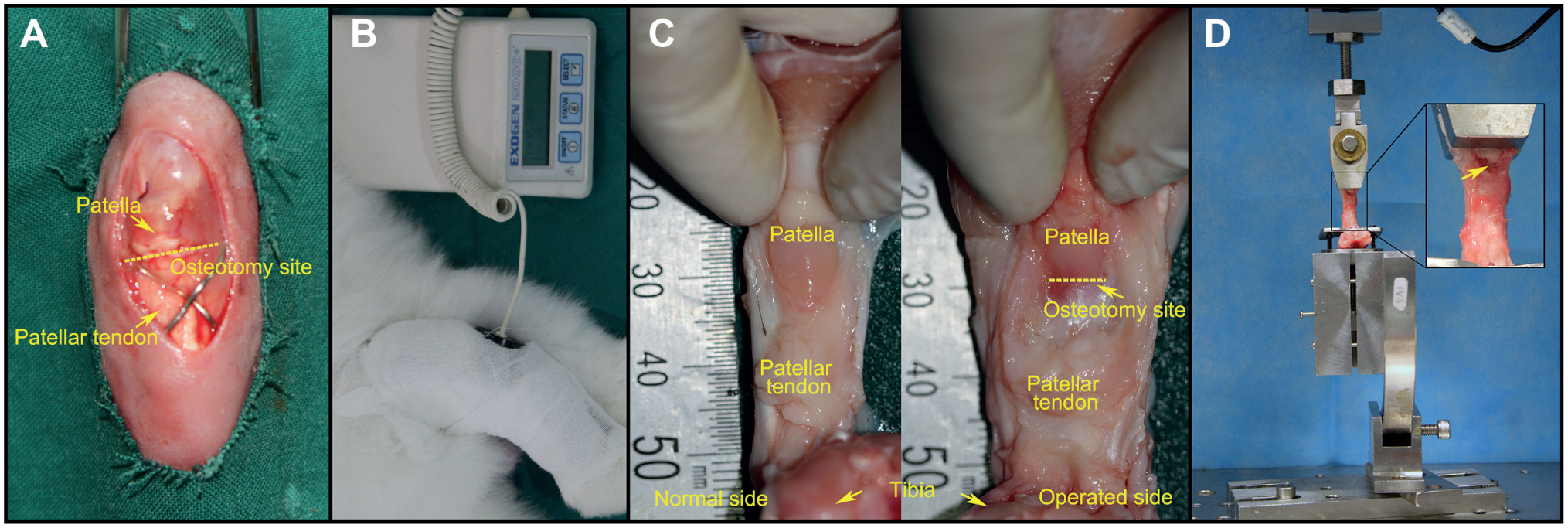
(A) The proximal patella and the residual patellar tendon after partial patellectomy. A figure-of-8 tension band wire was placed around the tibial tuberosity to the proximal pole of the patella to avoid separation of the junction reattachment. (B) A rabbit under low-intensity pulsed ultrasound stimulation (LIPUS) and placebo. The ultrasonic transducer was placed against the anterior surface of the patellar osteotomy site through an open window of the immobilization cast. (C) The quadriceps–patella–patellar tendon–tibia complex (QPPTT-C) compared between the operated side and the healthy side. (D) Mechanical testing of the QPPTT-C using a custom-made jig that includes an upper clamp and a lower clamp to fix the patella and the proximal tibia, respectively. The failure mode of the patella–patellar tendon junction in tensile testing. The yellow arrow labels the ruptured osteotomy site.
Grouping and LIPUS Treatment
After partial patellectomy, the rabbits were randomly assigned to 1 of 4 postoperative regimens: (1) daily mock sonication (control group; n = 28) or daily ultrasonication beginning (2) immediately postoperatively (immediate group; n = 28), (3) on postoperative day 7 (7-day delayed group; n = 28), or (4) on postoperative day 14 (14-day delayed group; n = 28). In the LIPUS-treated groups, 3 different initiation timings correspond to the early, middle, and late inflammatory phases, respectively. The rabbits were sacrificed at postoperative week 8 or 16 to harvest the quadriceps–patella–patellar tendon–tibia complex (QPPTT-C) (Figure 1C). Six specimens from each group at each time point were used for subsequent micro-CT and then histological evaluations, while the other 8 specimens were evaluated via biomechanical testing. The number of rabbits required for micro-CT, histological evaluations, and biomechanical testing was determined by power analysis.
After the rabbits were sedated with ketamine (0.25 mL/kg intramuscular; Alfasan International BV), ultrasound signals 20 minutes per day (operating frequency: 1.5 MHz; pulse width: 200 μs; spatial and temporal averaged incident intensity: 30.0 ± 5.0 mW/cm2) were delivered by a 2.5 cm–diameter transducer (Exogen; Smith & Nephew) and transmitted to the anterior surface of the patellar osteotomy site until the animal was sacrificed. A flowchart depicting the groups, time points for sacrifice, number of animals per group, and outcome assessments can be seen in Figure 2.
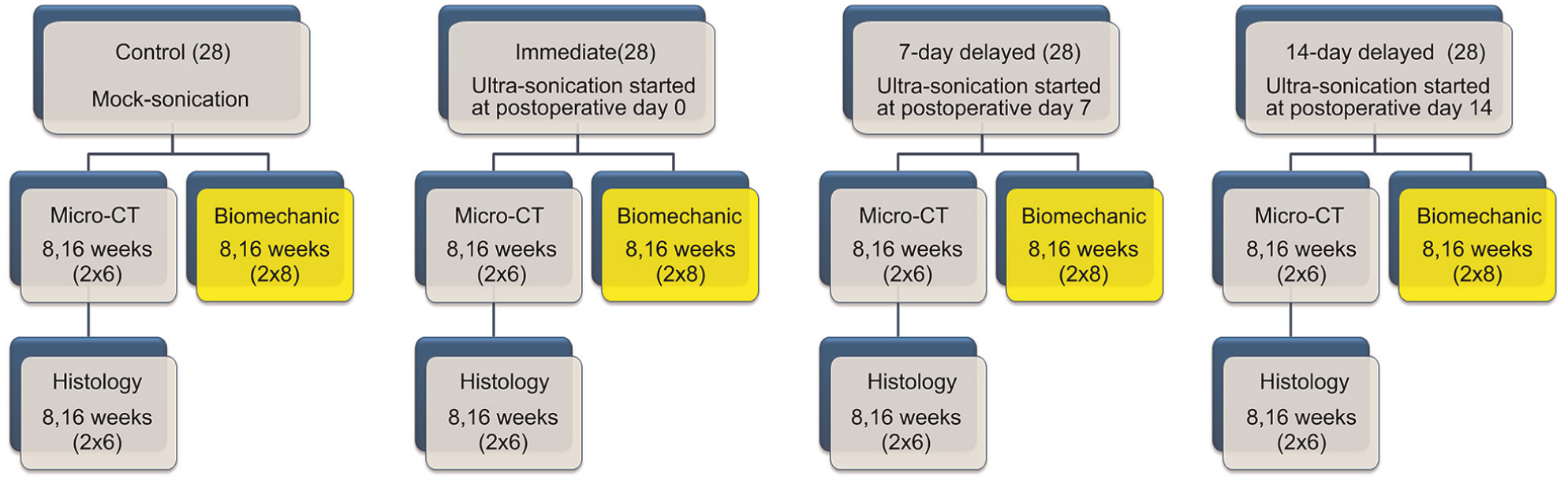
Flowchart depicting the groups, time points for sacrifice, number of animals per group, and outcome assessments.
Hematological Testing
Peripheral blood samples of every rabbit, collected from the auricular vein at postoperative day 1, 3, 5, 7, and 14, respectively, were transferred immediately to ethylenediaminetetraacetic acid (EDTA) tubes and then detected with an automatic hematology analyzer (Coulter LH 750; Beckman Coulter Inc) for leukocyte counts, which was a crucial and sensitive inflammatory indicator in the clinic. 5
Micro-CT Analysis
The microarchitecture of the newly formed bone at the patella–patellar tendon (PPT) junction was assessed by micro-CT (μCT 40; Scanco Medical). The 48 QPPTT-C specimens were carefully dissected to include only the PPT junction and attached quadriceps tendon for fixation in 4% neutral buffered formalin and then washed with 0.9% saline to remove the residual formalin. Each specimen was placed in the sample holder with their long axes in the vertical position and scanned using the conditions of 70 kV, 114 μA, and 30-μm voxel size. Scanning data of each specimen were then processed with a 3-dimensional (3D) Gaussian filter and a global threshold to extract bone from soft tissue or bone marrow for subsequent analysis. The newly formed bone at the T-B healing interface was separated from the remaining patella by the osteotomy site. Morphological parameters of the newly formed bone, such as bone volume (BV), bone volume to total volume ratio (BV/TV), and bone mineral content (BMC), were calculated.
Histomorphometric Analysis
After micro-CT analysis, the fixed specimens were decalcified with a 1-to-1 mixture of 20% sodium citrate and 50% formic acid and then embedded in paraffin. Serial 5 μm–thick sections from the midsagittal plane of each specimen were cut using a microtome (Leica RM2125; Reichert-Jung GmbH) and stained with hematoxylin and eosin (H&E) or toluidine blue O/fast green. To facilitate comparisons among groups, all histological images were captured under exactly the same conditions of illumination and settings by a transmitted light microscope (CX31; Olympus) or a polarized microscope (Leica DM5500B; Leica Microsystems Cambridge Ltd). The captured images were imported to Image-Pro Plus (IPP) (version 6.0.0; Media Cybernetics Inc) for semiquantitative assessments of histomorphology.
In images of toluidine blue O/fast green–stained sections, the thickness of the regenerated fibrocartilage layer was calculated by an established protocol. 43 Proteoglycans were stained blue by toluidine blue O, 6 and IPP was applied to calculate the integrated optical density (IOD) of the labeled blue zone, which represents the proteoglycan content. Ten rectangular areas (100 × 100 μm2) in 4 different sections per animal were randomly selected from the fibrocartilage zone, and the value of the IOD and the number of chondrocytes were respectively averaged as the proteoglycan content of the regenerated fibrocartilage layer and the density of fibrocartilage cells. In H&E-stained sections, histological features and collagen alignment of the PPT healing interface were observed using the abovementioned microscope. The collagen birefringence under polarized light was quantified by IPP to semiquantitatively analyze its alignment and maturation at the healing interface. The detailed measurement methods were as follows. The polarized images were converted to 8-bit grayscale images by IPP in which noncollagenous material was dark (zero) and collagenous material was depicted in grayscale with values from 1 to 255. The grayscale values of the 8 randomly selected rectangular areas (50 × 50 μm2) in 4 different sections per animal were averaged to represent the alignment and maturity of collagen fibers. All of the data analyses were performed by the same person on the investigational team (C.C.).
Biomechanical Testing
Biomechanical testing was used as the ultimate index to evaluate the effects of 3 different initiation timings of LIPUS on the overall quality of PPT healing. A total of 64 QPPTT-C specimens harvested at postoperative week 8 or 16 (n = 8 per group per time point) were allocated for biomechanical testing by a Hounsfield test machine (H25K-S; Hounsfield Test Equipment Ltd) (Figure 1D). After the periarticular connective soft tissues, the suture material and tension band wire were carefully removed, the thickness and width of the PPT junction were measured 3 times using a fine caliper under a constant 5-N tensile load, and the mean value was used to calculate the cross-sectional area (CSA; mm2) of the PPT healing interface. The QPPTT-C specimen was loaded to failure at a rate of 20 mm/min after a preload of 1 N. Failure load (N) was obtained from the recorded load-deformation curve, and stiffness (N/mm) was calculated from the linear portion of this curve with the use of Office Excel 2010 (Microsoft Corp). The CSA of the PPT healing interface was used to normalize the failure load for calculating ultimate stress (MPa). During testing, 0.9% saline was applied to prevent dehydration of the QPPTT-C specimens.
Statistical Analysis
All statistical analyses were performed using SPSS 17.0 software (SPSS Inc). All quantitative data were expressed as mean ± SD and analyzed statistically using 2-way analysis of variance with the Bonferroni post hoc test to detect differences among the 4 groups. Statistical significance was set at P < .05.
Results
Postoperative Situation and Hemogram
In our study, postoperative hydrarthrosis was prone to occur in the immediate group. The incidence of hydrarthrosis in the immediate group (67.8%) was significantly higher than that in the control (10.7%), 7-day delayed (14.3%), or 14-day delayed (10.7%) groups. Hydrarthrosis was completely absorbed at 5.1 days postoperatively on average (range, 4-6 days). In addition, as compared with the control group, peripheral leukocyte counts in the immediate group were significantly increased from postoperative day 1 to day 3 and then decreased to control levels at postoperative day 7 (Table 1). The leukocyte counts in the 7-day or 14-day delayed groups were similar to that of the control group.
Peripheral Leukocyte Counts After Partial Patellectomy a
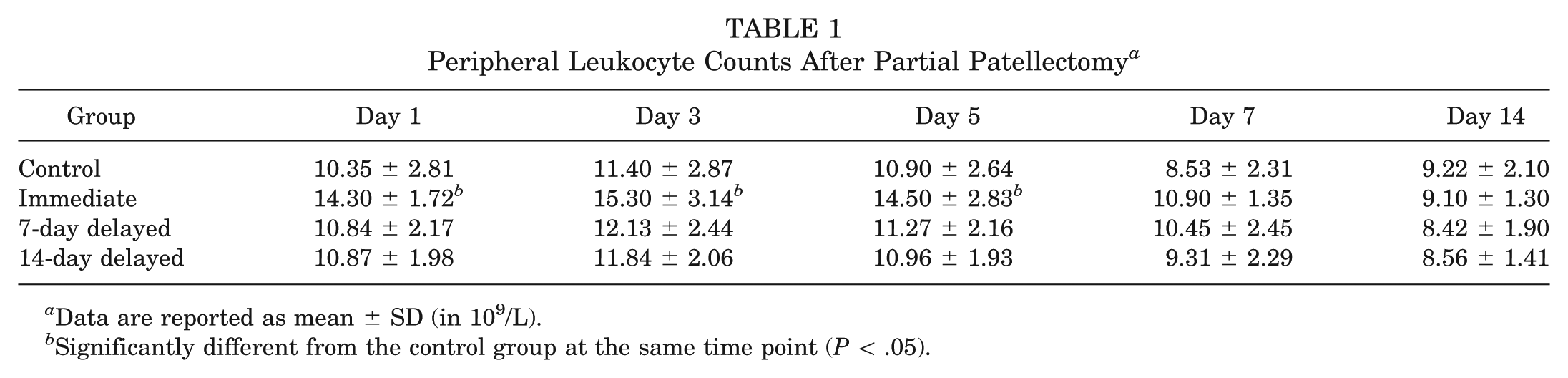
Data are reported as mean ± SD (in 109/L).
Significantly different from the control group at the same time point (P < .05).
Microstructural Analysis
After analyzing the scanning data of micro-CT, the 3D morphological parameters of the patella showed that the 3 LIPUS-treated groups had more new bone formation and mineralization at the PPT healing interface compared with the control group at 8 or 16 weeks postoperatively (Table 2 and Figure 3). At 8 weeks after surgery, the BV, BV/TV, and BMC of the 3 LIPUS-treated groups were significantly larger than those of the control group. Microstructural analysis of the newly formed bone showed that the 7-day delayed group had a significant increase of BV and BMC compared with the other groups (P < .05 for all). Additionally, BV/TV of the 3 LIPUS-treated groups was significantly greater than that of the control group (P < .05 for all). At postoperative week 16, BV of the 3 LIPUS-treated groups was significantly higher than that of the control group (P < .05 for all). Moreover, the difference in BV/TV and BMC was not statistically significant among the 4 groups.
Summary of Micro-CT Analysis of the Newly Formed Bone at the PPT Healing Interface a
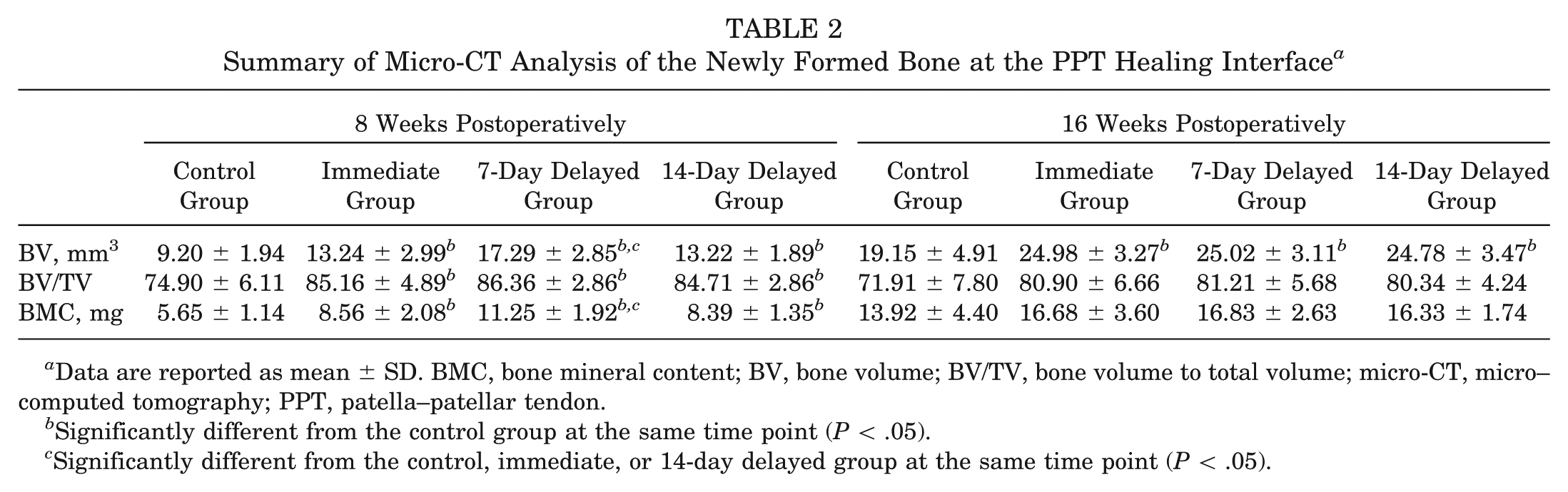
Data are reported as mean ± SD. BMC, bone mineral content; BV, bone volume; BV/TV, bone volume to total volume; micro-CT, micro–computed tomography; PPT, patella–patellar tendon.
Significantly different from the control group at the same time point (P < .05).
Significantly different from the control, immediate, or 14-day delayed group at the same time point (P < .05).
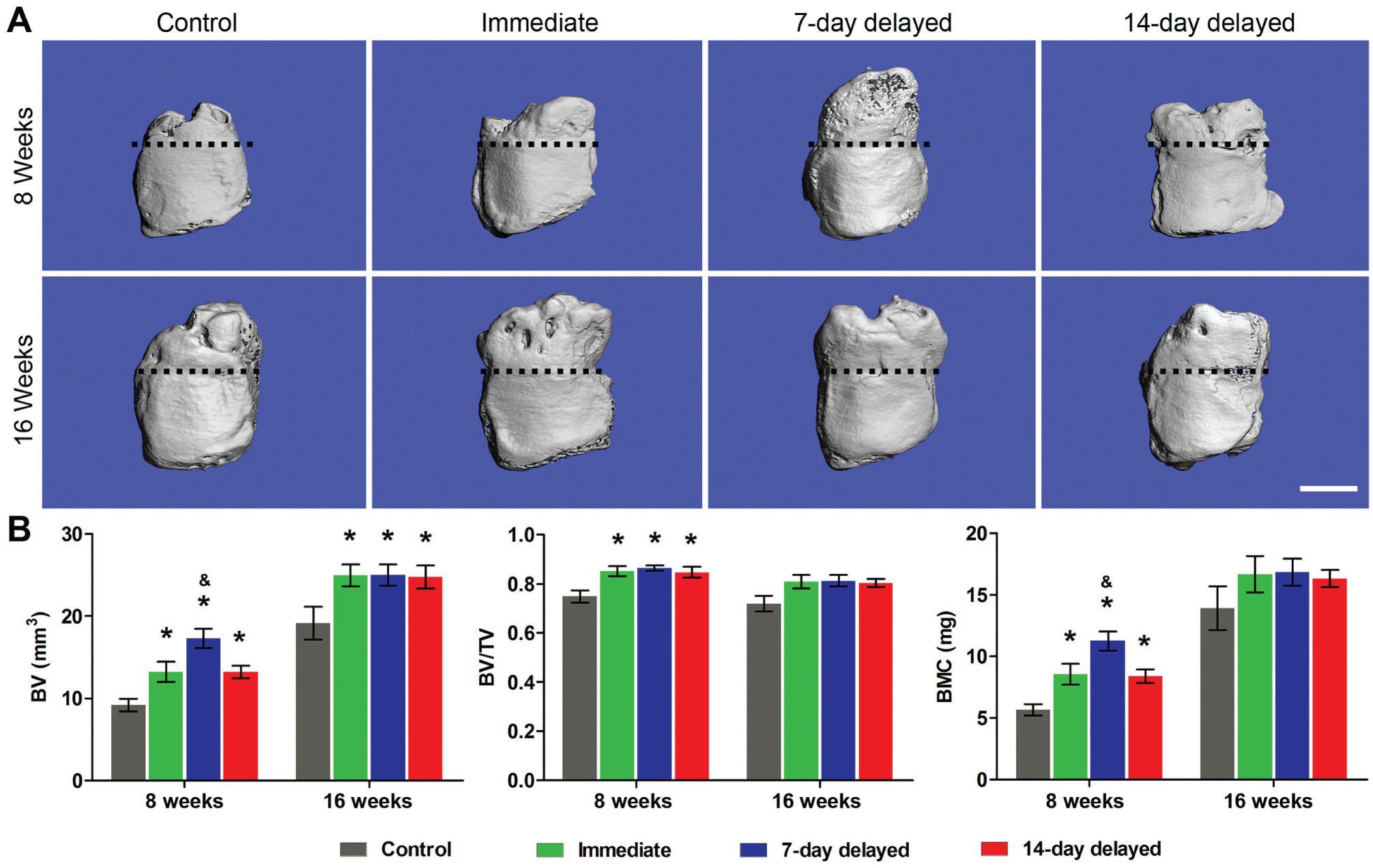
(A) Representative micro–computed tomography images of the proximal patella of the 3 low-intensity pulsed ultrasound stimulation (LIPUS)–treated groups and the control group at postoperative week 8 and week 16. The dotted line indicates the osteotomy site. n = 6 for each group/time point. Scale bar = 3 mm. (B) Comparison of the bone volume (BV), bone volume to total volume (BV/TV), and bone mineral content (BMC) in newly formed bone among the 4 groups at different time points. *Significantly different from the control group at the same time point (P < .05). &Significantly different from the control, immediate, or 14-day delayed group at the same time point (P < .05).
Histomorphological Assessments
According to H&E- or toluidine blue O/fast green–stained sections, the PPT healing interface at postoperative weeks 8 and 16 was characterized by newly formed bone extending from the proximal patella and a regenerated fibrocartilage layer bridging the newly formed bone and the residual patellar tendon in all groups (Table 3 and Figures 4 and 5). At 8 weeks after surgery, some histological differences of the PPT healing interface were observed between the LIPUS-treated groups and the control group. In the 3 LIPUS-treated groups, there was more woven bone, and a more robust fibrocartilaginous junction with a characteristic matrix rich in proteoglycans was seen at the PPT healing interface in comparison with the control group. Meanwhile, the remaining patella size of the LIPUS-treated groups enlarged more than that of the control group. In addition, only the immediate group or the 7-day delayed group showed a statistically thicker regenerated fibrocartilage layer compared with the control group (P < .05 for all). As for proteoglycan content and chondrocyte density in the regenerated fibrocartilage layer, statistical differences were found between the 3 LIPUS-treated groups and the control group (P < .05 for all). Under polarized light, collagen fibers in the healing interface did not show a significant difference among the 4 groups at postoperative week 8 (P > .05 for all) (Figure 6). At postoperative week 16, the healing interface in all 4 groups displayed better remodeling with respect to postoperative week 8. Healing and remodeling at the PPT junction were almost complete, with a resemblance to a healthy BTJ consisting of the characteristic 4 zones in all groups. However, the newly formed bone of the LIPUS-treated groups revealed better remodeling than that of the control group, characterized by well-developed lamellar bone and formation of more marrow cavities. Moreover, the difference of the remaining patella size between the LIPUS-treated groups and the control group became more apparent. Besides, the specimens in the LIPUS-treated groups contained a significantly thicker fibrocartilage layer and higher proteoglycan content than the control group (P < .05 for all), but the density of chondrocytes in the immediate and 7-day delayed groups displayed a significant decrease as compared with the control group (P < .05 for all). Furthermore, the 3 LIPUS-treated groups revealed significantly better parallel alignment and maturity of collagen fibers in the healing interface relative to the control group (P < .05 for all).
Comparison of the Histological Parameters at the PPT Healing Interface a
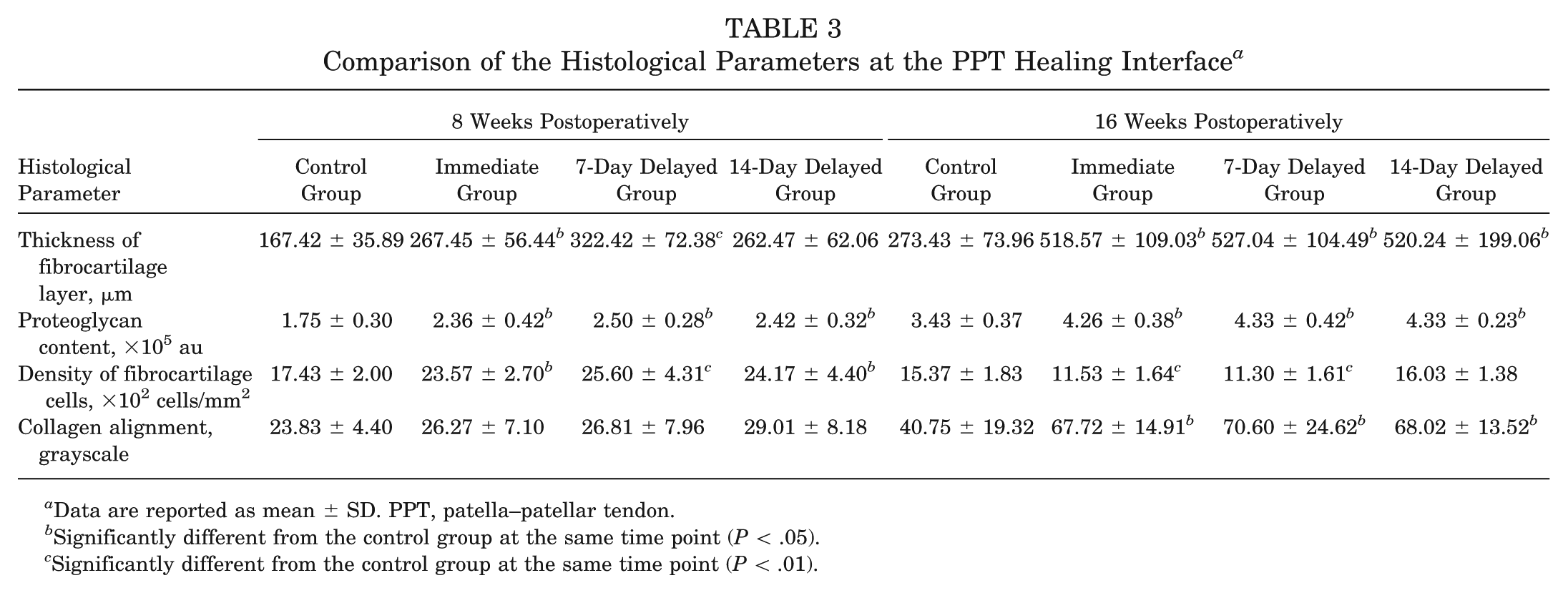
Data are reported as mean ± SD. PPT, patella–patellar tendon.
Significantly different from the control group at the same time point (P < .05).
Significantly different from the control group at the same time point (P < .01).
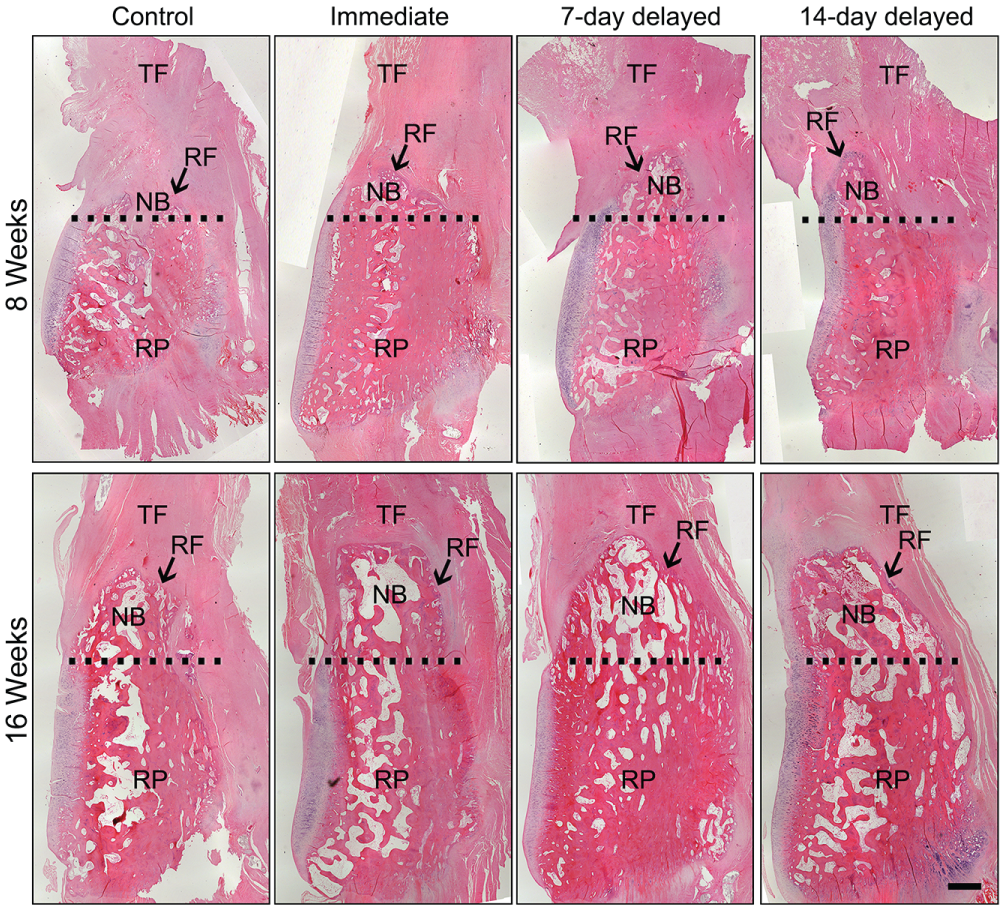
Representative midsagittal sections of the patella–patellar tendon healing interface of the 3 low-intensity pulsed ultrasound stimulation (LIPUS)–treated groups and the control group at postoperative week 8 or 16. The dotted line represents the osteotomy site. Newly formed bone enhanced in the 3 LIPUS-treated groups as compared with that of the control group at both 8 and 16 weeks postoperatively. Hematoxylin and eosin staining, n = 6 for each group/time point. Scale bar = 1 mm. NB, newly formed bone; RF, regenerated fibrocartilage layer; RP, residual patella; TF, tendon fiber.
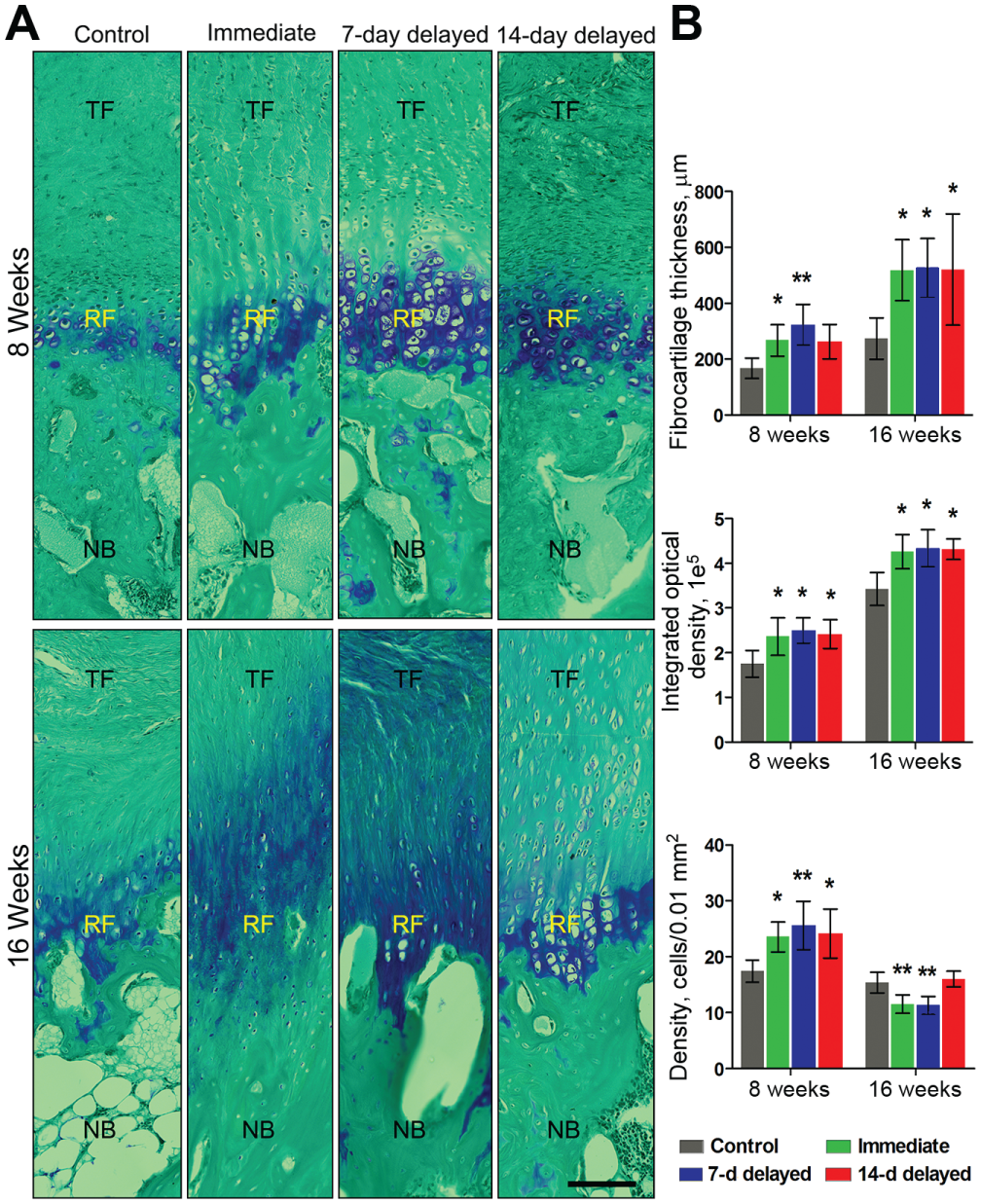
(A) The regenerated fibrocartilage zone as shown in toluidine blue O–stained sections. Toluidine blue O staining shows the deposition of proteoglycans, with an extracellular matrix composition in fibrocartilage. Toluidine blue O/fast green staining, n = 6 for each group/time point. Scale bar = 100 μm. (B) Comparison of the thickness of the fibrocartilage layer, the integrated optical density, and the density of fibrocartilage cells among the 4 groups at different time points. *Significantly different from the control group at the same time point (P < .05). **Significantly different from the control group at the same time point (P < .01). NB, newly formed bone; RF, regenerated fibrocartilage layer; TF, patellar tendon.
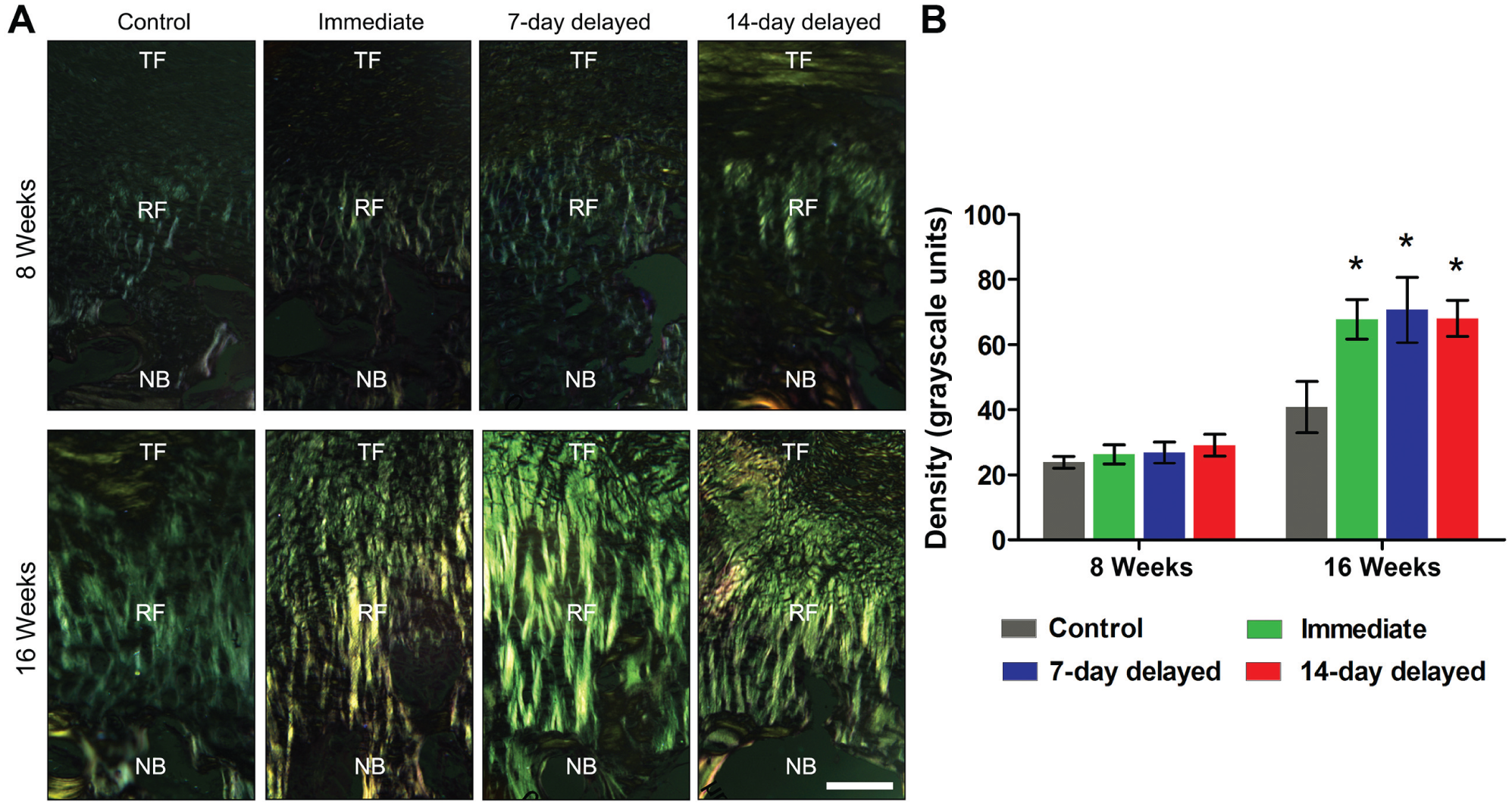
(A) Representative polarized images of collagen fiber alignment at the healing interface. Hematoxylin and eosin staining, n = 6 for each group/time point. Scale bar = 100 μm. (B) Comparison of the collagen birefringence among the 4 groups at different time points. *Significantly different from the control group at the same time point (P < .05). NB, newly formed bone; RF, regenerated fibrocartilage layer; TF, patellar tendon.
Mechanical Testing
Biomechanical testing indicated that the PPT healing quality enhanced with time and that PPT healing was optimized with LIPUS starting at postoperative day 7 (Table 4). At 8 weeks postoperatively, the values of failure load in the 3 LIPUS-treated groups were not significantly higher than that of the control group. However, ultimate strength, owing to the smaller CSA of the PPT healing interface, showed a significantly higher value in the 7-day delayed group when compared with the other groups (P < .05 for all). In addition, stiffness in the 7-day delayed group was significantly greater than that in all other groups (P < .05 for all). At 16 weeks postoperatively, failure load, stiffness, and ultimate strength of the PPT junction in the 3 LIPUS-treated groups improved significantly as compared with those of the control group (P < .05 for all). All specimens failed at the initial osteotomy site between the remaining proximal patella and the new bone during tensile testing, and no specimens were excluded (Figure 1D).
CSA and Biomechanical Properties of the PPT Healing Interface a
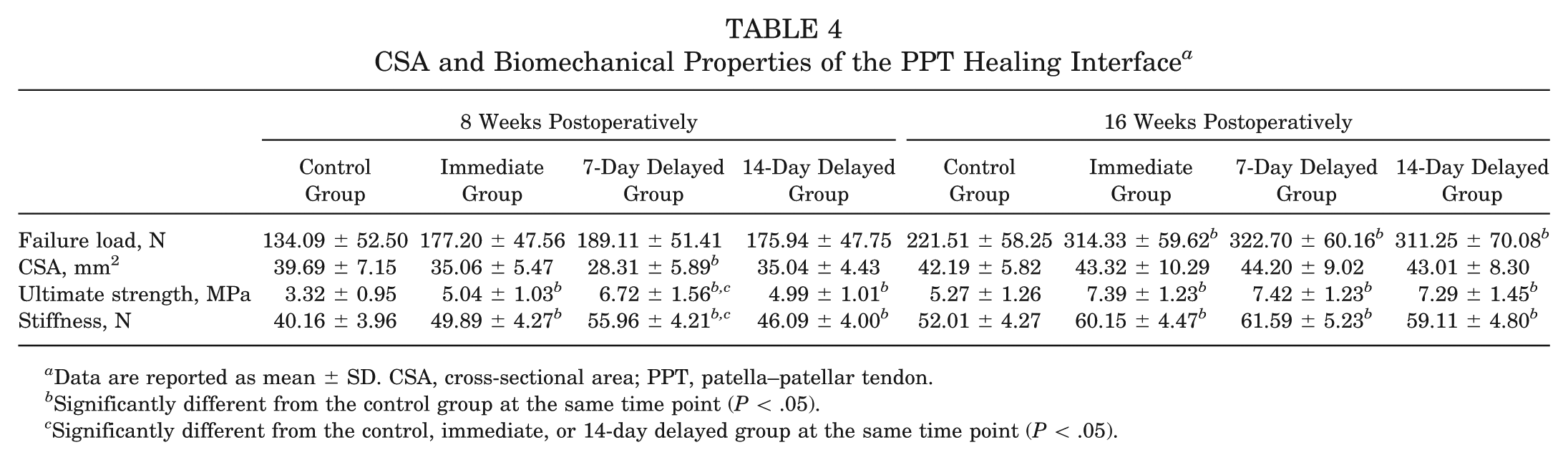
Data are reported as mean ± SD. CSA, cross-sectional area; PPT, patella–patellar tendon.
Significantly different from the control group at the same time point (P < .05).
Significantly different from the control, immediate, or 14-day delayed group at the same time point (P < .05).
Discussion
LIPUS was able to biomechanically accelerate T-B healing in an animal model, but in prior studies, the initiation timing of LIPUS was arbitrary, generally starting from the initial inflammatory phase after an injury to the time of sampling.19-22,35,37 In the current study, 3 representative and practicable time points were chosen to preliminarily optimize the initiation timing of LIPUS on T-B healing. The application of LIPUS initiated at day 0, 7, and 14 after partial patellectomy resulted in improved mechanical and biological parameters of PPT junction healing compared with those resulting from no treatment. A more mature PPT junction was achieved in the 7-day delayed group at 8 weeks postoperatively, as demonstrated by increased stiffness, ultimate strength, BV, and BMC. Thus, LIPUS initiated at 7 days postoperatively was more favorable for T-B healing. This study was the first to investigate the timing of initiation of LIPUS on T-B healing, which provides a valuable reference for further clinic and basic research about the optimal treatment protocols for LIPUS on T-B healing.
Prior studies have shown that LIPUS can accelerate new bone maturation by altering its microarchitecture.26,33,37,39 In the current study, the specimens in the 3 LIPUS-treated groups had a significant increase of new bone formation and maturation in the distal edge of the remaining patella by micro-CT and histology when compared with the control group, but the 7-day delayed group showed significantly more new bone volume and mineralization than the immediate and 14-day delayed groups at postoperative week 8. These variations in osteogenesis induced by the different ultrasonic treatment initiations might account for the biomechanical property difference of the 4 groups at week 8, as both newly formed bone size and mineral content were reported to be relevant to the biomechanical strength of the PPT complex. 18 Regrettably, the underlying cellular and molecular mechanisms regarding this osteogenic difference were not addressed in the current study. According to published studies, we suspect that different LIPUS treatment initiations might have disparate influences on the proliferation of osteoblasts, calcium uptake and endochondral ossification, and transiently upregulating expression of osteogenesis-related genes with the PPT healing interface.7,8,12,13,30,32,40 In addition, an enlarged remaining patella in the LIPUS-treated groups was shown in our results. This enlargement might be beneficial to decrease contact pressure of the patellofemoral joint so as to improve knee function and stability. 27
Apart from new bone formation, the regeneration of the fibrocartilage layer was another crucial factor contributing to T-B healing. 25 Histologically, this regenerated fibrocartilage layer is featured by chondrocytes uniformly embedded in an extensive extracellular matrix composed of collagen and proteoglycans. 20 Thus, collagen alignment, chondrocyte density, proteoglycan content, and fibrocartilage layer thickness were also used as vital indicators to evaluate PPT junction healing. In this study, the 3 LIPUS-treated groups showed more improved tissue integration with respect to the control group, characterized by a thicker fibrocartilage layer with increased proteoglycan content and better collagen fiber alignment. Potential explanations for this improvement may be that LIPUS can increase interleukin 1β (IL-1β), vascular endothelial growth factor (VEGF), β fibroblast growth factor (βFGF), and insulin-like growth factor 1 (IGF-1) levels at the healing interface, thus promoting protein synthesis, angiogenesis, and collagen deposition, as well as the proliferation of fibroblasts and chondroblasts within the previously avascular environment, resulting in an improvement of mechanical properties (stiffness, ultimate strength, and failure load).8,20,32,38,42
Above all, LIPUS with different initial timings can accelerate PPT healing more or less, but LIPUS initiated at postoperative day 7 was most effective among all of the treatment regimens in this study. The reasons for this difference may be that (1) under the regulation of growth factors and extracellular cytokines,2,24 such as VEGF, βFGF, bone morphogenetic proteins (BMPs), and transforming growth factor β1 (TGF-β1), pluripotent mesenchymal stem cells invaded the osteotomy site of partial patellectomy within 4 to 5 days and then differentiated into osteoblasts, chondroblasts, and fibroblasts.10,38,47 These cells gradually developed into a soft callus and subsequently woven bone penetrating into the tendon. 47 LIPUS treatment started at postoperative day 7 might be able to optimally regulate the production of those growth factors and extracellular cytokines, thus most effectively accelerating PPT junction healing. (2) LIPUS had certain proinflammatory effects when applied immediately after an injury.1,16,28 As shown in our study, peripheral leukocyte counts increased significantly at the inflammatory phase of the immediate group, and hydrarthrosis easily occurred in the operated knee of the immediate group. We speculated that the beneficial effects of LIPUS in the immediate group might have been partly offset by its proinflammatory effects. Consequently, the immediate group displayed significantly poorer tensile properties than the 7-day delayed group at postoperative week 8. (3) The rabbits in the 14-day delayed group missed LIPUS in the initial inflammatory phase and received the fewest numbers of ultrasonication in all of the LIPUS-treated rabbits. Therefore, the specimens of this group had the lowest healing quality among the 3 LIPUS-treated groups at postoperative week 8. To prove those interpretations, further research is required.
It is important to recognize the limitations of our study. First, only the early, middle, and later stages of postoperative inflammation were investigated in the current animal study, and more animal research should be performed to study the impacts of timing, duration, and intensity of LIPUS treatment on T-B healing before clinical trials. Second, there exist some differences in knee biomechanics and size of the repair region between rabbits and humans; thus, the findings of this study may not be simply translated to PPT junction healing of humans. Third, the LIPUS transducer size is about 1 cm larger than the PPT junction, which might also influence the peritendinous tissues around the healing enthesis. Although a larger transducer will guarantee the delivery of ultrasound to the healing interface, those affected peritendinous tissues may confuse the overall mechanical properties of the healing enthesis. Fourth, the relatively small sample size may lead to statistical errors while drawing a conclusion. Despite these limitations, this study indicated that LIPUS initiated at the middle inflammatory phase was more suitable for promoting T-B healing, and the findings of this study may offer some meaningful research foundations for future clinical and basic research.
Conclusion
For the first time, the initiation timing for LIPUS treatment on T-B healing was preliminarily optimized in the current study. While realizing that biological and functional T-B healing is still a significant challenge in sports medicine, the results of this study may serve as a research foundation for future clinical applications.
Footnotes
Acknowledgements
The authors thank Drs Dick Chow, Jiali Wang, Jerry Xu, and Huafang Li for their assistance at the Musculoskeletal Research Laboratory, Department of Orthopaedics and Traumatology, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong, China.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Natural Science Foundation of China (No. 81171699 and No. 84172072), the Specialized Research Fund for the Doctoral Program of Higher Education (No. 20110162110068), the Development and Reform Commission of Hunan Province of China (No. [2012]1493), and the Fundamental Research Funds for the Central Universities of Central South University (2016zzts124).