
Abstract
Background:
Bone peg grafting (BPG) has been advocated for early-stage humeral capitellar osteochondritis dissecans (COCD). However, the clinical and radiological results of BPG, along with its indications, have not been described in detail.
Hypothesis:
COCD classified as International Cartilage Repair Society (ICRS) osteochondritis dissecans (OCD) I or II in adolescent baseball players can be treated successfully by BPG.
Study Design:
Case series; Level of evidence, 4
Methods:
Eleven male baseball players (age range at surgery, 13-16 years) who underwent BPG for COCD were enrolled in this study. No improvement had been seen in any patient after 6 months of preoperative nonthrowing observation. During surgery, 2 to 5 bone pegs were inserted into the COCD lesion after confirmation of lesion stability to the bony floor. All patients were directly evaluated at 12 and 24 months after surgery by physical findings, radiological prognosis, and magnetic resonance imaging (MRI).
Results:
Of the 11 patients, 10 could return to comparable baseball ability levels within 12 months. The Timmerman-Andrews score improved significantly from a mean ± SD of 171.8 ± 12.1 preoperatively to 192.3 ± 6.5 at the final observation. Radiological healing of the lesions was determined as complete in 8 patients and partial in 3. Patients possessing a centrally positioned lesion or a lesion <75% of the size of the capitellum tended most strongly to achieve complete radiological healing, while growth plate status appeared unrelated to outcome. The mean Henderson MRI score improved from 6.3 ± 1.5 to 4.8 ± 1.6 at 12 and 24 months after BPG, respectively. MRI findings also suggested that remodeling of COCD lesions had continued to up to 24 months postoperatively.
Conclusion:
BPG enabled 91% of COCD patients with ICRS OCD I or II to return to preoperative baseball abilities within 12 months. Integration of the grafted site may continue until at least 24 months postoperatively. An ICRS OCD I or II lesion with central positioning and/or occupying <75% of the size of the capitellum in the coronal plane is a good indication for BPG.
Capitellar osteochondritis dissecans (COCD) is a focal injury of the articular cartilage involving separation of a segment of cartilage from subchondral bone that is rarely encountered in the dominant-side elbow of adolescent throwing athletes.3,6 The exact cause of COCD is unclear, although repetitive microtrauma at the capitellum created by compressive and shearing forces from valgus stress during the acceleration phase of throwing, as well as immaturity of the articular surface, seems to trigger this condition.3,16,21 If the COCD lesion is stable to the bony floor, it will likely heal with rest and nonoperative management. After the lesion becomes unstable or detached from the floor, however, surgical intervention provides better results.29,30,35
Minami et al 22 first established a radiological grading system of COCD in 1979 such that grade I lesions included elbows in which a translucent cystic shadow was seen in the lateral or middle parts of the capitellum; grade II lesions were split type, whereby a clear zone or split line was seen between the lesion and adjacent subchondral bone; and grade III lesions exhibited detached free body formation.22,26 As grade I and II lesions are mostly stable, nonoperative therapy constitutes the first choice of treatment—such as suspension of throwing, avoidance of carrying heavy loads, and passive range of motion exercise that includes the hip, shoulder, and elbow joint. The percentage of patients with Minami radiological grade I or II who are treated nonoperatively for >6 months and who could return to previous levels of sports ability has ranged from 58% 23 to 76%. 20 When symptoms persist with no sign of radiological recovery after 6 months of nonoperative management, surgical intervention should be considered.
The appropriate treatment procedure for COCD is commonly selected during intraoperative observation based on the International Cartilage Repair Society (ICRS) osteochondritis dissecans (OCD) classification system. 9 If the cartilage exhibits signs of advanced progression, such as a dead in situ lesion (ie, ICRS OCD III) or a free body formation (ie, ICRS OCD IV), an autologous osteochondral graft from the distal femur or rib may be the most suitable treatment course, especially for relatively large lesions, for which excellent clinical and radiological results have been reported.11,12,27 If the defect is small in such advanced lesions, bone resurfacing by marrow stimulation via microfracture or drilling may also be effective.14,33
In rare instances of COCD, the hyaline cartilage of the capitellum is preserved to result in softening alone (ie, ICRS OCD I) or a fissure in the cartilage (ie, ICRS OCD II). At this early disease stage, procedures are indicated that retain the normal contour of the capitellum and stabilize the osteochondral fragment to the floor.3,29 However, few studies on the surgical treatment of these lesions exist.
We hypothesized that cortical bone peg grafting (BPG) from the articular cartilage to the subchondral bone within the initial stages of COCD could unite the lesion with the bony floor and preserve the original local hyaline cartilage of the capitellum, not only by bone marrow stimulation, but also by stabilization of the fragment. Accordingly, we consecutively performed BPG on adolescent players with ICRS OCD I or II and retrospectively assessed their clinical and imaging results.
Methods
Participants
Eleven consecutive adolescent baseball players who underwent BPG for COCD at the senior author’s (H.K.’s) institution between February 2004 and May 2012 were enrolled in this study. The indications for BPG were as follows: (1) failure of at least 6 months of conservative nonthrowing observation, (2) Minami grade I or II COCD lesions evaluated with plain tangential anteroposterior radiographs of the forearm with the elbow at 45° of flexion within 1 month before surgery, and (3) ICRS OCD I or II confirmed by arthroscopy and direct observation immediately before the procedure. All patients were male and affected in the dominant-side elbow (10 on the right and 1 on the left). Regarding fielding position, the sample comprised 8 pitchers, 2 outfielders, and 1 infielder. All subjects had initially complained of elbow pain while playing baseball and were monitored by plain radiographs during an abstinence of throwing sports for at least 6 months. Since the lesions and symptoms persisted, all patients opted for surgical treatment. The average age at the time of surgery was 14 years (range, 13-16 years). The mean range of elbow flexion was 132°. As compared with the contralateral elbows, mean restriction was 9° for extension and 6° for flexion.
Immediately before surgery, plain radiographs demonstrated Minami grade I in 1 patient and grade II in 10 patients. Lesion size in the coronal plane was larger than half the width of the capitellum in the tangential anteroposterior view for all patients, with an average size of 67.5% (range, 55.0%-85.6%). Lesion locations as determined from plain radiographs in the tangential anteroposterior view were divided into 2 types: lateral, in which the radiolucency or fragmented lesion involved the lateral wall of the capitellum (7 patients), and central, whereby the lesion had not reached the lateral wall (4 patients). Growth plates at the lateral condyles of the affected elbows were open in 5 patients at the time of surgery and closed in the remaining 6. Preoperative magnetic resonance imaging (MRI) was obtained for all patients with a Signa Horizon LX 1.5T (GE Medical Systems) with a 20-cm circular surface coil. We procured unenhanced oblique-sagittal T1-weighted spin echo images (repetition time/echo time: 580/16 ms) and oblique-coronal and oblique-sagittal T2-weighted fast spin echo images (repetition time/echo time: 2000/14 ms) with a section thickness of 2 mm, an intersection gap of 0.5 mm, a matrix of 320 × (202-256), and a field of view of 120 mm. The MRI classification system recently proposed by Itsubo et al 10 was used for preoperative MRI assessment. Three patients were judged as stage 1, 5 as stage 2, 2 as stage 3, and 1 as stage 4. In terms of arthroscopic and direct visual findings just before the bone peg procedure, 2 patients were determined as ICRS OCD I and the remaining 9 as OCD II.
Surgical Technique
All operations were performed under general anesthesia by the senior author (H.K.), who assessed the continuity of the capitellar cartilage surface by direct vision and arthroscopy and evaluated the stability of the capitellar lesion by palpation with an arthroscopic probe. The capitellar lesion was explored between the extensor carpi ulnaris and the anconeus muscles. The elbow capsule was opened and the capitellar lesion exposed, after which the lesion was graded according to ICRS OCD classification. Stable lesions with a continuous but softened area covered by visually and elastically normal cartilage were classified as ICRS OCD I (2 patients), while those with partial discontinuity that were stable when probed were determined as ICRS OCD II (9 patients).
Another skin incision of 3 cm in length was made at the posterior metaphysis of the ipsilateral olecranon. The extensor carpi ulnaris and the flexor carpi ulnaris muscle were separated from each other, and the medial side of the cortex of ulna was exposed. A rectangle measuring approximately 20 × 10 mm was outlined on the medial cortex of the ulna, after which the 4 corners of the rectangle were bored with a 1-mm-diameter Kirschner wire. Thereafter, up to 3 bone pegs of roughly 20 mm in length were carefully harvested from the cortex with a surgical bone saw. A similar procedure was performed on the lateral side of the cortex of the ulna in patients requiring 4 or 5 bone pegs. The pegs were approximately 2 mm in diameter at the tip and 3 mm in diameter at the head (Figure 1A). Holes in the lesion for BPG were interspaced by approximately 5 mm. The depth of each hole was approximately 25 mm, as made with a 3-mm-diameter Kirschner wire instead of a drill, to protect the cartilage from excessive shearing stress. Bone pegs were inserted into the holes with tweezers to a depth of 10 mm, after which a flat surface rod was placed on the head of the bone peg to advance it by gentle tapping with a mallet to a depth slightly lower than the articular cartilage surface (Figure 1B). The incised joint capsule was left open; the fascia of the extensor carpi ulnaris and anconeus was firmly sutured; and the wound was closed.
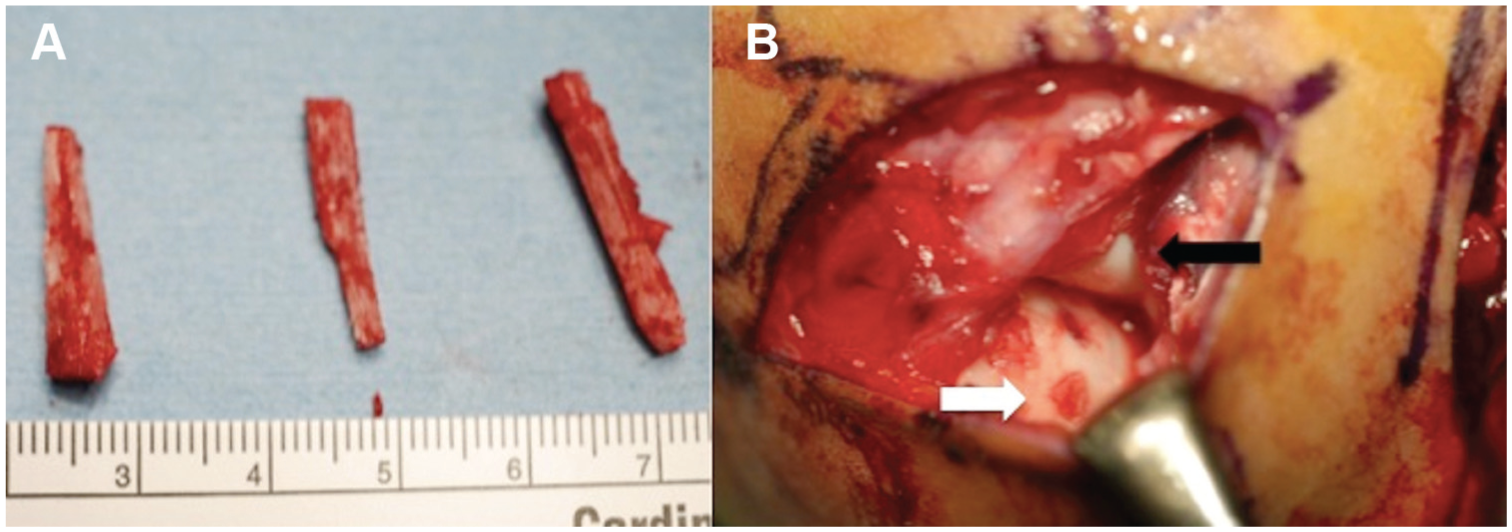
Intraoperative photographs (patient 3). (A) Bone pegs harvested from the cortex of the ipsilateral olecranon. (B) Capitellum after insertion of 3 bone pegs (white arrow). The elbow is flexed at 90°. The black arrow indicates the radial head.
Postoperatively, the elbow joint was immobilized in a plastic cast at 90° of flexion for 3 weeks. Active and assisted passive range of motion exercises were gently started after removal of the cast. Throwing was allowed 6 months after the operation, starting from short to longer distances at higher velocities. The patients were allowed to return to preinjury levels of competitive baseball between 8 and 12 months postoperatively.
This study was approved by the institutional review board and ethics committee. All patients and legal guardians provided informed written consent for inclusion in the study.
Postoperative Evaluation
All patients were clinically evaluated at 24 months postoperatively during a mean follow-up period of 33.9 months (range, 24-59 months). The rating system of Timmerman and Andrews 32 was used for comparisons between pre- and postoperative elbow conditions in each patient. We defined return to sports as a return to preinjury levels of sports ability, and we recorded the time required after surgery for a return to sports for all subjects.
In terms of postoperative radiographic changes, we divided the subjects into 3 groups—complete, partial, and no radiological healing—based on plain radiographs in the tangential anteroposterior and oblique views taken at 24 months after surgery. We regarded the following findings as being indicative of complete radiological healing: (1) disappearance of the radiolucent area without free body formation and (2) recovery of a spherical contour of the subchondral bone under the humeral capitellum on postoperative radiographs. We defined partial radiological healing as when the above findings were observed partly or when abnormal shadows remained in the capitellum. Patients displaying no improvement or worsening of radiological findings were classified into the no-healing group. Moreover, preoperative radiographs were retrospectively investigated in these groups and compared for the following aspects: (1) size of the lesion, as determined by width in the tangential anteroposterior view; (2) percentage of the lesion, defined as the width of the lesion divided by the diameter of the capitellum in the tangential anteroposterior view; (3) location of the lesion, as either central or lateral; and (4) condition of the growth plate, as either open or closed.
Sequential changes in repair sites were evaluated on MRI taken at 12 and 24 months after surgery by the first author (H.O.) using the scoring system of Henderson et al. 8 Although designed as an assessment tool for repair sites of autologous chondrocyte implantation, this system was found to be suitable for the evaluation of healing at surgically treated sites, especially those aimed at cartilage restoration. 12 The type and modality of MRI were identical throughout the study. Four subcategories—fill of repair site, signal at repair site, bone marrow edema, and joint effusion—were individually scored from 1 (best) to 4 (worst), after which overall scores were calculated for comparisons of postoperative MRI change between 12 and 24 months. A board-certified orthopaedic surgeon (H.O.) who was not the main BPG procedure operator performed the radiological and MRI review.
Statistical Analysis
All scoring data are presented as mean ± SD. The paired t test was used for comparisons between pre- and postoperative clinical scores and for those among postoperative MRI scores. Receiver operating characteristic (ROC) curve analysis was adopted for determining the optimal cutoff value of lesion size in relation to radiological prognosis. For the analysis of correlations between preoperative growth plate status and radiological healing status, we employed Fisher exact test. The level of statistical significance was set at P < .05. Statistical analyses were performed with the statistical package R (v 3.1.1; http://www.r-project.org).
Results
During the course of the study, we observed no postoperative complications, such as infection, neurological problems, fracture, or contracture. No patients complained of elbow pain during activities of daily living or sports throughout follow-up. Of the 11 participants, 10 (91%) could regain comparable baseball ability levels within 12 months after BPG, with the remaining adolescent switching to basketball between junior and senior high school (patient 10). Timmerman-Andrews scores improved in all patients and significantly overall from 171.8 ± 12.1 preoperatively to 192.3 ± 6.5 at the observation endpoint (P < .01). The subjects in this study possessed stable lesions and had no complaints in activities of daily living before surgery, stating occasional pain, swelling, and activity limitation for throwing activities only. Thus, the preoperative Timmerman-Andrews scores of the patients were high and ranged from 150 to 185 (Table 1).
Clinical Results and Radiological Healing of the Capitellar Osteochondritis Dissecans Lesion a
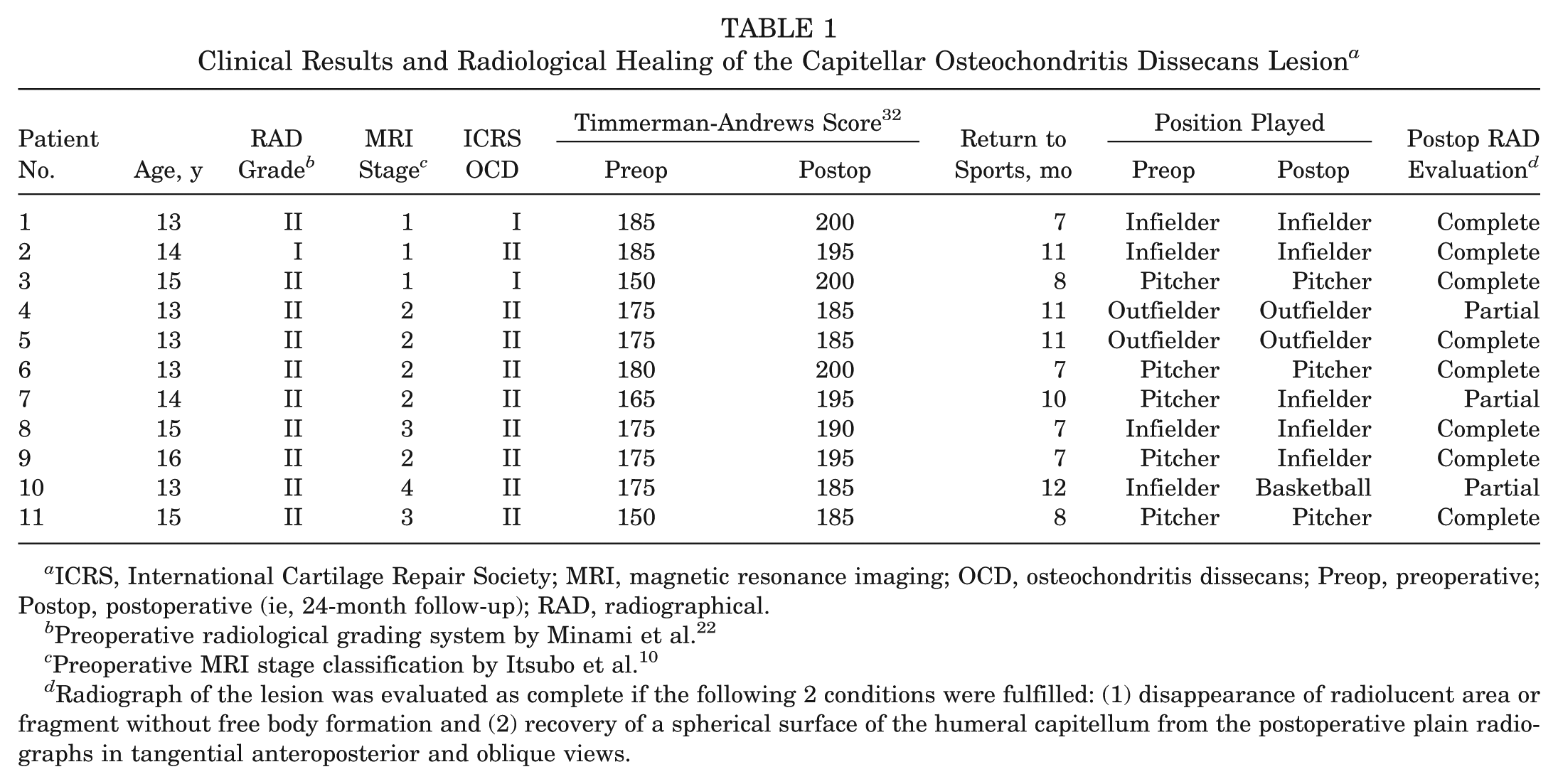
ICRS, International Cartilage Repair Society; MRI, magnetic resonance imaging; OCD, osteochondritis dissecans; Preop, preoperative; Postop, postoperative (ie, 24-month follow-up); RAD, radiographical.
Preoperative radiological grading system by Minami et al. 22
Preoperative MRI stage classification by Itsubo et al. 10
Radiograph of the lesion was evaluated as complete if the following 2 conditions were fulfilled: (1) disappearance of radiolucent area or fragment without free body formation and (2) recovery of a spherical surface of the humeral capitellum from the postoperative plain radiographs in tangential anteroposterior and oblique views.
Complete radiological healing of lesions was confirmed at 24 months in 8 subjects, who had all resumed competitive baseball at preoperative ability levels (Figure 2). In the 3 partial radiological healing patients (patients 4, 7, and 10), whereas the lateral part of the lesion was healed and its size reduced, the radiolucent line between the lesion and the bony floor remained (Figure 3). No patients were classified as no radiological healing.
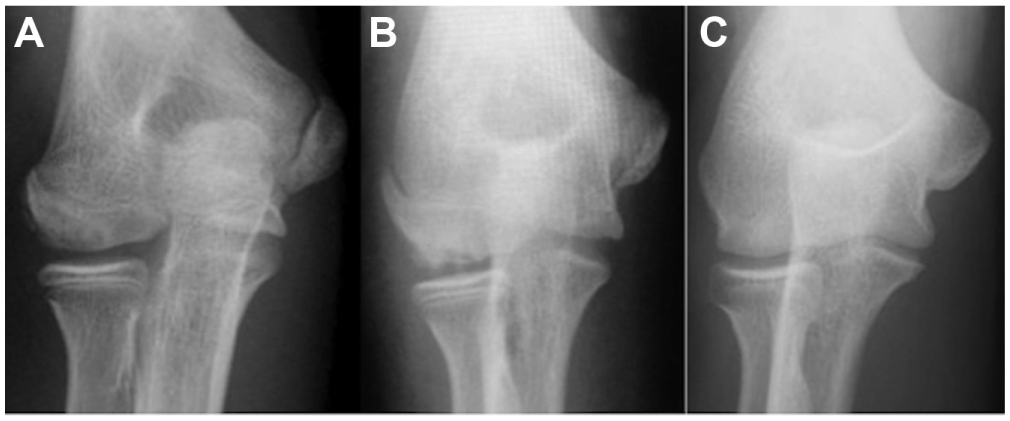
Tangential anteroposterior radiographs of an elbow exhibiting complete radiological healing (patient 1). (A) Preoperative radiograph disclosing lateral type grade II osteochondritis dissecans. The growth plate is open. The lesion is 10 mm in width, and the lesion percentage is 75.3%. (B) Immediately after grafting 3 bone pegs. (C) Postoperative radiograph at 24 months revealing complete healing of the lesion.

Tangential anteroposterior radiographs of an elbow exhibiting partial radiological healing (patient 4). (A) Preoperative radiograph showing Minami grade II, lateral type OCD. The growth plate is open. The lesion is 16.5 mm in width, and the lesion percentage is 85.6%. (B) Immediately after grafting 5 bone pegs. (C) Postoperative radiograph at 24 months disclosing partial radiological healing.
Table 2 summarizes the preoperative radiological features between the groups. In patients with complete radiological healing, lesion size and percentage tended to be smaller than those in patients with partial healing. According to ROC curve analysis, the cutoff point for the percentage of the lesion leading to complete radiological healing was <75.3% (sensitivity, 66.7%; specificity, 100%; area under the ROC curve, 0.750). Four of the 8 patients in the complete healing group displayed lateral-type COCD, while all 4 patients with central lesions achieved complete radiological healing. In contrast, 3 of 7 lateral-type lesions resulted in partial healing. There was no relationship between the status of the growth plate and radiological healing (P = .55, Fisher exact test). The bone pegs disappeared gradually and were undetectable at 12 months after surgery. There were no patients in which postoperative radiographs revealed fracture of grafted bone pegs.
Comparison of Preoperative Radiographs at the Capitellar Osteochondritis Dissecans Lesion Between Complete Healing and Partial Healing Groups
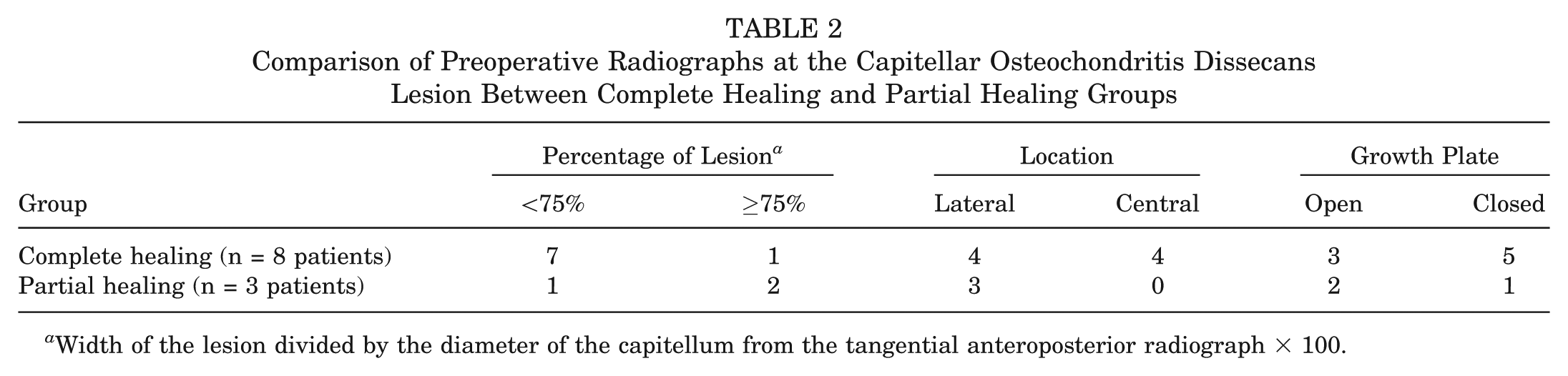
Width of the lesion divided by the diameter of the capitellum from the tangential anteroposterior radiograph × 100.
MRI of the elbow was performed before BPG and at 12 and 24 months afterward in all except 2 patients, which was due to claustrophobia at 24 months in patient 10 and economical reasons at 12 months in patient 11. In the remaining 9 data sets, the average overall MRI score improved significantly from 6.3 ± 1.5 to 4.8 ± 1.6 at 12 and 24 months after BPG, respectively (P < .01) (Table 3). MRI evaluation category scores were improved in 6 patients for signal at the repair site, 3 patients for bone marrow edema, and 4 patients for effusion at 24 months from 12 months postoperatively. One patient achieved an overall MRI score of 4 at 12 months after BPG, while 7 others attained this score at 24 months after surgery. Since capitellar hyaline cartilage signal was preserved postoperatively, we evaluated complete fill of the repair site for all patients at 12 and 24 months after BPG. Signals indicating that the grafted bone pegs remained were evident in 7 patients at 12 months postoperatively, but these had disappeared at 24 months in 5 patients (Figure 4). MRI revealed residual bone pegs in 2 patients at the study endpoint (patients 4 and 7). Several MRI scans disclosed that the lesion remained fragmented, with a T2 high-intensity gap between the subchondral bone and floor of the lesion. These were considered to represent an abnormal signal at the repair site. Bone marrow edema proximal to the bone pegs was observed in 5 of 10 patients, and joint effusion around the radial head or olecranon fossa was noted in 6 of 10 patients at 12 months postoperatively. These signals were absent at the observation endpoint in most patients (Table 3).
MRI Score at 12- and 24-Month Follow-up a
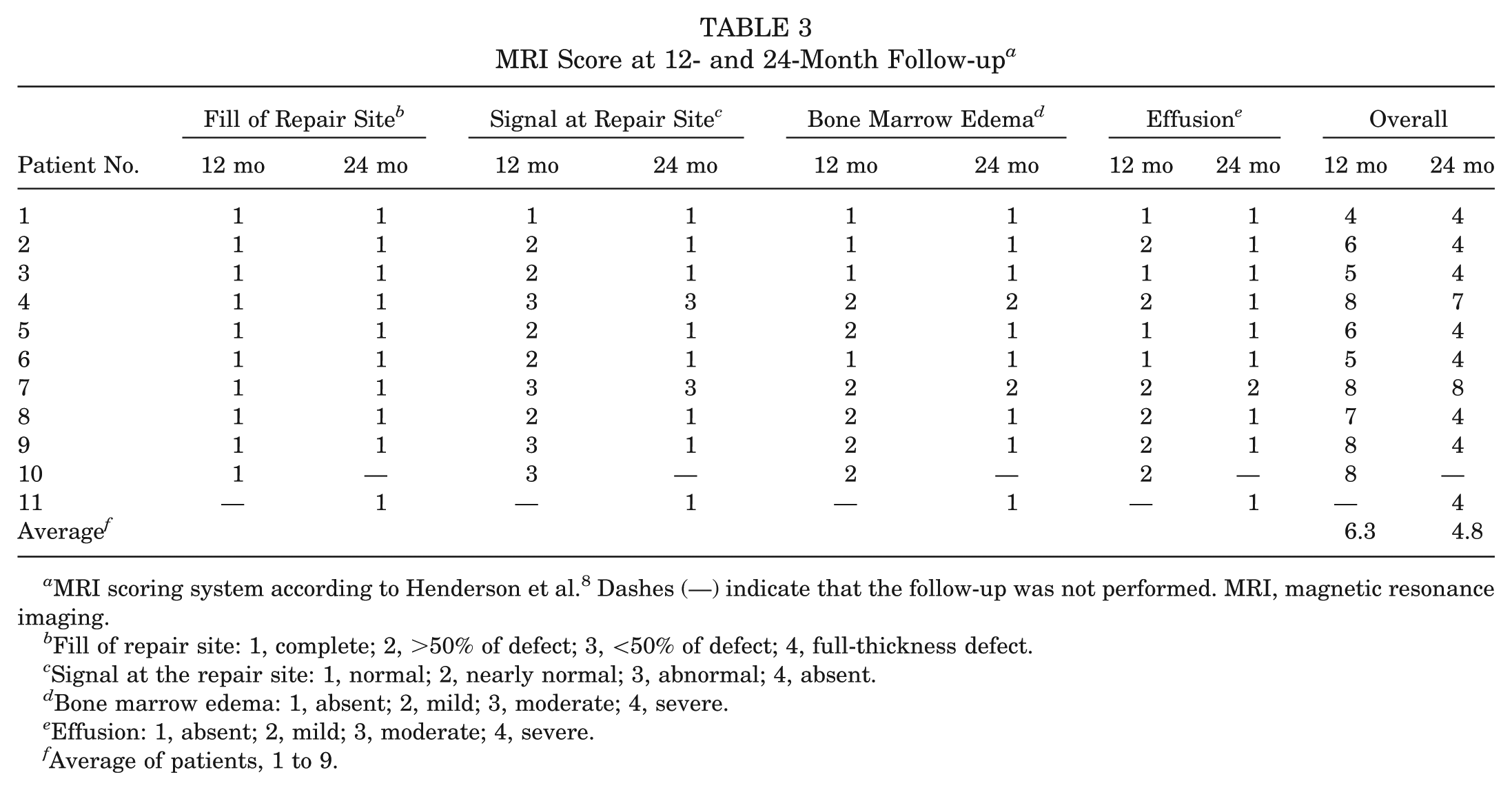
MRI scoring system according to Henderson et al. 8 Dashes (—) indicate that the follow-up was not performed. MRI, magnetic resonance imaging.
Fill of repair site: 1, complete; 2, >50% of defect; 3, <50% of defect; 4, full-thickness defect.
Signal at the repair site: 1, normal; 2, nearly normal; 3, abnormal; 4, absent.
Bone marrow edema: 1, absent; 2, mild; 3, moderate; 4, severe.
Effusion: 1, absent; 2, mild; 3, moderate; 4, severe.
Average of patients, 1 to 9.
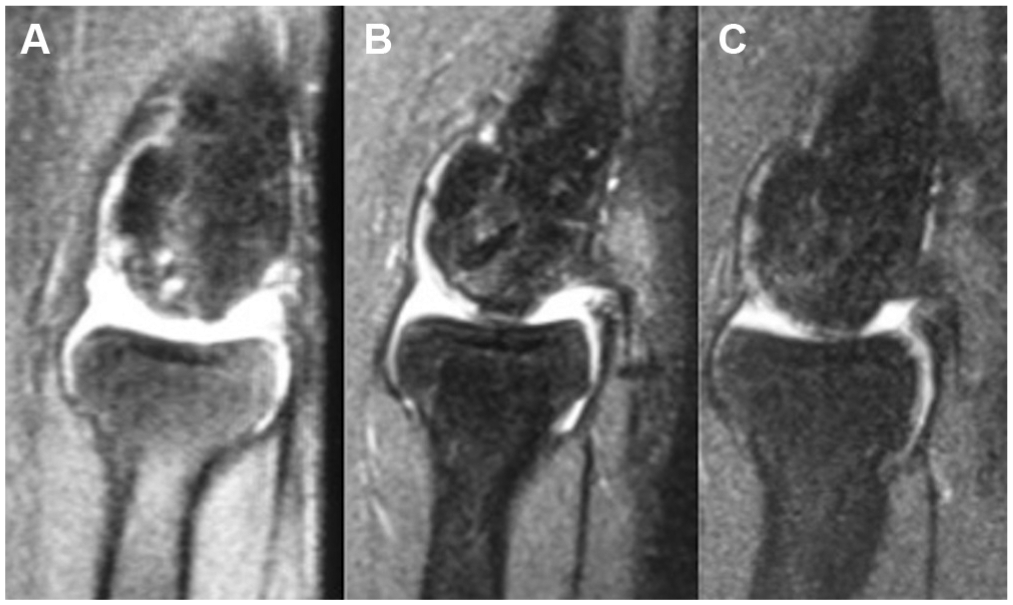
Oblique-sagittal T2-weighted fast spin echo magnetic resonance imaging (MRI) of an elbow exhibiting complete radiological healing (patient 8). (A) Preoperative MRI. Normally shaped capitellum—with several spotted areas of higher intensity than that of the cartilage, with discontinuity of the chondral surface signal, and with no high signal interface—is apparent between the lesion and the floor. Itsubo MRI classification stage is 3. (B) Postoperative MRI at 12 months reveals nearly normal signaling at the repair site, with mild bone marrow edema and joint effusion. The signal of a grafted bone peg (white arrow) remains. (C) Postoperative MRI at 24 months demonstrating normal signaling at the repair site, without evidence of bone marrow edema, joint effusion, or residual bone peg.
Discussion
The literature supports a high spontaneous healing potential of COCD in its early stages and recommends nonoperative management as the first treatment choice.20,29 However, there are some patients who persistently show no sign of radiological recovery after 3 to 6 months of throwing abstinence. In such situations, surgical intervention may be considered for competitive throwing athletes. The appropriate surgical procedure should be decided according to lesion size, stability, viability, location, and patient age.3,29 If the COCD lesion is progressed at ICRS OCD III or IV and unstable or detached from the floor, an autologous osteochondral graft from the distal femur or rib is generally the most suitable method, especially for a large lesion size.11,27 In patients with stable ICRS OCD I or II COCD lesions after nonoperative treatment, however, several surgical options are available. Mosaicplasty achieves excellent results but may be too invasive for this early stage, sacrificing the intact cartilage of the femur or rib. Arthroscopic debridement of the softened or fissured cartilage with or without loose body removal has also been shown to relieve symptoms, although the rate of return to preinjury sports activity varied from 40% 28 to 81%. 4 Moreover, 38% of patients receiving this procedure experienced a recurrence of locking or catching. 4 Bradley and Petrie 3 found that drilling of small lesions measuring <55% of the capitellum, along with debridement of the damaged cartilage to the stable margin, may have a good prognosis. Other authors have described the efficacy of arthroscopic bone marrow stimulation via transhumeral or transarticular drilling/microfracture for COCD,19,33 but these series contained various stages of cartilage lesion. Only Krijnen et al 15 reported good clinical results in 4 adolescent athletes with early-stage COCD, with an average follow-up of 5 months. Therefore, the clinical and radiological results of patients with ICRS OCD I or II after failed nonoperative treatment have not been precisely investigated.
It is known that recovery after cartilage debridement with marrow stimulation is not the regeneration of hyaline cartilage but rather the induction of fibrous cartilage. Since we believe that surgical intervention for early-stage COCD should aim for osteochondral fragment fixation with preservation of local cartilage, we opted for BPG to conserve the hyaline cartilage of the capitellum in our cohort with early-stage COCD lesions that involved >55% of the surface area of the capitellum. The main advantage of BPG as compared with simple drilling is that it secures the lesion to the floor as a physiological scaffold and becomes integrated into the grafted site.
Bandi and Allgöwer 2 were the first to describe the technique of drilling and BPG. In their single patient with OCD in the distal femur, the fragment was solidly united with the floor. Afterward, BPG was performed on patients with lesions corresponding to ICRS OCD II or III in the distal femoral articulation and resulted in a high rate of fragment union.7,13,18,24 Arcq 1 first performed BPG for COCD but did not describe the results in detail. Oka et al 26 then investigated the clinical and radiological results of BPG in 16 patients with Minami grade I or II COCD lesions and witnessed that 15 obtained bony union after average periods of 4.7 months for grade I and 7.1 months for grade II. On the basis of these findings, they proposed that BPG might be effective for relatively early-stage lesions. However, they did not address the possibility of returning to previous levels of sports ability, nor did they evaluate pre- or postoperative cartilage conditions in detail. Mihara et al 20 treated 7 patients at various stages of COCD by BPG in their 27-patient series. Two patients with early-stage COCD receiving BPG achieved Timmerman-Andrews scores of 185 and 200, respectively. Thus, this study restricted the indication for BPG to ICRS OCD I or II only.
We observed excellent clinical results for both ICRS OCD I and II lesions in this investigation. Timmerman-Andrews scores, pain, and range of motion of the elbow were improved in all patients. Of the 11 subjects, 10 (91%) could return to comparable ability levels within 12 months. However, the lesions remained fragmented at 24 months postoperatively in 3 of 11 patients. In these 3 patients with partial healing, Timmerman-Andrews scores were high (range, 185-195) and there were no obvious differences when compared with the scores of patients with complete healing. A restriction in elbow extension was the reason for point deduction in Timmerman-Andrews scores. The patient who quit baseball in this series belonged to this group. His cessation might have been due to incomplete radiological recovery. Retrospective comparisons of preoperative radiographs between the complete and partial healing groups uncovered that a larger size lesion and a lateral position tended to be potential factors associated with a poor radiological prognosis. Similar findings were reported in a case series of arthroscopic debridement: Byrd and Jones 5 pointed out that an avulsed lateral fragment may be indicative of an unfavorable result.
To our knowledge, this is the first study to perform pre- and postoperative MRI assessment of BPG for COCD. In 7 of 9 patients, a grafted bone peg signal clearly remained at 12 months after surgery with intensity different from that of the surrounding bone marrow. However, such signals were absent in 5 patients 12 months afterward and contributed to the improvement in Henderson score at 24 months compared with 12 months postoperatively. This observation implies that the integration of bone pegs may occur 12 months after BPG and that remodeling of the OCD lesion after BPG requires more than 12 months. Nobuta et al 25 reported good clinical and radiological results for pullout wiring in 28 patients with Minami grade I or II lesions. Kuwahata and Inoue 17 described the short-term results of 7 patients with COCD lesions treated with Herbert screw fixation of iliac cancellous bone grafts. They noted that all patients could return to their previous sporting activities with an 18° average increase in elbow range of motion. However, the metal hardware damaged the cartilage surfaces on both the embedded and facing sides and needed removal. Recently, biodegradable pins or screws made from poly-lactic acid or hydroxyapatite/poly-lactic acid have been used to arthroscopically fix osteochondral fragments.31,34 Although BPG cannot secure the lesion to the floor as strongly as these fragment fixation techniques, it may serve as an adequate physiological scaffold that is integrated gradually into the grafted site, with few, if any, complications.
There are several limitations to this retrospective study. First, the sample size was too small to obtain reliable statistical differences. Second, the minimum follow-up period was only 2 years and insufficient to evaluate for radiological osteoarthritic changes. Third, we could not perform arthroscopic reassessment of the repaired sites and were unable to obtain histological proof of hyaline cartilage preservation. Last, we did not include any control patients with same-stage COCD in which marrow stimulation via drilling or microfracture, fragment fixation by wiring, or mosaicplasty was performed.
Conclusion
This investigation showed that BPG enabled 91% of COCD patients with ICRS OCD I or II to return to preoperative baseball ability levels within 12 months. Based on MRI findings, integration of the grafted site continued until at least 24 months postoperatively. This study suggests that an ICRS OCD I or II lesion with central positioning and/or occupying <75% of the size of the capitellum in the coronal plane is a good indication for the BPG technique.
Footnotes
Acknowledgements
The authors thank for Mr Trevor Ralph for his English editorial assistance.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.