
Abstract
Background:
The physical risk factors for a medial elbow injury in junior baseball players are unknown.
Purpose:
To identify the risk factors for an initial medial elbow injury in junior baseball players.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Junior baseball players (aged 6-12 years) without a history of elbow pain underwent a clinical assessment, ultrasonography, and physical function measurements before the baseball season started. Bilateral passive range of motion (ROM) of elbow extension and flexion, external rotation (ER) and internal rotation (IR) of the shoulder, and ER and IR of the hip were measured. IR and ER strength of the shoulder and scapular muscles were measured on both sides. The thoracic kyphosis angle was measured with participants in a relaxed standing position. Before these examinations, every participant completed a questionnaire regarding his or her age, sex, total years of baseball played, position in baseball, number of balls thrown, and episodes of pain during throwing. After the initial test session, each participant was followed up for 12 months to assess for the occurrence of a new injury. Multiple regression analysis was used to identify the risk factors for a medial elbow injury.
Results:
Seventy-eight players (22.1%) sustained a medial elbow injury. Age ≥9 years (odds ratio [OR], 2.708; 95% CI, 1.224-5.990), pitcher position (OR, 2.620; 95% CI, 1.389-4.941), >100 throws per day (OR, 1.936; 95% CI, 1.072-3.497), thoracic kyphosis angle ≥30° (OR, 2.501; 95% CI, 1.381-4.531), and elbow extension deficit ≥5° (OR, 1.973; 95% CI, 1.022-3.809) were significantly associated with a medial elbow injury.
Conclusion:
The incidence of an initial medial elbow injury was 22.1%. Age, number of throws per day, thoracic kyphosis angle, and elbow extension deficit are newly discovered risk factors related to physical function. Improvement of the posture and early detection of a silent elbow extension deficit may prevent a medial elbow injury.
Although participation in sports has been linked to mental and physical benefits, the potential risk of injuries should not be ignored. Baseball is a widely played sport in Japan, with an estimated 8 million active baseball players. 5 Roughly a quarter of pitchers aged 9 to 12 years have reported elbow pain while pitching. 14 Andrews and Fleisig 1 have suggested that this age range may be the ideal time to intervene to prevent elbow pain because a significant number of throwing injuries occur during this period and future disabilities in throwing caused by pain or limited motion occur as a result of pitching at these ages. There are numerous risk factors hypothesized to predispose baseball throwers to elbow pain, and these factors can be classified as nonmodifiable or modifiable. 27 Nonmodifiable risk factors include age, number of years pitching, and height.14,23 Modifiable risk factors include pitching mechanics, amount of pitching (ie, the number and frequency), and physical function (ie, the joint range of motion [ROM], muscle flexibility, and muscle strength). ∥ As physical function directly affects the joint mechanical profile and is amenable to targeted intervention, it should be emphasized in prevention programs.
Many prospective studies have previously investigated the following physical risk factors in adolescent and professional players: altered shoulder ROM, increased posterior shoulder tightness, decreased grip strength, rotator cuff weakness, scapular dysfunction, lower extremity muscle tightness, and deficits in single-leg standing balance.4,10,19,26,29 With the exception of the Harada et al 10 study, no studies have examined the physical factors for elbow pain in junior baseball players (aged 6-12 years). In addition, Harada et al included players who already had prior elbow pain at the beginning of the study.
Matsuura et al 16 found that nearly 60% of players aged 7-12 years with initial elbow pain had already exhibited radiographic abnormalities (eg, medial epicondylar fragmentation and osteochondritis dissecans of the capitellum), and they suggested that it was necessary to examine the risk factors for elbow injuries without prior elbow pain. Furthermore, Lyman et al 15 reported that elbow pain occurred in various locations, including the medial, lateral, internal, and posterior elbow. Because each location of pain in the thrower’s elbow may have different predisposing factors, it is necessary to investigate the risk factors for each of them. Therefore, the purpose of this study was to identify the risk factors for an initial medial elbow injury in junior Japanese baseball players.
Matsuura et al 16 found that 30.5% of junior baseball players reported episodes of initial elbow pain over a year. Additionally, Lyman et al 15 reported that more than 68% of elbow pain occurred on the medial side of the elbow. Thus, we hypothesized that the incidence of a medial elbow injury would occur in more than 20% of participants. Additionally, we hypothesized that participants with risk factors would have double the risk of a medial elbow injury compared with those without risk factors, according to the Harada et al 10 study.
Methods
A prospective cohort design with a 12-month follow-up was used to identify the risk factors for an initial medial elbow injury in junior baseball players. The present study was approved by an institutional review board, and informed consent was obtained from all participants and their guardians before enrollment. The Strengthening the Reporting of Observational Studies in Epidemiology statement 31 was used as a guide when reporting on data.
Participants
We expected that the incidence of participants with risk factors would be double that of those without risk factors (30% vs 15%, respectively). A minimum sample size of 133 in each group would have a power of 80% to detect the difference of our hypothesis (2-tailed α of .05). A dropout rate of 10% was expected, and 30% of participants would have a history of elbow or shoulder pain. The planned accrual target was 422 participants.
We recruited junior baseball teams from 2 regional leagues in Yokohama from December 2012 to November 2013. Inclusion criteria required participants to be between the ages of 6 and 12 years. Exclusion criteria were those who could not participate on a baseball team for 1 year from the initial examination or those with an injury or illness that made it impossible to participate in baseball. Before the examination, every participant completed a detailed questionnaire regarding his or her personal data (age, sex, total years of baseball played, height, and weight), position in baseball (pitcher, catcher, or neither), typical number of throws per day, practice days per week, and whether he or she had ever had any episodes of elbow and/or shoulder pain while throwing the baseball. The typical number of throws per day was selected from the following: <50, 51-80, 81-100, and >100 throws. These categories were stratified according to those reported in previous studies.10,23
All participants underwent a clinical assessment, ultrasonography, and physical function measurements (ROM, strength, and posture) before the baseball season started. Each examination was performed by the same examiner.
Clinical Assessment and Ultrasonography of the Elbow
A physical therapist (J.S.), who had more than 5 years of experience in the rehabilitation of throwing injuries of junior baseball players, performed the clinical assessment of the elbow, which consisted of assessing medial elbow pain with flexion, extension, and valgus stress (30° of elbow flexion and a moving valgus stress test). To perform the moving valgus stress test, the examiner applied and maintained a constant moderate valgus torque to the fully flexed elbow and then quickly extended the elbow. 21 A positive sign was the presence of pain during the clinical assessment. A medical doctor (A.A.), with more than 10 years of experience in diagnosing throwing elbow injuries using an ultrasound device, evaluated the medial aspect of the elbow using a 3-dimensional/4-dimensional ultrasound device (Voluson I; GE Healthcare). Morphological conditions of both the medial epicondyles were assessed using a short-axis and long-axis ultrasound approach. Figure 1A shows a normal finding. We assessed whether the shape of the bottom edge of the medial epicondyle was irregular (Figure 1B), and we assessed whether the bone fragment existed completely or partially (Figure 1, C and D). A positive finding was defined as a case in which the aforementioned morphological conditions were only found on the throwing side.
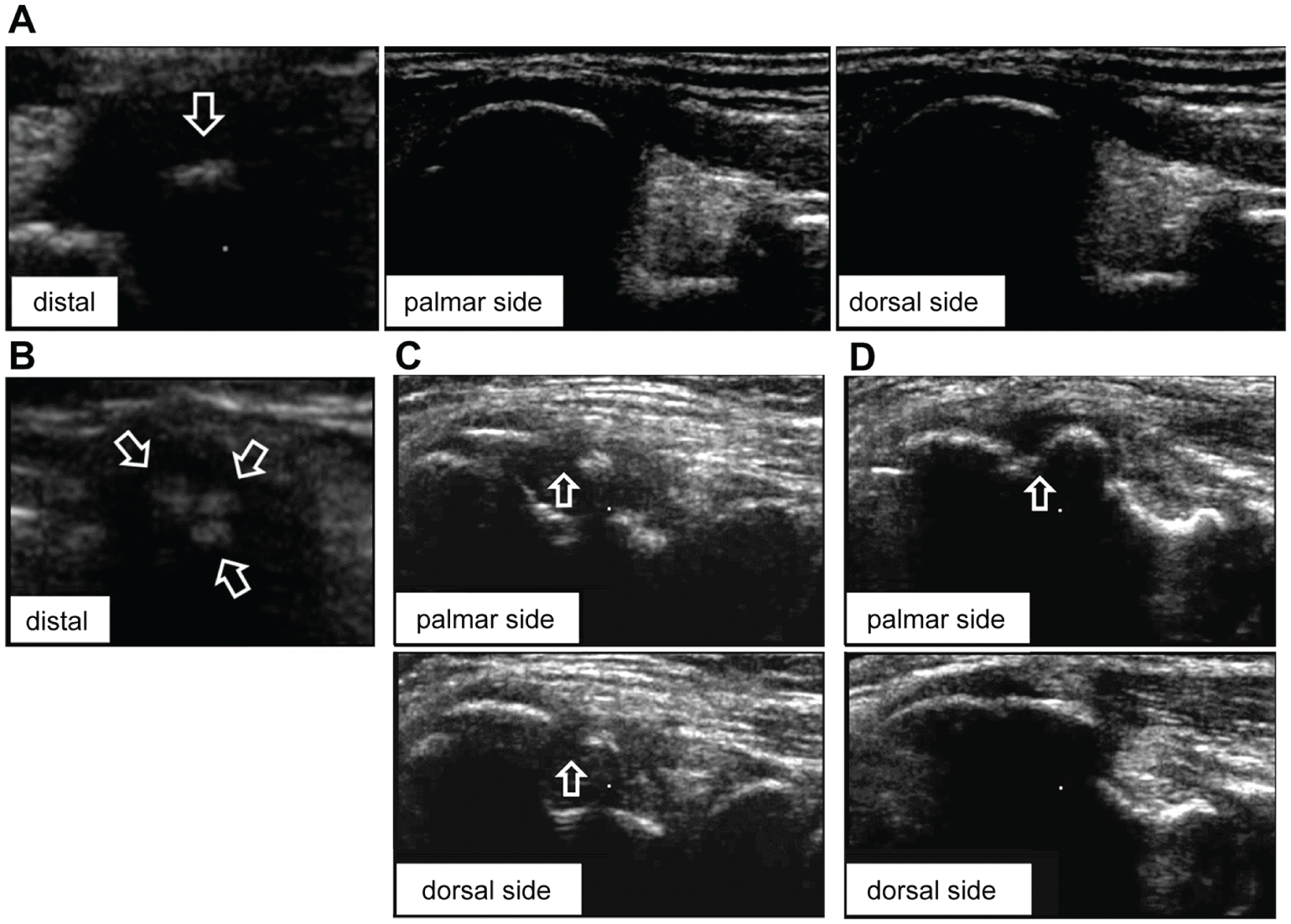
Ultrasonographic morphological assessment of the medial epicondyle. (A) Normal: the shape of the bottom edge of the medial epicondyle is clear (arrow; short axis), and the bone outline has continuity from the palmar side to the dorsal side (long axis). (B) Irregular: the shape of the bottom is irregular (arrows; short axis). (C) Complete fragment: the bone outline has full discontinuity (arrows) from the palmar side to the dorsal side (long axis). (D) Partial fragment: the bone outline has partial discontinuity (arrow; long axis).
Physical Function Measurements
The same physical therapist (J.S.) measured bilateral passive ROM of elbow extension and flexion, external rotation (ER) and internal rotation (IR) of the shoulder, and ER and IR of the hip using a standard goniometer. ROM of the shoulder was measured in the supine position, with the shoulder at 90° of abduction, the elbow at 90° of flexion, and the forearm at neutral rotation. The scapula was stabilized while measuring shoulder ROM. ROM of the hip was measured in the supine position, with the hip at 90° of flexion. Shoulder horizontal adduction (HA) ROM, as reported by Laudner et al, 11 was measured in the supine position, with the lateral border of the scapula stabilized by providing a posteriorly directed force via the examiner’s hand to limit scapular protraction, rotation, and abduction. The upper extremity was passively and horizontally adducted across the body with the arm starting at 90° of abduction in neutral rotation. A digital inclinometer (DWL-80Pro; Digi-Pas) was aligned with the humerus, and the angle relative to a line perpendicular to the ground was recorded. These ROM measurements were taken once.
Bilateral IR and ER strength of the shoulder and scapular muscles were also measured by a physical therapist (E.N.), with more than 5 years of experience in the rehabilitation of throwing injuries in junior baseball players, using a handheld dynamometer (MicroFET; Hoggan Health Industries Inc). This measurement technique has been shown to be valid and reliable for detecting weakness in the shoulder.17,28,30 IR strength was measured in the supine position, with the shoulder in 90° of abduction and the elbow in 90° of flexion. The arm was placed in neutral rotation, and the participant maximally resisted against the dynamometer placed on the volar aspect of the wrist. We tested ER strength in the prone position in a similar manner, with the dynamometer placed on the dorsal aspect of the wrist. The lower trapezius muscle was examined in the prone position, with the arm in 150° of scaption with the thumb up. The dynamometer was placed on the posterolateral corner of the acromion, and the participant maximally resisted a protraction-directed force. The serratus anterior muscle was examined in the supine position, with the shoulder at 90° of flexion and the elbow at 90° of flexion. Resistance was applied to the ulna at the olecranon process along the long axis of the humerus. These measurements were taken twice and then averaged and analyzed.
For the posture measurement, the thoracic kyphosis angle was measured in a relaxed standing position by a physical therapist (J.S.). An inclinometer (Bubble Inclinometer; Baseline Inc) was placed over the spinous processes of the first and second thoracic spines and over the twelfth thoracic and first lumbar spines; each angle was recorded. These measurements were taken once. The thoracic kyphosis angle was calculated by the summation of these angles. 22 The intratester and intertester reliability of this measurement has been established (intraclass correlation coefficient [single], 0.95; 95% CI, 0.91-0.97).12,13
To examine potential risk factors, the following variables were calculated: ROM deficits (nondominant − dominant) in extension and flexion of the elbow; ROM deficits (nondominant − dominant) in IR and HA of the shoulder; increased ROM (dominant − nondominant) in ER of the shoulder; passive shoulder total rotation (ER + IR) of the dominant and nondominant arms; and strength ratio (dominant/nondominant) of IR and ER of the shoulder, lower trapezius, and serratus anterior muscle.
Injury Surveillance
After the examination, researchers visited each baseball team every 3 months and performed a clinical assessment and ultrasonography of the elbow using the same methods as previously described. At the initial examination, participants were provided with baseball diaries to record elbow or shoulder pain daily. At each visit, participants reported any elbow or shoulder pain since the last date of contact in their baseball diaries. In reference to the study by Olsen et al, 23 we recorded elbow and shoulder pain if they had any of the following pain: (1) shoulder or elbow pain lasting >2 weeks, (2) shoulder or elbow pain that caused them to not play in a game or practice, or (3) recurrent elbow or shoulder pain. A medial elbow injury was defined as medial elbow pain during throwing with either an abnormal sonography finding or the presence of pain during the clinical assessment of the elbow. Players with a medial elbow injury were categorized into the medial elbow injury group, and players with shoulder pain and other elbow pain were excluded from the noninjured group. Athlete-exposure (AE) was defined as 1 athlete participating in 1 practice or game during which a player was at risk of sustaining an injury. The times of their practices or games were counted on their baseball diaries, and each elbow and shoulder injury rate was calculated.
Statistical Analysis
Means ± SDs were calculated for all variables. Univariate analyses were performed using the chi-square test for categorical variables to investigate risk factors for a medial elbow injury. For continuous data that were normally distributed (Kolmogorov-Smirnov test), an unpaired t test was used to compare the medial elbow injury group and noninjured group. Continuous data that failed the normality test were assessed with the Mann-Whitney U test to compare these 2 groups.
Multivariate logistic regression, using variables with P values <.20 from the 2-group comparisons, was then used to identify the most predictive variables of a medial elbow injury. A P value of .20 was used so that potentially important predictors would not be excluded from this comprehensive data set. Independent variables were age, sex, total years of baseball played, body mass index, number of throws per day, practice days per week, position in baseball, and physical functions. Only variables that were significant at P < .05 remained in the model for each set. Models were developed with forward stepwise (conditional) regression. Each continuous variable identified by the multivariate logistic regression model was then divided into a high group and a low group. The cutoff points for these variables, except for the thoracic kyphosis angle, were established based on previous studies.4,9,10,16,26 There was no reference for the thoracic kyphosis angle, so the initial point of its angle was established based on the average value. Finally, all categorized variables were entered into a final multivariate stepwise logistic regression analysis to determine a best predictive final model. Odds ratios (ORs) and profile likelihood 95% CIs from the last final model were reported. The likelihood ratio test was also performed, and differences between the −2 logarithmic likelihood of the submodel and the final model (deviance) were calculated to compare the effect of each predictor variable in this model. All data were analyzed using PASW Statistics 18 (IBM Japan).
Results
The target population consisted of 33 eligible junior baseball teams that we approached for recruitment; 593 players from 29 teams agreed to participate. Of these, 176 players had previous elbow or shoulder pain, and 64 players dropped out. Excluding these players, 353 completed the follow-up and were analyzed (Figure 2). At the initial examination, the morphological condition of the medial epicondyle was as follows: 269 normal, 51 irregular, 26 partial fragments, 3 complete fragments, 3 combined irregular and partial fragments, and 1 combined irregular and complete fragment.
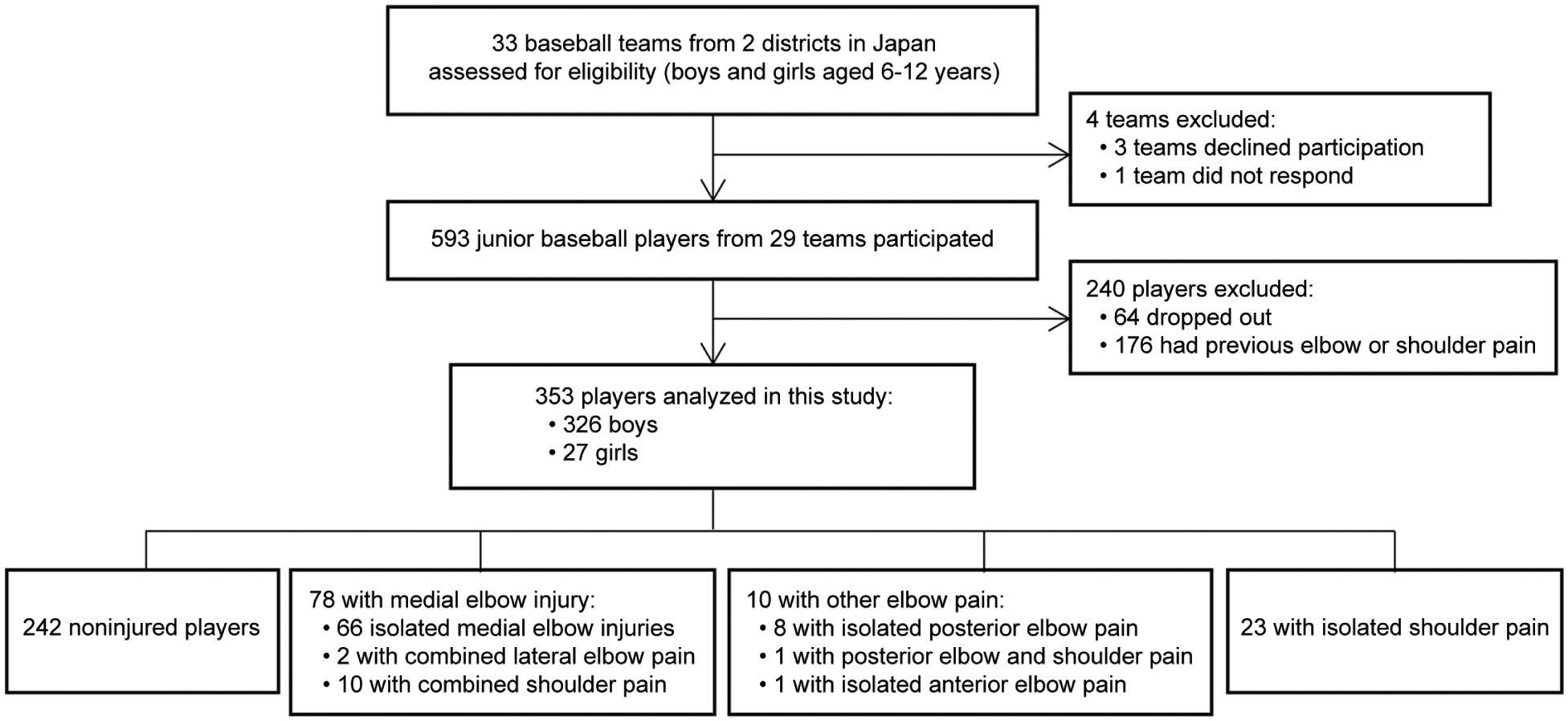
Flow diagram of exclusion criteria and the outcomes.
Eighty-eight players (24.9%) reported elbow pain in the throwing arm, and 34 (9.6%) reported shoulder pain during the 12-month follow-up period. Of the 88 players who reported elbow pain, 11 also reported shoulder pain. Furthermore, of the 88 players who reported elbow pain, 78 (22.1%) sustained a medial elbow injury. When a medial elbow injury occurred, the morphological condition of the medial epicondyle of these players was as follows: 3 normal, 26 irregular, 26 partial fragments, 14 complete fragments, 7 combined irregular and partial fragments, and 2 combined irregular and complete fragments.
Changes in their morphological condition from the initial examination are described as follows. All 3 participants who had normal ultrasonography findings after a medial elbow injury had normal findings at the initial examination. Of 26 participants who had irregular findings, 19 had normal findings, and 7 had irregular findings at the initial examination. Of 26 participants who had a partial fragment, 6 had normal findings, 13 had irregular findings, and 7 had a partial fragment at the initial examination. Of 14 participants who had a complete fragment, 3 had normal findings, 4 had irregular findings, 5 had a partial fragment, and 1 had a combined irregular and partial fragment at the initial examination. Of 7 participants who had a combined irregular and partial fragment, 2 had normal findings, 3 had irregular findings, and 2 had a partial fragment at the initial examination. Two participants who had a combined irregular and complete fragment had normal findings at the initial examination.
The overall incidence of elbow pain was 1.5 per 1000 AEs, and the rate of medial elbow injuries was 1.4 per 1000 AEs. The overall incidence of shoulder pain was 0.6 per 1000 AEs. In pitchers, the incidence of elbow pain was 2.5 per 1000 AEs, and the rate of medial elbow injuries was 2.2 per 1000 AEs. In addition, the incidence of shoulder pain was 0.5 per 1000 AEs in pitchers. The incidence of medial elbow injuries was significantly higher for the pitcher position than for other positions (P < .01) (Table 1).
Univariate Analysis for Categorical Variables
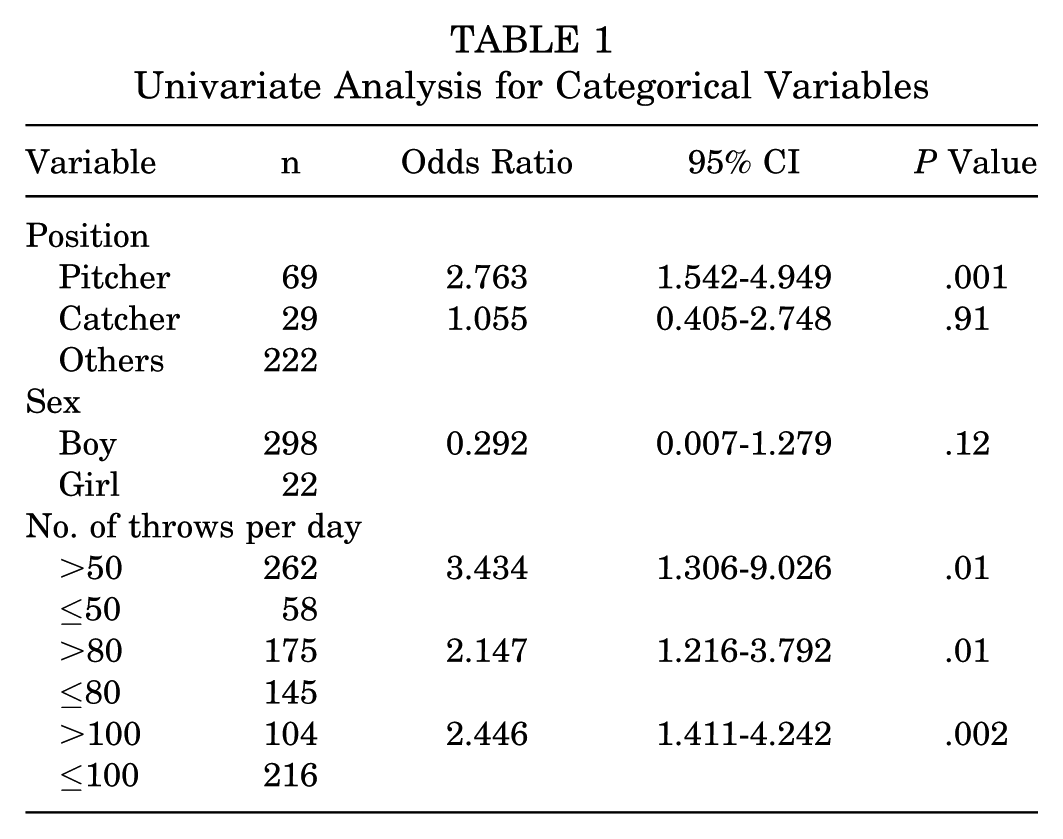
Table 2 presents the mean values of each continuous variable for players who sustained a medial elbow injury and the noninjured players. Univariate analysis showed that a medial elbow injury was significantly associated with older age, more experience, pitcher position, larger number of throws per day, more practice days per week, smaller passive shoulder total rotation of the dominant side, smaller hip IR ROM of the nondominant side, and larger thoracic kyphosis angle (Tables 1 and 2).
Univariate Analysis for Continuous Variables a
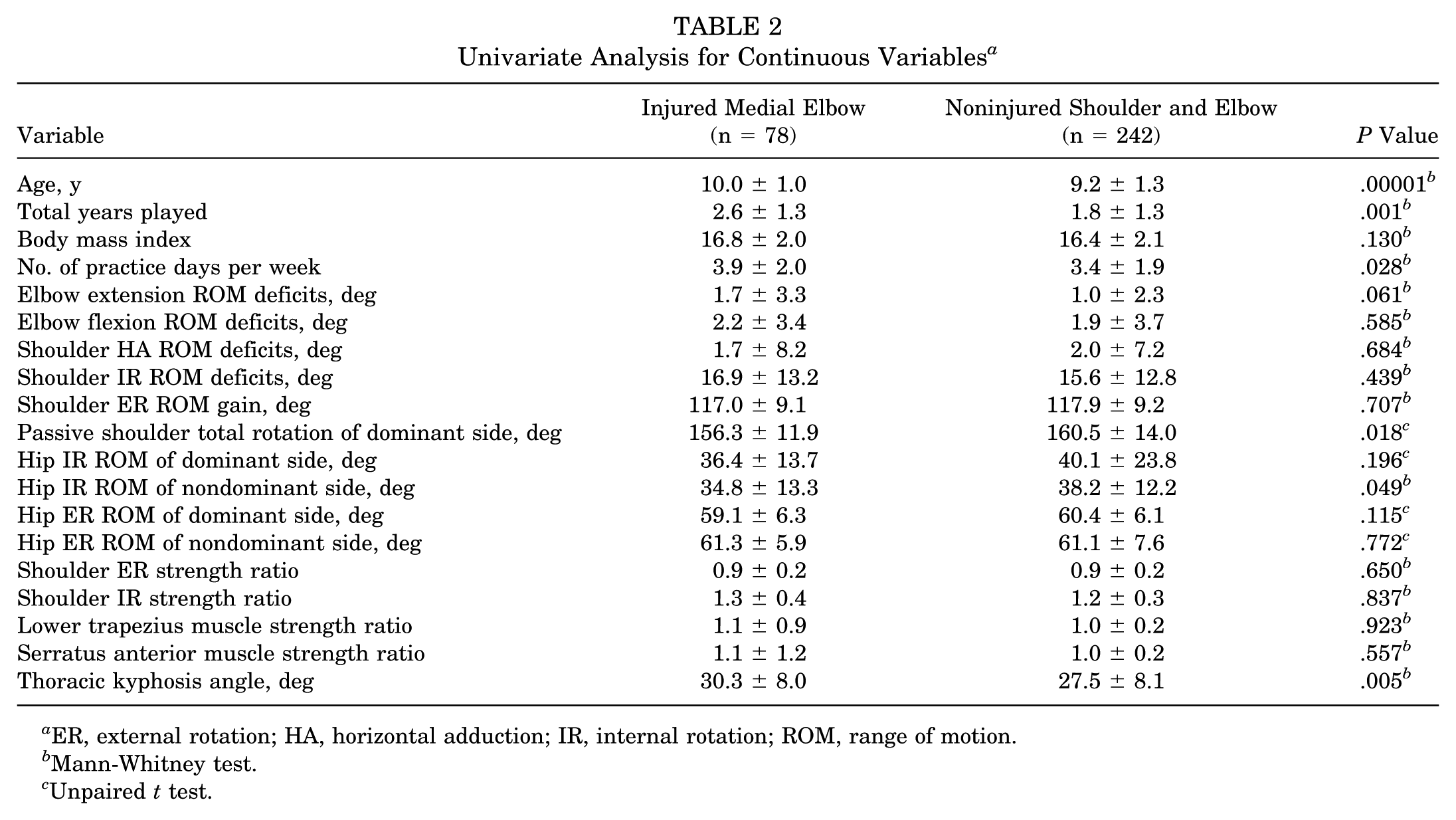
ER, external rotation; HA, horizontal adduction; IR, internal rotation; ROM, range of motion.
Mann-Whitney test.
Unpaired t test.
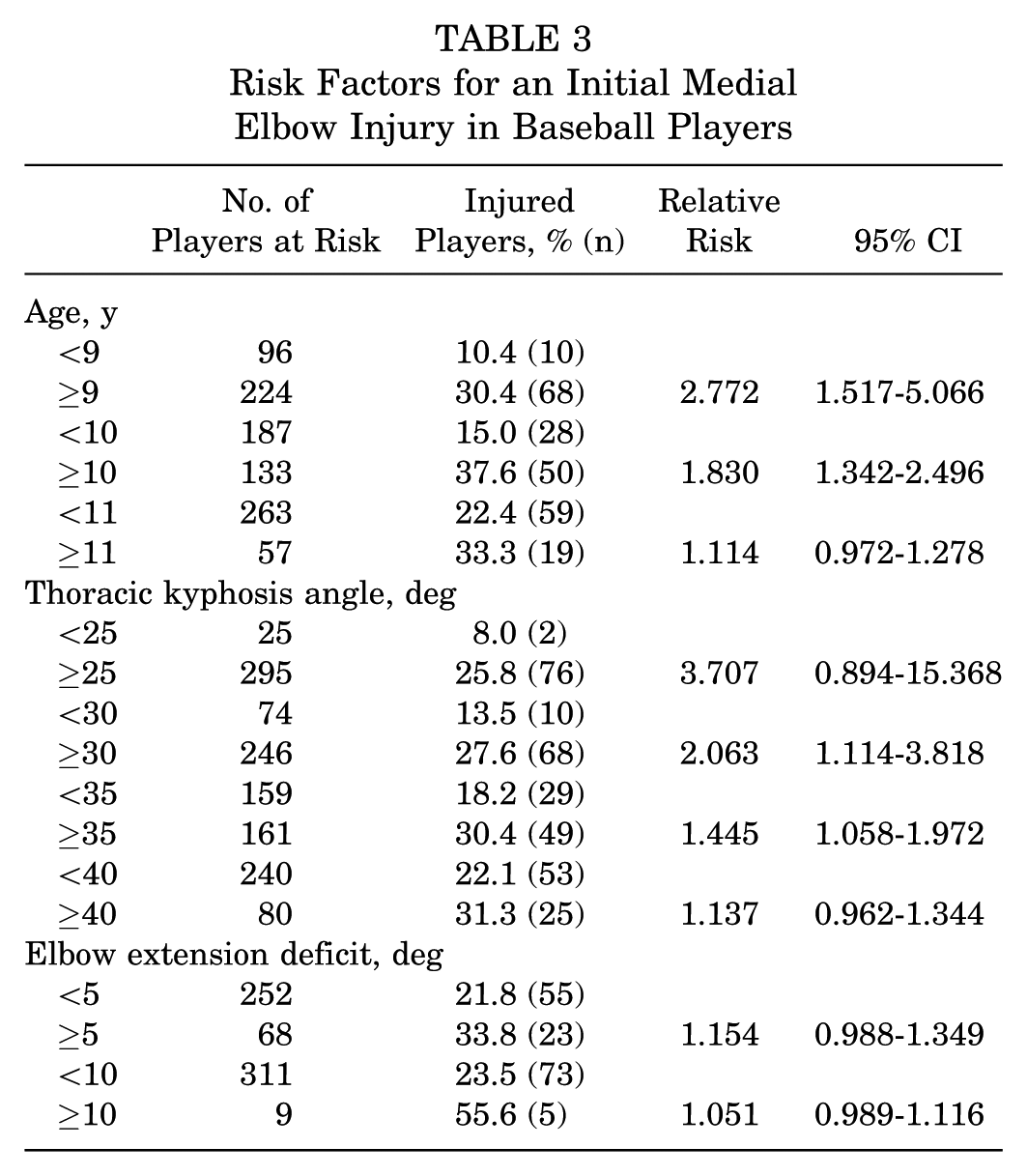
Multivariate logistic regression analysis identified 2 categorical variables (pitcher position and >100 throws per day) and 3 continuous variables (age, thoracic kyphosis angle, and passive elbow ROM deficit angle) as the most significant risk factors. The relative risk (RR) and corresponding 95% CIs of these continuous variables are shown in Table 3. The cutoff points for age was ≥9 years (RR, 2.772; 95% CI, 1.517-5.066), the thoracic kyphosis angle was ≥30° (RR, 2.063; 95% CI, 1.114-3.818), and the elbow extension deficit was ≥5° (RR, 1.154; 95% CI, 0.988-1.349). The final model of multivariate logistic regression identified 5 categorical variables, including age ≥9 years (OR, 2.708; 95% CI, 1.224-5.990), pitcher position (OR, 2.620; 95% CI, 1.389-4.941), >100 throws per day (OR, 1.936; 95% CI, 1.072-3.497), thoracic kyphosis angle ≥30° (OR, 2.501; 95% CI, 1.381-4.531), and elbow extension deficit ≥5° (OR, 1.973; 95% CI, 1.022-3.809), as predictive factors of a future medial elbow injury (Table 4). The deviance of each predictive factor was as follows (in descending order of values): 9.551 for thoracic kyphosis angle ≥30°, 8.740 for pitcher position, 6.864 for age ≥9 years, 4.768 for >100 throws per day, and 4.018 for elbow extension deficit ≥5°.
Risk Factors for an Initial Medial Elbow Injury in Baseball Players
Multivariate Logistic Regression Analysis of Factors Associated With a Medial Elbow Injury a
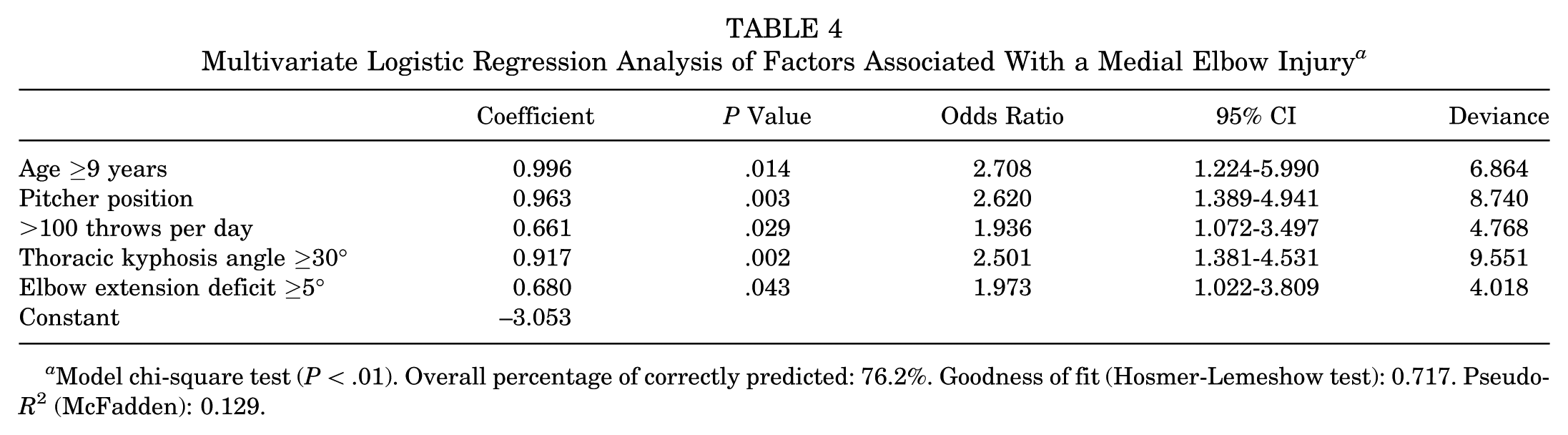
Model chi-square test (P < .01). Overall percentage of correctly predicted: 76.2%. Goodness of fit (Hosmer-Lemeshow test): 0.717. Pseudo-R2 (McFadden): 0.129.
Discussion
Injury Incidence
In this study, the shoulder pain rate was 0.6 per 1000 AEs, and the elbow pain rate was 1.5 per 1000 AEs in junior baseball players. Shanley et al 26 reported that the shoulder pain rate was 1.5 per 1000 AEs and that the elbow pain rate was 1.0 per 1000 AEs in high school baseball players (aged 13-18 years). This suggests that junior baseball players have a higher risk of elbow injuries compared with shoulder injuries, which is unique from older age groups.
In our study, the incidence of an initial medial elbow injury was 22.1% during the 12-month follow-up period. Several prospective surveys on a throwing elbow injury have been performed among youth baseball players,10,15,16 but their incidences were different. Lyman et al 15 showed that medial elbow pain was reported in 17.5% of pitchers during the spring season. In our study, 40.6% of pitchers (28/69) had an injured medial elbow over 1 year. The difference in the injury incidence may depend on the follow-up period. Matsuura et al 16 found that 30.5% of participants (aged 7-11 years) reported episodes of initial elbow pain over 1 year. We found that the incidence of elbow pain was 24.9% among participants (aged 6-12 years). The follow-up period and age were almost the same, but the survey approach and the criteria of pain were different. In the previous study, participants were asked whether they had pain by using questionnaires. In contrast, we directly asked whether participants had pain when throwing, and we recorded elbow pain that lasted >2 weeks as severe pain or recurrent pain. Harada et al 10 defined an elbow injury as ultrasonographic abnormalities of the elbow (eg, medial epicondylar fragmentation and osteochondritis dissecans of the capitellum) with or without pain, which was reported in 20.4% of participants. In most previous studies, the injury criterion was whether the players reported pain, and the site, duration, and severity of pain were not specifically assessed. We contacted each team every 3 months and performed a clinical assessment and ultrasonography of the elbow in all players. We were able to investigate the injury incidence precisely by administering a questionnaire and performing direct examinations.
According to Harada et al, 10 almost 10% of patients without elbow pain had signs of fragmentation. In our study, almost the same rate of participants (33/353) already had partial or complete fragmentation at the initial examination. In addition, 51 participants had irregular findings at the initial examination. These findings could not be found on the contralateral side, and over half of the participants (27/51) sustained a medial elbow injury later. Thus, the irregular finding may be a sign of an at-risk elbow.
Risk Factors for a Medial Elbow Injury
In the present study, the number of participants was sufficient to analyze the data. Five variables were identified as the most significant risk factors in the multivariate logistic regression model with a goodness of fit of 0.717 (P < .05). This means that the final model of this study fit the data. The McFadden R2 was not high, but the model had significant explanatory power.
In agreement with previous studies,10,16 we found that players’ age and position in baseball (ie, pitchers) were risk factors for a medial elbow injury. Matsuura et al 16 found that 12-year-old baseball players had higher rates of elbow pain compared with those 10 years or younger. They suggested that there is a relationship for the timing of secondary ossification centers of the elbow. These centers are vulnerable points in a young elbow, and those junior baseball players who are older may be more prone to an elbow injury. We found that players aged ≥9 years had a 2.7 times’ greater risk of a medial elbow injury than those aged <9 years within 1 year. It is suggested that medial elbow injuries should be prevented in players aged ≥9 years. According to the results of the likelihood ratio test, the pitcher position was estimated to have the second highest effect on medial elbow injuries in this study. Therefore, it is necessary to monitor the pitchers’ condition to prevent throwing injuries.
Some studies have found that the number of pitches was a risk factor for elbow pain in youth baseball pitchers, and they suggested that limitations on pitches thrown in a game and during the season could reduce the risk of injuries.7,14 We did not restrict participants to the pitcher position, but we included the position, number of throws, and practice days per week as independent variables in the multivariate logistic regression analysis. As a result, >100 throws per day was associated with a medial elbow injury. It was suggested that limiting the number of throws might be effective for preventing a medial elbow injury for any position in baseball. However, except for the pitcher position, it may be difficult to limit the number of accurate throws in other positions. Thus, we focused on physical function, which is one of the modifiable factors.
Multivariate logistic regression showed that a medial elbow injury was also associated with physical function, that is, the thoracic kyphosis angle and side-to-side difference of elbow extension ROM. To our knowledge, no study has investigated whether the thoracic kyphosis angle is a risk factor for an elbow injury. We found a relationship between a medial elbow injury and the thoracic kyphosis angle: a 2.5 times’ higher risk for ≥30°. In addition, thoracic kyphosis angle ≥30° had the highest effect on a medial elbow injury among all the predictor variables; the deviance was 9.551. During pitching, 67 N·m of shoulder IR torque and 64 N·m of elbow varus torque at most are generated. 8 Anz et al 2 showed that an elbow injury was associated with a higher elbow varus torque only at the event of maximum shoulder rotation and suggested that the late cocking phase of the pitching motion is indeed the critical point in terms of the elbow injury risk. Miyashita et al 18 found that glenohumeral joint movement and scapular and thoracic movements made major contributions to the maximum ER of the shoulder complex. Finley and Lee 6 reported that increased thoracic kyphosis significantly decreases the posterior tip and lateral rotation of the scapula, indicating that an increase in the kyphosis angle may decrease the contribution of scapular movement and increase stress on the elbow at maximum shoulder rotation during throwing. This finding also suggests that a future throwing injury prevention program should focus especially on improving the posture of baseball players.
In the current study, the side-to-side difference of elbow extension ROM was also associated with a medial elbow injury. In adolescent pitchers (aged 8-13 years), the overall elbow flexion/extension ROM during throwing is about 80°, and the elbow does not fully extend. 20 Thus, it is difficult to consider that an elbow extension deficit directly changes mechanical stress on the elbow. We believe that the silent elbow extension deficit (SEED) is an antecedent sign of an initial medial elbow injury. We compared the ratio of the ultrasound morphological abnormality of the medial epicondyle between participants with a SEED and healthy participants, and the abnormality was found in 39.7% (27/68) of participants with a SEED and 26.6% (67/252) of healthy participants. If players or their guardians can determine the SEED before throwing, they can identify the elbow problem before pain occurs. Performing an assessment of one’s own elbow with a guardian is important for the early detection and early response to an elbow injury, and it may decrease severe injury occurrences in this age group. This knowledge may be useful to baseball players.
Limitations
Our study has several limitations. First, the number of throws and history of elbow or shoulder pain were based on retrospective recall from the participants by using a questionnaire before the initial examination; thus, this may not have produced accurate and complete data. Second, other potential risk factors were not investigated, such as the strength of the lower extremity and pitching mechanics. Previous studies have yet to show that poor pitching mechanics increases the risk of elbow pain in adolescent baseball players.3,14,24 Davis et al 3 observed that pitching with an open shoulder at stride foot contact assessed by video cameras was associated with greater elbow varus loading. Oyama et al 24 evaluated the effects of excessive contralateral trunk tilt, a common issue identifiable by video observation, on pitching biomechanics and performance. The study showed that pitchers who exhibited an increased contralateral trunk tilt had statistically significant increases in both ball velocity and elbow varus moment. These findings suggested the potential for identifying pitchers who experience greater joint loading by screening the pitching technique using video camera analysis. A prospective study on pitching mechanics with a large sample size and accurate analysis is needed. Third, the sample size was not enough to prove our hypothesis; according to the results of the univariate analysis, 355 participants were needed. However, in the multivariate analysis, the sample size was sufficient to prove our hypothesis (78 participants with a medial elbow injury > explanatory variable × 10). 25 This seemed to suggest that the risk factors were not found separately but jointly. Finally, the follow-up period was only 12 months. Players who did not have an injury in 1 year may have sustained a medial elbow injury after this investigation. It is necessary to follow a cohort of baseball players from their first year of participation through the end of their growth to understand the throwing injury in junior baseball players whose skeleton is immature.
Conclusion
It is expected that >20% of junior baseball players will have a medial elbow injury each year. Our study showed that age was a nonmodifiable risk factor for a medial elbow injury. The number of throws, thoracic kyphosis angle, and elbow extension deficit were modifiable risk factors for a medial elbow injury. Based on our results, it may be possible to reduce the risk of medial elbow injuries by limiting players’ throws to <100 per day and improving their posture. Additionally, performing a self-assessment of one’s own elbow may help screen for an antecedent sign of an initial medial elbow injury.
Footnotes
Acknowledgements
All data were collected in junior baseball association fields of Kohoku and Tsurumi at Yokohama, Japan. The authors acknowledge the players, guardians, and coaches.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.