
Abstract
Background:
Numerous epidemiological studies have emphasized the burden of lateral ankle sprains in youth soccer players. However, no prospective study has identified intrinsic physical and modifiable risk factors for these injuries in this particular population. Although injury prevention programs in soccer incorporate proximal hip and core stability exercises, it is striking that the relationship between impaired proximal hip function and ankle sprains has not yet been prospectively investigated in youth soccer players.
Hypothesis:
This prospective study aimed to examine whether hip muscle strength is a risk factor for sustaining a lateral ankle sprain in youth soccer players. We hypothesized that decreased hip muscle strength would predispose youth soccer players to an increased risk of lateral ankle sprains.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This study included a total of 133 male youth soccer players (age divisions U11-U17) for analysis. At the beginning of the season, anthropometric characteristics were collected and hip muscle strength was assessed using a handheld dynamometer. Injury registration was performed by the team medical staff during 3 consecutive seasons. A principal-component, multivariate Cox regression analysis was performed to identify potential risk factors for sustaining a lateral ankle sprain.
Results:
Twelve participants (18% of all reported injuries) sustained a lateral ankle sprain (0.36 per 1000 athletic-exposure hours). After adjustment for body size dependencies and other hip muscle forces, an increase in hip muscle extension force was associated with a significant decrease in the hazard of the injury (hazard ratio, 0.3; 95% confidence interval, 0.1-0.9; P = .028). No other study variable could be identified as a risk factor for lateral ankle sprains.
Conclusion:
Reduced hip extension muscle strength is an independent risk factor for lateral ankle sprains in male youth soccer players. Other hip muscle strength outcomes were not identified as risk factors. Replication in larger samples with more injured cases is warranted to further ascertain the importance of this risk factor.
Soccer is currently the most popular sport played worldwide and its popularity continues to increase, especially among youth players. 13 Although playing sports at a young age is advocated because of its associated health benefits, 11 the high incidence of injury in youth soccer is a growing concern. 32 Compared with various sports disciplines, soccer has one of the highest injury rates among high school sports. 33 A large-scale epidemiological study in Canada showed that soccer injuries account for more than 10% of all sport injuries in youth aged 11 to 18 years. 9 In addition, a recent systematic review indicated that the overall incidence varied between 2 and 7 injuries per 1000 hours of soccer in players aged 13 to 19 years. 12 Ankle sprains occur most frequently, accounting for approximately 20% of all injuries in youth soccer players, 22 and lead to a marked loss of training and competition time. 3 Although ankle sprains are considered “easy to treat” with a good outcome, they may also evolve to chronic ankle instability, possibly resulting in lower activity levels or even a change of sports.1,21 Thus, to reduce the incidence of ankle sprains and their comorbidities in youth soccer players, risk factors should be identified to facilitate classification of players who are at increased risk as well as to inform effective prevention strategies.
In the past decade, a number of prospective studies have established several risk factors for sustaining soccer-related injuries in youth players, including age,15,23 a history of injury,4,10,40 game versus practice conditions,10,25 playing level,10,25 or psychological factors. 41 However, these risk factors were either identified in view of general injury rates or were extrinsic (eg, playing surface 37 ), nonmodifiable (eg, age15,23), or not amendable through physical rehabilitation (eg, psychosocial factors 41 ). Interestingly, however, common prevention programs (eg, the Fédération Internationale de Football Association’s FIFA 11+) implement a variety of exercises designed to improve coordination, reaction time, endurance, and the stability of ankle or knee joints as well as the lumbopelvic-hip complex.20,38 Regarding the latter, previous research has introduced the role of proximal stabilizing musculature in the occurrence of distal injury based on kinetic chain theories. 2 These theories postulate that impaired proximal function increases the likelihood of uncontrolled joint displacements or unsolicited accessory movements throughout the lower kinetic chain, which may contribute to the occurrence of injuries. 50 Hip muscle weakness has been identified as a predictor of lower extremity overuse injuries such as exertional medial tibial pain. 48 Adults sustaining an ankle sprain and subsequently suffering from chronic ankle instability also have impaired proximal hip function compared with ankle sprain copers. 7 Furthermore, Friel et al 14 found decreases in hip abduction strength in individuals with ankle sprains, whereas neuromuscular deficits in the tensor fascia latae and gluteus maximusmuscles were associated with chronic ankle instability.47,49 Although these findings suggest a relationship between impaired proximal hip function and ankle injury, to our knowledge, no prospective study to date has investigated the relationship between intrinsic proximal and modifiable risk factors such as hip muscle strength and the incidence of lateral ankle sprains in youth soccer players.
This prospective study aimed to examine whether hip muscle strength is a risk factor for sustaining a lateral ankle sprain in youth soccer players. We hypothesized that decreased hip muscle strength would predispose youth soccer players to an increased risk of lateral ankle sprains.
Methods
Study Overview
This was a prospective study monitoring youth soccer players over 3 consecutive seasons. Testing procedures involved collecting player demographic, anthropometric, and hip strength data. Although injury registration continued from the start of the study until completion of the third season, testing procedures were only performed at the start of the first season for each of the players.
Participants
A total of 140 male youth players from a first-division soccer team were enrolled in this study. All participants played in the national league of their age category, ranging from 10 to 16 years (number of players by age division: U11, 31; U12, 19; U13, 18; U14, 17; U15, 17; U16, 21; and U17, 17). None of the players were injured at the start of the study and none reported any lower limb musculoskeletal injury in the previous 6 months or a history of lower limb surgery. Goalkeepers were excluded from the current analyses (n = 7). This study was approved by the Ghent University Hospital Ethics Committee and all players and their parents/legal guardians signed informed consent forms. Participant baseline characteristics are presented in Table 1.
Baseline Characteristics for the Entire Sample and for Patients Who Did and Did Not Sustain a Lateral Ankle Sprain a
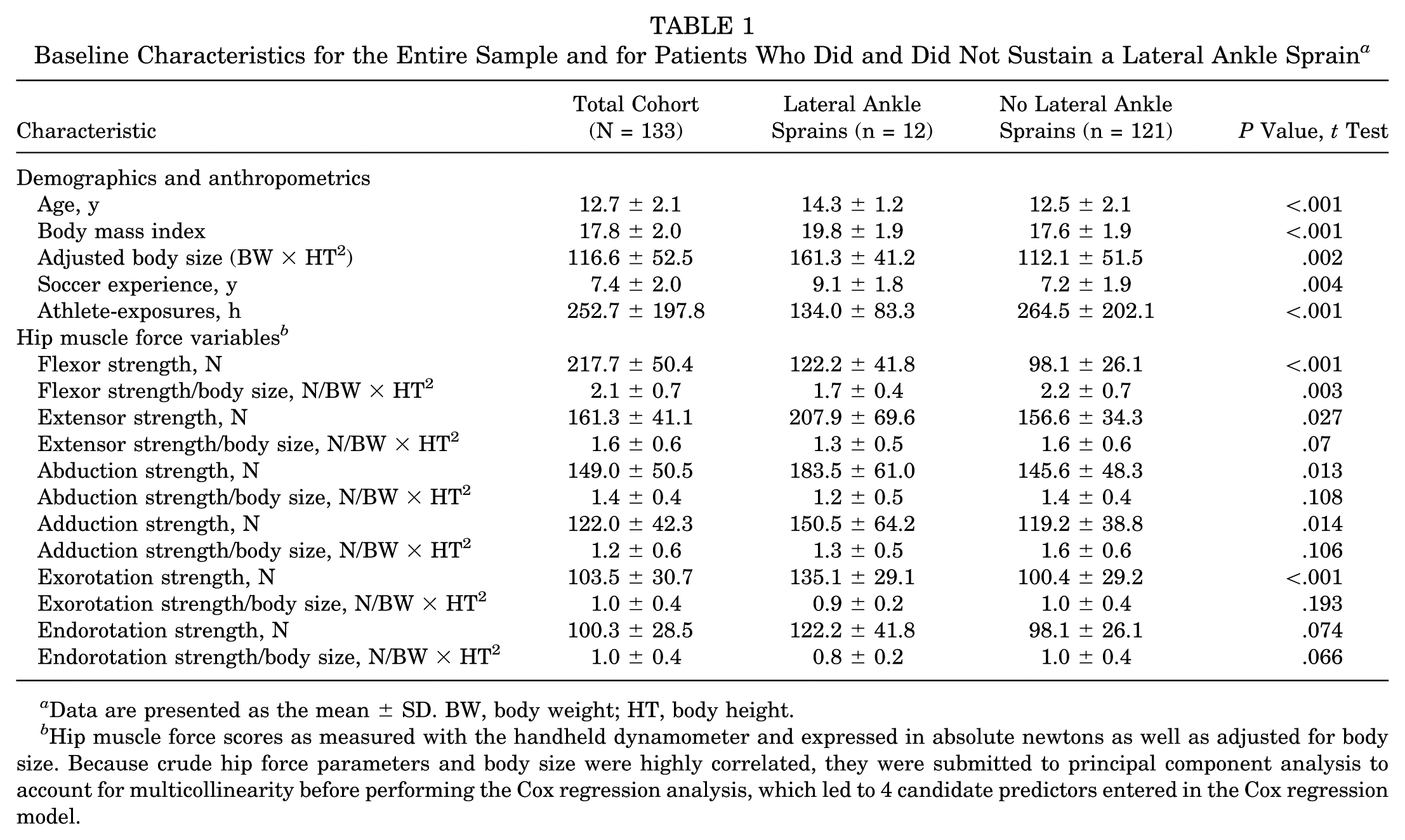
Data are presented as the mean ± SD. BW, body weight; HT, body height.
Hip muscle force scores as measured with the handheld dynamometer and expressed in absolute newtons as well as adjusted for body size. Because crude hip force parameters and body size were highly correlated, they were submitted to principal component analysis to account for multicollinearity before performing the Cox regression analysis, which led to 4 candidate predictors entered in the Cox regression model.
Testing Procedures
Player Demographics and Anthropometrics
Upon enrollment, all participants completed a baseline questionnaire documenting soccer experience (ie, years of experience playing soccer in a club) and leg dominance as defined by the preferred leg for kicking the ball. Anthropometric characteristics (body height [HT] and body weight [BW]) were collected for each player, and body mass index and the factor BW × HT2 were calculated for each player. According to Milgrom et al, 27 BW × HT2 (adjusted body size) is a significant predictor of lateral ankle sprains and incorporates the influence of variances in body size on sustaining the injury. Specifically, this factor implies that taller and heavier people have larger inertia moments around the ankle axis, putting them at increased risk of sustaining a lateral ankle injury. It was previously suggested that adolescent growth spurts lead to increased susceptibility for traumatic injuries in soccer players. 46 Therefore, we included BW × HT2 in our regression models to adjust hip strength variables for body size dependencies as well as to account for potential confounding stemming from growth spurts. 27 On the basis of assessments of maturity using anthropometric data, 28 the convergent validity of adjusted body size as a surrogate measure of growth spurt–related changes in body size in our team’s sample of 639 boys 8 (age range, 11-15 years) was evident from strong correlations with the percentage of predicted adult height (r = 0.8, P < .001) and predicted growth remaining (r = −0.8, P < .001). This confirms that increases in BW × HT2 also reflect the likelihood of growth spurts and enabled us to interpret the results accordingly.
In the present sample, however, BW × HT2 was highly correlated with chronological age (r = 0.9, P < .001) and soccer experience (r = 0.7, P < .001), signifying that these variables are multicollinear and cannot be entered together in a regression analysis. It was previously suggested that assessments of maturity are more appropriate than chronological age in ascertaining injury risks in youth players. 19 Therefore, regression analyses were adjusted for BW × HT2 instead of for chronological age or soccer experience.
Hip Strength
Hip strength of the flexors, extensors, abductors, adductors, and external and internal rotators was measured isometrically using a Microfet handheld dynamometer (Hoggan Health Industries Inc). To allow for a standardized testing procedure, all participants crossed their arms over their chest during the test; the exception was for hip extension, in which participants were in a prone position with their arms lying along their sides, with their elbows extended and palms down. For every muscle group, 2 isometric contractions were performed over 5 seconds, with 1 minute of rest between contractions; the peak force was retained for further analysis. 44 The force of the hip flexors and external and internal rotators was measured with the participants in a seated position and the upper leg supported by the table. While participants were instructed to push maximally against the dynamometer, resistance was applied on the anterior aspect of the distal thigh, 2 cm proximal to the knee, for hip flexion measurements and 2 cm proximal to the medial or lateral malleolus to assess hip external rotation or internal rotation force, respectively. For the abductors and adductors, participants lay supine with the hips in a neutral position and with both knees extended. As the participants were instructed to abduct or adduct the leg, the dynamometer was placed on the lateral or medial aspects of the thigh, respectively, and 2 cm proximal to the respective femoral epicondyles. Finally, hip extension force was assessed with subjects lying prone. Subjects were instructed to lift the leg with the knee flexed 90° while the dynamometer was placed on the posterior side of the thigh 2 cm proximal to the popliteal crease.35,43 Isometric hip strength as assessed with a handheld dynamometer has good to excellent intra- and intertester reliability.24,36 To allow for interpretation of hip strength across our sample, variances owing to body size were accounted for by adjusting hip force measurements for BW × HT2 in the regression models. 27 Muscle strength ratios for hip flexion/extension, internal rotation/external rotation, and abduction/adduction were also computed.
Injury Registration and Athletic-Exposure Time
Injuries were monitored by the team’s medical staff under the supervision of an orthopaedic surgeon and sports medicine fellow. For every injury, the date, type (eg, sprain), diagnosis (eg, lateral ankle sprain), and site (eg, left ankle) were documented, including the time of return to play and playing time lost. An injury was defined as a physical complaint that prohibited the player to participate in practices or games for at least 48 hours and was only taken into account when it occurred during soccer practice or a game. 23 Based on the duration of playing time lost, the overall severity of lateral ankle sprain injuries was appraised as mild if the average absence ranged between 1 and 7 days, moderate if the time lost was between 8 and 28 days, and severe if the average absence was longer than 28 days. 12
Time of athletic exposure was documented by the trainer staff on a standardized sheet and monitored to the nearest 5 minutes. Total exposure time was calculated for each player and was defined as the time of participation in soccer games and/or practice measured from the start of the study until the first injury in injured players or until the end of study in those who remained injury free. Sport activities other than soccer were not taken into account.
Statistical Analysis
Upon completion of the study, injury registration records were used to calculate injury incidence as the number of injuries per 1000 athlete-exposure hours (AEs) as well as to divide players into 2 categories: those who had sustained a lateral ankle sprain during the study (12 [9%]) and those who did not (121 [91%]). For the participants who sustained an injury, data from the injured leg were used for analysis; for controls who remained injury free, the study leg was randomly assigned using a simple randomization scheme (Microsoft Excel 2010). Descriptive statistics were calculated as the mean ± SD for continuous variables or the number (percentage) for categorical variables. Accordingly, differences between groups were investigated using Fisher exact tests or t tests for independent samples, whenever appropriate.
To determine whether hip strength is a risk factor for lateral ankle sprains in youth soccer players, a principal-component, multivariate Cox regression analysis was performed. This approach was chosen because it combined principal component analysis (PCA), which reduced the number of predictors while limiting multicollinearity among variables, with a Cox regression that allowed us to adjust the regression model for variance in exposure times across our sample. 18 This strategy reduced the number of variables to 4 candidate predictors that were entered in the final multivariate Cox regression model: (1) body size dependencies and anterior chain/horizontal plane hip muscle forces, (2) posterior chain hip muscle forces, (3) hip abductor force, and (4) hip adductor force. These 4 variables were identified implementing a 2-stage predictor selection process. First, univariate Cox regression analyses confirmed significant simple relationships between all candidate predictor variables (ie, hip strength variables and BW × HT2), except muscle strength ratios, and dichotomous injury outcomes (ie, lateral ankle sprain and no lateral ankle sprain). In the second step of variable selection, multicollinear variables of BW × HT2, hip flexion strength, and hip internal and external rotation strength were subjected to a PCA with oblimin rotation, which identified 2 components (explaining the cumulative variance of 87%). The variables of body size (BW × HT2) and force of hip flexors and internal and external rotators strongly loaded on factor 1, whereas the hip extension force variable strongly loaded on factor 2. Regression coefficients, hazard ratios (HRs), 95% confidence intervals (95% CIs), and P values were calculated. Because our approach retrieved regression coefficients that are unitless, Kaplan-Meier survival time series were appraised to facilitate the clinical interpretation of the model. Finally, the Allison R (pseudo R2) was calculated to evaluate goodness of fit.
The significance level was set at P < .05. Statistical analysis was performed using SPSS software (version 22.0; IBM Statistics).
Results
A total of 133 of 140 soccer players were included for analysis. No participants were lost to follow-up during the injury registration period. The overall injury incidence was 2.0 per 1000 AEs. In total, 12 participants sustained a lateral ankle sprain (0.36 per 1000 AEs) representing 18% of all reported injuries (U11, 0 [0%]; U12, 0 [0%]; U13, 0 [0%]; U14, 4 [33%]; U15, 2 [17%]; U16, 4 [33%]; and U17, 2 [17%]). Ankle sprain injuries resulted in a mean training and/or game time loss of 22.4 ± 11.7 days; thus, these injuries were considered moderate in severity. In the group that did not sustain a lateral ankle sprain, 56 players (46%) sustained another musculoskeletal injury. These included muscle-tendon injuries to the quadriceps (12 [18% of all reported injuries]), hamstrings (4 [6%]), adductors (13 [19%]), or triceps surae (6 [9%]) as well as apophysitis (5 [7%]), contusions (5 [7%]), fractures (2 [3%]), other sprains (ie, ankle eversion sprain or lateral collateral ligament of the knee, 2 [3%]), and miscellaneous injuries (7 [10%]). There was no significant difference in the proportion of dominant legs included for analysis between the lateral ankle sprain group and those that did not incur a lateral ankle sprain (P = .30). On average, the players had a mean 7.4 ± 2.0 years of soccer experience (Table 1).
After adjustment for body size dependencies and other hip muscle forces, the final principal-component, multivariate Cox regression model only identified posterior chain hip muscle force (factor 2) as an independent risk factor for lateral ankle sprains in youth soccer players. Specifically, the model showed that players with higher posterior chain hip muscle forces have significantly lower hazards to sustain a lateral ankle sprain (HR, 0.3; 95% CI, 0.1-0.9; P = .028).
When observing the time span that players remained injury free, mean survival times in participants with a lateral ankle sprain were up to 10% longer on average if posterior chain hip muscle force scores were higher than the sample means (127.5 ± 88.20 hours for lower hip extension force compared with the sample means, 153.9 ± 79.6 hours for higher hip extension force) as well as across the entire sample (216.1 ± 164.5 hours for lower hip extension force, 282.9 ± 215.6 hours for higher hip extension force). No other study variable could be identified as a risk factor for lateral ankle sprains. Table 2 presents the regression coefficients, HRs with 95% CIs, and P values. The Allison R for the entire model and for factor 2 was 0.11 and 0.08, respectively.
Principal-Component, Multivariate Cox Regression Model a

The regression coefficient (B [constant]) and HR were calculated using standard scores derived from the principal component analysis (for body size dependencies and anterior chain hip muscle force and for posterior chain hip muscle force) and from z scores (for hip adductor muscle force and for hip abductor muscle force). 95% CI, 95% confidence interval; HR, hazard ratio.
Significant at P < .05. A negative/positive value for B indicates that players sustaining a lateral ankle sprain had lower/higher variable scores compared with those that did not sustain the ankle injury. Alternatively, a HR of higher/lower than 1 indicates that an increase in 1 unit of (standard) variable scores increases/decreases the hazard of sustaining the lateral ankle sprain injury.
Discussion
Numerous epidemiological studies have emphasized the burden of lateral ankle sprains in youth soccer players.3,4 However, to our knowledge, no prospective study has yet identified intrinsic risk factors for these injuries in this population that are modifiable through physical rehabilitation. Our study reports the results of a 3-season prospective cohort study, which is the first to investigate the role of proximal hip strength as a risk factor for lateral ankle sprain injuries in youth male soccer players. In agreement with our hypothesis, we identified decreased hip muscle strength as a risk factor for lateral ankle sprains. Specifically, decreased strength of the posterior chain hip muscles, which was largely indicative of decreased hip extension strength, was retained as an independent risk factor after adjustment for body size dependencies and strength of the other hip muscles. This risk was evident from a decrease in survival time of 10% on average (ie, which equaled a loss of 13 hours on average during which the player could have remained injury free) in those players that had posterior hip muscle forces lower than the average of the sample, or vice versa.
In our study, the overall injury incidence was 2.0 per 1000 AEs, and the injury incidence was 0.36 per 1000 AEs for lateral ankle sprains in particular. Our overall injury incidence results, however, are somewhat lower than incidence rates reported previously in youth soccer populations, which ranged from 2 to 7 injuries per 1000 AEs. 12 Because the choice of injury definition might have accounted for these differences between studies, we excluded minor injuries such as abrasions and blisters compared with others who adopted a more inclusive approach. 31 When ankle injuries are specifically considered, our results are similar to Cloke et al, 3 who reported an injury rate of 0.34 ankle injuries per 1000 AEs, with lateral ankle sprains accounting for 63.5% of all ankle injuries.
To our knowledge, there is currently no prospective evidence available that associates decreases in posterior hip muscle strength with a higher incidence of lateral ankle sprains in a population exclusively comprising youth soccer players. In agreement with the previous work of McHugh et al, 26 we were unable to identify strength of the hip flexors, adductors, and abductors as a risk factor for ankle sprains. Interestingly, although these authors screened a general population of high school athletes, measurements of hip extension strength were not included in the protocol. 26 Although we did not perform motion analyses to determine the biomechanical link between hip muscle strength and ankle sprains, decreases in hip muscle strength may contribute to reduced dynamic control of the hip joint. Soccer is a high-intensity sport with substantial impact on the lower extremities, owing to the high-velocity performance, change of direction, and jump-landing movements the sport requires. 12 During landings, the hip extensor muscles play an important role in the deceleration of the body center of mass. 34 Thus, the capability to slow high-velocity maneuvers, and thus dampen or absorb impact, may be limited or inadequate in players with decreased hip extension strength. 30
Ankle sprains usually occur during the transition from unloaded to loaded conditions. 42 Because the ankle joint is relatively unstable during these transition phases, shock attenuation and deceleration of the body center of mass is crucial and is primarily achieved through eccentric muscle action. 29 In the case of reduced muscle function, the extent to which shock absorption is adequate is more likely to depend on contributions from passive stabilizers such as ligaments, the joint capsule, and articular congruity. Similarly, in knee injury studies, lower hip extension forces have been suggested to result in changes in muscle dependence, potentially increasing the reliance on passive restraints from frontal plane ligaments. 34 In a healthy population, prior research showed that when fatigue was induced during a single-leg drop landing protocol, a distal-to-proximal redistribution of muscle work occurred during shock attenuation. 5 This redistribution of muscle work was considered a compensatory response because it increased the reliance on the larger hip extensors, which are generally more capable of absorbing impact forces, while ankle work reduced. 5 Thus, the youth soccer players with relatively more impaired hip extension force in our study might not have been able to meet this higher demand, with increasing ankle loads and greater susceptibility to injury as a result. Doherty et al 7 showed that sustaining a lateral ankle sprain affected joint work throughout the kinetic chain in individuals with chronic ankle instability, increasing the dominance on hip joint movement strategies. However, this shift was suggested to be detrimental in the longer term, because differences in hip function were found to discriminate between ankle sprain copers and individuals who developed chronic ankle instability. 7 The higher risk of injury recurrence in their study population was also attributed to an improper or unbalanced mediation of landing forces. 6
While we observed no lateral ankle sprain injuries in the youngest age groups (ie, 10-12 years) as opposed the older age categories (ie, 13-16 years), one may argue that the risk of sustaining a lateral ankle sprain injury depended on maturity status and age rather than on hip muscle strength alone. It has indeed been indicated that younger players have fewer sprains and strains compared with older players, because older players take more risks and are more aggressive and competitive. 12 Because the players who sustained a lateral ankle sprain in our study indeed were likely more mature, one must consider that our statistical model identified hip extension muscle force as an independent risk factor even after adjustment for growth spurt–related variances in body size (BW × HT2). Considering that adjusted body size and age were highly correlated (r = 0.9, P < .001), this means that, across all age categories, players with decreased hip extension strength would exhibit higher hazards of sustaining a lateral ankle sprain. Adjusted regression coefficients were thus calculated independent of maturity-related anthropometric characteristics and were estimated also taking into account the strength and anthropometrics of those that did not sustain the injury and were younger. Furthermore, a post hoc analysis among the oldest players aged 15 and 16 years also supports that decreased hip extension is a risk factor for lateral ankle sprains regardless of maturity, age, or any body size influences (HR, 0.1; 95% CI, 0.02-0.71; P = .019; data not shown).
On the basis of our findings, one may suggest that increasing hip extension strength may be a valuable component in injury prevention programs for ankle sprain in youth soccer players. Although the effect of higher hip muscle force on the extent to which players remained injury free appeared modest (10% more injury-free play time), dedicated randomized controlled trials are also necessary to conclusively state that increasing posterior hip extension strength effectively decreases the likelihood of incurring an ankle sprain. Although no such trials exist to date, research has shown that hip strength is in fact a modifiable factor. Hoshikawa et al 17 reported that the addition of core stability exercises to regular soccer training in male youth soccer players effected considerable increases in hip extensor strength of 41% on average. Stearns and Powers 39 also showed that a hip-focused training program, which aims to improve hip muscle solicitation during the deceleration phase of landing, can increase hip extensor strength by 7% and shift energy absorption more proximal to the hip during landing tasks. These findings suggest that hip-focused or core stability training could be effective in improving dynamic hip control.
Strengths and Limitations
This was the first prospective study with a 3-season follow-up that identified a risk factor for lateral ankle sprains with potential to directly influence the design of physical rehabilitation schemes in youth soccer players. Unlike previous reports in which AEs were calculated as an overall mean based on the number and duration of games and training sessions per age category, 45 a strength of this study is that exposure time and injury registration was rigorously documented by the training staff and monitored on an individual player level, ensuring an accurate estimation of HRs.
Some methodological limitations, however, should be considered. First, although our study design incorporated the requirements of temporality associated with a prospective study, cause-and-effect relationships could not entirely be inferred because we did not include a comparator group consisting of soccer players who had never had an ankle sprain. This additional group would have further assisted in elucidating whether hip strength impairments would “cause” an index ankle sprain, because previous injury is also often considered a risk factor for reinjury. Although we did not account for the subjects’ injury history more than 6 months before entering the study, recent research has questioned the role of previous injury history in subsequent injury rates. Hamilton et al 16 showed that injury rates were unchanged for both second and third injuries compared with the first injury, suggesting that “previous injury” may mask the underlying causal risk factor. 16 Second, despite significant associations between hip extension force and the occurrence of ankle sprains, effects on survival or injury-free times were modest, which indicates that other factors will also play a role in the injury mechanism. Thus, the predictive value of our risk model warrants validation and replication in larger samples and/or samples with a greater proportion of players sustaining a lateral ankle sprain. This will further confirm whether decreased hip extension muscle force remains a risk factor for lateral ankle sprains in youth soccer players as opposed to other hip muscle groups (eg, hip abduction). 14 Finally, although we used clinical measurements that are easily implemented in the field and thus highly feasible in large-scale prospective studies, we acknowledge that isometric strength testing has disadvantages such as limited translation to sport-specific maneuvers.
Conclusion
In this 3-season prospective cohort study, decreased hip extension strength was identified as an independent risk factor for sustaining a lateral ankle sprain in youth male soccer players. Assessing hip extension strength may therefore be advisable in screening protocols as well as prevention programs. However, future research in larger samples with more injured players is necessary to further confirm the importance of hip extension force as a risk factor for ankle sprains.
Footnotes
Acknowledgements
The authors gratefully acknowledge the opportunity to work with soccer club SV Zulte Waregem (first division, Belgium) and be able to screen their players at their club.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.