
Abstract
Background:
Musculoskeletal injuries are prevalent among military trainees and certain occupations. Fitness and body mass index (BMI) have been associated with musculoskeletal conditions, including stress fractures.
Hypothesis:
The incidence of, and excess health care utilization for, stress fracture and non–stress fracture overuse musculoskeletal injuries during the first 6 months of service is higher among unfit female recruits. Those who exceeded body fat limits are at a greater risk of incident stress fractures, injuries, or health care utilization compared with weight-qualified recruits.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All applicants to the United States Army were required to take a preaccession fitness test during the study period (February 2005–September 2006). The test included a 5-minute step test scored as pass or fail. BMI was recorded at application. There were 2 distinct comparisons made in this study: (1) between weight-qualified physically fit and unfit women and (2) between weight-qualified physically fit women and those who exceeded body fat limits. We compared the incidence of, and excess health care utilization for, musculoskeletal injuries, including stress fractures and physical therapy visits, during the first 183 days of military service.
Results:
Among the weight-qualified women, unfit participants had a higher non–stress fracture injury incidence and related excess health care utilization rate compared with fit women, with rate ratios of 1.32 (95% CI, 1.14-1.53) and 1.18 (95% CI, 1.10-1.27), respectively. Among fit women, compared with the weight-qualified participants, those exceeding body fat limits had higher rate ratios for non–stress fracture injury incidence and related excess health care utilization of 1.27 (95% CI, 1.07-1.50) and 1.20 (95% CI, 1.11-1.31), respectively. Weight-qualified women who were unfit had a higher incidence of stress fractures and related excess health care utilization compared with fit women, with rate ratios of 1.62 (95% CI, 1.19-2.21) and 1.22 (95% CI, 1.10-1.36), respectively. Among fit women exceeding body fat limits, the stress fracture incidence and related excess health care utilization rate ratios were 0.79 (95% CI, 0.49-1.28) and 1.44 (95% CI, 1.20-1.72), respectively, compared with those who were weight qualified.
Conclusion:
The results indicate a significantly increased risk of musculoskeletal injuries, including stress fractures, among unfit recruits and an increased risk of non–stress fracture musculoskeletal injuries among recruits who exceeded body fat limits. Once injured, female recruits who were weight qualified but unfit and those who were fit but exceeded body fat limits had increased health care utilization. These findings may have implications for military accession and training policies as downsizing of military services will make it more important than ever to optimize the health and performance of individual service members.
Musculoskeletal conditions are prevalent among all age and sex groups, across all sociodemographic strata, and represent a major public health crisis in an otherwise generally young and healthy United States (US) military population. Within the US military, unintentional injuries lead all other medical conditions for the number of persons affected and number of medical encounters. 19 Injury-related musculoskeletal conditions are a leading contributor to lost duty time, with sports and physical training being the leading causes. 19 The occurrence of musculoskeletal conditions has been associated with poor physical fitness 13 and being overweight. 18
A 2006 review of the literature examining temporal trends in physical fitness of new US Army recruits from 1975 to 2003 suggested no change in muscular endurance or maximal oxygen uptake (VO2 max in mL/kg/min) over time. 14 However, slower times on 1- and 2-mile runs indicated declines in aerobic performance from 1987 to 2003. 14 The authors concluded that the apparent discrepancy between the VO2 max and endurance running data may indicate that recruits are not as proficient at applying their aerobic capability to performance tasks, such as timed runs, possibly because of factors such as increased body weight, reduced experience with running, lower motivation, and/or environmental factors. 14
Compounding the problem of reduced running endurance among military recruits is the obesity epidemic in the US, with the body mass index (BMI) having progressively increased among recruits for military service over a 25-year period (1978-2000). 14 This increase in the number and proportion of overweight recruits may lead to an increase in musculoskeletal injuries and specifically stress fractures during basic training, which put additional strain on an overburdened military health care system, contributing to delays in training and increased attrition among recruits and ultimately affecting operational readiness.
In 2004, the US Army Accessions Command instituted a simple “fitness and motivation” test as part of the Assessment of Recruit Motivation and Strength (ARMS) study and program. The goal was to determine the potential for allowing some usually weight-disqualified people to be screened into the Army. The ARMS study ran from February 2005 to September 2006, while the program ran from the end of the study through fiscal year 2009. Previous evaluations of this study demonstrated that men and women who did not complete the step test before entering active duty were significantly more likely to leave the military for any reason compared with those who had completed this test at a Military Entrance Processing Station (MEPS). 16 Men who met weight standards, but did not complete the step test, demonstrated an approximately 30% increase in the risk of musculoskeletal injuries during basic training (odds ratio, 1.31; 95% CI, 1.20-1.43), 2 while those who were over the weight standard and completed the step test were 47% more likely to experience a musculoskeletal injury (hazard ratio, 1.47; 95% CI, 1.30-1.66). 6 Preliminary analyses of women who met weight standards demonstrated a 76% higher stress fracture incidence and 35% higher incidence of other musculoskeletal injuries among those who did not complete the step test. 5
This report evaluates the incidence of, and health care utilization for, stress fracture and non–stress fracture overuse musculoskeletal injuries during the first 6 months of service, comparing differences between 2 potentially high-risk groups. The first comparison is among weight-qualified women, comparing the incidence and utilization between unfit and fit women. The second comparison is among fit women, comparing those who exceeded body fat limits to those who were weight qualified. The hypotheses were that (1) the incidence of, and excess health care utilization for, stress fracture and non–stress fracture overuse musculoskeletal injuries is higher among unfit female recruits and (2) those who exceeded body fat limits are at a greater risk of incident stress fracture injuries or health care utilization compared with weight-qualified recruits.
Methods
This study was approved by the Walter Reed Army Institute of Research Institutional Review Board. A prospective cohort study of women enlisting for the first time was conducted to determine the utility of a simple step test in screening people into the military. The ARMS step test consists of a 5-minute modified Harvard step test, administered to all Army applicants at 6 of the 65 MEPSs. The following sites were chosen to approximate a representative nationwide sample of Army applicants: Atlanta, Georgia; Buffalo, New York; Chicago, Illinois; Sacramento, California; San Antonio, Texas; and San Diego, California. Female participants stepped up and down on a platform 12 inches high at the metronome pace of 120 (30 steps/min). Those who completed the full 5 minutes were considered “fit,” while those who failed to continue at the proper pace were considered “unfit.” Additional details on the study methods have been published elsewhere. 16
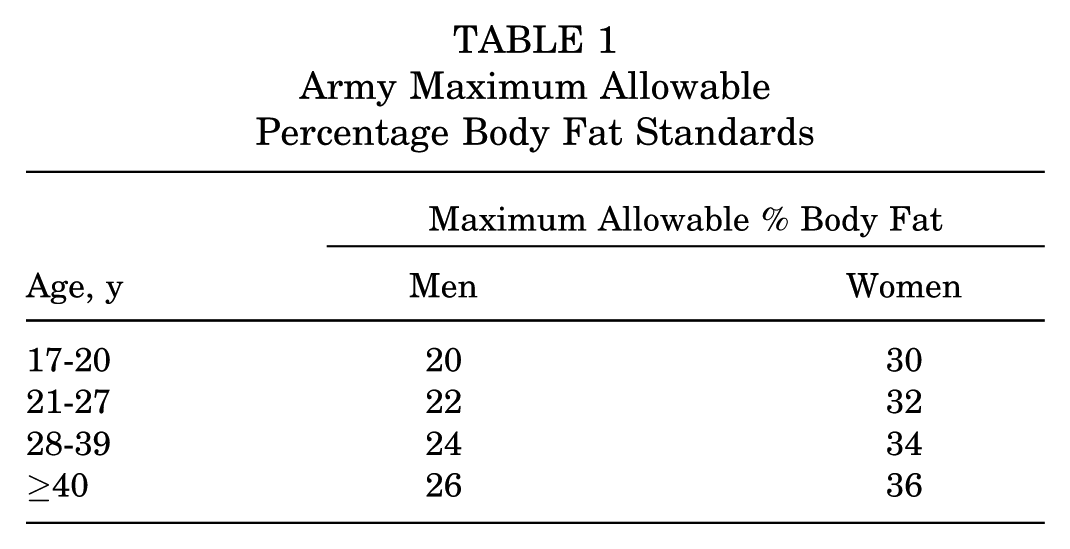
Applicants meeting weight-for-height and body fat standards (Table 1) were denoted as “weight qualified.” Applicants exceeding weight-for-height and body fat standards were labeled as “exceeds body fat.” The limits for exceeding body fat were based on the Army’s 2-tiered, age- and sex-specific screen for weight and body fat and were set at up to 36% for women (maximum body fat allowable to those ≥40 years). 7 Participants considered fit by the study’s definition who exceeded body fat limits were granted a waiver and allowed to enlist.
Army Maximum Allowable Percentage Body Fat Standards
Study Design and Population
Study participants included in these analyses were female US Army active-duty members aged ≥18 years who entered the military for the first time between February 2005 and September 2006. All participants provided informed consent and took the ARMS step test. Women who exceeded body fat limits and failed the test were precluded from entering service. Participants were observed for 183 days (those who left the military before this time were followed up to the time of discharge). Participants who entered active duty with waivers for any musculoskeletal disorders; discharged because of pre-existing musculoskeletal disorders; or missing weight, height, or accession dates were excluded from analyses. These women had not been excluded from previous analyses. 5
Data Sources
Accession data were provided by the Center for Accession Research, US Army Accessions Command. The US Military Entrance Processing Command (USMEPCOM) and the Defense Manpower Data Center provided demographic and separation codes. The USMEPCOM also provided discharge data related to pre-existing conditions and disqualifying medical status. The US Army Recruiting Command provided accession medical waiver data, and the Patient Administration Systems and Biostatistics Activity provided outpatient health care encounter data from the Standard Ambulatory Data Record.
Case Definitions
Participants who had at least 1 medical encounter resulting in a diagnosis of a stress fracture, using the International Classification of Diseases, 9th Revision (ICD-9) codes 733.93 (stress fractures of the tibia or fibula), 733.94 (stress fractures of the metatarsals), and 733.95 (stress fractures of other bone), were considered separately from all other musculoskeletal injuries. Non–stress fracture musculoskeletal injury incident cases were defined as participants who only experienced non–stress fracture musculoskeletal injuries including sprains and strains, based on the first outpatient medical encounter with ICD-9 codes 715-717, 719, 720, 724, 726-728, and 843-847. Specific conditions included pain, sprain/strain, arthropathy, fasciitis, enthesopathy and bursitis, and tendinosis/tendinitis. Injury sites included the ankle/foot, lower leg, lumbar and sacrum/coccyx regions of the back (lower back), knee, and hip/thigh/pelvis. Any musculoskeletal diagnosis was defined as the first medical encounter for stress fractures or other musculoskeletal injuries using all ICD-9 codes listed above. The focus of this study was stress fracture and non–stress fracture musculoskeletal injuries.
All medical encounters resulting in musculoskeletal injury diagnoses and all physical therapy visits (code V57.1) after the qualified musculoskeletal injury diagnosis and within 183 days were considered utilization visits. The rates of utilization were considered only among those women who had qualifying musculoskeletal injuries (non–stress fractures or stress fractures). That is, given that they had experienced a non–stress fracture or stress fracture, did women in the high-risk groups utilize more injury-related health care than those in the low-risk groups?
Statistical Analysis
Demographic categorical data were evaluated for statistical significance in differences and trends with the chi-square test. Risk was defined as the number of events divided by the population at risk multiplied by 100; relative risk was the risk in the exposed group divided by the risk in the unexposed group. The denominator for injury-specific risks excluded participants with another injury (eg, the denominator for stress fractures excluded participants who had non–stress fracture musculoskeletal injuries). Crude incidence rates of outcomes were defined as the number of cases per 1000 person-days of military service. Person-days accrued until the first non–stress fracture or stress fracture medical encounter, separation from service, or end of the study period. Crude and adjusted incidence rate ratios (IRRs) were calculated using Poisson regression for all outcomes. Variables in the regression models included the step test result (unfit/fit), body fat status (exceeds body fat limits/weight qualified), age, smoking status, BMI, race, and education. In the multivariable analysis, the overweight and obese categories were collapsed into one group because of the small number of women found in the highest BMI group.
The association between fitness, ARMS waiver for exceeding body fat limits, and number of outpatient medical encounters related to utilization with musculoskeletal injury diagnoses in the first 183 days of service was analyzed using Poisson regression. Person-days accrued until separation from service or end of the study period. In this analysis, only participants with musculoskeletal overuse injuries were included. All statistical analyses were performed using SAS version 9.3 (SAS Institute).
Results
Demographics
Of the 1900 female recruits who entered active duty during the study period, 315 (16.6%) exceeded body fat limits, and 1585 (83.4%) were weight qualified. Among the weight qualified, 1061 (66.9%) were fit and 524 (33.1%) unfit, while all those who exceeded body fat limits had to be fit to enter active duty (Table 2).
Characteristics of Female ARMS Study Participants a
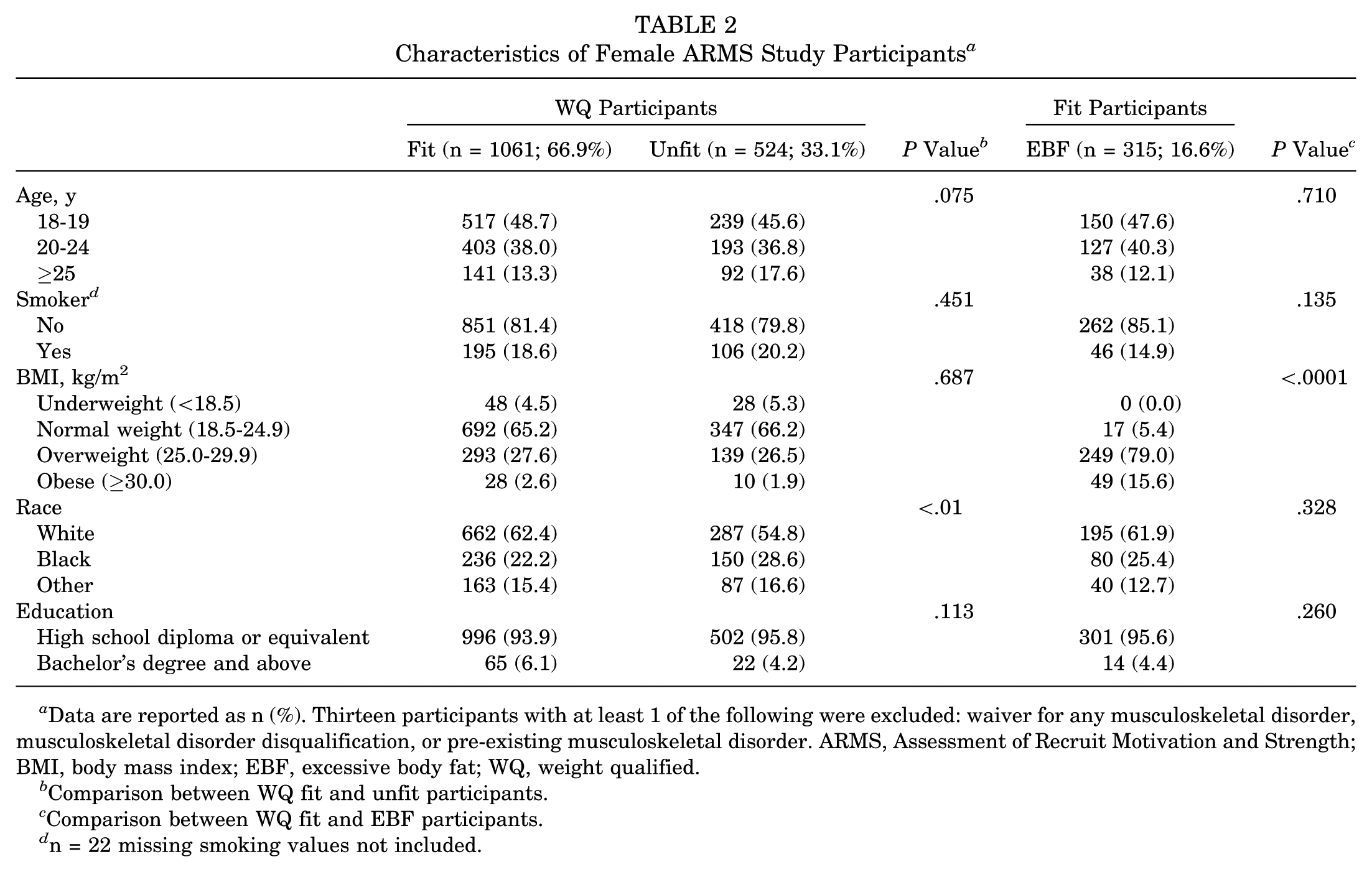
Data are reported as n (%). Thirteen participants with at least 1 of the following were excluded: waiver for any musculoskeletal disorder, musculoskeletal disorder disqualification, or pre-existing musculoskeletal disorder. ARMS, Assessment of Recruit Motivation and Strength; BMI, body mass index; EBF, excessive body fat; WQ, weight qualified.
Comparison between WQ fit and unfit participants.
Comparison between WQ fit and EBF participants.
n = 22 missing smoking values not included.
Among weight-qualified participants, race differed significantly between those considered fit and unfit. As expected, BMI was significantly higher among those who exceeded body fat limits.
Incidence of Non–Stress Fractures and Stress Fractures
As seen in Table 3, the incidence (per 1000 person-days) for non–stress fracture injuries was significantly higher for unfit than fit, weight-qualified women (adjusted IRR, 1.32; 95% CI, 1.14-1.53). Among fit women, those who exceeded body fat limits had a higher incidence than weight-qualified women (adjusted IRR, 1.27; 95% CI, 1.07-1.50). The risk of stress fractures was higher among unfit, weight-qualified women (adjusted IRR, 1.62; 95% CI, 1.19-2.21), but among fit women, there was no significant difference between participants who exceeded body fat limits and those who were weight qualified (adjusted IRR, 0.79; 95% CI, 0.49-1.28).
Incidence Rates and Adjusted IRRs for the Diagnosis of Non–Stress Fracture Musculoskeletal Injuries and Stress Fractures in the First 183 Days of Service a
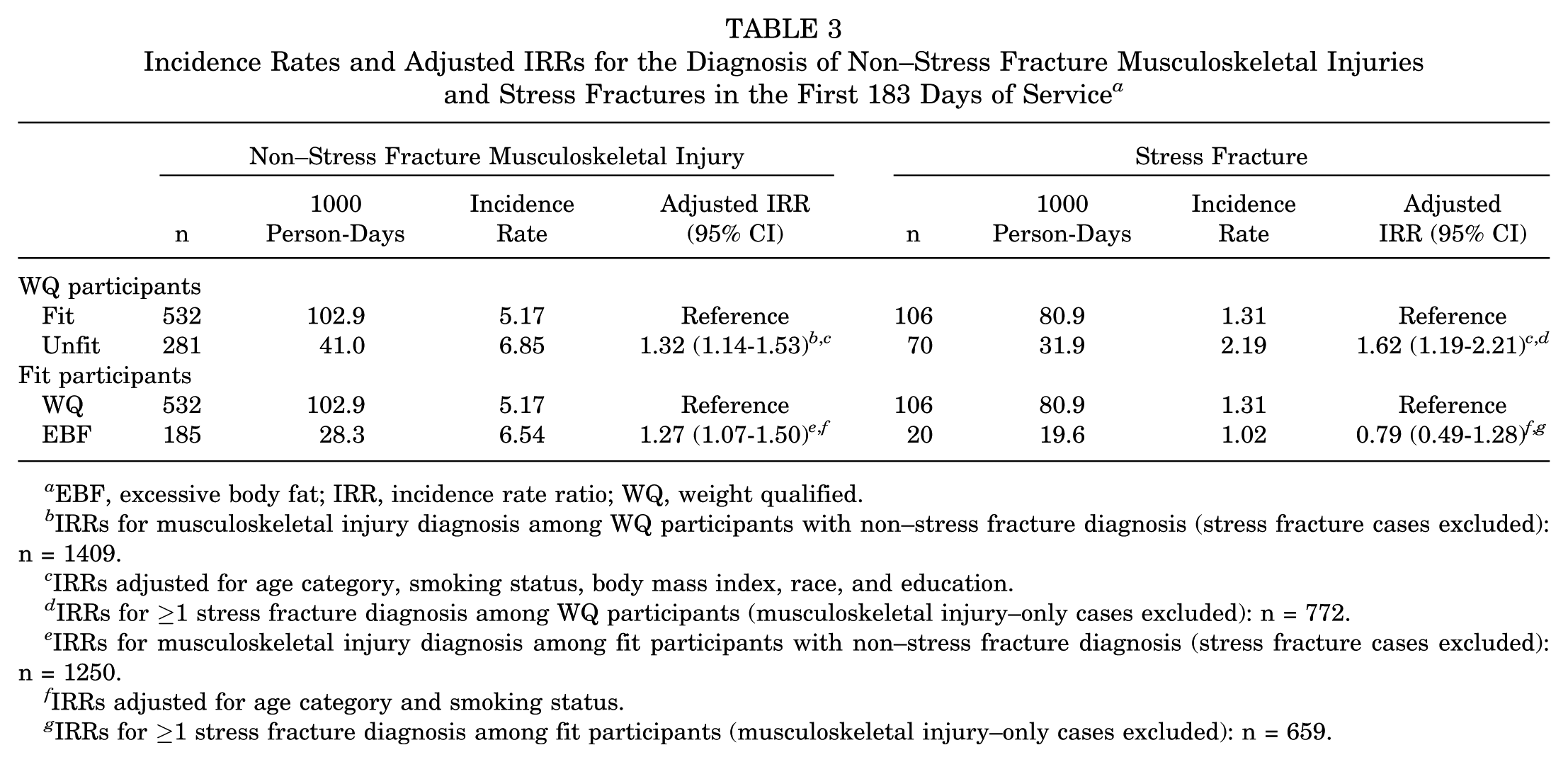
EBF, excessive body fat; IRR, incidence rate ratio; WQ, weight qualified.
IRRs for musculoskeletal injury diagnosis among WQ participants with non–stress fracture diagnosis (stress fracture cases excluded): n = 1409.
IRRs adjusted for age category, smoking status, body mass index, race, and education.
IRRs for ≥1 stress fracture diagnosis among WQ participants (musculoskeletal injury–only cases excluded): n = 772.
IRRs for musculoskeletal injury diagnosis among fit participants with non–stress fracture diagnosis (stress fracture cases excluded): n = 1250.
IRRs adjusted for age category and smoking status.
IRRs for ≥1 stress fracture diagnosis among fit participants (musculoskeletal injury–only cases excluded): n = 659.
Musculoskeletal Injury Health Care Utilization AfterDiagnosis of Non–Stress Fractures and StressFractures
As seen in Table 4, once weight-qualified women were diagnosed with an injury, unfit women had a higher adjusted utilization rate ratio (URR) for non–stress fractures (1.18; 95% CI, 1.10-1.27) and stress fractures (1.22; 95% CI, 1.10-1.36). Similarly, among fit women, those who exceeded body fat limits had a higher adjusted URR after any non–stress fracture injury (1.20; 95% CI, 1.11-1.31) and stress fracture (1.44; 95% CI, 1.20-1.72).
Postinjury Health Care Utilization Rates and Adjusted URRs Among Women With Non–Stress Fracture Musculoskeletal Injuries and Stress Fractures a
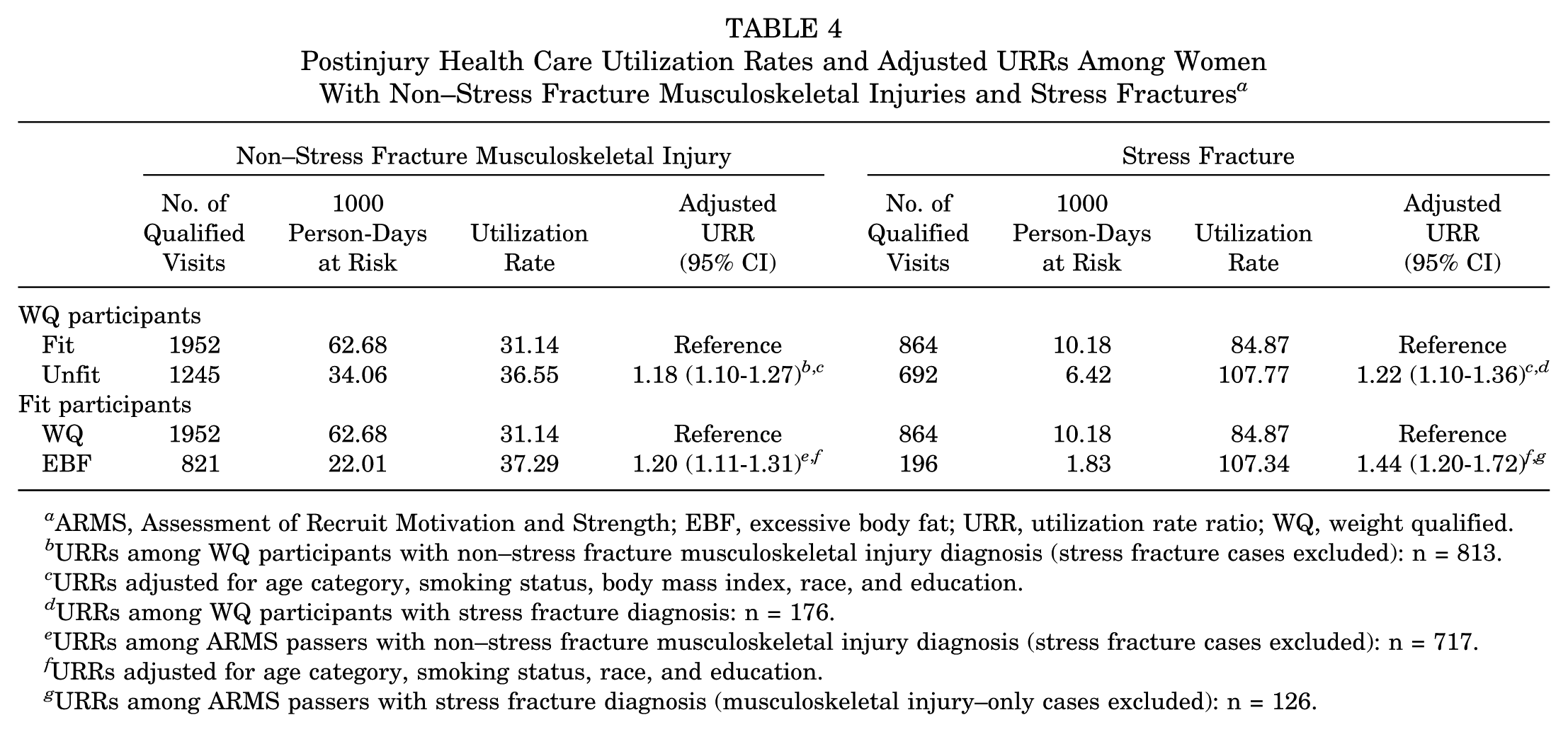
ARMS, Assessment of Recruit Motivation and Strength; EBF, excessive body fat; URR, utilization rate ratio; WQ, weight qualified.
URRs among WQ participants with non–stress fracture musculoskeletal injury diagnosis (stress fracture cases excluded): n = 813.
URRs adjusted for age category, smoking status, body mass index, race, and education.
URRs among WQ participants with stress fracture diagnosis: n = 176.
URRs among ARMS passers with non–stress fracture musculoskeletal injury diagnosis (stress fracture cases excluded): n = 717.
URRs adjusted for age category, smoking status, race, and education.
URRs among ARMS passers with stress fracture diagnosis (musculoskeletal injury–only cases excluded): n = 126.
Discussion
These current findings regarding fitness and injuries generally confirm those by Cowan et al 5 on the same population. However, a number of participants likely at an increased risk unrelated to their fitness or body fat levels (eg, those who received an accession medical waiver for a pre-existing injury) were excluded from the current analyses, and therefore, these findings may be more accurate because of the stricter exclusionary rules imposed. In addition, these analyses also evaluate the association between exceeding body fat limits and injuries.
Weight-qualified women who were unfit had a higher incidence of both non–stress fractures and stress fractures, with an adjusted IRR similar to that reported by Cowan et al. 6 Although women who exceeded body fat limits had a higher incidence of non–stress fracture injuries compared with weight-qualified women (adjusted IRR, 1.27), they had a lower risk of stress fractures, albeit not statistically significantly so (adjusted IRR, 0.79). It is not well understood why women with excessive body fat did not have a higher incidence of stress fractures than weight-qualified women but at the same time once injured had a higher rate of health care utilization. Once injured, women who exceed body fat limits may require prolonged management and recovery because of their increased weight. It is also possible that there are other unmeasured confounding variables that may account for the unexpected finding. Additional research is needed to provide insight into this obesity paradox.
There is substantial literature documenting that unfit people, both men and women, are at an increased risk of injuries during military training and, among civilians, if engaging in high levels of activity.3,10-12 A number of studies have documented that patients with extreme BMIs are at an increased risk of musculoskeletal disorders,1,4,6,8,17,18,20,21 but evidence of this among military personnel is not strong, 8 and the relationship with injuries may be modified by age and sex. 17
The identification of potentially modifiable risk factors (being unfit and exceeding body fat limits) presents opportunities for reductions not just in morbidity but excess health care utilization as well. Once they were injured, women who were weight qualified but unfit and women who were fit but exceeded body fat limits had increased health care utilization. Unfit, weight-qualified women had 18% more related visits after a non–stress fracture injury and 22% more after a stress fracture. Among fit women, those exceeding body fat limits had 20% more related visits after a non–stress fracture injury and 44% after a stress fracture.
Among weight-qualified but unfit women, these excess visit rates translate to 5.4 (per 1000 person-days) additional non–stress fracture injury–related visits and 22.9 (per 1000 person-days) additional stress fracture–related visits. Among women who exceeded body fat limits but were fit, it translates to 6.2 (per 1000 person-days) additional non–stress fracture injury–related visits and 22.2 (per 1000 person-days) additional stress fracture–related visits.
There are several limitations of this study, including a simple step test that was used as a surrogate for fitness rather than physiological parameters such as VO2 max, BMI and fitness were assessed before entry and not at the time of injury, no individual participant or group exposure data (exercise, activity level) were available, and no specific proximal cause of injury could be ascertained. To an unknown extent, completion of the step test may actually serve as a surrogate for motivation, but the same problem exists with timed runs used in many other military studies. Previous studies among Army recruits have demonstrated that physical fitness measures (VO2 max) can be discrepant with actual performance (endurance running data) and may indicate that recruits are not as proficient at applying their aerobic capability to performance tasks, such as timed runs, possibly because of factors such as increased body weight, reduced experience with running, lower motivation, and/or environmental factors.9,14,15 Our findings are consistent with these previous military studies. Strengths include the prospective study design, diverse population (in terms of demographic characteristics, fitness, and body fat), highly regulated training environment, assessment of risk factors before entry, and essentially 100% capture rate of all medical encounters.
Because the ARMS program has been terminated and persons who exceed body fat limits are no longer allowed to enlist, the effect of preaccession exceeding body fat limits on the risk of injuries or health care utilization is moot. However, the data in our study highlight the effect of poor fitness as important for both the risk of injuries and health care utilization for stress fractures and non–stress fracture musculoskeletal injuries. Poor fitness is a potentially modifiable risk factor, but additional research is required to ascertain if targeted interventions actually result in reduced injury incidence and health care utilization.
The issue of excess body fat, regardless of how defined, remains a concern among civilian women who wish to engage in higher levels of activity. Such women should consult with their health care provider and may benefit from weight loss before substantially increasing their level of activity to minimize the risk of future injuries and subsequent health care visits.
With downsizing of military services and significant budget cuts, it will be more important than ever to optimize the health and performance of individual service members. Depending on the recruiting environment, consideration should be given to disqualifying those not willing or able to complete a simple step test or providing targeted interventions to those motivated enough to improve fitness.
Footnotes
Acknowledgements
The authors thank COL Earl H. Lynch, MC USAR, for his careful review of the article.
The views expressed are those of the authors and should not be construed to represent the positions of the Department of the Army or Department of Defense.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the US Army Medical Research and Materiel Command with ManTech International Corporation.