
Abstract
Background:
Baseball players exhibit a more posteriorly oriented humeral head in their throwing arm. This is termed humeral retrotorsion (HRT) and likely represents a response to the stress of throwing. This adaptation is thought to occur while the athlete is skeletally immature, however currently there is limited research detailing how throwing activity in younger players influences the development of HRT. In addition, it is presently unclear how this changing osseous orientation may influence shoulder motion within young athletes.
Purpose:
To determine the influence of throwing activity and age on the development of side-to-side asymmetry in HRT and shoulder range of motion (ROM).
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Healthy athletes (age range, 8-14 years) were categorized into 2 groups based upon sports participation; throwers (n = 85) and nonthrowers (n = 68). Bilateral measurements of HRT, shoulder external rotation (ER), internal rotation (IR), and total range of motion (TROM) at 90° were performed using diagnostic ultrasound and a digital inclinometer. Side-to-side asymmetry (dominant minus nondominant side) in HRT and in shoulder ER, IR, and TROM were assessed. Statistical analysis was performed with 2-way analysis of variance and Pearson correlation coefficients.
Results:
Throwers demonstrated a larger degree of HRT on the dominant side, resulting in greater asymmetry compared with nonthrowers (8.7° vs 4.8°). Throwers demonstrated a gain of ER (5.1°), a loss of IR (6.0°), and no change in TROM when compared with the nondominant shoulder. Pairwise comparisons identified altered HRT and shoulder ROM in all age groups, including the youngest throwers (age range, 8-10.5 years). A positive correlation existed between HRT and ER ROM that was stronger in nonthrowers (r = 0.63) than in throwers (r = 0.23), while a negative correlation existed with IR that was stronger in throwers (r = −0.40) than in nonthrowers (r = −0.27).
Conclusion:
Throwing activity causes adaptive changes in HRT and shoulder ROM in youth baseball players at an early age. Other factors in addition to HRT influence shoulder motion within this population.
Humeral retrotorsion (HRT) refers to a twisting about the long axis of the humerus in which the humeral head is oriented in a more posteromedial direction.9,22 Several investigations have noted a greater degree of HRT present in the dominant arm of mature baseball players.3,4,17,19,20,27,29,32 This alteration may represent a healthy adaptation to the stress of throwing, allowing for increased performance 22 while at the same time offering protection from injury.7,19,20,28 Although the ideal amount of HRT is currently unknown, previous research has suggested that excessive HRT may contribute to upper extremity injury by increasing elbow stress and pain. 15 In addition, insufficient HRT has been proposed to increase the likelihood of internal impingement and labral stress. 20
At birth, the humeral head is in marked retrotorsion, and it undergoes a process of derotation (less retrotorsion) during the pediatric and adolescent years.5,9 This process occurs most rapidly up to the age of 8 years and then slows down, approaching mean adult values by the age of 16 years and ceasing with closure of the proximal humeral physis at skeletal maturity.5,8 It has been proposed that the alterations in throwing-limb HRT recognized in adult baseball players develops as an adaptive response to throwing while they are skeletally immature, with the forces generated during throwing slowing the process of humeral derotation and leading to increased HRT. 23
While it seems intuitive that the changes in osseous alignment expressed in adult baseball players occur during growth, studies investigating changes in HRT within the youth population are limited.6,28,33,34 It remains unclear at what age these adaptations develop, and how factors such as age of onset of throwing or volume of throwing influence this change. In addition, the relationship between HRT and shoulder range of motion (ROM) appears to be inconsistent and may vary between adult and youth athletes. 34 With increasing emphasis on injury prevention strategies in youth baseball, understanding the effect that throwing forces exert on the development of the throwing shoulder may help in the advancement of prevention programs. Thus, the primary purpose of this study was to investigate the influence of age and throwing activity on the development of HRT and glenohumeral ROM across varying groups of young athletes. In addition, we sought to determine the relationship between HRT and shoulder ROM in both throwing and nonthrowing youth athletes. Our primary hypotheses were that baseball players would have a higher side-to-side asymmetry in HRT angle than nonthrowers and that this asymmetry would increase in the older age groups.
Methods
Participants
This research study was performed at Arcadia University, and all protocols were approved by the institutional review boards of all participating institutions. Written parental consent and child assent were obtained before the collection of any data. Study participants were recruited from local youth athletic leagues, private sports performance centers, and private baseball academies, and data collection occurred on site at the facilities. Demographic and sports participation data, including age, height, weight, sports participation history, position(s) played, injury history, current volume of sports activity, and arm dominance (defined as the arm used to throw a ball) were collected with a questionnaire filled out with the help of a parent/guardian. Years of playing experience was calculated by subtracting the age of onset of baseball playing from the current age of the player. All subjects were healthy males between the ages of 8 and 14 years who were currently competing in baseball or other sports activity. Subjects were categorized based upon sports participation (thrower vs nonthrower groups) and then further classified into age categories for a portion of the analysis. The nonthrower group was defined as players who participated in baseball less than 1 month per year, having not participated in any formal baseball activity for the 12 months prior to the study. Throwers were players who participated in baseball at least 6 months per year. Subjects were excluded if they participated in other repetitive overhead-throwing sports such as tennis, squash, or swimming, or if they had any existing shoulder condition that limited sports participation, any history of humeral fracture, or any known systemic disorder that may result in joint hypermobility (eg, Ehlers-Danlos syndrome).
Shoulder External and Internal ROM
Subjects were positioned supine on a portable treatment table with 90° of shoulder abduction and elbow flexion. A coin flip was used to randomly determine which side (left vs right) was assessed first. Shoulder internal rotation (IR) and external rotation (ER) were assessed utilizing a digital inclinometer (Model 40-6060; Johnson Level & Tool Manufacturing Co Inc) with previously described validated methods.6,14,31 Briefly, the scapula was stabilized and the shoulder passively rotated externally or internally until resistance was felt by the examiner and motion no longer occurred at the glenohumeral joint. A digital inclinometer was then firmly placed along the ulnar aspect of the forearm to determine the degree of rotation relative to vertical. This measurement has been shown to have high intra- and intertester reliability, with intraclass correlation coefficient (ICC) values of >0.90 and a standard error of measurement (SEM) of 1.5° to 2.6°.6,11,15
Humeral Retrotorsion
HRT was assessed using indirect ultrasonographic techniques described and validated by Myers et al. 13 Briefly, the subjects remained supine with the shoulder abducted to 90° and the elbow flexed to 90°. A 5- to 13-MHz linear array ultrasound transducer (GE LOGIQe; General Electric) was placed on the anterior aspect of the shoulder perpendicular to the long axis of the humerus and aligned level to the treatment table with a bubble level. A second examiner then rotated the humerus so that the bicipital groove could be visualized directly with the apexes of the greater and lesser tubercles parallel to the horizontal plane (Figure 1). This examiner then placed a digital inclinometer firmly against the ulna, and the forearm inclination angle relative to horizontal was recorded. By standardizing the alignment of the proximal humerus and taking advantage of the consistent perpendicular arrangement of the ulnar to the transepicondylar axis, this measurement procedure represents the relative difference between the proximal segment (humeral head) and distal segment (epicondylar axis), thus giving an indirect measurement of the degree of longitudinal twisting within the humerus (HRT). The examiners underwent specific training for this measurement, and an independent reliability study conducted by the examiner team yielded ICCs of 0.91 to 0.98 and an SEM of 1.8°, which is consistent with other reliability studies using this technique. 1
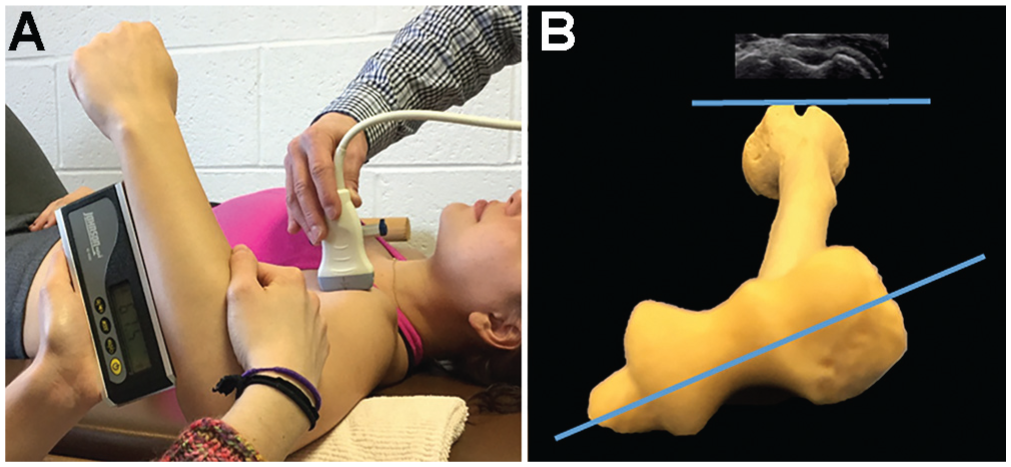
Humeral retrotorsion assessment. (A) The apexes of the greater and lesser tuberosities were identified utilizing ultrasound and aligned horizontally. (B) Measurement of the angle of the ulna relative to horizontal was taken, representing the difference in alignment between the humeral head and transepicondylar axis (degree of humeral retrotorsion).
Variables for Data Analysis
Consistent with previous literature, 6 the average of 3 trials was utilized for HRT, and an average of 2 trials was used for ROM analysis. Shoulder total range of motion (TROM) was calculated by adding ER and IR values. Glenohumeral internal rotation difference (GIRD), glenohumeral external rotation difference (GERD), and difference in TROM (dTROM) were calculated as the dominant side value minus the nondominant. Side-to-side difference in humeral retrotorsion (dHRT) was calculated as the dominant minus the nondominant side.
Statistical Analysis
All statistical analyses were conducted using SPSS (version 22.0; IBM Corp). A 2-way analysis of variance was performed, with throwing status (yes/no) and age (young: 8-10.5 years; preteen: 10.5-12.5 years; early teen: 12.5-14.9 years) as the primary factors. Dependent variables were side-to-side differences in HRT and shoulder ER, IR, and TROM. Interactions between age and throwing status were assessed followed by determination of main effects, utilizing Bonferroni post hoc procedures as appropriate. Paired-samples t tests were utilized to evaluate differences in HRT, ER, and IR ROM between limbs for each age group. In addition, a correlational analysis using Pearson correlation coefficients was performed to assess the relationship between HRT and ER/IR ROM. In all analyses, an α of 0.05 was used for statistical significance.
Results
A total of 153 subjects were included in the study. The subjects were divided into 2 groups based upon sports activity: throwers (n = 85) and nonthrowers (n = 68). There were no significant differences between thrower and nonthrower groups for age, height, or weight (Table 1), and participants demonstrated equivalent sports participation volumes (Table 2). All throwers began playing baseball between 4 and 6 years of age and had a minimum of 5.2 years of experience playing baseball.
Demographics of Study Participants a
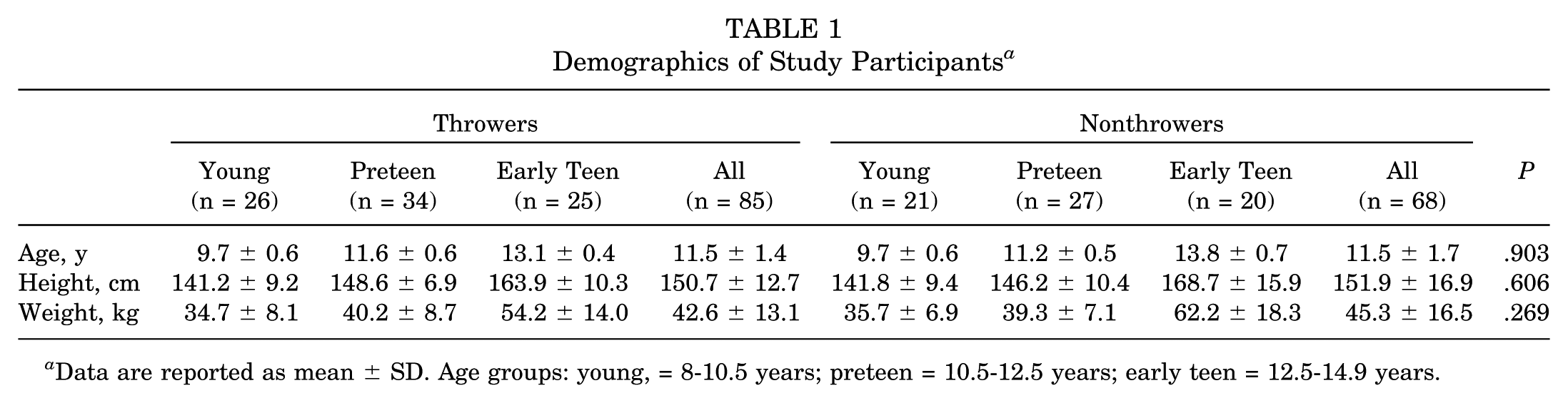
Data are reported as mean ± SD. Age groups: young, = 8-10.5 years; preteen = 10.5-12.5 years; early teen = 12.5-14.9 years.
Sports Participation by Age Group a
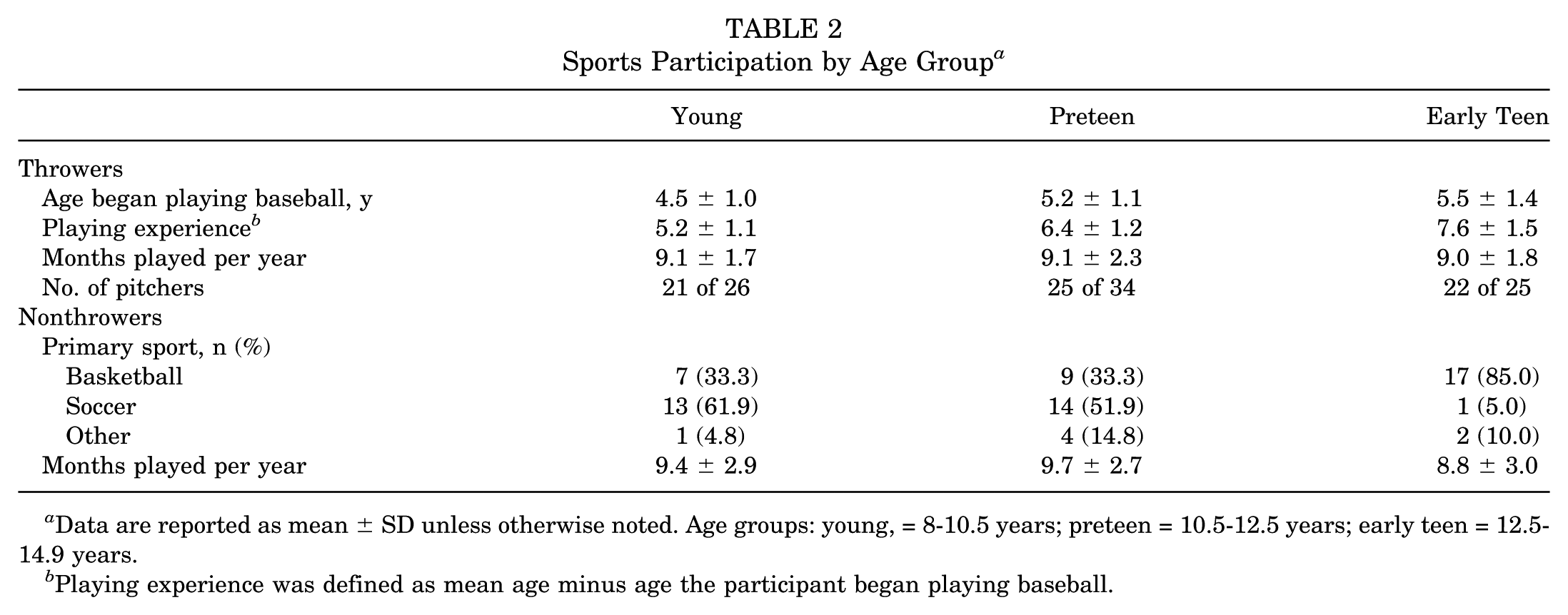
Data are reported as mean ± SD unless otherwise noted. Age groups: young, = 8-10.5 years; preteen = 10.5-12.5 years; early teen = 12.5-14.9 years.
Playing experience was defined as mean age minus age the participant began playing baseball.
The mean values for HRT, ER, IR, and TROM between the dominant and nondominant side in both groups are presented in Table 3. There was no interaction between factors. The thrower group showed increased asymmetry in HRT (8.7° vs 4.8°), with the dominant side having more retrotorsion. The throwing athletes also demonstrated greater GERD (5.2° vs 1.8°), indicating greater dominant-side ER, as well as GIRD (–6.0° vs −2.7°), indicating less dominant-side IR than nonthrowing athletes (Figure 2).
Humeral Retrotorsion and Ranges of Motion (in Degrees) by Study Group a
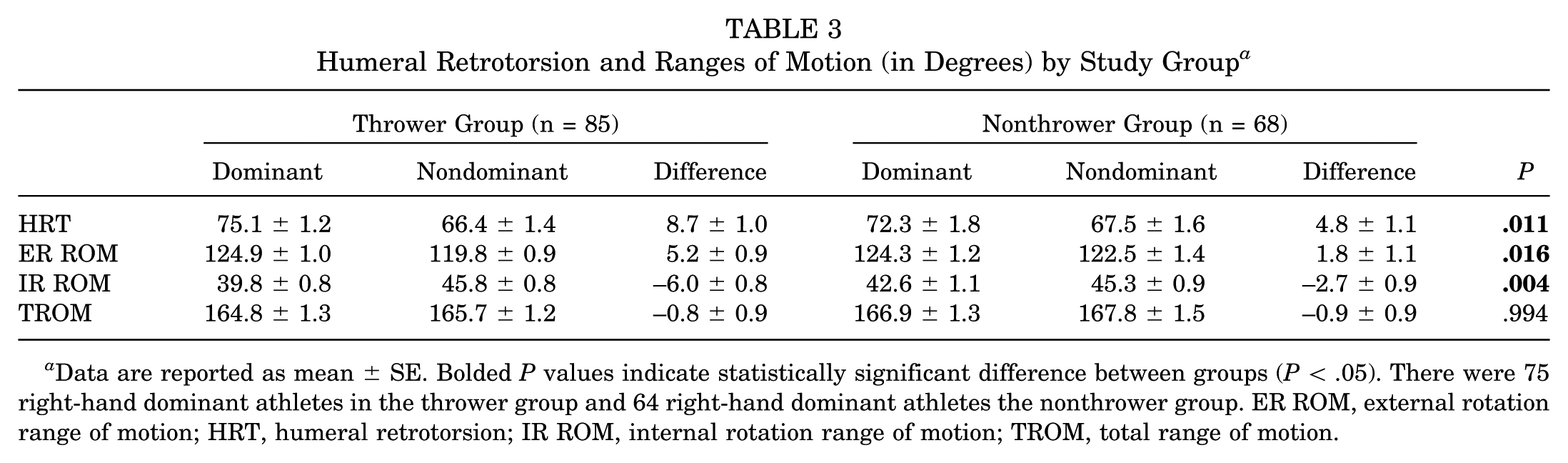
Data are reported as mean ± SE. Bolded P values indicate statistically significant difference between groups (P < .05). There were 75 right-hand dominant athletes in the thrower group and 64 right-hand dominant athletes the nonthrower group. ER ROM, external rotation range of motion; HRT, humeral retrotorsion; IR ROM, internal rotation range of motion; TROM, total range of motion.
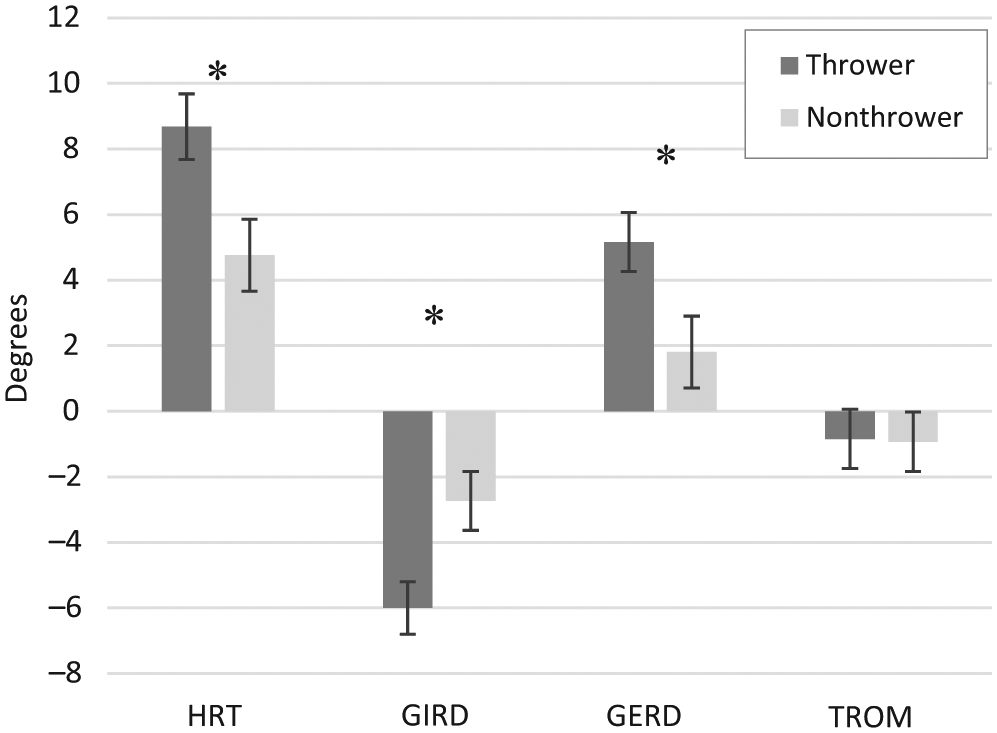
Side-to-side asymmetry by throwing group generally demonstrating greater asymmetry in throwers, with no differences in total range of motion (TROM). *Statistically significant difference between groups (P < .05). GERD, glenohumeral external rotation difference; GIRD, glenohumeral internal rotation difference; HRT, humeral retrotorsion.
Analysis of the main effect of age demonstrated significant differences for dHRT and GIRD. Post hoc testing for dHRT revealed significant differences between the young and early teen groups (3.9° vs 8.8°). Significant differences for GIRD existed between the young and early teen groups (–3.6° vs −7.2°) and preteen and early teen groups (−3.3° vs −7.2°). There were no significant differences seen between age groups for GERD or dTROM (Figure 3).
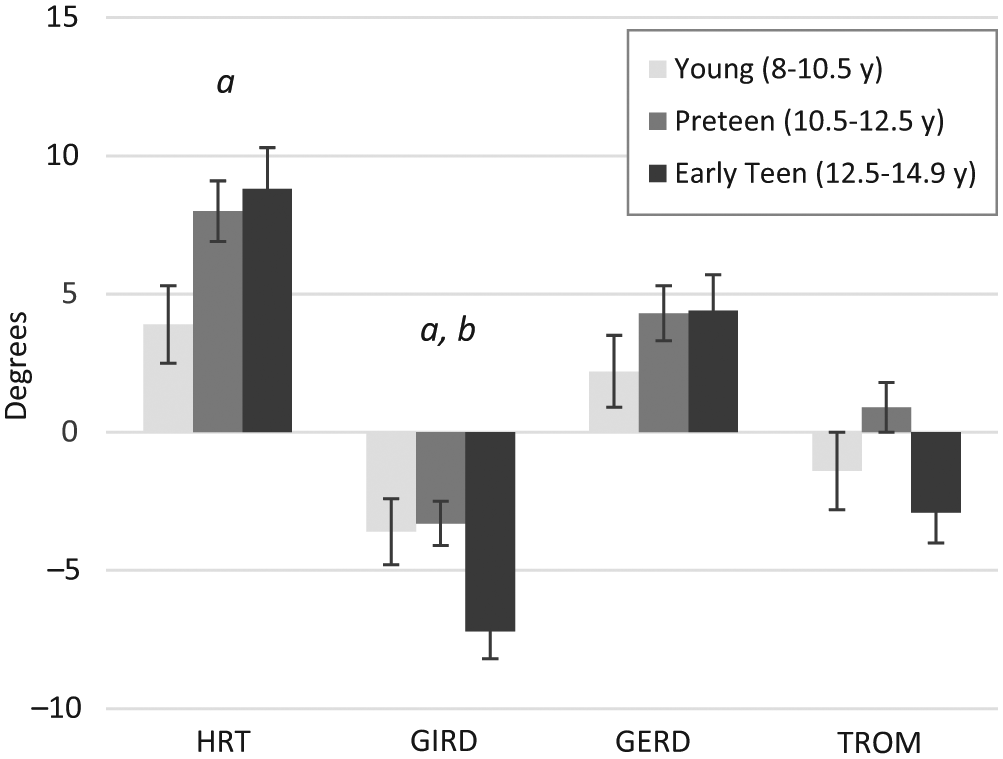
Side-to-side asymmetry by age group demonstrating statistically significant differences between the a young and early teen groups and the b preteen and early teen groups (P < .05). GERD, glenohumeral external rotation difference; GIRD, glenohumeral internal rotation difference; HRT, humeral retrotorsion; TROM, total range of motion.
Paired-samples t tests within the thrower group revealed significant differences (P < .05) between dominant and nondominant limbs in every age group for HRT, GERD, and GIRD. Within the nonthrowers, there was a significant difference in HRT in both the preteen and early teen groups, and a significant difference in GIRD in the early teen group; there were no significant differences seen in any age groups for GERD (Figure 4). Assessment of group differences between pitchers and position players was not possible because of the young age of our sample and because most players played multiple positions.
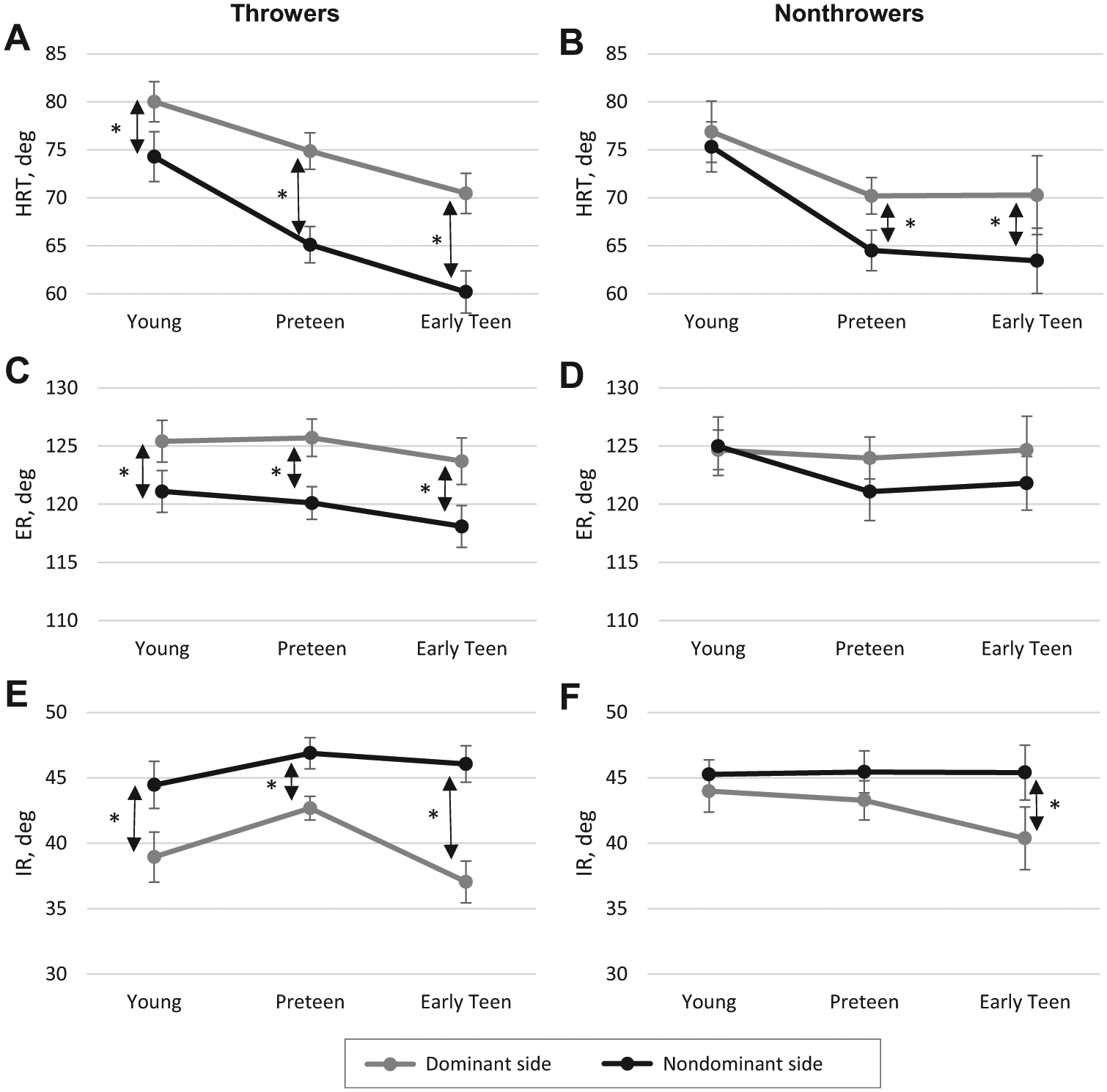
Side-to-side comparison within age and activity groups. *Statistically significant differences between dominant and nondominant sides within the indicated age groups for humeral retrotorsion in (A) throwers and (B) nonthrowers, shoulder external rotation in (C) throwers and (D) nonthrowers, and shoulder internal rotation in (E) throwers and (F) nonthrowers (P < .05, paired samples t test). ER, external rotation; HRT, humeral retrotorsion; IR, internal rotation.
Correlation analysis demonstrated significant (P < .05) weak to moderate relationships within the dominant shoulder of both throwers and nonthrowers for HRT and shoulder ROM. A positive correlation existed between HRT and ER ROM that was stronger in nonthrowers (r = 0.63) than for throwers (r = 0.23), while a negative correlation existed with IR that was stronger in throwers (r = −0.40) than in nonthrowers (r = −0.27) (Figure 5).
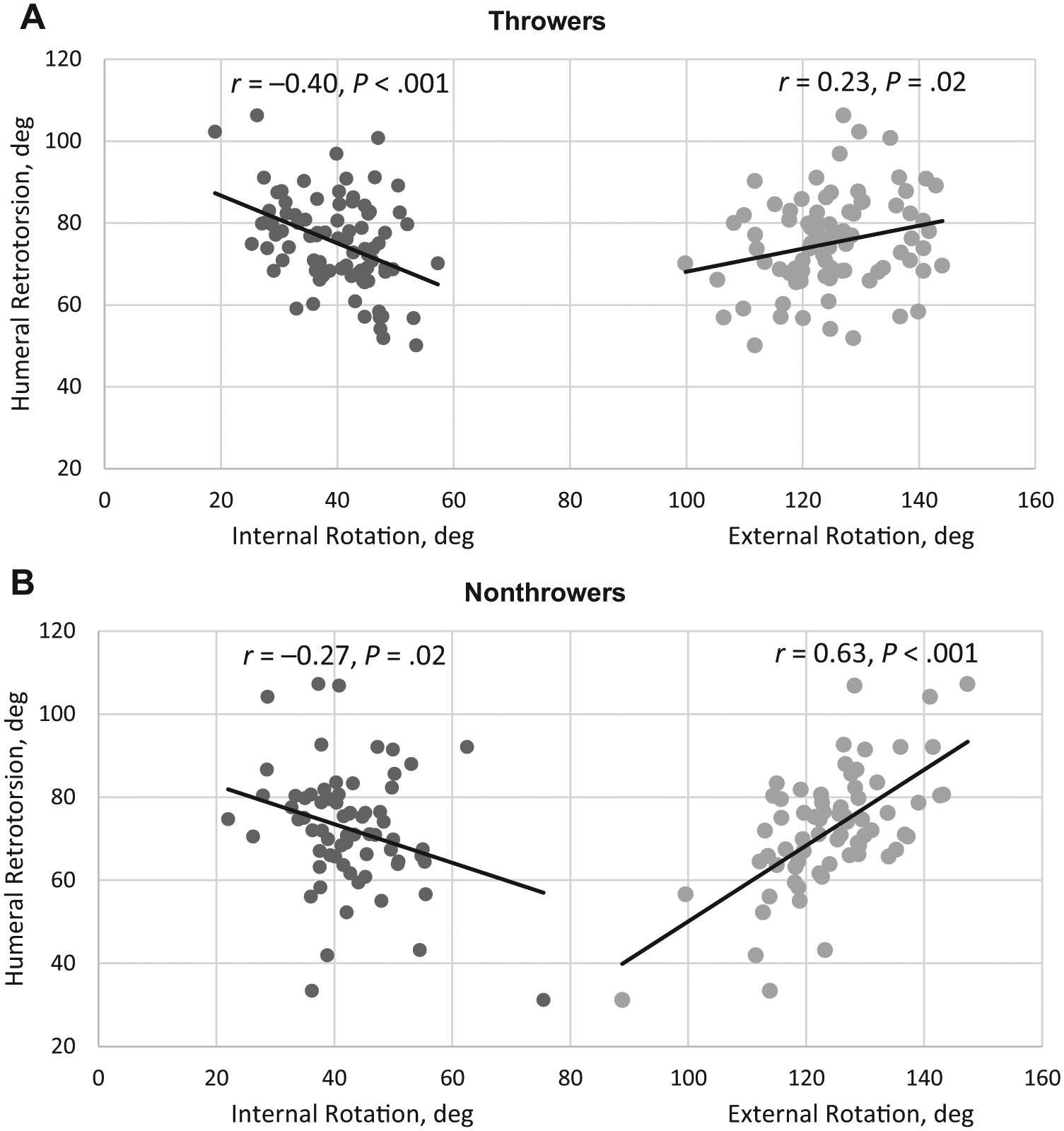
Scatter plot of relationship between dominant arm humeral retrotorsion and shoulder motion in (A) throwers and (B) nonthrowers. Overall correlations were weak to moderate, with a stronger relationship existing for external rotation in the nonthrower group.
Discussion
Our results show that youth baseball players who play more than 1 season per year demonstrate alterations in HRT and shoulder ROM at an earlier age and to a greater magnitude compared with young athletes who do not participate in baseball. Although other investigators have determined that youth baseball players demonstrate increased HRT within the dominant arm, resulting in a larger side-to-side asymmetry,6,27-29,33,34 none of these studies have included a control group. Typically, the nondominant arm is utilized as the control because this arm is not subjected to the stimulus of throwing, so it is believed to represent the subject’s baseline potential for overall HRT.6,27,33,34 However, without the presence of a true control group, researchers are unable to account for genetic predisposition of HRT levels or for the effects of physiological maturation and arm dominance. For example, if increased HRT in the dominant arm is advantageous to throwing athletes, there could be a tendency for those with higher retrotorsion to gravitate toward throwing activity,10,29 which would confound these results. To our knowledge, this is the first study to directly compare throwing athletes to a control group of age-matched nonthrowing athletes.
Our results indicate that the activity of throwing does significantly affect side-to-side bony changes in HRT and that these changes begin at an early age. Because we found differences in even our youngest group (8- to 10.5-year-olds), these changes likely occur before the age of 8 years. Prior studies report conflicting results regarding when these adaptations occur. Whiteley et al 28 found significant side-to-side asymmetry present in a group of adolescent baseball players at a mean age of 16.6 years. Yamamoto et al 34 performed a cross-sectional study within youth baseball players aged 9 to 14 years (N = 66) and found that side-to-side differences in HRT were only significant in a single group of fifth graders (usually about 10-11 years old, but this was not reported) but not in groups older or younger. In a similar study of 9- to 17-year-old baseball players, Yamamoto et al 33 found that side-to-side asymmetry in HRT did not become significant until 11 to 12 years of age. These results differ from those of the current study and those of Hibberd et al, 6 where significant side-to-side differences in HRT were observed much earlier (at ages 9.7 and 8.3 years, respectively). Differences in study populations may account for the observed variation in onset of HRT asymmetry. The baseball players involved in the current study consisted of players who participated in baseball a mean of 9.1 months per year. In addition, we had a high volume of pitchers (66 of 85 subjects), of whom 75% (51 of 68) began pitching when they were 8 years or younger.
Our results demonstrate that by a mean age of 11.5 years, baseball players also had an altered arc of overall ROM in the dominant shoulder, with a gain of ER (5.2°) and loss of IR (6.0°). However, we found no asymmetry in TROM. It has been suggested that the increased HRT may account for this shift in the overall ROM arc.14,17,21 While our overall population based analysis may seem to suggest that the bony adaptations could account for the shift in overall shoulder ROM, individual correlation analysis does not support this conclusion. The low correlation between shoulder ER and IR motion and HRT (r = 0.23 and −0.40, respectively) indicates that the bony changes in HRT do not exert a strong influence on overall shoulder rotation ROM within the dominant arm of throwing athletes. Thus, while the bony adaptations may influence the overall shoulder ROM, they do not fully account for the changes in TROM observed in the dominant shoulder of young throwers. These results are similar to those reported by Yamamoto et al, 34 who noted very weak and nonsignificant correlations for both ER (r = −0.043; P = .733) and IR (r = 0.193; P = .119) with HRT in a group of young baseball players with a mean age of 12 years. However, Hibberd et al 6 used retrotorsion-adjusted IR measurements and reached a different conclusion. Adjusting IR measurements based on HRT has been suggested as a way to isolate soft tissue contributions to changes in IR.6,14,18 However, the validity of this methodology has recently been questioned, as analysis of the relationship between HRT and ROM does not support the notion that 1° of HRT change relates to 1° of ROM change. 16 Hibberd et al 6 did not perform a direct correlational analysis, instead utilizing this retrotorsion-adjusted IR to analyze the relationship of HRT to shoulder IR loss in youth baseball players (aged 6-18 years), and concluded that HRT solely accounted for the observed loss of internal rotation within their sample. The low correlations between HRT and IR among our sample and that of Yamamoto et al 34 support the criticism of an absolute 1:1 correction and argue for an additional soft tissue component, such as posterior capsular tightness or loss of musculotendinous flexibility of the rotator cuff or other posterior shoulder muscles, contributing to the overall motion changes seen in some youth athletes. Our understanding of the relative contribution of bone and soft tissue effects on shoulder ROM is important, as other studies have identified a loss of shoulder motion is a risk factor for upper extremity injury.24,25,30 A decrease in musculotendinous or capsular flexibility can be addressed through rehabilitation measures, while an alteration of bony alignment cannot.
The timing of sports participation during growth and development and its influence on bony and soft tissue changes is important to understand. The proximal humeral derotation process happens most rapidly from ages 0 through 8 years, and the forces created while throwing act to slow down this process, leading to a larger degree of HRT within the dominant arm.5,23 Throwing at an early age exposes the proximal humerus to these remodeling forces during the period of most rapid derotation, and thus early pitching may allow for more pronounced effect on dominant humeral HRT and may facilitate a higher degree of asymmetry within these players. The fact that most of our throwers began playing baseball at age 4 to 5 years and began pitching at age 7 to 8 years may explain why our sample demonstrated more significant side-to-side asymmetry in HRT when compared with other studies of similar age athletes.33,34 Additionally, it has been suggested there may be a window of opportunity before skeletal maturity to develop an HRT adaptation that lies within a “sweet spot,” in which an ideal degree of HRT is protective against injury.4,20 It is possible that a high volume of throwing during these younger years of high susceptibility to HRT remodeling may give rise to HRT that is outside of the ideal sweet spot, leaving such athletes more susceptible to injury as adults.15,16 Our understanding of how throwing activity during childhood determines one’s adult retrotorsion asymmetry is critical, as researchers have identified an association between increased HRT and the development of elbow pain and pathological GIRD in adult pitchers.15,16,26 Further research is necessary to help identify how age of initiation of pitching and volume of pitching while skeletally immature may affect the development of HRT.
There are limitations within the current study. Because of the popularity of baseball, it was difficult to find youth athletes who had never participated in any baseball. Thus, our nonthrower group does not represent a true control group, as there were some children (n = 33) who had some history of baseball participation. However, more than half (n = 35) of our nonthrowers did not have any history of playing baseball. Interestingly, when we analyzed these subjects separately, we found that the group with some baseball exposure did have a higher asymmetry in HRT than those who never played any baseball (5.9° vs 3.6°). Therefore, this recruiting limitation actually reinforces our conclusions with the notion that even limited exposure to throwing stimuli can alter HRT development. In addition, there was no standardized warm-up before ROM assessment. This may have affected our shoulder rotation measurements, however, all data were obtained during active practice or tournament scenarios. All subjects had undergone a team-specific warm-up or were actively engaged in sports activity at the time of measurement. Therefore, we believe that there was likely proportionate tissue preconditioning across all measurements, limiting the effect of this factor. Another limitation is that there was no direct measure of physiological maturity. We grouped our subjects by chronological age, which may not have directly related to their degree of skeletal maturity because of differences in physiological maturation. As normal proximal humeral torsion development occurs as a result of bony maturation, this limitation may have affected our HRT measurements and may account for some of the variability in our results. Future studies should consider the use of more precise measures of physiological maturity (Tanner staging or skeletal age via plain radiographs) to more precisely define skeletal maturity.
In summary, our results clearly illustrate that throwing activity is associated with adaptive changes in HRT and shoulder ROM in children at a very young age. Throwing is associated with greater HRT, greater ER, and decreased IR on the dominant side. The relationship between changes in bony torsion and shoulder ROM in immature throwers is complex. Although the bony adaptations in HRT do influence overall shoulder rotation ROM to some degree, weak correlation in these changes indicates that soft tissue structures likely play a significant role within this population as well. Because loss of motion is a risk factor for injury in throwing athletes,2,12,25,30 understanding what elements contribute to this loss of motion is critical for directing appropriate treatment to prevent problems. Our findings suggest that soft tissue adaptations are present within youth pitchers, which may be able to be addressed through interventions such as stretching or manual therapy. This may have implications for maintaining the health of young pitchers. Further research is needed to expand our understanding of shoulder motion changes within the youth throwing athlete and to identify the age and volume of play that affect the changes in shoulder motion seen here.
Footnotes
Acknowledgements
The authors thank Kshamata Shah, Casey McKenna, Marcus Rowan, and Charles Kim for their assistance with various aspects of this project.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by The Legacy Fund Grant, administered by the Sports Section of the American Physical Therapy Association. E.M.G. receives payment for lectures, including service on speakers bureaus for the Professional Therapy Seminars Pediatric Sports Rehabilitation Course. J.T.R.L. received royalties from Sawbones Inc. P.M. has grants/grants pending from the National Institutes of Health and receives payment for lectures, including service on speakers bureaus for Rehab Education.