
Abstract
Background:
A capsular tear and humeral avulsion of the glenohumeral ligament lesion are not uncommon findings in association with a Bankart lesion. However, there have been few reports regarding the prevalence of such capsular lesions and the postoperative recurrence after capsular repair.
Purpose/Hypothesis:
This study investigated the prevalence of capsular lesions and clarified their influence on the postoperative recurrence of instability. In addition, factors were identified that were associated with the occurrence of capsular lesions and the postoperative recurrence of instability. We hypothesized that clinical outcomes would be improved by combining arthroscopic Bankart repair with simultaneous capsular repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Capsular lesions were retrospectively examined through operative records, still pictures, and videos in 172 shoulders with traumatic anterior instability. First, the prevalence of capsular lesions and their severity were investigated. Then, postoperative recurrence was determined in shoulders observed for a minimum of 2 years. Finally, factors were assessed that were associated with the occurrence of capsular lesions and the postoperative recurrence of instability.
Results:
A capsular lesion was recognized in 37 shoulders (21.5%), being severe and mild in 20 and 17, respectively. All were repaired simultaneously with the arthroscopic Bankart procedure. After follow-up for at least 2 years, recurrence of instability was detected in 10 of 34 shoulders (29.4%), including 6 (31.6%) with severe capsular lesions and 4 (26.7%) with mild lesions. The recurrence rate was significantly higher in shoulders with a capsular lesion than in shoulders without a capsular lesion (18 of 120, 15%; P = .013), but there was no significant difference between severe and mild lesions. Regardless of the sport played, capsular lesions were significantly more frequent in patients ≥30 years old, patients with complete dislocation, and patients with a coexisting Hill-Sachs lesion. Postoperative recurrence of instability was significantly more frequent in patients <30 years and competitive athletes.
Conclusion:
In shoulders undergoing arthroscopic Bankart repair, capsular lesions were often present and were associated with higher postoperative recurrence of instability. While these lesions were more frequent in older patients, postoperative recurrence of instability was more likely in young competitive athletes.
Keywords
For patients with traumatic anterior shoulder instability, a Bankart lesion is usually regarded as the main injury, and Bankart repair is considered the gold standard of treatment. However, a coexisting capsular tear and humeral avulsion of the glenohumeral ligament (HAGL) lesion 9 are not uncommon among patients with a Bankart lesion. While injury to the capsule is often assumed to be present, especially in shoulders with acute instability, the reported prevalence of a capsular tear ranges widely— from 32% to 72% on arthrography and 0% to 100% at arthroscopy. 6 In Baker’s arthroscopic classification of acute dislocation, a capsular tear without a labral lesion is classified as group 1; a capsular tear with partial labral detachment, group 2; and a capsular tear combined with a labral tear, group 3. 1 The reported prevalence of each group is 13.3%, 24.4%, and 62.2%, respectively, 1 suggesting that a capsular tear is present in all shoulders with acute instability. However, most acute capsular tears are generally believed to heal spontaneously, and large tears are considered to be rare in shoulders with chronic instability, even though there may be some stretching or laxity of the anterior capsule. 6
However, Ogawa and Yoshida 6 reported that tears in the midportion of the anterior capsule were a major cause of recurrent dislocation in 5 shoulders, and Mizuno et al 3 reported that an isolated complete capsular tear was the main pathologic condition in 12 shoulders. According to these reports, an isolated capsular tear can be responsible for recurrent dislocation. In shoulders with both a capsular lesion and a Bankart lesion, there may be a high risk of postoperative recurrence if the capsular tear is ignored at the time of Bankart repair. However, there have been few reports regarding the prevalence of capsular lesions and outcomes after capsular repair. Accordingly, this study was performed to investigate the prevalence of capsular lesions, including HAGL lesions, at the time of arthroscopic surgery for traumatic anterior instability and to clarify the clinical outcome after arthroscopic Bankart repair combined with simultaneous repair of the capsular lesion. Factors associated with the occurrence of capsular lesions and factors associated with postoperative recurrence of shoulder instability were also investigated. We hypothesized that a good clinical outcome would be achieved by arthroscopic Bankart repair combined with simultaneous repair of a coexisting capsular lesion.
Methods
Patient Profiles
Institutional review board approval was obtained for this study, which was performed retrospectively with prospectively collected clinical data on capsular tears and HAGL lesions. Between January 2010 and March 2014, arthroscopic Bankart repair was performed at our hospital for 163 patients (172 shoulders) with traumatic anterior shoulder instability, excluding patients with recurrent instability after previous anterior stabilization surgery (12 shoulders) and patients receiving the open Bristow procedure combined with arthroscopic Bankart repair (3 shoulders). The profile of the patients is shown in Table 1.
Shoulder Profiles a
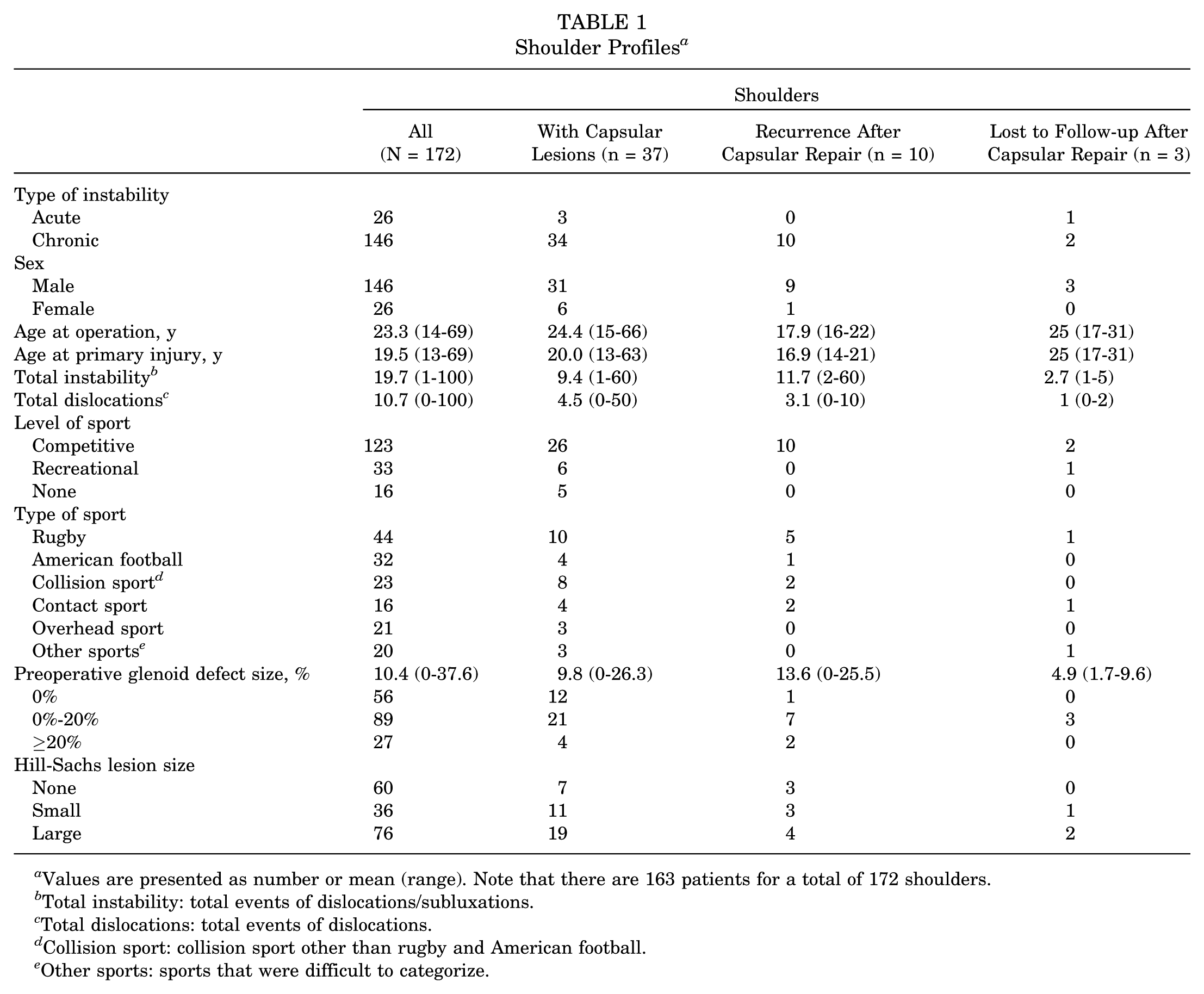
Values are presented as number or mean (range). Note that there are 163 patients for a total of 172 shoulders.
Total instability: total events of dislocations/subluxations.
Total dislocations: total events of dislocations.
Collision sport: collision sport other than rugby and American football.
Other sports: sports that were difficult to categorize.
Surgical Technique and Postoperative Rehabilitation
All operations were performed in a lateral decubitus position by a single surgeon. A capsular tear was diagnosed by arthroscopic examination if a defect of the capsular fibers was observed and the muscle belly of subscapularis was seen in the defect. Scar tissue at the defect was resected, and the capsular tissue was refreshed. Capsular tears located far from the Bankart lesion were repaired by side-to-side sutures (Figure 1). First, a shuttle relay suture (2-0 Prolene; Ethicon) was passed with a suture hook (Linvatec), after which the relay suture was replaced by a No. 2 strong suture (Ultrabraid; Smith & Nephew), and this procedure was repeated until the muscle belly of subscapularis could no longer be seen. Complete repair of the capsular tears was achieved with 2 to 4 strong sutures at 3- to 4-mm intervals. Then the anteroinferior glenohumeral ligament–labral complex was detached and mobilized from the glenoid neck (preparation of the Bankart space) and arthroscopic Bankart repair was performed with 4 to 7 single-loaded suture anchors. However, capsular tears located close to the Bankart lesion were not repaired individually (Figure 2). After preparation of the Bankart space, the capsular tear was repaired simultaneously with Bankart repair, with 4 to 7 single-loaded suture anchors. Some capsular tears were distant from the anterior glenoid rim at the caudal part, while the cranial part of the tear approached the anterior rim (Figure 3). For such tears, the caudal part was repaired first with side-to-side sutures; then, the cranial part was repaired simultaneously with the Bankart lesion after preparation of the Bankart space. If the patient had a HAGL lesion, the capsular attachment of the humeral head was refreshed, and the lesion was repaired with 2 or 3 single-loaded suture anchors, after which the Bankart space was prepared and arthroscopic Bankart repair performed. Additional reinforcement procedures, such as rotator interval closure or remplissage, were not performed in any of the shoulders, even for shoulders with a large glenoid defect or a large Hill-Sachs lesion.
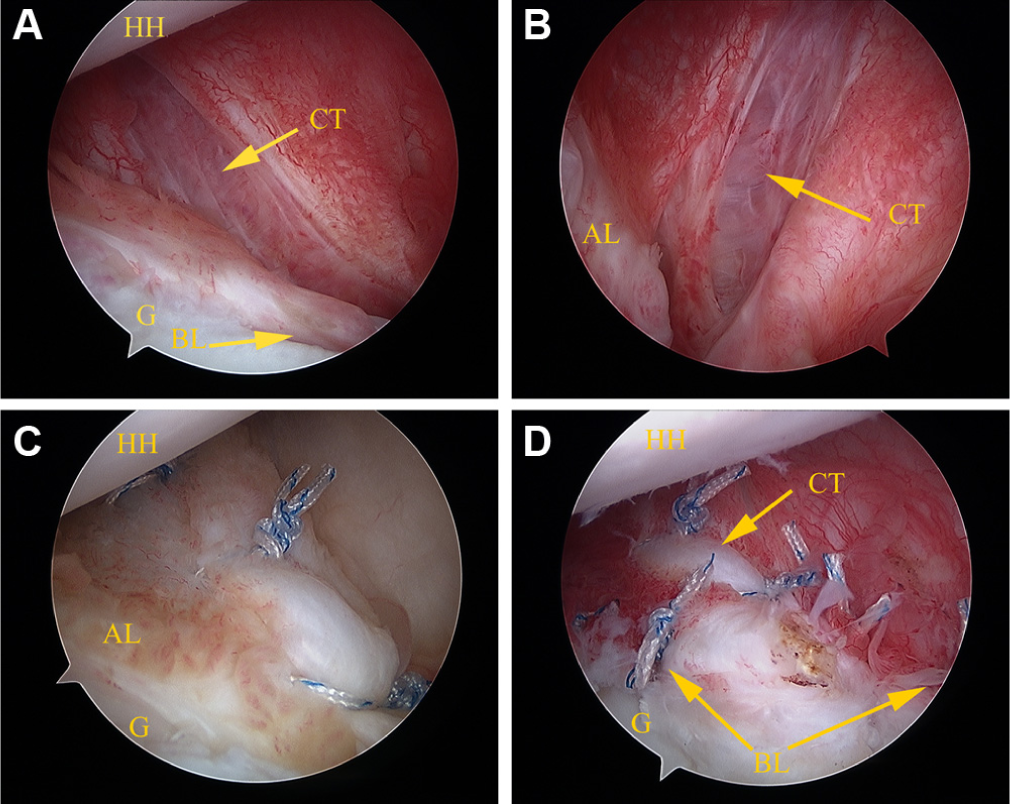
A capsular tear in the midportion of anterior capsule (15-year-old male rugby player, left shoulder). A capsular tear viewed from (A) the posterior portal and (B) the anterior portal. A severe capsular tear located far from the Bankart lesion was recognized in the midportion of anterior capsule. A defect of the capsular fibers was observed, and the muscle belly of subscapularis was seen in the defect. (C) The repaired capsule viewed from the posterior portal. The capsular tear was managed by side-to-side repair with No. 2 strong sutures. The muscle belly of subscapularis could no longer be seen. (D) The repaired capsular lesion and Bankart lesion viewed from posterior portal. After complete repair of the capsular tear, arthroscopic Bankart repair was performed individually with suture anchors. AL, anterior labrum; BL, Bankart lesion; CT, capsular tear; G, glenoid; HH, humeral head.
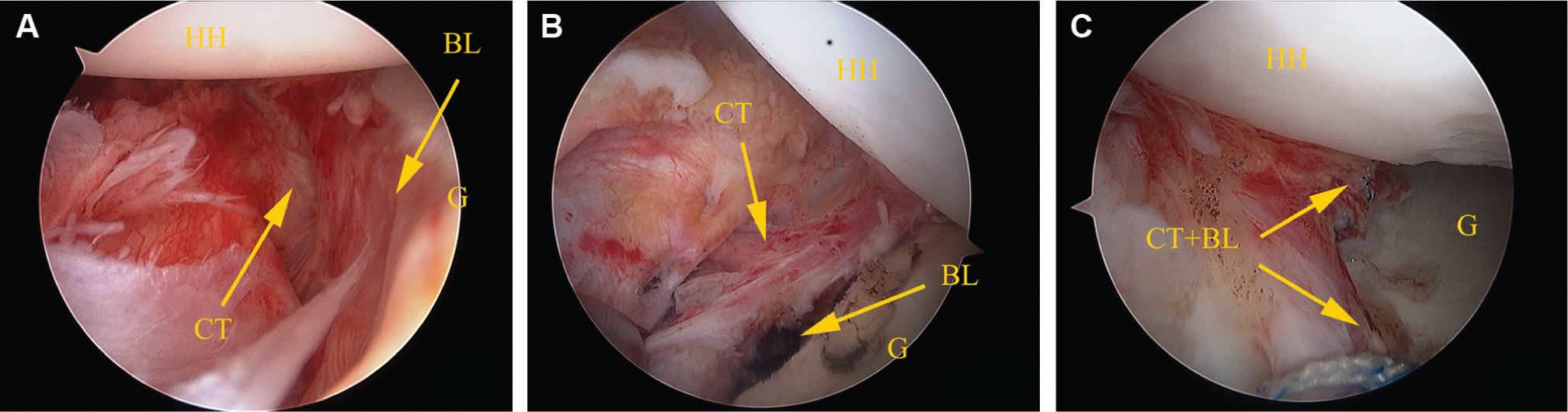
A capsular tear close to the Bankart lesion (16-year-old male wrestler, right shoulder). (A) A capsular tear viewed from the anterior portal. A severe capsular tear was recognized close to the Bankart lesion. (B) A capsular tear after preparation of the Bankart space viewed from posterior portal. A capsular tear located close to the Bankart lesion was not repaired individually. First, the anteroinferior glenohumeral ligament–labral complex was detached and mobilized from the glenoid neck. A capsular tear was located almost parallel to the prepared the Bankart space. (C) Simultaneously repaired capsular tear and Bankart lesion viewed from the anterior portal. The capsular tear and the Bankart lesion were repaired simultaneously with sutures from suture anchors. BL, Bankart lesion; CT, capsular tear; G, glenoid; HH, humeral head.
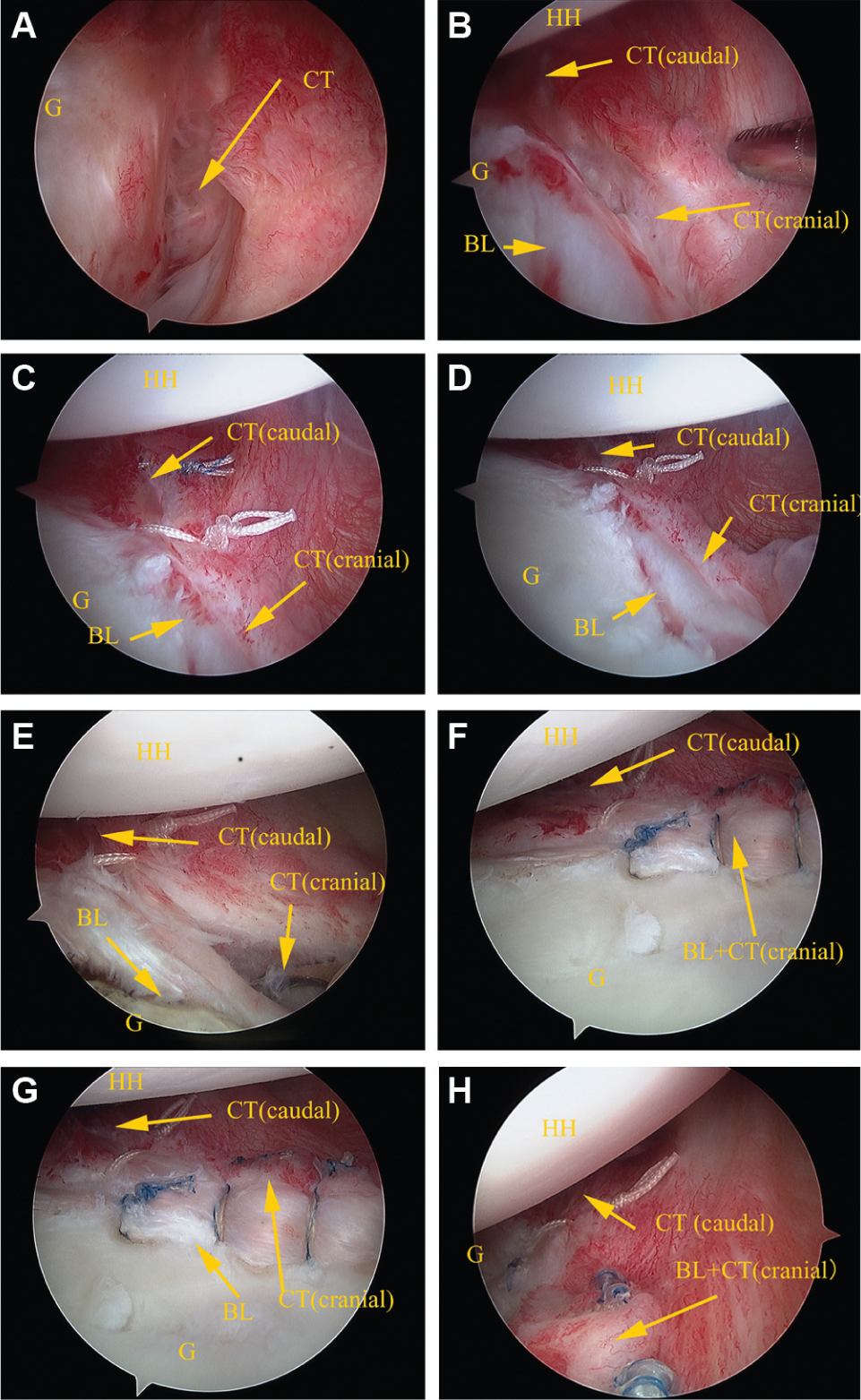
A capsular tear located distant from the anterior glenoid rim at the caudal part and close to the Bankart lesion at the cranial part (17-year-old male American football player, left shoulder). (A, B) A capsular tear viewed from the anterior portal. A severe capsular tear was distant from the anterior glenoid rim at the caudal part, while the cranial part of the tear approached to the anterior rim. (C, D) The repaired capsule at the caudal part, viewed from the anterior portal. The caudal part was repaired first with side-to-side sutures. The unrepaired cranial part of the capsule was located parallel to the Bankart lesion. (E) Preparation of the Bankart space after capsular repair of the caudal part, viewed from the posterior portal. The Bankart space was prepared after capsular repair of the caudal part. (F, G) The repaired capsular tear at the cranial portion and Bankart lesion, viewed from the posterior portal. (H) The repaired capsular tear at the cranial part and Bankart lesion, viewed from the anterior portal. The capsular tear at the cranial part and the Bankart lesion were repaired simultaneously with sutures from suture anchors. BL, Bankart lesion; CT, capsular tear; G, glenoid; HH, humeral head.
Patients wore a brace (allowing internal rotation toward the stomach) for 4 weeks postoperatively and started passive range of motion exercises after 2 weeks, similar to management after arthroscopic repair of an isolated Bankart lesion. For athletes involved in collision/contact sports, return to contact training and competition was not permitted for at least 6 and 8 months after surgery, respectively.
Investigation and Analysis
First, the prevalence of capsular lesions was investigated along with their severity and location. With regard to severity, a capsular lesion that widely exposed the muscle belly of subscapularis at arthroscopy was defined as severe, and a tear that caused only discontinuity of the capsule was defined as mild. The clinical profile of patients with capsular lesions was also investigated in detail. Then, the postoperative recurrence of instability after repair of capsular lesions was assessed among patients followed for a minimum of 2 years. The apparent history of dislocation and subluxation was defined as the postoperative recurrence. Furthermore, the clinical profile of patients with postoperative recurrence of shoulder instability was determined in relation to the severity of capsular lesions and the number of sutures required for capsular repair. Finally, factors associated with the occurrence of capsular lesions and factors associated with the postoperative recurrence of shoulder instability were investigated. The following factors were investigated: the type of instability (acute/chronic), sex, age at primary injury and age at operation (10-19, 20-29, or ≥30 years), interval between primary injury and operation (<1, 1-5, or ≥5 years), total events of dislocations/subluxations (1-5, 6-10, or ≥11), total events of dislocations (0, 1, 2-5, or ≥6), level of sport (competitive, recreational, or none), type of sport (rugby, American football, other collision sport, contact sport, overhead sport, or other sports that were difficult to categorize), preoperative glenoid defect size (0%, 0%-20%, or ≥20%), and Hill-Sachs lesion size (none, small, or large). To quantify the glenoid defect, the inferior portion of the glenoid rim was approximated to a true circle on en face 3-dimensional computed tomography scans reconstructed with elimination of the head of the humerus, and the extent of the defect was calculated as a percentage of the glenoid rim length. Hill-Sachs lesions were classified according to the arthroscopic criteria of Calandra et al 2 : grade 0 (no lesion) and grade 1 (defect of the articular surface not involving the subchondral bone) were defined as no lesion; grade 2 (small defect revealing ≤1 cm of subchondral bone), a small lesion; and grade 3 (large defect revealing >1 cm of subchondral bone), a large lesion.
Statistical analysis was performed with the Fisher exact probability test, the unpaired Student t test, and 1-factor analysis of variance, as appropriate, and significance was accepted at P < .05 with sufficient statistical power.
Results
Prevalence of Capsular Lesions and Surgical Repair
A capsular tear was found in 35 shoulders and a HAGL lesion in 2 shoulders, so there was a coexisting capsular lesion in 21.5% of the shoulders, while there were no isolated capsular lesions. Regarding the severity of the capsular lesion, it was severe in 20 shoulders (including the 2 with HAGL lesions) and mild in 17 shoulders. The capsular tear was located close to the Bankart lesion in 18 shoulders and at the midportion of the capsule in 17, but 2 midportion capsular tears extended to near the humeral attachment. A detailed profile of the 37 patients (37 shoulders) with capsular lesions is shown in Table 1.
All capsular lesions recognized in the present study were repaired simultaneously with the arthroscopic Bankart procedure. Among the 18 severe capsular tears, 17 were managed by side-to-side repair with strong sutures, with 2 sutures being employed for 9 tears, 3 sutures for 2 tears, and 4 sutures for 6 tears (Figure 1). One severe capsular tear and all 17 mild tears were close to the Bankart lesion, so these tears were repaired simultaneously with Bankart repair with the sutures from the suture anchors (Figure 2). Moreover, the cranial parts of 5 severe capsular tears were repaired simultaneously with the Bankart lesion after side-to-side repair of the caudal parts (Figure 3, Table 2). Regarding the 2 HAGL lesions, arthroscopic repair was performed with 3 suture anchors in 1 shoulder, while open repair with 2 suture anchors was required in the other shoulder. Apart from this 1 shoulder with open HAGL repair, the other capsular lesions and all Bankart lesions were treated arthroscopically.
Number of Sutures Required for Capsular Repair vs Postoperative Recurrence of Instability
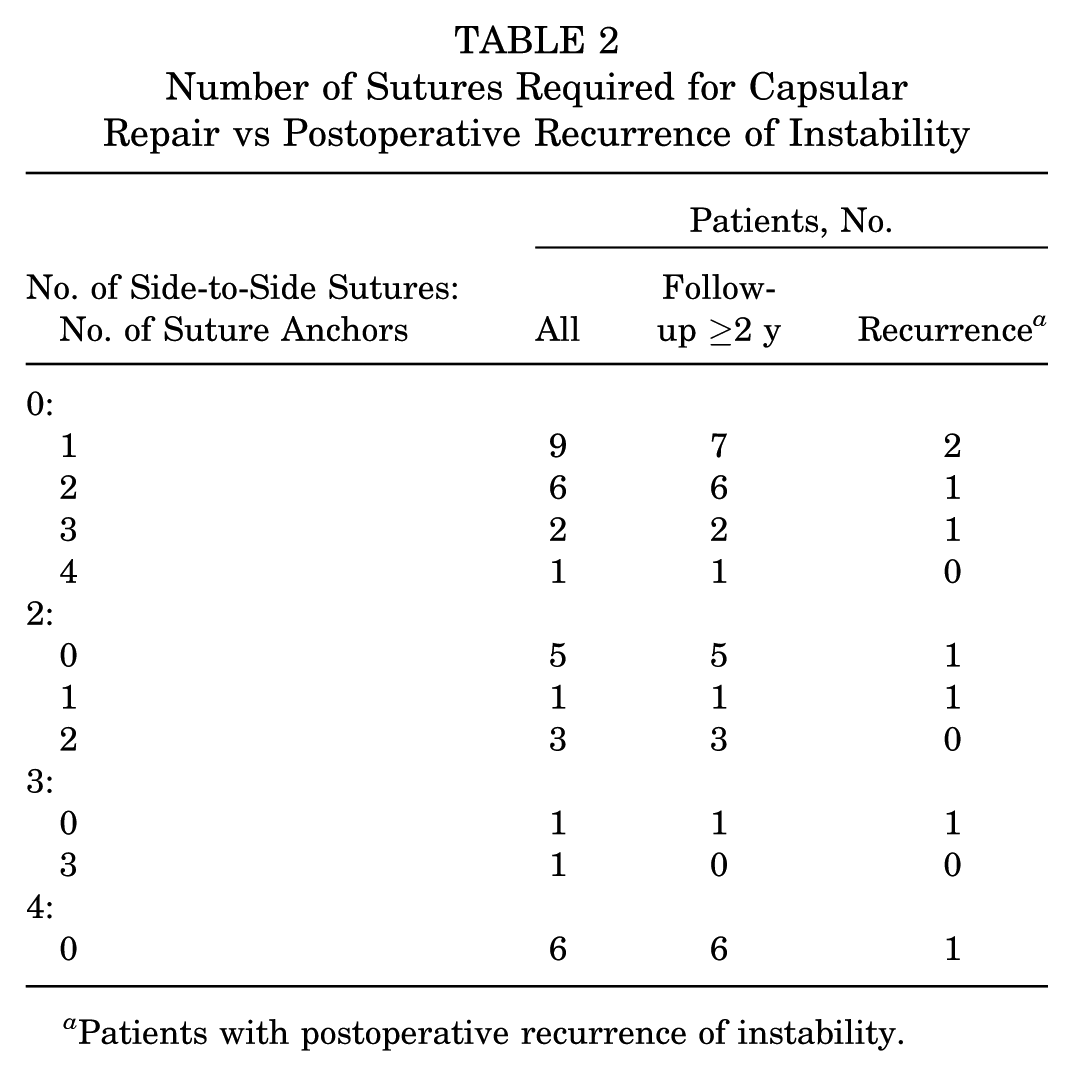
Patients with postoperative recurrence of instability.
Postoperative Recurrence of Instability
Data for at least 2 years of follow-up (mean: 27.6 ± 8.5 months, 24-67 months) were available for 154 of 172 shoulders that underwent arthroscopic Bankart repair with or without capsular repair (follow-up rate: 89.5%). Of 37 shoulders with capsular lesions, 34 were followed up for at least 2 years, and postoperative recurrence of instability occurred in 10 (29.4%). However, 120 of 135 shoulders without capsular lesions were followed up for at least 2 years, and postoperative recurrence of instability occurred in 18 (15%). Accordingly, the recurrence rate was significantly higher in shoulders with a capsular lesion (P = .013). Recurrence was detected in 6 of the 19 shoulders (31.6%) with severe capsular lesions, including 2 with associated HAGL lesions, and in 4 of the 15 shoulders (26.7%) with mild capsular lesions. There was no significant difference of recurrence between severe and mild capsular lesions.
There was no relationship between postoperative recurrence of instability and the number of strong sutures and suture anchors used, as shown in Table 2. When the influence of the total number of sutures required for repair of capsular tears was investigated by combining side-to-side sutures and sutures from suture anchors, recurrence was found in 2 of 7 shoulders (28.6%) with 1 suture, 2 of 11 (18.2%) with 2 sutures, 3 of 4 (75%) with 3 sutures, and 1 of 10 (10%) with 4 sutures. There was no relationship between the number of sutures and the recurrence rate.
All patients with recurrence of instability were young competitive athletes involved in collision/contact sports who had chronic instability (Table 1). Except for a 22-year-old footballer, these patients were teenagers. There was only 1 female patient, who was a judo athlete. One wrestler underwent reoperation at another hospital after recurrence of instability, and we could not obtain detailed information regarding the management of this patient. In the other 9 shoulders, the mean time of recurrence was 10.8 months postoperatively (range: 2-24 months). Recurrence was due to major trauma in only 2 shoulders (ie, trauma similar to that at primary instability), while moderate and minor trauma led to recurrence in 2 and 5 shoulders, respectively (ie, trauma that was a little weaker or much weaker for postoperative recurrence vs that at primary instability). Two patients experienced dislocation at the time of recurrence, but subluxation occurred in the other 7 patients.
Factors Associated With the Occurrence of Capsular Lesions and Postoperative Recurrence of Instability
Capsular lesions were significantly more frequent in patients ≥30 years old, patients with complete dislocation, and patients with a coexisting Hill-Sachs lesion (Table 3). However, capsular lesions occurred regardless of the level and type of sport and were even found in 5 of 16 shoulders (31.3%) among the patients not involved in sporting activity.
Factors Associated With the Occurrence of Capsular Lesions a
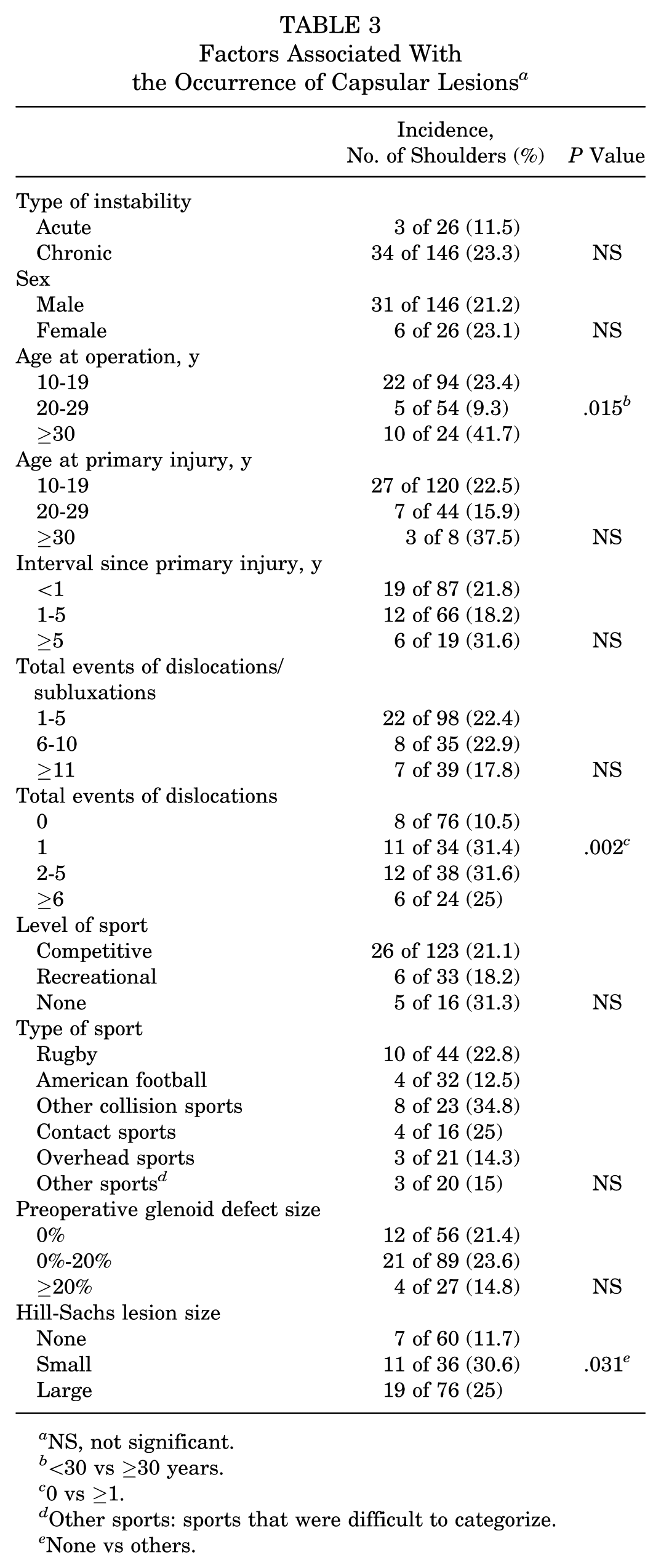
NS, not significant.
<30 vs ≥30 years.
0 vs ≥1.
Other sports: sports that were difficult to categorize.
None vs others.
Postoperative recurrence of instability was significantly more frequent in patients <30 years and in competitive athletes (Table 4). Among 15 collision athletes <20 years old, 7 athletes (46.6%) developed recurrence after arthroscopic repair (including 1 with open repair of a HAGL legion).
Factors Associated With Postoperative Recurrence of Instability a
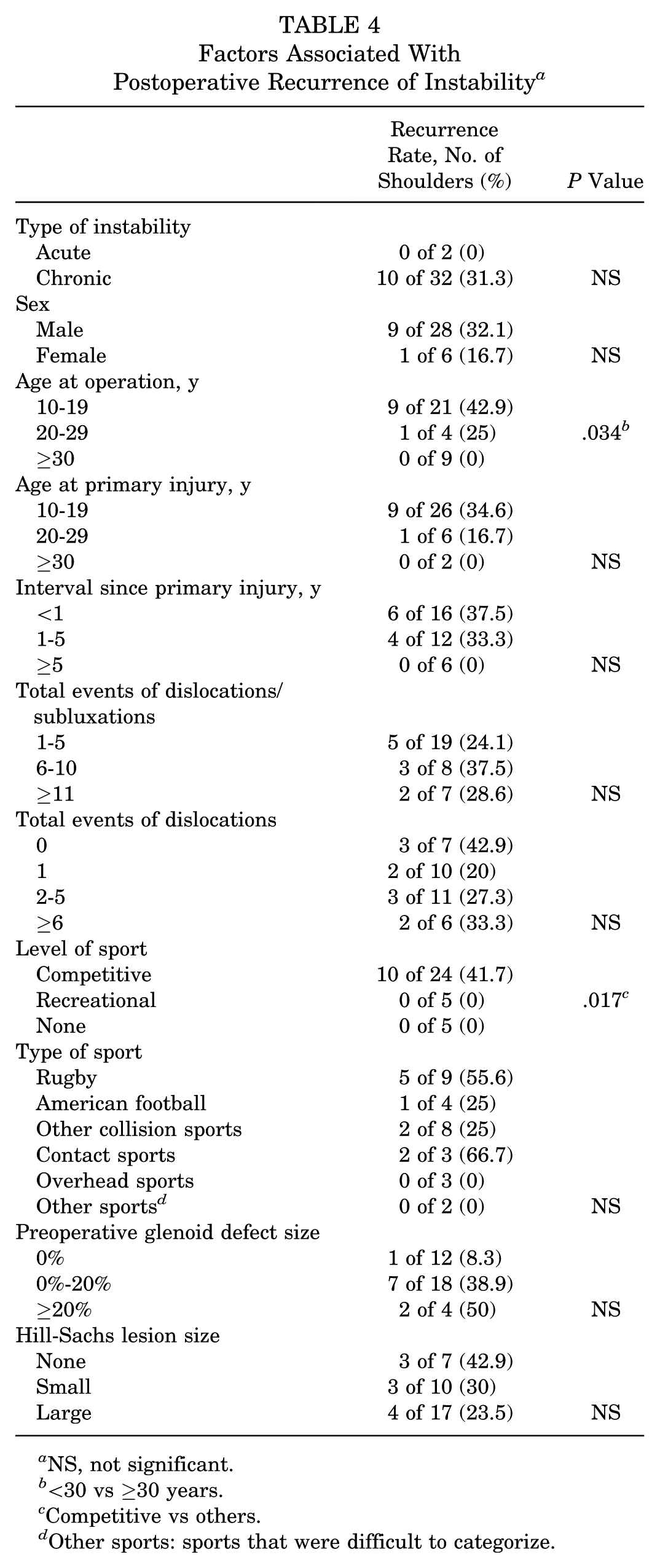
NS, not significant.
<30 vs ≥30 years.
Competitive vs others.
Other sports: sports that were difficult to categorize.
Discussion
The present study showed that of the shoulders that underwent arthroscopic Bankart repair, capsular lesions were present in 21.5%. Older age, complete dislocation, and an associated Hill-Sachs lesion were significant risk factors for the occurrence of capsular lesions. The recurrence rate of shoulder instability was significantly higher after combined capsular repair with Bankart repair than after isolated Bankart repair. Since mild capsular lesions had a similar high postoperative recurrence rate as severe lesions, both should be recognized as risk factors. The postoperative recurrence rate was significantly higher among young patients and competitive athletes. Accordingly, capsular lesions were more frequent in older patients, but recurrence of shoulder instability after surgical repair was quite rare, while frequent postoperative recurrence of shoulder instability was a problem in young competitive athletes.
There have been few previous reports regarding the prevalence of capsular lesions. Mizuno et al 3 studied 303 shoulders with recurrent anterior instability and reported that arthroscopy detected 12 isolated capsular tears (4.0%), 12 isolated HAGL lesions (4.0%), 21 capsular tears combined with Bankart lesions (6.9%), and 2 HAGL lesions combined with Bankart lesions (0.7%). Thus, the prevalence of capsular lesions in their patient population was almost 15%. In contrast, Ogawa and Yoshida 6 evaluated isolated capsular tears through open surgery and found a prevalence of 1.5% (5 of 333), while Rhee et al 8 reported that the prevalence of isolated capsular lesions was 1.8% and that of combined lesions was 3.6%. In the present series, the combined prevalence of capsular tears and HAGL lesions was 21.5%, which was higher than in other reports. However, this included mild tears confirmed at arthroscopy, and the prevalence of severe tears was 11.6%, which is more compatible with other reports.
Regarding the type of instability, the prevalence of capsular lesions was 11.5% among patients with acute instability, which was lower than reported previously. 1 However, the prevalence was higher (23.3%) among patients with chronic instability. Accordingly, it is not that capsular lesions created at the time of acute instability persist in the chronic phase but rather that their prevalence increases over time as a result of events related to instability. We sometimes encounter patients with recurrent instability and severe apprehension at a long interval after several instability events at a younger age. In the present study, capsular lesions were identified in 10 of 24 shoulders (41.7%) among patients aged ≥30 years. The primary episode of instability occurred before 30 years in 16 of these 24 shoulders, and capsular lesions were recognized in 7 of 16 shoulders (43.8%). Mizuno et al 4 divided their patients into 3 groups according to the age at the primary episode and at operation by 40 years, and they reported results similar to ours. They suggested that shoulders with an isolated Bankart lesion at a young age might develop a new capsular tear at recurrence owing to decreased viscoelasticity of the capsular tissue because of aging, and we support this hypothesis. Accordingly, at the time of operation among patients with a later onset of instability or among older patients whose instability occurred at a young age, the possibility of coexisting capsular lesions should be taken into consideration.
In the present study, complete dislocation and a coexisting Hill-Sachs lesion were also shown to be factors related to the occurrence of capsular lesions. As Ozaki et al 7 reported that (1) engagement of the humeral head with the anterior glenoid rim after (2) complete dislocation was essential for occurrence of a Hill-Sachs lesion, these 2 factors were considered to have a similar significance for capsular lesions. Accordingly, gross translation of the humeral head might lead to rupture of the anterior capsule. However, Mizuno et al 3 reported that most shoulders with isolated capsular tears or isolated HAGL lesions had only small (or no) Hill-Sachs lesions. While we did not obtain similar findings in the present study, the fact that there were no isolated capsular lesions might have influenced this discrepancy.
Regarding the clinical outcome after repair of capsular tears, Ogawa and Yoshida 6 reported that the outcome by open surgery was excellent in 3 shoulders followed for a minimum of 2 years. Mizuno et al 3 reported that 11 patients underwent arthroscopic capsular repair and 1 received open capsular repair, with the clinical results being favorable apart from recurrence in 1 patient (9.1%) after arthroscopic repair. Rhee et al 8 reported the results for 21 shoulders (7 isolated capsular tears and 14 capsular tears combined with a Bankart lesion), including open repair in 11 collision sport athletes and arthroscopic repair in the other 10 shoulders. Postoperative recurrence was recognized in 2 shoulders (20%) after arthroscopic repair and 1 (9.1%) after open repair. Recurrence occurred only in shoulders with combined lesions (3 of 14, 21.4%) and was not recognized in shoulders with isolated lesions. Taken with our findings, the recurrence rate was 4.5% (1 of 22) in shoulders with an isolated capsular tear and 27.1% (13 of 38) in shoulders with combined lesions, showing a significant difference between these groups, although the surgical procedures varied. Therefore, the repaired capsular tissues might be more fragile in shoulders with combined lesions.
However, the severity of capsular lesions and the number of sutures required for repair did not influence the surgical outcome. Furthermore, postoperative recurrence of instability was recognized solely in shoulders with chronic instability. Interestingly, while capsular lesions were frequently recognized in sedentary older patients, recurrence of instability frequently occurred in younger patients and collision/contact sport athletes. For patients with chronic instability, especially for active athletes, as the healing potential in the edge of the torn capsule appeared to be very poor, repair strength might be insufficient regardless of the severity of capsular lesions or suture materials. Excessive refreshment of the torn capsule and imbricating the capsule might induce the restriction of external rotation. So, procedures other than capsular repair—such as anteroinferior glenohumeral ligament reconstruction with soft tissue graft or bony augmentation with coracoid transfer or free bone graft—should be considered for such active young patients.
Regarding the influence of sport, Ogawa and Yoshida 6 performed open repair in 3 young athletes (including athletes playing rugby and American football) and reported no postoperative recurrence. Rhee et al 8 performed open repair for all collision athletes and reported recurrence in 1 professional wrestler. Mizuno et al 3 did not investigate young collision athletes and reported recurrence in only 1 middle-aged badminton player after arthroscopic repair. However, most of our subjects were young competitive athletes involved in collision/contact sports. As a result, almost half of competitive collision athletes younger than 20 years developed recurrence after arthroscopic repair, suggesting that arthroscopic Bankart repair might be contraindicated for such athletes with capsular lesions.
A limitation of the present study was its retrospective design, although we assessed preoperative clinical data that had been collected prospectively. The small cohort was another weakness of this study. Therefore, our statistical analysis was poor because of insufficient statistical power owing to the smaller number of patients, including postoperative recurrences. While we compared overall rates only, multivariate analysis should be performed if we experience a larger number of patients. Several factors—including type of sport and preoperative glenoid defect size—might be associated with postoperative recurrence of instability. As our subjects were limited to patients who underwent arthroscopic Bankart repair, isolated capsular tears were not studied, so this matter was a limitation of this study. Shoulders with an isolated capsular tear might have other features and might show another influence on postoperative recurrence of instability. Evaluation of Hill-Sachs lesion size was another weakness of this study. We classified Hill-Sachs lesions according to arthroscopic findings, but a more precise and simple computed tomography classification has recently been established.5,7 Precise investigation of the influence of Hill-Sachs lesions on postoperative recurrence of instability after arthroscopic Bankart repair is important, suggesting that further studies are needed.
Conclusion
In shoulders undergoing arthroscopic Bankart repair, capsular lesions were often present. Capsular lesions were associated with a higher recurrence rate of instability. Capsular lesions were more frequent in older patients regardless of their sporting activity. However, postoperative recurrence of shoulder instability after arthroscopic capsular repair combined with Bankart repair was more frequent in young competitive athletes regardless of the severity of their capsular lesions.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.