
Abstract
Background:
Generalized joint hypermobility (JH) might negatively influence the results of surgical femoroacetabular impingement (FAI) treatment, as JH has been linked to musculoskeletal pain and injury incidence in athletes. JH may also be associated with worse outcomes of FAI surgery in thin females.
Purpose:
To (1) determine the results of FAI surgery at a minimum 2-year follow-up by means of patient-reported outcome measures (PROMs) and failure rates, (2) assess the prevalence of JH in FAI patients and its effect on outcomes, and (3) identify other risk factors associated with treatment failure.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We included 232 consecutive patients (118 females; mean age, 36 years) with 244 hips surgically treated for symptomatic FAI between 2010 and 2012. All patients completed different PROMs preoperatively and at a mean follow-up of 3.7 years. Satisfaction questions were used to define subjective failure (answering any of the 2 subjective questions with dissatisfied/very dissatisfied and/or didn’t help/made things worse). Conversion to total hip replacement (THR) was defined as objective failure. JH was assessed using the Beighton score.
Results:
All PROM values significantly (P < .001) improved from preoperative measurement to follow-up (Oxford Hip Score: 33.8 to 42.4; University of California at Los Angeles Activity Scale: 6.3 to 7.3; EuroQol−5 Dimension Index: 0.58 to 0.80). Overall, 34% of patients scored ≥4 on the Beighton score, and 18% scored ≥6, indicating generalized JH. Eleven hips (4.7%) objectively failed and were converted to THR. Twenty-four patients (10.3%) were considered as subjective failures. No predictive risk factors were identified for subjective failure. Tönnis grade significantly (P < .001) predicted objective failure (odds ratio, 13; 95% CI, 4-45). There was a weak inverse association (r = −0.16 to −0.30) between Beighton scores and preoperative PROM values. There were no significant associations between Beighton scores and postoperative PROM values or subjective failure rates, but patients who objectively failed had lower Beighton scores than did nonfailures (1.6 vs 2.6; P = .049).
Conclusion:
FAI surgery yielded favorable outcomes at short- to midterm follow-up. JH as assessed by the Beighton score was not consistently associated with subjective and objective results. Joint degeneration was the most important risk factor for conversion to THR. Although statistical significance was not reached, female patients with no joint degeneration, only mild FAI deformity, and higher Oxford scores at the time of surgery seemed to be at increased risk for subjective dissatisfaction.
Today, surgical treatment of femoroacetabular impingement (FAI) has matured to a routine intervention. Outcomes at short- to midterm follow-up are favorable, and success rates are reported to be around 80% using either hip arthroscopy or open procedures.7,13-15,20 Several risk factors for failure (ie, total hip replacement [THR]) or subjective dissatisfaction have been identified. While older age and increased joint degeneration at the time of surgery seem to be the most important negative predictors, the effects of other factors, such as higher body mass index (BMI) or sex, are less clear.5,13,20,21
Generalized joint hypermobility (JH) might be another factor that could negatively influence the results of surgical FAI treatment. JH has been recognized as a risk factor for musculoskeletal pain and injury incidence in athletes.1,8,16,19,22,23 Also, it was thought that FAI surgery in thin and hypermobile females could be associated with worse outcomes. 13 The reason for this could be that, in JH, even normal or almost-normal joints impinge at a certain point, and FAI correction makes these joints even more mobile.11,13,24 Recently, the prevalence of JH in FAI patients has been reported to be high; more than 30% of the individuals scored ≥4 on the Beighton score, the instrument most frequently used to determine JH.3,11 Nevertheless, the association between JH and outcomes of FAI surgery is not widely known.
Considering the aforementioned, this study aimed to (1) determine the results of FAI surgery at a minimum 2-year follow-up by means of patient-reported outcome measures (PROMs) and failure rates, (2) assess the prevalence of JH in FAI patients and its effect on outcomes, and (3) identify other risk factors associated with treatment failure.
Methods
Between 2010 and 2012, a total of 283 patients (298 hips) were surgically treated for symptomatic FAI by 2 senior surgeons at our institution. This retrospective cohort study included 232 of those consecutive patients (244 hips) with complete follow-up data. The demographics of the nonresponders did not differ from those of the study cohort. There were 118 women (51%) and 114 men (49%). The mean age (±SD) was 35.8 ± 11.4 years, and the mean body mass index (BMI) was 24.0 ± 3.6 kg/m2. Thirty-five patients underwent surgical hip dislocation (SHD), 67 underwent mini-open surgery using an anterolateral approach, and 130 underwent hip arthroscopy. Indication for either type of surgery was dependent on the surgeon’s preference (one surgeon performed only mini-open surgery) and on the severity of deformity (SHD in cases with more severe FAI deformity). Patients in the SHD group were younger, and more male patients underwent open surgery (Table 1). Beighton scores and BMI did not differ (P > .05) between the 3 groups. Center-edge (CE) and alpha angles were significantly (P < .01) lower in the hip arthroscopy group. Twenty-three of the hips had at least 1 previous surgery (hip arthroscopy in 9, pelvic osteotomy for dysplasia in 8, femoral osteotomy in 3, and SHD in 1).
Preoperative Patient Demographics a
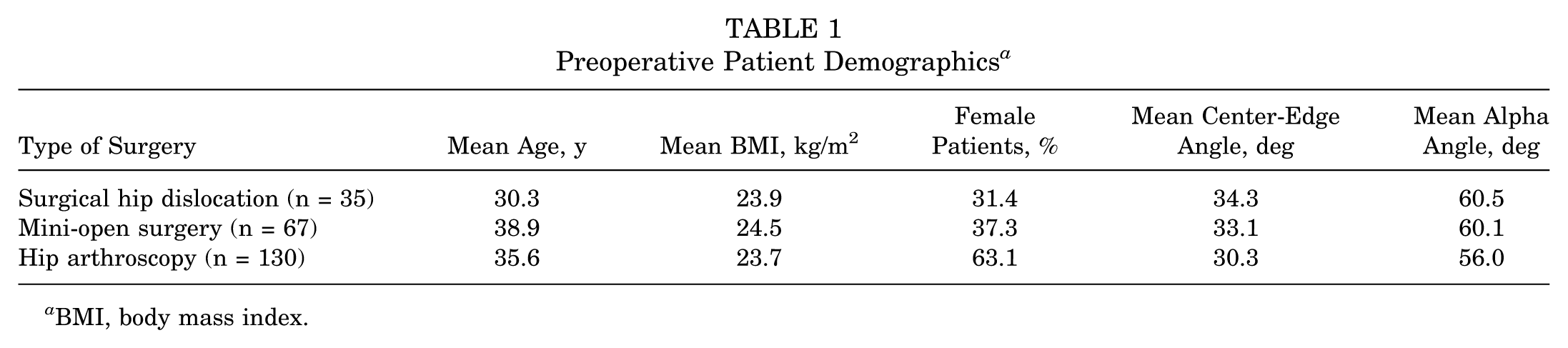
BMI, body mass index.
The diagnosis of FAI was based on standardized parameters that have been described in detail previously. 13 Briefly, a cam component was defined by an alpha angle >50° and a pincer component by global (coxa profunda or protrusio) or focal (crossing sign) acetabular (AC) overcoverage. Accordingly, 59% had mixed-type FAI, 20% had pincer-type FAI, and 21% had cam-type FAI. All patients underwent standardized radiographic examinations, including anteroposterior pelvis and cross-table lateral hip radiographs and MRIs with intra-articular gadolinium contrast. The following parameters were determined: Tönnis grade, lateral CE angle, AC roof angle, extrusion index, presence of AC overcoverage, and the alpha angle.
All patients completed the Oxford Hip Score (OHS), 6 EuroQol–5 Dimension (EQ-5D), 4 and University of California at Los Angeles (UCLA) Activity Scale 12 preoperatively and at follow-up. At follow-up, the patients also completed the self-reported version of the Beighton score,3,11 a question inquiring about subjective satisfaction (“How satisfied are you with the result of surgery?”: very satisfied, satisfied, neither satisfied nor dissatisfied, dissatisfied, very dissatisfied), and a question inquiring about the global treatment outcome (“the hip operation”: helped a lot, helped, helped only little, didn’t help, made things worse). Reoperations and conversions to THR were noted prospectively. Conversion to THR was defined as objective failure. Subjective failure was defined by answering any of the 2 subjective questions with dissatisfied/very dissatisfied and/or didn’t help/made things worse. The local ethical committee approved the study, and all patients provided written informed consent.
Statistical Analysis
To determine the results of FAI surgery at a minimum 2-year follow-up, pre- and postoperative values were compared using the paired t test. Failure rates were reported as percentages. To assess the prevalence of JH in FAI patients and its effect on outcomes, data were presented as percentage of patients scoring in each category of the response options and correlations (Pearson moment product coefficient) between Beighton scores and PROMs, radiographic parameters, and failure rates. To identify other risk factors associated with treatment failure, all the parameters differing between failure and nonfailure were analyzed using logistic regression with forward conditional selection. Odds ratios were calculated with 95% CIs. The magnitude of difference was expressed using the effect size calculated as Cohen d (difference/baseline SD) and interpreted using the following benchmarks: 0.2 to 0.5, small; 0.5 to 0.8, medium; >0.8, large. Analyses were performed with the use of SPSS version 17 (IBM Corp). Unless otherwise stated, all values are expressed as mean ± SD.
Results
Mean follow-up was 3.7 years (range, 2-5 years). Nine major revisions (3.6%) were performed at a mean of 14 months (range, 3-29 months) after index surgery (7 after hip arthroscopy, 1 after SHD, and 1 after mini-open surgery), all for residual FAI or intra-articular adhesions. One minor revision (secondary tractus closure due to dehiscence) was necessary after SHD. Overall, 11 hips (4.7%) objectively failed and were converted to THR at a mean of 24 months (range, 7-45 months) after index surgery (6 had arthroscopy, 5 had mini-open surgery). Seven of the converted hips had Tönnis grades 2 or 3 before FAI surgery, 3 hips had Tönnis grade 1, and 1 hip had Tönnis grade 0.
PROM values significantly improved from preoperative measurement to follow-up (Table 2). CE, AC roof, and alpha angles significantly decreased (Table 2). Effect sizes were small for CE angle, AC roof angle, extrusion index, and UCLA Activity Scale. The effect size of the remaining parameters and PROMs ranged from medium to large. Overall, 34.3% of the patients scored ≥4 on the Beighton score, and 18.0% scored ≥6, indicating generalized JH (Figure 1). The mean Beighton score was 2.5 ± 2.7. Patients with previous hip surgery did not differ in Beighton scores from those patients without. Female patients had significantly (P = .009) higher Beighton scores than did male patients (3.0 vs 1.9). There was a weak inverse association (P < .05) between Beighton scores and preoperative PROM values (r = −0.16 to −0.30). There were no significant associations between Beighton scores and postoperative PROM values and subjective failure rates. Subgroup analyses according to the surgical approach used showed similar results. Patients who objectively failed (ie, conversion to THR) had significantly lower Beighton scores than did the nonfailures (1.6 vs 2.6; P = .049).
Changes in PROMs and Radiographic Parameters From Preoperative Measurement to Follow-up a
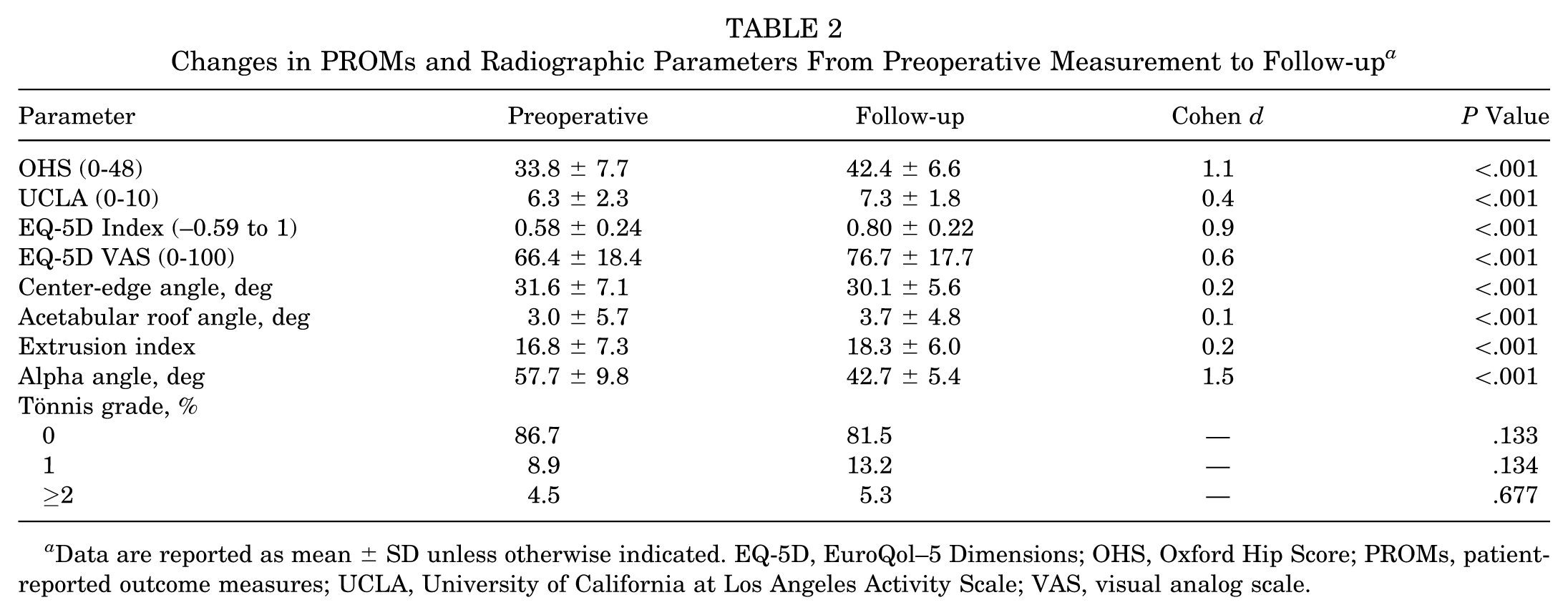
Data are reported as mean ± SD unless otherwise indicated. EQ-5D, EuroQol–5 Dimensions; OHS, Oxford Hip Score; PROMs, patient-reported outcome measures; UCLA, University of California at Los Angeles Activity Scale; VAS, visual analog scale.
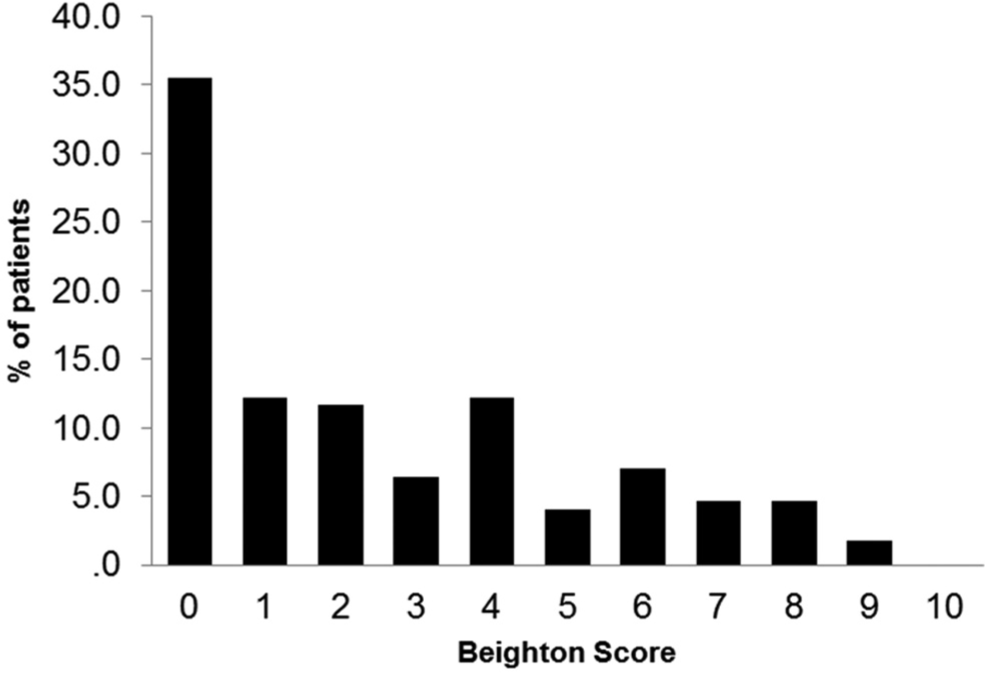
Distribution of Beighton scores (range, 0-9) in femoroacetabular impingement patients. Scores ≥4 are usually considered as cutoff defining generalized joint hypermobility.
Overall, 24 patients (10.3%) subjectively failed. Of these, 15 (62.5%) underwent hip arthroscopy as index surgery, 5 (20.8%) had mini-open surgery, and 4 (16.7%) had SHD. Patients with subjective failure did not differ from nonfailures in BMI, age, Beighton scores, and most radiographic parameters. Patients with subjective failure had significantly (P = .038) higher OHS values before surgery (36.4 vs 32.7) and lower (P = .006) mean Tönnis grades (0.04 vs 0.21). While there were more female than male patients (58.3% vs 41.7%) in the subjective failure group, this difference did not reach statistical significance (P > .2) in relation to the entire cohort. All PROM values at follow-up and change scores were significantly lower in the subjective failure group (OHS: 35.4 vs 42.4; UCLA: 6.5 vs 7.3; EQ-5D Index: 0.65 vs 0.80; EQ-5D visual analog scale: 62.0 vs 76.7; P < .01 for all).
Group comparisons demonstrated that patients who objectively failed were significantly older, had significantly lower preoperative OHS values, significantly higher Tönnis grades, lower Beighton scores, and higher BMI (Table 3). Effect sizes were medium to large. Radiographically, failures had higher CE angles and lower extrusion indices before surgery (Table 3). There were no significant differences in AC roof angles. Logistic regression analysis did not identify any predictive variable for subjective failure. Tönnis grade significantly (P < .001) predicted objective failure (Table 4).
Differences Between Objective Failures and Nonfailures a
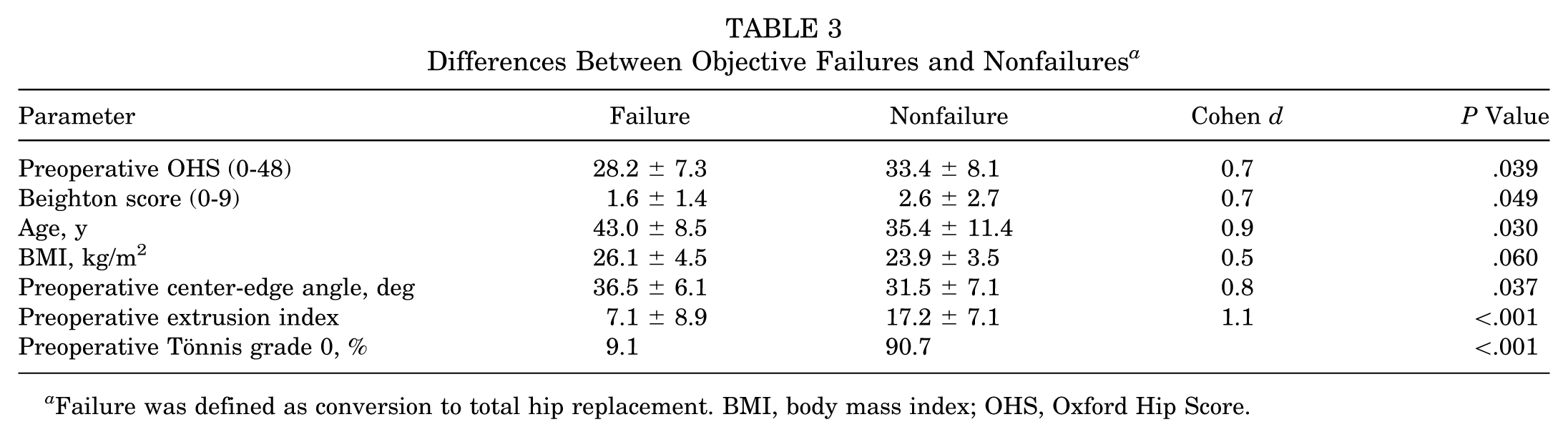
Failure was defined as conversion to total hip replacement. BMI, body mass index; OHS, Oxford Hip Score.
Predictive Risk Factors for Objective and Subjective Failure According to Logistic Regression Analysis a
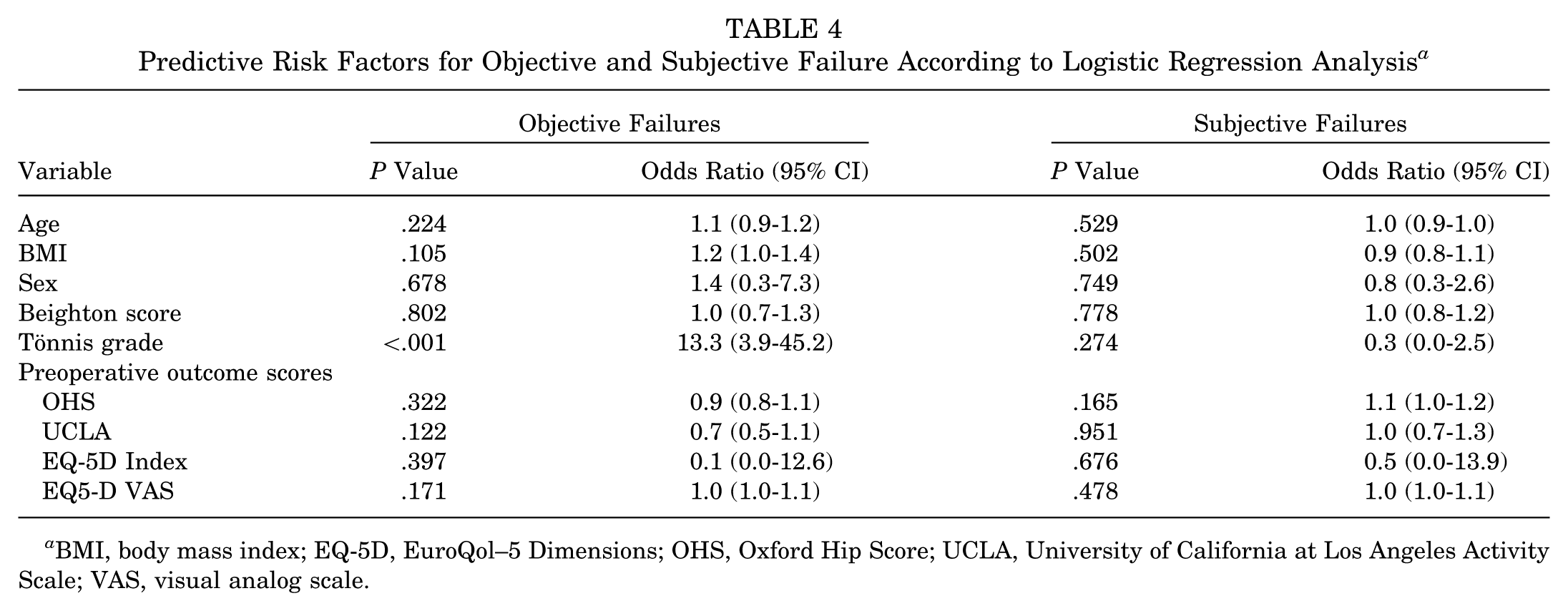
BMI, body mass index; EQ-5D, EuroQol–5 Dimensions; OHS, Oxford Hip Score; UCLA, University of California at Los Angeles Activity Scale; VAS, visual analog scale.
Discussion
Generalized JH has been linked to musculoskeletal pain and a higher injury incidence in an active population.1,8,16,19,22,23 Besides other known risk factors, JH might be associated with worse results after surgical FAI treatment.11,13,24 Therefore, assessing the possible association between JH and the results of FAI surgery is important.
Before interpreting the present results, several limitations have to be considered. First, the study sample is not uniform since patients undergoing 3 different surgical approaches to treat FAI were included. The indication for a specific approach was dependent on the preference of one surgeon and on the severity of the deformity, leading to selection bias that is reflected in the demographics of the different groups. While meaningful comparisons between approaches are therefore not possible, this cohort nevertheless reflects the clinical reality. Furthermore, subgroup analyses showed similar results related to JH, that is, only weak or no associations between the Beighton score and PROM values. Second, Beighton scores were not assessed before surgery but at follow-up; however, it is unlikely that generalized joint mobility changes over the course of a few years. Third, logistic regression analysis identified some potential risk factors for subjective and objective failure that showed wide ranges of overlapping CIs. Therefore, these factors did not reach statistical significance. This is a result of the relatively small number of failures; studies with larger numbers of patients and failures are required to identify other possible risk factors for poor results.
In general, surgical FAI treatment yielded favorable outcomes. All PROM values significantly increased, and the scores at follow-up compare well to values reported in the literature.7,13-15,20,21 The conversion rate to THR (defined as objective failure in this series) is 4.5% at 3.7 years, similar to the results of previous reports.13,15,20,21 Nevertheless, contrary to what we expected, we could not find conclusive associations between the outcomes and JH. In line with previous studies, the prevalence of JH was high in the present cohort.2,11 Depending on the Beighton cutoff score used, 34% (≥4) or 18% (≥6) of the individuals were diagnosed with JH. While hypermobile hip joints might have the risk of persistent impingement after FAI correction, Beighton scores did not correlate with PROM values or radiographic parameters. Moreover, higher Beighton scores seemed to be protective in terms of objective failure (significantly lower Beighton scores in the THR conversion group). These observations could be explained in 2 ways: Either generalized JH does indeed not substantially affect the outcomes of FAI surgery, or the Beighton score is not a suitable instrument to assess hip joint hypermobility. While these explanations are rather speculative, further research seems warranted to investigate whether higher Beighton scores indeed indicate hypermobility of the hip joint itself. A significant association between Beighton scores and hip range of motion (flexion and rotation in flexion) was previously found in a small series. 11
For objective failures (ie, conversion to THR), we could identify 1 well-known predictive risk factor and some other factors that significantly differed from patients without conversion. The most important negative predictor was the Tönnis grade. Patients with Tönnis grade 1 or higher at the time of FAI surgery had a 13-fold increased risk for conversion to THR compared with patients with Tönnis grade 0. Patient age of 40 years or older has been frequently considered as a significant negative predictor.15,20,21 Our results confirm these observations; patients requiring THR were significantly older than were those without conversion (43 vs 35 years). The effect of overweight is somewhat controversial in the literature. In a large series of FAI patients treated with SHD, lower BMI values were associated with THR conversion and revision surgery. 13 Peters et al 17 did not find an increased risk of poorer outcomes based on BMI but identified age as a risk factor. Steppacher et al 20 showed that being overweight was a risk factor for failure after SHD. Gupta et al 5 also reported a 2-fold increased THR and revision rate in obese FAI patients when compared with normal-weight counterparts, but probably due to the small sample size, these differences did not reach statistical significance. Our data suggest that overweight might be another risk factor for objective failure but not for subjective failure. Therefore, in summary, patients older than 40 years presenting with early joint degeneration (ie, Tönnis grade >0) and higher BMI should be considered as high-risk candidates for early objective failure after FAI surgery, irrespective of the surgical approach used. This conclusion also explains the observation that none of the THR conversions were performed after SHD. SHD was mainly performed in younger men with more severe FAI deformity but less joint degeneration. In an older patient with early degeneration, one would be more reserved with the indication for SHD. In such cases, hip arthroscopy or mini-open approaches might be considered as “palliative” treatment options; however, “stretching” indications can yield a high risk of early failure.
While the risk factors for THR conversion are relatively uniform in the literature, it is difficult to understand why surgery yields subjectively unsatisfactory outcomes in a relevant proportion of patients, despite favorable radiographic results and the absence of the above-mentioned risk factors. Finding reasons for this can be difficult, and identifying other predictive risk factors is mandatory. The present results suggest a vague picture of such kind of patients being relatively young and female, having no joint degeneration and less deformity, and having a quite well-functioning hip joint at the time of surgery. It might be a combination of higher expectations in such patients, and it may also be a false or borderline diagnosis of FAI yielding a lack of improvement after surgical treatment. The interdependence of fulfilled expectations and patient satisfaction after FAI surgery has been highlighted. 9 It is important to focus future work on patient selection processes and a clear exclusion of sources of groin pain other than FAI (such as muscle imbalance, sportsman’s groin, inguinal hernia, etc), particularly in cases with only mild deformity.10,18
Overall, FAI surgery yielded favorable outcomes in terms of PROM values and failure rates at short- to midterm follow-up. Generalized JH as assessed by the Beighton score had no conclusive associations with subjective and objective results. This might be related to the fact that JH is not linked to the outcome of FAI surgery or that the Beighton score is not a suitable tool to determine hypermobility of the hip joint itself. In line with previous investigations, joint degeneration, older patient age, and overweight were associated with THR conversion. Future research is warranted to identify reasons for subjective dissatisfaction. Female patients with no joint degeneration, only mild FAI deformity, and quite well-functioning hip joints at the time of surgery seem to be at increased risk.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: AFOR Stiftung supported this study.