
Abstract
Background:
Sleep disturbance is a major complaint of patients with rotator cuff disease that often leads them to seek treatment. The authors previously reported a prospective analysis of patients who underwent rotator cuff repair and found that sleep disturbance significantly improved at 3 months after surgery. That improvement in sleep was maintained at 6 months.
Hypothesis:
In the current study, the authors sought to gain medium-term data on this same population at greater than 2 years. The hypotheses were that improvement in sleep disturbance after arthroscopic rotator cuff repair is maintained at 2-year follow-up and that the continued use of narcotic pain medication has a negative effect on sleep quality at 2-year follow-up.
Study Design:
Case series; Level of evidence, 4.
Methods:
The original cohort of patients was contacted at a minimum of 24 months after their surgery. Thirty-seven of the 56 patients (66%) involved in the original study were available. Patient outcomes were scored using the Pittsburgh Sleep Quality Index (PSQI), Simple Shoulder Test (SST), visual analog scale (VAS) for pain, and Single Assessment Numeric Evaluation (SANE). The newly obtained scores were compared with prior scores, which ranged from preoperatively to 6 months postoperatively.
Results:
The statistically significant improvement of the PSQI score demonstrated in our prior analysis at 6 months postoperatively was maintained, with a mean PSQI score of 5.5 for the 37 patients followed beyond 24 months. Of those patients, 41% still had a PSQI score >5, indicative of sleep disturbance. However, even those patients in our study with a PSQI score >5, indicative of sleep disturbance, had an improved mean score of 9.3 at greater than 24 months compared with those patients with a PSQI score >5 at 6 months, who had a mean PSQI score of 11.5 (P = .13). Both the SST and VAS scores displayed continued improvement at greater than 24 months, with both displaying moderate strength correlation to the PSQI score (VAS: Spearman rho = 0.479, P < .001; SST: Spearman rho = −0.505, P < .001). Regression models again demonstrated the continued use of narcotic pain medication correlating with poor sleep as the difference in the mean PSQI score between users and nonusers increased as postoperative time increased. At greater than 24 months after surgery, patients using narcotics had a mean PSQI score that was 7.4 points higher than narcotic nonusers (standard error [SE] = 1.93; P = .00017).
Conclusion:
At greater than 24 months, 41% of patients still demonstrated sleep disturbance, with both SST and VAS scores showing improvement. The prolonged use of narcotic medication negatively affects sleep, with a greater effect seen over time.
Sleep disturbance is a major complaint of patients with rotator cuff disease. It is often sleep disturbance rather than pain and functional deficits that lead patients to seek treatment. Furthermore, after surgical rotator cuff repair, many patients continue to complain of sleep disturbance. Adequate sleep plays an important role in healing and satisfaction, and therefore, it is important to study sleep disturbance in patients with rotator cuff disease.
Few studies have examined the influence of rotator cuff injuries on sleep habits. Our group had previously reported the first study to characterize sleep disturbance after arthroscopic rotator cuff repair with a 6-month follow-up. 1 In that study, we found that 89% of patients reported preoperative sleep disturbance. A statistically significant improvement in sleep was seen at 3 months and maintained up until 6 months after surgery. At 6 months, nearly two-thirds of patients who underwent rotator cuff repair and who reported poor preoperative sleep quality scores displayed improvement to normal sleep score values. 1 We also evaluated many variables against sleep disturbance and found that the preoperative use of narcotic pain medication along with the prolonged postoperative use of narcotics (>6 weeks) was correlated to worse sleep disturbance postoperatively. There is no question regarding the importance of sleep to general health and, more importantly, to the healing of the postoperative patient. Tissue healing, the production of endogenous anabolic steroids such as human growth hormone, and psychological well-being are all strongly dependent on adequate sleep. As such, we believe that it is important to have long-term outcomes on the relationship between the quality of sleep and rotator cuff repair.
The primary purpose of this study was to extrapolate on our prior report and investigate medium-term postoperative sleep disturbance in patients who underwent arthroscopic rotator cuff repair. The secondary aim was to identify the factors that predispose patients to sleep disturbance at greater than 2 years from surgery. Our hypotheses were that (1) improvement in sleep disturbance after arthroscopic rotator cuff repair is maintained at 2-year follow-up and (2) the use of narcotic pain medication has a negative effect on sleep quality at 2-year follow-up.
Methods
Our institutional review board approved this study (Rothman Institute, AtlantiCare Regional Medical Center IRB Protocol #14-028EX). From June 2012 through January 2013, participating surgeons performed rotator cuff repair on 178 patients, of whom 142 patients met the criteria for inclusion in our study. Fifty-six of these eligible patients who underwent arthroscopic rotator cuff repair completed preoperative surveys and agreed to enroll in this prospective case series. All patients signed a written consent form that permitted involvement in the study. Any male and nonpregnant female patients aged ≥18 years with a full-thickness rotator cuff tear who underwent arthroscopic rotator cuff repair were included in this study. Patients receiving workers’ compensation benefits, those with an irreparable tear, those undergoing revision surgery, and those with concomitant severe glenohumeral arthritis or concurrent adhesive capsulitis were excluded from participation. All patients were asked to fill out questionnaires before surgery and during normally scheduled postoperative visits: 2 weeks, 6 weeks, 3 months, 4.5 months, and 6 months. If the patient did not come into the office within 1 week of the scheduled follow-up, the patient was called and completed the survey over the telephone. In these cases, no clinical evaluation was performed at that time. An additional time point was added to the study to follow patients’ outcomes beyond 24 months. Patients received 4 opportunities to complete the final survey. Initially, they were all called. If they were unable to be contacted, we mailed the survey with a return envelope. After that, patients were emailed and then called once more.
The primary outcome measure was the Pittsburgh Sleep Quality Index (PSQI). Secondary outcome measures included the Simple Shoulder Test (SST), visual analog scale (VAS) for pain, and Single Assessment Numeric Evaluation (SANE). The SST is a 12-item, yes-or-no function inventory; the SANE is a patient-reported subjective assessment of the normalness of the patient’s shoulder. Demographic information was also collected for analysis of contributing factors including age, sex, body mass index (BMI), previous diagnosis of sleep apnea, nicotine use, alcohol use, preoperative narcotic use, and continued use of narcotic pain medication. Patients were not screened for sleep apnea beyond their history.
All arthroscopic rotator cuff repairs were performed by 1 of 4 orthopaedic surgeons who were fellowship trained in either sports medicine or shoulder and elbow surgery. After surgery, the treating surgeon recorded the size of the rotator cuff tear (small [<1 cm], medium [1-3 cm], large [3-5 cm], massive [>5 cm]), number of suture anchors used, repair technique, biceps treatment, execution of subacromial decompression, execution of distal clavicle excision, and intraoperative complications.
All patients followed the same postoperative rehabilitation protocol involving 6 weeks of sling immobilization with an abduction pillow, with pendulum exercises starting at week 2. Passive range of motion was begun at 6 weeks and active range of motion at 8 weeks. At 3 months, patients were allowed progressive resistance exercises with a limit of 10 lb. At 4.5 months, patients progressed to a 20-lb weight restriction. At 6 months, patients were cleared for discharge and allowed full activity with no restriction.
All patients followed the same postoperative pain management protocol including pregabalin (75 mg, twice daily for 3 days), oxycodone/acetaminophen (10 mg/325 mg, every 4 hours as needed), and ketorolac (10 mg, every 6 hours as needed for pain) for 3 days.
Outcome surveys were collected and scored by a single research coordinator who recorded each patient’s outcome scores at the preoperative and postoperative time intervals. The PSQI is a valid and standardized measure of sleep quality. 2 It is used to track sleep disturbance over time and is designed to be administered monthly. Patients fill out a 19-question survey, from which 7 component scores are obtained: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, sleeping medications, and daytime dysfunction. 2 The PSQI was reported as a global score (total of 21 points), with a higher score indicating worsening sleep dysfunction and a score >5 indicative of poor sleep quality. The VAS and SST were scored as a single value, and the SANE was scored as a percentage of 100%. A lower VAS score corresponded with less pain. Higher scores for both the SST and SANE indicated greater function of the shoulder.
Statistical Analysis
Data were analyzed longitudinally using the nlme package in the R statistical language (R Foundation for Statistical Computing). Mixed-model linear regression was performed, controlling for repeated measures among patients. A full model was created including all possible predictors of the PSQI score (VAS score, time, baseline use of narcotics, size of tear, single- vs double-row repair, number of anchors, distal clavicle excision, biceps tenotomy/tenodesis, subacromial decompression, sleep apnea, alcohol and tobacco use, sex, age, and BMI). This model was then systematically pruned of least significant factors until the only factors left were associated with model predictive performance. These final pruned models accounted for the following factors: sex, narcotic use, SANE score, SST score, and time.
Results
Initially, 89% of patients (50/56) reported preoperative sleep disturbance (PSQI scores >5/21), with a mean (±SD) PSQI score of 11.7 ± 4.6. Sixty-six percent of the patients (37/56) were available for greater than 24-month follow-up at a mean of 28.8 months (range, 24.0-37.9 months), with a mean PSQI score of 5.5 ± 4.0 (Figure 1). This was not significantly different from the mean PSQI score of 6.2 seen for all patients at 6 months after surgery (mean PSQI score of 5.4 for the available 37 patients). The mean PSQI score of these 37 patients was 11.6 ± 4.4 preoperatively, which was not significantly different from the mean score of all the initial 56 patients (Appendix Table A1, available in the online version of this article). Of those patients who were followed up beyond 24 months, 41% (15/37) reported PSQI scores indicative of sleep disturbance, with a mean PSQI score of 9.3 ± 3.4. Those patients with PSQI-scored disruptive sleep were followed up at a mean of 27.8 months (range, 26.5-30.6 months). There was no correlation found between the duration of follow-up and PSQI scores.
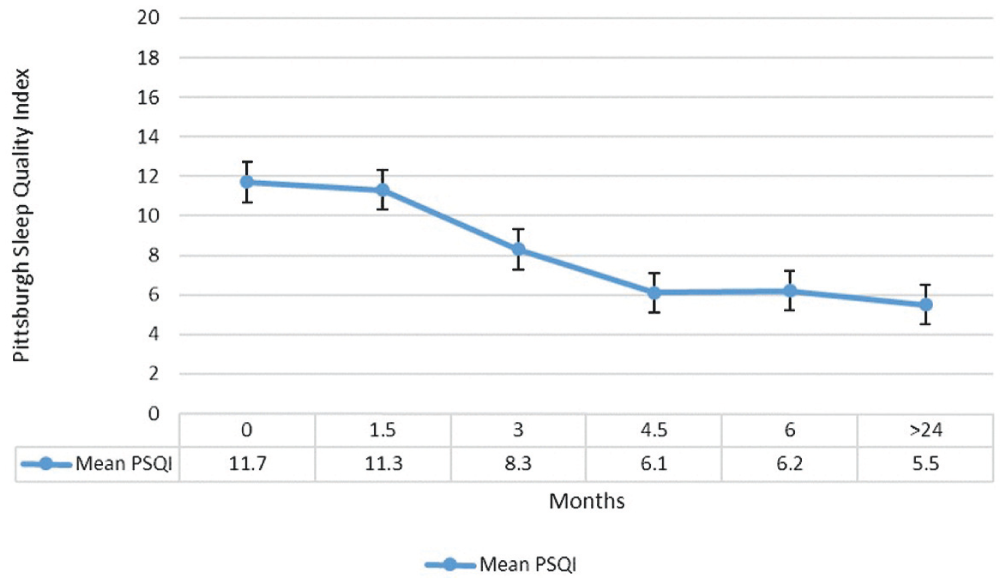
Reported sleep quality (mean Pittsburgh Sleep Quality Index score) versus time (months). Error bars show ±SE.
The only independent demographic or surgical parameter that affected postoperative sleep was the continued use of narcotic pain medication. Unlike our initial study, which showed a correlation of preoperative narcotic use with poor sleep quality, this was not found at greater than 24 months of follow-up. Only patients taking continued pain medication reported higher PSQI scores, with the mean difference of these scores between narcotic users and nonusers increasing as postoperative time increased (Figure 2). Preoperatively, narcotic users had a mean PSQI score of 12.0 compared with 11.6 in nonusers. At 6 months, narcotic users had a mean PSQI score of 8.6 compared with 4.9 in nonusers. At the latest follow-up of greater than 24 months, narcotic users averaged a PSQI score of 12.5 compared with 5.1 in nonusers.
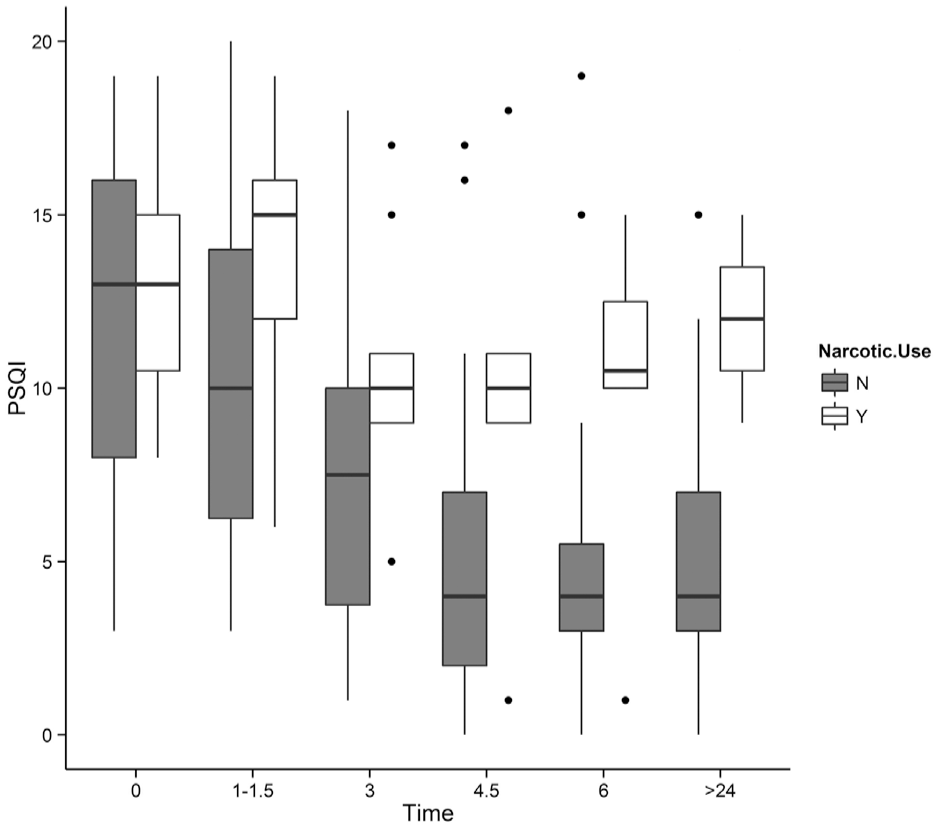
Reported sleep quality (mean Pittsburgh Sleep Quality Index score) versus time (months) for narcotic users and nonusers. Error bars show ±SE.
At 6 months after surgery, patients using narcotics had a mean PSQI score that was 3.7 points higher than narcotic nonusers (standard error [SE] = 1.67; P = .02). At greater than 24 months after surgery, patients using narcotics had a mean PSQI score that was 7.4 points higher than narcotic nonusers (SE = 1.93; P = .00017).
The SANE, VAS, and SST scores displayed a maintenance of improvement from 6 months postoperatively through to 2 years postoperatively (Figure 3).
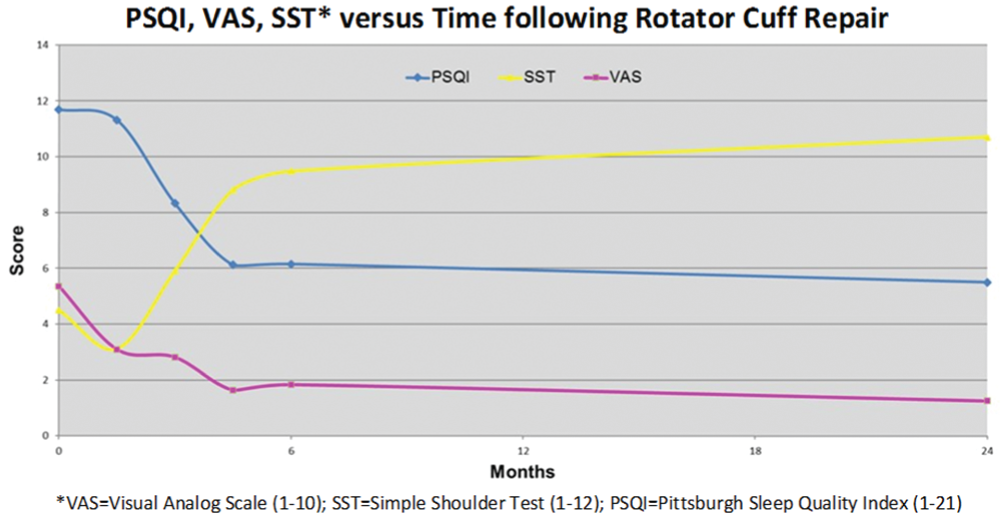
Reported outcomes at different time points throughout the study.
The VAS and SST scores both showed moderate strength correlation with the PSQI score at greater than 24 months after surgery as they had at 6 months after surgery. Both correlations to the PSQI score were again statistically significant, with the SST score having the strongest correlation (Table 1).
Spearman Rho Correlations of SST and VAS Scores With PSQI Scores at 6 Months and Greater Than 24 Months After Surgery a
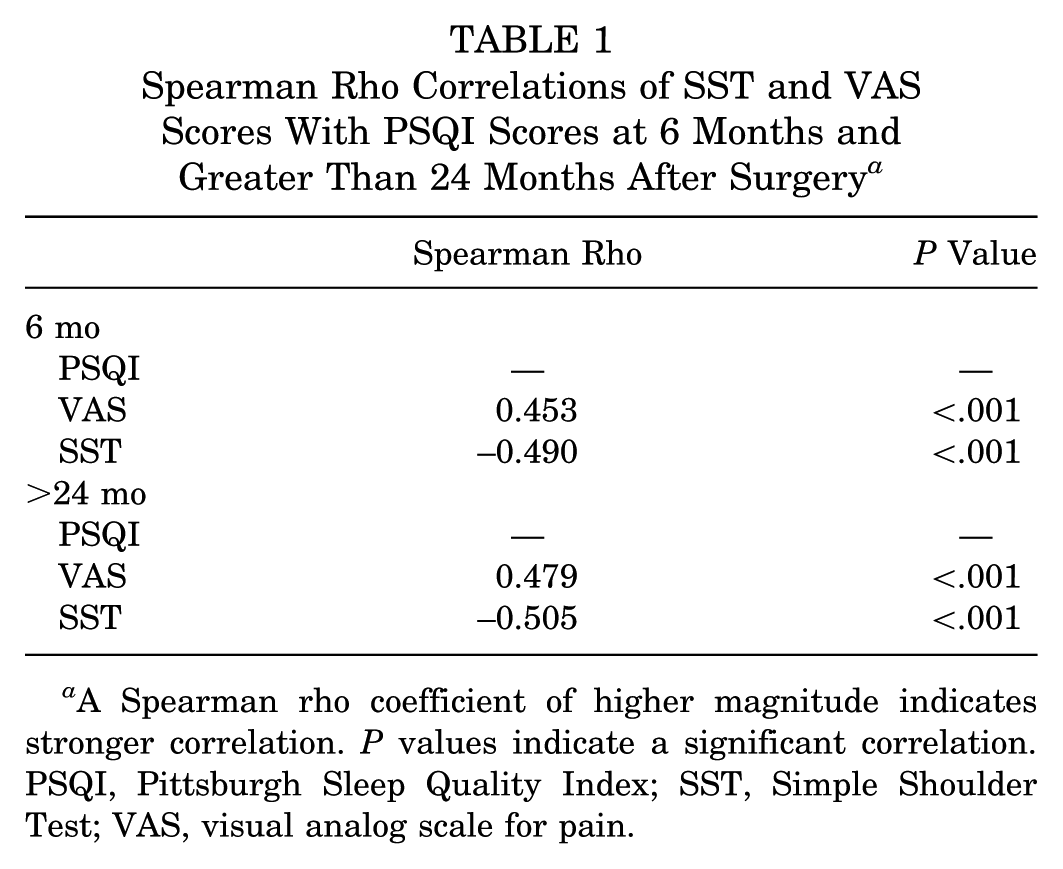
A Spearman rho coefficient of higher magnitude indicates stronger correlation. P values indicate a significant correlation. PSQI, Pittsburgh Sleep Quality Index; SST, Simple Shoulder Test; VAS, visual analog scale for pain.
Discussion
Sleep disturbance is a common complaint among patients with rotator cuff tears and is often the symptom that leads them to seek treatment. Our prior investigation found that 89% of patients complained of sleep disturbance before surgery (PSQI score >5). 1 After arthroscopic rotator cuff repair, patients experienced a significant improvement in sleep quality by 3 months. This improvement was sustained until 6 months after surgery, with almost two-thirds (62%) of patients reporting normal sleep habits. 1 The purpose of this study was to revisit these patients in the medium term to see how their sleep habits were affected by arthroscopic rotator cuff repair at 2 years postoperatively. Similarly, as we had done in our prior study, we wanted to examine which factors affected patients’ sleep.
Overall, the mean PSQI score of all the patients followed in this study continued to show improvement that was initially seen in our 6-month study that demonstrated a mean PSQI score of 11.7 preoperatively, which improved to 6.2 at 6 months postoperatively. This continued at greater than 2 years postoperatively, with a mean PSQI score of 5.5. When accounting for only the 37 patients followed at greater than 2 years in this study, the mean PSQI score of 5.5 was almost exactly that of 5.4 at 6 months. Before surgery, only 11% of patients with a symptomatic rotator cuff tear reported normal sleep scores (PSQI score ≤5). Six months after arthroscopic rotator cuff repair, 62% of patients reported normal sleep. 1 Of those 37 patients followed in the current study, 73% had PSQI scores indicative of normal sleep at 6 months after surgery. At greater than 2 years after arthroscopic rotator cuff repair, 59% of these patients continued to report normal sleep quality. This slight decrease in patients reporting normal sleep was not significantly different than the 6-month rate but remained substantially higher than before surgery (only 4/37 patients demonstrated PSQI scores ≤5). A closer analysis found that despite the slight increase in patients reporting disturbed sleep, there was improvement in sleep quality nonetheless.
The PSQI cutoff score for normal sleep quality is labeled at 5. Looking at the PSQI scores of only those patients with a total score >5 (disrupted sleep), we found that the mean of their scores trended more toward the normal PSQI cutoff score. Before surgery, 89% of the patients who reported sleep disturbance averaged a score of 11.7 ± 3.7. At 6 months (the final follow-up duration of our prior study), only 38% of patients had a PSQI score indicative of sleep disturbance, with a mean score of 11.5 ± 3.7. Of the 37 patients followed at greater than 24 months, 27% demonstrated sleep disturbance, with a mean PSQI score of 11.1 ± 4.5 at 6 months after surgery. At greater than 24 months, 41% of these patients maintained scores indicative of sleep disturbance, but only with a mean score of 9.3 ± 3.4. This means that even those patients classified as sleep-disturbed were likely trending toward sleeping better than they had before surgery. As with any scoring system, the PSQI has its limitations in trying to quantify many qualitative variables. Although a patient may still end up with a score that is considered above the cutoff for disrupted sleep (PSQI score >5), there can certainly be variables measured that show improvement, as was the case here. A further analysis of these 41% of patients with continued sleep disturbance would likely elucidate what exactly that trend is of their overall sleep quality, but this was beyond the analysis and scope of this article.
In addition, we used other various scoring systems to evaluate any correlation with the PSQI score in the search for specific factors associated with sleep disturbance. Our prior study found that the VAS score had a moderate correlation with the PSQI score (Spearman rho = 0.453, P < .001). 1 When revisited at the 2-year mark, it was relatively maintained (Spearman rho = 0.479, P < .001). This is consistent with numerous other reports. Mulligan et al 8 found that 91% of their patient population with shoulder disorders (osteoarthritis, rotator cuff disorder, or adhesive capsulitis) also reported nocturnal pain. The authors of that study suggested that the elevated inflammatory cytokines associated with inflammation about the rotator cuff are responsible for the increase in nocturnal pain levels.4,5,8 This inflammatory cascade is often exacerbated during sleep, secondary to the increased production of melatonin, which was recently shown to increase IL-6. 4 In addition, as we suggested in our prior study, an even stronger relationship existed between the SST and PSQI scores. At 6 months, the SST score displayed moderate correlation with the PSQI score that was marginally greater than the VAS score (Spearman rho = −0.490, P < .001). This was maintained at 2 years with again a marginal increase (Spearman rho = −0.505, P < .001) (Table 1). Although these correlations are moderate at best, it does help to show that there is some maintenance of the relationship between the PSQI score and the other measured scores as time continues out from surgery. The Spearman rho between narcotic use and the VAS score was generally between 0.3 and 0.4. This indicates that a relationship between these 2 factors exists, but it is relatively weak. The weakness is likely caused by the effect of other factors such as tolerance for narcotics, which are hard to measure objectively and beyond the scope of this study. This correlation may suggest that sleep quality after rotator cuff repair is affected by more than just pain, but further studies are indicated.
Pain control, however, remains a very integral part of caring for the patient with rotator cuff disease. It is not an uncommon scenario for the patient with a rotator cuff tear to be treated with narcotic pain medication both before and after surgical repair. In regards to sleep habits, our prior study had shown that the preoperative and continued postoperative use of narcotic pain medication were the only measured factors found to significantly disrupt sleep. 1 Narcotic medication use is known to disrupt the normal sleep cycle and result in decreased rapid eye movement sleep and increased wakefulness.3,6,7 Our data in this study demonstrated that sleep disturbance seemed to increase as patients continued to depend on narcotic pain medication. At 6 months postoperatively, the mean PSQI score was 3.7 points higher for those continuing to use narcotic pain medication (SE = 1.67; P = .02). This disturbance increased dramatically at 2 years, with narcotic-using patients reporting a mean PSQI score that was 7.4 points higher than those not using narcotics (SE = 1.93; P = .00017) (Figure 2). This finding reinforces our prior suggestion that counseling patients to discontinue narcotic use is essential to regaining a normal sleep cycle. Although it is often easier to submit to a patient’s request for more pain medication to help them sleep, surgeons must do a better job of counseling patients on the ill effects of taking narcotics and work in conjunction with pain management specialists to find alternatives.
This study had limitations. As a continuation of our prior analysis at 6 months postoperatively, many of these limitations remained the same. The most obvious limitation was the lack of a control group. This leads to inherent bias that can often plague case series studies. We did not have a nonoperative group of patients with rotator cuff tears. Although we believe that our study population was a good representation of the general population, the use of a control group treated nonoperatively would truly allow for all patients with rotator cuff tears to be analyzed. Within the group that we did follow in this study, there were limitations to their rate of response at the 2-year time point. All patients were called twice and mailed a letter twice, inviting them to participate in this study. Unfortunately, despite this reasonable mode of contact, only two-thirds of our initial 56 patients were available for follow-up at 24 months and beyond. This loss of 33% of the initial cohort could potentially bias the latest outcome and sleep scores, as patients who are doing well or did not seek further treatment elsewhere may be more willing to participate in our study. Another limitation of this study was the limitations of the measurement tools themselves. Many of the scores that we compared for patient outcomes, including the PSQI, are subjective measures reported by the patients themselves. A truly objective analysis would require the use of documented sleep habits using various physiological measurements and perhaps even recorded sleep habits. This is a vast undertaking but would allow for a more objective and accurate measure of true sleep habits. Additionally, we did not objectively measure the integrity of the rotator cuff repairs with any postoperative imaging such as magnetic resonance imaging or ultrasound. It is possible that patients who continued to display poor sleep quality were affected by a failed repair procedure. Although we measured outcomes with validated shoulder scores, more objective findings may have led to a better understanding of continued sleep disturbance. Another limitation in this study was the inability to analyze the role of continued narcotic pain medication in patients at 24 months and beyond as it pertains to their overall health. Narcotic use and dependence are multifactorial, and it is quite difficult to find an objective scoring system that can relate its use to the overall health of a patient, what other factors may be causing its use, and what tolerance or dependence level exists within each patient. As mentioned earlier, the correlation between the VAS score and narcotic use is weak because of this lack of objective characteristics to understand narcotic dependence and tolerance. Lastly, our study may be underpowered to detect the relationship between sleep disturbance and other associated factors such as BMI, size of the tear, and so on. However, the strengths of this study are that it is prospective and is the first study to evaluate medium-term follow-up of sleep disturbance after arthroscopic rotator cuff repair.
In conclusion, improvement in sleep disturbance after arthroscopic rotator cuff repair remained at 2-year follow-up but with no improvement seen between 6 months and greater than 24 months after surgery. Forty-one percent of patients continued to report sleep disturbance (PSQI score >5) at 2-year follow-up, but this was significantly improved from 89% preoperatively. This disturbance is not simply a function of pain but of shoulder function itself. Furthermore, this study shows that the continued use of narcotic pain medication after arthroscopic rotator cuff repair perpetuated sleep disturbance with a greater magnitude as time went on postoperatively. It remains critical for the treating surgeon to find alternatives to narcotic pain management early in the postoperative period and to reiterate these alternatives long after surgery has been performed.
Footnotes
Acknowledgements
The authors acknowledge Mitchell Maltenfort, PhD, for help with statistical analysis.
This work has been presented as a podium presentation at the 2016 American Academy of Orthopaedic Surgeons Annual Meeting in Orlando, Florida, entitled “Sleep Disturbance Following Rotator Cuff Repair: A Prospective 2-Year Investigation.” It was also presented as a podium presentation at that same meeting as part of the American Shoulder and Elbow Surgeons Specialty Day Meeting.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.