
Abstract
The anterolateral ligament (ALL) of the knee has gained attention recently for its potential role in rotational stability of the knee, especially in association with anterior cruciate ligament (ACL) injuries. Anatomic studies have characterized the ALL as it runs in an anteroinferior and oblique direction from the lateral distal femur to the anterolateral proximal tibia, although the prevalence and variance of this ligament are not well understood. Magnetic resonance imaging and ultrasound have identified the ligament and linked it with the classically described Segond fracture. While the ALL likely plays a role in rotational stability of the knee, further studies investigating the significance of ALL injuries and the role of ALL reconstruction in combination with ACL reconstruction are warranted.
The anterolateral ligament (ALL) of the knee has recently regained popularity. However, its roots go back to 1879 when Paul Segond described an avulsion fracture of the proximal anterolateral tibia as associated with “a pearly, resistant, fibrous band which invariably showed extreme amounts of tension during forced internal rotation.” 56 Many studies since that time have coined the “anterior band of the lateral collateral ligament,” 32 “mid-third capsular ligament,” 30 “anterior oblique band,” 3 and “capsule-osseous layer of the iliotibial tract.” 70
Despite generally good outcomes after anterior cruciate ligament (ACL) reconstruction, a number of patients have persistent instability and pivot shift on examination, and many are not able to return to preinjury competitiveness after surgery.1,7 Historically, lateral extra-articular tenodesis reconstruction was performed to enhance anterolateral stability, although there were some concerns that this could overconstrain the knee and contribute to early lateral compartment degeneration.14,41,48 With the resurgence of the ALL and its clinical importance, many studies have sought to examine its anatomy, biomechanics, and imaging and present the clinical outcomes and surgical technique of ALL reconstruction.5,8,9,11,27,71 Studies have reported variable identification of the ALL on anatomic dissection and imaging and questioned its role as a knee stabilizer.16,54,65,67 While there is substantial literature on this topic, investigations are warranted to further elucidate the role of the ALL in the knee.
Anatomy
The ALL has been identified in the fetal period. 29 It has a prevalence of 45% to 100% in cadaveric knee anatomic studies.11,53,65,71 It runs in an anteroinferior and oblique direction from the lateral distal femur to the proximal anterolateral tibia (Figure 1). Most studies agree that the ALL inserts onto the proximal tibia midway between the Gerdy tubercle and the fibular head, about 5 to 10 mm below the lateral tibial plateau’s joint line. The origin is near the lateral femoral epicondyle (LFE) but exactly where is controversial. More recent studies have tended to report the origin as posterior and proximal to the lateral collateral ligament (LCL) or the same as the LCL origin, but others have found it anterior and distal to the LCL origin.5,22 Of note, magnetic resonance imaging (MRI) studies have found the same 3 variants.37,40
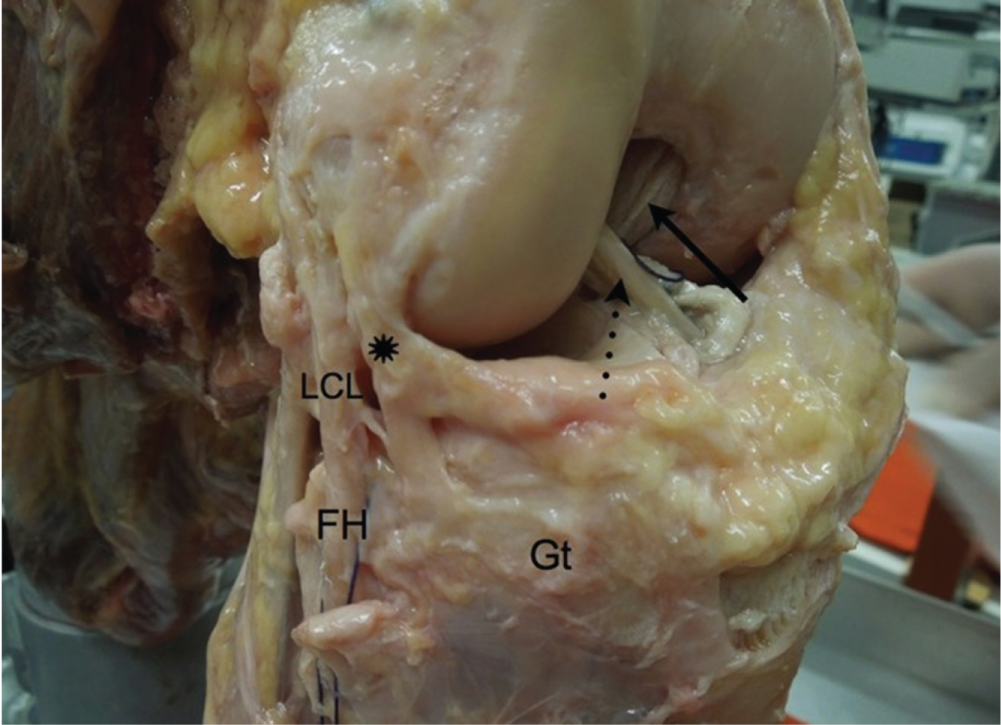
Anterolateral view of the right knee showing the anterolateral ligament (asterisk) running from the femur to the tibia, the anterior cruciate ligament (dotted arrow), the posterior cruciate ligament (solid arrow), the fibular head (FH), the Gerdy tubercle (Gt), and the lateral collateral ligament (LCL). Reprinted with permission from Helito et al. 22
The ALL may also have insertions on the lateral meniscus around its midpoint. As the ligament runs from proximal to distal, tibial and meniscal bifurcations have been identified (Figure 2). One MRI study classified meniscal attachments into complete, central, bipolar, or inferior-only, suggesting variability. 37 This remains controversial and is not consistently found. The ALL is, on average, 35 to 40 mm in length and 1 to 3 mm thick.11,22,71 The width varies from 4 to 11 mm at the origin, 4 to 8 mm at the midpoint, and 11 to 12 mm near its broad insertion.10-12
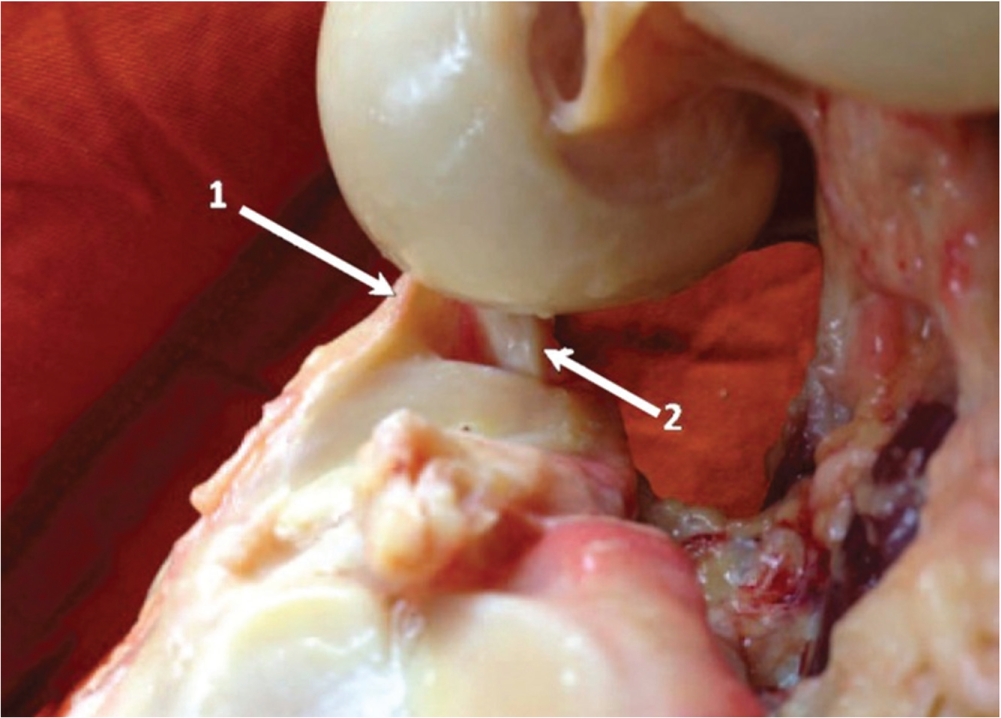
Lateral section of the right knee showing a triangular image with a distal base formed by the tibia, popliteus tendon (2), and meniscal portion of the anterolateral ligament (1). Reprinted with permission from Helito et al. 22
Histological analysis of the ALL revealed dense connective collagenous tissue with evidence of meniscal insertions.21,22,71 One study used immunohistochemistry to stain ALL tissue for neural filament protein, suggesting peripheral nerve innervation or a mechanoreceptor function for the ALL. 40 The implications of this have yet to be investigated.
As highlighted by the many variable anatomic characteristics, controversies remain. Many debate the fundamental idea of whether the ALL is a separate ligament or if it is a thickening of the anterolateral capsule. 16 The inconsistencies may arise from differences in the dissection technique or in defining the layers of the anterolateral knee anatomy. Interpersonal variability based on age, sex, and other patient-specific factors may play a role and has yet to be studied.
Imaging
Radiography
The purpose of radiographs is limited to identifying radiographic landmarks for the ALL anatomy using dissected cadaveric knees. This utility has potential application for anatomic ALL reconstruction. The lateral radiograph seems to be the most useful view to mark out landmarks for the ALL. On this view, the origin on the femur is described as approximately 50% of the anteroposterior (AP) distance from the posterior femoral cortex and slightly distal (3.7-9 mm) to the Blumensaat line (Figure 3).18,23,51 The insertion on the tibia is described as about 50% of the AP distance from the anterior edge of the tibial plateau.18,23,51 On the AP view, the femoral origin is described as 15 to 16 mm proximal from the line drawn perpendicular to the distal femoral condyles, and the insertion on the tibia is 7 to 14 mm distal to the lateral tibial plateau.18,23,51
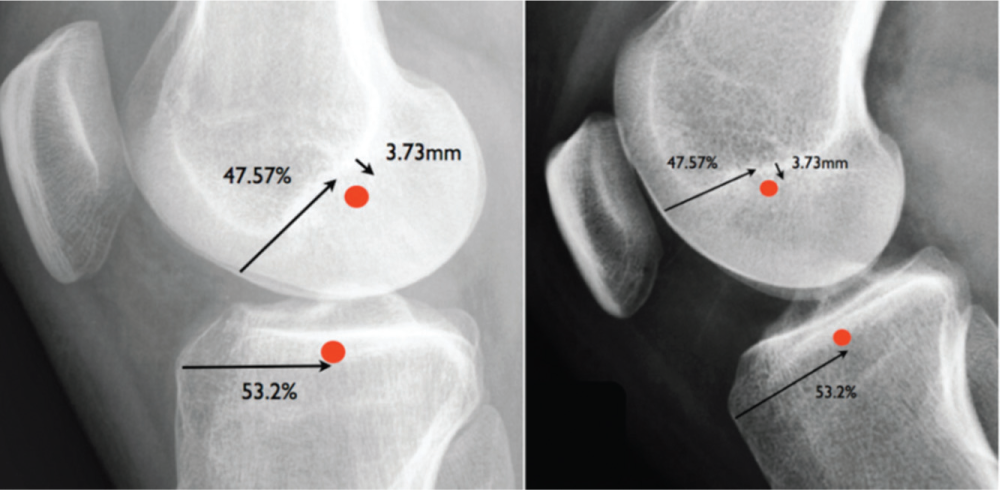
Radiograph of the knee in the absolute lateral view showing the midpoint of the origin of the anterolateral ligament (ALL) relative to the x- and y-axes and the midpoint of the insertion of the ALL relative to the tibial axis. Reprinted with permission from Helito et al. 23
Ultrasound
The extra-articular location of the ALL makes ultrasound a plausible tool for identification. Only a few studies have sought to use ultrasound. Most studies are able to identify at least part of the ALL on ultrasound, but studies conflict whether insertion and origin points can be accurately pinpointed.4,6 It is also difficult to differentiate the ALL from the posterior iliotibial band (ITB) and anterolateral capsule. 4 Identification of the ALL is enhanced with knee flexion and tibial internal rotation (IR). 8 Whether ALL injuries can be diagnosed with ultrasound routinely remains a question.
Magnetic Resonance Imaging
MRI is a useful modality to identify ligamentous and soft tissue. The T2 proton density–weighted sequence provides the most optimal view as a hyposignal through coronal-plane slices. The femoral, meniscal, and tibial portions of the ALL are visible on MRI (Figure 4). At least 1 portion was seen 51% to 100% of the time, whereas all 3 portions were seen less often.5,9,24,25,27,37,49,66 The insertion on the proximal lateral tibial plateau just distal to the joint line was well identified in nearly all studies. The origin on the lateral distal femur was difficult to visualize, which is likely because of the close proximity of LCL fibers. Real-time virtual sonography is a technique that synchronizes ultrasound and MRI to provide real-time detailed imaging. A single study found good identification of ALL insertion thickness and length but had difficulty in identifying the origin on the femur. 46
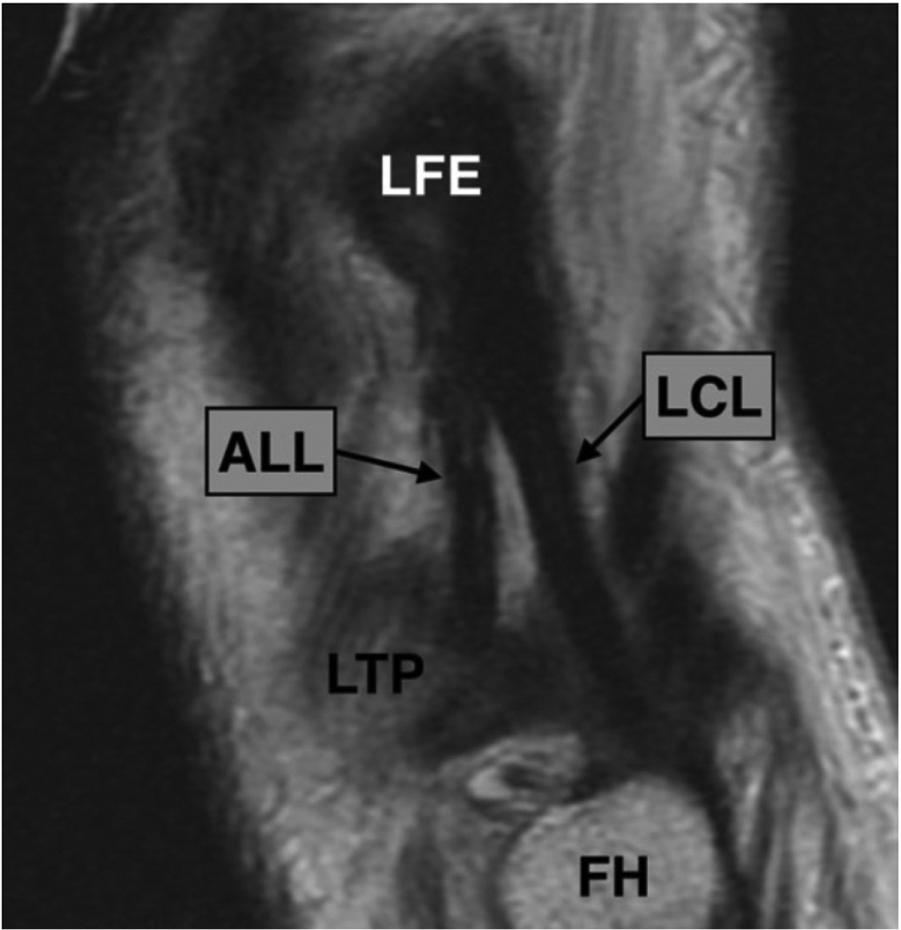
Sagittal proton density–weighted section of the right knee showing the relationship between the anterolateral ligament (ALL) and the lateral collateral ligament (LCL). FH, femoral head; LFE, lateral femoral epicondyle; LTP, lateral tibial plateau. Reprinted with permission from Helito et al. 25
It is suggested that MRI performed on injured knees provides better visualization of the ALL. Soft tissue inflammation and joint effusion may provide signal intensification, leading to this observation. Furthermore, studies varied between using 1.5-T and 3.0-T MRI machines. While it has been postulated that 3.0-T MRI may provide increased visualization, one study did not find a statistical difference. 28 However, it is not known how chronic knee ligamentous (ACL/posterior cruciate ligament) and ALL injuries affect visualization of the ALL. Interestingly, one study was able to better visualize the femoral portion of the ALL in male specimens and also found a longer ALL in male specimens, but this remains to be confirmed. 40 The inherent variability in identifying the ALL in anatomic dissections as discussed previously may also explain the range of findings seen in MRI studies.
There is disagreement about identifying ALL attachments to the lateral meniscus. Some studies found no meniscal attachments, 66 whereas others found them in all knees.5,37,49 One study subclassified patterns of meniscal attachments to the ALL into complete, central, bipolar, and inferior-only as seen on coronal-plane slices. 37 It is unknown whether this pattern of attachment has any clinical implications.
An avulsion fracture of the proximal lateral tibial plateau or Segond fracture is thought to be closely associated with the ALL. One study found the posterior ITB and anterior oblique band (known as the ALL) attached to the Segond fracture fragment. 3 Another study compared radiological data from MRI with Segond fractures to cadaveric dissections, determining the ALL footprint, and suggested that the ALL attaches to the Segond fracture. 10
The real utility of MRI lies in the ability to identify disruptions in the ALL after knee injuries to potentially help in deciding ligament reconstruction options. There is a high rate (37.5%-78.8%) of ALL abnormalities on MRI when an ACL tear is present.9,16,28,58 MRI studies have reported up to a 95% to 100% rate of ACL tears when there is an associated Segond fracture.10,13 Another study found disruptions of the anterolateral capsule in 51% of ACL injuries on MRI, which correlated to an increase in pivot-shift translation. 43 Studies have found ALL injuries in the proximal and distal ligaments as well as distal bony avulsions (Segond fractures). 9 Other associated injuries are variably reported but include medial collateral ligament tears, medial and lateral meniscal tears, posterolateral corner injuries, and bony contusions.13,17,69 One study found poor interrater reliability between musculoskeletal radiologists in identifying ALL abnormalities. 17
Biomechanics and Function
Biomechanical Properties
The ALL is considerably weaker than the cruciate and collateral ligaments of the knee. The load to failure (maximum load) is roughly 50 to 200 N.20,34,73 The tension is 32.78 N/mm2, and stiffness is 20 to 41.9 N/mm.20,34,73 It can deform 30% of the length before failure. 20 The sites of failure within the ALL can include soft tissue injuries, ranging from femoral to midsubstance or tibial, or as a bony Segond fracture.
The ALL is proposed to provide rotational stability to the knee. This is controversial in the literature as the ITB and anterolateral capsule may also play a similar role, and studies have conflicting reports.36,52 ITB injuries are not typically seen with concomitant ACL injuries, so the clinical relevance remains to be questioned. Most studies indicate that the ALL undergoes nonisometric length increases with increased knee flexion and tibial IR,26,35,39 although one anatomic study found isometric lengthening during 0° to 60° of knee flexion but decreasing length from 60° to 90°. 15 Tibial IR results in larger magnitude ALL length increases than knee flexion.
Role of ALL in ACL-Deficient Knee
The function of the anterolateral structures is highly controversial. Studies seem to indicate that the ALL is a restraint to tibial IR, but less so to anterior tibial translation, which is predominantly controlled by the ACL.2,47,50,52,61,63 The ACL seems to control tibial IR in early flexion (0°-30°), while the ALL takes over in deeper flexion (30°-90°). 47 Conflicting studies argue that the ALL may be a secondary knee stabilizer as it bears loads only beyond normal physiological motion in an ACL-deficient knee. 67 Kittl et al 36 argued that the ITB is the primary restraint to IR. However, this has been called into question on the basis of the variability in defining the ALL and dissection technique.
Studies have suggested that ALL deficiency results in a higher grade pivot shift compared with an ACL tear alone.42,61 However, one study did not find increased IR with pivot shift but rather an increase in acceleration of the lateral tibial compartment, which has been clinically correlated with pivot-shift changes.2,38 One study found increased pivot shift in patients with MRI evidence of anterolateral capsule, medial meniscal, and lateral meniscal tears. 43
Combined ALL and ACL Reconstruction
Most cadaveric studies suggest that combined ALL and ACL reconstruction improve rotational stability of the knee compared with ACL reconstruction alone. Nitri et al 44 found improved rotatory stability with combined ALL and ACL reconstruction. While one study found no decrease in IR or improvement in pivot shift after ALL reconstruction in cadaveric knees, the ACL was not concurrently reconstructed in this study. 59 Future studies comparing autograft, allograft, and synthetic reconstruction grafts are needed.
Lateral extra-articular tenodesis reconstruction was previously utilized to control rotational stability of the knee as a supplement to ACL reconstruction. However, a major concern was overconstraining the lateral knee, which may lead to decreased range of motion (ROM), stiffness, and/or lateral compartment osteoarthritis.14,41,48 This led to it falling out of favor. These concerns remain with ALL reconstruction, regardless of the ALL graft fixation angle. 55 However, this study used a traction force of 88 N, which may have led to the finding. 60 In addition, the overconstraint was measured as 1° to 2°, which may not be clinically relevant. 60 On the contrary, cadaveric studies are inherently limited by the lack of graft incorporation, soft tissue stretching, and lack of other associated capsuloligamentous and soft tissue injuries seen in ACL tears.45,64 A retrospective clinical study of combined ALL and ACL reconstruction did not find limitations in ROM. 62 However, prospective clinical studies in humans are needed.
ALL Reconstruction Techniques
Initial studies have examined the ALL to understand optimal reconstruction techniques. An ITB graft was found to resemble the native ALL most closely compared with a 2-strand gracilis graft. 72 The 2-strand gracilis graft had a higher load to failure and was stiffer than the ALL; however, a single-strand gracilis graft was not tested in this study.
Anatomic and MRI studies have not consistently found the exact location of the ALL origin on the femur. Whether an origin on the LFE, posterior/proximal or anterior/distal to the LCL origin, is optimal for reconstruction is unknown for this reason. With an ALL origin posterior/proximal to the LCL origin, the ALL was tight in extension, tight with IR at 30° of flexion, but relaxed at 120° of knee flexion and IR at 90° of flexion. 31 Another study found similar results when comparing tension changes. 33 Schon et al 55 chose a posterior/proximal starting point but found overconstraint of the knee at all fixation angles between 0° and 90° of flexion. No differences in anterior drawer, pivot-shift, and IR tests were found among the groups. An in vivo study modeled origin points using MRI and dual fluoroscopy techniques but found that length changes in the ALL were not isometric. 68
Surgical Reconstruction Techniques
A few studies have started to describe techniques for ALL reconstruction. Helito et al 19 described combined ACL reconstruction with extra-articular ALL reconstruction. They reported using either autograft or allograft hamstring tendons to form a quadruple ACL graft and part of the gracilis for the ALL graft. An incision over the iliotibial tract was made between the lateral femur and midway between the Gerdy tubercle and the fibular head. The ALL graft was anchored onto the landmark found on a lateral knee radiograph about 3 to 4 mm distal to the midpoint along the Blumensaat line. ACL reconstruction was then performed with arthroscopic assistance, and fixation was performed with the knee in 30° of flexion. The ALL graft was passed under the iliotibial tract and inserted into the tibia midway between the Gerdy tubercle and the fibular head. This point could be found on an AP knee radiograph 7mm distal to the lateral tibial plateau and midway along the tibial plateau on a lateral knee radiograph. The graft was fixed to the tibia between 60° and 90° of knee flexion.
Smith et al 57 also described a technique using hamstring autografts. The femoral origin was anterior to the LFE. The tibial insertion was similar to that in the previous study, except that the point was 11 mm distal to the joint line. In addition, 2 small skin incisions were made directly over the attachment sites on the femur (transverse) and tibia (longitudinal). After this, ACL reconstruction was performed using an all-inside technique. At the femoral origin, a 2.4-mm guide wire was passed anterior and proximal from an entry point anterior and superior to the LCL, and a 4.5-mm drill hole was made 25 mm deep. A similar drill hole was made aimed medially and inferiorly into the tibia. The ALL graft was fixed in the femur using 4.75- or 5.5-mm bioabsorbable knotless anchors. The tibial portion of the graft was modified to include a snare suture. The graft was passed under the ITB and fixed into the tibia with the knee at 30° of flexion and neutral foot rotation.
Although arthroscopic ALL reconstruction has not been described, one study reported an arthroscopic technique to identify the ALL. 59 The arthroscope was placed in an anterolateral portal to view the lateral gutter. A shaver was inserted through an accessory portal over the inferior portion of the lateral gutter. Once the synovial recess was shaved, the ALL was visible. The clinical ramifications of this approach to the ALL are yet to be determined.
Clinical Outcomes
There has been only one study, with 92 patients and 2-year follow-up, reported after combined ALL and ACL reconstruction. 62 ALL reconstruction was performed with a single femoral origin but a broader “double-bundle” tibial insertion (Figure 5). International Knee Documentation Committee and Lysholm scores were improved in patients with combined surgery, with no reports of limited ROM. One patient had an ACL graft rupture, and 7 had contralateral ACL ruptures. About 71% of the patients returned to the same activity level. Most patients who returned to a lower level of activity reported reasons unrelated to the injured knee, while 10 had anterior knee pain, painful tibial tunnels, or apprehension.
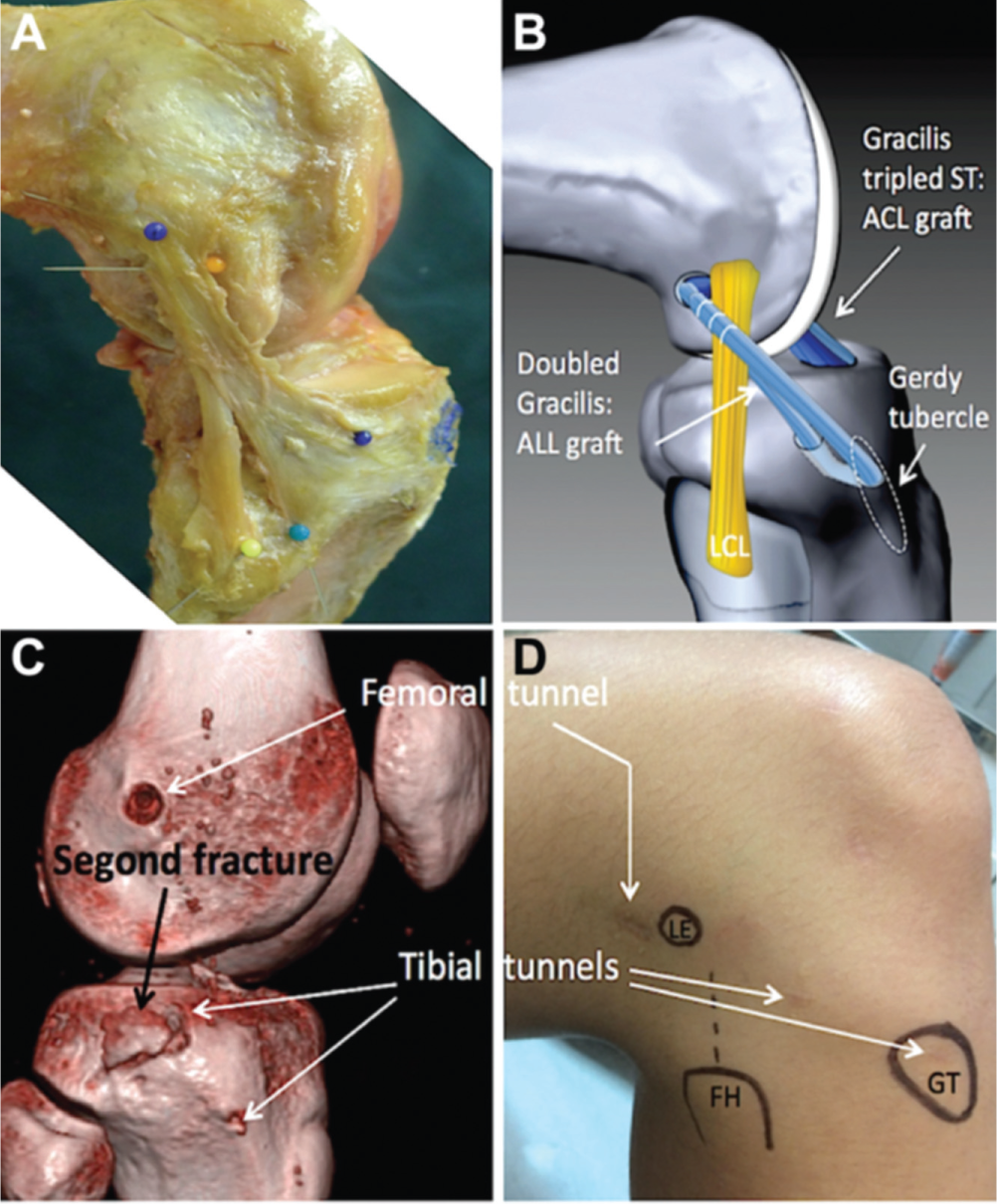
Images of the anterolateral ligament (ALL), the site of the graft, and its surrounding structures. (A) Anatomic, (B) graphic, (C) 3-dimensional computed tomography, and (D) surface markings. ACL, anterior cruciate ligament; FH, femoral head; GT, Gerdy tubercle; LE, lateral epicondyle. Reprinted with permission from Sonnery-Cottet et al. 62
Future Directions
Despite recent renewed interest in the ALL, many questions remain regarding this structure and its role in knee injuries. It is still unclear whether the ALL is a distinct ligament or an extracapsular thickening. Anatomic and biomechanical studies should focus on the anterolateral knee structures. Advanced imaging techniques should be developed to better identify ALL injuries. Given the variability seen among studies, ALL variants and differences among populations should be explored. The clinical importance of the ALL in the setting of ACL injuries remains unclear. Finally, the results of techniques for surgical reconstruction are just now being reported, and while early results appear promising, long-term, comparative clinical studies are needed.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.H.B. was a paid speaker for Arthrex.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.