
Abstract
Background:
The optimal treatment for middle-aged patients with knee pain and meniscal lesions has been extensively debated. Most previous studies have revealed only short-term beneficial results of knee arthroscopic surgery. The authors have previously shown a positive benefit of knee arthroscopic surgery and an exercise program after 1 year when compared with an exercise program alone.
Purpose:
To evaluate if knee arthroscopic surgery combined with an exercise program provided an additional long-term benefit after 3 years compared with an exercise program alone in middle-aged patients with meniscal symptoms.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
Of 179 eligible patients, aged 45 to 64 years, 150 were randomized to (1) a 3-month exercise program (nonsurgery group) or (2) the same as group 1 plus knee arthroscopic surgery within 4 weeks (surgery group). The primary outcome was the change in the Knee Injury and Osteoarthritis Outcome Score (KOOS) subscore of pain between baseline and the 3-year follow-up. Results from the 1-year follow-up have been published previously.
Results:
Both treatment groups improved significantly in the KOOS pain subscore at 3 years’ follow-up in the intention-to-treat and as-treated analyses (P < .001). The between-group difference for the change in the KOOS pain subscore between baseline and the 3-year follow-up was no longer statistically significant, neither in the intention-to-treat analysis (7.6 points; 95% CI, –0.6 to 15.9; P = .068) nor in the as-treated analysis (5.3 points; 95% CI, –3.1 to 13.8; P = .216). The factorial analysis of the effect of the intervention and age, onset of pain, and mechanical symptoms indicated that older patients improved more, regardless of treatment, and surgery may be more beneficial for patients without mechanical symptoms (as-treated analysis). The effect of the predictive factors on the KOOS pain subscore was uncertain because of the small sample size in the subgroup analyses.
Conclusion:
The benefit of knee arthroscopic surgery, seen at 1 year in middle-aged patients with meniscal symptoms, was diminished at 3 years and was no longer statistically significant.
Clinical Relevance:
Knee arthroscopic surgery may be beneficial for middle-aged patients with meniscal symptoms in addition to an exercise program. Older age and absence of mechanical symptoms should not be contraindications to surgery.
Registration:
NCT01288768 (ClinicalTrials.gov identifier)
In middle-aged patients, pain, locking, catching, and impaired function of the knee are common symptoms related to cartilage and meniscal lesions, which are parts of degenerative changes in the knee joint. 7 Meniscal tears are also common in nonsymptomatic middle-aged people, 6 and there have been controversies in recent years about the optimal treatment of knee pain and meniscal lesions in this population. § Comprehensive reviews suggested that exercise has at least a slight short-term effect. 10 Exercise reduces knee pain and improves physical function in patients with knee osteoarthritis (OA).10,22,24,38 The positive effect from exercise is likely caused by a combination of increased muscle strength, proprioception, and improvement in range of motion. 33
In addition to exercise, knee arthroscopic surgery is a treatment option, and its effect may depend on the removal of loose fragments of meniscus, cartilage, and other soft tissues or a washout of cytokines.2,28 Most cohort studies have shown good clinical results after arthroscopic surgery for meniscal symptoms.1,4,34 Knee arthroscopic surgery may be superior to nonoperative treatment for a 6-month period, although only the randomized clinical trial from our research group demonstrated a statistically and clinically significant positive effect of knee arthroscopic surgery and an exercise program after 1 year versus an exercise program alone. 11 The other randomized studies have not shown any significant benefit in relation to exercise or sham surgery after 1 year or longer.13,14,18,21,22,36,38,40 The present study is a follow-up of our previous study, 11 which presented short-term and midterm effects at 3 months and 1 year. The primary aim of this study was to evaluate whether knee arthroscopic surgery combined with an exercise program could provide additional long-term benefit at the 3-year follow-up, compared with an exercise program alone, in middle-aged patients with meniscal symptoms.
Methods
Study Design and Participants
Participants were recruited from the Department of Orthopaedics at Linköping University between 2010 and 2012. For this study, one orthopaedic surgeon (H.G.) evaluated all referred patients with a suspected meniscal injury for eligibility. Inclusion criteria were age 45 to 64 years, symptoms lasting more than 3 months, standing radiographs with Ahlbäck grade 0 (<50% reduction of the joint space, without consideration of possible osteophytes), and prior physical therapy. All consecutive patients who fulfilled the inclusion criteria and did not meet any exclusion criteria were invited to participate in the study (Figure 1). Details about the recruitment process were published previously. 11 The study was approved by the ethics committee at Linköping University (Dnr M2010/6-31).
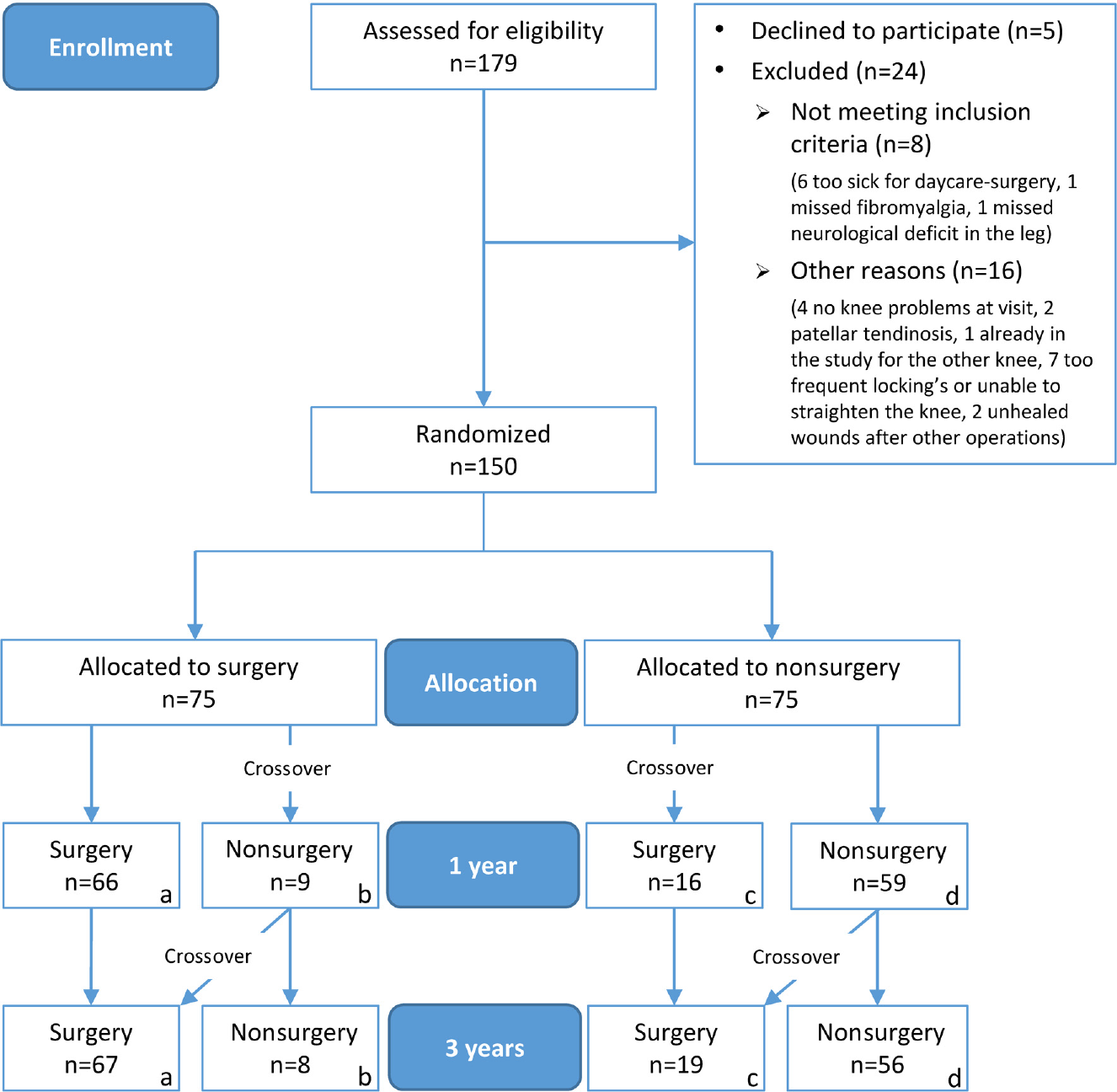
Patient enrollment and randomization. Exclusion criteria were locked knee or joint locking for more than 2 seconds more often than once a week, rheumatic or neurological disease, fibromyalgia, replacement of hip or knee joints, or a contraindication to surgery at the day surgery clinic (body mass index >35 kg/m2 or a serious medical illness). Groups analyzed in the intention-to-treat analysis: (A, B) surgery group and (C, D) nonsurgery group. Groups analyzed in the as-treated analysis: (A, C) surgery group and (B, D) nonsurgery group.
The participants were randomly allocated to 1 of 2 parallel intervention groups. One group (nonsurgery) received a physical therapy session within 2 weeks, with a functional assessment and instructions for an exercise program. The other group (surgery) received the same physical therapy treatment within 2 weeks as the nonsurgery group plus underwent knee arthroscopic surgery within 4 weeks of inclusion. Any significant meniscal injuries were resected during arthroscopic surgery. The orthopaedic surgeon who enrolled and assessed participants was blinded to the allocation sequence. The allocations were placed in sequentially numbered, opaque, sealed envelopes in 15 blocks, with a block size of 10. Envelopes were opened after enrollment by the patient and a nurse.
Interventions
The exercise program aimed to increase muscle function and postural control and lasted for 3 months. The physical therapy sessions were held at an independent physical therapy clinic. Patients received full or local anesthetics during surgery, which was performed by 1 of 2 experienced arthroscopic surgeons at an independent day surgery clinic. The surgeons judged, according to their experience, whether meniscal resection was indicated. All patients could perform full weightbearing activities immediately after surgery. Detailed information about the interventions was published previously. 11
Outcome Measures
Before randomization (baseline), the orthopaedic surgeon assessed the symptom history, onset of pain (eg, sudden onset, the patient could tell that the pain started during a particular activity), daily joint catching, and joint locking for more than 2 seconds over the past month. Then, the patient sat alone to complete the evaluations, including the Knee Injury and Osteoarthritis Outcome Score (KOOS) and EuroQol 5 dimensions (EQ-5D). Patients completed the same questionnaires at 3 months, 1 year, and 3 years after baseline. There were no planned follow-up visits for the patients at the orthopaedic clinic. Patients completed all follow-up questionnaires at home and returned them to a nurse in an envelope with prepaid postage. The primary endpoint for the main study was the 1-year follow-up, and the primary outcome was the change in the KOOS subscore of pain between baseline and the 1-year follow-up. For the present 3-year follow-up study, the outcomes were analyzed with a prolonged follow-up time. Detailed information about the outcomes was published previously. 11
Adverse Events
We identified adverse events using the 3-year questionnaire and a review of the electronic medical records after 3 years. All hospitals including ours, the independent day surgery clinic, and the general practitioners in the catchment area have common electronic records. These were checked for the first time at 1 year and for a second time at 3 years. There had been 2 revision arthroscopic surgeries in the surgery group; 1 participant underwent revision resection of the medial meniscus at 10 months and 1 participant at 21 months after inclusion. There were no reports of deep venous thrombosis, infections, or other complications. One patient in the surgery group, who underwent arthroscopic surgery in March 2011, died in 2014.
Statistical Analysis
Both the intention-to-treat and as-treated approaches were used. Data were analyzed using SPSS Statistics for Windows (Version 22.0; IBM Corp), and all analyses were 2-sided with the significance level set at P < .05. The Student t test was used for between-group comparisons of the KOOS, EQ-5D index, EuroQol visual analog scale (EQ-VAS), and age at baseline at each follow-up and for the change in scores. Within-group changes between time points were analyzed with the paired-samples t test. Between-group differences in the duration of knee pain at baseline were estimated with the Mann-Whitney U test. Categorical data were analyzed with the Pearson chi-square test or Fisher exact test. Two-way analysis of variance (ANOVA) was used to analyze the effect of the intervention and the predefined factors: (1) sudden onset of pain, (2) mechanical symptoms (ie, daily joint catching and/or joint locking for more than 2 seconds in the past month), or (3) the effect of age ≥55 years on the change in the KOOS pain subscore between baseline and 3-year follow-up. Three separate models were estimated, and each model included the intervention plus one predefined factor and a 2-way interaction between the 2 binary variables. A minimal clinically important change of 8 to 10 points is considered appropriate for the KOOS pain subscore. A 10-point change was used as the cut-off indicating recovery. 30 To detect a mean (±SD) between-group difference of 10 ± 19 points in the KOOS pain subscore (α = .05, β = .8), we included 75 participants in each group; this accounted for a crossover and dropout rate of 33%.
Results
Study Participants
Participants were randomly assigned to either the surgery (n = 75) or nonsurgery (n = 75) group. Nineteen patients (25%) crossed over from the nonsurgery group to undergo surgery, with 3 of them after the 1-year follow-up. Eight patients (11%), allocated to the surgery group, did not go through with surgery (Figure 1). The 1-year questionnaire was completed by 130 patients (87%) and the 3-year questionnaire by 119 patients (79%). Patient baseline characteristics and OA severity, according to the Kellgren-Lawrence classification, are presented in Appendix Table A1 (available in the online version of this article).
Patient Characteristics and Baseline Data
In the intention-to-treat analysis, there were no differences in patient characteristics or KOOS subscores at baseline (Table 1 and Appendix Table A1). In the as-treated analysis, the surgery group had a higher proportion of women (36% vs 16%, respectively; P = .006) (Appendix Table A1) and had a worse mean KOOS sports subscore than the nonsurgery group at baseline (26 ± 19 vs 36 ± 25 points, respectively; P = .010) (Appendix Table A2).
Primary and Secondary Outcomes in Intention-to-Treat Analysis a
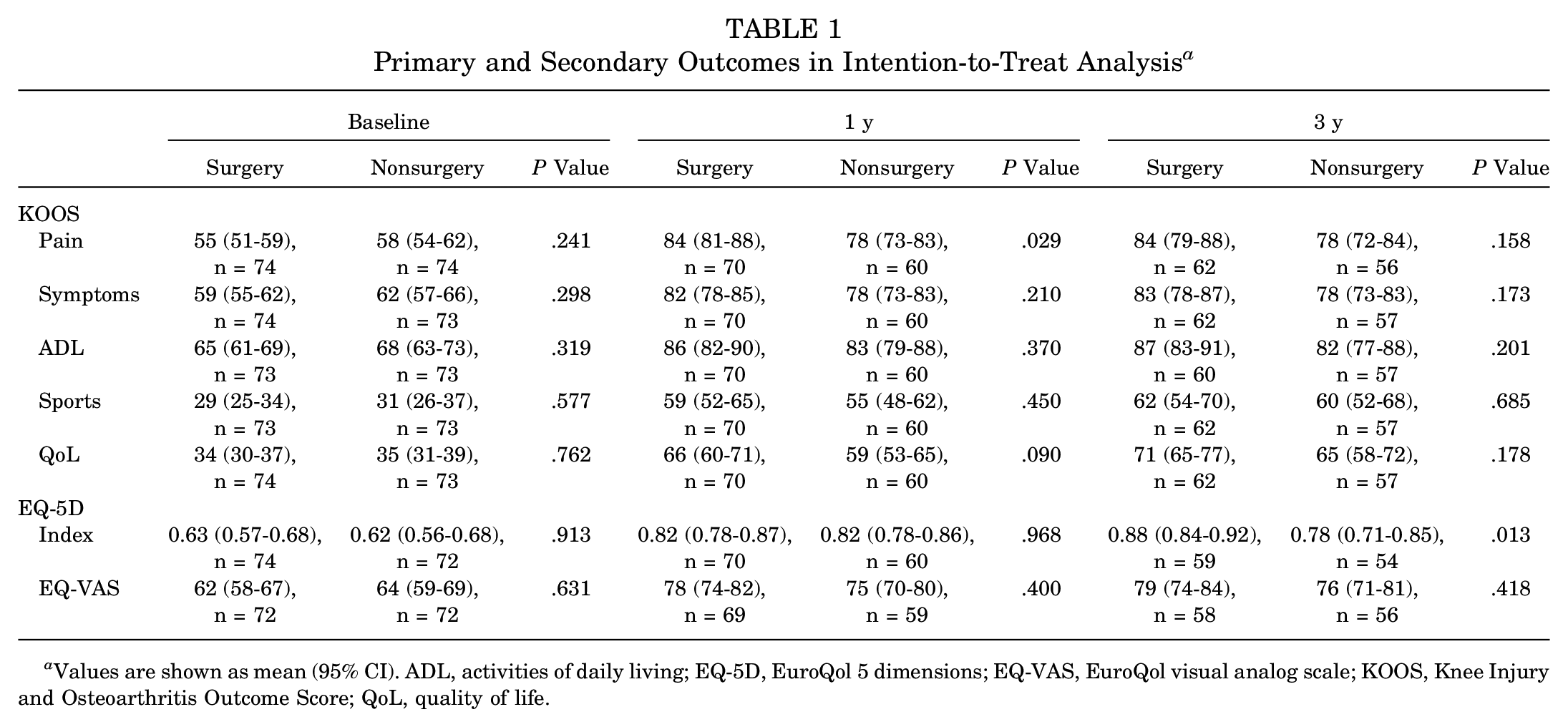
Values are shown as mean (95% CI). ADL, activities of daily living; EQ-5D, EuroQol 5 dimensions; EQ-VAS, EuroQol visual analog scale; KOOS, Knee Injury and Osteoarthritis Outcome Score; QoL, quality of life.
Primary Outcome
There was a nonsignificant between-group difference in the change in the KOOS pain subscore between baseline and the 3-year follow-up in both the intention-to-treat analysis (7.6 points; 95% CI, –0.6 to 15.9; P = .068) (Table 2 and Figure 2) and as-treated analysis (5.3 points; 95% CI, –3.1 to 13.8; P = .216) (Appendix Table A3 and Appendix Figure A1). There was a significant improvement in both treatment groups in the KOOS pain subscore at the 3-year follow-up in both the intention-to-treat analysis (surgery group: 29.1 points; 95% CI, 23.6-34.5; P < .001) (nonsurgery group: 21.4 points; 95% CI, 15.1-27.7; P < .001) and as-treated analysis (surgery group: 27.6 points; 95% CI, 22.1-33.0; P < .001) (nonsurgery group: 22.2 points; 95% CI, 15.7-28.8; P < .001).
Change in Primary and Secondary Outcomes in Intention-to-Treat Analysis a
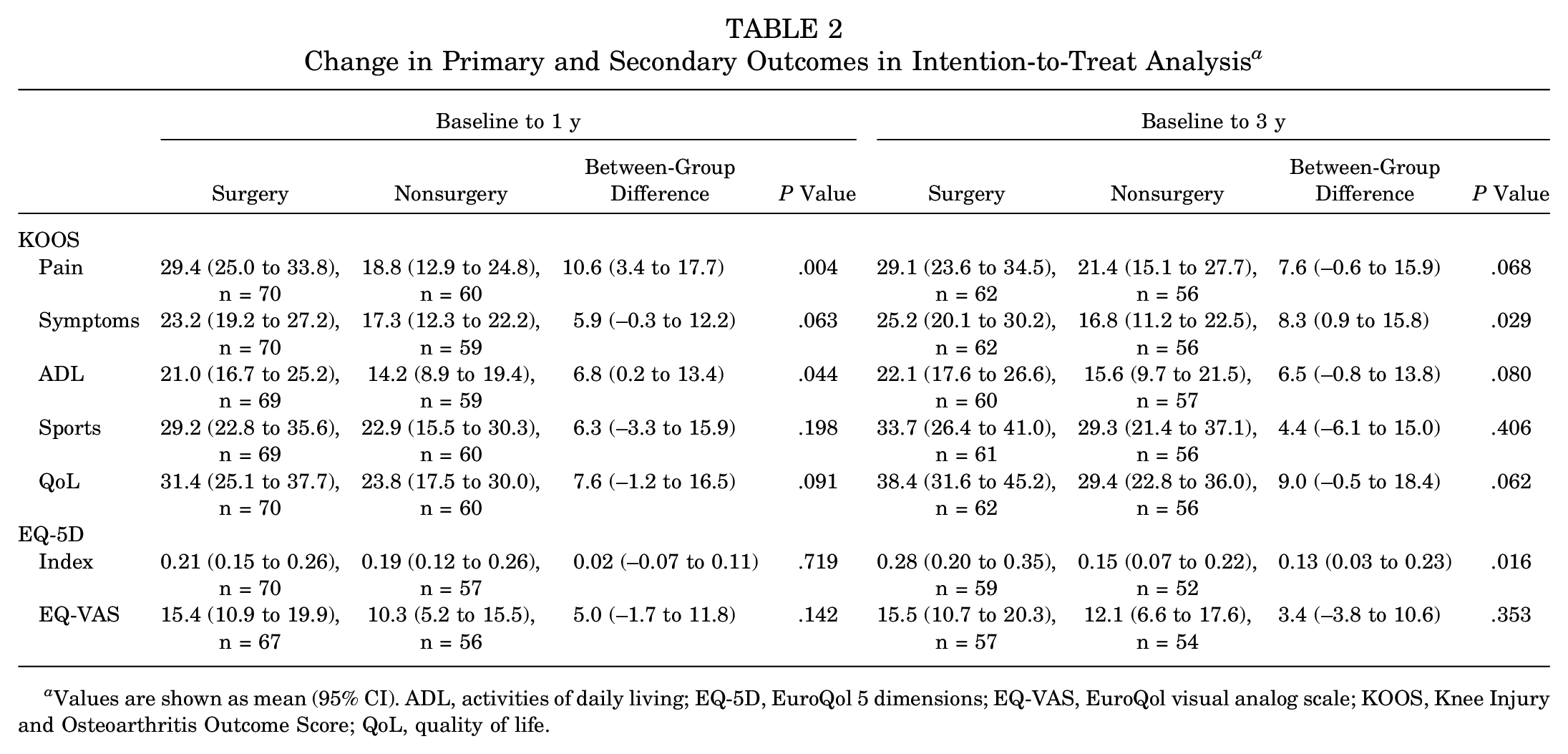
Values are shown as mean (95% CI). ADL, activities of daily living; EQ-5D, EuroQol 5 dimensions; EQ-VAS, EuroQol visual analog scale; KOOS, Knee Injury and Osteoarthritis Outcome Score; QoL, quality of life.
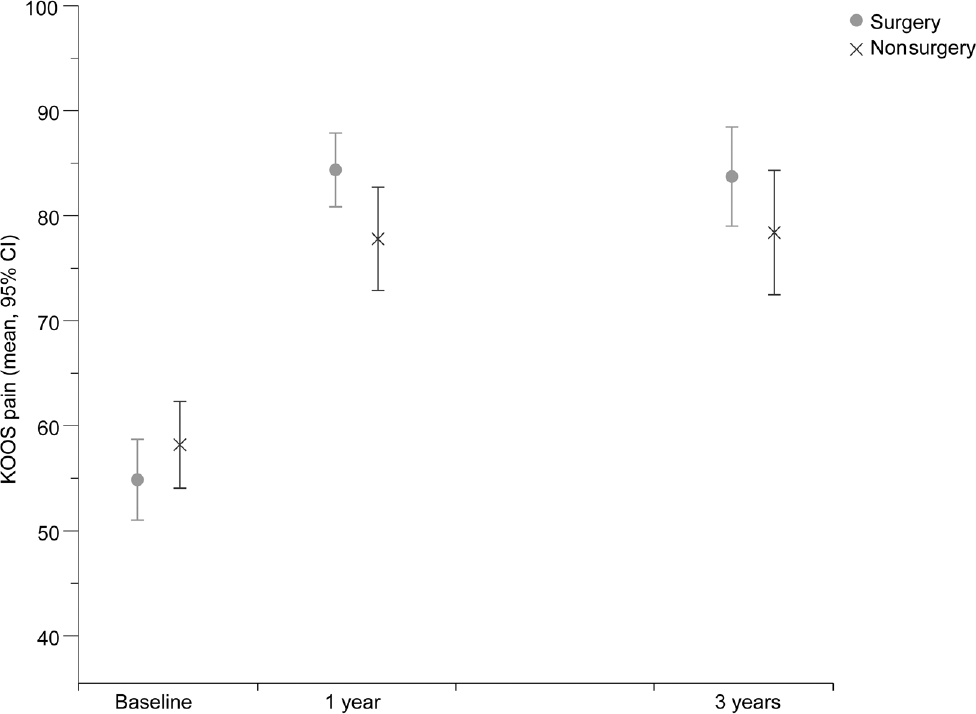
Mean Knee Injury and Osteoarthritis Outcome Score pain subscores at baseline, 1 year, and 3 years according to treatment group in the intention-to-treat analysis.
In the intention-to-treat analysis (Figure 3), 81% of the patients in the surgery group (50/62) improved by more than 10 points in the KOOS pain subscore at 3-year follow-up versus 73% of the patients in the nonsurgery group (41/56). In addition, no patient in the surgery group deteriorated by more than 10 points in the KOOS pain subscore at the same time point compared with 11% in the nonsurgery group (6/56) (Fisher exact test, 7.094; df = 2; P = .030). In the as-treated analysis (Appendix Figure A2), 77% of the patients in both the surgery group (55/71) and nonsurgery group (36/47) improved by more than 10 points in the KOOS pain subscore at the 3-year follow-up. In addition, 3% in the surgery group (2/71) versus 9% in the nonsurgery group (4/47) deteriorated by more than 10 points in the KOOS pain subscore at the same time point (Fisher exact test, 2.176; df = 2; P = .308).
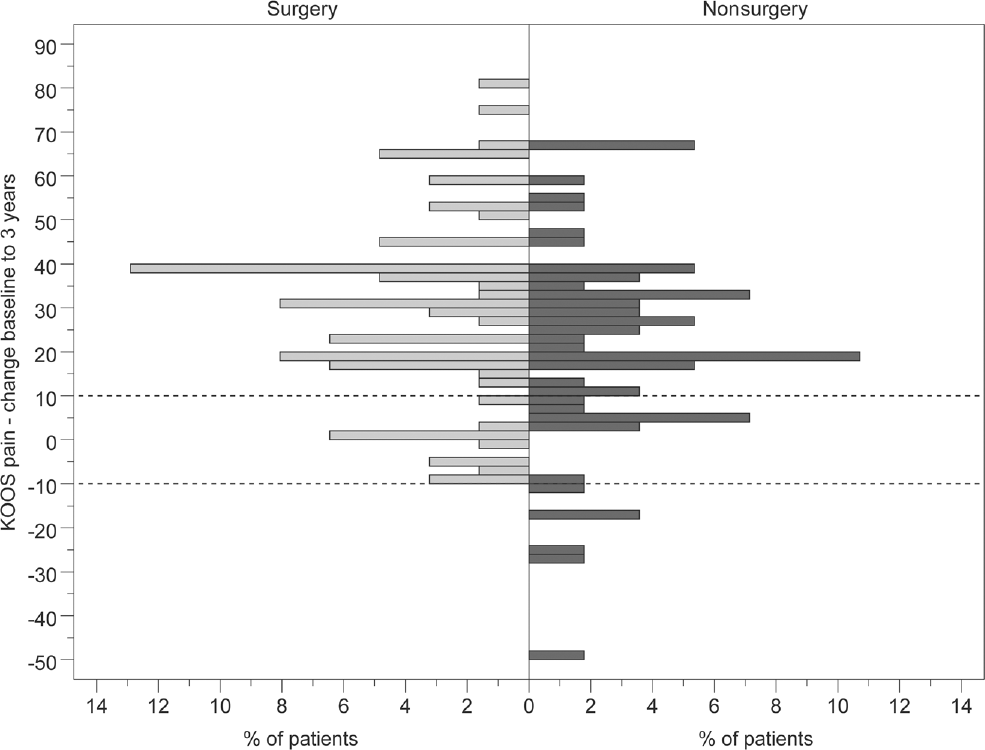
Percentage of patients in each group that showed the indicated change in the Knee Injury and Osteoarthritis Outcome Score pain subscore from baseline to 3 years in the intention-to-treat analysis. Dotted horizontal lines indicate a 10-point change from baseline.
The subgroup analysis of patients who completed the KOOS subscale for pain at both the 1-year and 3-year follow-ups revealed the following results. The intention-to-treat analysis (n = 59 surgery group; n = 52 nonsurgery group) showed a significantly larger improvement for the surgery group compared with the nonsurgery group at the 1-year follow-up (10.9 points; 95% CI, 3.3-18.4; P = .005). No between-group difference in change was found at the 3-year follow-up (6.0 points; 95% CI, –1.9 to 13.8; P = .137). In the as-treated analysis (n = 63 surgery group; n = 44 nonsurgery group), there was a significantly larger improvement at the 1-year follow-up in favor of the surgery group (9.6 points; 95% CI, 2.3-16.9; P = .010). No between-group difference in change was found at the 3-year follow-up (6.4 points; 95% CI, –1.6 to 14.4; P = .115).
Secondary Outcome
In the intention-to-treat analysis, the surgery group demonstrated a larger improvement at the 3-year follow-up in the KOOS symptoms subscore (8.3 points; 95% CI, 0.9-15.8; P = .029) and EQ-5D index (0.13 points; 95% CI, 0.03-0.23; P = .016) compared with the nonsurgery group (Table 2). In the as-treated analysis, the change in the EQ-5D index at 3-year follow-up was significantly greater in the surgery group (0.12 points; 95% CI, 0.01-0.23; P = .031) (Appendix Table A3). There was no other between-group difference in change found at the 3-year follow-up.
The results from 2-way ANOVA on the effect of the intervention and the predefined factors on the change in the KOOS pain subscore at 3-year follow-up are presented in Table 3 and Appendix Table A4. In the intention-to-treat analysis, age had a significant main effect on the change in the KOOS pain subscore at the 3-year follow-up after controlling for the intervention (F(1,114) = 6.7, P = .011). This indicates that patients aged ≥55 years improved more in the KOOS pain subscore than patients aged 45 to 54 years, regardless of treatment (10.5 points; 95% CI, 2.5-18.5; P = .011). There was no significant main effect of treatment or interaction effect between treatment and age on the change in the KOOS pain subscore. Sudden onset of pain had no main or interaction effect on the change in the KOOS pain subscore. Treatment had a significant main effect on the change in the KOOS pain subscore after controlling for mechanical symptoms (F(1,113) = 4.8, P = .030), indicating a larger improvement in the surgery group compared with the nonsurgery group (9.4 points; 95% CI, 0.9-17.9; P = .030), regardless of the presence or absence of mechanical symptoms. There was no significant main effect of mechanical symptoms or interaction effect between treatment and mechanical symptoms on the change in the KOOS pain subscore.
Change in KOOS Pain Subscore at 3-Year Follow-up a
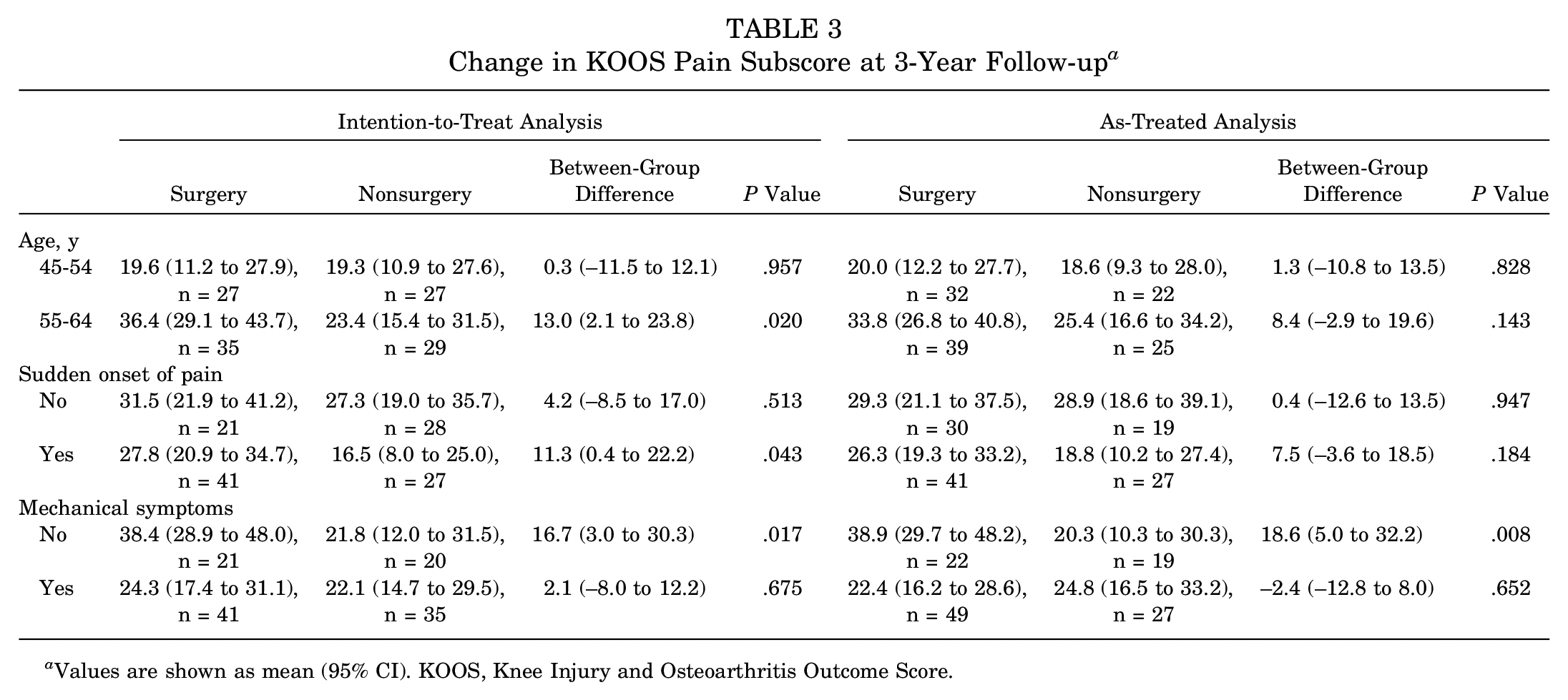
Values are shown as mean (95% CI). KOOS, Knee Injury and Osteoarthritis Outcome Score.
In the as-treated analysis, age had a similar main effect on the change in the KOOS pain subscore as in the intention-to-treat analysis (F(1,114) = 6.1, P = .015), indicating a larger improvement among patients aged ≥55 years compared with those aged 45 to 54 years, regardless of treatment (10.3 points; 95% CI, 2.0-18.6; P = .015). There was no significant main effect of treatment or interaction effect between treatment and age on the change in the KOOS pain subscore. Sudden onset of pain had no main or interaction effect on the change in the KOOS pain subscore. There was no significant main effect of either treatment or mechanical symptoms, but there was a significant interaction effect between the 2 variables on the change in the KOOS pain subscore at the 3-year follow-up (F(1,113) = 5.9, P = .017). This indicates that the effect of treatment differs depending on the presence or absence of mechanical symptoms. The effect of surgery was nonsignificant in the group with mechanical symptoms (2.4 points; 95% CI, –8.0 to 12.8; P = .652) but significant in the group without mechanical symptoms (18.6 points; 95% CI, 5.0 to 32.2; P = .008).
Discussion
The previous report of the present study showed that knee arthroscopic surgery provided more benefit to middle-aged patients with meniscal symptoms compared with no surgery, with a larger reduction in pain from baseline to 3 months and 1 year. 11 Other studies have only shown short-term effects up to 6 months and no effect after 1 year or longer.21,22,38 In line with these previous studies, we found that the superior improvement for the primary outcome in the surgery group, KOOS pain subscore, did not persist at a statistically significant level at the 3-year follow-up. However, the surgery group had a greater improvement at 3 years in the secondary outcome of the KOOS symptoms subscore for the intention-to-treat analysis and EQ-5D index for both the intention-to-treat and as-treated analyses when compared with the nonsurgery group. Furthermore, the effect of surgery was significant up to 3 years for the KOOS pain subscore in the group without mechanical symptoms (as-treated analysis).
The optimal treatments for middle-aged patients with knee pain and meniscal lesions have been extensively debated in recent years.3,14,20,22,23,27,36-38,40 We strongly believe, in line with the international guidelines, 29 that physical therapy in most instances should be the initial treatment in middle-aged patients with meniscal symptoms. Exercise therapy reduces knee pain and improves physical function10,24,37,38 possibly by increasing muscle strength, proprioception, and range of motion. 33 Physical exercise also has many other positive health effects and hardly any risks.8,17 Still, knee arthroscopic surgery may be beneficial for some patients because we were able to show that our patients had faster improvement after surgery and minimal adverse effects. A faster improvement meant that patients spent less time with pain, and this may facilitate increased physical activity and function.
Today, we are unable to predict which patients will benefit from knee arthroscopic surgery. It has been suggested that patients with mechanical symptoms of the knee, that is, joint catching and locking, may require surgery. 7 This has been questioned in a recent study. 35 In our previous study, 11 we specifically analyzed the effect of the mechanical factors, but we could not find any predictive value for an early selection of appropriate surgical candidates. In the present longer term follow-up, there was an unexpected result from the as-treated analysis that patients with mechanical symptoms treated with surgery had less benefit from the operative procedure. The cause of this finding is unknown. One explanation might be that it is not primarily a soft, degenerative rupture of the meniscus that causes catching and locking but the rugged, uneven cartilage. If so, catching could imply more pronounced OA and a worse prognosis. Patients aged ≥55 years experienced a larger improvement in both treatment groups compared with younger patients. Older patients may accept more symptoms before they are referred to the orthopaedic department. Accordingly, even older patients with more severe symptoms and without radiological signs of OA will improve over time to the same levels as younger ones. However, based on the sample size calculation, these analyses may be underpowered and should be interpreted with caution.
Despite the large improvement seen during the study period, regardless of treatment, patients in the present study scored 5 to 10 points lower in all KOOS subscales at the 3-year follow-up compared with reference data from the national population register. 26 This might indicate that the knee complaints may not be caused by a damaged meniscus alone but rather to other degenerative changes in the joint. The KOOS pain subscores in the present study are comparable with those of other cohorts undergoing meniscectomy at 3 months 32 and a cohort with slight posttraumatic OA. 31
No surgical procedure is complete without risks, but the disadvantages of knee arthroscopic surgery performed with modern techniques were insignificant when compared with a control group,18,36 and the procedure is affordable, especially when performed under local anesthetics in an outpatient setting. 9 Large, retrospective register studies12,15 probably exaggerated the risk because there was no comparison with a population of similar ages and knee-related symptoms and no surgery performed. Previous studies have shown an increased risk for cartilage defects after arthroscopic surgery in short-term 39 and long-term follow-ups.5,39 Our patients improved faster after knee arthroscopic surgery, and the adverse effects were minimal. In addition, more patients in the nonsurgery group deteriorated more than 10 points in the KOOS pain subscore (Figure 3). We are planning to include radiographic data for a 5-year follow-up to analyze if knee arthroscopic surgery affects the risk of developing OA.
The strengths of our study include the strict inclusion criteria, being a single-center study with access to the majority of the population, and a minor dropout rate. All caregiver contact was limited to the first 3 months during the inclusion process, exercise program, and possible surgery. The outcomes were patient reported, and the patients filled out the 3-month, 1-year, and 3-year questionnaires at home and returned them by mail. Only patients who wanted a crossover or revision arthroscopic surgery contacted the clinic. Moreover, almost all eligible patients agreed to participate in the study. This is important because excluding patients from the analysis in a randomized trial may bias the estimate of the treatment effect in an unpredictable way. 25 This study also had limitations. Twenty-five percent of participants in the nonsurgery group crossed over to undergo surgery, and 11% crossed over in the other direction. Only 79% of patients completed the 3-year questionnaire compared with 87% at 1 year. The number of patients who were lost to follow-up could have influenced the results.
In summary, the benefit of knee arthroscopic surgery seen at 1 year in middle-aged patients with meniscal symptoms and no radiographic OA was diminished at 3 years and was no longer statistically significant compared with patients who only completed an exercise program. Older patients improved to the same levels as younger patients, regardless of treatment. Patients without mechanical symptoms may benefit more from surgery, and the absence of mechanical symptoms should not be a contraindication to surgery. However, the results of 2-way ANOVA are uncertain because of the small sample size in the subgroup analyses.
Footnotes
Acknowledgements
The authors thank the orthopaedic surgeons, Magnus Lundberg and Jonas Holmertz, at Medicinskt Centrum, Linköping, for performing the arthroscopic procedures, and the physical therapists, Johan Carlsson, Peter Edenholm, Marcus Egelstig, and Marie Ryding-Ederö, at Linköping Health Care who performed the physical therapy sessions.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.