
Abstract
Background:
There is considerable debate on the recovery of rotator cuff muscle atrophy after rotator cuff repair.
Purpose:
To evaluate the serial changes in supraspinatus muscle volume after rotator cuff repair by using semiautomatic segmentation software and to determine the relationship with functional outcomes.
Study Design:
Case series; Level of evidence, 4.
Methods:
Seventy-four patients (mean age, 62.8 ± 8.8 years) who underwent arthroscopic rotator cuff repair and obtained 3 consecutive (preoperatively, immediately postoperatively, and later postoperatively [≥1 year postoperatively]) magnetic resonance imaging (MRI) scans having complete Y-views were included. We generated a 3-dimensional (3D) reconstructed model of the supraspinatus muscle by using in-house semiautomatic segmentation software (ITK-SNAP) and calculated both the 2-dimensional (2D) cross-sectional area and 3D volume of the muscle in 3 different views (Y-view, 1 cm medial to the Y-view [Y+1 view], and 2 cm medial to the Y-view [Y+2 view]) at the 3 time points. The area and volume changes at each time point were evaluated according to repair integrity. Later postoperative volumes were compared with immediately postoperative volumes, and their relationship with various clinical factors and the effect of higher volume increases on range of motion, muscle power, and visual analog scale pain and American Shoulder and Elbow Surgeons scores were evaluated.
Results:
The interrater reliabilities were excellent for all measurements. Areas and volumes increased immediately postoperatively as compared with preoperatively; however, only volumes on the Y+1 view and Y+2 view significantly increased later postoperatively as compared with immediately postoperatively (P < .05). There were 9 patients with healing failure, and area and volume changes were significantly less later postoperatively compared with immediately postoperatively at all measurement points in these patients (P < .05). After omitting the patients with healing failure, volume increases later postoperatively became more prominent (P < .05) in the order of the Y+2 view, Y+1 view, and Y-view. Volume increases were higher in patients who healed successfully with larger tears (P = .040). Higher volume increases were associated only with an increase in abduction power (P = .029) and not with other outcomes.
Conclusion:
The supraspinatus muscle volume increased immediately postoperatively and continuously for at least 1 year after surgery. The increase was evident in patients who had larger tears and healed successfully and when measured toward the more medial portion of the supraspinatus muscle. The volume increases were associated with an increase in shoulder abduction power.
A rotator cuff tear is a common injury that causes pain and functional disability, and surgical repair is a commonly accepted treatment of full-thickness rotator cuff tears. 11 However, healing failure after surgery remains one of the most common and well-known complications, and recent studies have reported an unacceptably high failure rate in spite of the advancements in surgical techniques and instrumentation.3,6 Chronic rotator cuff tears lead to rotator cuff muscle atrophy, hindering mechanical loading onto the rotator cuff muscle, and rotator cuff muscle atrophy is one of the most important prognostic factors that determine postoperative anatomic and functional outcomes.14,16,25,26 Rotator cuff muscle atrophy is mainly associated with the clinical outcomes of decreased postoperative strength, limited shoulder motion, and tendon repair failure.12,14,25
There is considerable debate on the recovery of rotator cuff muscle atrophy after rotator cuff repair. Some authors have reported that atrophy and fatty infiltration improve after successful rotator cuff repair,5,12,34 while others have reported that they are irreversible even after successful repair.7,14,22
However, most of the studies that evaluated changes in rotator cuff muscle atrophy compared preoperative magnetic resonance imaging (MRI) scans to a single series of postoperative MRI scans, and the evaluations were performed from a single image slice by considering the tangent sign, occupation ratio, or 2-dimensional (2D) cross-sectional area.34,38 The comparison with a single series of postoperative MRI scans may result in interpretation errors due to the difficulty in selecting identical image slices from both preoperative and postoperative MRI scans and due to the lateral migration effect of the rotator cuff muscle mass after repair.18,30 As Jo and Shin 18 previously reported, when the retracted tendon is reduced by repair, the muscle area assessed at the fixed MRI plane is more likely to increase immediately after surgery, owing to lateral migration of the muscle mass, which would lead to misinterpretation.
Therefore, 2 series of postoperative MRI scans, with an immediately postoperative scan as a baseline for comparison, are necessary to evaluate the actual changes in rotator cuff muscle atrophy after rotator cuff repair. In addition, the 2D cross-sectional area in a single image slice might not fully reflect the morphological changes of the muscle and may be strongly influenced by medial retraction of the rotator cuff tendon after tearing and lateral migration of the muscle mass after rotator cuff repair. Therefore, a volumetric measurement of the rotator cuff muscle is required for the accurate evaluation of muscle atrophy changes after rotator cuff repair; however, few studies have performed 3-dimensional (3D) assessments of rotator cuff muscle volume.
The purpose of this study was to evaluate the serial changes in supraspinatus muscle atrophy after rotator cuff repair at 3 time points (preoperatively, immediately postoperatively, and later postoperatively) by measuring the supraspinatus muscle volume at a position up to 2 cm medial to the Y-view on MRI using semiautomatic segmentation software and further to assess the factors associated with the volume changes and the relation between volume changes and outcomes.
Methods
Patient Selection
The Konkuk University Medical Center’s institutional review board approved our study protocol (No. KUH1060127). Among the 264 patients who underwent arthroscopic rotator cuff repair at our hospital between September 2012 and February 2015, we included patients with full-thickness rotator cuff tears as confirmed by arthroscopic findings and those who had 3 consecutive MRI scans with full Y-views performed preoperatively, immediately postoperatively (within 2 days after surgery), and later postoperatively (at least 1 year after surgery; mean, 13.8 ± 2.2 months [range, 12-17 months]). The postoperative MRI scans were obtained as part of routine follow-up, and there was no special indication for these scans. We excluded patients based on the following criteria: absence of any of the 3 MRI scans (n = 61), loss to follow-up within 1 year after surgery (n = 73), presence of partial-thickness rotator cuff tears (n = 27) and isolated subscapularis tears (n = 4), prior surgery on the shoulder being studied (n = 7), incomplete repair (n = 5), and workers’ compensation status (n = 13). There were no significant differences in any demographic or clinical factors between those who were included and those who dropped out or were excluded (all P > .05) (Appendix Tables A1 and A2, available in the online version of this article). Finally, 74 patients (34 men, 40 women) with a mean age of 62.8 ± 8.8 years (range, 30-83 years) were enrolled.
Demographic and Clinical Data
Sports activity level was defined as high (dynamic or contact sports such as boxing, rugby, basketball, football), medium (static sports such as golf, yoga, swimming, bicycling, running), and low. Work level was defined as high (heavy manual labor), medium (manual labor with less activity), and low (sedentary work). 4 The tear size was measured arthroscopically with a calibrated probe at the time of surgery and classified according to the rating system of DeOrio and Cofield. 8 There were 22 small tears (<1 cm; 29.7%), 28 medium tears (≥1 to <3 cm; 37.8%), 18 large tears (≥3 to <5 cm; 24.3%), and 6 massive tears (≥5 cm; 8.1%). There were 51 patients with crescent-shaped tears, 7 patients with U-shaped tears, 4 patients with L-shaped tears, and 12 patients with reverse L–shaped tears. The fatty infiltration of each rotator cuff muscle (supraspinatus, infraspinatus, and subscapularis) was evaluated from preoperative scans according to the criteria established by Goutallier et al 15 and modified by Fuchs et al. 9 Two raters (S.W.C. and K.-S.O.) evaluated the fatty infiltration of each rotator cuff muscle, and the means of the values were used for later analyses. The demographic and clinical data are summarized in Table 1.
Demographic and Clinical Data a
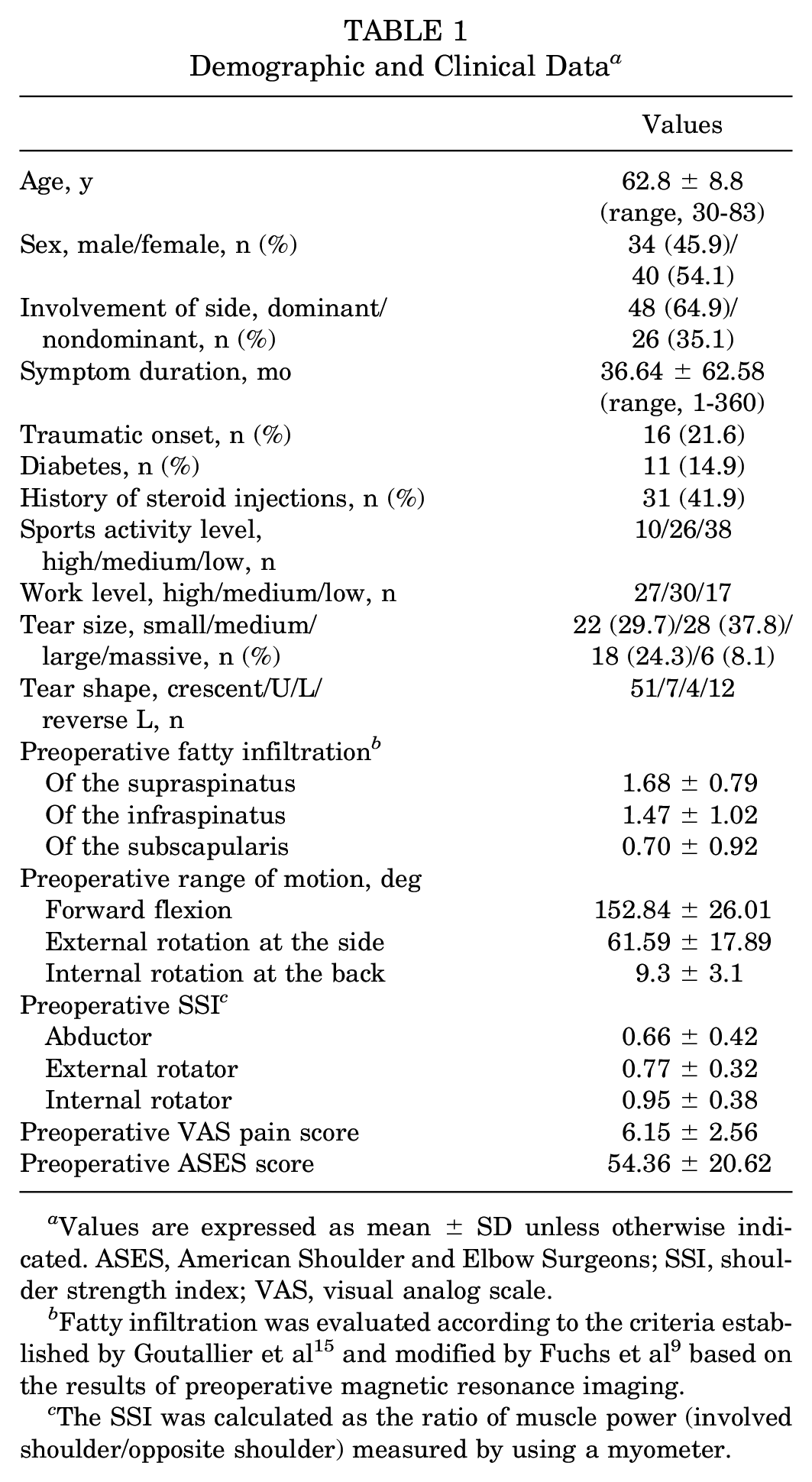
Values are expressed as mean ± SD unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; SSI, shoulder strength index; VAS, visual analog scale.
Fatty infiltration was evaluated according to the criteria established by Goutallier et al 15 and modified by Fuchs et al 9 based on the results of preoperative magnetic resonance imaging.
The SSI was calculated as the ratio of muscle power (involved shoulder/opposite shoulder) measured by using a myometer.
3D Reconstruction and Visualization of the Supraspinatus Muscle From MRI Scans
Each MRI scan was obtained on a 3.0-T system (Signa HDx; GE Healthcare) with a dedicated shoulder coil. The arms were placed in a neutral position at the side of the body, with the position being maintained consistently throughout scanning. The following MRI sequences were used: axial images obtained with T1-weighted spin echo (repetition time [TR]/echo time [TE], 550-733/15-17 ms) sequences, and coronal and sagittal images obtained with T2-weighted spin echo (TR/TE, 3500-4000/60-110 ms) sequences. The slice thickness was 4 mm, with an interslice gap of 0 or 0.4 mm and a field of view of 16 × 16 cm.
To generate the 3D model of the supraspinatus muscle, we used ITK-SNAP, a semiautomatic segmentation software. 37 After the MRI scans were loaded into ITK-SNAP by using the Digital Imaging and Communications in Medicine (DICOM) format, the supraspinatus area of every sagittal image was delineated by applying user-interactive graphic tools (Figure 1A). From the delineated contour, new binary DICOM images were created (supraspinatus area: 1; background: 0) (Figure 1B). Then, the 3D model of the supraspinatus was reconstructed from the 2D supraspinatus contours on each sagittal image (Figure 1C). The reconstructed 3D model was saved as a standard 3D model in the stereolithography file format (*.STL).
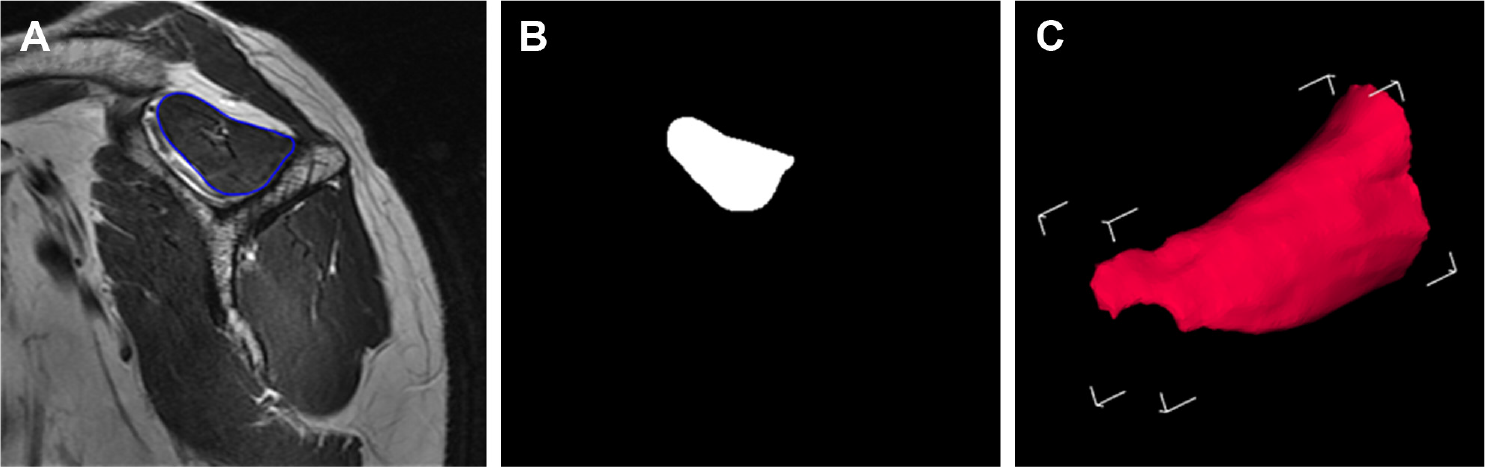
(A) Marked contour of the supraspinatus on the Y-view, (B) converted binary image of the marked contour, and (C) 3-dimensional reconstructed model of the supraspinatus.
The 3D reconstructed supraspinatus model and the original MRI scans were visualized using our in-house software (Figure 2A). We implemented the software using open-source libraries: (1) Visualization Toolkit (Kitware Inc) to process and visualize the 3D data and (2) Insight Toolkit (Insight Software Consortium) to load the DICOM images. Figures 2B and 2C show the cross-section of the 3D supraspinatus model aligned onto the original MRI scans. The in-house software for 3D supraspinatus modeling was validated in our previous study. 19 In that previous study, 19 we quantitatively evaluated the performance of the software with 4 measurements: accuracy (statistical measurement of agreement between reference and experiment), Dice coefficient (spatial overlap between 2 models), average distance, and maximal distance. The evaluation results proved the software’s reliability: accuracy (0.995 ± 0.001), Dice coefficient (0.951 ± 0.011), average distance (0.440 ± 0.086 mm), and maximal distance (3.045 ± 0.433 mm).
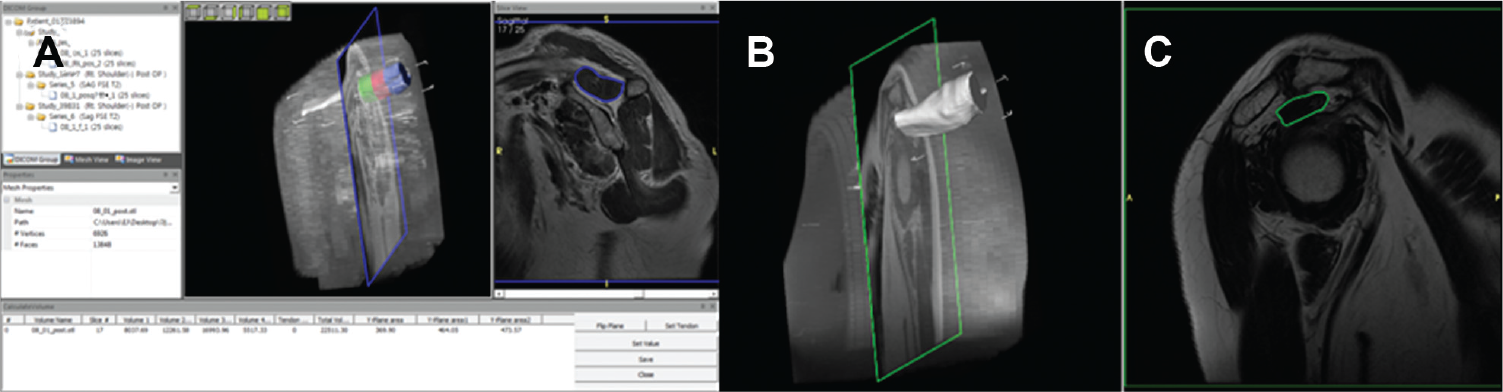
(A) In-house software and visualization of the original magnetic resonance imaging scan, slice image, and reconstructed supraspinatus model in (B) the 3-dimensional view generated by using ITK-SNAP and (C) the 2-dimensional view.
Measurement of the Volume and Cross-sectional Area of the Supraspinatus Muscle
We defined the Y-view as the reference for measuring the volume and cross-sectional area of the supraspinatus. Our in-house software allows a user to interactively select the Y-view. Based on the Y-view, the volume and cross-sectional area are automatically calculated. The user can choose the Y-view, where the body of the scapula, scapular spine, and medial border of the coracoid process form a Y-shape in oblique sagittal images while watching the current slice image. The supraspinatus muscle range was defined as the area from the most lateral end of the supraspinatus muscle, where the MRI signal changes from the tendon to the muscle on oblique sagittal images, to the designated medial end of the supraspinatus muscle, that is, the Y-view. After defining the supraspinatus muscle range, the software automatically computed the 3D volume of the model.
We performed 3 volume measurements: from the most lateral end of the supraspinatus muscle to the Y-view, 1 cm medial to the Y-view (Y+1 view), and 2 cm medial to the Y-view (Y+2 view) (Figure 3A). With regard to the 3 consecutive scans (preoperatively, immediately postoperatively, and later postoperatively), all 74 patients had Y-view scans, 64 had Y+1 view scans, and 37 had Y+2 view scans. In some patients (n = 10), the MRI scans did not reach up to 1 cm medial to the Y-view; thus, we could evaluate the Y+1 view in 64 (n = 74 – 10) patients. In addition, the MRI scans of another 27 patients did not reach up to 2 cm medial to the Y-view; thus, we could evaluate the Y+2 view in 37 (n = 74 – 10 – 27) patients.
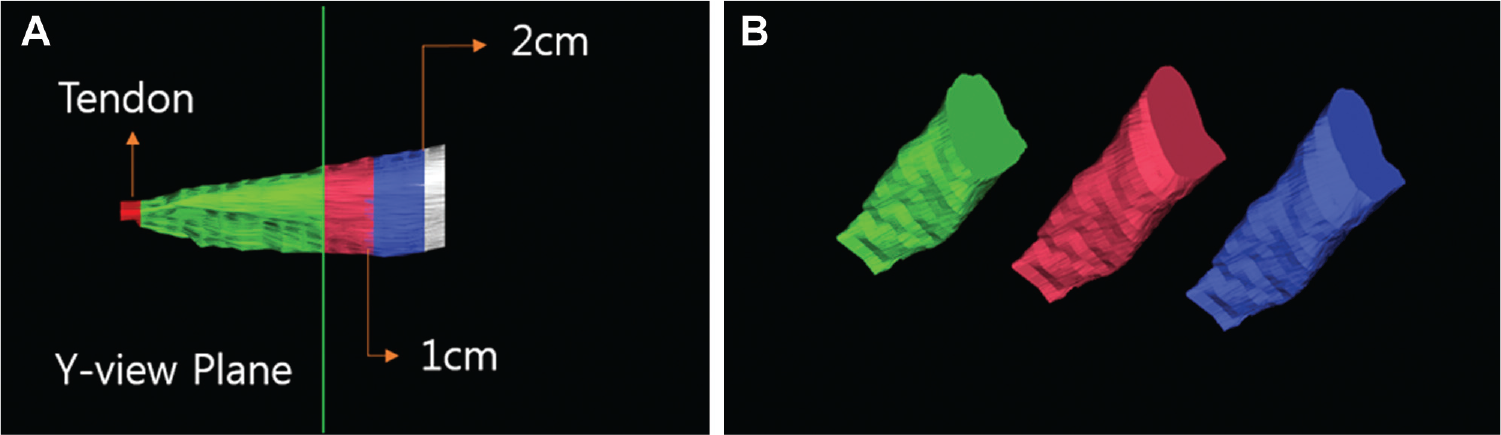
(A) Definition of the Y-view and clipped planes and (B) the clipped models to measure the volume and cross-sectional area of the supraspinatus.
In addition, the cross-sectional area of each plane was also measured for 2D sectional analysis for comparison. The clipped supraspinatus models used for measurement for the 3 positions (Y, Y+1, and Y+2 views) are shown in Figure 3B.
The 2 independent raters (S.W.C. and E.S.) used this software to measure the 2D cross-sectional area of the supraspinatus and the 3D muscle volume on the Y, Y+1, and Y+2 views preoperatively, immediately postoperatively, and later postoperatively to assess interrater reliability. These values were then adjusted for the body mass index of each patient, and the means of the adjusted values were used for later analyses.
The serial changes in each 2D area and 3D volume between preoperatively and immediately postoperatively and between immediately postoperatively and later postoperatively were evaluated at each measurement point according to repair integrity. In addition, the patients with successful healing were further divided into a higher volume change group (volume change was higher than average later postoperatively compared with immediately postoperatively assessed on the Y-view) and a lower volume change group (volume change was lower than average later postoperatively compared with immediately postoperatively assessed on the Y-view). Then, the possible relationship between various clinical factors, including tear size and the postoperative volume change in the supraspinatus muscle later postoperatively compared with immediately postoperatively, and the effect of a higher volume increase later postoperatively compared with immediately postoperatively on the range of motion (ROM), muscle power, and visual analog scale (VAS) pain and American Shoulder and Elbow Surgeons (ASES) scores, which were assessed at a mean of 22.7 ± 4.2 months (range, 18-41 months), were evaluated.
Surgical Procedures and Rehabilitation
All surgical procedures were performed arthroscopically with the patient in a beach-chair position. Subacromial decompression and acromioplasty were performed to create a flat acromion in all patients. Biceps tenotomy (n = 19) or tenodesis (n = 13) was performed in cases with dislocations, subluxations, and tears involving more than 50% of the long head of the biceps tendon or for a symptomatic, degenerative superior labral anterior and posterior (SLAP) lesion depending on the age or activity level of the patient. Concomitant subscapularis repair was performed in 9 patients to treat the associated subscapularis tears. No patients underwent distal clavicle resection or coracoplasty. The margin of the tear was debrided to obtain better quality tendon tissues. For reattachment of the rotator cuff tendons, a cancellous bone bed was prepared by using a bur until bleeding occurred. Procedures to mobilize the tendon were performed if the mobility of a tendon was insufficient for repair. All patients underwent arthroscopic suture bridge repair, and all knots were tied securely by applying a self-locking, sliding knot.
Immobilization after rotator cuff repair was maintained with an abduction brace, and the duration of immobilization ranged from 4 to 6 weeks and was based on the tear size measured at the time of surgery. Shrugging of both shoulders, active elbow flexion and extension, active forearm supination and pronation, and active hand and wrist motion were encouraged immediately after surgery. Active-assisted ROM exercise was allowed after weaning off the brace. Muscle strengthening exercises were initiated at 9 to 12 weeks postoperatively. Muscle strengthening was achieved by active resistance muscle training using a rubber band (HCM-Hygenic Corp). Specifically, supraspinatus muscle training was performed by abducting and externally rotating the shoulder while holding the rubber band fixed to a door handle or to the foot by stepping on it. Sports activities and heavy labor were allowed after 6 months. The rehabilitation protocol was home based and did not change during the study period.
Outcome Evaluation
Shoulder ROM, VAS pain and ASES scores, rotator cuff muscle strength, and repair integrity were evaluated in all patients. For the evaluation of shoulder ROM, passive motion in 3 directions (forward flexion, external rotation at the side, and internal rotation across the back) was measured. Forward flexion was measured in degrees between the arm and the thorax with the elbow held straight, and external rotation at the side was measured in degrees between the thorax and the forearm with the arm held in an adducted position and the elbow flexed 90°. Internal rotation across the back was measured by determining the vertebral level that the patient could reach with the tip of his or her thumb. The VAS pain score ranged from 0 to 10, with 10 indicating the highest level of pain, and the ASES score consisted of a total based on a 100-point system (50 points for daily function and 50 points for pain). Rotator cuff muscle strength was checked using a portable myometer (Mecmesin) by a single laboratory technician who was unaware of this study. The muscle power of the supraspinatus was determined with the shoulder in the empty-can position, and the muscle power of the external and internal rotators of the shoulder was determined with the joint in neutral abduction. 29 These measurements were normalized to those of the opposite shoulder and reported as a ratio for each muscle (shoulder strength index). 28 Repair integrity was investigated on the postoperative MRI scan performed at least 1 year after surgery by using the Sugaya classification: type I, sufficient thickness with homogeneously low intensity; type II, sufficient thickness with partial high-intensity areas; type III, less than half the thickness without discontinuity; type IV, minor discontinuity; and type V, major discontinuity. Types IV and V were defined as healing failure. 33
Statistical Analysis
The intraclass correlation coefficient (ICC), a 2-way random model with absolute agreement, was used to evaluate interrater reliabilities. Descriptive statistics were used to report changes in the 2D cross-sectional area and 3D supraspinatus muscle volume after arthroscopic rotator cuff repair on the Y, Y+1, and Y+2 views at the 3 different time points. The paired t test was used to compare the changes in each area and volume and fatty infiltration between preoperatively and immediately postoperatively and between immediately postoperatively and later postoperatively. The Student t test for continuous variables and the chi-square or Fisher exact test for categorical variables were used to determine the differences between the higher and lower volume change groups. The software SPSS Statistics 23.0 (SPSS Inc) was used for all statistical analyses, and P < .05 was considered statistically significant.
Results
The postoperative clinical outcomes were evaluated at a mean of 22.7 ± 4.2 months (range, 18-41 months) after surgery, the mean final postoperative VAS pain score was 1.20 ± 1.69 (range, 0-4.5), and the mean postoperative ASES score was 90.81 ± 13.41 (range, 72-100).
The interrater reliabilities were found to be excellent for all 2D cross-sectional area (ICC, 0.955-0.993; P < .001), 3D volume (ICC, 0.893-0.993; P < .001), and rotator cuff muscle fatty infiltration measurements (ICC, 0.714-0.832).
Both the 2D areas and 3D volumes were increased immediately postoperatively as compared with preoperatively. The 2D areas did not differ significantly between immediately postoperatively and later postoperatively; however, the 3D volumes on the Y+1 and Y+2 views increased significantly later postoperatively as compared with immediately postoperatively (P = .033 and .048, respectively) (Table 2 and Appendix Figure A1, available online).
Serial Changes in Supraspinatus Muscle Area and Volume in All Patients a
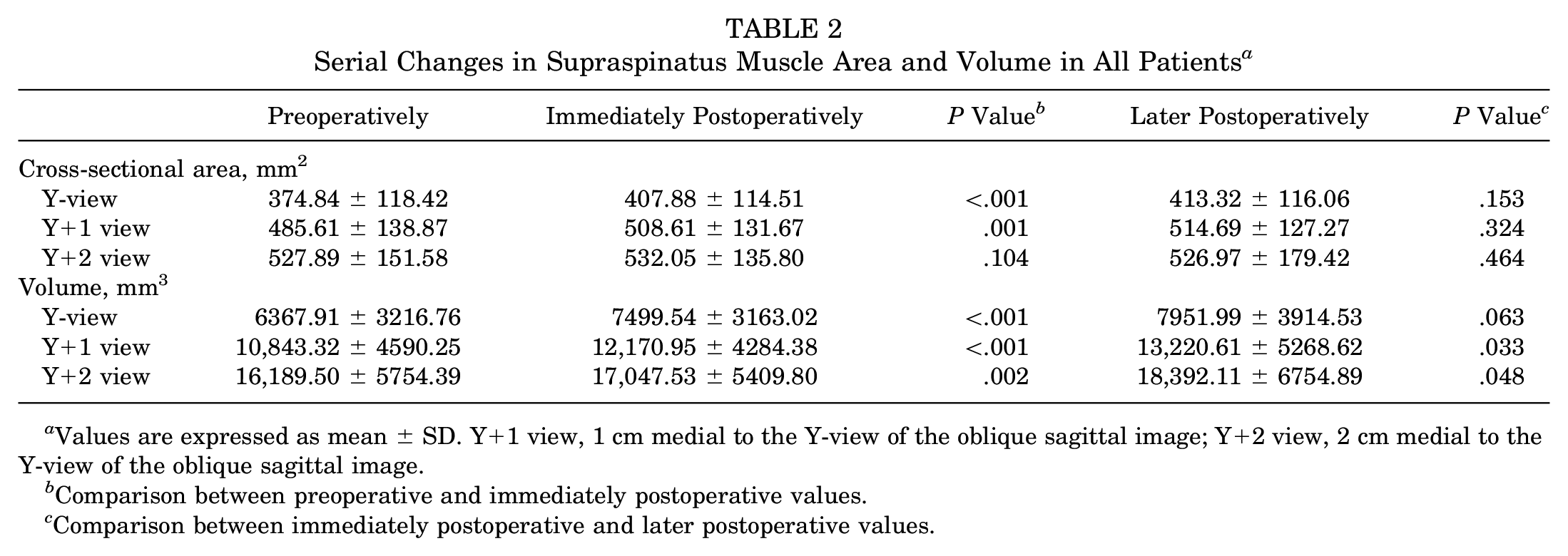
Values are expressed as mean ± SD. Y+1 view, 1 cm medial to the Y-view of the oblique sagittal image; Y+2 view, 2 cm medial to the Y-view of the oblique sagittal image.
Comparison between preoperative and immediately postoperative values.
Comparison between immediately postoperative and later postoperative values.
Among the 74 patients, 9 patients displayed healing failure, and those patients showed significantly decreased 2D areas (Y-view: P = .012; Y+1 view: P = .042) and 3D volumes (Y-view: P = .016; Y+1 view: P = .007; Y+2 view: P = .047) later postoperatively compared with immediately postoperatively (Table 3 and Appendix Figure A2, available online).
Serial Changes in Supraspinatus Muscle Area and Volume in Patients With Healing Failure a

Values are expressed as mean ± SD. Y+1 view, 1 cm medial to the Y-view of the oblique sagittal image; Y+2 view, 2 cm medial to the Y-view of the oblique sagittal image.
Comparison between preoperative and immediately postoperative values.
Comparison between immediately postoperative and later postoperative values.
In addition, there were significant differences in the 2D area and 3D volume changes later postoperatively compared with immediately postoperatively between those with and without healing failure at all measurement points (P < .05). After omitting the patients with healing failure, the 3D volume increase later postoperatively compared with immediately postoperatively became more prominent (P < .05) in the order of the Y+2 view (most prominent, 1859.5-mm3 increase), Y+1 view (1402.8-mm3 increase), and Y-view (879.0-mm3 increase) (Table 4 and Appendix Figure A3, available online).
Serial Changes in Supraspinatus Muscle Area and Volume in Patients With Healing Success a
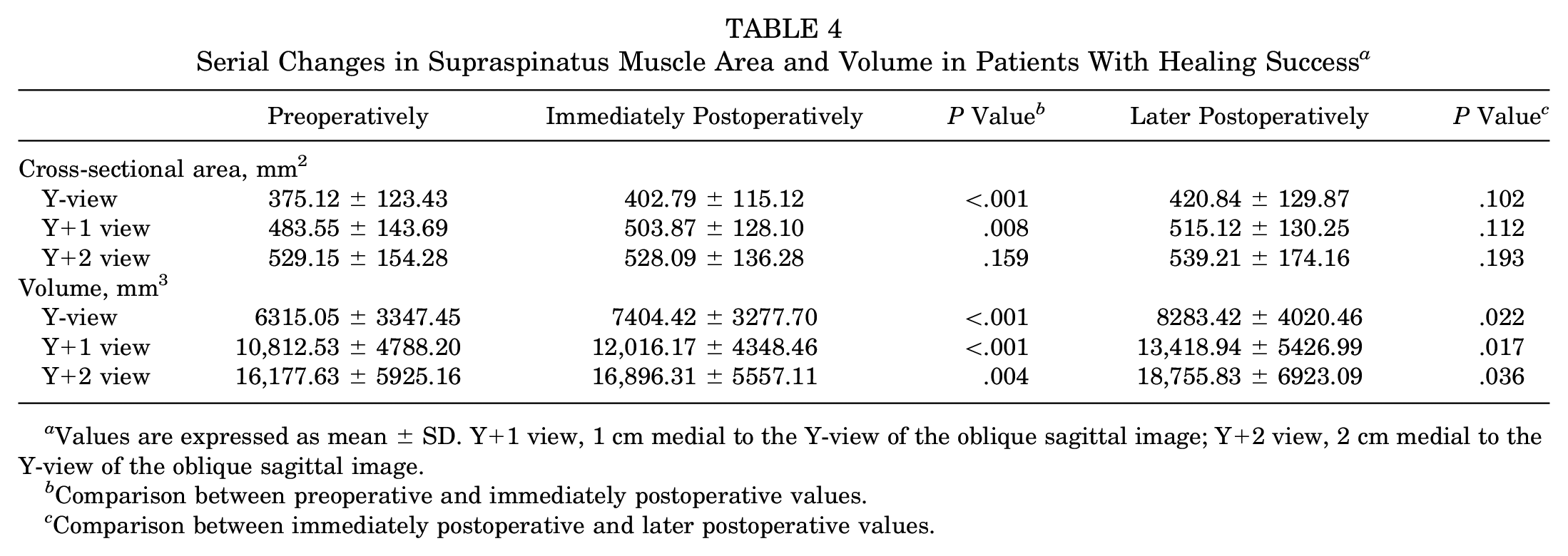
Values are expressed as mean ± SD. Y+1 view, 1 cm medial to the Y-view of the oblique sagittal image; Y+2 view, 2 cm medial to the Y-view of the oblique sagittal image.
Comparison between preoperative and immediately postoperative values.
Comparison between immediately postoperative and later postoperative values.
However, there were no differences in the rotator cuff muscle fatty infiltration grade according to the classification of Goutallier et al 15 between preoperatively and immediately postoperatively and between immediately postoperatively and later postoperatively (P > .05) (Appendix Table A3, available online).
In this study, 14 patients needed mobilization of the torn tendon and were repaired under tension. These patients showed less change in the volume assessed on the Y-view at least 1 year after rotator cuff repair compared with immediately postoperatively (574.75 ± 2132.31 mm3 in tension-free repair and 314.19 ± 3345.93 mm3 in under-tension repair); however, the difference was not to the point of being significant (P = .432).
After omitting the patients with healing failure, we compared the differences between the higher (n = 40) and lower (n = 25) volume change groups among the patients with successful healing (n = 65) and found no significant differences among the various demographic and clinical factors, except for tear size. That is, larger tears were associated with a higher muscle volume increase later postoperatively compared with immediately postoperatively (P = .040). The relationship between volume changes and demographic and clinical factors is shown in Table 5.
Relationship Between Volume Changes and Demographic and Clinical Factors a
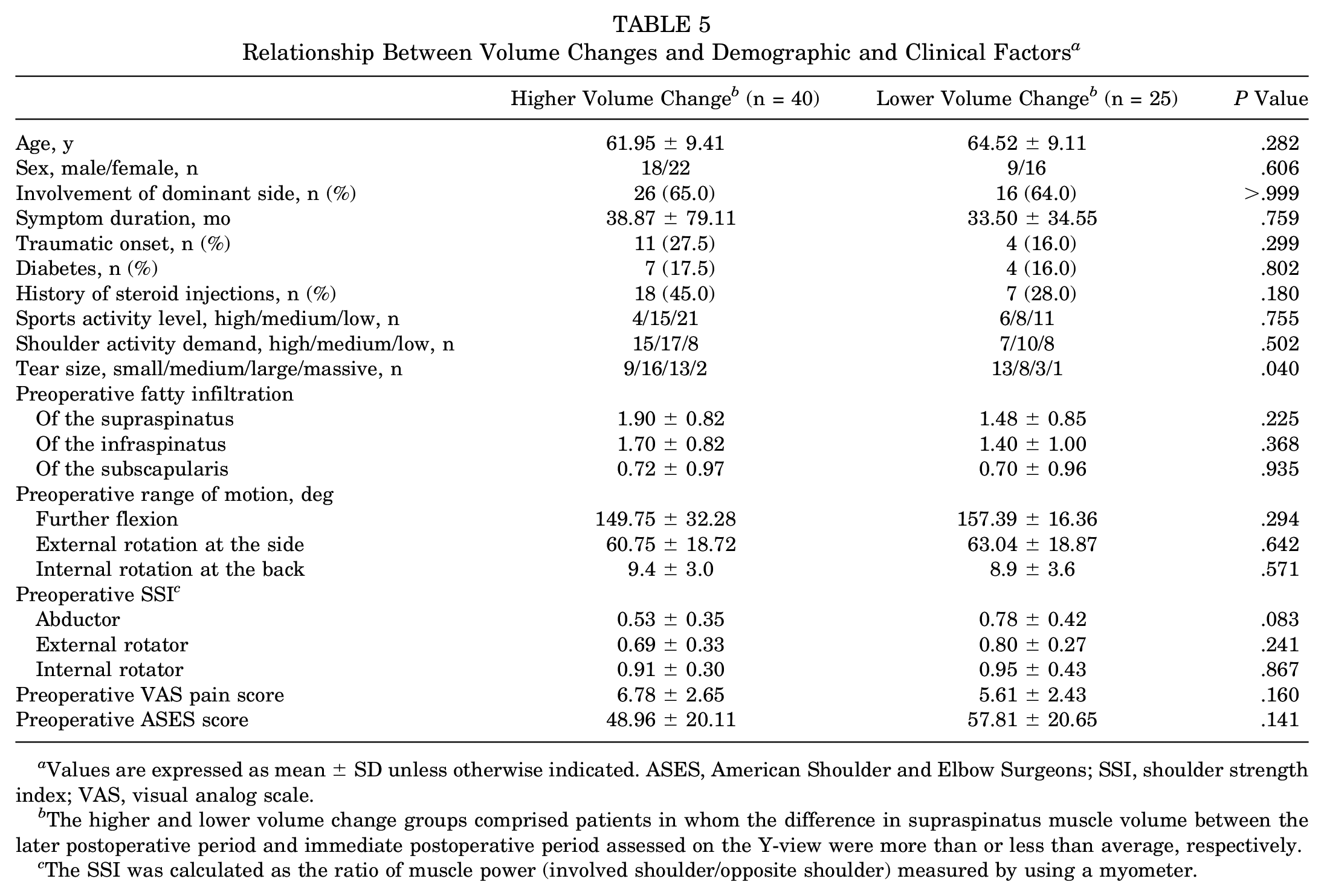
Values are expressed as mean ± SD unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; SSI, shoulder strength index; VAS, visual analog scale.
The higher and lower volume change groups comprised patients in whom the difference in supraspinatus muscle volume between the later postoperative period and immediate postoperative period assessed on the Y-view were more than or less than average, respectively.
The SSI was calculated as the ratio of muscle power (involved shoulder/opposite shoulder) measured by using a myometer.
In addition, the higher volume increase later postoperatively compared with immediately postoperatively was associated with a higher increase in abduction power (P = .029); however, no association was found with other outcome measurements such as ROM and VAS pain and ASES scores (Table 6).
Relationship Between Volume Changes and Clinical Outcomes a
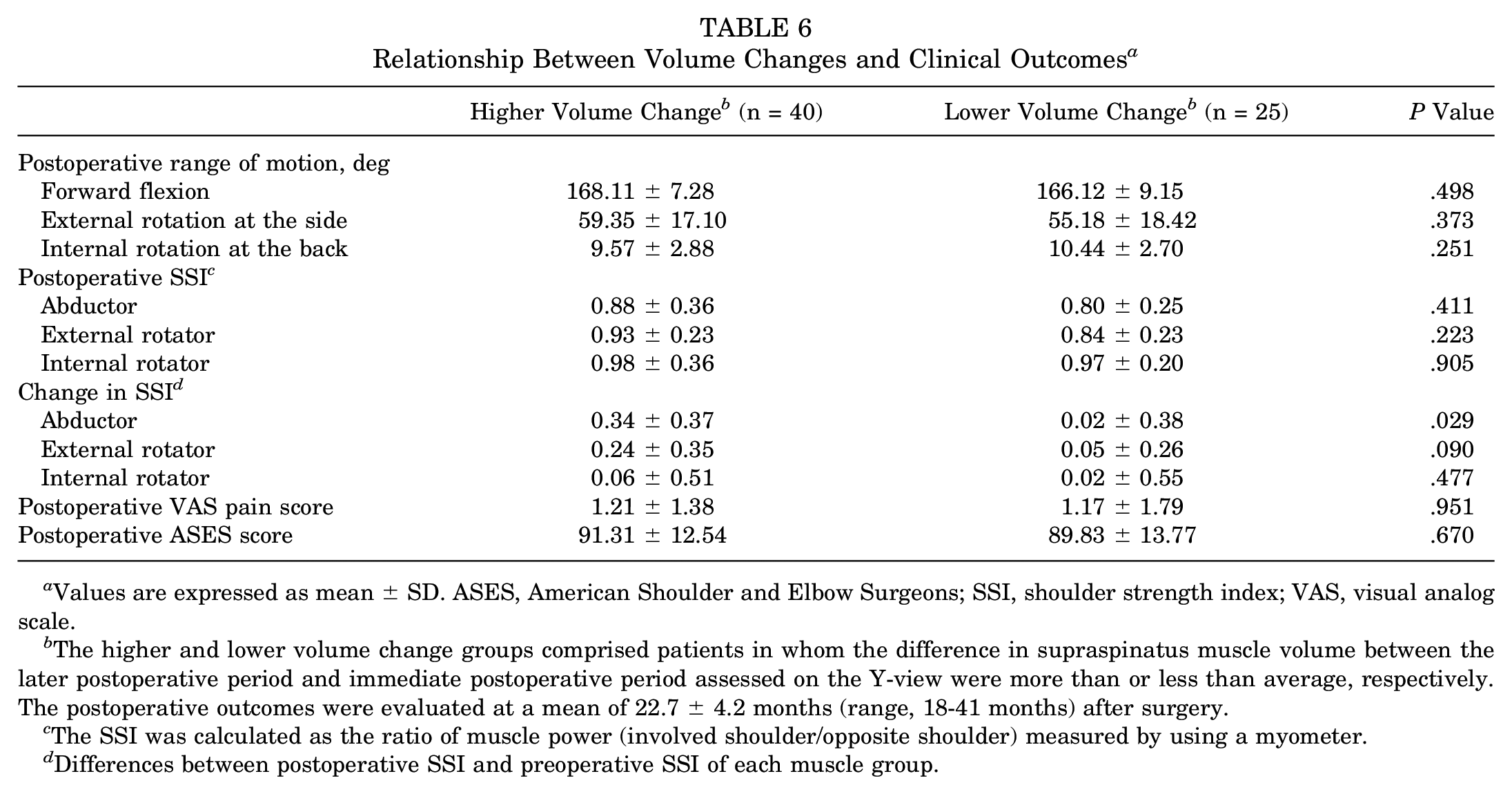
Values are expressed as mean ± SD. ASES, American Shoulder and Elbow Surgeons; SSI, shoulder strength index; VAS, visual analog scale.
The higher and lower volume change groups comprised patients in whom the difference in supraspinatus muscle volume between the later postoperative period and immediate postoperative period assessed on the Y-view were more than or less than average, respectively. The postoperative outcomes were evaluated at a mean of 22.7 ± 4.2 months (range, 18-41 months) after surgery.
The SSI was calculated as the ratio of muscle power (involved shoulder/opposite shoulder) measured by using a myometer.
Differences between postoperative SSI and preoperative SSI of each muscle group.
Discussion
Our study, which involved 3D supraspinatus muscle volume measurements at 3 different time points, showed that supraspinatus muscle atrophy could be improved after rotator cuff repair. We not only confirmed the lateral migration effect of the supraspinatus muscle mass previously reported by Jo and Shin 18 by comparing the preoperative and immediate postoperative volumes but also showed that the supraspinatus muscle volume evaluated at least 1 year after surgery increased as compared with that in the immediate postoperative period.
To our knowledge, there are 2 very recent studies that have compared the change in muscle atrophy at 3 time points.17,30 These studies reported an increase in the cross-sectional area of the supraspinatus muscle of 19.6% 17 and 9.0% 30 in the immediate postoperative period compared with the preoperative period, respectively; however, the findings for the later postoperative period were conflicting. Park et al 30 reported an 8.1% increase of the supraspinatus muscle area at a minimum 2 years compared with 6 months after surgery. On the contrary, Jo et al 17 reported a 5.9% decrease at 1 year as compared with the immediate postoperative period. In a 2D assessment of the cross-sectional area, we also found a similar increase of 8.8% in the immediate postoperative period compared with the preoperative period; also, there was no significant difference in the cross-sectional areas between the immediate postoperative period and later postoperative period, despite a slight increase by 1.3%. However, a 2D assessment of a single Y-view scan would be insufficient for estimating the amount of muscle mass and may overlook important morphological information, 35 and a comparison of exact MRI slices between 2 scans may not be feasible because of the slice thickness. Therefore, we evaluated the 3D volume of the supraspinatus to overcome this limitation and showed a significant increase in the muscle volume compared with the immediate postoperative period. Even though no significant changes were observed in the cross-sectional areas, the 3D volume showed significant changes. This significant volume increase may have arisen from the summation of the insignificant minimal increase in the cross-sectional areas. We believe that 3D muscle volume assessments, rather than 2D cross-sectional area assessments, provide a true indication of supraspinatus muscle atrophy, and we therefore suggest that muscle atrophy could be reversed to some degree, especially in patients who have healed successfully.
During the 3D volume measurement, we tried to evaluate the muscle volume in images with a greater medial view (Y+1 view: 64 patients; Y+2 view: 37 patients) rather than the conventional Y-view. A trial to evaluate rotator cuff muscle atrophy and fatty infiltration in a more medial MRI view was recently performed by Fukuta et al. 10 Although they did not perform 3D volume measurements, they measured the cross-sectional areas of the supraspinatus muscle from the Y-view to 3 more medial slices and concluded that supraspinatus atrophy might be overestimated when the evaluation is performed on the Y-view; a sufficient number of slices medial to the musculotendinous junction should be used for evaluation. 10 In the current study, the increase in the volume was more prominent when measured with a more medial slice from the Y-view (in the order of Y+2 view, Y+1 view, and Y-view). This result is consistent with the findings of Fukuta et al 10 and indicates that measurements performed on images that are more medial represent the supraspinatus muscle condition better. It seems obvious that assessments performed on images that are more medial would show a prominent change in volume because the evaluation at a more medial point would enable a greater integration of the increased muscle areas, even if the increase is minimal. Therefore, we believe that it is better to assess changes in the supraspinatus muscle volume on images that provide a more medial view. In this sense, the most ideal method of estimating muscle atrophy would be to measure the entire muscle volume to the most medial side of the muscle, even though the optimal method for measurement of the total volume is not known yet. Future clinical studies in which the entire supraspinatus muscle volume is measured may be necessary to confirm our results.
There are controversies regarding the reversibility of muscle atrophy after rotator cuff repair. Although several authors have suggested that atrophy and fatty infiltration are irreversible phenomena even after successful repair,7,14,22 others have shown that they can be reversed after successful rotator cuff repair.5,12,34,36 In this study, we observed significant improvement in the supraspinatus muscle volume after rotator cuff repair. We consider that the improvement of muscle atrophy after successful rotator cuff repair may be related to mechanical reloading of the torn tendon after repair, thereby possibly stimulating protein synthesis in the atrophied rotator cuff muscles and resulting in recovery of the muscle mass.1,27 However, unlike the observed increase in muscle volume, we were unable to identify any improvement in fatty infiltration after rotator cuff repair as assessed by the criteria described by Goutallier et al. 15 This result is consistent with the study of Barry et al, 2 who demonstrated that atrophy and fatty infiltration are separate processes, and that of Vidt et al, 35 who observed aggravated muscle atrophy without marked increases in fatty infiltration after rotator cuff tears. We are also of the opinion that fatty infiltration may be underestimated if there is an increase in the muscle volume, as the fat proportion may appear to be less in relation to the increased muscle volume. In addition, the grading system of Goutallier et al 15 may not be sensitive enough to detect the small, but possibly important, differences in fatty infiltration. 23 Perhaps a more subdivided grading system or more sophisticated quantitative grading system may reveal the statistically significant differences in fatty infiltration after rotator cuff repair.
In this study, the patients with healing failure showed significantly decreased supraspinatus muscle volumes when compared with the immediate postoperative period, and the volume was significantly smaller than that of the patients who healed successfully. This is consistent with previous reports,14,24 which have suggested that changes in rotator cuff muscle atrophy were closely related to integrity of the repaired rotator cuff tendon. Therefore, surgeons should make an effort to improve the healing rate by applying such methods as strong fixation during repair, biological augmentation, or appropriate rehabilitation processes.20,21 In addition, we also found a higher increase in the supraspinatus volume in cases with a larger sized tear. We postulate that because the initial supraspinatus volume is small in cases of larger tears, there may be plenty of room for volume increases, which may lead to a higher volume increase as compared with cases with smaller tears. Tension-free repair 32 is another important issue in rotator cuff repair, especially in large to massive tears. In this study, the patients whose torn rotator cuff tendons were repaired under tension showed less change in the supraspinatus volume compared with those who underwent tension-free repair, even though it was not statistically significant.
Another important finding of this study is the relationship with the improvement in supraspinatus muscle atrophy and abduction muscle power. Several authors have suggested that muscle atrophy is an important contributor to strength deficits in patients with rotator cuff tears.13,14,35 In addition to these findings, in this study, we first demonstrated that strength can be improved via the improvement of muscle atrophy after successful rotator cuff repair. Muscle strength has important functional implications that affect the performance of daily activities and quality of life, especially in older patients with a low muscle mass. 31 Therefore, efforts to preserve or improve the muscle volume in patients with rotator cuff tears must be made. The significant relationship between the muscle volume increase and muscle strength in patients with full-thickness rotator cuff tears who have healed successfully may reinforce the use of rotator cuff repair surgery rather than nonoperative treatment to increase strength production by improving atrophy, which may in turn improve functional outcomes, even though this has not been proven in this study.
This was the first study to report changes in the reconstructed supraspinatus muscle volume, measured at 3 different points on oblique sagittal MRI scans at 3 different time points, and to show the relationship between the volume changes and contributing factors and clinical outcomes. Nevertheless, this study has several limitations. First, the number of patients in this study was relatively small. There is a possibility that the lack of statistical significance found when assessing some factors may be caused by the relatively small number of cases. Second, the dropout rate (27.7%, 73/264) was high, and not all patients who underwent arthroscopic repair for full-thickness rotator cuff tears were included in this study, as we limited patients to those who had all 3 consecutive MRI scans. In our institute, the cost of postoperative MRI scans is less than half that of preoperative scans, and therefore, we could obtain more than 2 rounds of postoperative scans, including scans obtained during the immediate postoperative period. Nevertheless, some patients refused postoperative scans because they did not want to undergo the still rather expensive and time-consuming procedures. This major dropout from the cohort might have led to the risk of selection bias, which we are not aware of. Third, even though we measured the supraspinatus muscle volume up to 2 cm medial to the conventional Y-view, we could not determine the total muscle volume because of the practical difficulty in extending the shoulder MRI field up to the medial scapula in a real clinical situation. The optimal method for estimating muscle atrophy would be to measure the entire supraspinatus muscle. Further studies involving the total volume measurement might be needed to confirm our result. Finally, although we observed a significant increase in the supraspinatus muscle volume at least 1 year after surgery as compared with the immediate postoperative period, the evaluation time of 1 year may be rather early for the final assessment of postoperative changes, as measurements may continue to change beyond 1 year. Further studies with longer follow-up times may be needed to evaluate additional changes in the supraspinatus muscle volume and their correlation to function.
Conclusion
The supraspinatus muscle volume increased immediately after rotator cuff repair and continuously for at least 1 year after surgery. This volume increase was evident in patients who healed successfully and in those with larger tears, especially when measured toward the more medial portion of the supraspinatus muscle. Further, the increase in supraspinatus muscle volume was associated with an increase in shoulder abduction power.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This research is supported by the Korea Institute of Science and Technology (2E26210, 2E26276).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.