
Abstract
Background:
Most Achilles tendon ruptures are sports related. However, few studies have examined and compared the effect of surgical repair for complete ruptures on return to play (RTP), play time, and performance across multiple sports.
Purpose:
To examine RTP and performance among professional athletes after Achilles tendon repair and compare pre- versus postoperative functional outcomes of professional athletes from different major leagues in the United States.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
National Basketball Association (NBA), National Football League (NFL), Major League Baseball (MLB), and National Hockey League (NHL) athletes who sustained a primary complete Achilles tendon rupture treated surgically between 1989 and 2013 were identified via public injury reports and press releases. Demographic information and performance-related statistics were recorded for 2 seasons before and after surgery and compared with matched controls. Statistical analyses were used to assess differences in recorded metrics.
Results:
Of 86 athletes screened, 62 met inclusion criteria including 25 NBA, 32 NFL, and 5 MLB players. Nineteen (30.6%) professional athletes with an isolated Achilles tendon rupture treated surgically were unable to return to play. Among athletes who successfully returned to play, game participation averaged 75.4% (P < .001) and 81.9% (P = .002) of the total games played the season before injury at 1 and 2 years postoperatively, respectively. Play time was significantly decreased and athletes performed significantly worse compared with preoperative levels at 1 and 2 years after injury (P < .001). When players were compared with matched controls, an Achilles tendon rupture resulted in fewer games played (P < .001), decreased play time (P = .025), and worse performance statistics (P < .001) at 1 year but not 2 years postoperatively (P > .05). When individual sports were compared, NBA players were most significantly affected, experiencing significant decreases in games played, play time, and performance.
Conclusion:
An Achilles tendon rupture is a devastating injury that prevents RTP for 30.6% of professional players. Athletes who do return play in fewer games, have less play time, and perform at a lower level than their preinjury status. However, these functional deficits are seen only at 1 year after surgery compared with matched controls, such that players who return to play can expect to perform at a level commensurate with uninjured controls 2 years postoperatively.
An Achilles tendon rupture is a devastating injury, most commonly afflicting the middle-aged male “weekend warrior.” 32 Rupture of the Achilles tendon requires two entities to be present: (2) tendinosis, or a focus of degeneration within the tendon, and (2) an eccentric contracture of sufficient force to rupture the tendon. The incidence of Achilles tendon ruptures in the general population ranges from 8.3 to 24 per 100,000, and it appears to be increasing with time.8,11,16,18,24,33,35 The majority of Achilles tendon ruptures are sports related,13,15,23,27,29 and while the optimal treatment for Achilles tendon ruptures continues to be debated, there are proponents for surgical repair in elite athletes. 17
Outcomes after various orthopaedic procedures have been documented in a number of professional athletes from the National Basketball Association (NBA),1,5,9,10,37 National Football League (NFL),2,4,6,31 Major League Baseball (MLB),7,21,28 and National Hockey League (NHL).12,26,30 Despite near limitless resources to help facilitate appropriate rehabilitation, an Achilles tendon rupture can be a career-threatening injury among elite athletes. Significant decreases in return to play (RTP), play time, and performance have been shown in NBA and NFL players who sustain an Achilles tendon rupture requiring surgical repair at various investigated time points.1,19,22,25 Overall, these studies document an approximate 60% to 70% RTP rate among NBA and NFL players.
Despite the above data, the literature has certain limitations and does not clearly elucidate the functional effect of an Achilles tendon rupture on athletic careers. For example, to our knowledge, no data are available regarding assessment of Achilles tendon ruptures in either MLB or NHL players. Further, no standardized definition of RTP is used within the literature, making comparisons between investigations difficult. Finally, the literature lacks comparisons of injured players with uninjured matched controls, a comparison that would provide a better assessment of postoperative function than do comparisons of preinjury and postinjury levels of performance. The purpose of the current investigation is to compare RTP rates and functional outcomes of athletes in multiple professional leagues after a primary Achilles tendon repair. This information will assist orthopaedic surgeons in managing expectations and counseling injured patients, whether professional athletes or weekend warriors, regarding expected functional prognosis.
Methods
Publicly available injury reports, press releases, and player profiles were accessed to yield a list of professional athletes in the NBA, MLB, NFL, and NHL who sustained a primary complete Achilles tendon rupture and subsequently underwent surgical repair between the 1988-1989 and 2012-2013 seasons. Inclusion criteria for athletes required professional participation in at least 1 game for 2 consecutive seasons before injury and no other identifiable or confounding injuries. Two years of professional play were required due to the various barriers that players face in making a professional team’s active roster, obtaining a contract, and establishing themselves in the league. Matched controls were selected for all returning players. A list of potential controls was first generated by identifying athletes of the same position and years of professional experience as the player to whom they would be matched. Next, a control was chosen from this list by selecting the athlete with the most similar sport-specific career performance statistic at the point in his career in which his total number of seasons played was identical to that of his matched study participant at the time of injury. Controls were verified to have no history of significant lower extremity surgical treatments.
Online databases and publically available sports statistic websites were mined to find demographic, play time, and performance-related data for players and controls. Demographic information obtained included age, body mass index (BMI), years of professional league experience, and position. The primary outcome of the investigation was RTP and assessment of the proportion of games played by each athlete pre- versus postoperatively. A strict definition of RTP was implemented requiring professional involvement in at least 1 game for a consecutive 2 years of play after surgery. Secondary outcomes included measurements of play time and performance. Play time measurements included minutes played for the NBA, games started for the NFL, and innings played for MLB.
Performance statistics used included player efficiency rating (PER) for the NBA, season approximate value (SAV) for the NFL, batting average (BA) for MLB field players, and earned run average (ERA) for MLB pitchers. The PER is an established, standardized measurement used in basketball analysis to assess player performance across different positions and seasons. It has been used as a primary measure of performance in numerous recent studies that have examined RTP and performance after injury.1,3 The SAV was recorded from www.sports-reference.com, which created this performance metric. A greater number correlates to a player’s performance contributing to a larger fraction of his team’s success. Performance of MLB players was measured using BA for position players and ERA for pitchers. Both BA and ERA are established, standardized performance measurements used in baseball analysis, and both have been used in a number of recent studies to assess performance after various injuries.14,20,34,36
The season in which injury and surgical repair occurred was considered to be the index season. Statistics of interest as outlined above were recorded for the season before surgery and 1 and 2 years after surgery. In matched controls, the same measurements were recorded 1 year before, 1 year after, and 2 years after the season in which the control had participated in an equal number of seasons as the matched athlete at the time of injury.
Statistical analyses were conducted with SPSS version 19 (IBM). Performance before versus after injury was compared in athletes with Achilles tendon rupture by use of a 2-tailed paired t test, and comparisons between athletes with Achilles tendon rupture and matched controls were performed by use of 2-tailed unpaired t tests. An a priori power analysis was performed based on a 2-sided paired t test to compare the population of Achilles tendon rupture cases to controls. The study was powered to detect a 15% difference in games played between athletes with ruptures and controls, with an alpha of 0.05 and a beta of 0.20. This power analysis determined that a minimum of 38 athletes with ruptures and 38 matched controls would be necessary to demonstrate statistical significance.
Results
Eighty-six athletes were identified as sustaining an Achilles tendon rupture, of which 62 met inclusion criteria. Reasons for exclusion included not completing at least 2 seasons preinjury (n = 15) or having a confounding injury (n = 9). Nineteen of the remaining 62 (30.6%) athletes did not return to play in the 2 seasons after surgery (Figure 1). The RTP rates for the NBA, NFL, and MLB were 68.0%, 65.6%, and 100%, respectively.
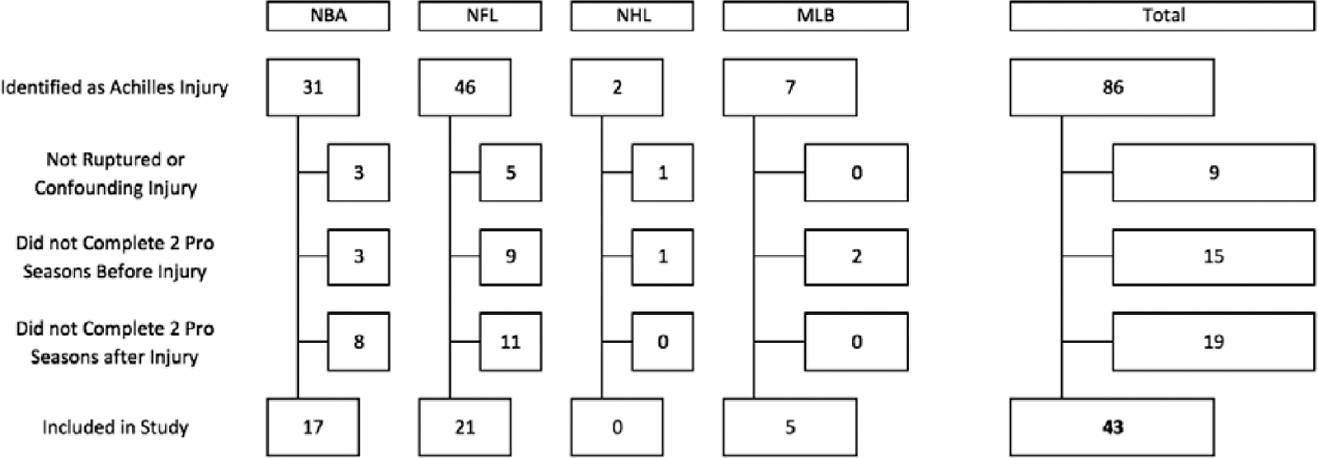
CONSORT (Consolidated Standards of Reporting Trials) flow diagram of inclusion and exclusion criteria for athletes. MLB, Major League Baseball; NBA, National Basketball Association; NFL, National Football League; NHL, National Hockey League.
The 43 athletes who returned to play consisted of 17 NBA, 21 NFL, and 5 MLB players (Table 1). No NHL players were included in the analysis. The average age of athletes returning to play was 29.5 years (range, 23.8-36.7 years) with average ages of 29.1, 29.4, and 31.3 years for the NBA, NFL, and MLB, respectively. The average number of professional seasons played for all athletes was 6.4 (range, 2-16) with an average 7.2, 6.0, and 5.0 seasons played in the NBA, NFL, and MLB, respectively. The mean BMI was 26.1, 33.3, and 27.7 kg/m2 in the NBA, NFL, and MLB, respectively, and was 29.8 kg/m2 overall. Of the 19 athletes who did not return to play, 8 were in the NBA and 11 were in the NFL. No differences were found in the average age, seasons played, or BMI between players who achieved RTP and those who did not (P > .05). Of players unable to return to play, the average age was 29.7 years (range, 24.0-34.3 years), the average number of seasons of professional play was 7.1, and average BMI was 26.7 kg/m2.
Demographic Data for Athletes Returning to Play a
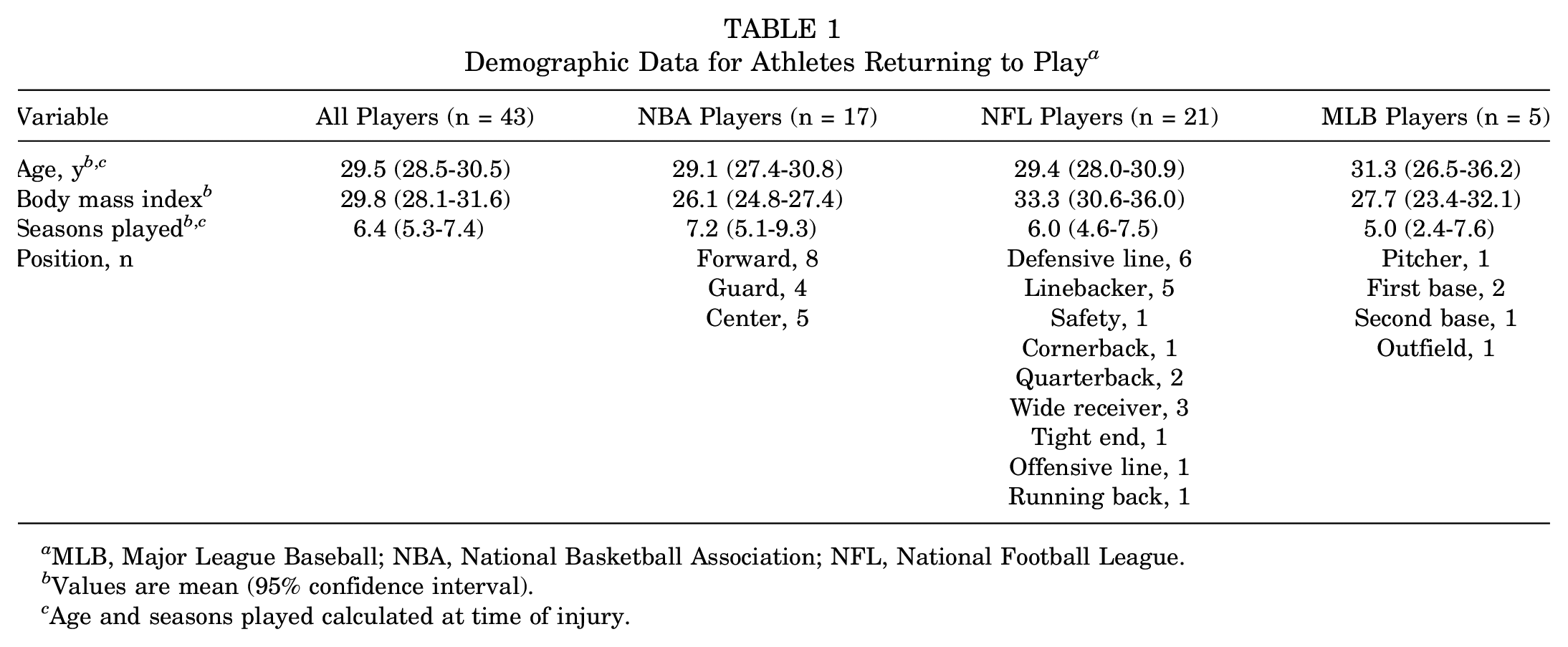
MLB, Major League Baseball; NBA, National Basketball Association; NFL, National Football League.
Values are mean (95% confidence interval).
Age and seasons played calculated at time of injury.
Among athletes returning to play, a significant decrease was noted in games played per season when compared with preoperative baseline values (Table 2, Figure 2). At 1 and 2 years postoperatively, athletes played an average of 75.4% (P < .001) and 81.9% (P = .002) of the games played in the season before injury. When the 3 leagues were analyzed separately, only NBA players played in significantly fewer games at 1 and 2 years postoperatively, 67.5% and 68.5%, respectively (P < .001). NFL players were found to play in fewer games only 1 year after injury (84.4%, P = .040), and no difference was identified in the amount of games played pre- versus postinjury in MLB players.
Comparison of Games Played Preoperatively Versus Postoperatively
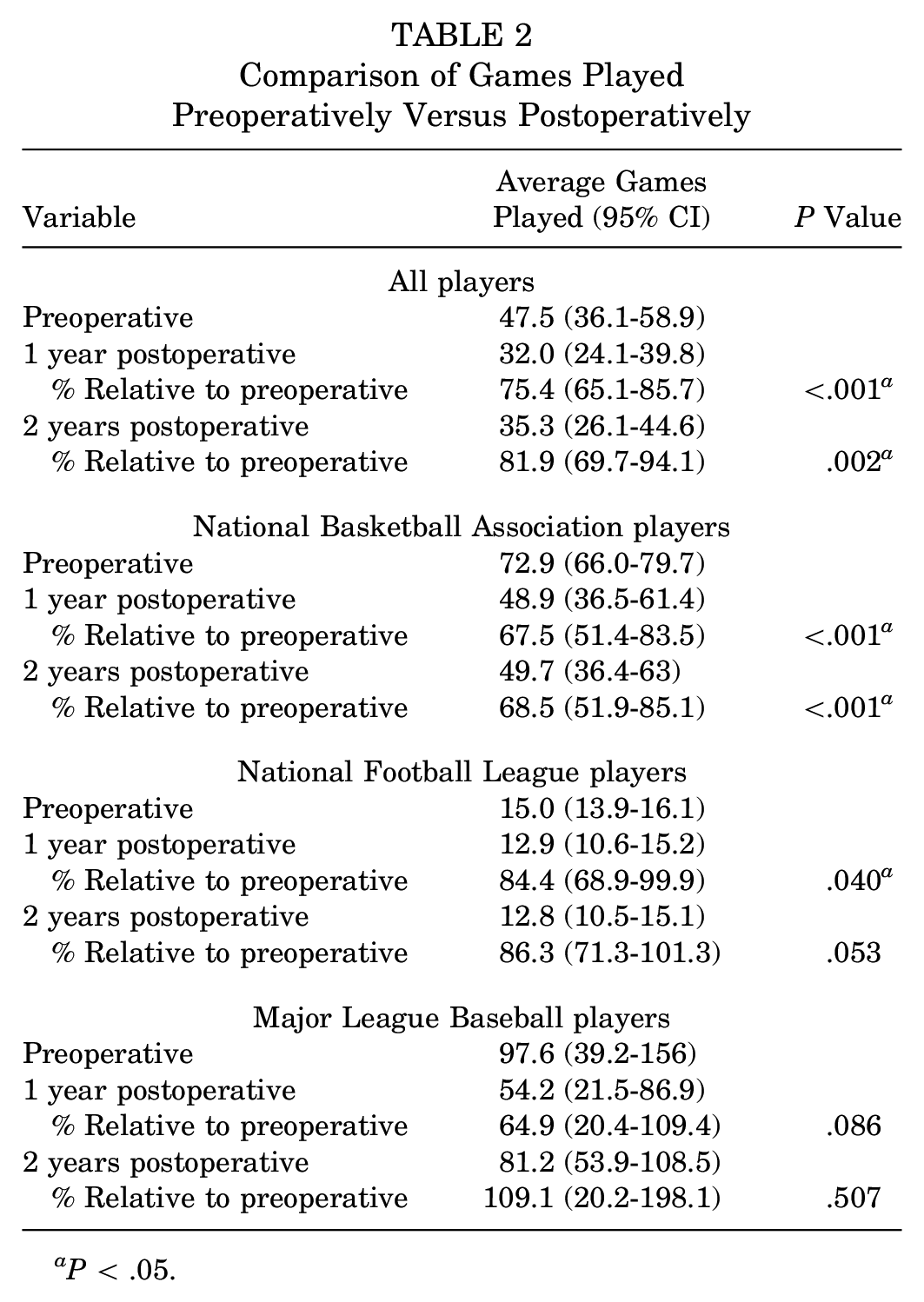
aP < .05.
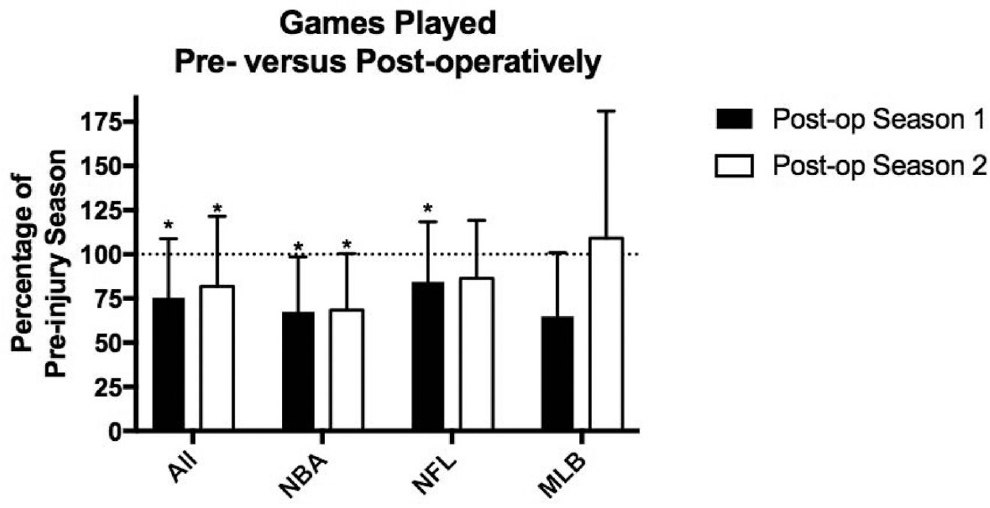
Preoperative versus postoperative comparison of games played among all players and players from the National Basketball Association (NBA), National Football League (NFL), and Major League Baseball (MLB). *P < .05.
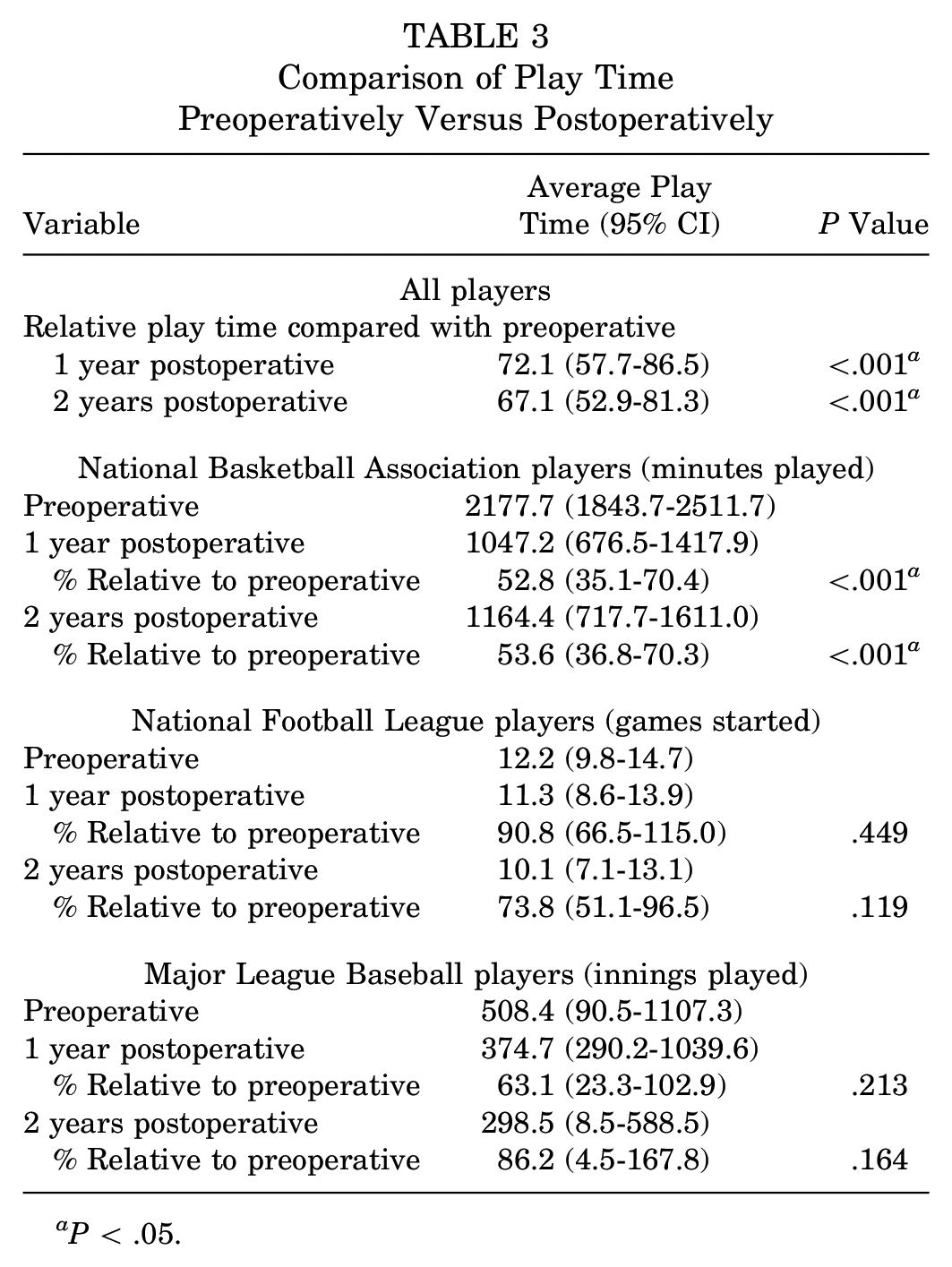
Among all athletes, play time was significantly reduced at 1 year (P < .001) and 2 years (P < .001) postoperatively to 72.1% and 67.1%, respectively, of the preinjury season (Table 3, Figure 3). Similar to our findings regarding games played, NBA players had the greatest reduction in play time: 52.8% and 53.6%, respectively, at 1 and 2 years postoperatively (both P values < .001). No significant decreases in playing time were found after injury in either NFL or MLB players at either time points.
Comparison of Play Time Preoperatively Versus Postoperatively
aP < .05.
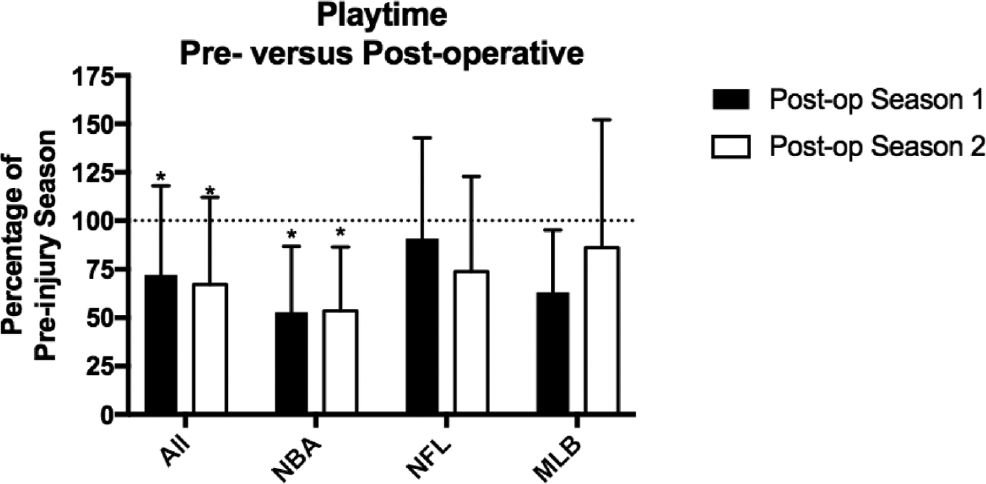
Preoperative versus postoperative comparison of play time among all players and players from the National Basketball Association (NBA), National Football League (NFL), and Major League Baseball (MLB). *P < .05.
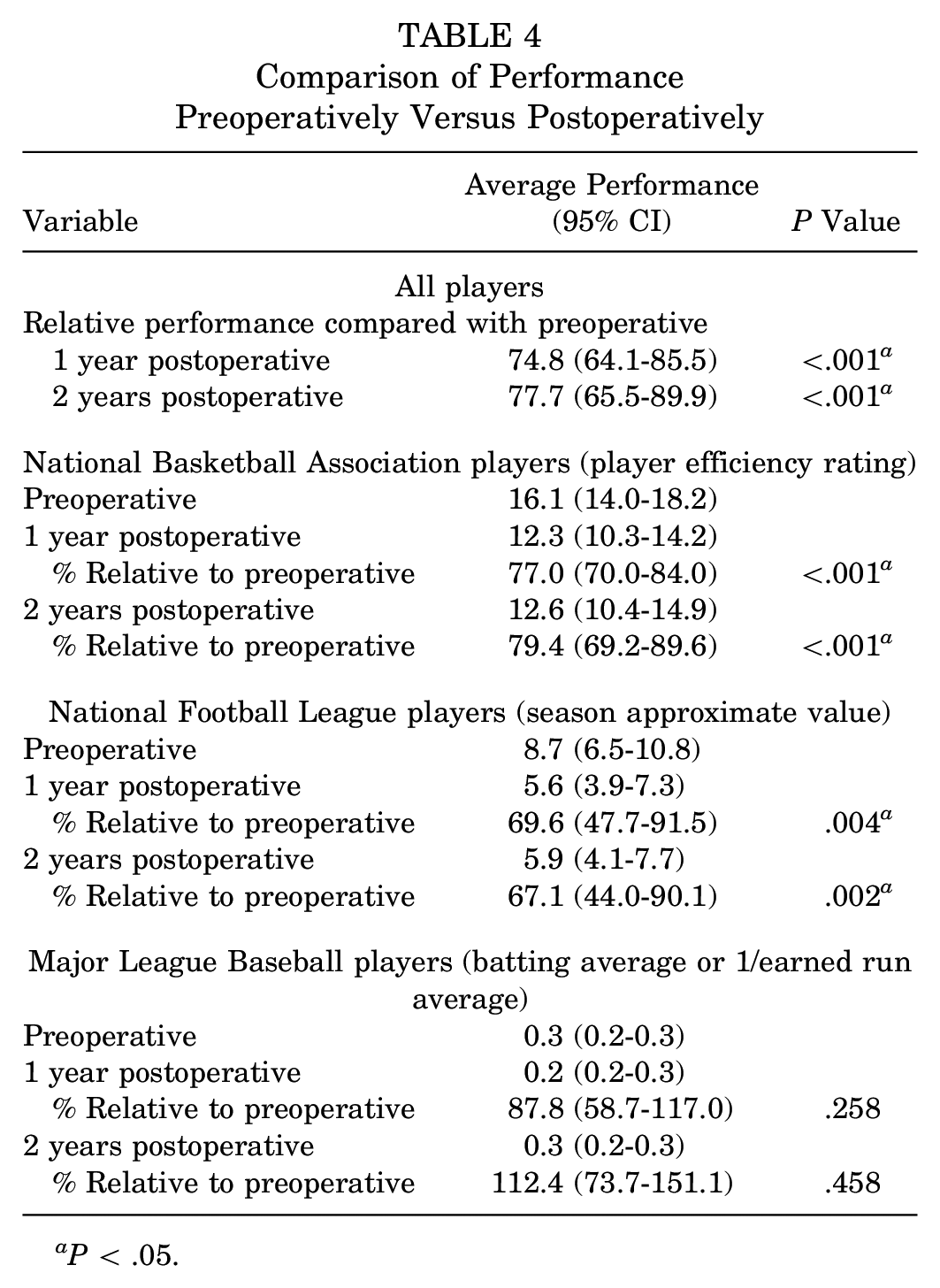
When performance statistics were evaluated among all athletes, players were found to have performed at a significantly lower level at 1 year (74.8%) and 2 years (77.7%) (P < .001) postoperatively (Table 4, Figure 4). NBA players’ performance decreased to 77.0% (P < .001) and 79.4% (P < .001) compared with preinjury baselines, while NFL players performed even worse: 69.6% (P = .004) and 67.1% (P = .002) at 1 and 2 years postoperatively. In contrast, MLB players’ performance was unaffected.
Comparison of Performance Preoperatively Versus Postoperatively
aP < .05.
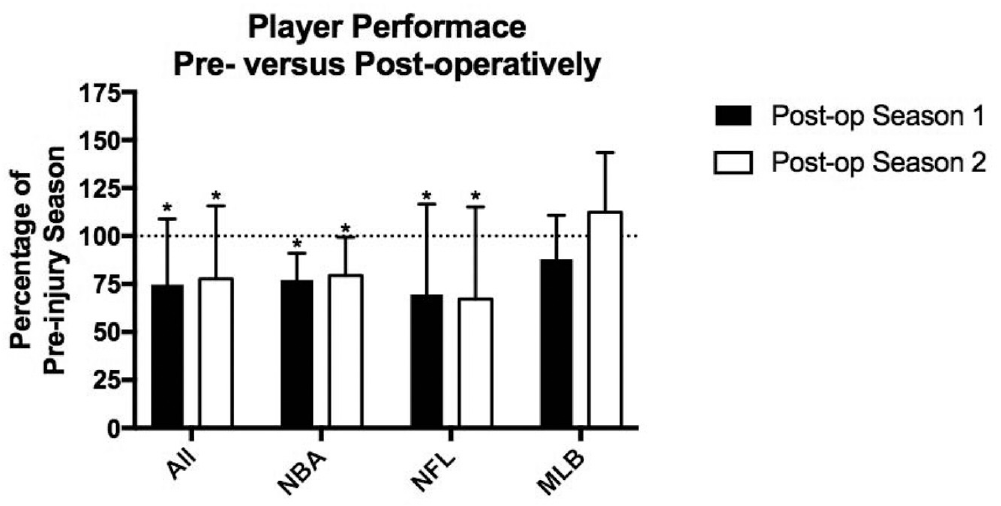
Preoperative versus postoperative comparison of performance among all players and players from the National Basketball Association (NBA), National Football League (NFL), and Major League Baseball (MLB). *P < .05.
When compared with matched controls, injured athletes played significantly fewer games (P < .001), had significantly reduced play time (P = .026), and performed worse (P < .001) 1 year out from injury (Table 5, Figure 5A). However, when players were compared with controls at 2 years after injury, no differences were found in any variable measured (Figure 5B).
Games Played, Play Time, and Performance of Participants Versus Controls Relative to Preoperative Season
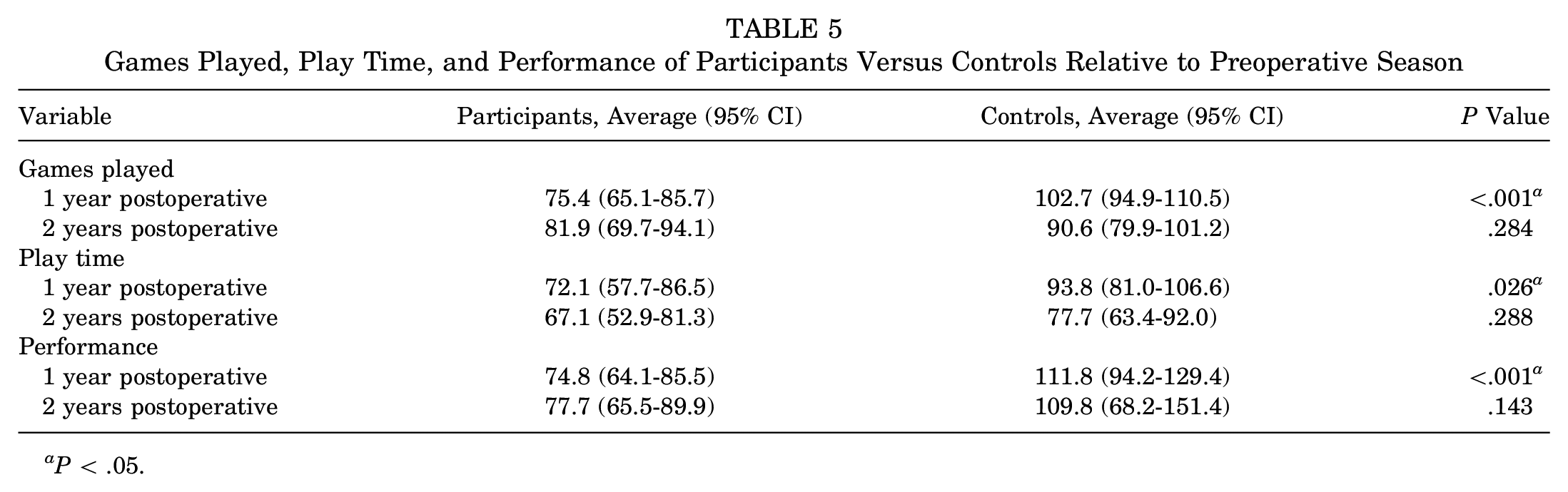
aP < .05.
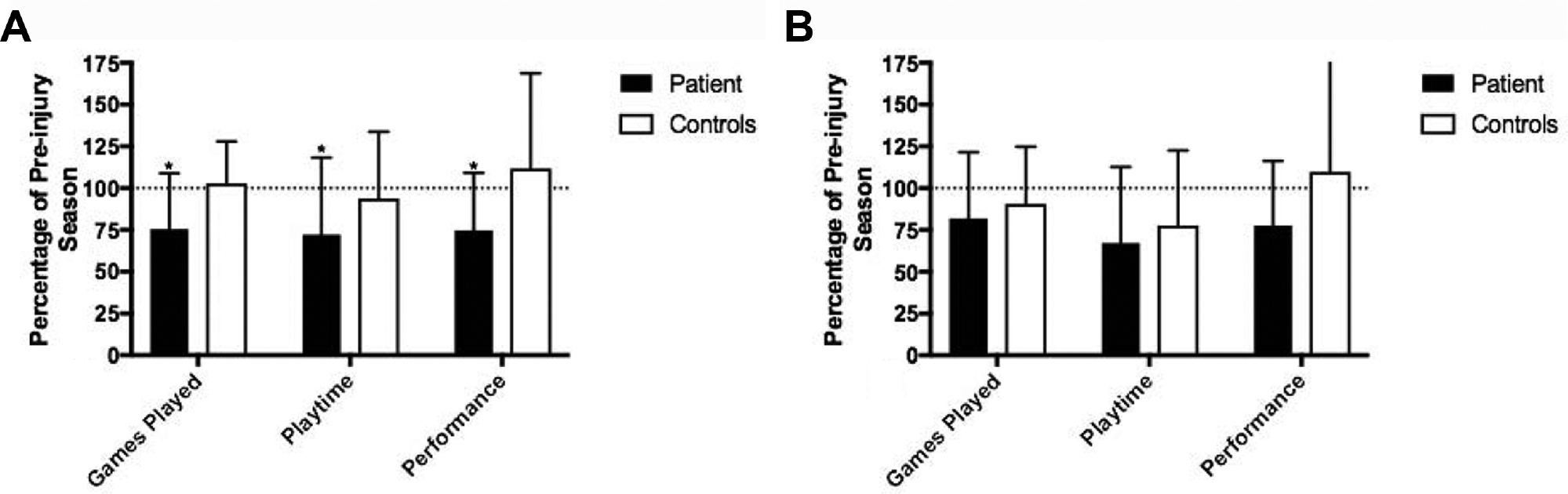
Comparison of functional outcomes between patients and matched controls at postoperative (A) season 1 and (B) season 2. *P < .05.
Discussion
The success of an Achilles tendon repair in the population at large is measured by return to daily activities and athletic endeavors with the avoidance of complications such as rerupture and wound breakdown. Elite athletes, in contrast, represent a unique patient population given the high physical demands of their profession. As such, the success of an Achilles tendon repair requires increased objective scrutiny including RTP and performance metrics. Knowledge of how elite athletes perform after injury is critical for appropriate pre- and postoperative consultation and prognostic expectations for both the weekend warrior eager to return to activity and the professional athlete.
Prior investigations have shown how detrimental an Achilles tendon rupture is to a professional athlete’s career.1,19,22,25 The rate of RTP for NFL athletes was 79.4% after common orthopaedic procedures but was lower after Achilles tendon ruptures. 19 Between 1997 and 2002, Parekh et al 25 identified 31 Achilles tendon ruptures in NFL players and found an RTP rate of 68%. Between 2003 and 2013, Mai et al 19 identified 80 NFL players who underwent an Achilles tendon repair with an RTP rate of 72.5% and significant decreases in games played and performance levels at postoperative season 1. Interestingly, the authors found that performance and games played recovered to baseline levels during postoperative seasons 2 and 3; however, the authors did not compare athletes with matched controls and did not specify how their performance metrics were calculated. This may explain why the current investigation found significantly impaired performance metrics in NFL players at 1 and 2 years postoperatively using the SAV, whereas Mai et al found equivalent performance measures at postoperative seasons 2 and 3. In a similar investigation by the same group on NBA players, Minhas et al 22 found that an Achilles tendon repair was the orthopaedic procedure leading to the highest rate of retirement among players and poorest performance in postoperative seasons. Among the 24 patients identified, RTP was 70.8%. Finally, Amin et al 1 found an RTP rate of 61% among 18 NBA players between 1988 and 2011.
In the current investigation, NBA, NFL, MLB, and NHL athletes were investigated to determine the general effect of Achilles tendon repairs on professional athletes. Overall, 30.6% of athletes were unable to return to play for 2 consecutive years after injury. Furthermore, all functional outcomes investigated were significantly affected compared with preinjury levels. However, the crux of this investigation is that for the participants, compared with controls, only 1-year outcome metrics were inferior. This implies that if professional athletes are able to return to play and endure beyond their first season, they may achieve playing time and performance equivalent to those of controls. Our study indicates that there is likely a bimodal distribution of successful RTP: A significant portion of athletes undergoing repair never return to their prior level of competition, but those who do return to their prior level can often perform at a level commensurate with noninjured controls after 2 years.
To our knowledge, this study reports on the second largest collection of professional athletes undergoing Achilles tendon repair and is the first to compare functional outcomes across multiple professional leagues. While the NFL and NBA had similar RTP rates, 65.6% and 68.0%, respectively, basketball players were the most significantly affected in regard to all functional outcomes measured at both postoperative time points. In contrast, NFL players performed worse postoperatively but had no significant changes in postoperative games played or overall play time. All 5 MLB players were unaffected by their Achilles tendon repair in regard to functional outcomes, and no NHL player was identified to include within our analysis.
While previous investigations have suggested that age and BMI are independent negative predictors of RTP after various orthopaedic operations, 22 we found no difference in the average age, years of professional experience, or BMI in players undergoing an Achilles tendon repair who returned to play versus those who did not return. However, according to publically available demographics information regarding the average age and career lengths in professional leagues, athletes who sustained an Achilles tendon rupture regardless of RTP status were on average 2.7 years older with 1.7 years more professional experience than the average professional player. As such, and in line with findings from prior investigations,1,19,22 an Achilles tendon rupture is an injury of veteran professional athletes. Given that the average age for rupture in the general male population has increased to 44.4 years, it is possible that more experienced professional players are more likely to develop tendinosis, predisposing them to rupture, especially since professional athletes in these sports will be subject to regular eccentric contracture of the tendon.27,35
The increased age and experience level of athletes rupturing their Achilles tendon may be a key reason why the RTP rate after rupture is so poor. These athletes may have been approaching retirement age before their injury, giving them less incentive to undergo the rigorous rehabilitation process necessary to play at a professional level. It also may explain why athletes had worse functional outcome scores postoperatively at 1 and 2 years, when players were on average 30 and 31 years old, compared with their preinjury levels, when they were on average 28 years old. As such, not only were athletes overcoming a serious surgical injury, but they were also playing against younger competition postoperatively. Thus, the use of matched controls allowed for a fairer assessment of athletes’ postoperative function.
The strengths of this investigation include the use of simple and reproducible outcome variables. Additionally, by excluding any athlete with less than 2 years of preinjury professional play, we ensured that athletes were included for analysis only if they were well-established in their leagues. This avoided inclusion of rookies and players who only transiently played professionally. Furthermore, a strict definition of RTP was implemented ensuring a sustained return to professional involvement for a minimum of 2 years. Finally, this is the first large investigation to assess postoperative professional performance in players who have undergone Achilles tendon repair compared with matched controls. Previously, the only such case-control study was by Amin et al, 1 who compared 11 NBA players to matched controls and found a decrease in performance and minutes played postoperatively.
Our investigation has certain limitations. To begin, various confounding variables that could not be controlled by our method may have affected a player’s RTP and performance. These include differences in team playing style, concomitant minor or unreported injuries that were not identified, athletes’ personal or professional decisions for retirement unrelated to medical conditions, and selection bias where more popular or well-known players were more easily identified for inclusion. Additionally, we did not have access to any information regarding plausible preinjury symptoms that may have preceded rupture, which would have been useful information in regard to preventive care. Further, given that the majority of data obtained in this investigation were from publically accessible websites, there is no legitimate method to verify the accuracy or completeness of the available data. Moreover, over the period of time during which these data were collected, treatment paradigms changed significantly with regard to both surgical treatment and rehabilitation in a way that this investigation could not take into account, as we had no clinical data on these patients. The study design also could not account for various factors that may have affected recovery, including repair technique, use of augmentation (such as cartilage matrix or bone marrow aspirate), unreported complications, or individual rehabilitation protocols. Finally, our analysis was limited by the number of athletes in each league, particularly the MLB, who had sustained an Achilles tendon rupture treated surgically. Despite this, our a priori power analysis indicated that we did identify enough athletes to find a significant difference in performance metrics between patients and controls.
In conclusion, across multiple professional leagues, the failure rate for RTP after an Achilles tendon rupture treated surgically is 30.6%. However, those athletes who do return can expect to perform at a level equivalent to that of healthy controls by their second season after injury. These results can assist orthopaedic professionals caring for athletes of all levels in regard to managing patient expectations and prognosis after an Achilles tendon rupture.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: J.K.G. is a paid consultant for and receives research support from Extremity Medical and receives publishing royalties from Saunders/Mosby-Elsevier. J.T.V. is a paid consultant for DJ Orthopaedics.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.