
Abstract
Background:
A goal of anterior cruciate ligament (ACL) reconstruction is to provide a meniscal protective effect for the knee.
Purpose:
(1) To evaluate whether there was a different likelihood of subsequent meniscal surgery in the ACL-reconstructed knee or in the normal contralateral knee and (2) to compare the risk factors associated with subsequent meniscal surgery in the ACL-reconstructed knee and contralateral knee.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Using an integrated health care system’s ACL reconstruction registry, patients undergoing primary ACL reconstruction, with no meniscal injury at the time of index surgery and a normal contralateral knee, were evaluated. Subsequent meniscal tears associated with ACL graft revision were excluded. Subsequent meniscal surgery in either knee was the outcome of interest. Sex, age, and graft type were assessed as potential risk factors. Survival analysis was used to compare meniscal surgery–free survival rates and to assess risk factors of subsequent meniscal surgery.
Results:
Of 4087 patients, there were 32 (0.78%) patients who underwent subsequent meniscal surgery in the index knee and 9 (0.22%) in the contralateral knee. The meniscal surgery–free survival rate at 4 years was 99.08% (95% CI, 98.64%-99.37%) in the index knee and 99.65% (95% CI, 99.31%-99.82%) in the contralateral knee. There was a 3.73 (95% CI, 1.73-8.04; P < .001) higher risk of subsequent meniscal surgery in the index knee compared with the contralateral knee, or a 0.57% absolute risk difference. After adjustments, allografts (hazard ratio [HR], 5.06; 95% CI, 1.80-14.23; P = .002) and hamstring autografts (HR, 3.11; 95% CI, 1.06-9.10; P = .038) were risk factors for subsequent meniscal surgery in the index knee compared with bone–patellar tendon–bone (BPTB) autografts.
Conclusion:
After ACL reconstruction, the overall risk of subsequent meniscal surgery was low. However, the relative risk of subsequent meniscal surgery in the ACL-reconstructed knee was higher compared with the contralateral knee. Only graft type was found to be a risk factor for subsequent meniscal surgery in the ACL-reconstructed knee, with a higher risk for allografts and hamstring autografts compared with BPTB autografts.
Anterior cruciate ligament (ACL) tears are one of the most common sports injuries, and frequently these injuries require surgical reconstruction. 9 It is estimated that there are nearly 200,000 ACL reconstructions performed annually in the United States. 1 ACL reconstruction is performed in an attempt to restore knee stability and allow the patient to return to athletic activity. It is also thought that ACL reconstruction will provide protection from subsequent meniscal injuries, which may ultimately help decrease the progression of degenerative joint disease.
Determining the effectiveness of ACL reconstruction is challenging. Commonly used measurements to assess the success of ACL reconstruction include subjective measurements (eg, patient-reported function, pain, quality of life), objective measurements of stability (eg, Lachman test, pivot-shift test, KT-1000 arthrometer), postoperative imaging, and reoperations (eg, irrigation and debridement of infections, hardware removal). While these various outcome variables are useful, they all have shortcomings. These include reporting bias, varying reliability of subjective measures,3,21,24 possible lack of interrater reliability in stability testing22-24 and imaging, 25 and general lack of reliable and consistent clinical examinations. 18 In addition, obtaining these measurements in large cohorts of patients is both difficult and costly. 2 Another common outcome measurement for ACL reconstruction is revision ACL reconstruction. Revision ACL reconstruction represents an obvious failure of the initial surgery and is the outcome most often reported by large ACL reconstruction registry studies.8,15 However, revision ACL reconstruction is relatively rare, and determining the effectiveness of ACL reconstruction in providing stability can be difficult.
One potential way to evaluate postoperative stability is to determine the incidence of subsequent meniscal surgery after ACL reconstruction. Ideally, ACL reconstruction restores normal stability and kinematics to the injured knee, and therefore, the likelihood of requiring subsequent meniscal surgery should be the same in the reconstructed knee and the uninjured contralateral knee. While multiple studies have looked at reoperations after ACL reconstruction,5,14,26 few studies have focused specifically on meniscal injuries or surgery after ACL reconstruction.4,6 Those studies focusing on subsequent meniscal tears or surgery have suggested that ACL reconstruction provides a meniscal protective effect compared with nonoperative treatment.4,6 However, large studies comparing meniscal surgery after ACL reconstruction in the uninjured contralateral knee are lacking.
There were 2 main objectives of this study. The first was to determine the meniscal protective effect of ACL reconstruction. This was accomplished by evaluating whether there was a different risk of subsequent meniscal surgery in the ACL-reconstructed knee compared with the uninjured contralateral knee. The second was to compare the risk factors associated with subsequent meniscal surgery in the ACL-reconstructed knee and the uninjured contralateral knee. Our hypothesis was that the incidence of subsequent meniscal surgery would be higher in the operative knee than in the contralateral knee and that the incidence of subsequent meniscal surgery would vary with graft type.
Methods
Study Design, Setting, Data Source, and Sample
A retrospective analysis of prospectively collected data of a cohort of patients undergoing ACL reconstruction, registered in the Kaiser Permanente ACL Reconstruction Registry (KPACLRR), was performed. The KPACLRR data collection procedures, participation, and data integrity have been published previously.15,17 In brief, demographic and surgical data are collected by the surgeon at the point of care. Additional data for the registry are abstracted from administrative databases and the institution’s electronic health record (EHR) system. The registry prospectively monitors patients for postoperative complications, including reoperations and revisions. All postoperative events are reviewed by trained clinical content experts using EHRs.
Between February 1, 2005, and December 31, 2014, 243 surgeons from 42 hospitals in 6 geographic regions throughout the United States (Hawaii, Southern California, Northern California, Northwest, Mid-Atlantic, and Colorado) registered patients in the KPACLRR. Patients undergoing primary single-ligament ACL reconstruction were included in the study; patients with concomitant meniscal pathological changes (as defined by the operating surgeon), abnormal contralateral knees noted at the time of surgery (as defined by the operating surgeon), primary ACL reconstruction in both knees, revision ACL surgery, and patients in whom the graft type was unknown were excluded (Figure 1). Subsequent meniscal tears associated with ACL graft revision were not counted; thus, only patients with an intact ACL graft were included in this analysis. This study was approved by the institutional review board of the integrated health care system before data collection.
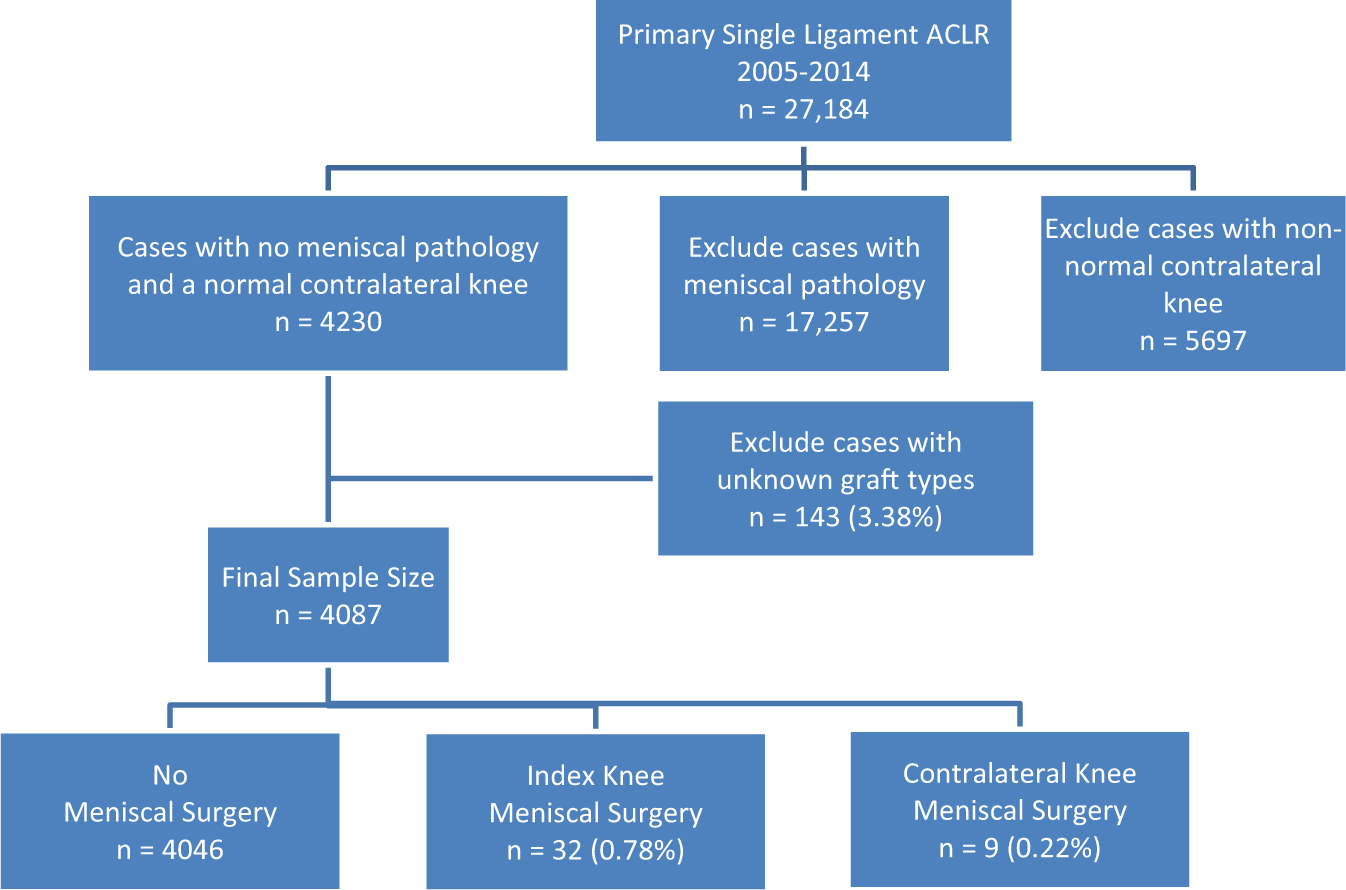
Flowchart of study sample selection. ACLR, anterior cruciate ligament reconstruction.
Outcome of Interest
The main outcome of this study was meniscal surgery (in either knee) after primary ACL reconstruction. Meniscal surgeries were prospectively captured by the registry using passive surveillance (surgeon-reported) and validated through a review of patients’ EHRs.
Exposures of Interest and Covariates
Primary ACL reconstruction was the main exposure of interest in this study. In the first analysis, the risk of subsequent meniscal surgery was evaluated by comparing the ACL-reconstructed knee to the contralateral nonreconstructed knee. In the second analysis, patients’ sex, age, and graft type used for ACL reconstruction were examined as possible risk factors for meniscal reoperations in both the index knee and contralateral knee. Graft type was classified as bone–patellar tendon–bone (BPTB) autograft, hamstring autograft, and any type of allograft determined from intraoperative KPACLRR forms.
Statistical Analysis
The study sample characteristics and graft type were described using frequencies, proportions, means, SDs, medians, and interquartile ranges (IQRs). Categorical characteristics were compared using chi-square tests. Continuous characteristics were compared using nonparametric Wilcoxon-Mann-Whitney tests. In the first analysis, a Poisson regression model with a likelihood ratio test was used to compare meniscal surgery per 100 years of observation for the index knee versus the contralateral knee. Survival analyses were performed using Kaplan-Meier curves (log-rank test compared survival distributions) to describe cumulative survival probabilities; gamma frailty models examined the risk of meniscal surgery in the index knee compared with the contralateral knee. For the second analysis, multivariable Cox proportional hazards models (Wald test) were used to assess potential risk factors for subsequent meniscal surgery in the same knee compared with the contralateral knee. Follow-up time was defined as the difference between the date of the original ACL reconstruction and the date of meniscal surgery, the date of revision surgery, the date of membership termination from the integrated health care system, the date of death, or the end date of the study period, whichever occurred first. Survival analyses censored patients who underwent revision surgery, died before the end of the study period, or terminated their membership. Hazard ratios (HRs), 95% CIs, and Wald chi-square P values are provided. Nesting of observations within the surgeon variable (clustering) was accounted for in the model. 12 No outliers were observed in this sample. The proportionality assumption for age was verified using the supremum test for functional form. Proportionality assumptions for sex and graft type were verified using Kaplan-Meier curves. Collinearity was assessed with variance inflation factors and tolerance values. Graft information was missing for 3.38% (n = 143) of patients, and these were excluded from the sample. Data were analyzed using SAS v9.2 software (SAS Institute), with an alpha of 0.05 as the statistical threshold for significance.
Results
Study Sample
There were 4087 patients who underwent primary ACL reconstruction included in the sample. Characteristics of the patient sample are provided in Table 1. The cohort included 2295 male patients (56.15%), and the median age at the time of surgery was 26.09 years (IQR, 18.02-36.17 years). There were 1113 (27.23%) ACL reconstructions performed with BPTB autografts, 1385 (33.89%) with hamstring autografts, and 1589 (38.88%) with allografts. The mean (±SD) follow-up time was 3.51 ± 2.41 years (IQR, 1.40-5.51 years). There were 874 (21.38%) patients lost to follow-up, and the mean follow-up time for these patients was 2.96 ± 2.10 years.
Study Sample Characteristics Overall and by Subsequent Meniscal Surgery Status a
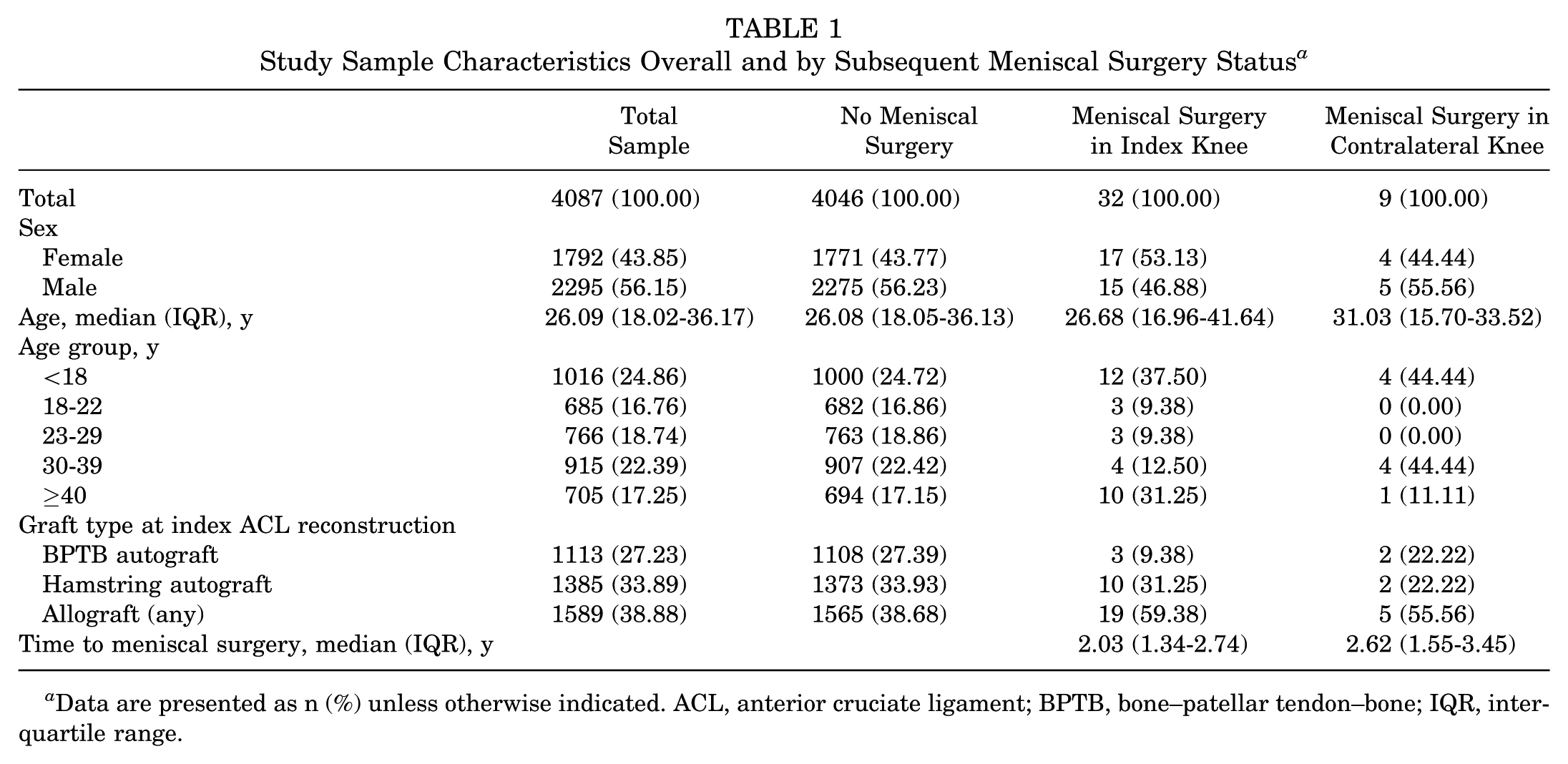
Data are presented as n (%) unless otherwise indicated. ACL, anterior cruciate ligament; BPTB, bone–patellar tendon–bone; IQR, interquartile range.
Risk of Subsequent Meniscal Surgery in the Index Knee Compared With the Contralateral Knee
There were 32 (0.78%) patients with subsequent meniscal surgery in the ACL-reconstructed knee and 9 (0.22%) patients with subsequent meniscal surgery in the contralateral knee (Table 2). The meniscal surgery–free survival probability at 4 years was 99.08% (95% CI, 98.64%-99.37%) in the ACL-reconstructed knee and 99.65% (95% CI, 99.31%-99.82%) in the contralateral knee (Figure 2). There was a 3.73 (95% CI, 1.73-8.04; P < .001) higher risk of subsequent meniscal surgery in the index knee compared with the contralateral knee, or a 0.57% absolute risk difference.
Crude Incidence and Incidence Density of Meniscal Surgery After Primary ACL Reconstruction a
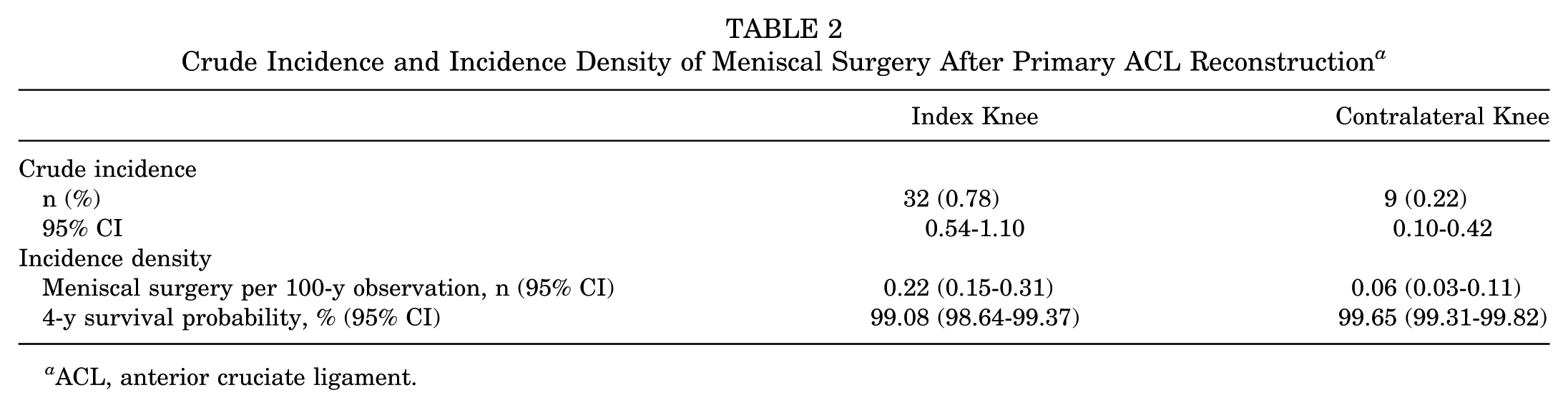
ACL, anterior cruciate ligament.
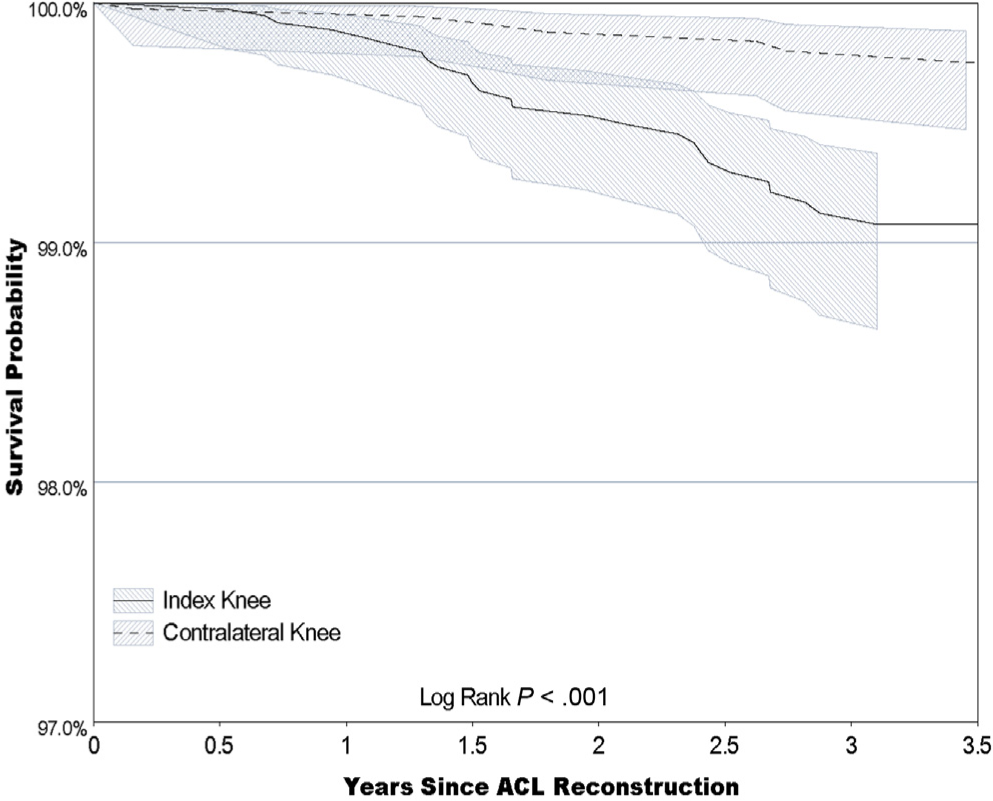
Kaplan-Meier meniscal surgery–free survival estimates of primary anterior cruciate ligament (ACL) reconstruction by knee.
Risk Factors Associated With Subsequent Meniscal Surgery
After adjusting for all variables, sex and age were not associated with a risk of subsequent meniscal surgery on either the ACL-reconstructed knee or the contralateral knee (Table 3). Allografts (HR, 5.06; 95% CI, 1.80-14.23; P = .002) and hamstring autografts (HR, 3.11; 95% CI, 1.06-9.10; P = .038) were associated with a higher risk of meniscal surgery in the ACL-reconstructed knee when compared with BPTB autografts. No association between graft type and meniscal surgery in the contralateral knee was observed.
Risk Factors of Meniscal Surgery After Primary ACL Reconstruction a
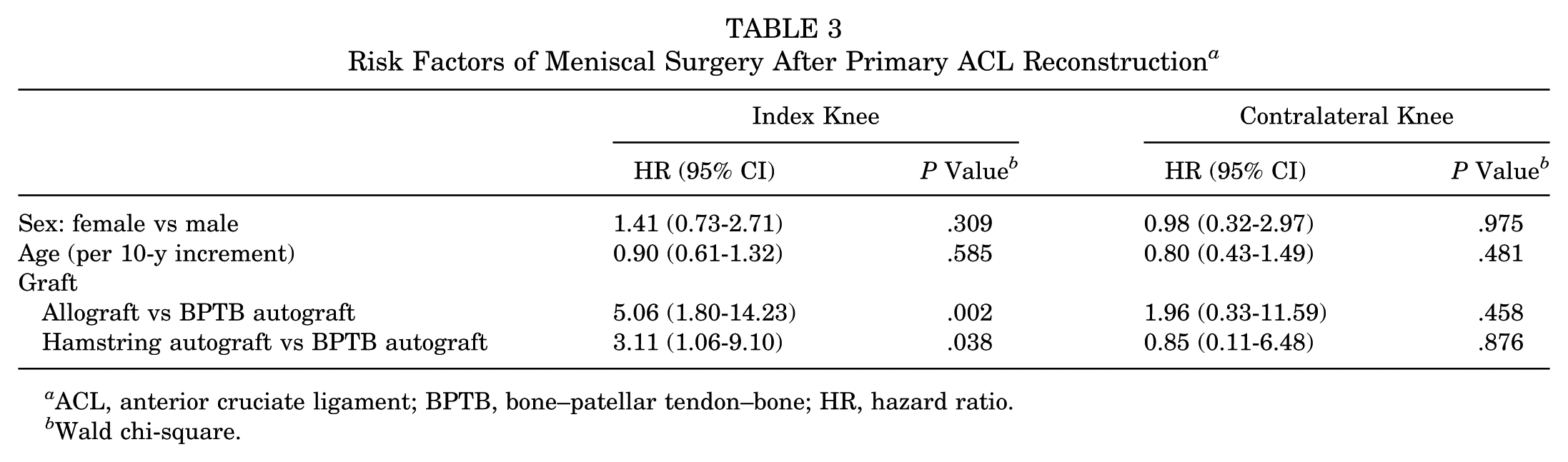
ACL, anterior cruciate ligament; BPTB, bone–patellar tendon–bone; HR, hazard ratio.
Wald chi-square.
Discussion
ACL graft tears and revision ACL reconstruction are obvious failures of ACL reconstruction. However, it is possible that a knee may demonstrate functional instability even with a graft that remains intact. The purpose of this study was to evaluate the meniscal protective effect of ACL reconstruction in knees in which the graft remains intact. To accomplish this, we evaluated patients from a large community-based ACL reconstruction registry with no meniscal injuries at the time of ACL reconstruction and a normal contralateral knee. Subsequent meniscal surgery in either knee was then evaluated. There was a 3.73 times higher likelihood (0.57% absolute risk difference) of subsequent meniscal surgery in the index knee compared with the contralateral knee.
A few studies have evaluated subsequent meniscal injuries and surgery after ACL reconstruction.4-6,11,14 A small case series by Ichinohe et al 11 evaluated subsequent meniscal tears in the same knee after ACL reconstruction with second-look arthroscopic surgery in 72 patients. At the initial surgery, 40 medial menisci and 31 lateral menisci demonstrated no tears. At repeat arthroscopic surgery, approximately 16 months after ACL reconstruction, there were 3 new medial meniscal tears and 3 new lateral meniscal tears. No association was reported between subsequent meniscal tearing and knee stability, but it is likely that their sample size was too small to detect such differences. Lyman et al, 14 using a database of hospital admissions and ambulatory surgeries in New York state, found a subsequent surgery rate of 6.5% for either knee at 1 year. Of these, 24.5% were meniscectomies. However, the data in the New York state system only listed laterality in a minority of cases, so a comparison between the ACL-reconstructed knee and the contralateral knee was not possible. Csintalan et al, 5 using the same data source as the current study, showed an overall reoperation rate for meniscal surgery in the ACL-reconstructed knee of 1.6%. Although this rate is similar to the meniscal reoperation rate in the current study, the 2 values are not directly comparable. The study by Csintalan et al 5 had a shorter length of follow-up than the current study (1.9 years vs 3.5 years, respectively), and their study did not exclude patients with meniscal injuries at the time of ACL reconstruction.
Dunn et al 6 performed a retrospective cohort study using an administrative database. Active-duty soldiers who underwent ACL reconstruction were compared with a cohort of patients who underwent nonoperative treatment for an ACL tear. 6 The authors reported that ACL reconstruction was protective against subsequent lateral meniscal injuries requiring surgery (56% relative reduction) and medial meniscal reoperations (42% relative reduction). The authors concluded that ACL reconstruction was protective against subsequent meniscal and cartilage injuries requiring surgery. Similarly, in a recent meta-analysis, Chalmers et al 4 reported that patients who had undergone ACL reconstruction underwent fewer subsequent meniscal surgeries (13.9%) than patients who had undergone nonoperative treatment for their ACL tear (29.4%). This represents an absolute risk difference of 15.5%. In a study comparing early ACL reconstruction to rehabilitation without ACL reconstruction, Frobell et al 7 reported that 19 of 59 patients in the nonreconstruction treatment group underwent subsequent meniscal surgery while only 5 of 60 in the early ACL reconstruction group underwent subsequent meniscal surgery. This represents an absolute risk difference of 23.9%. The authors attributed this difference to the fact that small meniscal tears at the time of ACL injury were more likely to be left untreated in the nonreconstruction group than in the ACL reconstruction group. However, the number of subsequent meniscal tears (ie, tears that were not present at the time of ACL injury but occurred later) in the nonreconstruction group was not reported. While these studies indicated that ACL reconstruction provides a meniscal protective effect compared with nonoperative treatment, they did not provide a comparison to the uninjured knee.
The results of our study are consistent with those reported from the Multicenter Orthopaedic Outcomes Network (MOON) and published by Hettrich et al. 10 In this study, 905 ACL reconstructions with a 6-year follow-up were evaluated. 10 The reported incidence of subsequent meniscal surgery was 5.7% for the medial meniscus and 3.7% for the lateral meniscus. For the contralateral knee, the reported incidence of subsequent meniscal surgery was 4.0% for the medial meniscus and 2.7% for the lateral meniscus. However, this study did not take into account meniscal procedures performed at the time of index surgery nor the condition of the contralateral knee at the time of index surgery. Because the confounding issue of existing meniscal injuries was not removed in their study, one cannot assume that subsequent meniscal surgery represents new meniscal injuries.
The overall incidence of subsequent meniscal surgery in the ACL-reconstructed knee in our study was quite low, with a crude incidence of 0.78% (95% CI, 0.54%-1.10%). This is consistent with the previously discussed studies. However, the current study indicates that while the meniscal protective effect of ACL reconstruction is excellent, it is not quite as good as the native ACL. There are 3 likely reasons for the higher incidence of subsequent meniscal surgery in the ACL-reconstructed knee. The first possibility is that the higher incidence is because of an intrasubstance meniscal injury that was not seen at the time of surgery or postoperative factors such as residual knee stiffness or persistent loss of strength. However, if these were the main factors, it is unlikely that graft type would lead to a variation in the incidence of subsequent meniscal surgery. The other likely possibilities are that (1) current ACL reconstruction techniques, in general, do not stabilize the knee as well as the native ACL and (2) ACL reconstruction has meniscal protective effects comparable with the native ACL except when the surgical technique or graft incorporation is suboptimal (eg, graft malposition or graft stretch). If the latter is true, which is more likely the case, then subsequent meniscal surgery may represent another method for determining graft failure beyond revision surgery. Further investigation on this topic is necessary.
In the current study, allografts and hamstring autografts were associated with a higher risk of meniscal surgery in the ACL-reconstructed knee when compared with BPTB autografts. In fact, only 3 index and 2 contralateral reoperations were needed when a BPTB autograft was used. Other similarly large registry studies have reported a higher risk of revision ACL reconstruction with allografts or hamstring autografts when compared with BPTB autografts8,13,16,19,20,26 but not a higher risk of meniscal surgery when those grafts are used. It may be that allografts and hamstring autografts do not restore stability or kinematics as well as BPTB autografts. It is also possible that subsequent meniscal surgery after ACL reconstruction represents an early marker for failure of the graft, and thus, the increased incidence of meniscal surgery is related to the higher failure rates reported for allografts and hamstring autografts. Further study is needed to determine if knees undergoing subsequent meniscal surgery go on to a higher rate of revision ACL surgery.
There are several limitations to this study. The outcome was defined by subsequent meniscal surgery; postoperative magnetic resonance imaging or second-look arthroscopic surgery was not used to determine a subsequent meniscal tear. By including only operative meniscal tears, we are likely underestimating the cumulative incidence of meniscal injuries in our patients, but probably not underestimating the risk estimates, as we do not expect this underestimation to differ according to the index knee and contralateral knee. Another limitation includes those lost to follow-up in our cohort. Although this study includes a large number of patients, 21.38% of those included in the study were lost to follow-up. In addition, when evaluating the risk factors for subsequent meniscal surgery in each knee, our analysis could be biased by unmeasured confounding. Because of the nature of our study design and data source, certain possible confounders could not be evaluated. For example, the type of reconstruction and postoperative rehabilitation were left up to the individual surgeon and patient and were not standardized or recorded for analytical adjustments. Other possible confounders such as postoperative activity levels were not assessed. Finally, although the higher incidence of meniscal surgery in the index knee indicates that the ACL-reconstructed knee did not return to normal stability, the stability of the knee as determined by other objective measurements (Lachman test, pivot-shift test, KT-1000 arthrometer) is not known.
The strengths of this study include its large and representative sample. This large number of patients allows for the evaluation of multiple risk factors including graft type, age, and sex. In addition, every attempt was made to eliminate the confounding effects of prior meniscal injuries. To achieve this, only patients with no meniscal injury in the operative knee at the time of ACL reconstruction were included in this study. In this registry, all visible meniscal tears at the time of surgery are reported including partial-thickness tears and small tears not requiring treatment. Meniscal injuries that cannot be seen at the time of arthroscopic surgery are not captured. Similarly, only those patients with a normal contralateral knee (as deemed by the operating surgeon) were included in the study. This strict inclusion criterion allows us to assume that, immediately after the index ACL reconstruction, both knees have an intact ACL and no meniscal tears. Therefore, any subsequent meniscal surgery can be considered to represent a new meniscal injury. We recognize that it is possible that because the contralateral knee did not routinely undergo magnetic resonance imaging before the index ACL reconstruction, asymptomatic meniscal pathological conditions may have existed in the contralateral knee at the time of index ACL reconstruction. However, this suggests that the observed incidence of subsequent meniscal tears in the contralateral knee is actually higher than the expected number of new subsequent meniscal tears had we been able to initially exclude patients with asymptomatic meniscal pathological conditions in the contralateral knee at the time of ACL reconstruction. Thus, the higher incidence of subsequent meniscal surgery in the ACL-reconstructed knee compared with the contralateral knee is likely to be underestimated rather than overestimated. Another strength of our study is the large and diverse patient, surgeon, and hospital sample from a United States community-based setting, making these results generalizable to most sports medicine practices. The prospective data collection of our data source and the methodology for the ascertainment of reoperations ensure that the data presented have high internal validity.
Conclusion
The overall incidence of subsequent meniscal surgery in an ACL-reconstructed knee in our study was quite low. However, the current study indicates that this meniscal protective effect is not perfect and that the ACL-reconstructed knee remains at a higher risk for subsequent meniscal surgery than the contralateral knee. In addition, allografts and hamstring autografts were associated with a higher risk of subsequent meniscal surgery in the ACL-reconstructed knee when compared with BPTB autografts. This information should be considered when determining the appropriate graft choice for ACL reconstruction, and meniscal surgery after ACL reconstruction should be considered as an outcome variable when comparing various ACL reconstruction techniques.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.