
Abstract
Background:
No meta-analysis has compared outcomes of operative and nonoperative proximal hamstring avulsion treatment.
Purpose:
To compare outcomes of operative and nonoperative proximal hamstring avulsion treatment, including acute, chronic, partial, and complete repairs.
Study Design:
Meta-analysis.
Methods:
PubMed, CINAHL, SPORTdiscus, Cochrane Library, EMBASE, and Web of Science were searched up to July 2016. Three authors screened the studies and performed quality assessment using criteria from the Methodologic Index for Nonrandomized Studies. A best evidence synthesis was subsequently used.
Results:
Twenty-four studies (795 proximal hamstring avulsions) were included. Twenty-two studies included proximal hamstring avulsion repairs; 1 study had proximal hamstring avulsion repairs and a control group of nonoperatively treated proximal hamstring avulsions; and 1 study had solely nonoperatively treated proximal hamstring avulsions. The majority of studies were of low methodological quality. Overall, repairs had significantly higher patient satisfaction (90.81% vs 52.94%), hamstring strength (85.01% vs 63.95%), Lower Extremity Functional Scale scores (72.77 vs 69.53), and single-legged hop test results (119.1 vs 56.62 cm) (all P < .001); complications occurred in 23.17% of cases. Compared with chronic repairs, acute avulsion repairs had greater patient satisfaction (95.48% vs 83.79%), less pain (1.07 vs 3.71), and greater strength (85.2% vs 82.8%), as well as better scores for the Lower Extremity Functional Scale (75.64 vs 71.5), UCLA activity scale (University of California, Los Angeles; 8.57 vs 8.10), and Single Assessment Numeric Evaluation (93.36 vs 86.50) (all P < .001). Compared with partial avulsion repairs, complete avulsion repairs had higher patient satisfaction (89.64% vs 81.35%, P < .001), less pain (1.87 vs 4.60, P < .001), and higher return to sport or preinjury activity level, but this was insignificant (81.43% vs 73.83%, P = .082). Partial avulsion repairs had better hamstring strength (86.04% vs 83.71%, P < .001) and endurance (107.13% vs 100.17%, P < .001). Complete repairs had significantly higher complication rates (29.38% vs 11.27%, P = .001).
Conclusion:
Proximal hamstring avulsion repair resulted in superior outcomes as compared with nonoperative treatment, although the complication rate was 23.17%. The nonoperative group was quite small, making a true comparison difficult. Acute repairs have better outcomes than do chronic repairs. Complete avulsion repairs had higher patient satisfaction, less pain, and a higher complication rate than partial avulsion repairs, although partial avulsion repairs had better hamstring strength and endurance. Studies of high methodological quality are lacking in terms of investigating the outcomes of proximal hamstring avulsion repairs.
Posterior thigh injuries are commonly seen in athletes after rapid hip flexion with concurrent knee extension. The degree of injury sustained can vary greatly, ranging from a muscle strain to an avulsion of 1, 2, or all 3 tendinous insertions on the ischial tuberosity. Anatomically, the proximal hamstring originates from the lateral aspect of the ischial tuberosity and is composed of the semimembranosus, semitendinosus, and the long head of the biceps femoris. 20 The semimembranosus has a more lateral origin than the semitendinosus and long head of the biceps femoris, which together make up the conjoint tendon. 20 Furthermore, the initial diagnosis can be made in the acute setting, or it can be delayed, resulting in a chronic presentation. No consensus has been reached to define an acute injury, but it has been characterized most commonly as <4 weeks, ∥ with other studies defining it as <6, 8, or 12 weeks.2,22,25,28,31,33 Given this wide variety of hamstring injuries that a clinician might encounter, it is not surprising that a clear consensus for treatment has yet to be established.
Two recent systematic reviews investigated the outcomes of acute and chronic hamstring injuries. van der Made et al 32 examined 13 studies with 387 operatively treated proximal hamstring avulsions. This study demonstrated that delayed repair of proximal hamstring avulsions was as effective as acute repairs, with little to no difference in strength testing, pain scores, return to sports, and overall patient satisfaction. In contrast, Harris et al 12 reported that acutely repaired injuries had significantly better strength testing, endurance levels, pain scores, return to sports, and overall patient satisfaction as compared with chronic avulsions in their analysis of 18 studies with 300 hamstring injuries. Harris et al 12 also compared operative and nonoperative treatment outcomes of proximal hamstring avulsions, reporting that operative treatment demonstrated significantly better strength testing, endurance levels, and return to sports. This study’s conclusions are significantly limited by both small sample size (14 nonoperative) and lack of confirmation of diagnosis by advanced imaging in the nonoperative group.
In addition to the chronicity of a proximal hamstring avulsion, clinicians often consider the extent of the injury when choosing a treatment approach. Nonoperative management has been proposed for single- or 2-tendon avulsions with <2 cm of retraction, with operative intervention reserved for 3- or 2-tendon avulsions with >2 cm retraction4,8,23 or if symptoms fail to improve after 6 months. However, few data support the efficacy of this treatment algorithm. Neither Harris et al 12 nor van der Made et al 32 compared the surgical outcomes of partial and complete tendon avulsion repairs.
The aim of this study was to undertake a meta-analysis to comprehensively assess the various factors involved in the management of proximal hamstring avulsions confirmed by advanced imaging or intraoperative findings. Specifically, we sought to compare the outcomes of operative versus nonoperative treatment, acute versus chronic repairs (<2 vs ≥2 months), and partial versus complete repairs.
Methods
Search Strategy
A systematic literature search was performed up to July 2016 in PubMed, CINAHL, SPORTdiscus, Cochrane library, EMBASE, and Web of Science. The following keywords were used: “hamstring,” “avulsion,” “rupture,” “semitendinosus,” “semimembranosus,” “biceps femoris,” “femoral biceps,” “proximal,” “origin,” “tendon.” Boolean operators “OR” and “AND” were used to combine synonyms and categories. “ACL,” “PCL,” and “cruciate ligament” terms were excluded.
Eligibility Criteria
Articles were included if they investigated proximal avulsions of the biceps femoris, semimembranosus, semitendinous, or any combination. Included articles must have confirmed the diagnosis intraoperatively or with ultrasound or magnetic resonance imaging. Articles were excluded if they had a mean follow-up <12 months or <5 participants. Exclusions included imaging reviews without outcome data reported, anatomic/histologic studies, surgical technique reports, and animal studies. Articles examining solely avulsion fractures of the ischial tuberosity were excluded.
Study Selection
Three reviewers (J.A.K., J.M.R., N.S.J.) independently reviewed studies returned from the initial database search (Figure 1). The articles were included or excluded per the aforementioned criteria. When the decision could not be reached for any particular article, the article was submitted to a fourth author (B.M.B.) for review and ultimate decision. Throughout the duration of the search, the content of each article as well as the reference list were screened for overlap of patients from other studies.
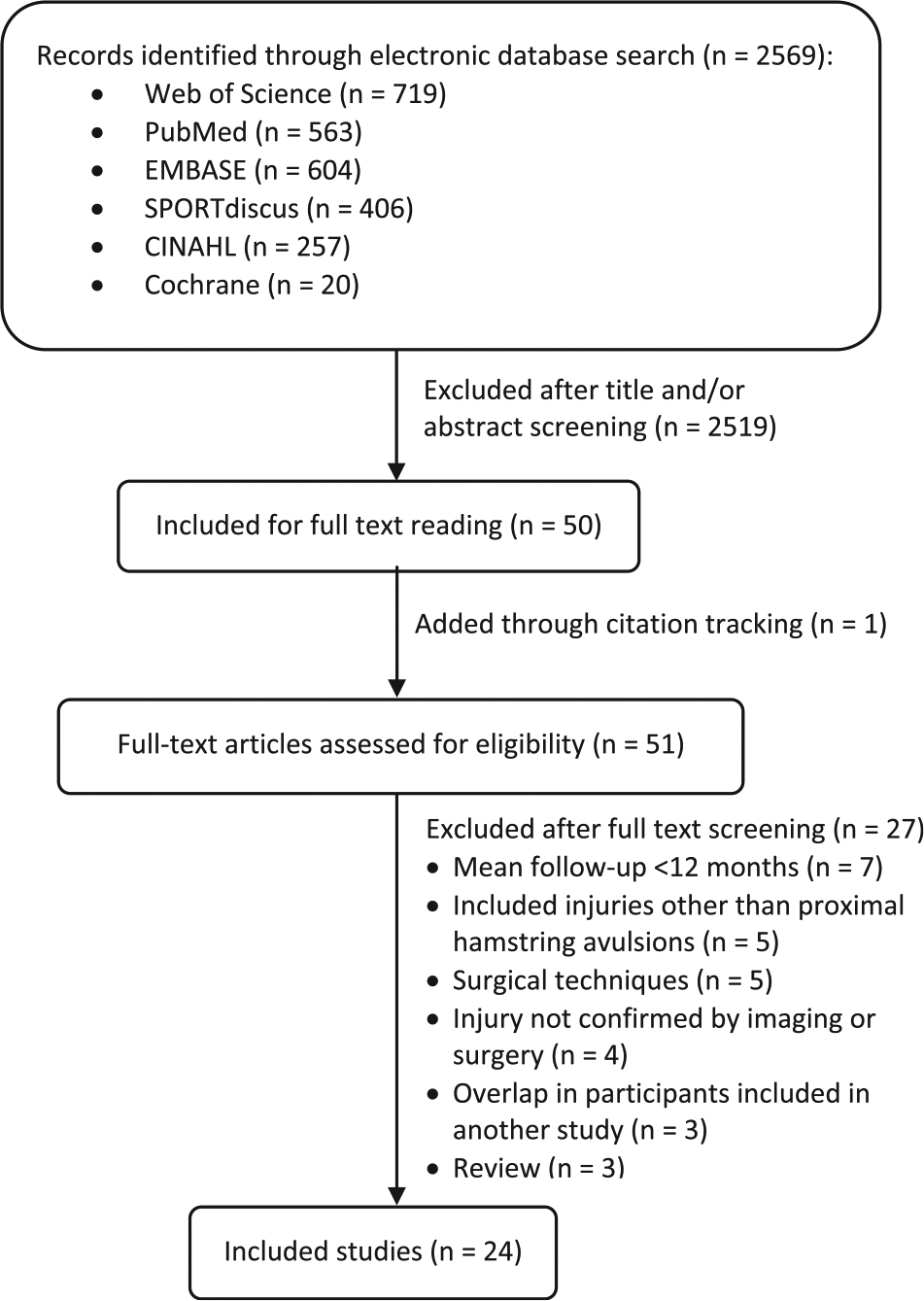
Selection process for included studies.
Data Extraction
Data were extracted by review of each study for number of participants, mean age, mean duration of follow-up, timing of surgery, and surgical outcomes: Lower Extremity Functional Scale (LEFS), single-legged hop, return to sport or preinjury activity, Harris Hip Score, strength, endurance, Tegner score, visual analog scale for pain, Single Assessment Numeric Evaluation (SANE), patient satisfaction, SF-12 (12-Item Short Form Survey), Marx score, UCLA activity scale (University of California, Los Angeles), Proximal Hamstring Injury Questionnaire, and complications (Table 1). Whenever values were recorded at multiple follow-ups for the same outcome, the most recent values were recorded. The data were then grouped into various categories that compared acute repair (<2 months) versus chronic repair (≥2 months), partial repair versus complete repair, acute complete repair versus chronic complete repair, and operative versus nonoperative treatment. Complications were pooled into the following categories: rerupture (including dislocated anchor), reoperation, infection/wound complications (including seroma and hypertrophic scarring), neurological complications (including transient sciatic nerve palsy, sciatica, numbness, and paresthesias), peri-incisional numbness, deep venous thrombosis/pulmonary embolism, and miscellaneous (including new-onset hip pain, hematoma, posterior thigh atrophy, and complex regional pain syndrome).
All Studies Included for Meta-analysis a
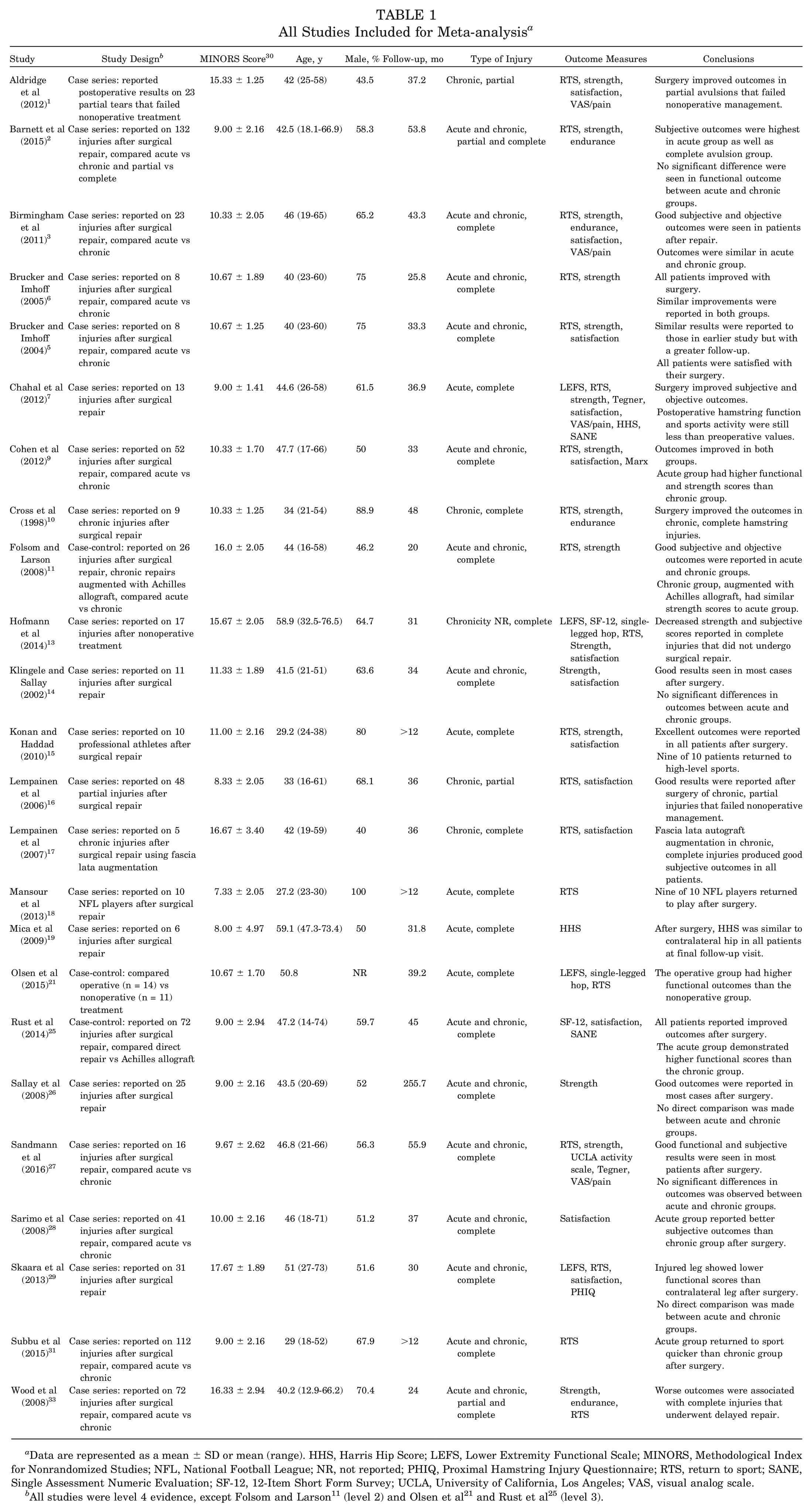
Data are represented as a mean ± SD or mean (range). HHS, Harris Hip Score; LEFS, Lower Extremity Functional Scale; MINORS, Methodological Index for Nonrandomized Studies; NFL, National Football League; NR, not reported; PHIQ, Proximal Hamstring Injury Questionnaire; RTS, return to sport; SANE, Single Assessment Numeric Evaluation; SF-12, 12-Item Short Form Survey; UCLA, University of California, Los Angeles; VAS, visual analog scale.
Quality Assessment
Each article went through a quality assessment by 3 authors (A.J.C., J.M.R., N.S.J.) using criteria from the Methodological Index for Nonrandomized Studies (MINORS), a validated tool to discern the methodological quality of nonrandomized studies. 30 These 3 values were averaged to compose a final score for each study, with higher scores correlating with higher quality studies (Table 1). When validating the MINORS criteria, Slim et al 30 noted that 15 high-quality randomized trials had a mean rating of 23.1. In comparison, the studies included in this meta-analysis scored a mean score of 11.31 (SD, 3.04; range, 7.33-17.67), indicating lower methodological quality.
Best Evidence Synthesis
Each article’s level of evidence was evaluated with the American Academy of Orthopaedic Surgeons’ levels of evidence system. The majority of the articles were of low methodological quality, composed of 1 level 2 study, 11 2 level 3 studies,21,25 and 21 level 4 studies. ¶
Statistical Methods
Point estimates were obtained by pooling estimated means and the corresponding standard deviations across studies. Weighted means and standard deviations were obtained from the studies considered. As an example, if 3 studies had means and standard deviations of 3 ± 2, 5 ± 3, and 8 ± 4 and these 3 studies had respective sample sizes of 4, 5, and 6, point estimates for their weighted means and standard deviations would be obtained by multiplying the means and standard deviations by each respective sample size, pooling the sums, and dividing by the total sample size. This example would yield a weighted mean and standard deviation of 5.67 ± 3.13. Pooled means with associated ranges and standard deviations (when available) are presented in Tables 1 to 7. P values for continuous variables were obtained by Student t tests and categorical variables by Fisher exact tests, and complications were compared through a test of difference in proportions. Significance was set at a P value of .05.
Outcomes for Operatively and Nonoperatively Treated Proximal Hamstring Avulsions a
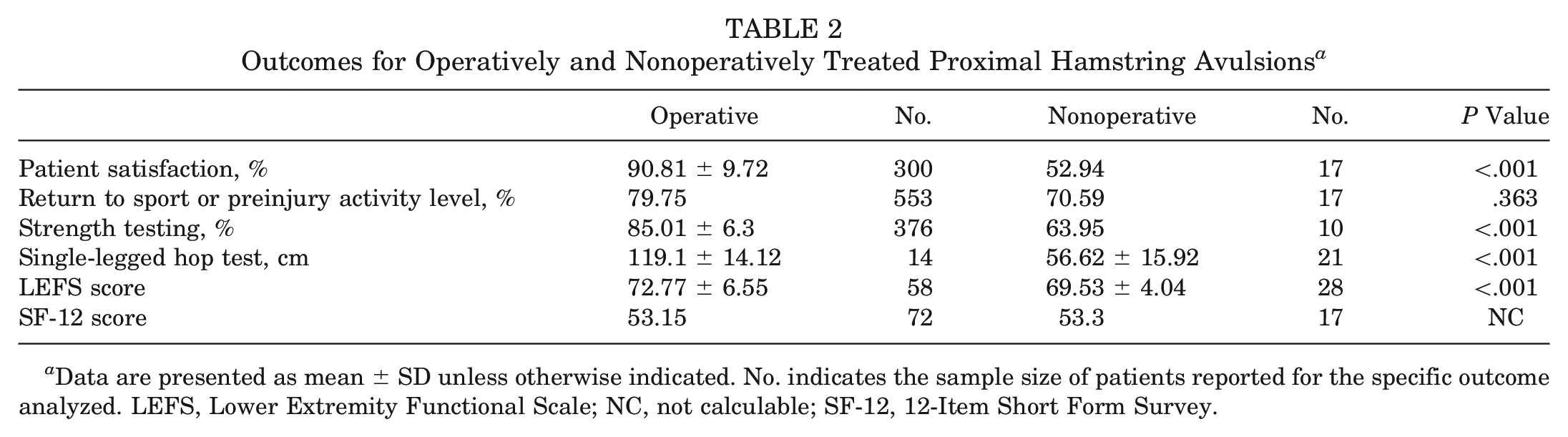
Data are presented as mean ± SD unless otherwise indicated. No. indicates the sample size of patients reported for the specific outcome analyzed. LEFS, Lower Extremity Functional Scale; NC, not calculable; SF-12, 12-Item Short Form Survey.
Complications for Operatively Treated Proximal Hamstring Avulsions a
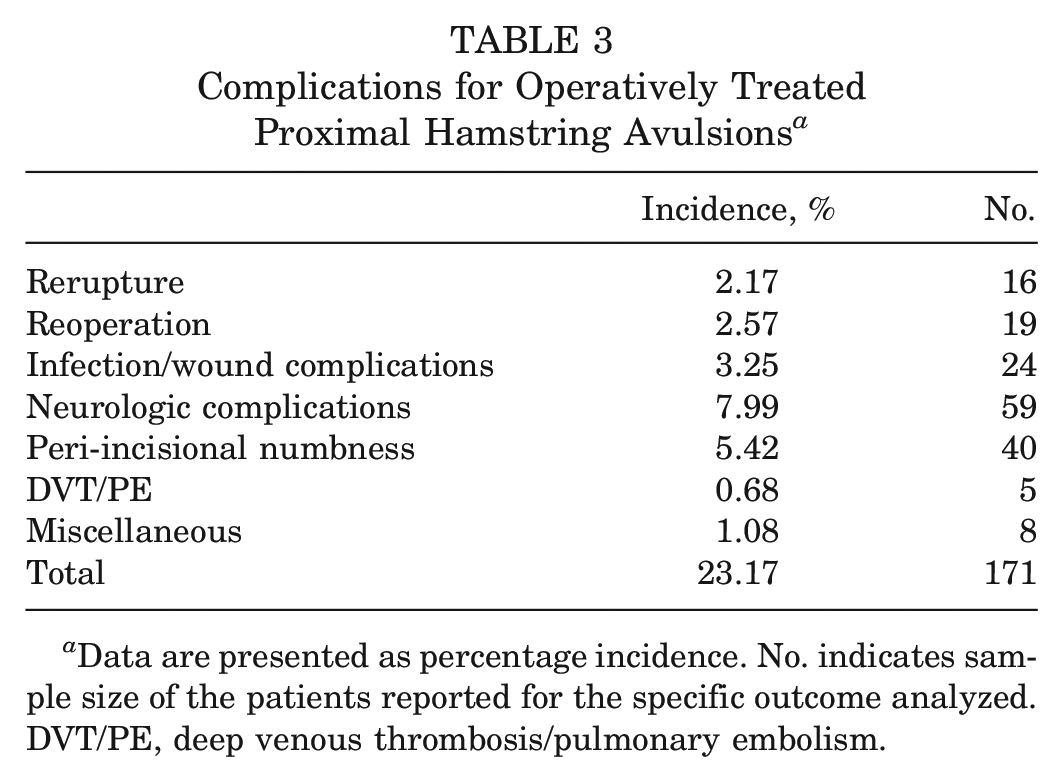
Data are presented as percentage incidence. No. indicates sample size of the patients reported for the specific outcome analyzed. DVT/PE, deep venous thrombosis/pulmonary embolism.
Outcomes for Operatively Treated Acute and Chronic Proximal Hamstring Avulsions a
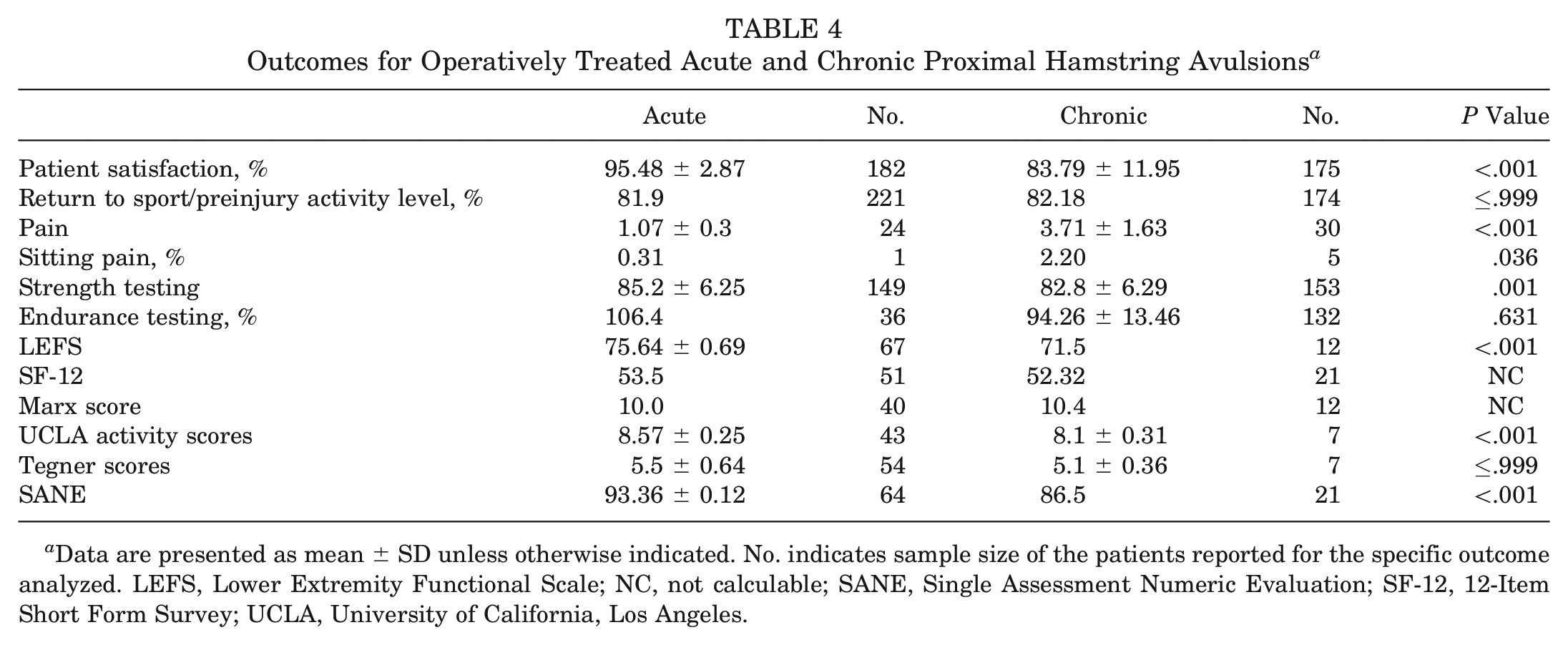
Data are presented as mean ± SD unless otherwise indicated. No. indicates sample size of the patients reported for the specific outcome analyzed. LEFS, Lower Extremity Functional Scale; NC, not calculable; SANE, Single Assessment Numeric Evaluation; SF-12, 12-Item Short Form Survey; UCLA, University of California, Los Angeles.
Complications for Operatively Treated Acute and Chronic Proximal Hamstring Avulsions a
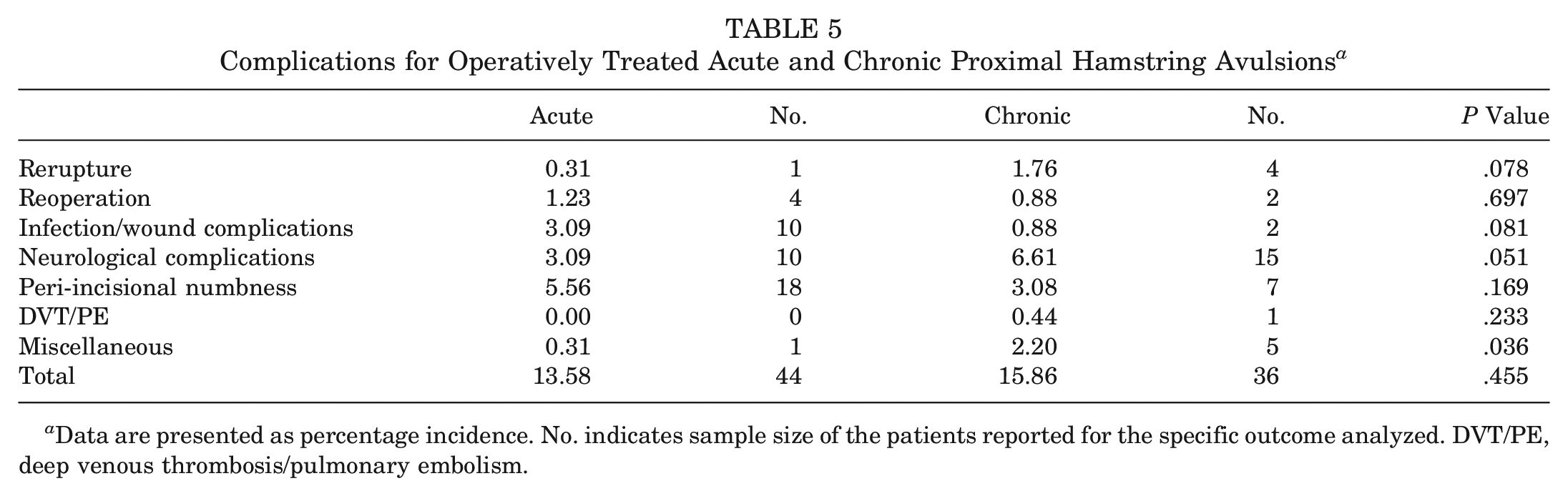
Data are presented as percentage incidence. No. indicates sample size of the patients reported for the specific outcome analyzed. DVT/PE, deep venous thrombosis/pulmonary embolism.
Outcomes for Operatively Treated Partial and Complete Proximal Hamstring Avulsions a
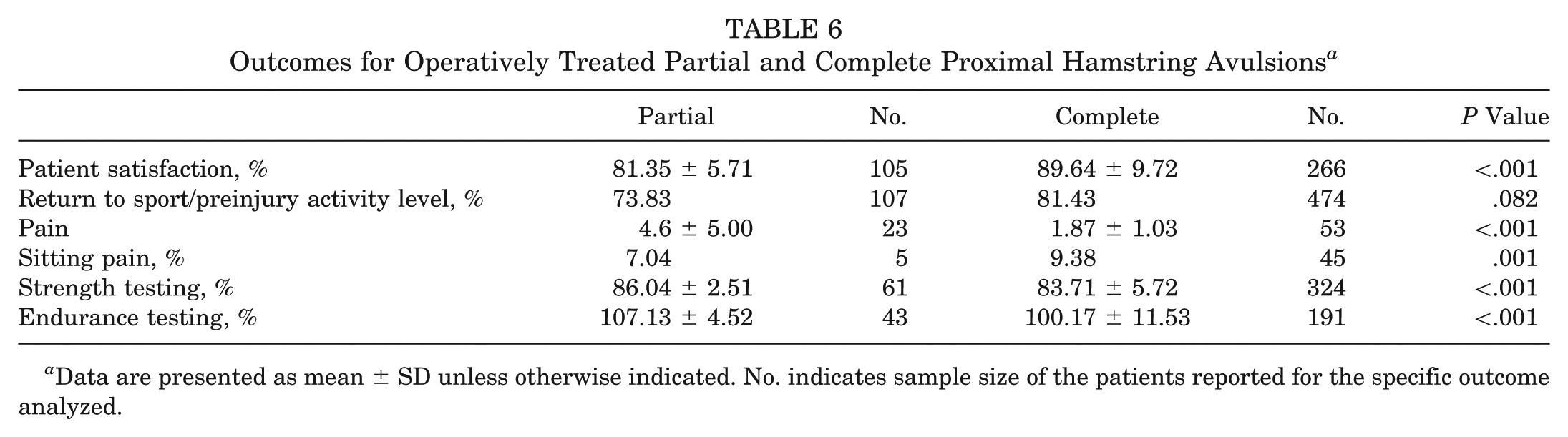
Data are presented as mean ± SD unless otherwise indicated. No. indicates sample size of the patients reported for the specific outcome analyzed.
Complications for Operatively Treated Partial and Complete Proximal Hamstring Avulsions a
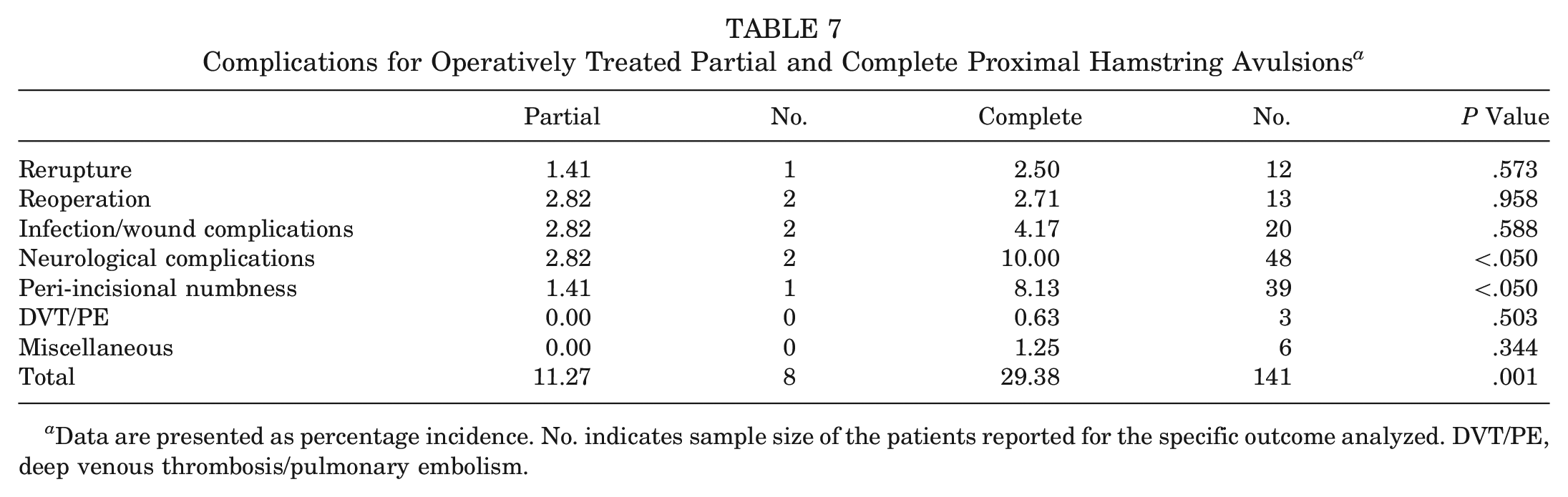
Data are presented as percentage incidence. No. indicates sample size of the patients reported for the specific outcome analyzed. DVT/PE, deep venous thrombosis/pulmonary embolism.
Results
Twenty-four studies # were included, comprising 795 proximal hamstring avulsions (Table 1). Fifteen patients11,25 from 1 study and 8 patients5,6 from another study were duplicates, resulting in a total of 772 separate injuries reported. However, these 23 patients were still included in the data analysis since different outcome measures were reported in the 2 articles in which these patients were presented.
Twenty-two studies included operative management of proximal hamstring avulsions ** ; 1 study reported only nonoperative treatment 13 ; and 1 study consisted of operative and nonoperative groups. 21 There were a total of 767 operatively treated patients, with 7 acute partial avulsions, 375 acute complete avulsions, 107 chronic partial avulsions, and 213 chronic complete avulsions; there were an additional 28 nonoperatively treated complete avulsions. Demographic data were gathered and averaged when available. The operative group consisted of a younger cohort than the nonoperative group, with mean ages of 41.4 and 57.6 years of age, respectively; 61.7% of the operative patients and 64.7% of the nonoperative patients were male. Operative and nonoperative patients were followed up for a mean of 48.4 and 32 months, respectively. The mean time from injury to surgery was 202.3 days for the operative group. Most patients were treated with primary repair. However, a total of 24 chronic complete avulsions were treated with repair augmented with graft; 18 were performed with Achilles allograft in 2 studies11,25; 5 were performed with fascia lata autograft in another study 17 ; and 1 was performed with iliotibial band autograft in a separate study. 28
After repair, 90.81% (SD, 9.72%) of patients were satisfied with their outcome, which was significantly greater (P < .001) than the nonoperative group (52.94%). However, the operative and nonoperative groups reported similar numbers of patients returning to sport, 79.75% and 70.59% (P = .363), respectively; 7.05% of the operative patients reported sitting pain, which was not reported for the nonoperative group. Operative patients had significantly greater strength testing as a percentage of the contralateral leg (85.01% vs 63.95%) and greater single-legged hop distance (119.1 vs 56.62 cm) when compared with the nonoperative group (P < .001). The operative group outscored the nonoperative group on the LEFS (72.77 vs 69.53, P < .001), but SF-12 scores were nearly identical (see Table 2). While no complications were reported in the nonoperative patients, the operative group reported a 23.17% complication incidence, including 2.17% rerupture and 2.57% reoperation rates (Table 3).
Acute avulsions were arbitrarily defined as patients who were operatively treated within 2 months after the injury, while chronic avulsions underwent surgery after 2 months. Two months was used as the cutoff to maximize inclusion while preserving the ability to delineate between acute and chronic repairs, since studies have used varying definitions of acute and chronic. While the majority of the studies defined acute injuries as <1 month, 3 studies2,25,31 chose 6 weeks as their cutoff. Two studies28,33 defined acute injuries as <3 months. Only patient satisfaction and demographic data were extracted from the Sarimo et al 28 study, which included 22 acute injuries treated within 3 months (mean 2.4 months) and 19 chronic injuries treated after 3 months. The Wood et al 33 study had available data within an appendix, which was divided by 2 months from injury to surgery, yielding 72 additional patients with chronic injuries. Thus, by applying 8 weeks as our definition for acute injuries, the patients from these 5 studies (189 acute, 221 chronic) could also be included in our subgroup analysis. The mean time from injury to intervention for the acute and chronic groups was 20 and 374 days, respectively. Therefore, despite our definition of 8 weeks as the cutoff for acute versus chronic injuries, the mean time to surgery of the acute group was still <1 month. The acute group had a mean follow-up time of 43.8 months, as opposed to 50.8 months for the chronic group; the respective mean ages were 39.1 and 39.3 years for acute and chronic groups. The percentage of male patients was also found to be similar between the acute and chronic groups, with means of 67.1% and 68.5%, respectively. Of the 382 acute avulsions, 375 (98.17%) were complete, with the remaining 7 (1.83%) being partial. Of the 320 chronic avulsions, 213 (66.56%) were complete, with the remaining 107 (33.44%) being partial.
Patients in the acute group were found to have significantly (P < .001) higher patient satisfaction (95.48%) and lower pain scores (1.07) in comparison with the chronic group (83.79% and 3.71, respectively). Postoperatively, 0.31% of the acute and 2.20% of the chronic group reported sitting pain, which was significantly different (P = .036). In regard to returning to sport, the acute (81.8%) and chronic (82.18%) groups demonstrated similar results (P ≤ .999). Compared with the chronic group, acutely treated patients reported (Table 4) significantly better results (P < .001) in strength testing versus the contralateral leg (85.2% vs 82.8%) and LEFS (75.64 vs 71.5), UCLA (8.57 vs 8.1), and SANE (93.36 vs 86.5) scores. Similar outcomes were seen in both groups for Marx (10.0 vs 10.4) and Tegner (5.5 vs 5.1) scores (P ≤ .999) and endurance testing (106.4 vs 94.26, P = .631). Complications were reported in 44 of 324 (13.58%) acute cases, as opposed to 36 of 227 (15.86%) chronic cases (P = .455). Rerupture occurred in 4 of 227 (1.76%) chronic cases versus 1 of 324 (0.31%) acute cases (P = .078), and reoperation occurred in 2 of 227 (0.88%) chronic cases versus 4 of 324 (1.23%) acute cases (P = .697) (Table 5).
A partial avulsion was defined as detachment of 1 or 2 hamstring tendons, with the remainder of the musculotendinous complex still intact and connected with its bony insertion. The mean time from injury to intervention for the partial and complete groups was 380 and 139 days, respectively. The partial avulsion group had a mean follow-up time of 40.4 months, as compared with 53 months for the complete avulsion group. The respective mean ages were 38.7 and 41.7 years for partial and complete groups. The percentage of male patients was also found to be similar between the partial and complete groups, with means of 60.1% and 60.5%, respectively. Of the 114 partial avulsions, 107 (93.86%) were chronic, with the remaining 7 (6.14%) being acute. Of the 588 complete avulsions, 375 (63.78%) were acute, with the remaining 213 (36.22%) being chronic.
Complete repairs fared significantly better (P < .001) than partial avulsion repairs in overall patient satisfaction (89.64% vs 81.35%) and pain scores (1.87 vs 4.06). Postoperatively, 7.04% of partial and 9.38% of complete groups reported sitting pain, which was significantly different (P = .001). A greater percentage of patients with complete avulsions (81.43%) returned to sport in comparison with those having partial injuries (73.83%), although this was not statistically significant (P = .082). Patients who underwent partial repair had significantly higher strength testing (86.04% vs 83.71%, P < .001) and endurance scores (107.13 vs 100.17, P < .001) when compared with those having complete repairs (Table 6). The mean reported complication rate was 11.27% for partial repairs and 29.38% for complete repairs, which was significantly different (P = .001). Patients in the complete repair group had significantly higher incidences of neurological complications (10.00% vs 2.82%, P < .050) and peri-incisional numbness (8.13% vs 1.41%, P < .050) (Table 7).
A separate comparison was carried out for acute and chronic complete ruptures because 33.4% and 0.9% of the acute and chronic groups were composed of partial avulsions, respectively, which could have led to skewed results. Acute complete repairs fared significantly better (P = .05) than chronic complete repairs in overall patient satisfaction (95.35% vs 70.67%) and pain scores (1.07 vs 3.71). Postoperatively, 0.31% of patients with acute complete repairs and 2.2% of those with chronic complete repairs reported sitting pain, which was significantly different (P = .036). Patients with acute and chronic complete repairs had similar return-to-sport and preinjury activity levels rates (81.90% vs 81.80%, P = .994). Acute complete repair patients had higher strength testing when compared with chronic complete repairs (88.10% vs 82.80%), but this was not statistically significant (P = .685). Acute complete repairs resulted in higher LEFS, UCLA, and SANE scores than the chronic complete repairs (P < .001) (Table 8). The mean reported complication rates were similar for acute and chronic complete repairs (11.19% vs 12.73%). Chronic complete repairs had a higher rate of rerupture (1.50% vs 0.25%) and neurological complications (4.87% vs 2.49%), while acute complete repairs had a higher rate of infection or wound complications (2.49% vs 0.75%) and peri-incisional numbness (4.48% vs 2.62%). However, no specific complication had statistically significant differences between groups (Table 9).
Outcomes for Operatively Treated Acute and Chronic Complete Proximal Hamstring Avulsions a
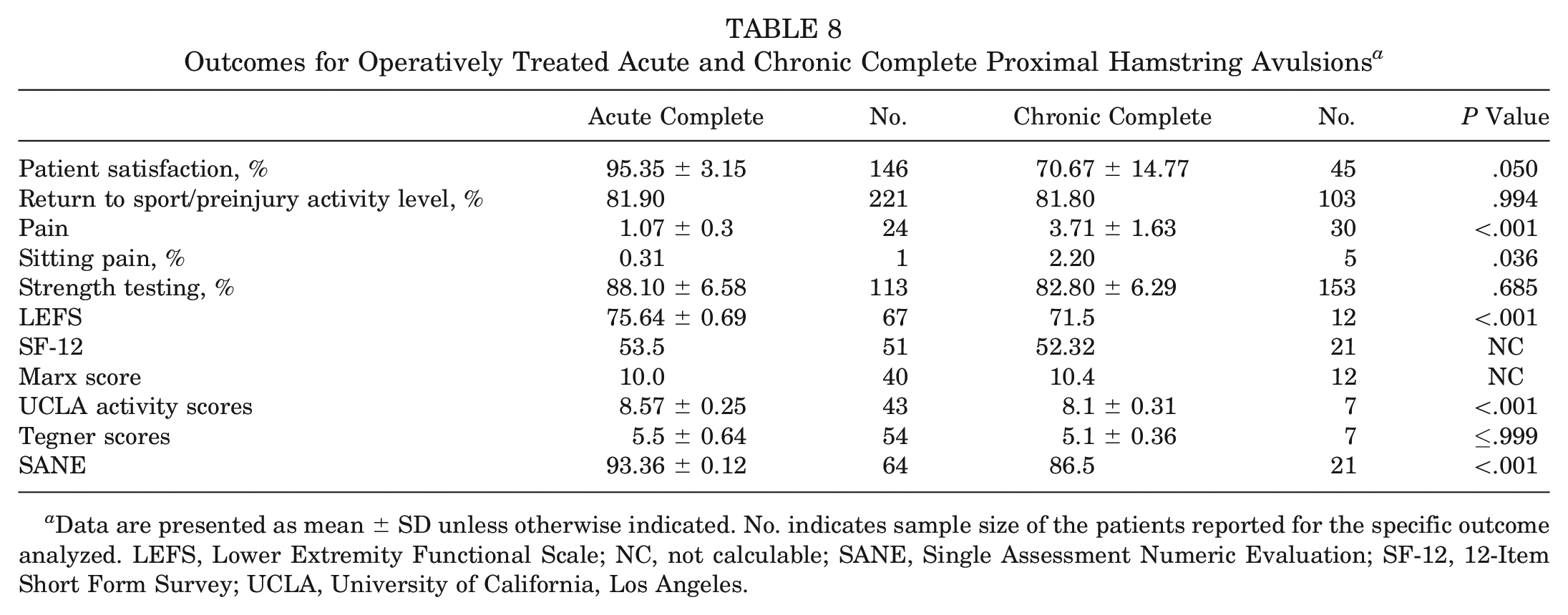
Data are presented as mean ± SD unless otherwise indicated. No. indicates sample size of the patients reported for the specific outcome analyzed. LEFS, Lower Extremity Functional Scale; NC, not calculable; SANE, Single Assessment Numeric Evaluation; SF-12, 12-Item Short Form Survey; UCLA, University of California, Los Angeles.
Complications for Operatively Treated Acute and Chronic Complete Proximal Hamstring Avulsions a
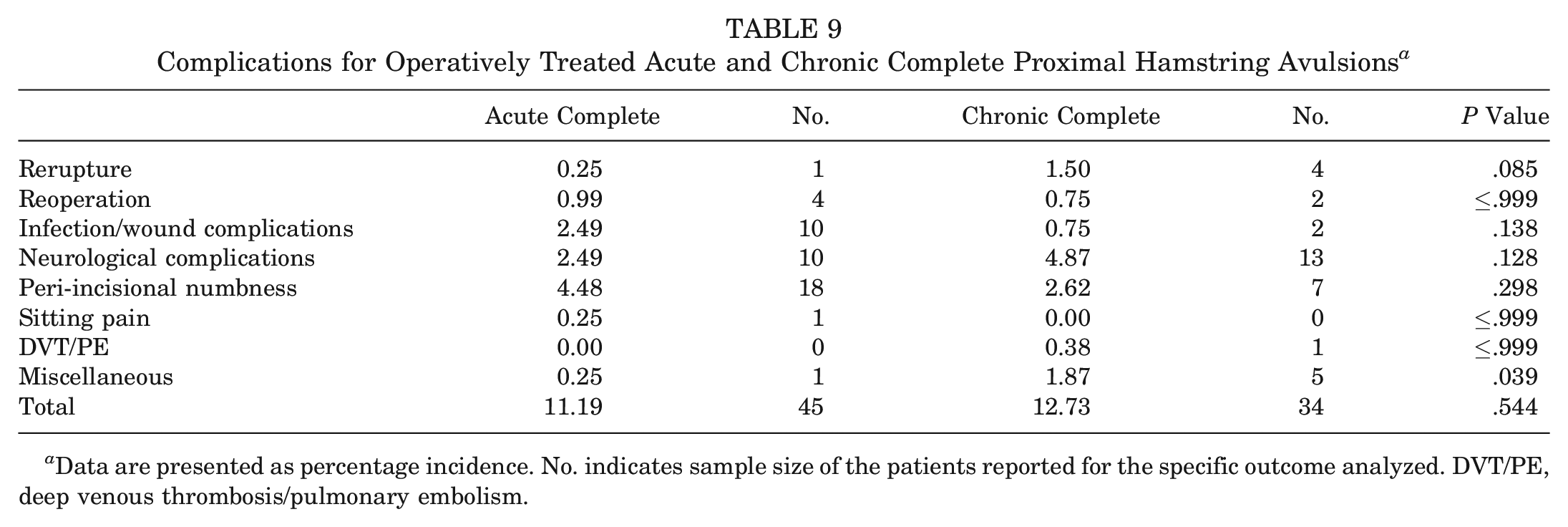
Data are presented as percentage incidence. No. indicates sample size of the patients reported for the specific outcome analyzed. DVT/PE, deep venous thrombosis/pulmonary embolism.
Discussion
This is the most comprehensive study and first meta-analysis to date for the treatment of proximal hamstring avulsions, as well as the only study to compare the outcomes of surgically repaired partial and complete avulsions. With the exception of 1 article, the data reported came from studies of low methodological quality with level 3 or 4 evidence, which was supported by low MINORS scores.
Operative Versus Nonoperative Intervention
Before this study, Harris et al 12 performed a systematic review that compared outcomes of operative and nonoperative management of proximal hamstring avulsions, concluding that operative patients reported significantly (P < .050) better strength testing, endurance levels, and return to sports. However, there were only 14 patients in the nonoperative group, 10 of which came from 1 study 22 that was not included in our review, since the hamstring injury was not confirmed for all patients by magnetic resonance imaging or ultrasound. This review included 2 studies of level 3 and 4 evidence that assessed a total of 28 hamstring injuries treated nonoperatively. Operative patients scored significantly higher than the nonoperative group in most categories, including patient satisfaction, strength testing, single-legged hop test, and LEFS (P < .001). The complication rate was 23.17% in the operative group. A 2017 study by Piposar et al, 23 published after the completion of the literature search for this study, compared operative and nonoperative treatment for partial and complete injuries with <2 cm of retraction after failing nonoperative treatment. There were 15 nonoperative patients and 10 operative patients. Similarly, the study showed significantly greater LEFS scores in the operative group (77 vs 64.3, P = .01). There was also a greater physical component of SF-12 scores in the operative group (55 vs 48, P = .03). Single-legged hop distances for the injured extremity were 128 cm for the operative group and 111 cm for the nonoperative group, but there was no significant difference when injured extremities were compared with uninjured extremities within these groups. Additionally, operative and nonoperative treatment showed no significant difference in strength (P = .70).
Acute Versus Chronic Injuries
Two prior systematic reviews reported conflicting data comparing the outcomes of repaired acute and chronic proximal hamstring avulsions. Harris et al 12 noted that acute injuries had significantly (P < .001) better strength testing, pain scores, return to sports, and overall patient satisfaction, whereas van der Made et al 32 reported little difference between acute and chronic groups in these same outcome measures. van der Made et al attributed this discrepancy to differences in study selection for the review. We found that acutely repaired injuries demonstrated significantly better patient satisfaction (P < .001), visual analog score for pain (P < .001), incidence of sitting pain (P = .036), strength testing (P = .001), LEFS (P < .001), UCLA scores (P < .001), and SANE scores (P < .001). Even with all partial injuries removed from this comparison (ie, acute complete vs chronic complete repairs), these same differences were statistically significant. However, it is debatable whether these statistical differences in outcomes would be clinically significant, which may be reflected in the similar percentages of patients returning to sport for each group. Chronic repairs are technically more demanding than acute repairs owing to the greater amount of scar tissue in the zone of injury and in proximity to the sciatic nerve, making dissection and mobilization quite difficult. These bandlike scars typically are at the lateral border of the semimembranosus, associated with chronic localized pain (ie, “hamstring syndrome”) at the ischial tuberosity with repetitive motions during running or weight training. 24 This, with greater tendon retraction seen in chronic injuries, may relate to increased sitting pain (P = .036), overall complications (P = .455), neurological complications (P = .051), rerupture (P = .078), and miscellaneous complications (P = .036) reported in this group.
Partial Versus Complete Avulsions
No prior review has compared the outcomes of partial and complete avulsions after surgical repair. In this review, 4 studies, all with level 4 evidence, delineated between partial and complete injuries, and 3 of these studies reported separate outcome measures for the partial group. The partial avulsion group demonstrated significantly (P < .001) better scores on strength and endurance testing. However, the complete avulsion group showed greater patient satisfaction (P < .001), likely attributed to its significantly lower reported pain levels (P < .001). Both groups had a relatively high incidence of postoperative sitting pain, with incidence rates of 7.04% and 9.38% for partial and complete avulsions, respectively. Patients with complete repairs did have a higher rate of return to sport or preinjury activity level (81.43% vs 73.83%), but this was statistically insignificant (P = .082). It is worth noting that the partial avulsions were repaired after a mean of 380 days, while the complete injury group underwent surgery much sooner, with a weighted mean of 139 days. Partial avulsions are more frequently chronic and repetitive injuries, as opposed to an isolated traumatic event with complete avulsions. Therefore, the chronicity of these partial injuries may be a confounding factor in this analysis. However, it should be noted that, traditionally, treatment for partial injuries has been nonoperative, and operative intervention has been reserved for patients who fail to improve after 6 months of nonoperative therapy.4,23 Therefore, the chronicity of treatment for the patients included in this meta-analysis matches what has been the mainstay of modern treatment for these injuries. Of the 3 studies that constituted the partial injury group, only 1 study 2 offered a separate group of complete avulsions for direct comparison, which reported significantly (P = .004) higher subjective scores for the complete avulsions but similar return to sports between the groups.
Strengths and Weaknesses
Limitations of this review include the low methodological quality of the majority of studies from which the data were extracted, such as differing surgical techniques, limited long-term follow-up, and lack of randomization or blinding. Also, the diverse outcome categories reported in each study made it difficult to aggregate the results into large groups for data analysis (ie, many studies reported complications but did not specify the chronicity or severity of the associated injury). The assorted patient population, which ranged from professional athletes to regular adults, may be reflective of what a clinician would encounter in practice. However, this heterogeneity of patients could have confounded the results, which may be more accurately assessed in a subgroup analysis for future studies. Lack of clear injury descriptions across studies could have produced discrepancies in the type or extent of hamstring avulsions. Furthermore, the small sample size of the operative partial avulsion (n = 114) and nonoperative (n = 28) groups provided a limited representation of the outcomes seen in these specific patients, especially when compared with the aggregated sample size (n = 795). In particular, the small sample size of the nonoperative group, which represents the aggregated data available in the literature, weakens any comparison between operative and nonoperative groups. With these numbers, our results and conclusions comparing operative and nonoperative outcomes should be regarded as speculative.
The greatest strength of this study is centered on the large aggregated sample size of 795 proximal hamstring avulsions, which is more robust than any previous study. This allowed for a more comprehensive data analysis and reduces the effect of bias from any individual study, allowing for the first meta-analysis of this topic to be performed. Furthermore, this review compiles and analyzes a new pool of data for partial proximal hamstring avulsions, which has yet to be addressed in any previous review. Also, this is the first study of proximal hamstring avulsions to provide a quality assessment of the included studies using a validated tool (MINORS criteria 26 ) designed specifically for nonrandomized trials.
Conclusion
This study demonstrates the paucity of high-quality studies regarding the treatment and outcomes of proximal hamstring avulsions. Our results suggest that operatively treated patients have higher patient satisfaction, return of strength, athletic capacity, and overall functional recovery. Patients undergoing acute repair have higher patient satisfaction, less pain, return of strength, and higher functional scores. Chronic repair was associated with a higher rate of sitting pain and neurological complications. Compared with complete repairs, partial repairs demonstrated better strength and endurance testing and a lower complication rate, but worse patient satisfaction and pain scores.
Footnotes
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the US government.
J.A.K. is a military servicemember. This work was prepared as a part of his official duties. Title 17 USC 105 provides that “copyright protection under this title is not available for any work of the United States Government.” Title 17 USC 101 defines a US government work as a work prepared by a military servicemember or employee of the US government as part of that person’s official duties.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.