
Abstract
Background:
The arthroscopic management of hip dysplasia has been controversial and has historically demonstrated mixed results. Studies on patients with borderline dysplasia, emphasizing the importance of the labrum and capsule as secondary stabilizers, have shown improvement in patient-reported outcomes (PROs).
Purpose/Hypothesis:
The purpose was to assess whether the results of hip arthroscopic surgery with labral preservation and concurrent capsular plication in patients with borderline hip dysplasia have lasting, positive outcomes at a minimum 5-year follow-up. It was hypothesized that with careful patient selection, outcomes would be favorable.
Study Design:
Case series; Level of evidence, 4.
Methods:
Data were prospectively collected and retrospectively reviewed for patients aged <40 years who underwent hip arthroscopic surgery for intra-articular abnormalities. Inclusion criteria included lateral center-edge angle (LCEA) between 18° and 25°, concurrent capsular plication and labral preservation, and minimum 5-year follow-up. Exclusion criteria were severe dysplasia (LCEA ≤18°), Tönnis grade ≥2, pre-existing childhood hip conditions, or prior hip surgery. PRO scores including the modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), and Hip Outcome Score Sport-Specific Subscale (HOS-SSS) and the visual analog scale (VAS) score for pain were collected preoperatively, at 3 months, and annually thereafter. Complications and revisions were recorded.
Results:
Twenty-five hips (24 patients) met the inclusion criteria. Twenty-one hips (19 patients, 84%) were available for follow-up. The mean age at surgery was 22.9 years. The mean preoperative LCEA and Tönnis angle were 21.7° (range, 18° to 24°) and 6.9° (range, –1° to 16°), respectively. The mean follow-up was 68.8 months. The mean mHHS increased from 70.3 to 85.9 (P < .0001), the mean NAHS from 68.3 to 87.3 (P < .0001), and the mean HOS-SSS from 52.1 to 70.8 (P = .0002). The mean VAS score improved from 5.6 to 1.8 (P < .0001). Four hips (19%) required secondary arthroscopic procedures, all of which resulted in improved PRO scores at latest follow-up. No patient required conversion to total hip arthroplasty.
Conclusion:
While periacetabular osteotomy remains the standard for treating true acetabular dysplasia, hip arthroscopy may provide a safe and durable means of managing intra-articular abnormalities in the setting of borderline acetabular dysplasia at midterm follow-up. These procedures should be performed by surgeons with expertise in advanced arthroscopic techniques, using strict patient selection criteria, with emphasis on labral preservation and capsular plication.
Keywords
Hip dysplasia is known to be a significant contributor to the development of hip osteoarthritis. 31 This is thought to occur because of overloading and damage to the labrum, edge loading of the acetabulum, and subsequent degeneration of articular cartilage.43,44 Recent studies on patients with mild acetabular undercoverage, termed borderline dysplasia, have defined it as those with a lateral center-edge angle (LCEA) between 18° and 25°.4,11,25,27 In these patients, it is thought that the soft tissues of the hip, including the labrum and capsule, contribute significantly to joint stability.21,33 Left untreated, patients may develop microinstability, leading to failure of the chondrolabral complex. 22 Periacetabular osteotomy (PAO) is considered to be the gold standard and has been shown to improve long-term outcomes in patients with true acetabular dysplasia (LCEA ≤18°),27,40 especially when combined with hip arthroscopic surgery.8,24 Because of the morbidity associated with PAO, including significant blood loss, maximum invasiveness, prolonged operative and recovery times, and possibility of major complications, surgeons who perform open hip preservation may be reluctant to perform this procedure in patients with minor degrees of hip dysplasia. 45
On the other hand, because of a potentially higher reoperation rate secondary to persistent instability, hip arthroscopic surgeons are sometimes hesitant to provide arthroscopic treatment to patients with borderline dysplasia. 23 Indeed, some authors have abandoned hip arthroscopic surgery in the setting of hip dysplasia because of the possibility of iatrogenic instability and accelerated arthritis.23,29,35 However, the senior author (B.G.D.) and others have demonstrated that by preserving the labrum and addressing capsular restraints, arthroscopic management can be a viable treatment option for a select group of patients with minimal acetabular deficiency.11,25,34 The senior author previously reported significant improvement in patient-reported outcomes (PROs), as well as the maintenance of outcomes, at a minimum 2-year follow-up in patients with borderline acetabular dysplasia who underwent hip arthroscopic surgery for intra-articular abnormalities when preservation of the labrum and capsular plication were also performed.11,25 The present study aimed to assess whether the results of hip arthroscopic surgery with labral preservation and concurrent capsular plication in patients with borderline hip dysplasia had lasting, positive outcomes at a minimum 5-year follow-up.
Methods
Patient Characteristics
Between February 2008 and December 2010, data were prospectively collected and retrospectively reviewed for all patients who underwent arthroscopic surgery of the hip for the treatment of intra-articular abnormalities. Patients <40 years of age at the time of surgery who had borderline dysplasia, defined as an LCEA between 18° and 25°; had a minimum 5-year follow-up; and underwent concurrent labral preservation and capsular plication met the inclusion criteria for this study. This included all of the patients from a previously published study with a minimum 2-year follow-up. 11 The exclusion criteria were age ≥40 years, Perthes disease, slipped capital femoral epiphysis, inflammatory arthritis, osteoarthritis (Tönnis grade ≥2), or avascular necrosis. We have limited our study cohort to this age group because the results of hip arthroscopic surgery in patients aged >40 years have been found to be more variable. 18 All patients underwent hip arthroscopic surgery by the senior author. This study was conducted at the American Hip Institute and was approved by an institutional review board (No. 5726).
Radiographic Evaluation
All patients had standardized preoperative and postoperative radiographs. These included an anteroposterior pelvis radiographs in the supine and standing positions, which were used to measure the LCEA, Tönnis angle, joint space, presence of an acetabular crossover sign, and presence of a prominent ischial spine sign. A 45° Dunn view was used to measure the alpha angle, and a false-profile view was used to measure the anterior center-edge angle. A cam deformity was defined as an alpha angle >50° on the modified Dunn view. All patients underwent an evaluation with magnetic resonance arthrography to confirm the presence of labral and chondral damage. Cartilage integrity (ie, degree of degenerative change) in this analysis was assessed prospectively and based solely on radiographic criteria and not on intraoperative findings.
Surgical Technique
Surgical treatment involving labral preservation and capsular plication was performed using the technique previously described by Domb et al 11 (Figure 1). The patient was placed in a modified supine position on a traction table with a well-padded perineal post. Access to the joint was achieved through a standard anterolateral portal. Midanterior and distal lateral accessory portals were established under direct visualization for routine joint inspection as well as to facilitate instrument access and the performance of intra-articular procedures. Capsulotomy was undertaken using a Beaver blade, parallel to the labrum, connecting the anterior and anterolateral portals and extending medially as needed to address all intra-articular abnormalities. A routine evaluation of the joint was then undertaken. The labrum was evaluated and, if torn, graded according to Seldes et al. 38 Acetabular cartilage was evaluated and graded using the acetabular labrum articular disruption (ALAD) classification. 5 The size of the acetabular labrum was recorded in 4 quadrants (anterosuperior, anteroinferior, posterosuperior, and posteroinferior) according to the clockface. The ligamentum teres was evaluated according to Gray and Villar 16 and Botser et al. 3
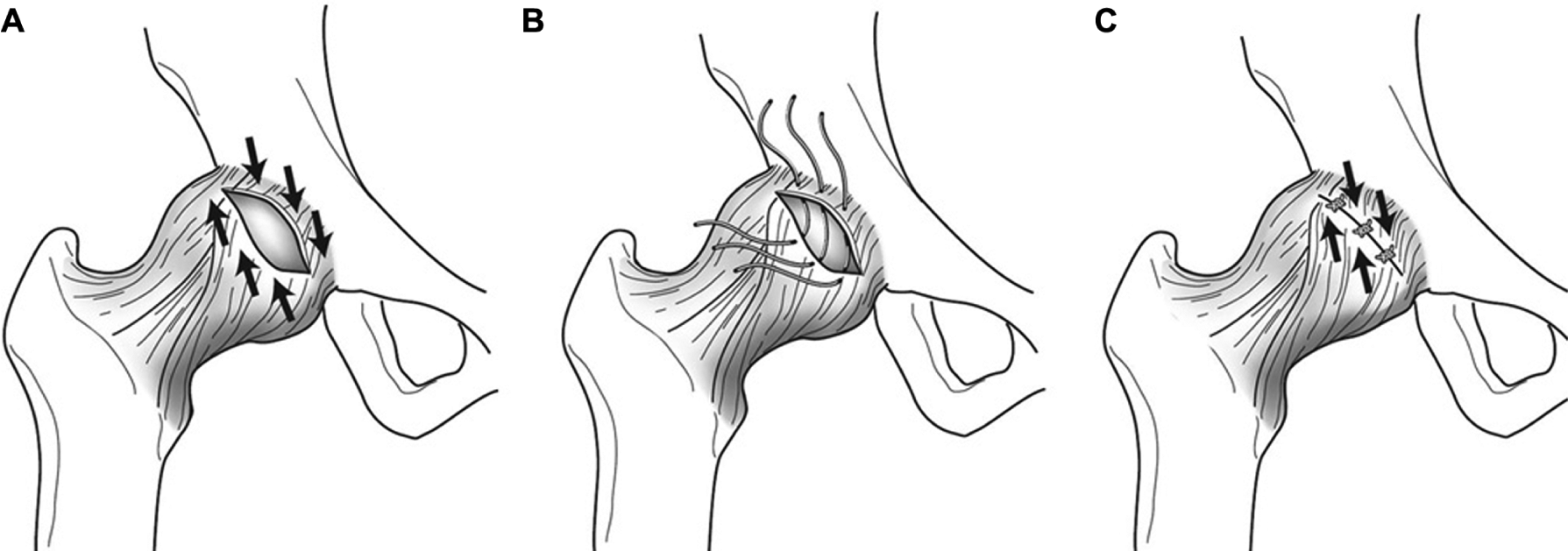
Capsular shift/plication. (A) The goal of arthroscopic capsular plication at the end of hip arthroscopic surgery is to proximally shift the inferior capsule. (B) Sutures are placed on the inferior side of the capsulotomy site and crossed obliquely. (C) Tying the sutures leads to capsular shift. (Reprinted with permission from Domb BG, Philippon MJ, Giordano BD. Arthroscopic capsulotomy, capsular repair, and capsular plication of the hip: relation to atraumatic instability. Arthroscopy. 2013;29(1):162-173. © Benjamin G. Domb, MD.)
During labral repair, capsular elevation from the labrum was performed with electrocautery to preserve enough capsular tissue for later repair. Minimal decortication of the acetabular rim using a round bur was undertaken to improve the biology for labral healing, while taking care not to further decrease bony coverage. Labral repair was achieved with suture anchors via a labral base refixation technique or circumferential suture technique based on labral thickness and the quality of tissue. 15 Additional necessary procedures in the central compartment of the hip were performed. Traction was then released and the hip flexed approximately 45° to evaluate the peripheral compartment. Femoroplasty was performed if a cam deformity was present. Capsular plication was then undertaken with bioabsorbable sutures (Figure 2). With the use of an arthroscopic penetrating device, sutures were placed sequentially, first through the acetabular side of the capsule and then inferomedially on the femoral side of the capsule, in an oblique orientation so as to effect a 1- to 2-cm shift of the iliofemoral ligament (Figures 1 and 2). Larger bites of the capsule effect a greater change. This was repeated to place 4 to 6 sutures. The limb was then gradually brought into extension while viewed arthroscopically to ensure that no separation of the repair construct occurred. Patients were prescribed an X-Act ROM brace (DJO Global) and used crutches with touch-toe weightbearing for 2 weeks. Physical therapy was begun as early as postoperative day 1 to begin passive range of motion with either continuous passive motion or a stationary bicycle. Range of motion was restricted for 6 weeks, including the limitation of extension to 0° and external rotation to 30° at 90° of flexion and 20° at neutral (prone).
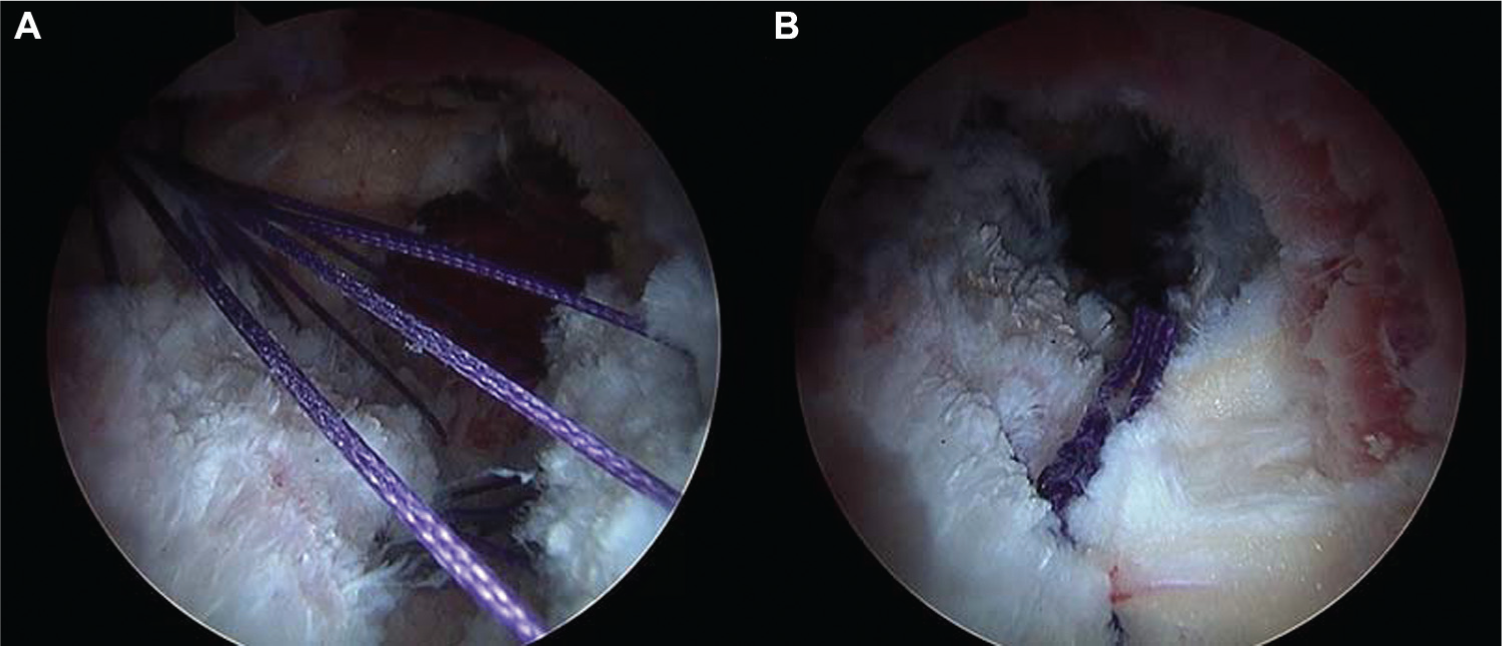
Intraoperative view of arthroscopic capsular plication/shift. (A) Sutures are passed through the inferior side of the capsulotomy site in an oblique orientation. (B) The sutures are tied to produce proximal capsular shift. The hip is brought into extension to ensure that no separation of the repair construct occurs.
Outcome Scores
Patients were prospectively assessed preoperatively and postoperatively using the modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), and Hip Outcome Score Sport-Specific Subscale (HOS-SSS) at 3 months, 12 months, and annually thereafter. Pain was documented on the visual analog scale (VAS) (0, no pain; 10, extreme pain). The reasons for and time to revision arthroscopic surgery were documented. Patient satisfaction with surgery was documented (0, not satisfied at all; 10, completely satisfied). PRO, VAS, and satisfaction scores were collected at clinic appointments, via telephone calls, or via encrypted emails. Complications that occurred after surgery were recorded.
Statistical Analysis
The threshold for statistical significance was set to .05. The Shapiro-Wilk test was performed to determine normal distributions in data. Parametric comparisons of continuous data were performed using the 2-tailed Student t test. The Wilcoxon signed-rank test was performed for nonparametric comparisons. The chi-square and Fisher exact tests were used to identify risk factors for undergoing revision arthroscopic surgery. Statistical analyses were performed using Excel (Microsoft).
Results
Patient Characteristics
There were 631 hip arthroscopic procedures performed between February 2008 and December 2010; 308 cases were excluded because of age ≥40 years, 56 cases were excluded for previous hip conditions and surgeries, 136 cases did not include concomitant capsular plication and labral preservation, 105 cases were excluded because of an LCEA ≥25° or LCEA ≤18°, and 1 case was excluded because of Tönnis grade ≥2.
This left a total of 25 hips (24 patients) eligible for inclusion, and 21 hips (19 patients, 84%) had a minimum 5-year follow-up. Characteristics are presented in Table 1.
Characteristics a
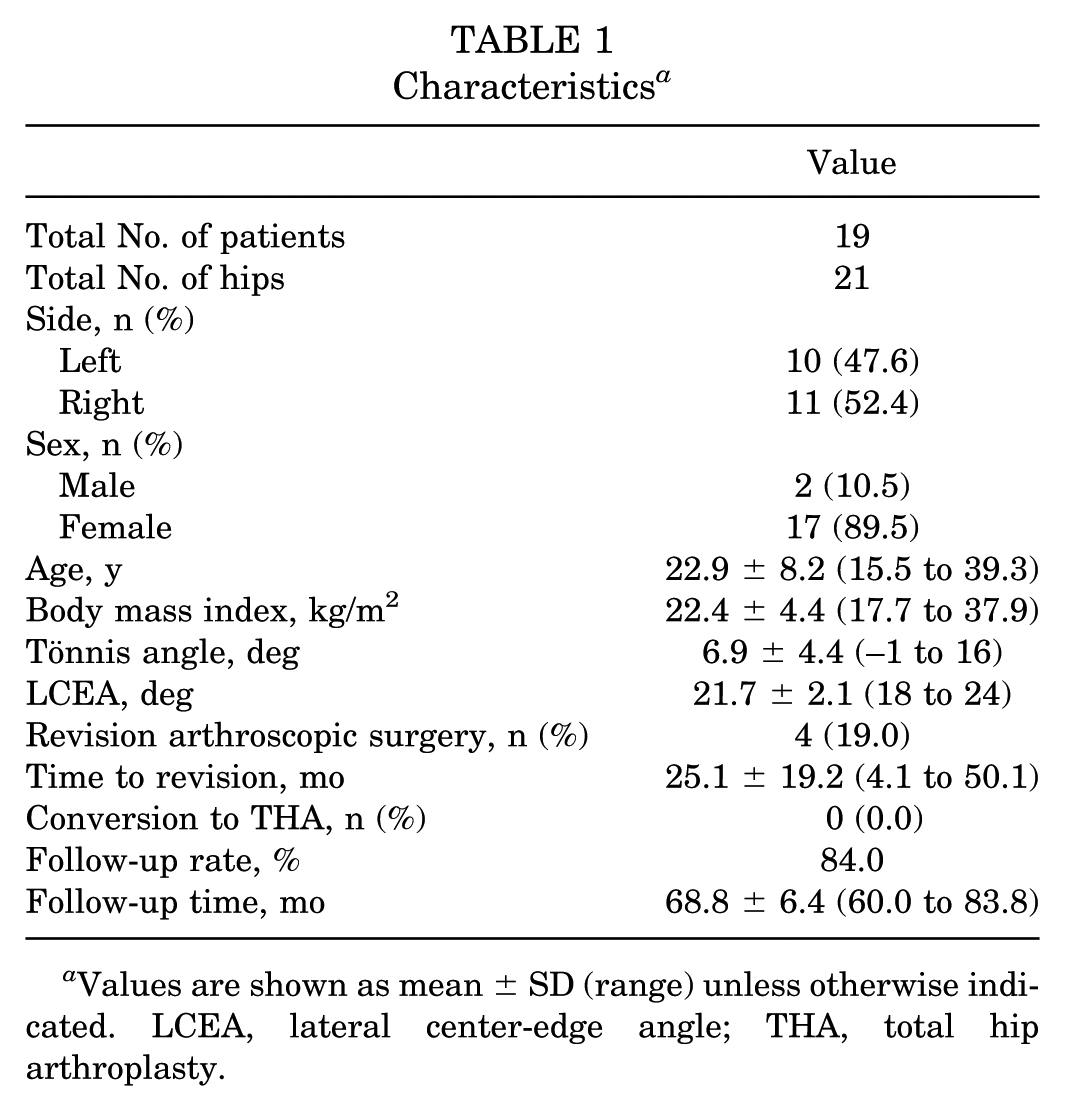
Values are shown as mean ± SD (range) unless otherwise indicated. LCEA, lateral center-edge angle; THA, total hip arthroplasty.
Intraoperative Findings
All hips had a labral tear. Ninety-five percent of the hips were noted to have damage to acetabular cartilage. There were no Outerbridge grade 4 acetabular chondral injuries. One hip (4.8%) had an Outerbridge grade 4 chondral lesion of the femoral head. There were 13 (61.9%) hips with a partial ligamentum teres tear and 1 (4.8%) with a complete ligamentum teres tear. Findings at arthroscopic surgery are documented in Table 2.
Intraoperative Findings a
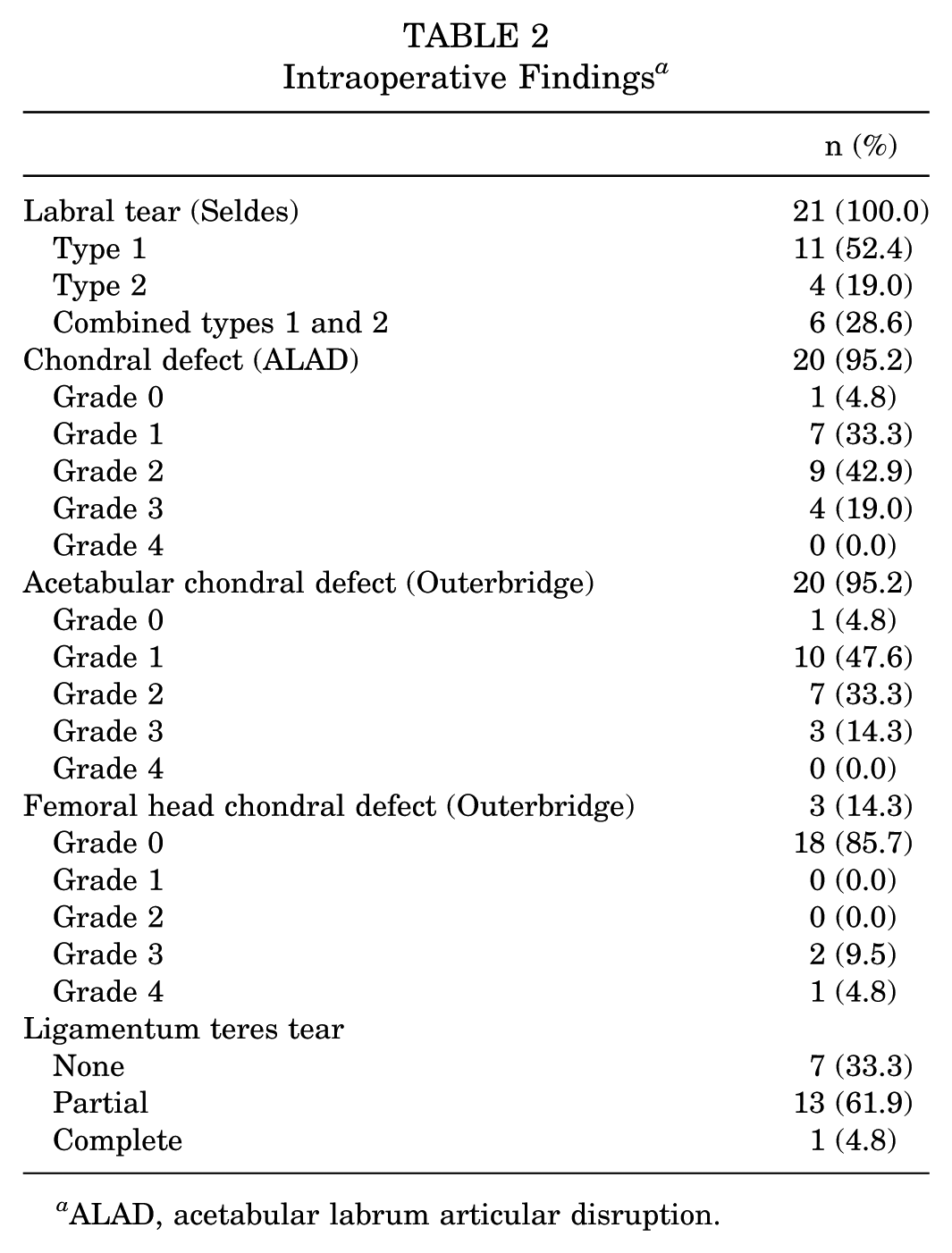
ALAD, acetabular labrum articular disruption.
Arthroscopic Procedures
All patients underwent capsular plication. Twenty (95.2%) hips underwent labral repair, and 1 (4.8%) underwent selective debridement. Eighteen (85.7%) hips underwent minimal rim decortication only. Twelve (57.1%) hips underwent debridement of the ligamentum teres. Iliopsoas fractional lengthening was performed in 11 (52.4%) hips for painful internal snapping. Eleven (52.4%) hips underwent femoroplasty, and 6 (28.6%) underwent limited acetabular chondroplasty. No patients underwent acetabular or femoral head microfracture, and 2 hips (9.5%) underwent loose body removal. One hip underwent arthroscopic trochanteric bursectomy for recalcitrant trochanteric symptoms.
Patient-Reported Outcomes
PRO scores are listed in Table 3. Regarding the trend in PROs over time, there was steady improvement in all scores until 2 years postoperatively; thereafter, there was a slight diminishment in scores, with the HOS-SSS approaching significance (Figure 3).
Patient-Reported Outcome, VAS, and Satisfaction Scores a
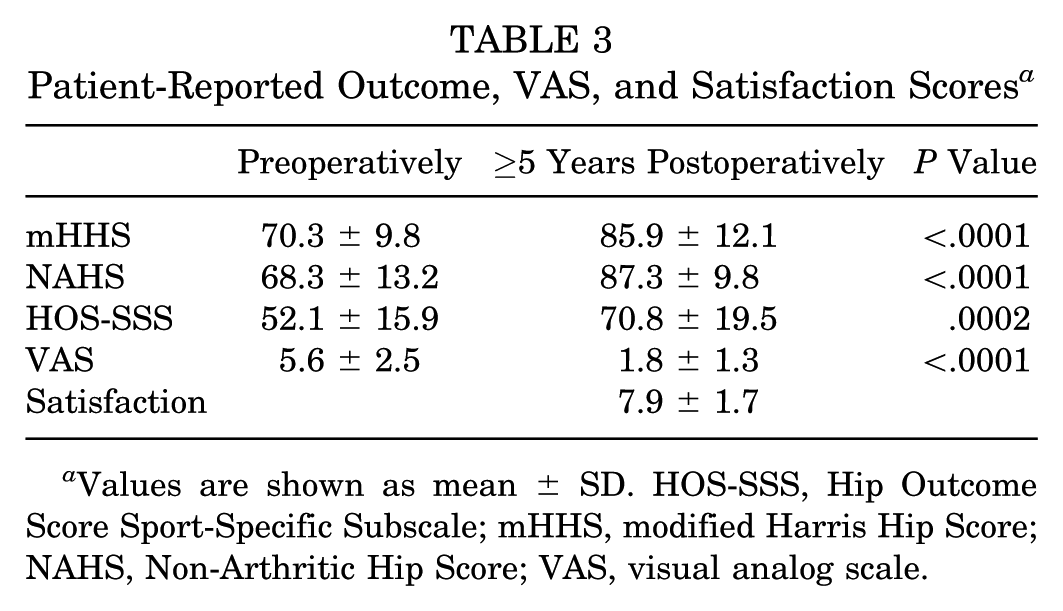
Values are shown as mean ± SD. HOS-SSS, Hip Outcome Score Sport-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; VAS, visual analog scale.
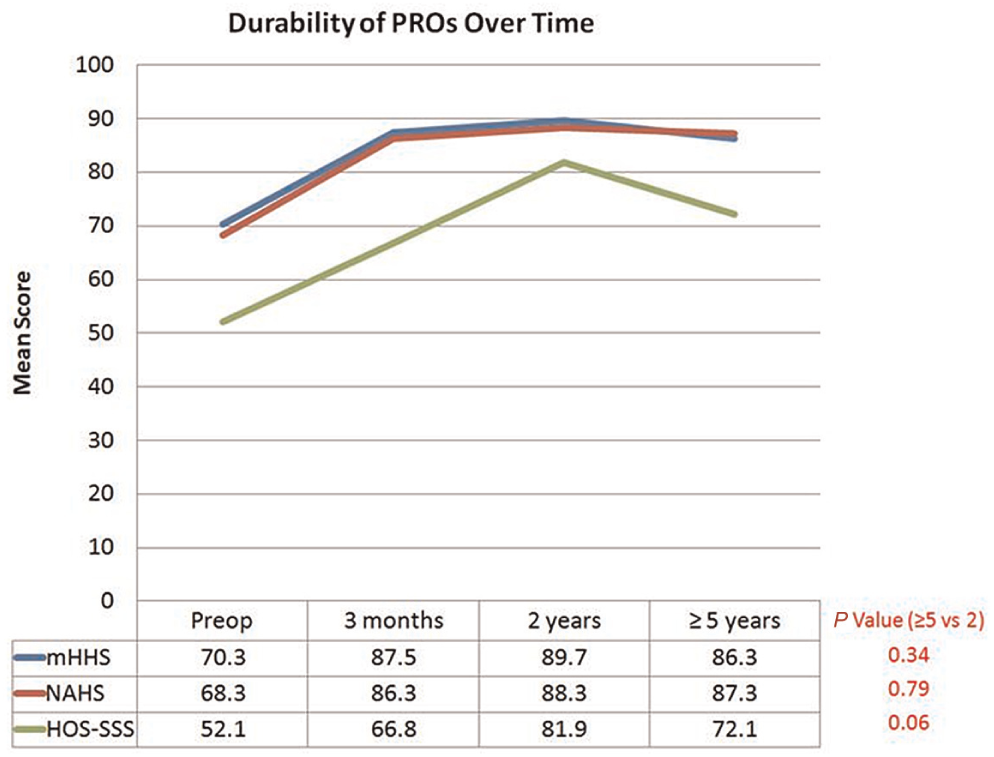
Durability of patient-reported outcomes (PROs) over time for all patients with PRO scores at the preoperative, 3-month, 2-year, and minimum 5-year time points. Drop-offs in scores were not significant. HOS-SSS, Hip Outcome Score Sport-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score.
Secondary Surgery and Complications
Four hips (19.0%) required revision hip arthroscopic surgery (Table 4). The mean time to revision surgery was 25 months (range, 4.1-50.1 months). Two hips underwent loose body removal, one of which was heterotopic ossification measuring >5 mm and the other consisting of residual suture material related to a rupture from previous capsular plication. All patients were noted to have improvements in their PROs at a mean of 42.3 months after revision. One hip (4.8%) had a minor wound infection that resolved with oral antibiotics. One hip (4.8%) had persistent anterolateral thigh numbness. No other complications were noted.
Indications for Patients Requiring Revision Arthroscopic Surgery a
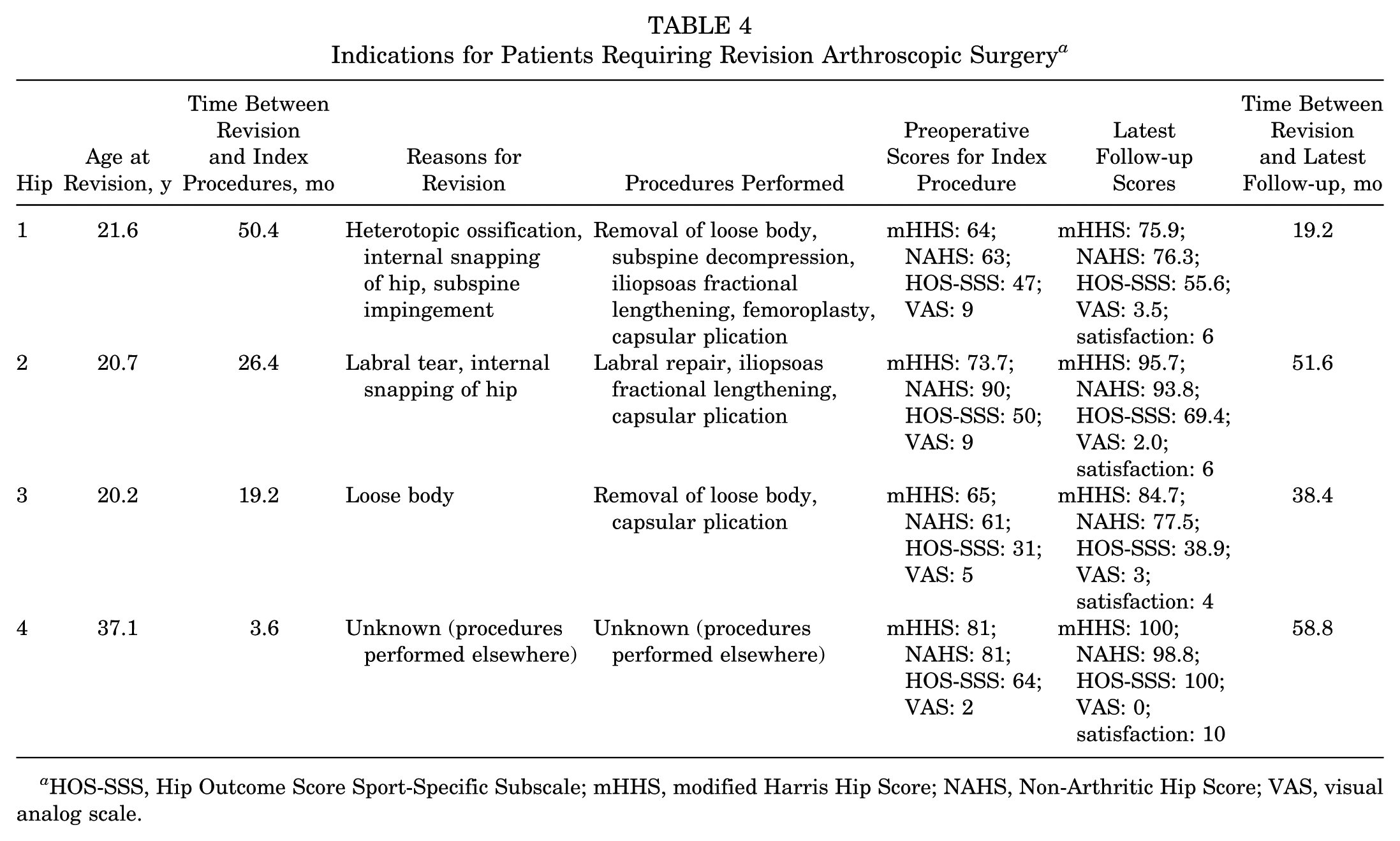
HOS-SSS, Hip Outcome Score Sport-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; VAS, visual analog scale.
To analyze the risk factors for requiring revision, the 4 hips that required revision were compared with the 17 that did not (Table 5). No significant differences were found regarding demographics, intraoperative findings, procedures, or preoperative outcome scores. A trend of higher body mass index and higher preoperative VAS score was observed in the revision group.
Risk Factors for Requiring Revision Arthroscopic Surgery a
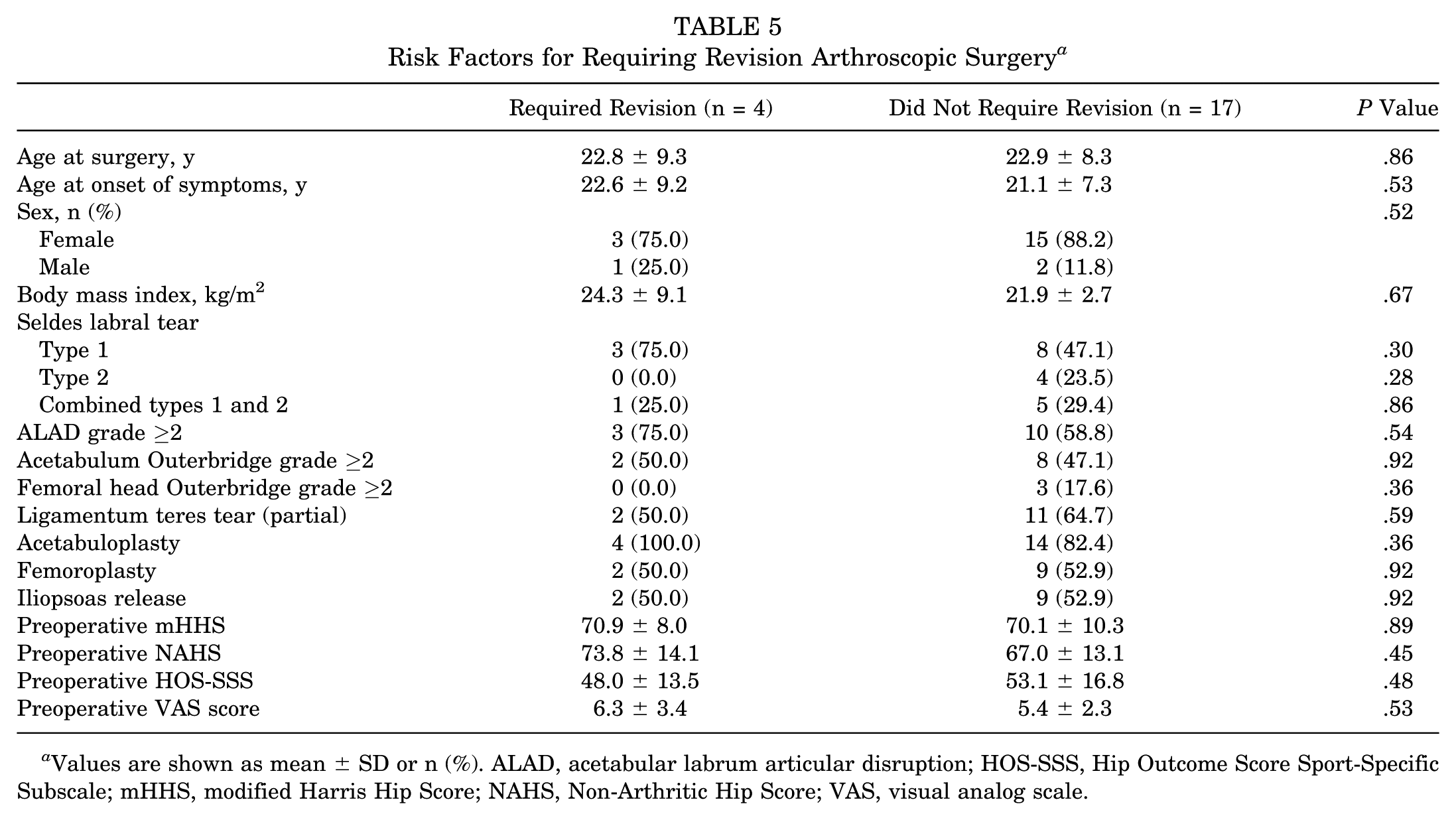
Values are shown as mean ± SD or n (%). ALAD, acetabular labrum articular disruption; HOS-SSS, Hip Outcome Score Sport-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; VAS, visual analog scale.
Discussion
Our study demonstrates that patients with borderline acetabular dysplasia who undergo hip arthroscopic surgery for intra-articular abnormalities with labral preservation and concurrent capsular plication have consistent improvement in outcome scores that are maintained at a minimum 5-year follow-up. To our knowledge, this is among the longest follow-up studies for patients undergoing hip arthroscopic surgery in the setting of borderline dysplasia who have undergone concomitant capsular plication and labral preservation.
The normal hip joint is inherently stable primarily because of the bony anatomy. 6 However, recent studies have highlighted the role of the capsule and labrum as significant contributors to hip stability. 33 Natural history studies have shown that patients with true acetabular dysplasia are predisposed to developing early coxarthrosis. 31 Open procedures such as PAO reliably improve the outcomes of treatment for these patients, have good results over long-term follow-up, and are considered the gold standard in treating patients with true acetabular dysplasia. 40 However, they can be associated with significant morbidity such as extended operative times, increased blood loss, prolonged rehabilitation, fractures, and possibility of inducing femoroacetabular impingement (FAI).1,19,26,41 There is also the potential for major complications such as sciatic nerve palsy and inaccurate or loss of fragment orientation.42,45 Hip arthroscopic surgery as a primary modality in treating patients with hip dysplasia is controversial because of the concern that despite addressing the intra-articular abnormalities, it may not adequately correct the underlying bony abnormalities. 36 Furthermore, there are reports of catastrophic failure after hip arthroscopic surgery in patients with dysplasia, including iatrogenic anterior dislocation and progression of degenerative changes.2,30 Parvizi et al 35 cautioned against the use of hip arthroscopic surgery in patients with hip dysplasia because they showed in their study that 39% of patients had evidence of accelerated arthritis and 36% of patients had femoral head migration. However, all patients in their cohort were noted to have an LCEA <20° and underwent labral debridement, and no mention was made of capsular management.
Multiple cadaveric models have elucidated the role of the labrum and hip capsule as important stabilizers of the hip joint, particularly in the setting of mild acetabular undercoverage.17,21,33 Because of anterosuperior and superolateral bony deficiencies in dysplastic hips, there is increasing recruitment of the soft tissues, including the capsule and labrum. 39 This can lead to chondrolabral overloading and subsequent injuries. 37 The concept of microinstability has led to the development of soft tissue procedures stressing the importance of addressing the secondary stabilizers of the hip, including the capsule and labrum.9,22
Recent studies with a short-term follow-up specifically focusing on patients with very mild bony undercoverage (borderline dysplasia) who underwent hip arthroscopic surgery for intra-articular abnormalities have shown favorable outcomes with arthroscopic surgery when management of the soft tissue factors was emphasized. Nawabi et al 34 compared the outcomes of 46 arthroscopically treated patients with FAI and borderline dysplasia to a matched cohort of 131 patients without dysplasia and showed similar improvement in multiple PROs (mHHS, Hip Outcome Score Activities of Daily Living [HOS-ADL], HOS-SSS, and international Hip Outcome Tool–33 [iHOT-33]) at a mean follow-up of 31.3 months.
Larson et al 25 found improvement in the mHHS in an age-matched cohort of patients with hip dysplasia undergoing hip arthroscopic surgery for a variety of intra-articular disorders compared with those with FAI. Specifically, there were 73% good to excellent results (mHHS >80) in the dysplastic group as compared with 81.2% in the FAI group and failure of 18% as compared with 10%, respectively, when labral repair and capsular plication were added for patients with dysplasia. Failure was defined as an mHHS ≤70 or the eventual need for a pelvic procedure or total hip arthroplasty (THA). Grade 4 chondral lesions were predictive of poor outcomes, and there were no other statistically significant differences noted for outcomes regarding sex, age, or radiographic parameters. There were no iatrogenic subluxations/dislocations. 25 In our study, 16 of the 21 hips (76.2%) had an mHHS ≥80, 2 (9.5%) had scores between 70 and 80, and 3 (14.3%) had an mHHS ≤70.
Domb et al 11 reviewed the outcomes of 22 patients with borderline hip dysplasia who underwent arthroscopic surgery for symptomatic intra-articular hip abnormalities with concurrent labral preservation and capsular plication. They showed significant improvement in 3 PROs (mHHS, NAHS, HOS-SSS) and the VAS at a mean of 26 months postoperatively, with 77% having good to excellent results as indicated by an mHHS >80 and 23% of patients having fair results. No patient had escape of the femoral head. Our study, which includes all patients from the previous study 11 with 2-year follow-up, compares favorably to the abovementioned studies in that it demonstrates significant improvement in multiple PROs, with no patient experiencing femoral head escape in this select group of patients. More importantly, our study shows that with a longer follow-up, the favorable outcomes remain durable. We do note that the HOS-SSS had a drop-off from 81.9 to 70.8 between 2- and 5-year follow-up, which was not statistically significant, although this may be influenced by the small number of patients in this cohort. It could also reflect the normal gradual diminishment in performance in patients involved in high-level sports.
The success or failure of any procedure can be gauged by several different metrics. Byrd and Jones 4 reported on hip arthroscopic surgery in patients with evidence of dysplasia, with a mean follow-up of 27 months, and found a mean mHHS of 77, with 2 patients converting to THA at an average follow-up of 12 and 23 months, respectively. Both patients were noted to have preoperative hip arthritis. 4 No patients in our study required conversion to THA.
Four hips (19.0%) in our study required revision arthroscopic surgery. This is higher than that noted in the study by Nawabi et al 34 (4.3%), although the mean follow-up of that study was significantly shorter at 31 months compared with 68.8 months in our study. Similar to Nawabi et al’s 34 study, all our patients showed an improvement in their PROs after revision surgery that were comparable with nonrevision patients at latest follow-up. We believe that secondary arthroscopic surgery is a far less invasive procedure than a repeat open procedure. There were also few minor complications, which were transient.
We believe that our study has several strengths. All data were collected prospectively, and outcomes were evaluated with 3 different outcome scores, which together have been validated for patients with prearthritic hip conditions.7,28 Second, to our knowledge, this study has among the longest follow-ups of patients with borderline or mild dysplasia who have undergone the arthroscopic management of intra-articular hip abnormalities with capsular plication and labral preservation as inherent components of their management.
We recognize that our study has several limitations. First, this study represents a relatively small cohort of patients. It may be that this is a select group of patients with an uncommon diagnosis. Indeed, of the 631 hip arthroscopic procedures performed during the study period, only 25 hips met all the inclusion criteria. With that said, it compares with the small numbers of patients seen in other studies. In addition, the concept of capsular plication for the management of patients with borderline dysplasia is relatively new in the emerging field of hip arthroscopic surgery. Second, we were unable to report on radiographic findings for all the patients at final follow-up. This reflects a logistical problem of having patients return for radiographs when they are relatively asymptomatic. However, we were able to show consistent improvement in multiple PROs, which have been shown to correlate well with perceived outcomes, independent of radiographic findings. 7 Third, we recognize that patients with hip dysplasia have multiple anatomic differences compared with patients with normal hips, including increased femoral anteversion and smaller femoral heads, which suggests that hip instability in this group of patients may be multifactorial. However, Domb et al 11 and others have shown that through capsular plication, improved soft tissue stability can compensate for the effect of minor bony undercoverage. 21 Additionally, although it has been shown in some studies that increased anteversion can also result in more extensive labral tears, 12 Jackson et al 20 did not find a difference in PROs when comparing patients with different degrees of femoral anteversion who underwent hip arthroscopic surgery for labral lesions. It should be noted that femoral version was not consistently recorded in this cohort. However, it is now the authors’ practice to do so for every patient. We also understand that defining the degree of acetabular dysplasia on a single radiograph view may incompletely represent the 3-dimensional deformity and may incompletely take into account all of the aspects of the dysplastic hip. With that said, there is no universal consensus as to the definition of hip dysplasia. 32 Therefore, we have tried to maintain consistency with prior studies. Future studies may focus on 3-dimensional measurements of acetabular coverage.
Patients with increased femoral anteversion and hip dysplasia will frequently have a finding of internal snapping hip (coxa saltans) from the iliopsoas tendon (Domb et al., unpublished data). This has been shown to be a cause of labral abnormalities. 10 In this study, 52.4% of patients underwent fractional lengthening of this tendon for painful internal snapping. Some authors have expressed concern that in the setting of hip dysplasia with increased anteversion, iliopsoas release may compromise its function as a secondary stabilizer. 14 On the other hand, El Bitar et al 13 showed that patients undergoing hip arthroscopic surgery who had iliopsoas fractional lengthening as an adjunctive procedure for internal snapping hip had greater improvement in PROs than patients who had persistent snapping at a minimum 2-year follow-up. The senior author and others believe that the iliopsoas should not normally act as a stabilizer in the hip and that its action as a secondary stabilizer represents a pathological situation. By imbricating the capsule and preserving the labrum, the static restraints of the hip may be restored, obviating the need for the iliopsoas to act as a stabilizer and allowing the successful treatment of iliopsoas impingement. 10
As this study represents a medium-term follow-up of a soft tissue procedure in patients with an underlying bony problem, a long-term follow-up may show gradual deterioration. However, in this study, there were no subluxations or dislocations, suggesting that capsular plication may impart necessary stability to the hip to prevent recurrent injuries to the capsulolabral complex. No patient in the study required conversion to THA.
Last, we acknowledge that PAO has been the procedure of choice for patients with true acetabular dysplasia, showing lasting improvement at 20-year follow-up. 40 We also again note that catastrophic results have been reported in patients with hip dysplasia undergoing hip arthroscopic surgery. 35 Therefore, we do not believe that any arthroscopic procedure is a substitute for redirectional acetabular osteotomy when it is deemed necessary. In this regard, we believe that in the select group of patients with mild dysplasia (LCEA ≥19°), meticulous capsular plication with inferior shift accompanying labral repair or reconstruction can restore the static stabilizers of the hip. In these select patients, these arthroscopic techniques in the hands of a hip arthroscopic surgery expert may offer a less invasive treatment option. However, we recommend caution when selecting arthroscopic treatment for patients with hip dysplasia and limit this modality only to those hips with mild deformity. Furthermore, it may be advantageous to consider the arthroscopic approach only in centers where all alternatives can be offered and contemplated, including both arthroscopic surgery and PAO.
Numerous patient selection criteria are taken into account when hip arthroscopic surgery is being considered and capsular plication is planned. Caution should be taken in patients with more severe deficits in acetabular coverage (LCEA <19° or anterior center-edge angle <20°), generalized ligamentous laxity as determined by the Beighton criteria, increased femoral anteversion (>30°), coxa valga, and younger female patients. Furthermore, every attempt is made to preserve or reconstruct the labrum, which is an important static stabilizer in the unstable hip. It is notable that all patients were managed in a high-volume hip arthroscopic surgery and joint preservation center, where both open and arthroscopic techniques are performed and offered to patients with dysplasia.
In conclusion, while periacetabular osteotomy remains the standard for treating true acetabular dysplasia, hip arthroscopy may provide a safe and durable means of managing intra-articular abnormalities in the setting of borderline acetabular dysplasia at midterm follow-up. These procedures should be performed by surgeons with expertise in advanced arthroscopic techniques, using strict patient selection criteria, with emphasis on labral preservation and capsular plication.
Footnotes
Presented at the 43rd annual meeting of the AOSSM, Toronto, Ontario, Canada, July 2017.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G.D. is a board member of the American Hip Institute, which receives research support from Adventist Hinsdale Hospital, Arthrex, ATI, Breg, Medacta, Pacira, and Stryker; receives consulting fees from Amplitude, Arthrex, Medacta, Pacira, and Stryker; and receives royalties from Arthrex, DJO Global, and Orthomerica. No funding or support was given for this study in particular.