
Abstract
Background:
The J-bone graft is presumably representative of iliac crest bone grafts in general and allows anatomic glenoid reconstruction in cases of bone defects due to recurrent traumatic anterior shoulder dislocations. As a side effect, these grafts have been observed to be covered by some soft, cartilage-like tissue when arthroscopy has been indicated after such procedures.
Purpose:
To evaluate the soft tissue covering of J-bone grafts by use of magnetic resonance imaging (MRI) and histological analysis.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients underwent MRI at 1 year after the J-bone graft procedures. Radiological data were digitally processed and evaluated by segmentation of axial images. Independent from the MRI analysis, 2 biopsy specimens of J-bone grafts were harvested for descriptive histological analysis.
Results:
Segmentation of the images revealed that all grafts were covered by soft tissue. This layer had an average thickness of 0.87 mm compared with 1.96 mm at the adjacent native glenoid. Of the 2 biopsy specimens, one exhibited evident hyaline-like cartilage and the other presented patches of chondrocytes embedded in a glycosaminoglycan-rich extracellular matrix.
Conclusion:
J-bone grafts are covered by soft tissue that can differentiate into fibrous and potentially hyaline cartilage. This feature may prove beneficial for delaying the onset of dislocation arthropathy of the shoulder.
Current concepts in the treatment of anterior posttraumatic instability of the shoulder have evolved. In a large number of patients, soft tissue repair is still indicated, but more attention has been paid to the amount of glenoid bone loss in recurrent cases. Several authors have linked high recurrence rates after soft tissue–based stabilization procedures to underestimations of the amounts of glenoid bone loss.2,34 Moreover, it is well established that glenoid bone defects require reconstruction when they exceed a certain size.16,30,31,33,39 Over the years, the variety of procedures that have been reported for this indication has increased. The most commonly used procedure is the Latarjet procedure,1,6,7,19,36 followed by autologous iliac crest bone graft transfer.4,17,18,27,28,32,37 Additionally, newer methods, such as the use of femoral, 38 tibial, 26 or clavicle 35 allografts, have been reported to be suitable for the treatment of posttraumatic glenoid defects in chronic shoulder instability.
The goals of all of these procedures are to restore stability, preserve a satisfying range of motion, and delay the onset of instability arthropathy. While the first 2 goals seem attainable, delaying the onset of instability arthropathy appears to be more difficult. As early as 1996, Hovelius et al 13 reported that 20% of young patients exhibited signs of arthropathy 10 years after primary traumatic anterior shoulder dislocation, and some of those patients had experienced no recurrence. Later, this group of investigators reported on 118 Latarjet procedures that were followed for 15 years. 15 These authors stated that signs of arthropathy were present in 56 of 115 shoulders of which radiographs were available. Before surgery, the sample included 22 cases of mild arthropathy and 4 cases of moderate arthropathy. 15 Five cases of mild arthropathy and 1 case of moderate arthropathy had reverted to normal by 15 years after the operations. This finding implies that 36 (31.3%) initially unsuspicious shoulders among these 115 shoulders had developed arthropathy during the follow-up. At a follow-up of 25 years, Hovelius et al 14 found fewer cases of moderate or severe arthropathy among those patients who had undergone surgical stabilization compared with those who had not had surgery. When the investigators included cases of mild arthropathy and excluded patients with alcoholism, the overall rate of arthropathy was 39.7% (23/58) after stabilization compared with 38.6% (61/158) among the nonoperated shoulders. Regarding Latarjet procedures only, these authors reported a total rate of arthropathy of 29.6% (8/27). 14 Earlier, Allain et al 1 had reported on 58 shoulders, of which 34 had arthropathy, for an incidence of 58.6%. A review of the Latarjet procedure and its modifications reported a wide range of the frequency of postoperative arthropathy: from 6% up to approximately 59%. 36 Within the past decade, the literature on iliac crest grafts for the treatment of recurrent shoulder dislocation with osseous defects has increased.4,18,27,28,32,37 Up to 12 years postoperatively, the reported overall rate of arthropathy after the J-bone graft procedure was 22.2%, including mild, moderate, and severe cases. 4 Steffen and Hertel 32 reported the results of autologous iliac crest grafts at 5 to 19 years after surgery. Accounting for the fact that preoperative arthropathy status was unknown in 5 cases, these authors found arthropathy in 7 of 35 cases (20%) at a mean follow-up of 9.2 years.
J-bone grafts, in particular, have been found to be covered by some soft tissue layer at approximately 1 year after stabilization, 4 and this layer could influence the development of arthropathy. Therefore, the objective of this study was to investigate the morphological characteristics and composition of the soft tissue that covers J-bone grafts. While the evaluation of the layer’s thickness by magnetic resonance imaging (MRI) was our primary focus, we also had the opportunity to harvest biopsy specimens of 2 J-bone grafts for histological analyses.
Methods
This investigation was approved by the regional ethics committee under the official notice labeled 415-EP/73/708-2017. Fifteen patients were invited for MRI at a minimum follow-up of 1 year after a J-bone graft procedure. The applied technique is similarly suitable for primary stabilization and revision cases. Our indication for this procedure was bony glenoid defects exceeding 15% of the glenoid surface in cases of primary stabilization. In cases of revision surgery after a failed soft tissue repair, we set the threshold at 10%. The only general exclusion criterion was age over 60 years because of the assumed decreased bone quality at the iliac crest. For this particular investigation, another exclusion criterion was an additional screw fixation of the graft because of expected MRI interference. Based on 3-D reconstructions of routinely performed computed tomography (CT) scans, the defect sizes were preoperatively determined by the Pico method, 5 which allows high inter- and intraobserver reliabilities. 8 The procedures were performed according to previously published literature3,4 and are briefly described here.
Using an anterior approach to the shoulder joint, the surgeon reached the glenoid via a separate split of the subscapularis tendon and the joint capsule. The generally intact but medialized anteroinferior labrum was horizontally cut and mobilized in the cranial and caudal direction. Thus, the defect site was exposed and planed with a rasp. Next, by use of a chisel, a vertical osteotomy at the glenoid neck was created 5 mm medial to the joint surface at an angle of 30° medially. Then, a bicortical graft comprising the upper and outer cortex of the iliac crest was harvested. The initial triangular bone block was shaped to form a graft with a body of cortical and cancellous bone and a keel of blank cortical bone that approximated a “J” shape in the lateral view. Next, the cortical keel of the graft was fit into the produced crevice at the glenoid neck and impacted for a press-fit fixation. In cases of a weak outer cortex, the graft occasionally succumbed to the pressure. In such cases, an additional fixation of the graft body with 2 cannulated 3.0-mm screws was performed. When the graft was stable, its body of cortical and cancellous bone, which faced the humeral head, was molded with an olive-shaped bur to restore the glenoid concavity. The osseous surface of the graft was then positioned in-plane with the cartilage surface of the intact glenoid. Next, the split labrum was sutured around the body of the graft, and the capsule was sutured to enclose the intra-articular portion of the graft. The split subscapularis tendon was sutured separately, and the wound was closed with subcutaneous and skin sutures.
Images were acquired with a 3.0-T scanner (Achieva; Philips Medical Systems) through use of flexible coils for the shoulder examination (SENSE Flex-M; Philips Medical Systems). Axial images (Figure 1) were obtained by use of a 3D gradient echo sequence with selective water excitation (e3D_WATSc HR) (repetition time, 20 ms; echo time, 6.91 ms; flip angle, 10°; slice thickness, 1.5 mm; slice spacing, 0.75 mm; in-plane resolution, 0.3 × 0.3 mm). The MRI data were further processed using custom-designed software (Chondrometrics). In each patient, both the complete glenoid cartilage and the tissue covering the graft were analyzed separately by manual segmentation. The border between these areas was defined by the previously described step formation technique. 22 Both the surface area of the cortical bone and the surface area of the attached tissue layer were evaluated. This process facilitated the calculations of the subchondral bone area (tAB), the mean cartilage thickness over the subchondral bone area (ThCtAB.Me), and the volume of cartilage (VC) of both regions alone and in relation to each other.
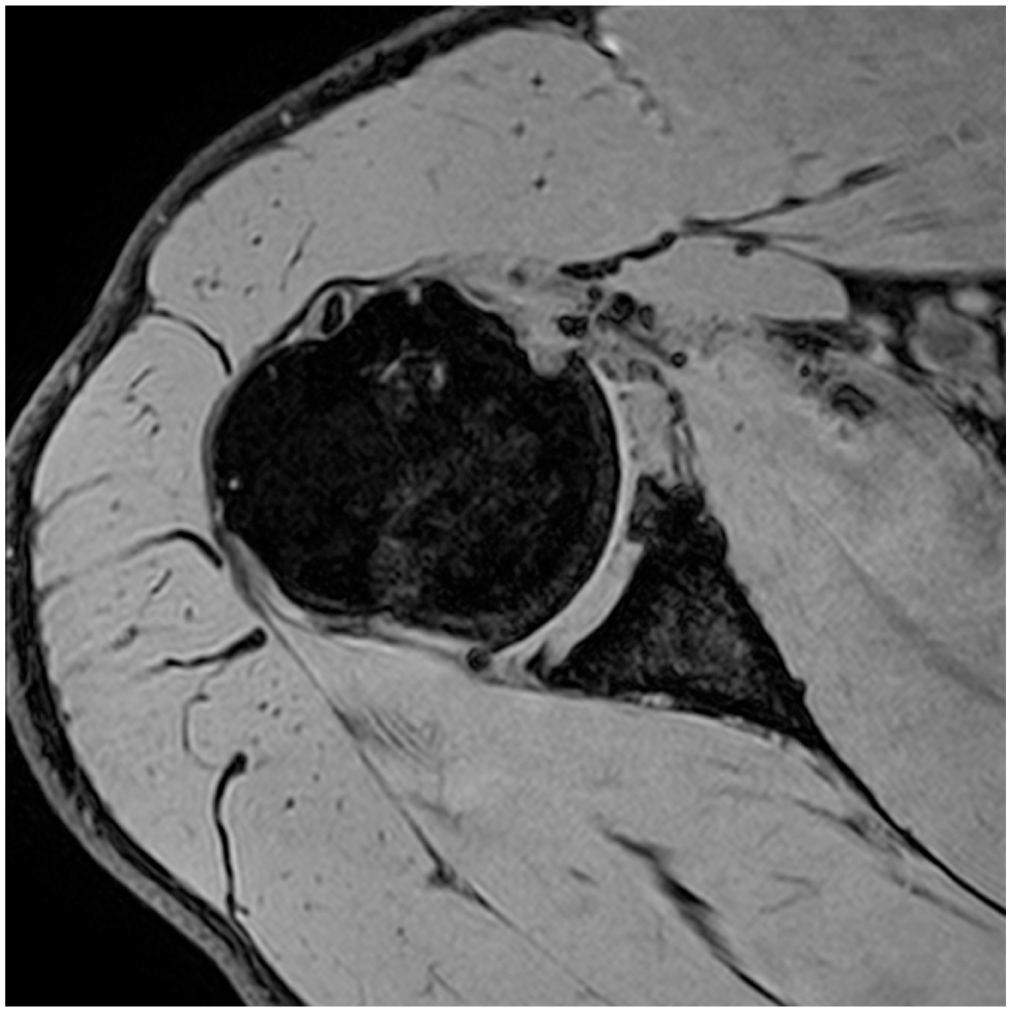
Axial view of a magnetic resonance image collected with a 3D gradient echo sequence with selective water excitation.
Independent from the patients who underwent follow-up assessment with MRI, 2 biopsy specimens of J-bone grafts were obtained. One sample was harvested from an intact graft during arthroscopy for subacromial impingement by use of a 2-mm punch for bone marrow biopsy. In the second case, revision surgery after a J-bone graft procedure was indicated, and the fractured and medialized graft was removed and examined. The histological workups were performed by 2 independent investigators (D.N. and A.T.). One investigator (D.N.) used hematoxylin and eosin staining, and the other investigator (A.T.) used Safranin-O and Fast-Green staining after routine calcifications with ethylenediaminetetraacetic acid (EDTA) to visualize the areas that were rich in glycosaminoglycans.
Results
Analysis of the MRI Data
Twelve of the 15 patients accepted their invitations to participate in this investigation. The MRIs obtained from 8 patients were appropriate for segmentation (Figure 2). The images of the remaining 4 shoulders exhibited artifacts that made reliable analyses impossible, as illustrated in Figure 3.
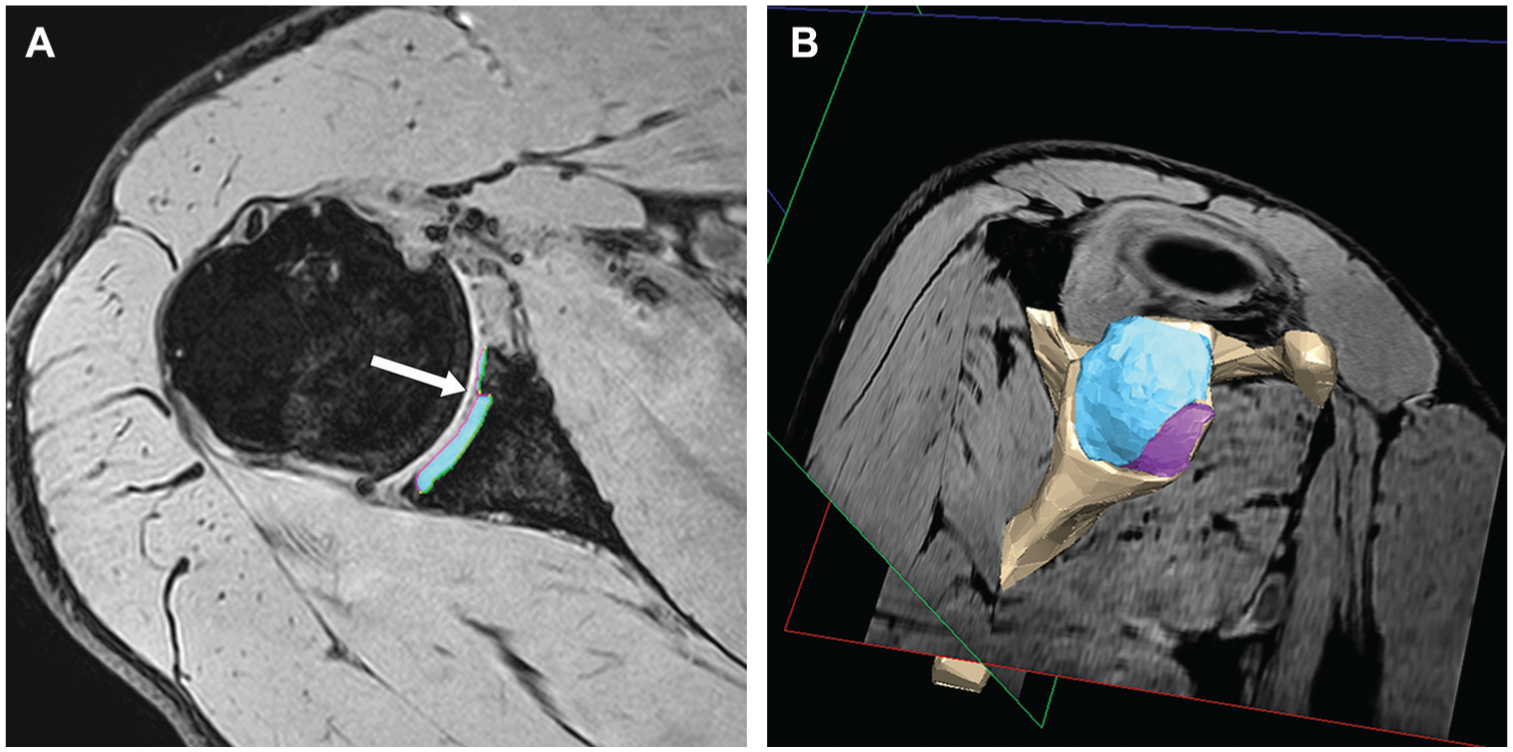
(A) Image from Figure 1 after manual segmentation. The arrow marks the step formation. The green lines mark the cortical bone surface, and the pink line indicates the cartilage surface. The turquoise area represents the cartilage thickness. (B) Three-dimensional reconstruction of the entire set of segmented axial images in the same patient presented in Figures 1 and 2A. The turquoise area indicates the glenoid cartilage, and the pink area depicts the cartilage covering the J-bone graft.
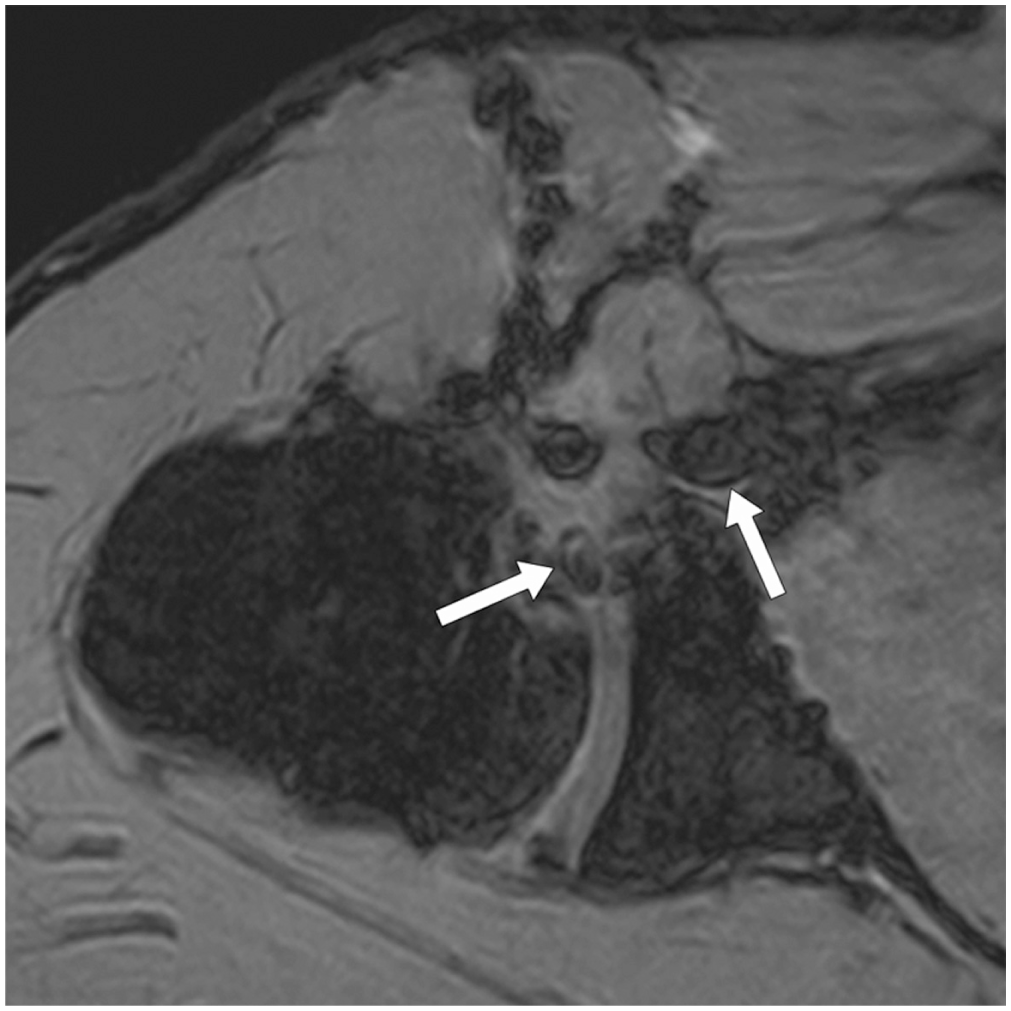
Axial magnetic resonance image depicting artifacts around the anterior portion of the glenoid and the former anterior surgical approach (white arrows).
We believe that these artifacts were most likely caused by nonabsorbable sutures or scar tissue along the surgical approach. All 8 patients were male. On the day of surgery, their average age was 25.8 years (range, 17.3-37.2 years). The average time from surgery to follow-up was 2.3 years (range, 1.1-3.4 years). The mean preoperative defect size was 17.6%. The procedures were performed as primary stabilizations in 6 cases, and 2 patients had undergone revision surgeries for failed soft tissue repairs.
The mean areas of the subchondral bone (tAB) were 8.02 cm2 (range, 4.81-9.80 cm2) for the glenoid and 1.42 cm2 (range, 0.76-2.10 cm2) for the graft. Thus, the tAB averaged 9.44 cm2 (range, 5.57-11.77 cm2). The average relative graft size was 14.9% (10.9%-19.8%). The average cartilage surface area (AC) of the glenoid was 9.45 cm2 (range, 5.30-12.42 cm2), and the area of the soft tissue layer on the graft averaged 1.77 cm2 (range, 1.00-2.63 cm2). The graft was completely covered by soft tissue in all cases. The mean cartilage thickness (ThCtAB.Me) of the glenoid was 1.96 mm (range, 1.67-2.25 mm) with a standard deviation ranging from 0.51-0.81 mm, which was evaluated for the whole set of segmented images of each patient. The mean thickness of the soft tissue layer covering the graft was 0.87 mm (range, 0.61-1.11 mm) with a standard deviation of 0.27 mm (range, 0.20-0.35 mm). The average volume of the glenoid cartilage was 1708.75 mm3 (range, 845.30-2335.10 mm3), and the average volume of the layer covering the graft was 157.06 mm3 (range, 62.17-280.73 mm3) (Table 1).
Data Evaluated by Segmentation a
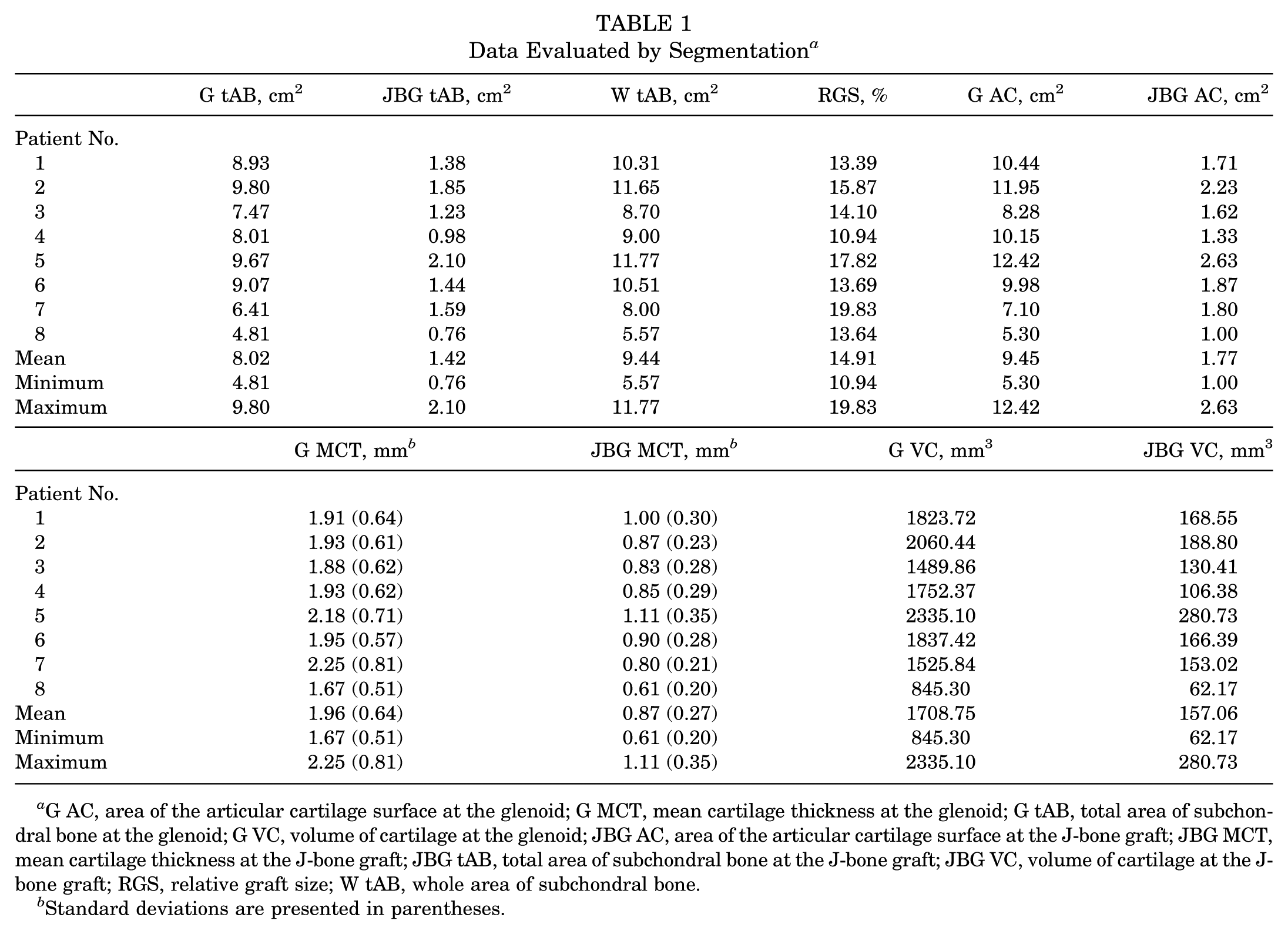
G AC, area of the articular cartilage surface at the glenoid; G MCT, mean cartilage thickness at the glenoid; G tAB, total area of subchondral bone at the glenoid; G VC, volume of cartilage at the glenoid; JBG AC, area of the articular cartilage surface at the J-bone graft; JBG MCT, mean cartilage thickness at the J-bone graft; JBG tAB, total area of subchondral bone at the J-bone graft; JBG VC, volume of cartilage at the J-bone graft; RGS, relative graft size; W tAB, whole area of subchondral bone.
Standard deviations are presented in parentheses.
Histological Analysis
Patient 1 was a man who was 28 years old when he received the J-bone graft. He was admitted for arthroscopic subacromial bursectomy 10.3 years after this procedure. At the time of biopsy, he had no radiological signs of arthropathy. At arthroscopy, the graft was covered by soft tissue (Figure 4). Slices were stained with hematoxylin and eosin.
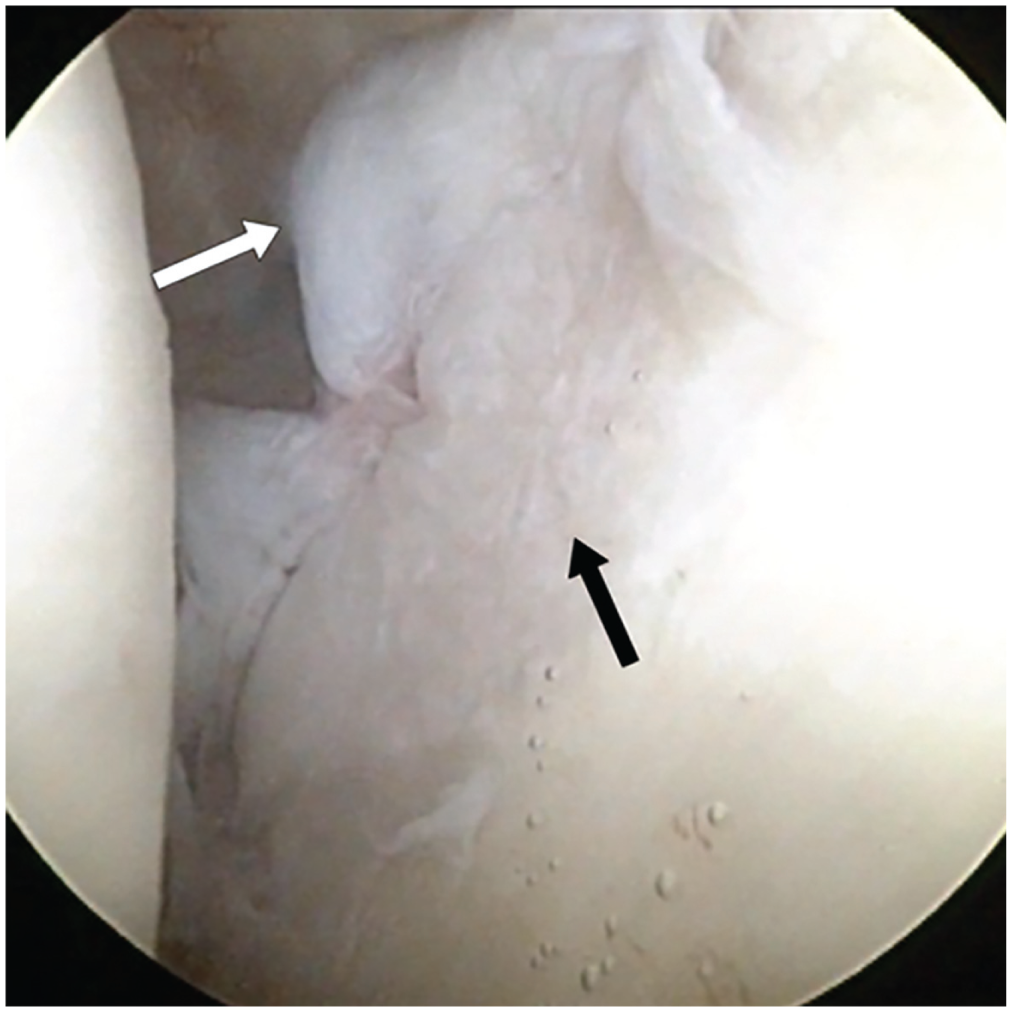
Appearance of a J-bone graft (black arrow) with the surrounding labrum (white arrow) at arthroscopy.
Examinations revealed hyaline-like cartilage covering the graft (Figure 5A). The chondroid surface was irregular but not fissured. Relative to regular hyaline cartilage, the chondrocytes were not as evenly arranged and were surrounded by a more inhomogeneous chondroid matrix (Figure 5B). The chondrocytes embodied nuclei, which was a sign of vitality. No necrosis was evident. The subchondral bone marrow structures exhibited signs of remodeling with trabeculae of different widths, as demonstrated in Figure 5C.
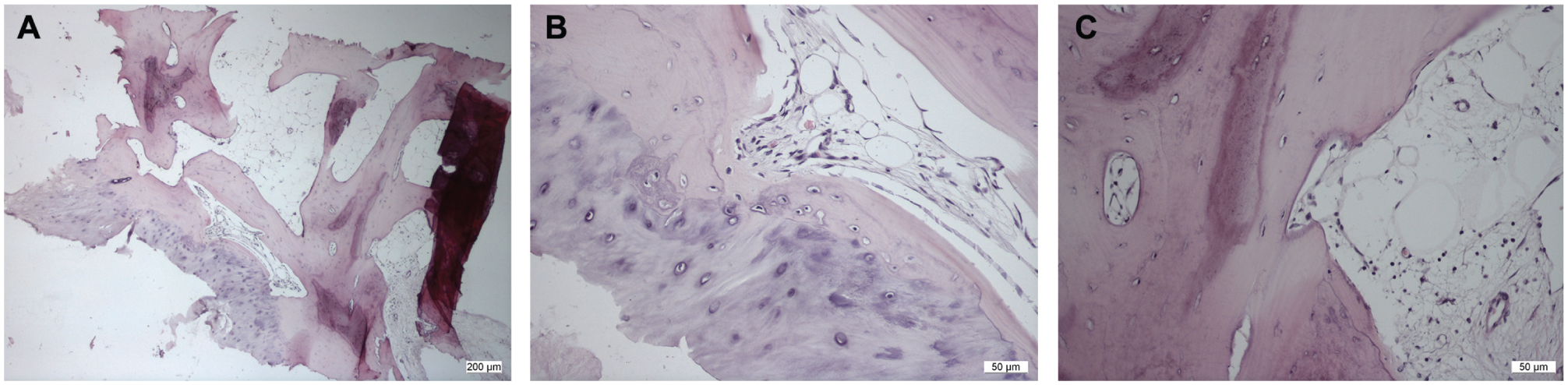
(A) Overview of the histological sample 1 (hematoxylin and eosin staining). (B) Detailed view of the cartilage layer showing irregularly arranged chondrocytes and chondrocytes surrounded by a more inhomogeneous matrix as seen in regular hyaline articular cartilage. (C) Osseous trabeculae of different widths indicate that remodeling had occurred.
The second patient sustained a graft fracture at an uncertain time point. He was 3 weeks late for his first postoperative appointment when he stated that he had experienced another dislocation 2 days earlier. If the fracture had not occurred earlier than that, the graft had been in place for 34 days (Figure 6A). The patient initially refused revision surgery. Five months after the primary procedure and several recurrent dislocations, revision was performed. The primary graft was osteolytic and, by then, too small to fill the defect at the glenoid (Figure 6B). Thus, the graft was replaced with another J-bone graft with additional screw fixation. The removed fragment was again evaluated by descriptive histological analysis. As shown in Figure 7A, the majority of the graft was covered in fibrous tissue devoid of cartilaginous extracellular matrix. However, a significant portion of the area resembled cartilage-like tissue as identified by Safranin-O and Fast-Green staining. The chondrocytes were embedded close to the underlying bone and were covered by a layer that contained flat fibrocartilaginous cells (Figure 7).
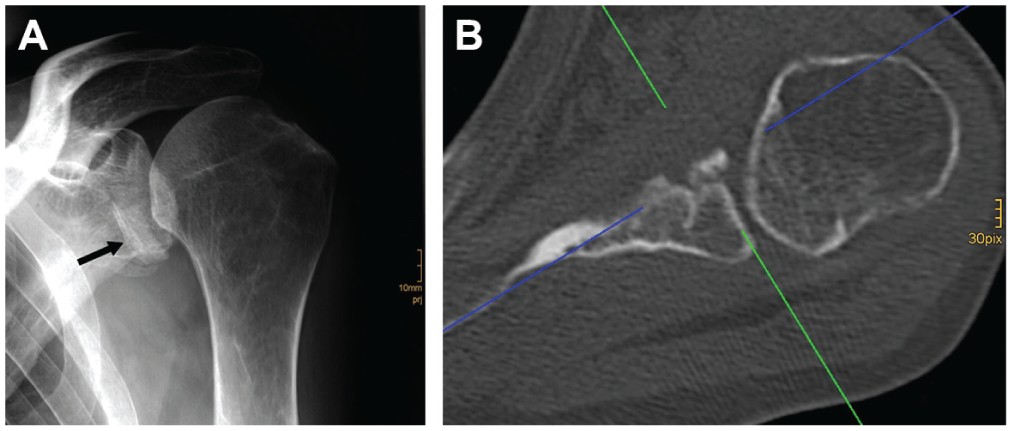
(A) Radiograph of the fractured J-bone graft at the patient’s first postoperative visit 36 days after surgery. The black arrow marks the graft. (B) Appearance of the resorbed graft on an axial computed tomography image 5 months after primary surgery.
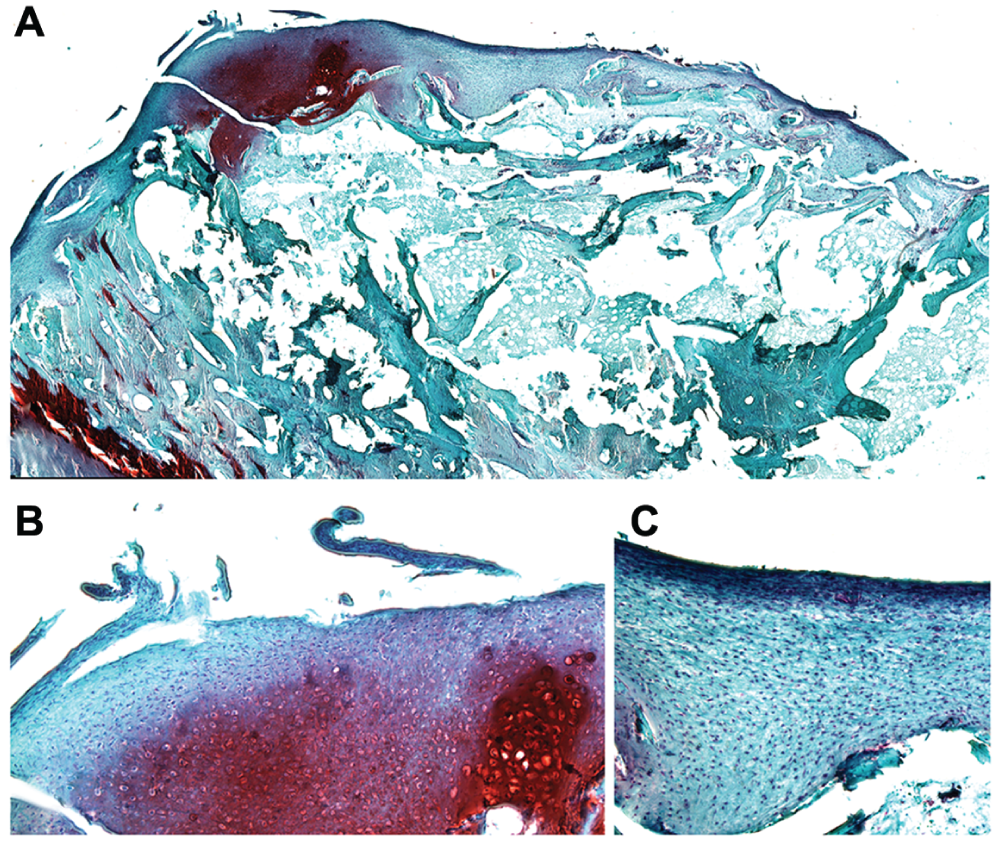
(A) Overview of histological sample 2 (Safranin-O staining and Fast Green staining). (B) A detailed view showing the chondrocytes embedded in a glycosaminoglycan-rich matrix. (C) A detailed view of the tissue surrounding the cluster described in Figure 7B showing a layer of flat fibrocartilaginous cells.
Discussion
The segmentation of MRIs revealed that the J-bone grafts were completely covered by soft tissue. The assumption that cartilage-like tissue was covering these grafts was correct.
Graichen et al 12 demonstrated that quantitative MRI can be used to accurately determine volumes and thicknesses in joints with highly curved and thin cartilage layers, such as the shoulder joint. Moreover, using segmentation, these authors reported 1.7 ± 0.13 mm to be the mean ± SD cartilage thickness at the glenoid cavity, and they found the thickest cartilage layer of up to 3.1 ± 0.1 mm in the periphery of the glenoid. Later, Zumstein et al 40 found a comparable thickness distribution of glenoid cartilage as determined with CT scans. In contrast, Schleich et al 29 recently detected only minor differences in cartilage thickness at the glenoid. In comparison, the soft tissue layers we found on the grafts, which were positioned in the periphery of the glenoid, were only just a third to a fifth of the maximum thickness that has been reported for the glenoid marginal region.12,29,40 The reason for this difference may be the technique of shaping the graft surface flush to that of the adjacent glenoid cartilage. This technique allows for the restoration of joint congruity. Incongruity could either promote arthropathy or lead to unsatisfactory graft remodeling or even graft resorption due to reduced compression according to Wolff’s law. 9
Generally, the development of arthropathy after shoulder dislocation seems to be predetermined with or without surgical intervention. Long-term results at 15 to 25 years, such as those reported for the Latarjet procedure,1,6,15,20,36 are not available for the J-bone graft procedure or other iliac crest grafts. The available average follow-up periods for these procedures are approximately 10 years, and the reported rates of arthropathy all lie near 20%, as Hovelius et al 13 had already recorded in 1996. The creation of a congruent joint has been reported to decelerate the onset of arthropathy.14,15 This creation can be achieved with both the Latarjet and iliac crest procedures. More specifically, data on graft remodeling 21 and the restoration of glenoid shape 22 have been published for the J-bone grafts and are probably representative of the iliac crest crafts used in this context in general. Additionally, the fact that such grafts are covered by soft tissue that partially resembles cartilage may be an advantage in the long term. The origin of the cartilage layer could in part stem from multipotent mesenchymal stromal cells contained within the bone marrow of the J-bone graft. In addition to the differentiation and engraftment of mesenchymal stromal cells, paracrine secretions could drive the repair/remodeling process. 25 A heterogeneous tissue consisting of fibrocartilage, fibrous tissue, and hyaline cartilage formed around the J-bone grafts, and this process is reminiscent of the outcome described for the healing process after microfracture, a technique that is widely used to regenerate hyaline cartilage after bone marrow stimulation.10,11 As a probable alternative explanation, Ockert et al 24 reported that fibrocartilage was found in all regions of the labrum around the glenoid. This fibrocartilage could be the origin of the cartilage tissue that we found because the labrum is sutured around the J-bone graft. Similarly, the tissue could result from a combination of both processes, and this supposition may be supported by the capacity of mesenchymal stem cells to differentiate into chondrocytes that is induced when pressure is applied. 23 A similar effect might be observed with other iliac crest bone grafts, but we find it questionable whether this effect could be expected with coracoid transfers, because, with these transfers, the cortical bone faces the joint surface.
This investigation has some limitations. First, the number of cases was relatively low. However, the presented cases suffice for this descriptive study. Second, the 2 patients who were available for histological analyses were heterogeneous in terms of age and the time from surgery to biopsy. However, these were random samples, which, due to ethical considerations, could not be obtained in a more standardized fashion or in larger numbers. Nonetheless, now that we have described the quantity of tissue covering these grafts, the next question is what type of tissue forms these covering layers. From this perspective, we believe that these histological samples delivered some supplemental information.
To our best knowledge, this is the first investigation of the quantitative and qualitative properties of soft tissue coverings such as those that occur on intra-articular iliac crest bone grafts. The true benefit of this biological and anatomic glenoid restoration over the long term is yet to be assessed, but we believe it may prove beneficial for delaying the onset of dislocation arthropathy of the shoulder. Long-term results from randomized controlled trials including iliac crest bone grafts and coracoid transfers have not yet been reported, but such data will enable critical comparisons of both techniques.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: M.H. and W.W. were formerly employed by Chondrometrics.