
Abstract
Background:
Previous research has examined associations between concussion history and adverse health outcomes among former professional football players. Less is known about the potential effects of concussion among former college football players without additional exposure at the professional level.
Purpose:
To examine the association between concussion and adverse health outcomes in a cohort of former college football players without exposure to professional football, 15 years after their playing careers ended.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A sample of 204 former collegiate football players (23.4% of eligible athletes with available contact information)—all of whom played at least 1 season of football from 1999 to 2001 in the National Collegiate Athletic Association (NCAA) and had no professional football exposure—completed a general health survey that assessed lifetime concussion history and included the following: the Veterans RAND 36 Item Health Survey, containing a physical composite score (PCS) and mental composite score (MCS); the depression module of the Patient Health Questionnaire; and the 4-item CAGE alcohol dependence questionnaire (for “cutting down, annoyance by criticism, guilty feeling, and eye-openers”). Multivariable binomial regression models estimated adjusted prevalence ratios (PRs) with 95% CIs while controlling for demographics and playing history covariates through forward selection model building.
Results:
Most participants reported a concussion history (84.3%). Overall, 22.1% and 39.2% of participants reported a PCS and an MCS <50, respectively (indicating worse health than the US national average); 19.1% reported Patient Health Questionnaire scores ≥10 (indicating moderate/severe depression); and 24.8% reported CAGE scores ≥2 (indicating alcohol dependence). The prevalence of having an MCS <50 was higher among those reporting ≥3 versus 0 concussions (PR, 2.5; 95% CI, 1.3-4.9). Controlling for body mass index (BMI), the prevalence of moderate/severe depression was higher among those reporting ≥3 versus 0 concussions (PR, 4.2; 95% CI, 1.0-16.3). Controlling for BMI, the prevalence of having a PCS <50 was higher among those reporting ≥3 versus 1 or 2 concussions (PR, 2.6; 95% CI, 1.3-5.0) but not 0 concussions (PR, 1.5; 95% CI, 0.6-3.6). No associations were found for alcohol dependence.
Conclusion:
Associations between a history of multiple concussions and adverse health outcomes were found among former collegiate football players without professional football exposure but were limited to those reporting ≥3 prior concussions. Because only 23.4% of eligible athletes responded to the survey, the possibility of ascertainment bias exists, and our findings should thus be interpreted with some caution. Continued examination within nonprofessional football populations is needed, but findings highlight the need for prevention efforts to reduce concussion incidence.
While concussions occur in just about every sport, concussion incidence in football consistently exceeds that of nearly all other sports in studies of high school and collegiate athletes. Data from high school sports-related injury surveillance reported concussion rates of 0.47 to 0.64 per 1000 athlete exposures (ie, 1 athlete’s participation in 1 practice or 1 competition).9,35 Similar rates (0.61 per 1000 athlete exposures) were reported in college football.9,32,50 Of all football positions, running backs and linebackers have a higher risk of concussion.9,35
The original National Collegiate Athletic Association (NCAA) Concussion Study of 2905 college football players from 1999 to 2001 yielded several seminal findings. 14 Players with a history of concussion were more likely to sustain future concussive injuries than were those with no history. Furthermore, 1 of every 15 players who were concussed sustained a within-season repeat concussion, and nearly all repeat concussions (92%) occurred within 10 days of the initial concussion. As compared with a single concussive injury, these repeats were also associated with slower recovery of neurologic function. 14 The NCAA Concussion Study also focused on the acute recovery after concussion and identified that several days were required for recovery from symptoms, cognitive dysfunction, and postural instability, with recovery rates varying significantly across athletes. 14
Equally important to defining the acute concussion recovery course of active athletes is advancing our understanding of the potential long-term effects of concussion on neurologic and psychological health. Cross-sectional comparisons based on estimates of the prevalence of Alzheimer disease, mild cognitive impairment, and depression in the general US population showed that retired professional football players appear to develop Alzheimer disease at a younger age than the average US male.12,13 Those with a history of ≥3 concussions during their playing careers are at increased risk of being diagnosed with mild cognitive impairment and depression than are those without a concussion history.12,13 Our studies of >3700 retired professional football players provided an impetus for future research in this area. However, these findings are limited by their retrospective and cross-sectional nature and involve only former football players who had added exposure at the professional level. A similar study examined former college athletes but was not restricted to football players and included a number who subsequently played professionally.22,23 These studies served as the impetus for a similar study in a college-only sample.
Therefore, the purpose of this study was to examine the association between concussion and adverse health outcomes among former college football players without exposure to professional football, 15 years after their playing career ended. An additional purpose is to establish a data set to prospectively follow health outcomes across the life span in a large cohort of former NCAA football athletes.
Methods
Data Collection
The study was approved by the institutional review board of the University of North Carolina at Chapel Hill. The cross-sectional study is based on a cohort of former collegiate football players from 22 universities who participated in the original NCAA Concussion Study (n = 2905). 14 These individuals played at least 1 season during the 1999, 2000, or 2001 college football season.
To locate these former college football athletes, we contacted the athletic director, sports information director, alumni representatives, and athletic trainers of each university to obtain contact information. We were able to obtain contact information for 1383 athletes: 617 with valid email addresses, 513 with invalid contact information, and 253 with a postal address or phone number. This cohort was sent an invitation by email or postal mail to participate in the research study, which included the URL to our online questionnaire (housed in Qualtrics). Upon visiting the URL, the participant received additional study information and research staff contact information and was asked to electronically consent to participate.
The online questionnaire was modified from the Retired NFL Players General Health Survey12,13,24 as well as a previous questionnaire that has been administered to samples of former collegiate athletes from all sports.22,23 Data collected included demographics, medical history, injury history, and health history. Nonrespondents were recontacted via email, a second postal mailing, and/or telephone follow-up. With multiple contact attempts, a total of 224 participants completed surveys.
Inclusion Criteria
For this study, we focused on athletes who played at least 1 season of collegiate football during the NCAA Concussion Study (1999-2001). In addition, to examine the association between concussion history and health outcomes exclusively among those whose highest level of competition was at the collegiate level, we excluded respondents who went on to play professional football. Our final sample consisted of 204 former collegiate football players (23.4% of those with valid contact information).
Measures Included in the Current Study
Main Exposure: Lifetime Concussion History
Respondents were provided with a definition of concussion that was adapted from one utilized in previous research. 36 Concussions were defined as occurring typically but not necessarily from a blow to the head, followed by a variety of symptoms that may include any of the following: headache, dizziness, loss of balance, blurred vision, “seeing stars,” feeling in a fog or slowed down, memory problems, poor concentration, nausea, throwing up, and loss of consciousness. Respondents were then asked to report the number of concussions that they believed they had sustained during participation in sports, including before and at the high school and collegiate levels. In addition, respondents reported the number of nonsport-related concussions (eg, from a motor vehicle accident, fall, or violence). We stratified total lifetime concussion history data into 3 categories: 0 (referent), 1 or 2, and ≥3 concussions. This approach is consistent with that employed by prior studies.12,13,22,23
Main Outcomes
Physical and Mental Health
The Veterans RAND 36 Item Health Survey (VR-36) is a self-administered instrument in the public domain that assesses health status and estimates how well individuals function with activities of daily living. The VR-36 was developed from the RAND 36-Item Health Survey used in the RAND Medical Outcomes Study 20 ; specifically, the VR-36 replaces yes/no responses with 5-point choices.
The VR-36 yielded 2 composite scores: first, a physical composite score (PCS), which included scores of physical functioning, role physical, bodily pain, and general health; second, a mental composite score (MCS), which included scores of vitality, social functioning, role emotional, and mental health. 20 Higher PCS and MCS indicated better physical and mental health. Scores were standardized to data of the general US population via norm-based scoring, which employed a linear T score transformation with a mean of 50 and a standard deviation of 10. Thus, scores >50.0 suggested better physical or mental health than that of the general US population. Previous research suggested that the minimal clinically important differences (MCIDs; ie, the smallest differences that would be deemed important by clinicians) 18 for PCS and MCS range from 1 to 5 points in a variety of population segments, including those seeking care through Veterans Affairs health care facilities and patients diagnosed with arthritis.20,21,43-45
Depression
In addition to the MCS, the depression module of the Patient Health Questionnaire (PHQ-9) has been used to screen and diagnose health disorders. The PHQ-9 is a self-administered version of the PRIME-MD (Primary Care Evaluation of Mental Disorders) diagnostic tool. 30 Thedepression module consists of the 9 criteria provided by the Diagnostic and Statistical Manual of Mental Disorders (fourth edition), scored from 0 (not at all) to 3 (nearly every day). PHQ-9 scores were categorized into a binomial depression severity classification via standardized cutoffs that differentiated between no or mild depression (PHQ-9 scores <10) and moderate to severe depression (PHQ-9 scores ≥10). 30 The MCID for PHQ-9 is not well established; however, 1 study examining older primary care patients suggested a 5-point difference to be clinically meaningful. 33
Alcohol Dependence
Alcohol dependence was assessed with the CAGE, a 4-item questionnaire that refers to “cutting down, annoyance by criticism, guilty feeling, and eye-openers”. 8 Scores ≥2 (at least 2 of the questions answered “yes”) have good positive predictive value (ie, individuals with these scores are likely to actually suffer from alcohol dependence). 28 The measure was validated in multiple clinical and research settings.2,28 CAGE scores were recoded into a dichotomous variable (scores <2 and ≥2). No MCID is available for the CAGE.
Covariates: Demographics and Playing History
We obtained self-reported information on age, race/ethnicity, body mass index (BMI), year in which athletes started playing football, and whether or not athletes played professional football.
Statistical Analyses
Analyses were conducted on SAS (v 9.4; SAS Institute Inc). Frequencies and percentages for all variables were calculated. Next, crude prevalence ratios (PRs) and mean differences (MDs) with total concussion history as the main exposure were estimated with classic tabular methods and linear regression, respectively. Outcomes of interest included physical health (PCS), mental health (MCS), depression (PHQ-9), and alcohol dependence (CAGE). Five cases had incomplete data from the VR-36 and consequently did not have PCS and MCS; 6 cases had missing data for CAGE. These cases with missing data were not considered in their respective analyses.
Adjusted PRs and 95% CIs were estimated through binomial regression. Fitting algorithms for binomial regression models were stabilized via Poisson residual and robust variance estimation.11,41,49 To satisfy assumptions of linear regression, models originally utilized transformed variables. However, these transformations did not change the direction or significance of effect estimates. Thus, effect estimates from models with untransformed variables were reported. 16 In addition, we did not find evidence of multicollinearity, as no covariates yielded variance inflation factors above the recommended cutoff point of 10. 15
All regression models utilized forward selection model building with total concussion history as the main exposure. With the exception of the models for physical health, covariates determined from the multivariable binomial regression and linear regression models were the same. Given the small range of scores for CAGE (0-4), we opted to solely use binomial models and not linear regression models. All PRs with 95% CIs excluding 1.00 and all MDs with 95% CIs excluding 0.00 were deemed statistically significant.
Results
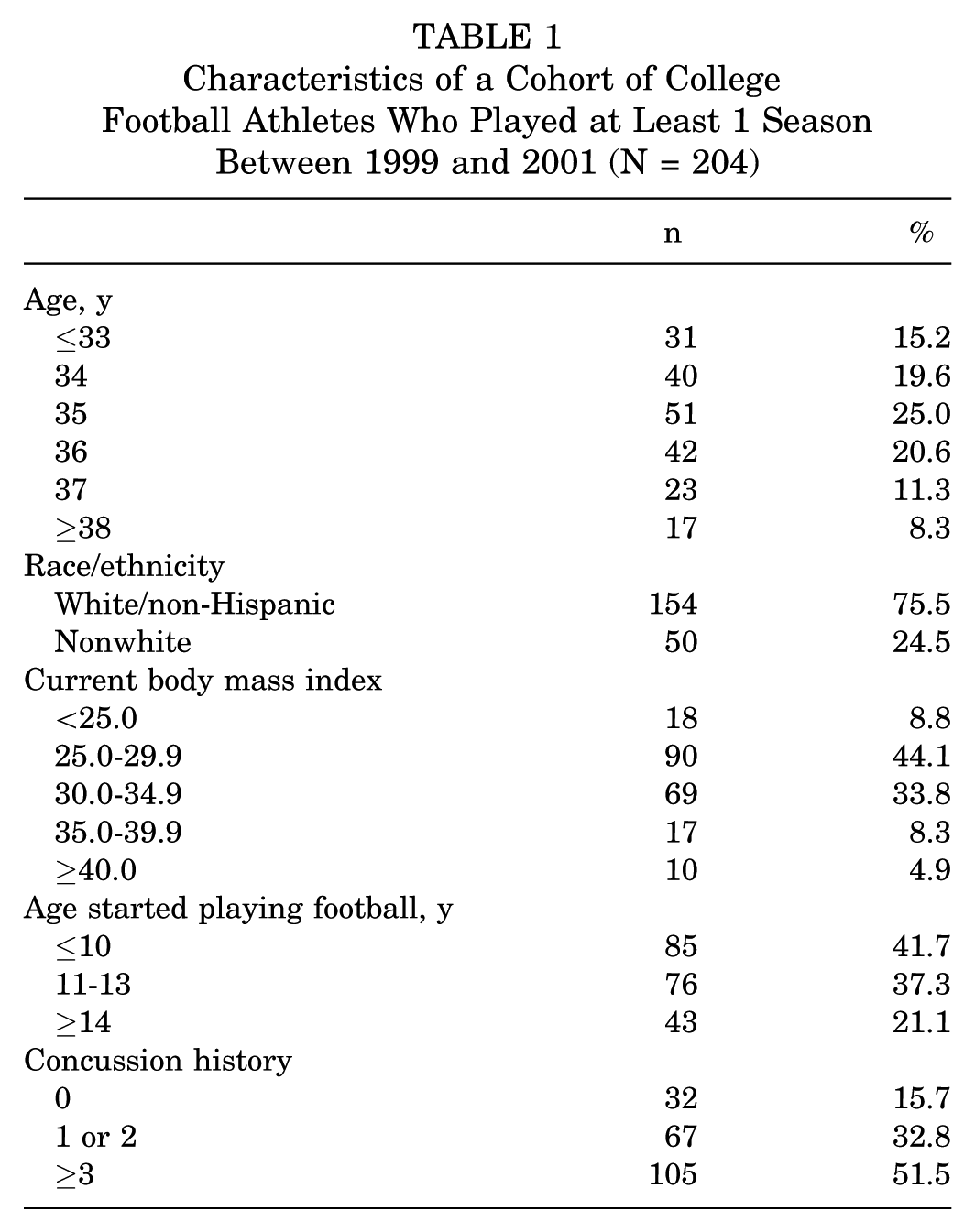
Most participants were 34 to 36 years old (65.2%, n = 133) and white/non-Hispanic (75.5%, n = 154), began playing football at age ≤13 years (78.9%, n = 161), and reported a concussion history (84.3%, n = 172) (Table 1). Among those with ≥3 concussions, the median number of concussions reported was 5 (interquartile range, 4-8).
Characteristics of a Cohort of College Football Athletes Who Played at Least 1 Season Between 1999 and 2001 (N = 204)
Physical Health
The mean PCS among the sample was 53.8 (SD = 7.3; Table 2), with 22.1% (n = 44) having scores <50 (indicative of a score less than the US national average; ie, worse health). Former college football athletes reporting ≥3 concussions had the lowest mean PCS (52.6; SD = 7.8). Across the groups stratified by concussion history, the only statistically significant concussion-related differences were between former college football athletes reporting ≥3 concussions and 1 or 2 concussions. Controlling for BMI, the prevalence of having a PCS <50 among former college football athletes reporting ≥3 concussions in total was 2.6 times (95% CI, 1.3-5.0) that of former college football athletes reporting 1 or 2 concussions. In addition, for every 5-point increase in BMI, the prevalence of having a PCS <50 increased by 75% (95% CI, 38%-122%).
Prevalence Ratios and Mean Differences of the VR-36 PCS by Self-reported Total Concussion History in a Cohort of College Football Athletes Who Played at Least 1 Season Between 1999 and 2001 a
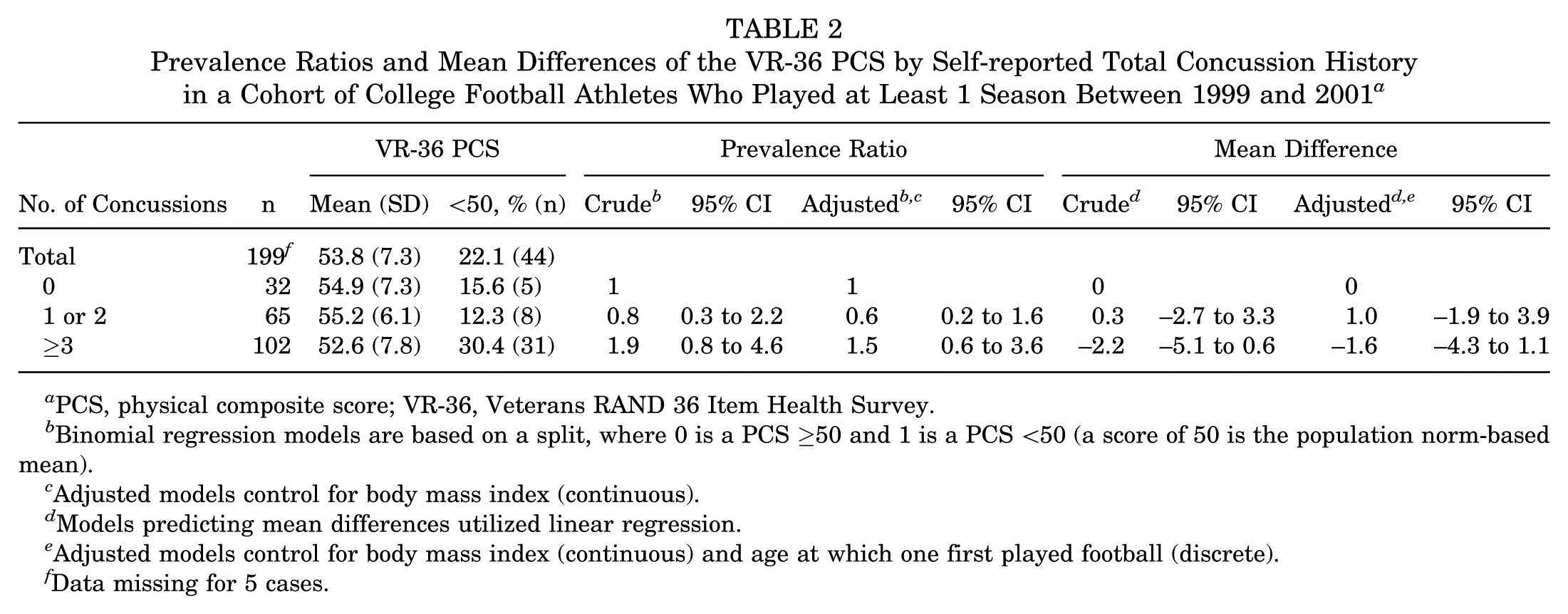
PCS, physical composite score; VR-36, Veterans RAND 36 Item Health Survey.
Binomial regression models are based on a split, where 0 is a PCS ≥50 and 1 is a PCS <50 (a score of 50 is the population norm-based mean).
Adjusted models control for body mass index (continuous).
Models predicting mean differences utilized linear regression.
Adjusted models control for body mass index (continuous) and age at which one first played football (discrete).
Data missing for 5 cases.
Similar findings were also found in linear regression models. Controlling for BMI and age at which one first played football, former college football athletes reporting ≥3 concussions had a lower mean PCS than did former college football athletes reporting 1 or 2 concussions (MD = −2.7; 95% CI, −4.8 to −0.6). Also, controlling for concussion history and age at which one first played football, for every 5-point increase in BMI, the PCS decreased by 2.2 (95% CI, 1.1-3.3). Last, controlling for concussion history and BMI, for every additional 3 years back for which one started playing football, the PCS decreased by 1.0 (95% CI, 0.0-2.0).
Mental Health
The mean MCS among the sample was 48.7 (SD = 11.2; Table 3), with 39.2% (n = 78) having scores <50 (ie, less than the US national average). Statistically significant crude associations were observed between concussion history and mental health. The prevalence of having an MCS <50 among former college football athletes reporting ≥3 concussions was 2.5 times (95% CI, 1.3-4.9) that of former college football athletes reporting 0 concussions. In addition, the prevalence of having an MCS <50 among former college football athletes reporting ≥3 concussions was 2.2 times (95% CI, 1.4-3.5) that of former college football athletes reporting 1 or 2 concussions. Forward model building yielded no covariates to include in final models.
Prevalence Ratios and Mean Differences of the VR-36 MCS by Self-reported Total Concussion History in a Cohort of College Football Athletes Who Played at Least 1 Season Between 1999 and 2001 a

MCS, mental composite score; VR-36, Veterans RAND 36 Item Health Survey.
Binomial regression models are based on a split, where 0 is an MCS ≥50 and 1 is an MCS <50 (a score of 50 is the population norm-based mean). Forward model building yielded no covariates.
Models predicting mean differences utilized linear regression.
Data missing for 5 cases.
Statistically significant prevalence ratio (95% CI excludes 1.00).
Statistically significant mean difference (95% CI excludes 0.00).
Statistically significant findings were also found in the linear regression models. Former college football athletes reporting ≥3 concussions in total also had a lower mean MCS than that of former college football athletes reporting 0 concussions (MD = −7.7; 95% CI, −11.9 to −3.4) and 1 or 2 concussions (MD = −6.1; 95% CI, −9.4 to −2.7).
Depression
The mean PHQ-9 score among the sample was 4.8 (SD = 5.4; Table 4), with 19.1% (n = 39) having scores ≥10 (indicative of moderate to severe depression). Statistically significant crude associations were observed between concussion history and depression. In multivariable binomial regression models controlling for covariates, the statistically significant association was attenuated but still present. Controlling for BMI, the prevalence of moderate to severe depression among former college football athletes reporting ≥3 concussions in total was 4.2 times (95% CI, 1.0-16.3) that of former college football athletes reporting 0 concussions. In addition, controlling for BMI, the prevalence of moderate to severe depression among former college football athletes reporting ≥3 concussions was 2.8 times (95% CI, 1.3-6.0) that of former college football athletes reporting 1 or 2 concussions. Finally, controlling for concussion history, for every 5-point increase in BMI, the prevalence of moderate to severe depression increased 37% (95% CI, 4%-81%).
Prevalence Ratios and Mean Differences of Depression by Self-reported Concussion History in a Cohort of College Football Athletes Who Played at Least 1 Season Between 1999 and 2001 a
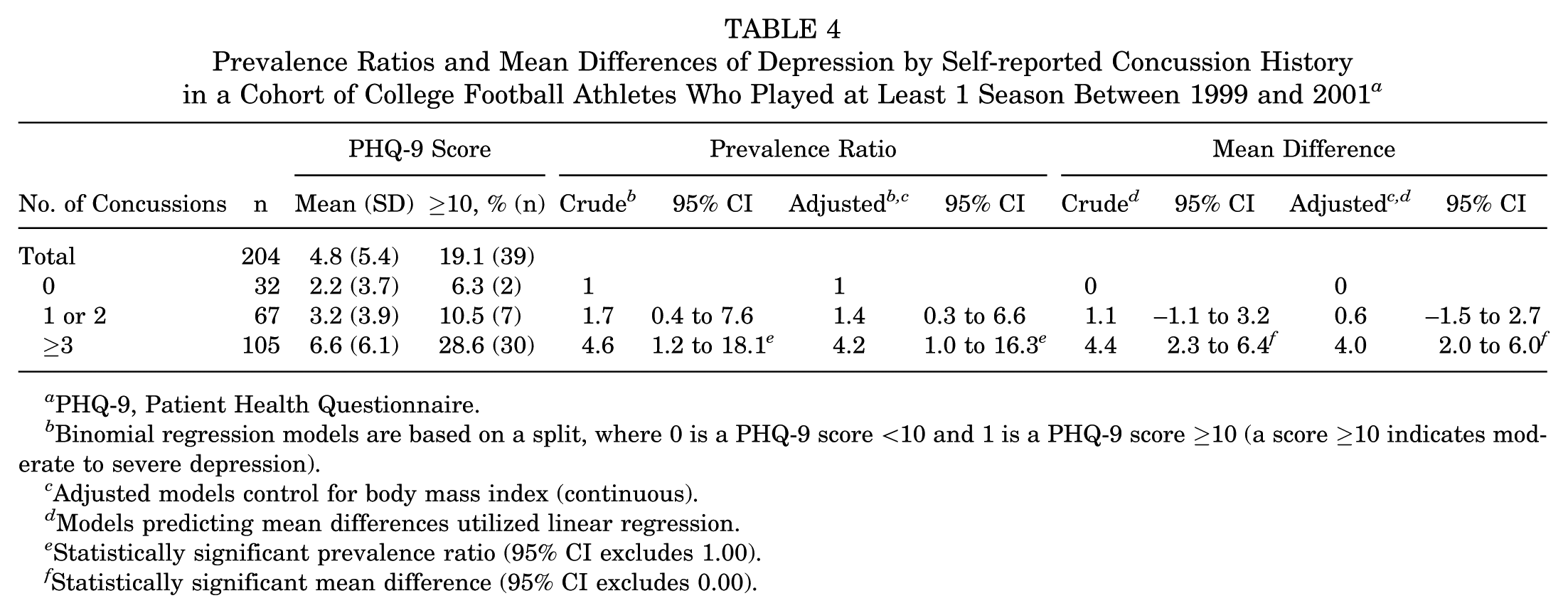
PHQ-9, Patient Health Questionnaire.
Binomial regression models are based on a split, where 0 is a PHQ-9 score <10 and 1 is a PHQ-9 score ≥10 (a score ≥10 indicates moderate to severe depression).
Adjusted models control for body mass index (continuous).
Models predicting mean differences utilized linear regression.
Statistically significant prevalence ratio (95% CI excludes 1.00).
Statistically significant mean difference (95% CI excludes 0.00).
Similar findings were also found in the linear regression models. Controlling for BMI, former college football athletes reporting ≥3 concussions in total had higher mean scores for the PHQ-9 than did former college football athletes reporting 0 concussions (MD = 4.0; 95% CI, 2.0-6.0) and 1 or 2 concussions (MD = 3.4; 95% CI, 1.9-5.0). Also, controlling for concussion history, for every 5-point increase in BMI, the PHQ-9 score increased 1.2 (95% CI, 0.4-1.9).
Alcohol Dependence
Overall, 24.8% (n = 49) produced CAGE scores ≥2 (indicative of alcohol dependence; Table 5). Although the proportion of former college football athletes with CAGE scores ≥2 was lowest among those reporting 0 concussions (16.1%, n = 5), statistically significant associations were not found between concussion history and alcohol dependence in binomial regression models. Forward model building yielded no covariates to include in final models.
Prevalence Ratios of Alcohol Dependence by Self-reported Concussion History in a Cohort of College Football Athletes Who Played at Least 1 Season Between 1999 and 2001 a
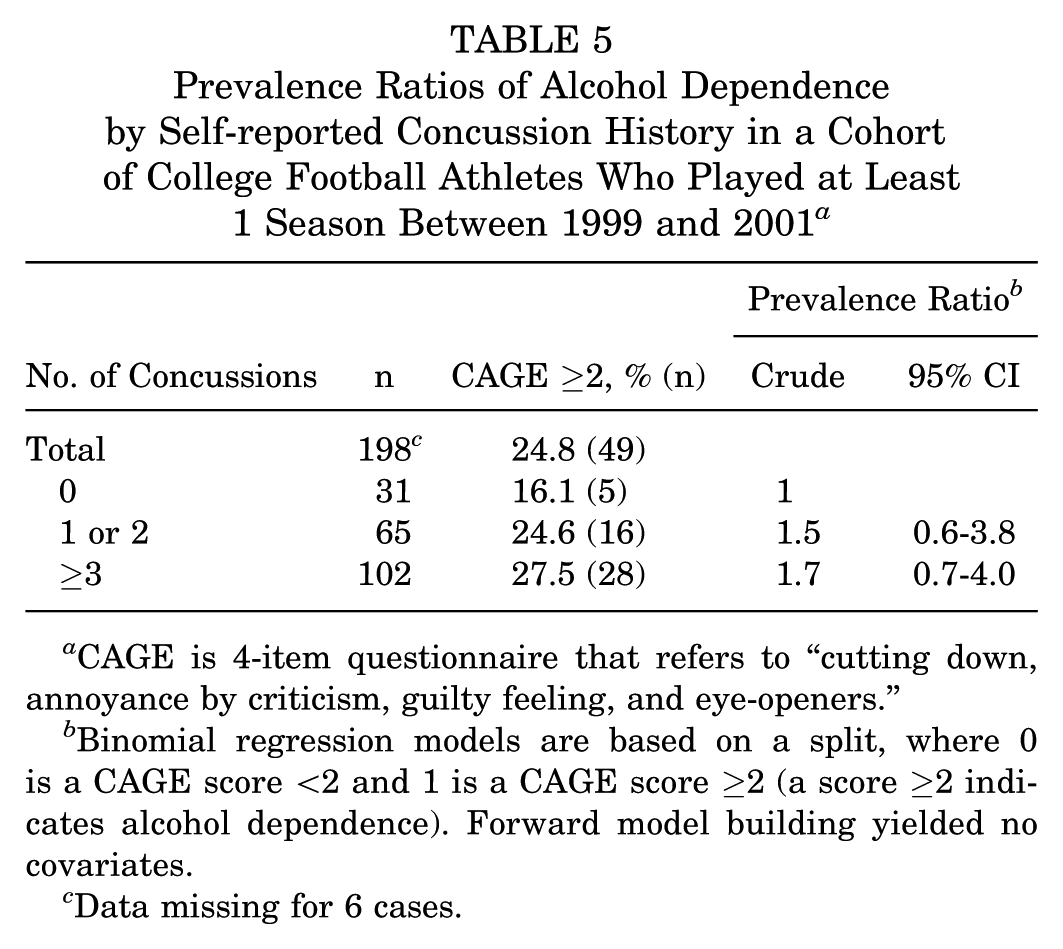
CAGE is 4-item questionnaire that refers to “cutting down, annoyance by criticism, guilty feeling, and eye-openers.”
Binomial regression models are based on a split, where 0 is a CAGE score <2 and 1 is a CAGE score ≥2 (a score ≥2 indicates alcohol dependence). Forward model building yielded no covariates.
Data missing for 6 cases.
Discussion
Our findings suggest a limited association between a history of multiple concussions and adverse physical and mental health outcomes among this sample of 204 former collegiate football players. Specifically, these significant associations were limited to those reporting a history of ≥3 concussions. These findings are important as they focus on NCAA players who played collegiate football and completed their sports careers as student-athletes approximately 15 years ago. In doing so, we were able to prospectively examine physical and mental health after football participation with a relatively young group of former collegiate athletes, while controlling for any preceding exposure. Although previous research suggested an association between concussion and adverse health outcomes— both short and long term5,12-14—such findings were generally gathered from older former professional football players. Thus, it is important to examine similar research questions among athletes whose at-risk exposure to contact and collision sports may have concluded at the amateur elite level (eg, college).
Concussion History and Health Outcomes
In our examination of the associations between concussion history and health outcomes—including general physical and mental health, depression, and alcohol dependence—we found mixed results. Differences by concussion history were found only for general mental health (ie, MCS) and depression (ie, PHQ-9). Furthermore, differences were statistically significant only for those self-reporting ≥3 concussions. Thefindings suggest a dose-response effect in which adverse outcomes are most associated with sustaining a higher number of concussions. In fact, athletes stratified into the ≥3-concussion group had a median of 5 prior concussions, making them even more distinct from the other groups. However, we caution interpretation, as findings comparing prevalence between 0 and 1-2 concussions, though trending in similar directions, may have been underpowered. We recommend continued research examining the dose-response association between concussion history and health outcomes, particularly to identify how multiple concussions may exacerbate the onset of such outcomes. More important, our findings continue to advocate the need for prevention strategies to mitigate the incidence of concussion and improve the diagnosis and management of a suspected concussion.
Despite these statistically significant findings, it is important to consider the MCID 18 —that is, the smallest difference that would be deemed important by clinicians. For the PCS and MCS, the MCID would range from 1 to 5 points.20,21,43-45 Thus, clinical evidence of a concussion history (1-2 or 3+) being associated with physical and mental health would be dependent on the MCID threshold chosen. The one exception is the MD between ≥3 and 0 concussions in the multivariable linear regression model (MD = −7.7), which is larger than all MCIDs. The MCIDs for PHQ-9 are less established, with 1 study suggesting a 5-point MCID based on a sample of older patients in primary care. 33 Despite our statistically significant findings for depression scores between those self-reporting 0 and ≥3 concussions, no MD reached the MCID. Overall, our findings, in conjunction with previous research,5-7,24 add to a body of evidence suggesting an association between history of multiple concussions and health outcomes, most evident in athletes with the highest number of prior concussions. However, our mixed results in relation to statistical significance versus clinical significance merit additional research.
Comparisons of Health Outcome Measures With Population Norms
The use of preestablished measures, such as the VR-36 and PHQ-9, allows for comparisons between our sample of former collegiate football players and a generalized US population (normative data for the CAGE are not available). Although PCS and MCS are standardized to a mean score of 50.0, more specific population scores are available by sex and age group. 47 As compared with US population norm scores for men aged 35 to 44 years, our sample’s PCS was slightly better (53.8 vs 53.0); however, its MCS score was worse (48.7 vs 50.4). 47 Also, our sample’s mean PHQ-9 score (4.8) and percentage with scores ≥10 (19.1%) were both higher than those reported from previous normative data (2.0-2.3 and 7.0%, respectively).29,30 Although these general comparisons between our sample and the US population may indicate worse current health for the former collegiate football players, it is important to note that these higher scores were attributable to former collegiate football players self-reporting concussions; those reporting 0 concussions had either a similar or better PCS (54.9), MCS (53.1), and PHQ-9 score (2.2; 6.3%).
Concussion Prevention
Currently, all 50 states and the District of Columbia have concussion-related legislation that oversees high school football, although specific content varies by state. 10 At the collegiate level, the NCAA Executive Committee adopted a new concussion policy in April 2010 mandating that each member institution’s concussion management plan include the following: annual concussion education for athletes, immediate removal from play if a concussion is suspected, elimination of same-day return to play of a concussed athlete, and a process for clearance for return to play by a medical professional.1,38 Furthermore, the NCAA, alongside certain college athletic conferences and various state high school associations, has enacted policies aimed at reducing head impact exposure through contact during preseason practice.6,7,19,39 Because the former collegiate athletes in this sample played well before such legislation and policies were enacted, it will be important to prospectively examine the effectiveness and implementation of such prevention strategies. Current concussion reporting appears to have increased since implementation of the NCAA concussion policy. 27 However, minimal change in players’ knowledge of concussion has been documented for other sports, such as ice hockey. 31
Additional Covariates of Interest
Aside from concussion, additional covariates of interest were found to be associated with health outcomes in our sample of former collegiate football players. First, BMI had a positive correlation with PHQ-9 and a negative correlation with PCS. Specifically, as BMI increased, the prevalence of having a PCS <50 and the prevalence of having moderate to severe depression scores increased. The relationship between an increased BMI and decreased general physical health is well established in the literature for adolescents, young adults, and older adults.17,46,48 In our sample of former collegiate football players, 91% were considered overweight or obese according to BMI; in the general US population, 64% are considered overweight or obese per BMI. 4 Not only does this unique population have an increased risk of sustaining a concussion, but it also has a higher prevalence of obesity, predisposing it to lower quality-of-life scores and other comorbidities (eg, diabetes, hypertension, heart disease, cancer).34,40 These comorbidities speak to the “snowball effect” that can arise with former athletes, as 1 medical condition can either lead to or exacerbate others. They furthermore contribute to worse physical and mental health outcomes, making it difficult to isolate the source of depression, which can be attributed to a variety of factors, including neurologic injury, musculoskeletal pain, inability to exercise regularly, and so on. Our results underscore the importance of studying these relationships to better understand how treatments may help mitigate depression among former athletes.
Finally, unlike previous research, 42 our study found no evidence suggesting that worse overall mental health outcomes are associated with an earlier age of starting participation in football. However, we did find evidence suggesting that a lower age at which one started playing football was associated with a lower PCS. To reach the MCID for the PCS,20,21 former collegiate football players would have to have started an additional 3 to 6 years earlier (eg, starting football in grade school as opposed to high school). We emphasize caution when interpreting this finding. Additional research postulated that the age of first playing football was not as relevant as the estimated cumulative amount of impact exposure. 37 Furthermore, the characteristics of youth football during the period in which our sample may have participated may be different from today’s climate, given the advent of preventive measures, including but not limited to those focused on player education, coaching education, and practice contact restriction guidelines.3,25,26 Continued prospective research is needed to gauge the benefits and risks of starting football participation at an early age.
Limitations
Our sample is smaller than that of previous studies utilizing former athletes.5,12-14 However, to control for potential confounding owing to postcollegiate sports at-risk exposure or playing era, we chose to restrict our sample to those collegiate football players who had played and were prospectively enrolled in the original NCAA Concussion Study during the 1999-2001 college football seasons and who never played professionally. This restriction aimed to maximize the internal validity of our study, but it consequently affected the external validity in that our findings may not be generalizable to other former athletes. In addition, the approximate 15-year follow-up may not be sufficient to allow for the development of certain adverse health outcomes, such as Alzheimer disease and other neurologic issues seen at advanced ages. Longitudinal follow-up studies are warranted. This study also utilized survey research; brain studies—particularly those that examine participants with varying levels of football exposure, health outcomes, and comorbidities—may further contribute to the literature base. As in any survey study, there is the possibility of ascertainment bias (eg, those experiencing physical or mental symptoms may have been more likely to respond to the survey, while those experiencing no such difficulties were less likely to respond). In addition, we used nonrandom sampling of athletes, and only 23.4% of eligible athletes responded to the survey. Thus, the possibility of ascertainment bias and respondent bias exists, and findings should thus be interpreted with some caution. Furthermore, generalizability may be further affected given that concussion diagnosis and management are likely to differ today as compared with when our sample played football. Finally, as our study used self-administered questionnaires, bias typical of survey research may be present (eg, respondent bias, recall bias). Nevertheless, our study contributes to the growing body of literature on this important topic.
Conclusion
Our study found modest evidence of an association between history of ≥3 concussions and mental health outcomes in a sample of 204 former collegiate football players. The findings underscore the need for prevention efforts to reduce the incidence of concussion, as well as efforts to support former athletes who may experience such adverse effects. Continued research is needed, however, to further demonstrate the clinical meaningfulness of reported differences in health outcomes associated with concussion history. To that end, the rich cohort of athletes from the NCAA Concussion Study should continue to be followed through additional prospective studies to better understand the development and progression of long-range neurologic health problems across the life span.
Footnotes
Acknowledgements
The authors thank the research staff who assisted in this project, including Amy Nader, Robyn Furger, and Jennifer Hill.
The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research was funded in part by a grant from the National Collegiate Athletic Association’s Sport Science Institute, in which K.M.G. and M.M. served as co–principal investigators.