
Abstract
Background:
Meniscal lesions represent one of the most common intra-articular knee injuries. Meniscus replacement devices are needed to restore load distribution and knee stability after meniscectomy. Fixation of these devices is crucial to the generation of hoop stresses and the distribution of loads in the joint.
Purpose:
To evaluate 2 different fixation techniques (suture endobutton and interference screw) for implantation of a novel meniscus device.
Study Design:
Controlled laboratory study.
Methods:
In 7 human cadaveric knees (aged 17-61 years), 1 anterior and 2 potential posterior tunnel locations were investigated, and both fixation techniques were tested in each tunnel. The native meniscus roots, devices fixed with a suture endobutton, and devices fixed with an interference screw were gripped with cryoclamps, and tibias were drilled and loaded into a custom jig. Samples were preloaded, preconditioned, loaded for 500 cycles (50-150 N), and tested in tension until failure.
Results:
For all 3 tunnels, suture fixation resulted in greater elongation (54.1%-150.7% greater; P < .05) during cyclic loading than interference screw fixation, which approximated the native roots. Both fixation techniques displayed ultimate tensile loads in the same range as native roots. However, stiffness of the suture fixation groups (36.5-41.6 N/mm) was only 28% to 37% of that of the interference screw fixation groups (98.7-131.6 N/mm), which had values approaching those of the native roots (anterior: 175.4 ± 24.2 N/mm; posterior: 157.6 ± 22.9 N/mm).
Conclusion:
Interference screw fixation was found to be superior to suture fixation with regard to elongation and stiffness, a finding that should be considered in the design and implantation of novel meniscus replacement devices.
Clinical Relevance:
With the emergence of various devices for total meniscus replacement, the establishment of fixation strategies is crucial for the generation of tensile hoop stresses and the efficacy of these approaches.
Meniscal injuries occur in over 1 million people in the United States annually. The resulting meniscectomies alleviate short-term symptoms, 32 but there is significant evidence linking the amount of tissue removed to long-term joint deterioration, causing patients pain and discomfort.5,46 Current options for meniscus replacement include allograft transplantation17,27 and synthetic augmentation (ie, Collagen Meniscus Implant37,41 and Actifit 18 ), but both have shown long-term inconsistency with regard to functional outcomes.8,9,15,20 Novel medical devices are required to fill this void in the treatment of meniscal injuries.
The menisci are semilunar fibrocartilaginous discs attached to the tibial plateau via anterior and posterior meniscotibial ligaments, also known as meniscus roots. These roots are integral to transmitting circumferential hoop stresses to the bone, preventing meniscus extrusion during loading. 16 Improper load transmission and extrusion result in reduced joint stability and increased stresses on the articular surface.4,39 Thus, total meniscus replacement devices must not only re-create the properties of the meniscus body but also achieve adequate anchorage for hoop stress generation. Therefore, fixation is crucial to device function and efficacy. While meniscus roots have been mechanically characterized, 12 the fixation properties of replacement devices have yet to be investigated.
Of the total meniscus replacement devices tested in large animal models, the majority are fixed through transosseous tunnels with sutures.11,23,44 This technique involves augmenting the anterior and posterior horns of the device with sutures, pulling them through the tunnels, and fixing them distally by tying a knot or tying over an endobutton. Unfortunately, many of these studies have resulted in device extrusion or ruptures. A potential alternative is interference screw fixation.21,30 This method is frequently used during anterior cruciate ligament (ACL) reconstruction, providing frictional interference by compressing the graft against the bone tunnel. If meniscus devices can be augmented with tails,28,47 they can be fixed similarly to prevent extrusion.
Previous success has been achieved using fiber-reinforced scaffolds for total meniscus reconstruction. 6 The implants were fixed via interference screws and showed success in an ovine model for up to 1 year.28,34 The goal of this study was to evaluate the fixation mechanics of this device in a human cadaveric knee model. We hypothesized that interference screw fixation would provide superior mechanics to suture fixation in response to both dynamic and ultimate tensile stresses. The results of this study serve as a template for comparable meniscus devices, giving great insight into adjustments that may need to be made to device design and implantation.
Methods
This study aimed to characterize the mechanical properties of fixation techniques for a novel total meniscus replacement device (Meniscofix; NovoPedics). Based on the architecture of the tibial plateau and direction of the meniscus roots, 1 anterior tunnel location and 2 potential posterior tunnel locations were identified. This study first tested the mechanics of the native anterior and posterior roots, followed by both suture and screw fixation mechanics for each of the 3 tunnels. Testing of the existing meniscus roots (native roots) was performed to determine benchmarks for adequate fixation. To conserve both polymer fiber and time, device tails were fabricated rather than entire implants (Figure 1A). Tails were fabricated and tested in 7 human cadaveric knees. Both cyclic and ultimate tensile properties were evaluated.
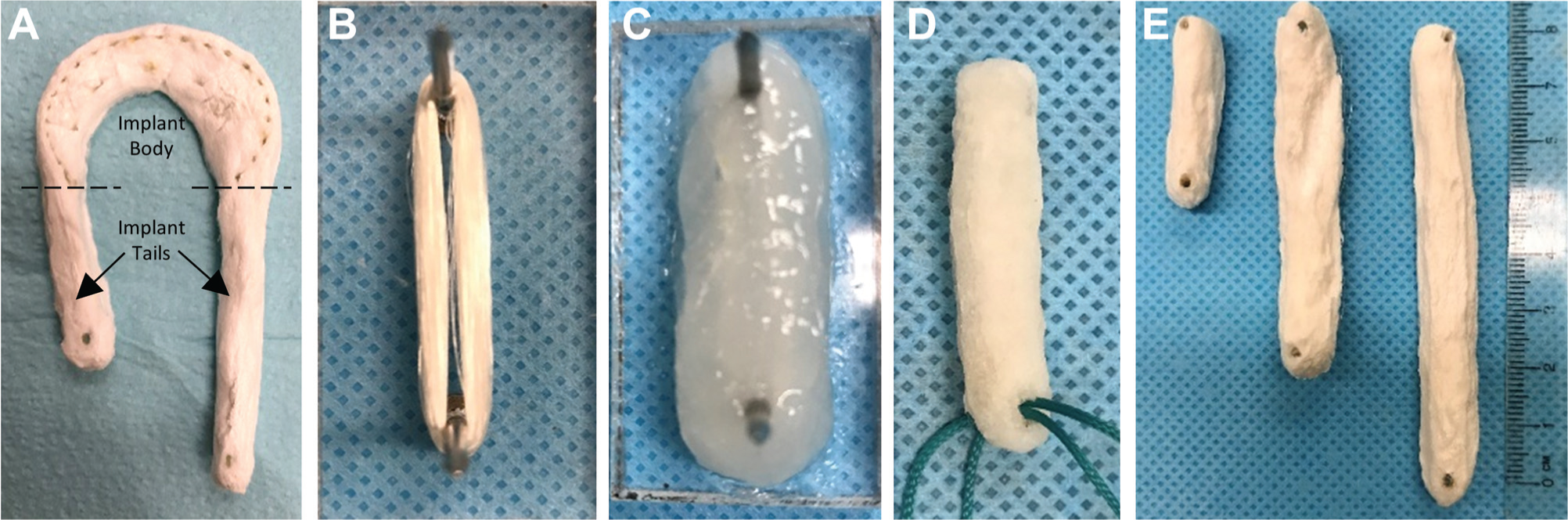
Tail fabrication. (A) Fiber-reinforced meniscus scaffold, Meniscofix, with implant body and tails. (B) Polymer fiber (p(DTD DD)) woven around 2 pins with 660 fibers per cross section. (C) Fiber injected with collagen-hyaluronan dispersion. (D) Final tail after cross-linking and sterilization, with double-bundle suture. (E) Samples of short (30 mm), intermediate (60 mm), and long (80 mm) tails.
Tail Fabrication
Three different tail sizes were fabricated for testing: short (30 mm), intermediate (60 mm), and long (80 mm). Short tails were used for suture fixation in all 3 tunnels (n = 3 × 7 knees = 21 tails), intermediate tails were used for anterior interference screw fixation (n = 1 × 7 knees = 7 tails), and long tails were used for posterior interference screw fixation (n = 2 × 7 knees = 14 tails). In this study, we used poly(desaminotyrosyl-tyrosine dodecyl ester dodecanoate) (p(DTD DD)) fiber, similar to previous in vivo work.28,34 The p(DTD DD) was polymerized into pellets, melt-extruded, and drawn into 100-µm filaments at the New Jersey Center for Biomaterials. Fiber was woven (Figure 1B) around a set of 2 pins spaced 30, 60, or 80 mm apart to create 660 fibers per cross section. A collagen-hyaluronan dispersion (20 g/L–0.25 g/L in dilute HCl; pH 2.35) was injected into and around the woven fibers (Figure 1C), frozen via an ethanol–dry ice bath for 30 minutes, and lyophilized for 24 hours (–50°C; 0.05 mbar). Tails were cross-linked for 6 hours in 1-ethyl-3-(dimethylaminopropyl)carbodiimide (EDC; 10 mM) and N-hydroxysuccinimide (NHS; 5 mM) solution and subjected to three 10-minute DI H2O rinses, a 2-hour sodium phosphate wash (Na2HPO4; 100 mM), and a 24-hour DI H2O rinse. Tails were frozen and lyophilized again (Figure 1D) and gamma-irradiated at 25 kGy (Sterigenics) to yield 1 of 3 tail lengths (Figure 1E). Tails were weighed before and after weaving, and after sterilization, to quantify the polymer weight percentage. Tails were also measured for length, height, and width using vernier calipers.
Testing Preparation
Seven left human cadaveric tibias with attached medial menisci were obtained from the Musculoskeletal Transplant Foundation, with a mean age of 48.9 years (range, 17-61 years) and no preexisting knee injury. Studies were performed under an approved biosafety protocol from Rutgers Environmental Health & Safety. Tibias were dissected of all soft tissue except the medial meniscus. A radial cut was made in the body region of the meniscus, creating anterior and posterior segments for testing. After mechanical testing (detailed later) of native meniscus roots, three 6-mm bone tunnels were drilled: anterior, posterior medial, and posterior lateral. The anterior tunnel was drilled at the anterior root location, down into the tibia 30 mm (Figure 2A). This anterior tunnel was chosen because of easy access through the small medial arthrotomy site that is typically created for implant or allograft insertion. A 2.5-mm guide hole was then drilled 30 mm from the tibial plateau, perpendicular to the anterior tunnel, for suture retrieval. The posterior medial tunnel was drilled by placing the tip of an aiming guide (45°) at the posterior root location, with the tunnel exit 30 mm below the medial tibial plateau (Figure 2B), similar to ACL fixation. The posterior medial exit hole avoided any major musculature, vasculature, or innervation. The posterior lateral tunnel was similarly drilled with the tunnel exit on the lateral tibial shaft (Figure 2C), which could be accessed through a small incision in the tibialis anterior muscle. In the event that native root testing compromised bone quality, tunnels were drilled slightly lateral to the original root locations.
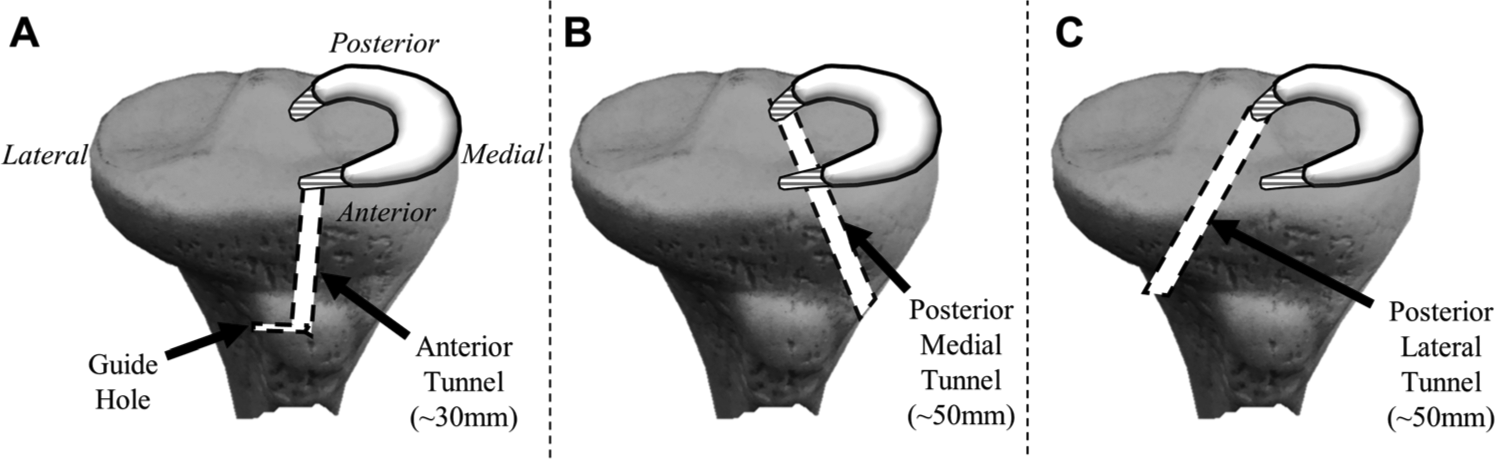
Tunnel locations. (A) Anterior tunnel drilled (6 mm) from root attachment into tibia approximately 30 mm, followed by guide hole drilling for suture/tail retrieval. (B) Posterior medial tunnel (~50 mm) and (C) posterior lateral tunnel (~50 mm) as 2 potential posterior tunnel locations.
Fixation Technique
For suture fixation in each tunnel, a short tail (30 mm) was augmented with a double bundle of braided polyester suture (No. 5 Ethibond; Ethicon), similar to previous meniscus and ligament studies.7,40,45 The double bundle (4 suture strands) was passed through the tunnel, leaving the 30-mm tail segment outside of the proximal end of the tunnel to allow for gripping. Strands were tied over a metal endobutton 29 (Endobutton Direct; Smith & Nephew) at the distal end of the tunnel with 10 throws (Figure 3A) to ensure that knots were not the source of failure. For anterior interference screw fixation, an intermediate tail (60 mm) was augmented with 2-0 suture to aid in tail “implantation” and fed through the anterior tunnel and guide hole. Approximately 30 mm of tail was placed into the tunnel, leaving the remaining 30 mm proximal to the tunnel for gripping with freeze clamps. The tail was then fixed via a titanium interference screw (7 × 25 mm, REF 013454; Smith & Nephew) from the proximal end of the tunnel in an anterograde fashion (Figure 3B). The aiding suture at the distal end of the tunnel was removed through the guide hole. For posterior interference screw fixation (both medial and lateral), a long tail (80 mm) was augmented with suture and pulled through the posterior tunnel, with approximately 50 mm within the tunnel and 30 mm outside for gripping. The tail was fixed in the tunnel via an interference screw from the distal end of the tunnel in a retrograde fashion (Figure 3C), and the aiding suture was removed. Anterograde screw fixation was chosen for the anterior tunnel because of the angle between the tunnel and tibial cortex, leaving little cortex for a retrograde approach. Retrograde screw fixation was chosen for both posterior tunnels because of difficult access to the posterior root for screw insertion. All fixation procedures were performed by the same orthopaedic surgeon to limit variability.
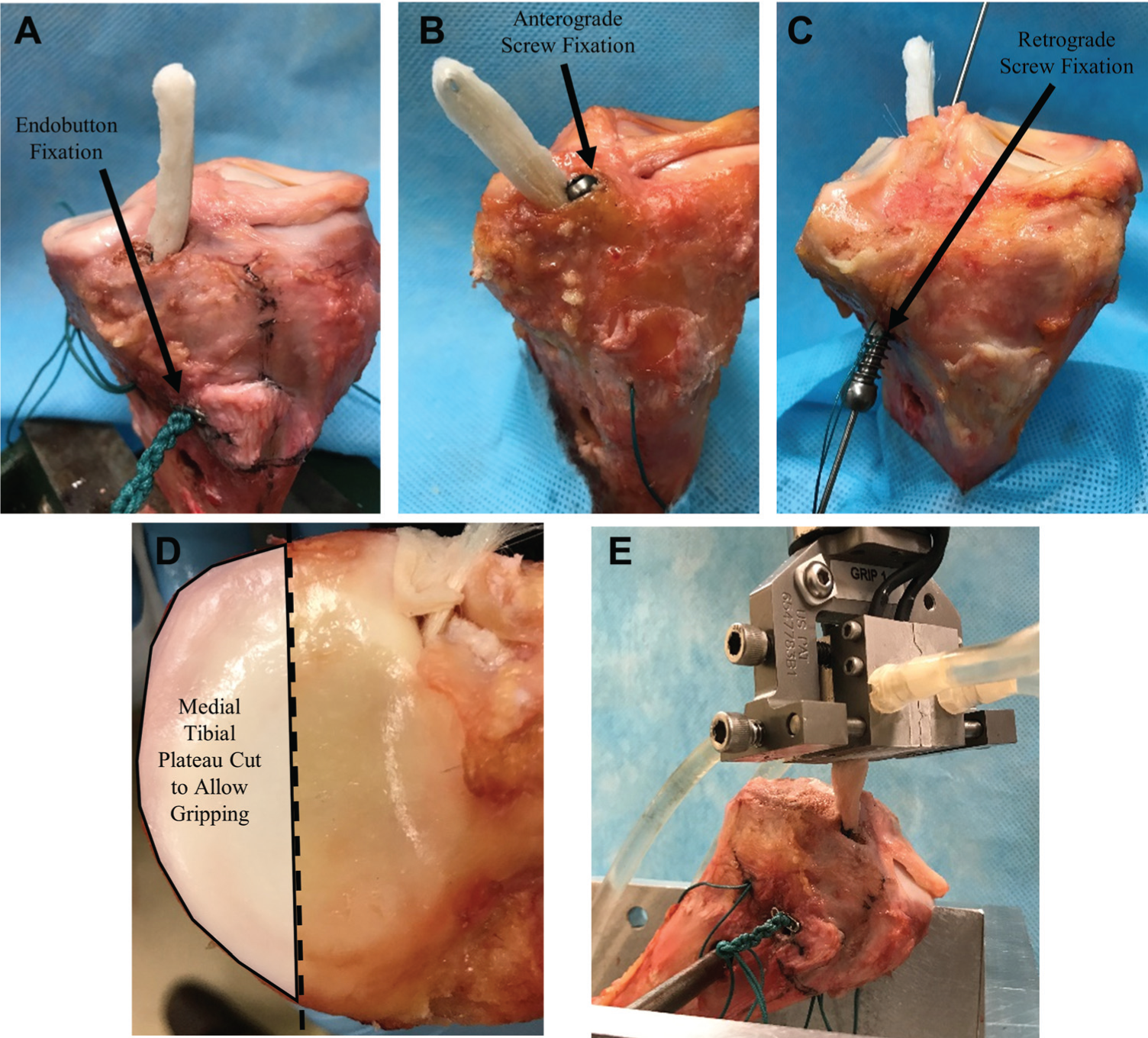
Fixation techniques and testing setup. (A) Tail fixed through tunnel using braided suture and tied over endobutton with 10 knots. (B) Tail pulled through anterior tunnel and fixed via interference screw in an anterograde fashion. (C) Tail pulled through posterior tunnel (either medial or lateral) and fixed via interference screw in a retrograde fashion. (D) Tibial plateau cut approximately 10 mm from roots to allow for gripping. (E) Tibia loaded into custom Instron jig at approximately 45°, and sample (native meniscus or tail) gripped with ElectroForce cryoclamps.
Tensile Testing
Tensile testing was performed by placing the tibias into a custom Instron apparatus. To do so, a 9-mm anterior-posterior hole was drilled perpendicular to the tibial shaft approximately 50 mm below the tibial plateau to not interfere with any of the fixation tunnels. The medial tibial plateau was also cut approximately 10 mm from the meniscus roots to allow for gripping (Figure 3D). Tibias were then loaded into the custom jig and fixed into position at approximately 45° (Figure 3E) to simulate the direction of meniscus extrusion while simultaneously allowing for adequate gripping. Samples (native meniscus or tail) were gripped with cryoclamps (ElectroForce; TA Instruments) approximately 10 mm from the bony insertion. All samples were hydrated for at least 10 minutes before testing and hydrated repeatedly throughout testing. Samples were preloaded to 5 N and preconditioned (10 cycles of 10-50 N at 30 mm/min). 12 Cyclic testing was performed based on previous ACL fixation studies,13,21,42,43 which were performed to approximately 25% of the native ACL’s ultimate tensile load. Thus, with an ultimate tensile load of approximately 600 N for the native meniscus roots, 12 cyclic testing was performed from 50 to 150 N for 500 cycles at 50 mm/min to obtain a frequency of approximately 0.5 Hz. 33 After the 500 cycles, samples were tested in tension until failure at 30 mm/min, mimicking a meniscus root study by Ellman et al. 12 The mode of failure was recorded for native roots (rupture in meniscus body, rupture at root, rupture in bone), suture fixation (tail broke at suture, suture broke at tail, suture broke at endobutton, bone cut to failure), and interference screw fixation (tail broke outside tunnel, tail broke at screw, tail slipped from tunnel). Cyclic elongation was calculated as the difference in extension between the end of the 1st cycle and the end of the 500th cycle. From the ultimate tensile test, ultimate tensile load and stiffness were obtained. Seven No. 5 Ethibond sutures (double-bundle) and 7 short tails were also tested under cyclic and ultimate conditions to serve as baseline material values.
Statistical Analysis
The 3 parameters (cyclic elongation, ultimate tensile load, stiffness) were compared between the 3 anterior groups and between the 5 posterior groups using repeated-measures analysis of variance with post hoc Bonferroni adjustment (multiplication of P values by the number of comparisons). P values <.05 and <.001 were considered significant and highly significant, respectively. All statistical analyses were performed with Stata 14 software (StataCorp).
Results
Tail Fabrication
Tails were produced with consistency with regard to weight and dimensions (Table 1), with a polymer weight percentage of approximately 80% to 85% and a cross-sectional area of approximately 45 to 50 mm2.
Tail Properties a
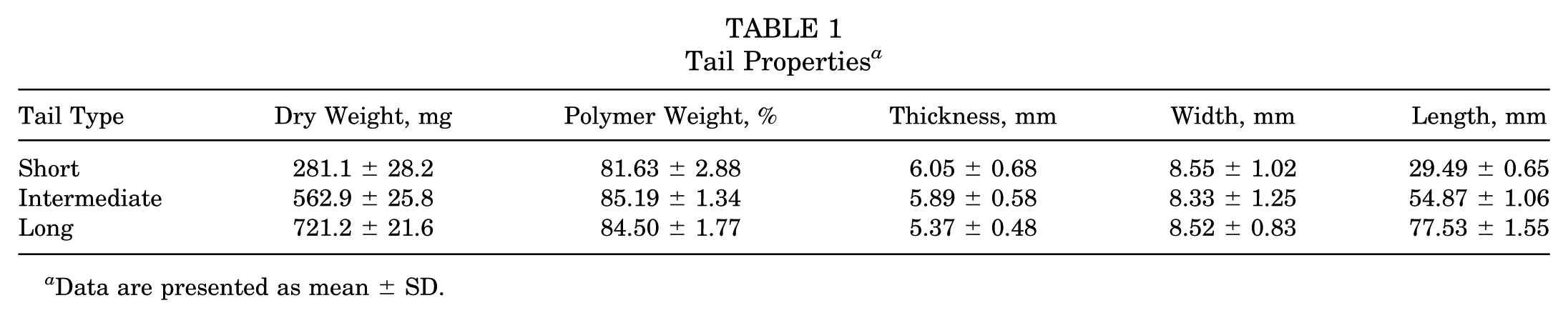
Data are presented as mean ± SD.
Mode of Failure
No samples slipped from the cryoclamps. One native posterior root sample was removed because of a radial incision in the posterior horn during dissection, and 1 anterior screw fixation sample was removed because of catastrophic bone failure during native testing. Six of 7 native anterior root samples broke within the bone, and 1 broke in the ligamentous attachment region. All 6 native posterior root samples broke in the ligamentous attachment. Of the 21 suture fixation samples (7 knees × 3 tunnels), 8 resulted in a suture rupture at the suture endobutton interface, 11 resulted in a suture or tail rupture at the suture-tail interface, and 2 failed because of the suture’s cutting through the bone (“bone cutting”). Overall, suture fixation led to consistent bone cutting or failure, ranging from 2 mm to complete cutting between the proximal and distal ends of the tunnel (~30 mm) (Figure 4). Of the 6 anterior screw samples (1 excluded), 5 slipped from the tunnel, and 1 resulted in tail failure at the screw-tail interface. Of the 14 posterior screw samples (7 knees × 2 tunnels), 6 slipped from the tunnel, and 7 resulted in a tail rupture at the screw-tail interface. Overall, 5 of 20 (6 anterior, 14 posterior) of the screw fixation samples exhibited some polymer fiber rupture before testing. The failure modes of each group are shown in Table 2.
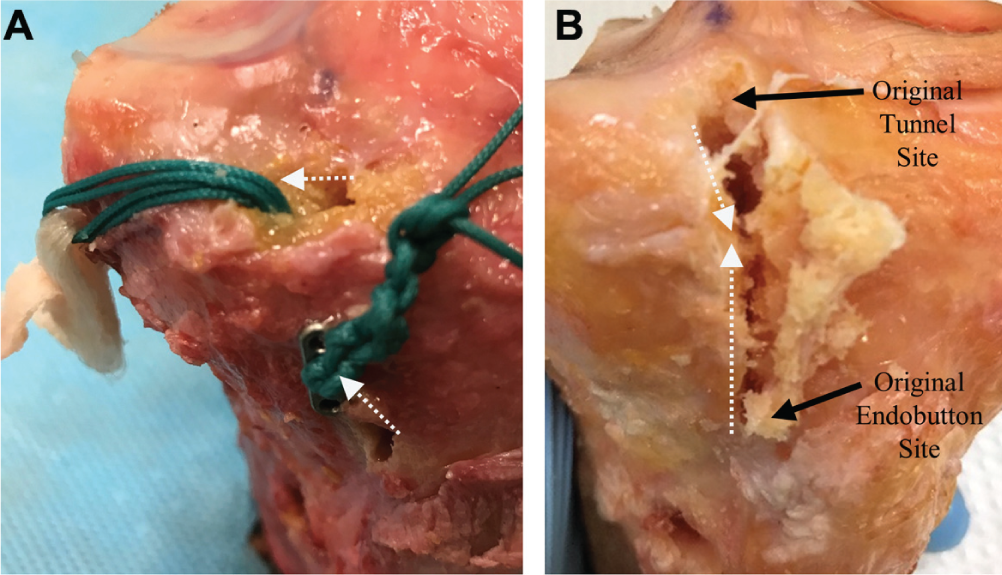
Bone cutting in suture fixation group. (A) Intermediate bone cutting (~5 mm) and (B) severe bone cutting (~30 mm). White dotted arrows indicate cutting.
Fixation Failure Modes a
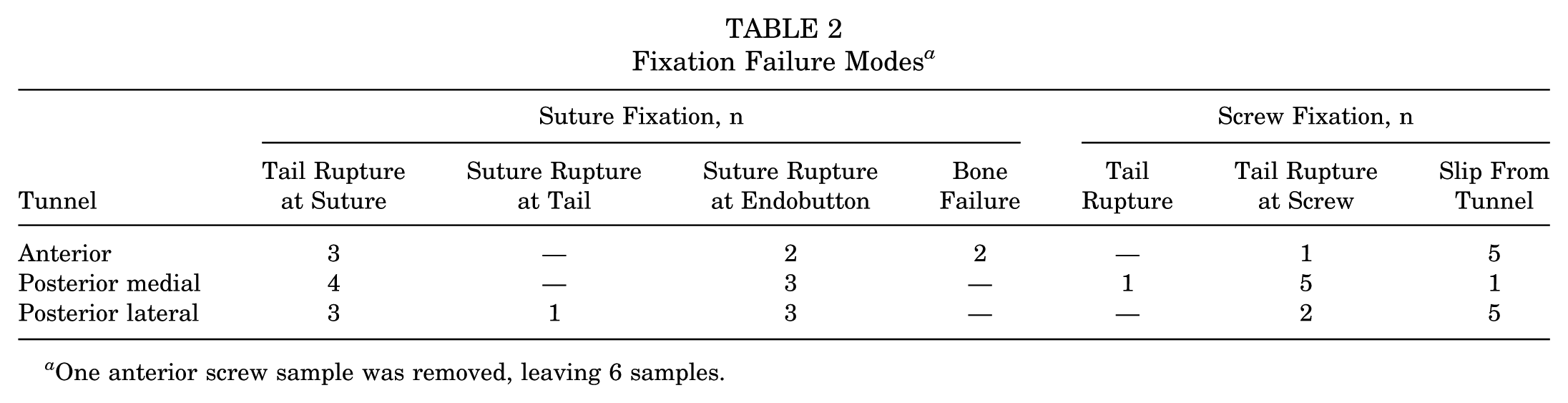
One anterior screw sample was removed, leaving 6 samples.
Cyclic Elongation
Elongation during cycling loading (Figure 5) was 403% greater (P < .001) for anterior suture fixation than for the native anterior root and 2.5 times greater than that of anterior interference screw fixation. Similarly, both posterior suture fixation groups exhibited significantly greater (P = .002 and P = .001) elongation than their respective screw fixation groups. Posterior medial screw fixation displayed the best elongation, only 36.5% greater than that of the native posterior root, whereas posterior medial suture fixation exhibited 115.4% greater elongation than the native posterior root. Sutures alone experienced elongation (1.39 ± 0.27 mm) similar to the suture fixation groups, while tails alone experienced elongation of only 0.20 ± 0.05 mm.
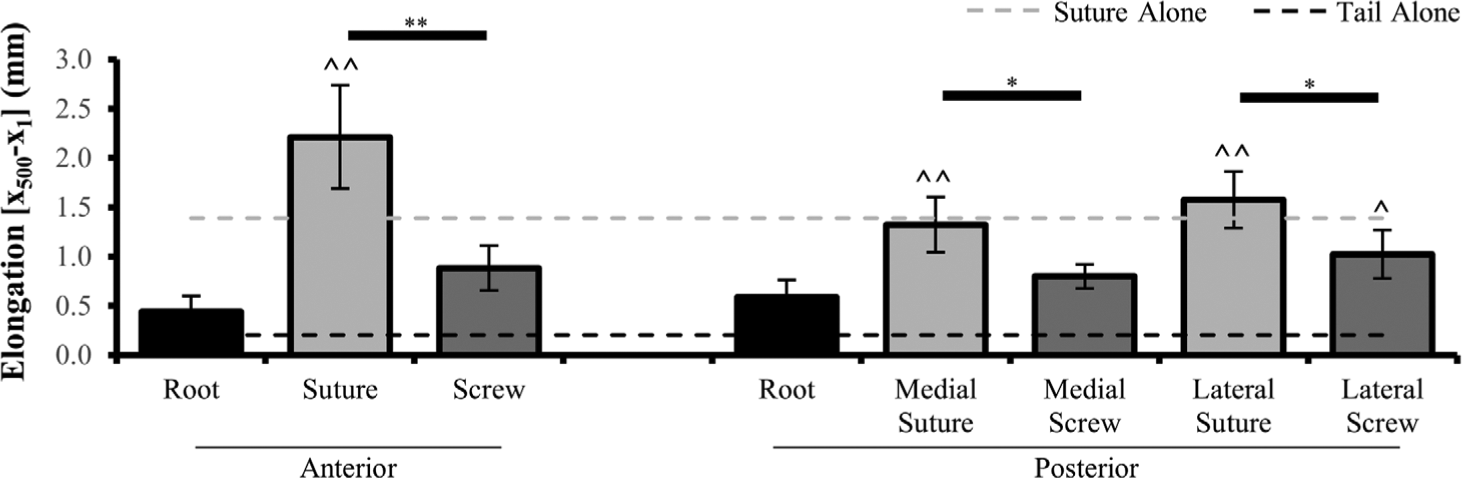
Cyclic elongation values (x500 – x1) of native roots and of suture and screw fixation of 3 tunnels. n = 6 for posterior root and anterior screw groups; n = 7 for all other groups. Values are presented as mean ± SD. *Statistically significant (P < .05) and **highly statistically significant (P < .001) differences. ^Statistically significant (P < .05) and ^^highly statistically significant (P < .001) differences from native root values. Grey dashed line represents average for sutures alone. Black dashed line represents average for tails alone.
Ultimate Tensile Load
In the anterior groups, suture fixation and screw fixation exhibited comparable ultimate tensile loads (P = .553), but these loads were significantly lower than that of the native anterior root. On the other hand, all posterior fixation groups, except posterior lateral screw fixation, were comparable with the native posterior root. Posterior medial screw fixation exhibited the greatest ultimate tensile load and was 2.5% greater than the native root. Posterior medial and posterior lateral suture fixation resulted in ultimate loads comparable (9.6% and 6.1% greater, respectively) with that achieved during testing of the suture alone. Representative load-extension curves and ultimate tensile load values are shown in Figures 6A and 6B, respectively.
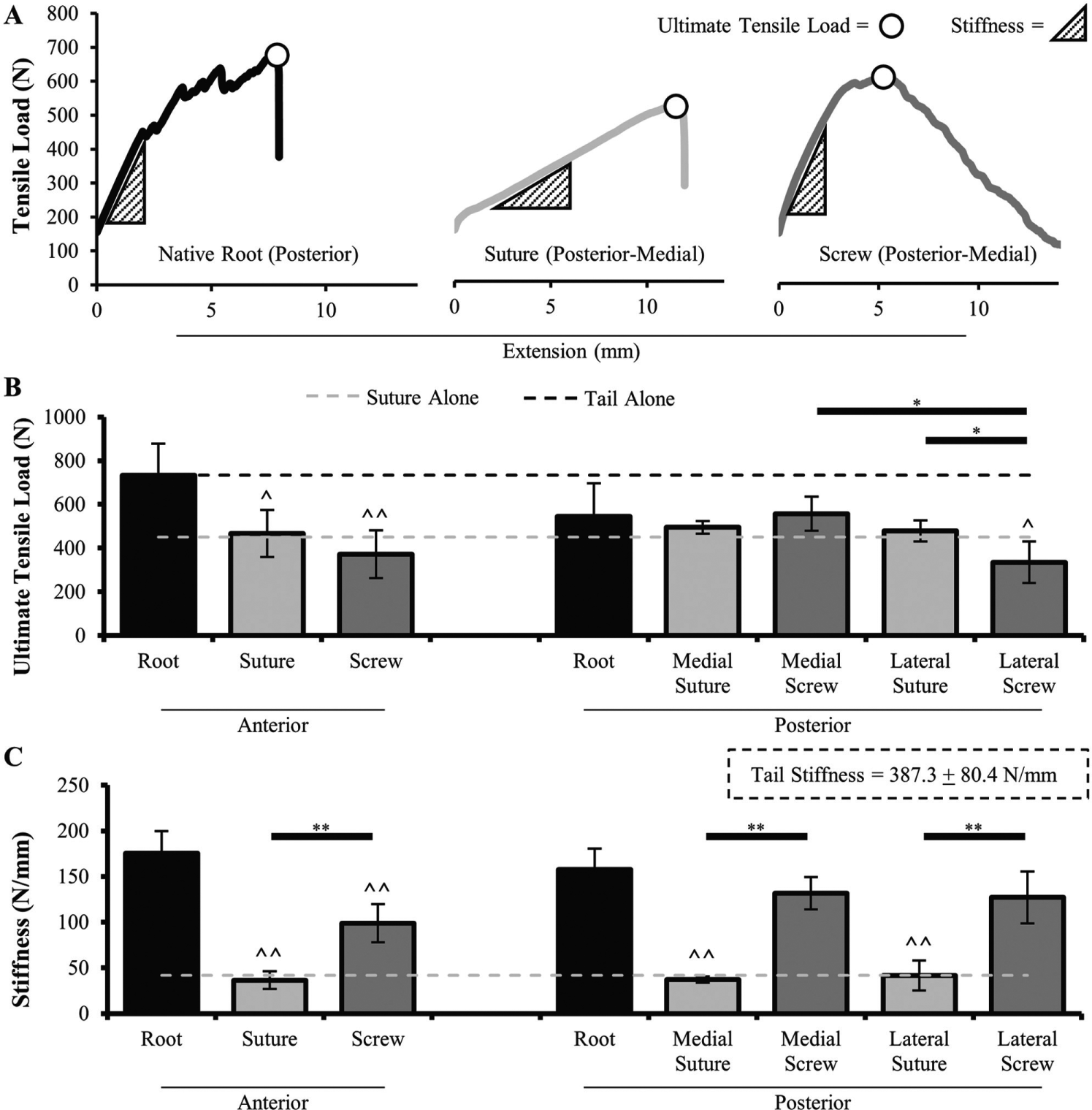
Ultimate fixation properties. (A) Representative load-extension curves of native root, suture fixation, and screw fixation groups. Circle represents ultimate tensile load. Triangle represents stiffness (slope). (B) Ultimate tensile load and (C) stiffness values during ultimate tensile test. n = 6 for posterior root and anterior screw groups; n = 7 for all other groups. Values are presented as mean ± SD. *Statistically significant (P < .05) and **highly statistically significant (P < .001) differences. ^Statistically significant (P < .05) and ^^highly statistically significant (P < .001) differences from native root values. Grey dashed line represents average for sutures alone. Black dashed line represents average for tails alone.
Stiffness
Stiffness values (Figure 6C) in the screw fixation groups were noticeably greater (170.7%-253.0% greater) than their suture fixation counterparts. While anterior screw fixation stiffness was significantly less than the native anterior root stiffness, it was 2.7 times the value of the suture fixation group. Similar results were observed in the posterior region, except posterior medial and posterior lateral screw fixation were 83.5% and 80.6% as stiff as the native posterior root (P = .233 and .086, respectively). All 3 suture fixation groups exhibited little variation (0.1%-12.5% less) in stiffness from the suture alone.
Discussion
Several tissue-engineered meniscus replacement devices are currently under investigation in the preclinical or clinical stages. Integral to the function of these devices is their surgical fixation to properly generate hoop stresses and distribute loads in the joint. While a variety of materials, cells, and growth factors have been considered,23,24,26,35,44 little attention has been given to achieving adequate fixation. The current study presents, to our knowledge, the first investigation of the fixation properties of a total meniscus replacement device. Suture endobutton and interference screw fixation were chosen because of their high rate of usage in both preclinical meniscal studies and clinical ACL studies. Moreover, both techniques are relatively easy to implement arthroscopically. In this study, interference screw fixation was shown to be superior to suture endobutton fixation, confirming our hypothesis. Specifically, interference screw fixation resulted in less elongation and greater stiffness and was relatively comparable with native meniscus roots. These findings should be considered in the design and implantation of meniscus replacement devices.
Meniscus root properties have previously been characterized, similarly finding that the native anterior root had greater ultimate tensile properties than the posterior root. 12 However, to date, this is the first study to characterize the cyclic elongation properties of human meniscus roots. During cyclic loading, the anterior and posterior native roots in the present study experienced elongation of only 0.44 and 0.59 mm, respectively. This low degree of elongation minimizes extrusion and allows the meniscus to maintain its load-distributing properties and protect the knee from cartilage damage. 36 For example, for meniscus allograft transplantation, a greater degree of extrusion with suture fixation than bone plug fixation1,3 resulted in increased peak contact stresses. 45
In our study, interference screw fixation (0.90 mm) displayed significantly better elongation (39.9%-64.9%) than suture endobutton fixation. These findings were consistent with an ACL fixation study in porcine knees 42 in which interference screw fixation (5.5 ± 1.7 mm) experienced elongation that was 53.4% that of suture fixation (10.3 ± 1.6 mm). Moreover, Ezechieli et al 14 reported comparable results in cadaveric knees, showing that antegrade screw fixation (0.84 ± 0.15 mm) yielded significantly better elongation than FiberWire suture (1.14 ± 0.90 mm). Much of the elongation of the suture groups can be attributed to elongation of the suture itself (1.39 mm) and to the cutting of bone (Figure 4). Previous studies have also shown that sutures can cut through both bone 22 and soft tissue,10,25 increasing the incidence of extrusion and ruptures. On the other hand, extended device tails do not elongate nearly as much and do not cause any failure of the bone. Clinically, increased elongation would lead to scaffold extrusion, ultimately reducing the load-bearing efficacy of implants fixed with the suture endobutton technique.
These elongation results are most likely explained by the increased stiffness of the interference screw fixation groups. With tails alone exhibiting considerably higher stiffness, the measured fixation stiffness was primarily related to the frictional interference created by the screw. While the anterior screw exhibited significantly lower stiffness than the native anterior root, both posterior medial and posterior lateral screw fixation were comparable with the native posterior root. The interference screw fixation groups exhibited stiffness values that were 170.8% to 253.0% greater than their respective suture fixation groups (mean, 38.5 N/mm). The stiffness of these suture fixation groups was almost identical to the suture alone and comparable with that achieved with transtibial suture repair of porcine posterior meniscal tears (44.8 ± 9.9 N/mm). 38 While this stiffness was adequate for the porcine meniscus (mean, 53.7 ± 6.5 N/mm), it was only 20.8% to 26.4% that of the native human meniscus roots in our study. Thus, the combination of decreased cyclic elongation and increased stiffness of interference screw fixation over suture fixation would limit extrusion and provide superior contact stress mechanics.
With these 2 superior mechanical properties, the only potential mechanical drawback of the interference screw group would be slipping of the tail, leading to a low ultimate tensile load. The anterior and posterior medial interference screw groups were statistically similar to their suture fixation counterparts, showing comparable values and trends to ACL fixation (screw: 311.7 ± 120.3 N; suture: 367.0 ± 115.8 N). 14 The posterior lateral interference screw group in this study did display a notably lower ultimate tensile load (40.0% less than posterior medial interference screw fixation), which is likely attributed to the difference in bone mass density between the medial and lateral tibial condyles. Akamatsu et al 2 showed that the medial tibial condyle density (0.954 gm/cm2) was more than 50% greater than the lateral tibial condyle density (0.631 gm/cm2), allowing for the titanium screw to create greater interference against a tougher bone. Moreover, the posterior lateral tunnel is much more likely to disrupt musculature and innervation than the posterior medial tunnel. Therefore, both medial and lateral meniscus replacement devices should aim to use bone tunnels through the medial condyle rather than the lateral. However, tunnel placement will need to be carefully considered during concomitant ACL transplantation procedures, as additional tunnels in proximity may compromise bone quality.
The majority of previous in vivo meniscus replacement studies have exhibited some degree of failure, typically resulting in extrusion and/or ruptures.19,23,24 Much of this can be attributed to the method of fixation, most commonly transtibial suture fixation, either on the tibial cortex or over endobuttons. While too rigid of a fixation technique can lead to implant ruptures, 19 one that is not stiff enough can lead to extrusion and increase stresses on the articular surface. Herein, we showed elongation and stiffness properties that are relatively comparable with, but do not surpass, native human meniscus roots using interference screw fixation. Moreover, the use of elongated tails within tibial bone tunnels allows for bony ingrowth into the tails, 34 further enhancing fixation with time.
The present study did have limitations. First, only one type of suture (braided polyester) was investigated, as it has previously been used in meniscus allograft transplantation and ACL reconstruction procedures. Many of the previous meniscus tissue-engineering studies have utilized different suture sizes or materials (eg, polyethylene); however, it is important to note that these sutures have comparable material properties. 31 While thicker sutures could provide even greater suture properties, it is difficult to tie knots with them clinically. Second, only 1 anterior tunnel was investigated because testing 2 tunnels would compromise tibial condyle bone integrity. Future testing may attempt to drill both the anterior and posterior tunnels in the medial direction because of increased bone mass density. Along those lines, this study did not investigate bone density, a parameter that may be influential in interference mechanics. While no age-related trends were observed with regard to fixation mechanics, bone density may need to be considered when applying these findings clinically.
Two potential future directions involve testing protective sheaths and/or hybrid fixation (combination of screw and suture fixation). Eight of the 20 interference screw tests resulted in a tail rupture at the screw, some of which may have occurred during tail implantation. A protective sheath may allow for the same interference while simultaneously protecting the tail from a rupture. Second, the ultimate tensile properties, especially for anterior screw fixation, were not at the level of the native root. Thus, hybrid fixation with the use of an interference screw and endobutton could further improve on fixation biomechanics.
To date, this is the first study to characterize the surgical fixation properties of a total meniscus device, a feature that is crucial to the implant’s success. Specifically, interference screw fixation resulted in less elongation than suture endobutton fixation during cyclic loading, with significantly greater stiffness. We recommend that designs incorporate extended tails that can be fixed via an interference screw to limit extrusion and maintain load-sharing properties.
Footnotes
Acknowledgements
The authors thank the Musculoskeletal Transplant Foundation for supplying cadaveric specimens. They also thank the staff of the Department of Orthopaedic Surgery at Rutgers Biomedical and Health Sciences, and specifically Barbara Perry, for their help with handling cadaveric specimens. They further thank Dr Joachim Kohn and Dr Sanjeeva Murthy for synthesizing and drawing the polymer fiber.
One or more of the authors has declared the following potential conflict of interest or source of funding: The research herein was funded, in part, by a research contract with NovoPedics. The meniscus device described in this article has 3 issued patents (US 8,623,085 B2; US 9,078,756 B2; US 9,579,212 B2) and 2 patents pending. The technology has been licensed for product development (Meniscofix; NovoPedics). The Musculoskeletal Transplant Foundation supplied the cadaveric specimens. J.M.P. serves as a consultant for NovoPedics. M.G.D. serves as interim secretary and treasurer of and owns stock in NovoPedics. C.J.G. serves as interim president of and owns stock in NovoPedics and receives honoraria from the Musculoskeletal Transplant Foundation.