
Abstract
Background:
The occurrence of physiologic knee hyperextension (HE) in the revision anterior cruciate ligament reconstruction (ACLR) population and its effect on outcomes have yet to be reported.
Hypothesis/Purpose:
The prevalence of knee HE in revision ACLR and its effect on 2-year outcome were studied with the hypothesis that preoperative physiologic knee HE ≥5° is a risk factor for anterior cruciate ligament (ACL) graft rupture.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
Patients undergoing revision ACLR were identified and prospectively enrolled between 2006 and 2011. Study inclusion criteria were patients undergoing single-bundle graft reconstructions. Patients were followed up at 2 years and asked to complete an identical set of outcome instruments (International Knee Documentation Committee, Knee injury and Osteoarthritis Outcome Score, WOMAC, and Marx Activity Rating Scale) as well as provide information regarding revision ACL graft failure. A regression model with graft failure as the dependent variable included age, sex, graft type at the time of the revision ACL surgery, and physiologic preoperative passive HE ≥5° (yes/no) to assess these as potential risk factors for clinical outcomes 2 years after revision ACLR.
Results:
Analyses included 1145 patients, for whom 2-year follow-up was attained for 91%. The median age was 26 years, with age being a continuous variable. Those below the median were grouped as “younger” and those above as “older” (age: interquartile range = 20, 35 years), and 42% of patients were female. There were 50% autografts, 48% allografts, and 2% that had a combination of autograft plus allograft. Passive knee HE ≥5° was present in 374 (33%) patients in the revision cohort, with 52% being female. Graft rupture at 2-year follow-up occurred in 34 cases in the entire cohort, of which 12 were in the HE ≥5° group (3.2% failure rate) and 22 in the non-HE group (2.9% failure rate). The median age of patients who failed was 19 years, as opposed to 26 years for those with intact grafts. Three variables in the regression model were significant predictors of graft failure: younger age (odds ratio [OR] = 3.6; 95% CI, 1.6-7.9; P = .002), use of allograft (OR = 3.3; 95% CI, 1.5-7.4; P = .003), and HE ≥5° (OR = 2.12; 95% CI, 1.1-4.7; P = .03).
Conclusion:
This study revealed that preoperative physiologic passive knee HE ≥5° is present in one-third of patients who undergo revision ACLR. HE ≥5° was an independent significant predictor of graft failure after revision ACLR with a >2-fold OR of subsequent graft rupture in revision ACL surgery.
Registration:
NCT00625885 (ClinicalTrials.gov identifier).
The Multicenter ACL Revision Study cohort was conceived to evaluate the outcomes of revision anterior cruciate ligament reconstruction (ACLR) when it was determined that existing prospective cohorts not specifically focused on revision ACLR lacked sufficient numbers of revision cases for efficient and meaningful analysis.6,16,19 Previous outcome studies of ACLR generally reported results of the entire patient cohort, and few considered the variable of passive knee hyperextension (HE) as a risk factor. 14 The risk factors that predispose a person to an anterior cruciate ligament (ACL) injury vary. It is well known that many knees passively extend past 0° and that some but not all of these may have generalized laxity.9,13-15,23 Knee HE was previously reported to be an intrinsic factor contributing to ACL injury.13,14 The occurrence of knee HE in the revision ACLR population and its effect on outcomes have yet to be reported. As such, the purpose of this study was to determine the prevalence of preoperative physiologic knee HE in a large revision ACLR population and to determine its effect on 2-year outcome. The study hypothesis was that HE ≥5° is an independent risk factor for ACL graft rupture 2 years after revision ACL surgery.
Methods
Study Design
With the backing of the American Orthopaedic Society for Sports Medicine, this study began enrolling patients on March 1, 2006. This prospective longitudinal cohort design was established to determine prognosis and identify predictors of outcome of revision ACLR. The consortium consists of 83 enrolling surgeons at 52 sites in 28 American states and 2 Canadian provinces. Surgeons in this study practice in both academic (n = 23; 44%) and private practice (n = 29; 56%) sites. The epidemiology, demographics, and specific methods of this consortium were previously published. 19
Data Sources
Because double-bundle reconstructions were reported to potentially limit terminal extension and graft outcomes among patients with HE,10,23 only those patients who received a single-bundle ACL graft at the time of their revision surgery were included for this study. After informed consent was obtained, participants were asked to complete a patient questionnaire that contained a series of validated patient-oriented outcome instruments, including the subjective IKDC (International Knee Documentation Committee), the KOOS (Knee injury and Osteoarthritis Outcome Score), WOMAC (Western Ontario and McMaster University Osteoarthritis Index), and the Marx Activity Rating Scale. The surgeon completed a form detailing the injury, treatment history of the knee, associated intra-articular injuries, examination under anesthesia according to IKDC guidelines, surgical technique, and graft utilized in the revision surgery. As such, all passive range of motion measurements were obtained under anesthesia by each participating study surgeon at the time of the revision surgery. Passive motion of both knees was documented. Knee HE was measured with a goniometer or by bed-heel distance (1 cm = 1°).
Patient Follow-up
Patients were followed up for 2 years and asked to complete the identical set of outcome instruments. Patients were also contacted by telephone to determine if graft failure (diagnosed by magnetic resonance imaging [MRI]) and any subsequent surgery had occurred since their initial revision reconstruction. If so, operative reports were obtained, whenever possible, to verify pathologic findings and treatment.
Statistical Analysis
To describe our patient sample, we summarized continuous variables with medians and interquartile ranges (IQRs) and categorical variables with frequencies and percentages. These variables were compared with nonparametric statistics (Wilcoxon test for continuous variables, Pearson test for categorical variables). Graft failure or subsequent revision surgery at 2-year follow-up was the primary endpoint. A logistic regression model was used to analyze 4 independent variables—age, sex, graft type (autograft vs allograft), and symmetric knee HE ≥5° versus <5°—to assess these potential risk factors on outcomes 2 years after revision ACLR. Age was treated as a continuous variable, and the median was 26 years. Those below the median were grouped as “younger” and those above the median as “older” (age: IQR = 20, 35 years). The statistical model would support the analysis of only 4 independent variables. Statistical analysis was performed with free and open-source statistical software (R; www.r-project.org).
Results
Baseline Characteristics
Analyses included 1145 patients, as 54 were excluded from the overall cohort because a double-bundle reconstruction was performed and 6 had missing range of motion values (Table 1). Two-year follow-up was attained on 91%. The median age was 26 years (IQR = 20, 35), and 42% were female. There were 50% autografts, 48% allografts, and 2% that had a combination of autograft plus allograft. Passive knee HE ≥5° was present in 374 (33%) of our revision cohort, with 52% being female. There was no difference in baseline characteristics between the groups.
Baseline Demographic and Clinical Characteristics at the Time of Revision ACLR by Cohort a
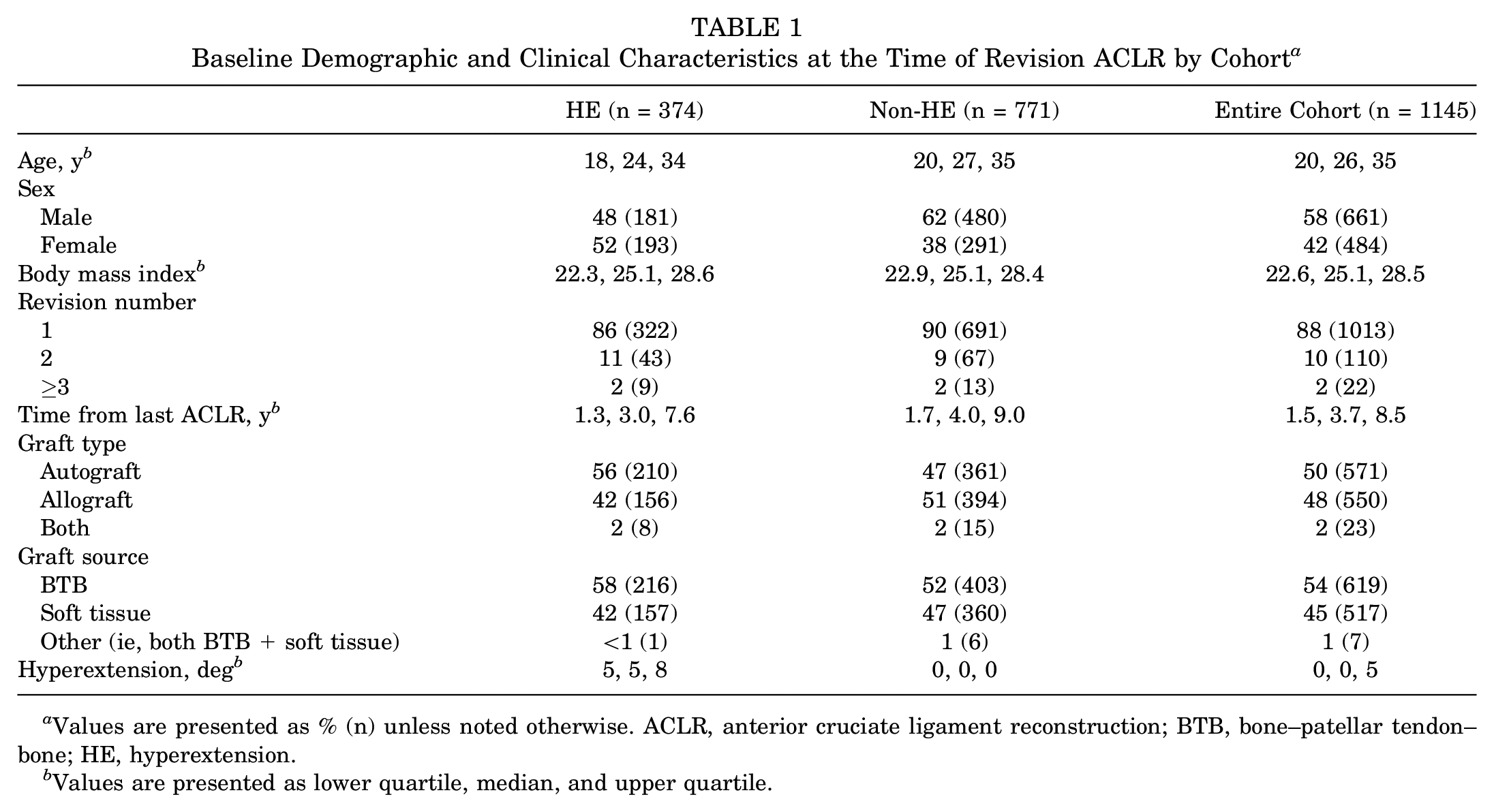
Values are presented as % (n) unless noted otherwise. ACLR, anterior cruciate ligament reconstruction; BTB, bone–patellar tendon–bone; HE, hyperextension.
Values are presented as lower quartile, median, and upper quartile.
Graft Failure
Known graft rupture occurred in 34 cases in our entire cohort, of which 12 were in our HE ≥5° group (3.2% failure rate) and 22 in our nonhyperextender group (2.9% failure rate) (Table 2, Figure 1). The median age of subjects who failed was 19 years, as opposed to 26 years for those with intact grafts. Three variables in our regression model were significant independent predictors of graft failure: younger age (odds ratio [OR] = 3.6; 95% CI, 1.6-7.9; P = .002), use of allograft (OR = 3.3; 95% CI, 1.5-7.4; P = .003), and HE ≥5° (OR = 2.12; 95% CI, 1.1-4.7; P = .03). Sex was not predictive of graft failure in our study (OR = 1.59; 95% CI, 0.7-3.2; P = .18).
ACL Graft Failures at 2-Year Follow-up by Group a
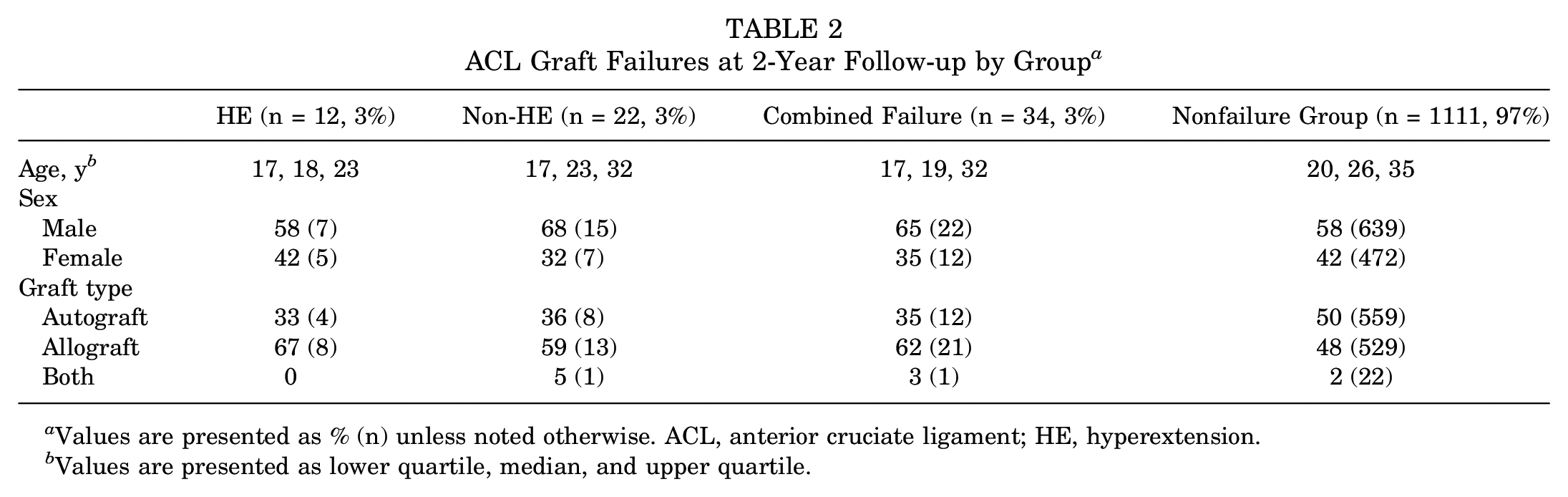
Values are presented as % (n) unless noted otherwise. ACL, anterior cruciate ligament; HE, hyperextension.
Values are presented as lower quartile, median, and upper quartile.
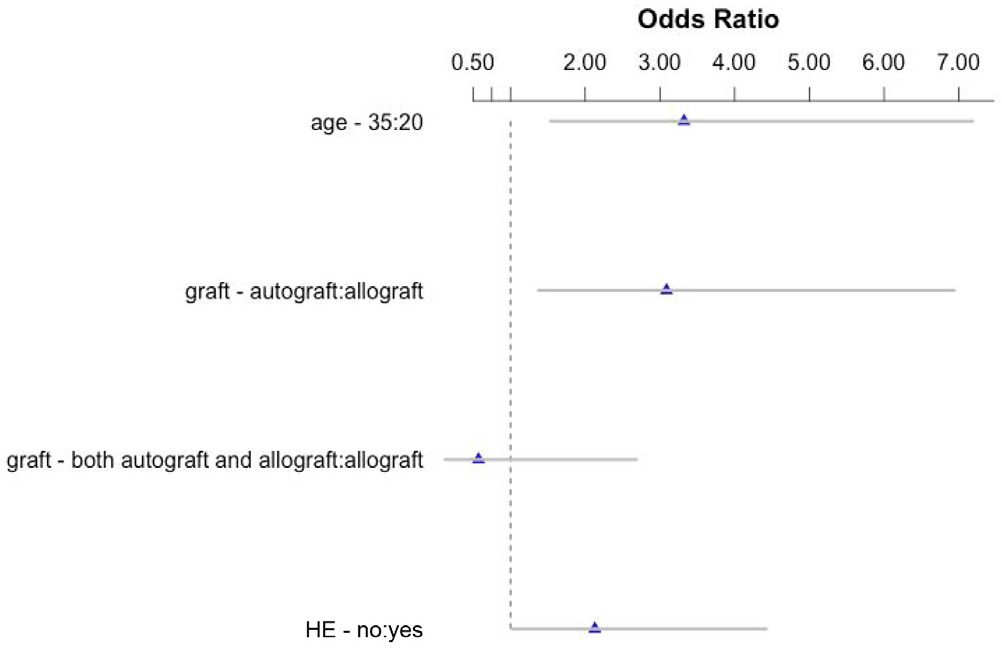
The median age was 26 years (interquartile range = 20, 35). The increased odds ratio of graft failure was associated with young age (3.6), allograft (3.3), and hyperextension ≥5° (2.12).
Discussion
Our group previously reported that young age and allograft use were predictive of graft failure in a revision ACL cohort.3-6,16-20 This report reaffirms that conclusion. Additionally, the hypothesis that HE ≥5° is predictive of graft failure at 2 years in a revision ACL cohort is supported by the results of this study. This is the first evidence-based report of such an association.
When studying physiologic knee HE in relation to ACL tears, there are several topics for consideration: prevalence in an ACL tear cohort, relative risk for ACL tear, association with increased anterior-posterior knee laxity, relative risk for ACL graft rupture after primary versus revision ACLR, whether restoration of full HE increases the risk of ACL graft rupture in primary or revision ACLR, and whether loss of full HE after primary or revision ACLR leads to knee osteoarthritis (OA).
Published reports suggest that knee HE is not necessarily associated with increased anterior-posterior laxity or increased risk of ACL tear.1,2,10,13,14,21,23,28 As compared with single-bundle ACLR, double-bundle ACLR was shown to capture the knee and limit HE after ACLR.21-23,26 Changes of OA after ACLR are related to loss of full knee HE. There is some suggestion that the loss of HE may be causal of OA and not simply a result of it.24-26,29
Many surgeons have the opinion, based on their clinical experience, that it is more difficult to achieve long-term ACL graft integrity in a knee that hyperextends significantly. However, there has been relatively little investigation into this subset of ACL cases, so evidence-based data are lacking. Few have studied preoperative knee HE as a separate cohort when reporting results. Benner et al 2 reported that knee HE was not associated with an increased risk of graft rupture in a large cohort of primary ACLRs treated by a single surgeon with a consistent surgical technique: bone–patellar tendon–bone autograft, graft tensioning in full HE, and fixation with sutures tied over ligament buttons. 29 This is in contrast to our findings for a cohort with numerous surgeons and techniques. It is possible that the less rigid fixation and tensioning in full HE could reduce the risk of excessive graft tension and failure with the methods described by Benner et al. 2 It is possible that certain graft tensioning and fixation techniques might increase the risk of graft rupture as compared with others. This might be the reason why our data support HE ≥5° as an independent risk factor for graft rupture in a revision ACL cohort. However, our methods do not address this issue.
This study includes numerous surgeons with differing graft choices, knee flexion angles when tensioning, and methods of fixation.3-6,16-20 The methods and power of this cohort study allow for the multivariate analysis of the binary comparison of HE <5° versus ≥5° but do not allow the analysis of HE as a continuum of numbers. The cutoff of 5° was an arbitrary decision based on the hypothesis. This multivariate data analysis yielded significant findings, and the use of multivariate analysis is essential to identify the independent risk factors—for the seemingly small difference between 2.9% and 3.2% graft failure in the 2 groups can be affected by >1 independent variable. The increased risk (OR = 2.12) of graft failure in HE knees in our cohort raises the suspicion that surgical technique in the recurvatum knee will affect risk of graft failure. Future study is warranted to determine the ideal graft, knee flexion angle for graft tensioning, and fixation method. 29 Although the OR of graft failure in HE knees (2.12) was not as striking as in the younger-age (3.6) and allograft (3.3) groups, it was significant (P = .03) with the previously published regression model used in all reports from this cohort.
This study provides a high level of evidence that HE ≥5° is an independent risk factor for failure in revision ACL surgery. This revision ACL cohort had a large number of HE ≥5° knees (33%), and it is possible that there would be more HE ≥5° knees in a revision population if in fact HE is a risk factor for failure in ACL surgery. Knowing this to be the case, we retrospectively reviewed data from the MOON cohort and found that 32% of the knees in a primary ACLR cohort had HE ≥5°. 3 It is beyond the scope of this study to compare the 2 groups or determine if HE ≥5° is a risk factor in primary ACLR, but it is certainly of note that roughly one-third of knees in both a primary ACLR cohort and a revision ACLR cohort demonstrate passive HE ≥5°.
Physiologic HE is an important variable in the surgical technique of ACLR, given that several studies showed increasing tension and elongation in the native ACL in terminal extension.7,8,11,12,27 However, none of these studies looked at extension past 10°, and only a few examined extension past 0°. Larson et al 14 recently reported on outcomes in ACLR comparing generalized laxity and knee HE >10° and found that these variables increased the rates of both graft failure and contralateral ACL tear. The knee HE + generalized laxity group had triple the risk of graft rupture (24.4% vs 7.7%) in a large cohort with 6-year follow-up. Regarding combined graft failure plus contralateral ACL tear rates, the knee HE + generalized laxity group also had much greater risk (34% vs 12%). 14
Akelman et al 1 reported that there was no difference in clinical outcomes between a low graft tension group and a high graft tension group in long-term follow-up. The authors of this study did not seek to assess the relative risk of graft tensioning or fixation as a function of knee position. We believe that this issue is an important subject for future study. Additionally, the biomechanics literature is deficient as it relates to knee kinematics and ACL tension patterns in the knee with HE ≥5°. Yet, fully one-third of primary and revision ACLR populations are in this category.
There are limitations to this study that need to be addressed. Wide variability exists among surgeons as related to knee flexion angle for ACL graft fixation. In our study’s surgeon group, this varied from a position of full passive HE to 20° or 30° of knee flexion. Given wide variability in HE, one must realize the adverse effects on graft excursion, tension, and even overload to failure that may be caused by the combination of HE and a graft that has increasing strain in terminal extension yet is fixed with the knee in flexion. This is particularly concerning with the recent trend for lower “anatomic” femoral tunnel positions, which do create slightly more graft excursion, as compared with “higher” anteromedial femoral bundle techniques.1,7,8,11,27 Second, we did not have MRI, physical examination, or objective laxity measurements (ie, KT-1000) to determine knee laxity in the patient cohort. Rather, our determination of graft failure was based on patient telephone calls to determine the status of each graft. We considered MRI and/or revision surgical confirmation as evidence of graft failure. Examination of each patient by a single examiner would have been exceedingly difficult given the number of patients and the fact that they were treated at 52 sites in 28 American states and 2 Canadian provinces.
Conclusion
This study found that preoperative physiologic knee HE ≥5° is present in one-third of patients who undergo revision ACLR. HE ≥5° was found to be an independent significant predictor of graft failure after revision ACLR, with a >2-fold OR of subsequent graft rupture. Younger age (<26 years) and use of allograft tissues for ACLR are associated with a >3-fold OR of subsequent graft rupture.
Footnotes
Acknowledgements
We express our appreciation to the late Barton Mann, PhD (AOSSM, Rosemont, Illinois, USA), Timothy M. Hosea, MD (University Orthopaedic Associates LLC, Princeton, New Jersey, USA), and Allen F. Anderson, MD (Tennessee Orthopaedic Alliance, Nashville, Tennessee, USA), whose contribution to this work was of great significance.
Presented at the annual meeting of the AOSSM, Colorado Springs, Colorado, July 2016.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study received funding from the AOSSM, Smith & Nephew, National Football League Charities, and Musculoskeletal Transplant Foundation. This project was partially funded by grant 5R01-AR060846 from the National Institutes of Health / National Institute of Arthritis and Musculoskeletal and Skin Diseases.