
Abstract
Background:
Low-molecular-weight heparin (LMWH) thromboprophylaxis is widely used for reducing the risk of thrombosis after major orthopaedic surgery. However, the effect and safety on knee arthroscopic surgery are still controversial.
Purpose:
To assess the efficacy and safety of LMWH for the prevention of symptomatic venous thromboembolism (VTE) after knee arthroscopic surgery and anterior cruciate ligament reconstruction (ACLR) by conducting a meta-analysis of randomized controlled trials (RCTs).
Study Design:
Meta-analysis.
Methods:
The authors searched the electronic databases of MEDLINE, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), ClinicalTrials.gov, and Web of Science for all studies from inception to June 30, 2017. All selected studies were categorized into 2 subgroups: simple knee arthroscopic surgery and ACLR. The primary effect and safety endpoint were the incidence of major VTE and major bleeding events (BEs), respectively. The secondary effect and safety endpoint were the incidence of all VTE and all BEs, respectively. Relative risks (RRs) with 95% CIs were calculated using Review Manager 5.3.
Results:
Eight RCTs with 4113 patients were included. For patients undergoing simple knee arthroscopic surgery, LMWH prophylaxis did not bring a significant reduction in the risk of major VTE (RR, 1.00 [95% CI, 0.37-2.67]; P > .99) and all VTE (RR, 0.63 [95% CI, 0.31-1.29]; P = .21) and did not increase the risk of major BEs (RR, 0.98 [95% CI, 0.06-15.72]; P = .99) but did have a higher risk of all BEs (RR, 1.64 [95% CI, 1.18-2.28]; P = .003) in comparison with non-LMWH prophylaxis. For patients undergoing ACLR, LMWH prophylaxis was associated with a significantly lower rate of major VTE (RR, 0.23 [95% CI, 0.12-0.43]; P < .001) and all VTE (RR, 0.22 [95% CI, 0.06-0.73]; P = .01) but no increase in major BEs (RR, 1.80 [95% CI, 0.19-17.25]; P = .61) and all BEs (RR, 1.12 [95% CI, 0.72-1.74]; P = .61) in comparison with non-LMWH prophylaxis.
Conclusion:
Compared with non-LMWH treatment, LMWH had no significant efficacy in preventing VTE in patients undergoing simple knee arthroscopic surgery but increased the risk of BEs. However, LMWH had significant efficacy in preventing VTE for patients mainly undergoing ACLR and did not increase the risk of BEs.
Currently, knee arthroscopic surgery is the most commonly performed orthopaedic procedure for bone and joint diseases in the world, with over 5 million patients undergoing knee arthroscopic surgery globally every year.10,12 Knee arthroscopic surgery has been considered to be minimally invasive and therefore has a relatively low risk of venous thromboembolism (VTE), ranging from 3.1% to 17.9%.4-6,17,30,31 A meta-analysis determined an overall weighted rate of deep vein thrombosis (DVT) of 9.9%. 13 More recent studies with large populations have reported rates of pulmonary embolism from 0.05% to 0.11% and the rate of DVT of 0.46%.16,23
However, extending the indication for arthroscopic surgery, some arthroscopic procedures make use of a tourniquet or femoral nerve blockade during the perioperative period that will result in an increased risk of DVT. 7 One recent study even showed that 41.2% of patients who received placebo had DVT confirmed by magnetic resonance venography after anterior cruciate ligament reconstruction (ACLR). 15
The use of low-molecular-weight heparin (LMWH) as thromboprophylaxis after most orthopaedic interventions is well recommended in that it strongly reduces the risk of thrombosis, although it increases the risk of bleeding.9,25,27 However, the use of this prophylaxis in patients after knee arthroscopic surgery remains controversial. Several randomized trials have demonstrated that using LMWH could reduce the risk of DVT by 65% to 93%, in patients after knee arthroscopic surgery.2,15,17,31 However, 2 previous published systematic reviews did not form a consistent conclusion.21,26 Two recent larger randomized controlled trials (RCTs) of high quality including ACLR also reported conflicting results.1,29 On the basis of this evidence, thromboprophylaxis recommendations after knee arthroscopic surgery vary from one country to another; for example, pharmacological prophylaxis after knee arthroscopic surgery is not routinely recommended by the American College of Chest Physicians 8 but is suggested by the French Society of Anaesthesia and Intensive Care. 24
In view of this situation, a meta-analysis of all available randomized trials investigating the prophylactic administration of LMWH compared with placebo or no treatment was undertaken. This type of analysis increases the statistical power and thus allows more precise estimation of LMWH efficacy in patients after knee arthroscopic surgery. The primary aim of this meta-analysis including RCTs was to compare anticoagulant therapy (LMWH) for the prevention of symptomatic VTE with no LMWH therapy after simple knee arthroscopic surgery and ACLR. We hypothesized that treatment with anticoagulants after knee arthroscopic surgery would be effective in the prevention of symptomatic VTE and that the benefit would outweigh the risk of bleeding, especially for ACLR.
Methods
Literature Search
This study was designed and conducted according to the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). 18 We searched the electronic databases of MEDLINE, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), ClinicalTrials.gov, and Web of Science for studies in all languages from inception to June 30, 2017. Two independent reviewers (J.Z. and H.J.) searched each database. The following text words and corresponding heading terms were used as the search subject terms: “thromboembolism” or “venous thromboembolism” or “pulmonary embolism” or “venous thrombosis” and “LMWH” and “arthroscopy.” The detailed search strategy is provided in the Appendix (available in the online version of this article). A manual search of the references of included articles was also conducted to ensure that no eligible studies were missed. After title screening, we evaluated abstracts for relevance and identified them as included, excluded, or requiring further assessment.
Inclusion and Exclusion Criteria
The inclusion criteria for enrolling studies were all prospective RCTs that compared LMWH with placebo or no treatment or other nonpharmaceutical therapy for the prevention of symptomatic VTE after knee arthroscopic surgery; used objective methods to confirm the diagnosis of symptomatic VTE; and reported the main clinical outcomes measured by the incidence of asymptomatic proximal DVT, symptomatic VTE, and all-cause mortality and the combined incidence of major and clinically relevant bleeding events (BEs) in their study. Major VTE was defined as the cumulative incidence of all-cause mortality, symptomatic VTE, and asymptomatic proximal DVT during the follow-up. The data on asymptomatic DVT from these studies were included if systematic screening was carried out with venography or ultrasonography. Major bleeding was mainly defined as follows: (1) fatal bleeding, (2) symptomatic bleeding in a critical area or organ, (3) extrasurgical site bleeding causing a fall in the hemoglobin level of ≥2.0 g/dL or leading to transfusion of ≥1 U of whole blood or red cells, (4) surgical site bleeding that required a second intervention or hemarthrosis interfering with rehabilitation or surgical site bleeding that needed blood transfusion,1,2,15,17,29 (5) hemarthrosis with joint drainage of more than 450 mL, 2 or (6) overt bleeding with a bleeding index of ≥2. 15 The bleeding index was calculated from the prebleeding hemoglobin concentration (g/dL) minus postbleeding hemoglobin concentration (g/dL). 15 A clinically relevant nonmajor BE, including minor bleeding, was defined as hemarthrosis with joint drainage of 100 to 450 mL that was not life threatening and did not require a reintervention 2 ; all other BEs not meeting the criteria for major bleeding1,15,17; or overt bleeding not meeting the criteria for major bleeding but associated with a medical intervention, unscheduled contact with a physician, (temporary) cessation of study treatment, or discomfort such as pain or impairment of activities of daily life. 29 The exclusion criteria were as follows: retrospective comparison studies, case series and cohort studies, revision surgery, multiligament injuries, studies failing to clearly report data that meet our interest, review articles, irrelevant topics, nonknee arthroscopic surgery, and animal experimental studies. Disagreements on study selection were resolved by a discussion and consensus between the 2 reviewers.
Data Extraction
Data from eligible studies were extracted independently by the same 2 reviewers (J.Z. and H.J.) according to predefined selected criteria: (1) article or publication information, such as first author’s name and year of publication; (2) patient characteristics, such as age, sex, and surgical procedures; (3) study designation information: phase, total sample size, sample size per arm, length of follow-up, and loss to follow-up; (4) information about treatment: treatment approach, dose, and name and cycle of LMWH used; and (5) measurement methods of outcomes. Data about efficacy and safety including asymptomatic DVT were carefully extracted, documented by ascending lower limb contrast venography and duplex ultrasound scanning, recorded on a data collection form, and then entered into an electronic database. Disagreements on data extraction were resolved by a discussion. For Camporese et al’s 2 study, we combined LMWH for 7 days with LMWH for 14 days for the LMWH group.
Assessment of Risk of Bias
Two senior authors (J.L. and X.T.) independently assessed the methodological quality of the selected studies using the Cochrane Collaboration’s risk of bias tool, 11 which contains 6 items as follows: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other bias. Each of the included studies was rated as having low, unclear, or high risk to the above items. Publication bias was not detected because of the limited number of included studies. Disagreements were resolved by a discussion.
Subgroup Categorization
To explore whether LMWH would have a different effect on ACLR and simple knee arthroscopic surgery, all selected studies were categorized into 2 subgroups on the basis of the surgical setting: (1) ACLR group including ACLR in selected studies and (2) simple knee arthroscopic surgery group only including meniscectomy, removal of loose bodies, or diagnostic arthroscopic surgery and no ACLR.
Endpoints
The primary endpoint of the meta-analysis was the incidence of major VTE, which was defined as the cumulative incidence of all-cause mortality, symptomatic VTE, and asymptomatic proximal DVT during the follow-up. The secondary efficacy outcome was the incidence of all VTE, which was defined as the cumulative incidence of all-cause mortality, symptomatic VTE, and asymptomatic (proximal + distal) DVT. DVT was confirmed by venography or ultrasonography at the end of the study period. Pulmonary embolism was confirmed with lung computed tomography.
The primary safety endpoint was the incidence of major BEs, as defined in each study. The secondary safety endpoint was the related cumulative incidence of all BEs including clinically major bleeding, nonmajor bleeding, and all other relevant cases of hemorrhage.
Statistical Analysis
Data analyses were performed using Review Manager software (version 5.3; Cochrane Collaboration). The relative risk (RR) and its corresponding 95% CI were calculated for dichotomous data. The Mantel-Haenszel method was used to generate the summary statistics for the effect of LMWH overall and in prespecified subgroups of studies. Heterogeneity was assessed by I2 tests. An I2 value >50% and P < .1 were considered significant heterogeneity. A fixed-effects model was applied for outcome data with no evidence of significant heterogeneity, whereas a random-effects model was used if significant heterogeneity existed among the studies.
Results
Characteristics of Included Studies
Through an initial search of the online databases, a total of 48 articles were collected for screening. We included another 5 studies by an examination of references in the primary publications. Articles that did not meet the inclusion criteria of this study were excluded. Eventually, 8 RCTs (Canata GL, Chiey A. “Prevention of venous thromboembolism after ACL reconstruction: a prospective, randomized study.” Presented at the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine, 2003)1,2,15,17,22,29,31 were included in this study (Figure 1) after the removal of duplicates and further screening of the full text of these articles.
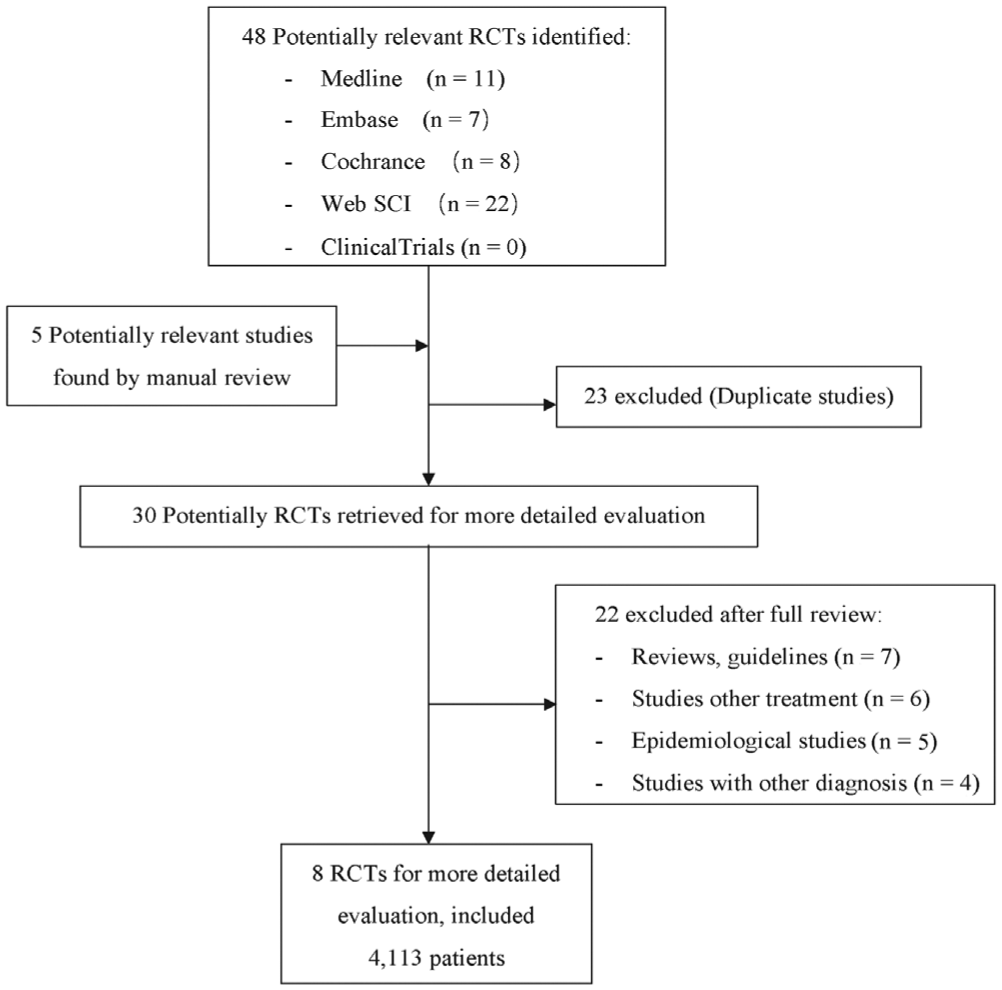
Flow diagram of study selection. RCT, randomized controlled trial.
Two of 8 studies1,15 compared LMWH with placebo. Five studies (Canata GL, Chiey A., unpublished, 2003)17,22,29,31 compared LMWH with no anticoagulant therapy. One study 2 compared LMWH (divided into 2 groups: 7 and 14 days) with compression stockings (7 days) for thromboprophylaxis after knee arthroscopic surgery.
Four (Canata GL, Chiey A., unpublished, 2003)1,2,15 of the 6 selected studies including ACLR were categorized into the ACLR group. Of the 4 studies, 2 (Canata GL, Chiey A., unpublished, 2003) 15 included 201 (100%) patients, and the other 2 studies by Camporese et al1,2 partially included patients undergoing ACLR. Of the 2 studies, 1 2 included 432 (39.2%) patients in the trial group and 249 (37.7%) in the control group; the other study 1 included 10 (8.2%) patients in the trial group and 5 (4.2%) in the control group. The characteristics of the RCT studies fulfilling the inclusion criteria are listed in Table 1.
Characteristics of 8 Studies Included in the Analysis a
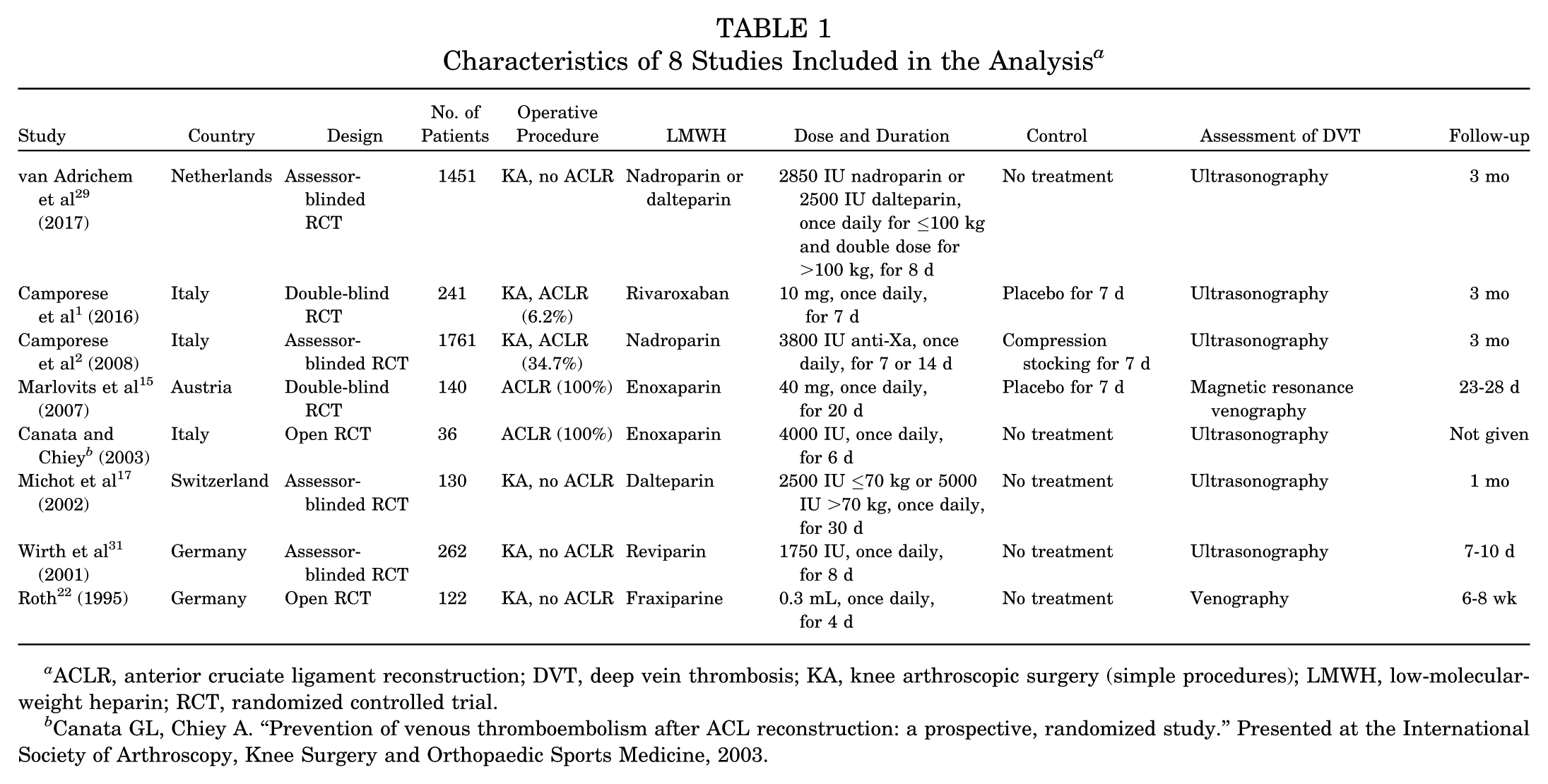
ACLR, anterior cruciate ligament reconstruction; DVT, deep vein thrombosis; KA, knee arthroscopic surgery (simple procedures); LMWH, low-molecular-weight heparin; RCT, randomized controlled trial.
Canata GL, Chiey A. “Prevention of venous thromboembolism after ACL reconstruction: a prospective, randomized study.” Presented at the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine, 2003.
Based on the purpose of this study, a combination of the placebo group, the no anticoagulant group, and compression stockings was formed to represent the non-LMWH group, and therefore, data of the 3 groups were merged for the meta-analysis. Finally, a total of 4113 patients (2286 in LMWH group and 1827 patients in non-LMWH group) were included in this meta-analysis. Among the 4113 patients, 2171 were included in the ACLR group and 1942 in the knee arthroscopic surgery group.
Assessment of Risk of Bias
The results of the assessment of risk of bias on included studies are summarized in Figure 2. Two studies were double blinded (406 patients).1,15 Only 1 study could be rated as low risk in methodological bias. 1 Four studies (Canata GL, Chiey A., unpublished, 2003)15,22,31 did not clearly report the procedure of randomization and were thus rated as unclear risk. Four studies1,2,17,29 used the appropriate procedure of randomization, but 3 of these studies did not describe the blinding of patients and were thus rated as high risk of performance bias.2,17,29 Two studies (Canata GL, Chiey A., unpublished, 2003) 22 did not describe the blinding of outcome assessments and were rated as unclear risk of detection bias. One study did not provide the same course of procedure for each patient, which may result in a high risk of other bias. 15
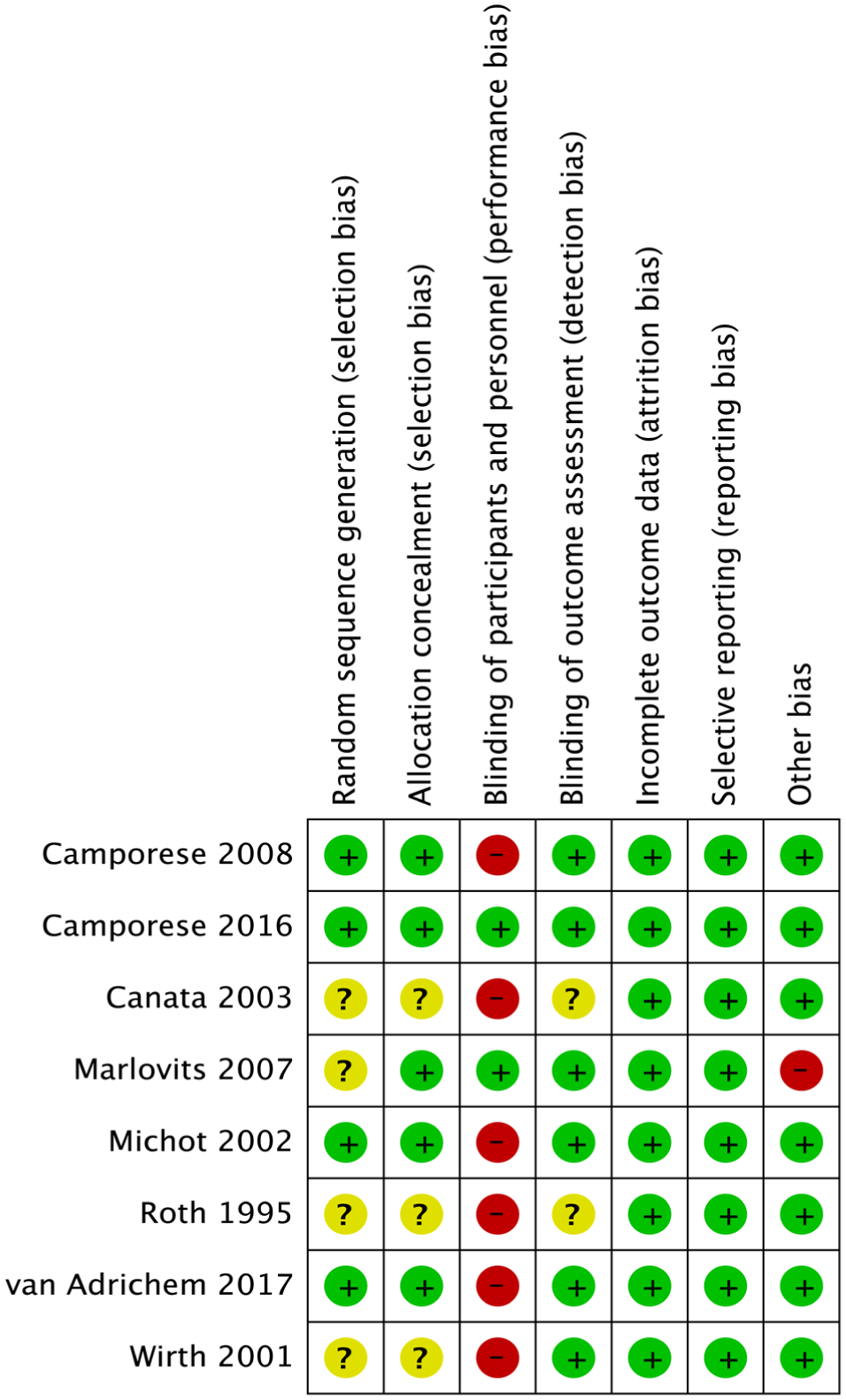
Risk of bias of included studies. +, low risk; –, high risk; ?, unclear risk.
Major VTE
Major VTE was reported in 7 studies including 4077 patients.1,2,15,17,22,29,31 For knee arthroscopic surgery, the overall mortality rate of major VTE was 0.72% in those who received non-LMWH prophylaxis, with an overall incidence of 0.72% in the LMWH group. No significant difference was observed in the risk of major VTE between the 2 groups for simple knee arthroscopic surgery (RR, 1.00 [95% CI, 0.37-2.67]; P > .99) (Figure 3A).

Forest plot diagram showing major venous thromboembolism compared between low-molecular-weight heparin (LMWH) and non-LMWH prophylaxis for patients undergoing (A) knee arthroscopic surgery and (B) anterior cruciate ligament reconstruction. M-H, Mantel-Haenszel method.
However, for ACLR, the overall mortality rate of major VTE was 4.75% in those who received non-LMWH prophylaxis, with an overall incidence of 1.01% in the LMWH group. A significant 77% reduction in the risk of major VTE was observed in favor of LMWH compared with non-LMWH prophylaxis (RR, 0.23 [95% CI, 0.12-0.43]; P < .001) (Figure 3B). No heterogeneity was observed among trials (I2 = 0%, P = .66).
All VTE
The second endpoint was also reported in the same 7 studies (Canata GL, Chiey A., unpublished, 2003).1,2,15,17,22,29,31 For knee arthroscopic surgery, the rate of second endpoints was 1.96% in those who received non-LMWH prophylaxis, with an overall incidence of 1.23% in the LMWH group. No difference was observed in the risk of all VTE between the LMWH group and non-LMWH group, although a 37% reduction in the risk of VTE was observed in favor of LMWH (RR, 0.63 [95% CI, 0.31-1.29]; P = .21) (Figure 4A).
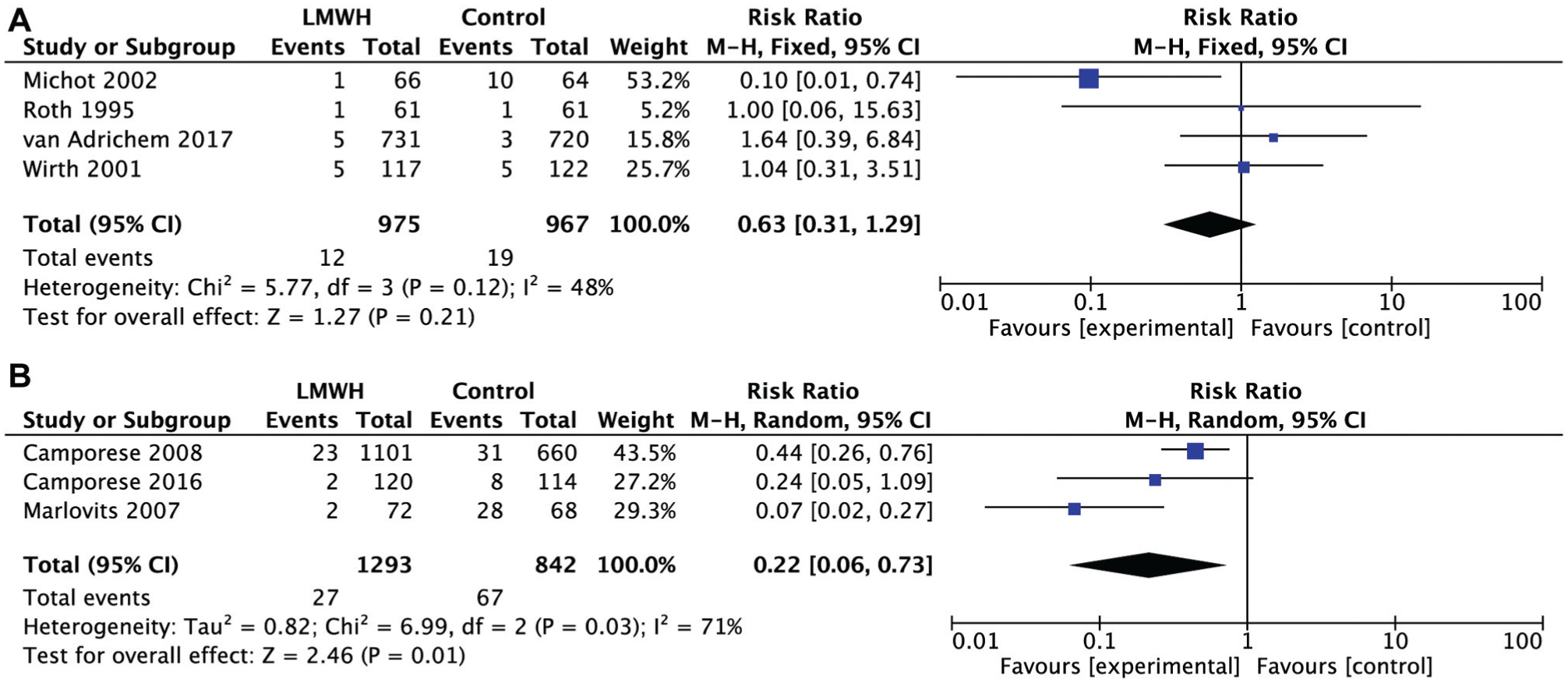
Forest plot diagram showing all venous thromboembolism compared between low-molecular-weight heparin (LMWH) and non-LMWH prophylaxis for patients undergoing (A) knee arthroscopic surgery and (B) anterior cruciate ligament reconstruction. M-H, Mantel-Haenszel method.
For ACLR, the meta-analysis showed a significant difference in the risk of all VTE between the LMWH group and non-LMWH group (RR, 0.22 [95% CI, 0.06-0.73]; P = .01) (Figure 4B), which indicated a better outcome with LMWH prophylaxis in patients undergoing ACLR.
Major BEs
Six of the 8 selected studies (Canata GL, Chiey A., unpublished, 2003)1,15,17,22,31 including 743 patients reported no major BEs. Only 2 studies2,29 including 3212 patients reported 6 major BEs. One study 2 was included in the ACLR group and the other 29 in the simple knee arthroscopic surgery group. Of the 6 major BEs, 4 were treated with LMWH prophylaxis and 2 without LMWH prophylaxis.
For patients who underwent simple knee arthroscopic surgery, no difference was found in the risk of major BEs between the LMWH and non-LMWH groups (RR, 0.98 [95% CI, 0.06-15.72]; P = .99) (Figure 5A). For patients who underwent ACLR, the meta-analysis also showed no significant differences between the LMWH group and non-LMWH group in major BEs (RR, 1.80 [95% CI, 0.19-17.25]; P = .61) (Figure 5B).
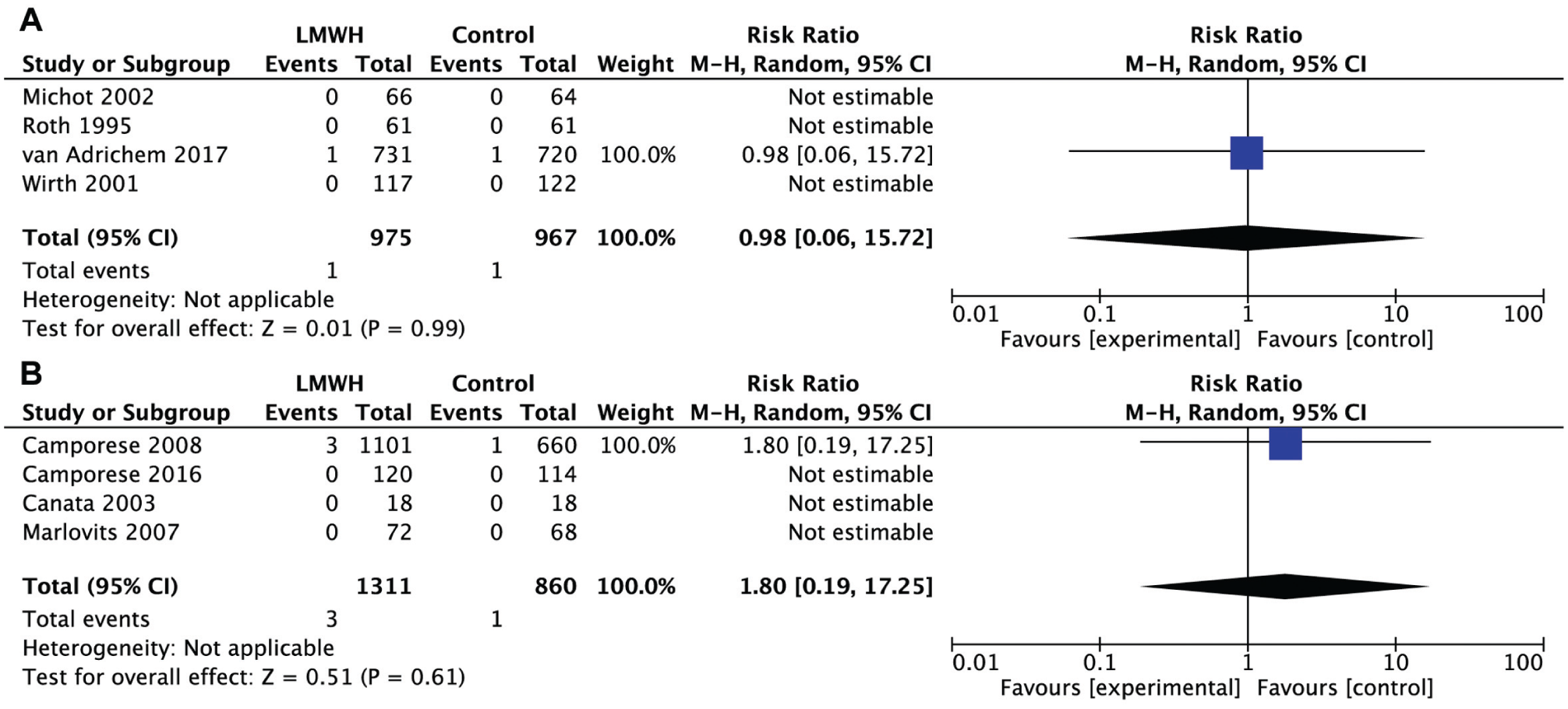
Forest plot diagram showing major bleeding events compared between low-molecular-weight heparin (LMWH) and non-LMWH prophylaxis for patients undergoing (A) knee arthroscopic surgery and (B) anterior cruciate ligament reconstruction. M-H, Mantel-Haenszel method.
All BEs
One study 15 did not report the cumulative incidence of all BEs, so we did not include the safety data (all BEs) from this study. Finally, 7 selected studies (Canata GL, Chiey A., unpublished, 2003)1,2,17,22,29,31 reported a total of 225 BEs. Of the 225 BEs, 141 (62.7%) occurred in the LMWH group and 84 (37.3%) in the non-LMWH group.
For patients who underwent simple knee arthroscopic surgery, the overall rate of all BEs was 9.03% in the LMWH group as compared with 5.48% in the non-LMWH group. The meta-analysis showed significant differences between the LMWH group and non-LMWH group in all BEs (RR, 1.64 [95% CI, 1.18-2.28]; P = .003) (Figure 6A), which favored non-LMWH prophylaxis. No significant heterogeneity was found (I2 = 0%, P = .53). However, for patients who underwent ACLR, the meta-analysis showed no significant difference in the risk of all BEs between the LMWH group and non-LMWH group (RR, 1.12 [95% CI, 0.72-1.74]; P = .61) (Figure 6B). No significant heterogeneity was found (I2 = 0%, P = .48).
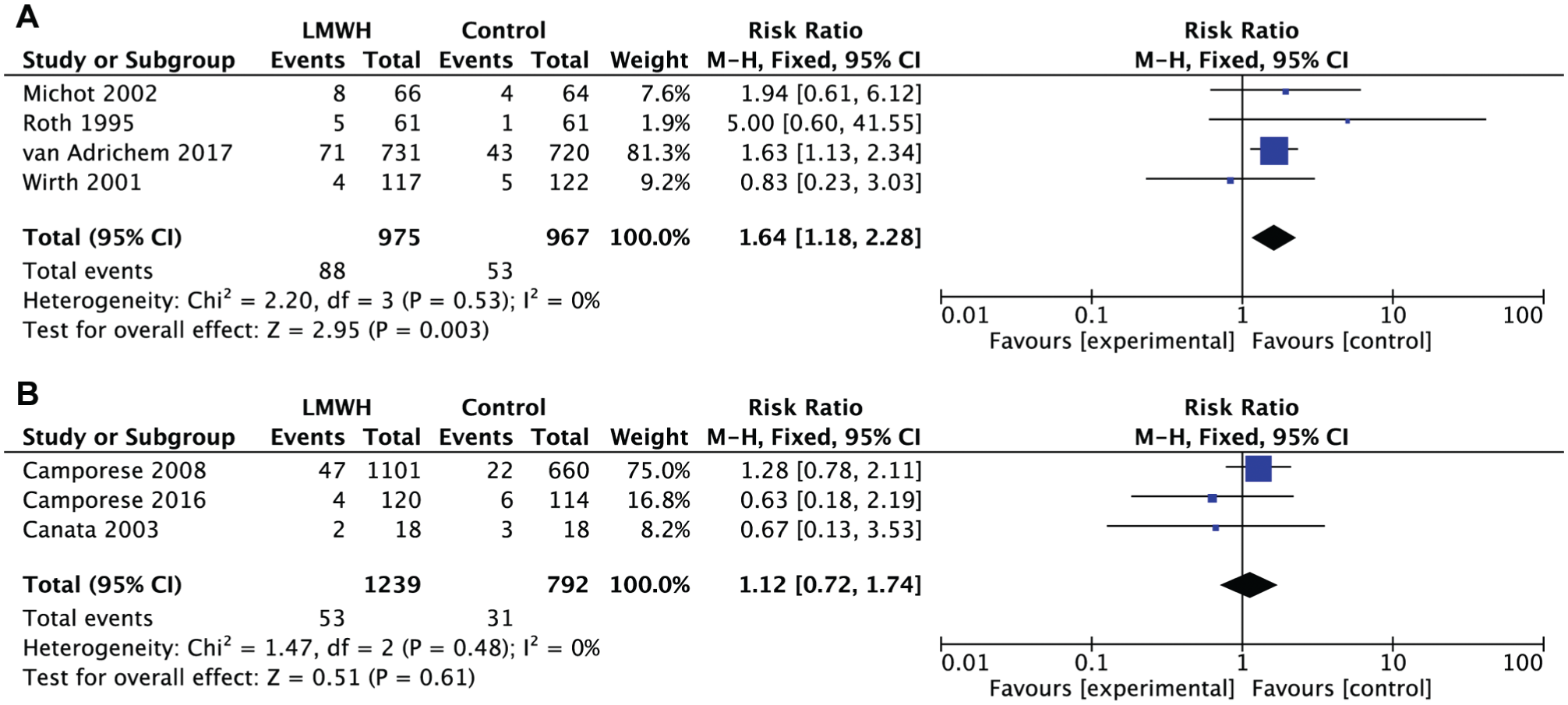
Forest plot diagram showing all bleeding events compared between low-molecular-weight heparin (LMWH) and non-LMWH prophylaxis for patients undergoing (A) knee arthroscopic surgery and (B) anterior cruciate ligament reconstruction. M-H, Mantel-Haenszel method.
Discussion
This meta-analysis included 8 randomized studies assessing the efficacy of LMWH in 4113 patients undergoing simple knee arthroscopic surgery and ACLR. The main finding was that in patients undergoing simple knee arthroscopic surgery, LMWH prophylaxis did not significantly reduce the risk of major VTE (asymptomatic proximal DVT and symptomatic VTE) and all VTE; the patients who received LMWH prophylaxis did not increase the risk of major BEs but had a little higher risk of all BEs compared with those in the control group (9.03% vs 5.48%, respectively). For ACLR, a difference in favor of LMWH was seen in comparison with the non-LMWH group in major VTE and all VTE, while no significant differences were found in major BEs and all BEs in the LMWH group compared with those in the control group.
A few published meta-analysis studies have evaluated the effect of LMWH in preventing VTE in patients after knee arthroscopic surgery or nonmajor orthopaedic surgery including knee arthroscopic surgery and other surgery.3,21,26 Two previous meta-analyses3,26 indicated the potential efficacy of LMWH in preventing thromboembolic events in patients with reduced mobility after undergoing knee arthroscopic surgery compared with placebo or no treatment and did not increase BEs. Another meta-analysis 21 suggested that there was no strong evidence to conclude that thromboprophylaxis is effective in preventing thromboembolic events and safe in people undergoing knee arthroscopic surgery.
However, there were some problems with these meta-analyses. Chapelle et al’s 3 meta-analysis included 14 RCTs, but only 6 studies contained knee arthroscopic subgroups. In Sun et al’s 26 systematic review and meta-analysis, 9 prospective uncontrolled studies were included, and only 4 were RCTs. These 2 reviews both did not include 2 recent large-sized RCTs of high quality.1,29 In Sun et al’s 26 systematic review, the positive findings were mainly based on data from observational studies, so potential selection and allocation bias acted as major confounders. The third systematic review 21 only included 4 RCTs published before 2003 and a small sample size of 527 patients.
Previous studies have shown that the risk of VTE is affected by the type of surgery. For example, arthroscopic ACLR, as the most important and popular surgical procedure in knee sports medicine, leads to a higher risk of VTE than arthroscopic surgery for diagnostic purposes, chondroplasty, or meniscectomy because of both the complexity of the procedure with tourniquet use and a relatively long surgical time.15,19,28 Unfortunately, few studies and no meta-analyses have included formal analyses of LMWH for preventing VTE after different types of knee arthroscopic surgery, especially knee arthroscopic ACLR.
The present meta-analysis includes data from 8 RCTs with 4113 patients who underwent knee arthroscopic surgery. The 8 selected RCTs might be more likely to accurately represent the efficacy and safety of LMWH in patients undergoing knee arthroscopic surgery. Importantly, the more patients in a study, which let us conduct a subgroup analysis, allowed us to obtain a more accurate report regarding different types of knee arthroscopic surgery.
In our meta-analysis, the subgroup analysis found that LMWH reduced the risk of major VTE and all VTE in patients undergoing ACLR but did not increase the risk of major BEs and all BEs. This finding was similar to that in the study by Marlovits et al 15 and suggested that we should use thromboprophylaxis in patients who undergo arthroscopic ACLR with a tourniquet. This finding strongly supports the French guidelines recommending the use of prophylaxis in patients undergoing knee arthroscopic surgery, 24 especially ACLR. Moreover, our meta-analysis showed that for patients who undergo simple knee arthroscopic surgery, LMWH could not reduce the risk of VTE but increased the risk of BEs. This finding partially supports the 2012 American College of Chest Physicians guidelines recommending no use of thromboprophylaxis in patients undergoing knee arthroscopic surgery who do not have a history of VTE. 8 Based on this finding, a different option for thromboprophylaxis for ACLR or simple knee arthroscopic surgery should be selected.
As an alternative antithrombotic agent, aspirin has been widely used in orthopaedic surgery. Previous studies have showed the efficacy of aspirin on thromboprophylaxis in total joint arthroplasty. 20 One study conducted a randomized trial to research if the use of aspirin could prevent VTE after arthroscopic knee surgery in a low-risk population. 14 However, the result of a lack of VTE cases in the included population made the prevention of VTE impossible to ascertain. Future studies that investigate the effect and safety of aspirin on knee arthroscopic surgery are required.
To our knowledge, this meta-analysis is the first study to systematically evaluate the effect and safety of LMWH treatment for preventing VTE in knee arthroscopic surgery and ACLR in 4113 patients and 8 RCTs. Two independent investigators also rigorously assessed the methodological quality.
Our study also has several limitations. First, although 8 RCTs were included in this meta-analysis, 6 of the included studies were not double blinded (assessor blinded). It might not influence the primary outcome (major VTE and major BE), but there is still potential for performance bias. Second, although we extracted data at the end of the follow-up, the duration of each study varied from 7 to 10 days after surgery in 1 study 31 to 90 days in 3 studies.1,2,29 Although the endpoints of different follow-up periods could modify the absolute risk, they should not bias the overall RR. Third, the variation in baseline among studies might also offer some contributing factors to clinical and possibly statistical heterogeneity. For instance, each study used different LMWH products and doses. In addition, the surgical intervention in each study was not the same. All of the patients in Marlovits et al’s 15 study underwent ACLR, while less than 50% patients in Camporese et al’s 2 study underwent ACLR. Last but not least, the intervention in the control group was different among studies, which might provide other bias.
In conclusion, the available RCTs indicated that LMWH had no potential efficacy in preventing VTE in patients undergoing simple knee arthroscopic surgery but increased the risk of all BEs compared with non-LMWH treatment; however, LMWH had favorable efficacy in preventing VTE in patients who underwent arthroscopic ACLR and did not increase the risk of BEs in those undergoing ACLR, which suggests a different option for LMWH prophylaxis in patients who undergo different knee arthroscopic surgery. Further high-quality RCTs comparing LMWH and placebo treatment are required.
Supplemental Material
DS_10.1177_0363546518782705 – Supplemental material for Low-Molecular-Weight Heparin for the Prevention of Venous Thromboembolism in Patients Undergoing Knee Arthroscopic Surgery and Anterior Cruciate Ligament Reconstruction: A Meta-analysis of Randomized Controlled Trials
Supplemental material, DS_10.1177_0363546518782705 for Low-Molecular-Weight Heparin for the Prevention of Venous Thromboembolism in Patients Undergoing Knee Arthroscopic Surgery and Anterior Cruciate Ligament Reconstruction: A Meta-analysis of Randomized Controlled Trials by Jing Zhu, Hai Jiang, Brandon Marshall, Jian Li and Xin Tang in The American Journal of Sports Medicine
Footnotes
In the original online version, panels A and B in Figure 3 and in Figure 4 were switched. This has been corrected online and in print.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.