
Abstract
Background:
For the treatment of femoral condyle cartilage defects with osteochondral allograft transplantation (OCA), many surgeons have relaxed their graft-recipient size-matching criteria given the limited allograft supply. However, since the anteroposterior (AP) length is typically correlated with the radius of curvature for a given condyle, a large mismatch in graft-recipient AP length can indicate a corresponding mismatch in the radius of curvature, leading to articular incongruity after implantation.
Purpose:
To evaluate the association between femoral condyle graft–recipient AP mismatch and clinical outcomes of OCA.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A retrospective review was conducted of patients treated with OCA for femoral condyle chondral defects from 2000 to 2015. Graft characteristics, including AP and mediolateral dimensions, were gathered from vendor-specific allograft offering documents. Patient condyle dimensions were measured on preoperative magnetic resonance imaging. Reoperations and patient responses to validated outcome measures were reviewed. Failure was defined by any partial removal/revision of the allograft or conversion to knee arthroplasty. A multivariable logistic regression model was fitted to examine the association of AP mismatch with OCA failure while adjusting for patient age and number of previous ipsilateral knee surgical procedures.
Results:
A total of 69 knees from 69 patients (mean age, 35.7 years; 71% male) met the inclusion criteria. Mean duration of follow-up was 4 years (range, 2-16 years). The mean absolute graft-recipient AP mismatch was 6.7 mm (range, 0-20 mm; P < .01). At final follow-up, 19 knees had failed. There was no significant difference in the mean absolute AP mismatch between failures (8.1 mm) and nonfailures (6.2 mm; P = .17). Multivariate logistic regression revealed that AP mismatch was not associated with graft failure (P = .14). At final follow-up, significant improvements were noted in the 36-Item Short Form Health Survey, International Knee Documentation Committee subjective form, and Knee Outcome Survey–Activities of Daily Living (P < .01 for all). Magnitude of AP mismatch was not associated with postoperative outcome scores or achievement of minimal clinically significant differences in outcome scores.
Conclusion:
Magnitude of graft-recipient AP mismatch was not associated with midterm OCA failure rates or patient-reported outcome scores, suggesting that AP length mismatch within the limits measured here is not a contraindication for graft acceptance.
Osteochondral allograft transplantation (OCA) is a reliable technique for the management of large articular cartilage defects (≥2 cm2) of the femoral condyles and trochlea. Multiple studies have demonstrated good long-term results, with improvements in postoperative pain and function.1,12,38 OCA has unique advantages over other cartilage procedures, such as microfracture, autologous chondrocyte implantation, and biologic scaffolds (eg, collagen, hyaluronic acid), in that it is a single-stage procedure, can be utilized for contained and uncontained lesions, and addresses underlying pathologic subchondral bone that may contribute to the pain and progression of osteoarthritis.
The goal of the dowel method OCA is to replace the chondral defect with an allograft plug that restores the native articular topography of the hemicondyle with minimal articular step-off between graft and host. Multiple morphologic studies of the distal femur have demonstrated wide variability in the dimensions of the femoral condyles of patients.5,7,18,25 Therefore, most surgeons have traditionally sought grafts matched perfectly to the recipient anteroposterior (AP) and mediolateral (ML) dimensions to, in theory, (1) optimize articular congruity and (2) reduce the potential risk of graft failure. However, from a practical standpoint, complete size matching restricts the number of compatible osteochondral allografts, which delays surgical treatment and prolongs graft storage, potentially leading to the disposal of unused grafts. 28
A growing body of cadaveric and simulation literature suggests that strict size-matching criteria may be unnecessary to achieve the aforementioned surgical goals. In a cadaver study, Mologne et al 30 found that 20-mm medial condyle defects could be adequately filled with grafts from medial or lateral condyle donor allografts while achieving <1-mm articular congruity. Nishizawa et al 33 performed 3-dimensional laser scanning of cadaveric knees and concluded that articular grafts taken from the midportion of the femoral trochlea closely matched the articular contour of the anterior condyle, while grafts taken from the periphery of the trochlea closely matched the articular contour of the posterior condyle. Bernstein et al 3 found it possible to appropriately match 100% of 20-mm defects created in a cadaveric model using nonorthotopic graft sources matched solely on the basis of the radius of curvature. Given these results and the limited availability of osteochondral allografts, many surgeons have recently relaxed their matching criteria and currently match donor to recipient using only the ML dimension to ensure that an adequately sized dowel can be harvested. Consequently, any graft-recipient mismatch in AP length is typically ignored. Since the AP length is typically correlated with the radius of curvature for a given condyle, a large AP mismatch can indicate a corresponding mismatch in radius of curvature between graft and host, leading to potential articular incongruity after implantation. Nonetheless, it is unknown at what threshold an AP mismatch will affect the clinical outcomes of OCA or if any AP mismatch can generally be tolerated.
The purpose of this study was to evaluate the association between femoral condyle graft–recipient AP mismatch and clinical outcomes of OCA at midterm follow-up. Failure was defined as any partial removal/revision of the allograft or conversion to knee arthroplasty, and a case-control study was performed comparing failures and nonfailures. We hypothesized that the failure group would have a larger mean graft-recipient AP mismatch than that of the nonfailure group.
Methods
In 1999, a prospective registry dedicated to the tracking of patient outcomes after articular cartilage restoration procedures was implemented at our institution. An institutional review board approved the registry, and all patients signed an informed consent form before participation. Patients included in the registry were preoperatively evaluated and prospectively followed at postoperative 6 months and 1, 2, 3, 4, 5, and 10 years. A total of 1950 registry patients from 17 surgeons were screened for this study.
Inclusion and Exclusion Criteria
Inclusion criteria included (1) symptomatic focal cartilage lesions of the medial or lateral femoral condyle that were classified as Outerbridge grade IV at the time of arthroscopic surgery, (2) no substantial bone loss requiring additional bone grafting, (3) treatment with fresh osteochondral allograft, and (4) a minimum follow-up of 2 years. Exclusion criteria for this cartilage procedure were advanced osteoarthritis exceeding a Kellgren-Lawrence grade 2, simultaneous multiligamentous reconstruction, inflammatory arthritis or autoimmune conditions, and inability to comply with the postoperative rehabilitation protocol. Patients who received isolated patellar or trochlear OCA or tibial OCA and those who underwent prior or concomitant meniscus transplantation were excluded. Two surgeons (S.A.R. and R.J.W.) at this institution performed OCA according to the specified matching criteria; thus, OCA procedures performed by other surgeons were excluded. Additionally, patients were excluded if their preoperative magnetic resonance imaging (MRI) could not be retrieved to measure condyle dimensions.
Surgical Indications for OCA
Fresh OCA was selected as the treatment option for these patients based on clinical judgment of defect complexity, defect size, and failure of previous surgical or nonsurgical treatments. Generally, OCA was performed for focal chondral defects ≥2 cm2 diagnosed on MRI or prior arthroscopy. Failure of prior cartilage restoration procedures, such as microfracture, was not a contraindication. Autologous chondrocyte implantation was seldom performed at our institution during the study period, given its 2-stage process and slower rehabilitation compared with OCA.
Patients
A total of 1950 registry patients were screened, and 88 consecutive patients who were treated between 2000 and 2015 met the inclusion and exclusion criteria. Seven patients were lost to follow-up by examination and responses to outcome measures. Allograft data sheets could not be located for 12 patients. As a result, 69 knees from 69 patients were analyzed. Demographic and pre-, intra-, and postoperative data were collected for all patients. Demographic data included age, sex, and body mass index. Preoperative data included the number and type of previous ipsilateral knee surgical procedures and baseline patient-reported outcome scores. Standing lower-limb alignment was assessed and recorded during the preoperative office visit. For the majority of patients, long-leg radiographs were obtained only if gross malalignment was detected and osteotomy was being considered. Intraoperative data included laterality; examination under anesthesia (range of motion, ligamentous stability); location, size, and depth of the chondral defects; concomitant procedures performed; and postoperative rehabilitation protocol. Postoperative data included complications, reoperations, and patient-reported outcome scores at a minimum of 2 years after surgery. A reoperation was defined as any subsequent surgical procedure on the ipsilateral knee, including arthroscopic chondroplasty, removal of loose bodies, lysis of adhesions, and hardware removal. Graft failure was defined as any procedure that involved partial removal of the allograft, revision OCA, or conversion to unicompartmental knee arthroplasty or total knee arthroplasty.
Of the 69 knees, 19 failures (28%) were documented at last follow-up. A power analysis for a case-control study demonstrated that with 19 failures and 50 nonfailures, an AP mismatch ≥3.8 mm could be detected with at least 80% power and an alpha of .05.
Donor-Recipient Matching and Dimension Measurements
Preoperatively, donor allografts were accepted for OCA if the ML dimension of the hemicondyle was equal to or larger than the corresponding dimension of the recipient condyle on standard radiographs or MRI. This was done to ensure that an adequately sized dowel could be harvested. Donor and patient condyles were not matched for laterality (right/left), condyle (medial/lateral), AP dimension, or radius of curvature. 37
Commercial vendor–specific allograft offering documents were retrospectively reviewed to obtain the AP and ML dimensions of the graft, donor age, donor sex, and processed date. To obtain the patient’s condylar dimensions, preoperative MRI was reviewed, and the AP and ML dimensions were measured on axial views at the widest portion of the recipient condyle (Figure 1). If chondral defects on the medial and lateral femoral condyles were treated with OCA, the condyle with the largest defect treated was measured and analyzed.
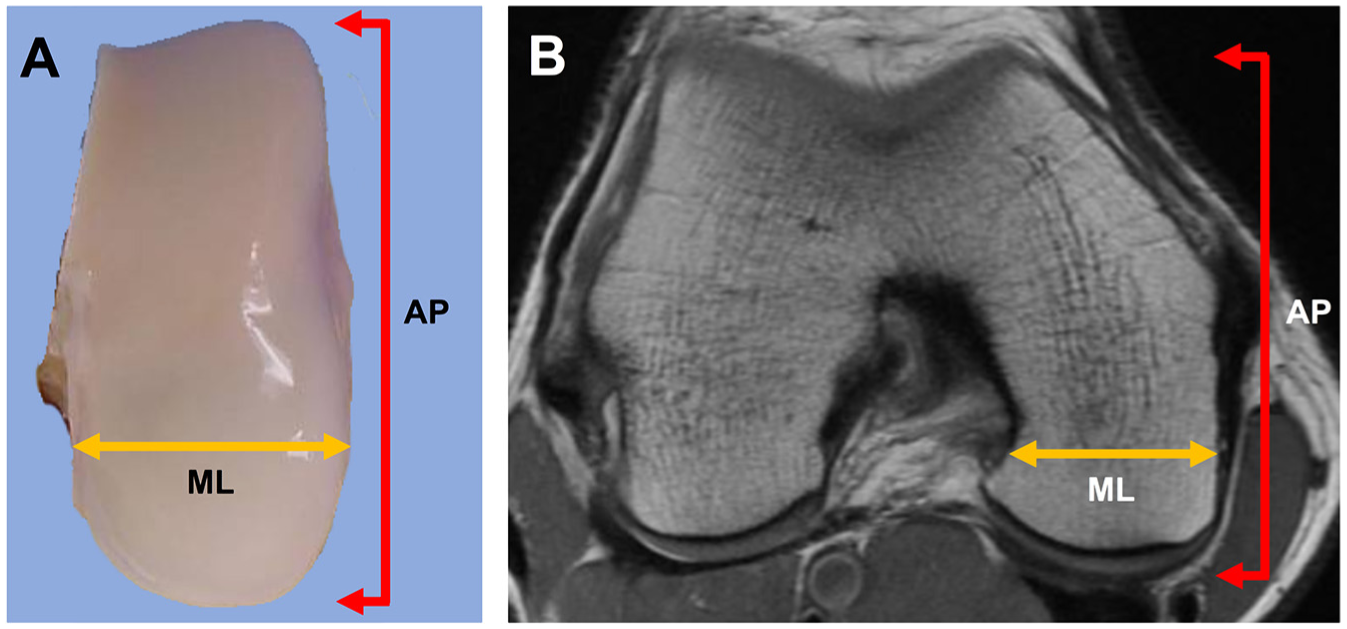
(A) Anteroposterior (AP) and mediolateral (ML) dimensions provided on the commercial source dissection sheets. (B) Corresponding AP and ML dimensions were measured on preoperative magnetic resonance imaging on axial views at the widest portion of the recipient condyle.
Surgical Technique
All surgical procedures that met the inclusion and exclusion criteria were performed by 2 fellowship-trained orthopaedic surgeons at a single institution with extensive experience in OCA. After induction of neuraxial anesthesia and examination of the knee under anesthesia, patients were treated with an initial diagnostic arthroscopy of the joint for assessment of the chondral lesion as well as the other articular surfaces, menisci, and ligaments. Any meniscus tears were addressed with partial meniscectomy or repair.
Fresh cold-stored osteochondral allografts were obtained from commercially available sources. Donor tissue was screened and processed according to American Association of Tissue Banks standards. 26 After the arthroscopic portion of the procedure, OCA was performed via the dowel technique described by Williams et al. 38 Briefly, chondral lesions were exposed via a small parapatellar arthrotomy and debrided to a stable rim. Lesions were then sized and reamed to a bed of normal bone, and an appropriate graft was taken from the corresponding region of the osteochondral allograft. Lesion depth was carefully measured at 3 to 4 points around the lesion, marked, and matched on the donor tissue. Grafts were then gently impacted into place for press-fit fixation. For a single recipient condyle, transplanted grafts consisted of a single dowel or 2 dowels in a stacked configuration (ie, snowman technique), depending on lesion shape.
Postoperatively, patients remained touchdown or nonweightbearing in a hinged knee brace for 1 week, followed by progression to full weightbearing as tolerated. Those treated with concomitant realignment osteotomy were kept touchdown weightbearing for a minimum of 6 weeks. During this initial period, patients were permitted to begin active-assisted range of motion exercises, quadriceps sets, straight-leg raises, and patellar mobilization. Full range of motion was immediately permitted and encouraged with the use of a continuous passive motion device. Brace wear was required for a minimum of 2 weeks, with the total duration of bracing dependent on the restoration of quadriceps control and strength. A supervised physical therapy program was undertaken postoperatively in all cases. The duration of the postoperative physical therapy program depended on the restoration of normal gait, the return of quadriceps function, and the performance of sport-specific skills. Return to higher-level activities and athletics was initiated on an individual patient basis, typically starting with a running program at 6 months. Sports-specific training and unrestricted activities were then progressed thereafter depending on return of lower extremity strength.
Assessment of Clinical Outcomes
The general health outcome for each patient was assessed with use of the 36-Item Short Form Health Survey (SF-36; v 1.0), 29 which evaluates 8 domains of general well-being. The only domains reported in this study were pain, physical functioning, and role limitations due to physical health (hereafter, role limitations). Knee function was assessed with the International Knee Documentation Committee (IKDC) subjective form and the Knee Outcome Survey–Activities of Daily Living (KOS-ADL). The IKDC score is a reliable and valid knee-specific measure of symptoms and function and was shown to provide a good overall measure of knee-related disability among patients who have undergone a cartilage restoration procedure.13,15 Similarly, the KOS-ADL was shown to have high reliability, validity, and responsiveness among athletic patients with various knee conditions. 23 Patient activity level was assessed with the Marx Activity Rating Scale. 24 An independent observer performed postoperative data collection for all clinical outcome instruments. All of these knee-specific outcome instruments were previously used to prospectively evaluate articular cartilage repair procedures of the knee.19,21,23
Statistical Analysis
Comparisons between groups were performed with the independent samples t test for continuous characteristics and the chi-square or Fisher exact test for discrete variables. Kaplan-Meier survivorship analysis was performed for graft failures. A multivariable logistic regression model was fitted to investigate the association of AP mismatch with graft failure while adjusting for patient age and number of previous ipsilateral knee procedures, both of which have been associated with OCA failure.22,36 Donor-recipient AP and ML mismatches and changes in subjective patient outcome scores (SF-36, IKDC, KOS-ADL, Marx Activity Rating Scale) between pre- and postoperative time points were assessed with the paired t test. Two-tailed tests were used for all statistical analyses, with a P value <.05 to indicate significance. All analyses were conducted with SAS (v 9.4; SAS Inc).
Results
The mean patient age was 35.7 years (range, 11-61 years), and the mean duration of follow-up was 4.0 years (range, 2-16 years). Table 1 presents patient demographics and intraoperative data. Twenty knees (29%) had previously undergone a cartilage restoration procedure, including microfracture (n = 13), mosaicplasty (n = 2), autologous chondrocyte implantation (n = 1), synthetic scaffold (n = 3), and decellularized OCA (n = 1). Six knees (9%) were treated with OCA in multiple compartments; 3 (4%) were treated with condylar and patellar OCAs; and 3 (4%) were treated with medial and lateral condylar OCAs. Twenty knees (29%) had ovoid lesions that were treated with OCA in a stacked configuration. For these knees, the mean diameter of the largest dowel was 21.8 mm (range, 15-30 mm), and the mean diameter of the second dowel was 17.9 mm (range, 10-25 mm). Five knees had >5° varus alignment preoperatively and were treated with concomitant opening-wedge valgus-producing high tibial osteotomy. Two knees had >5° valgus alignment preoperatively and were treated with concomitant opening-wedge varus-producing distal femoral osteotomy. For all other patients, alignment was normal, or the mechanical axis did not fall through the region of the planned cartilage restoration procedure.
Patient Characteristics and Intraoperative Data a
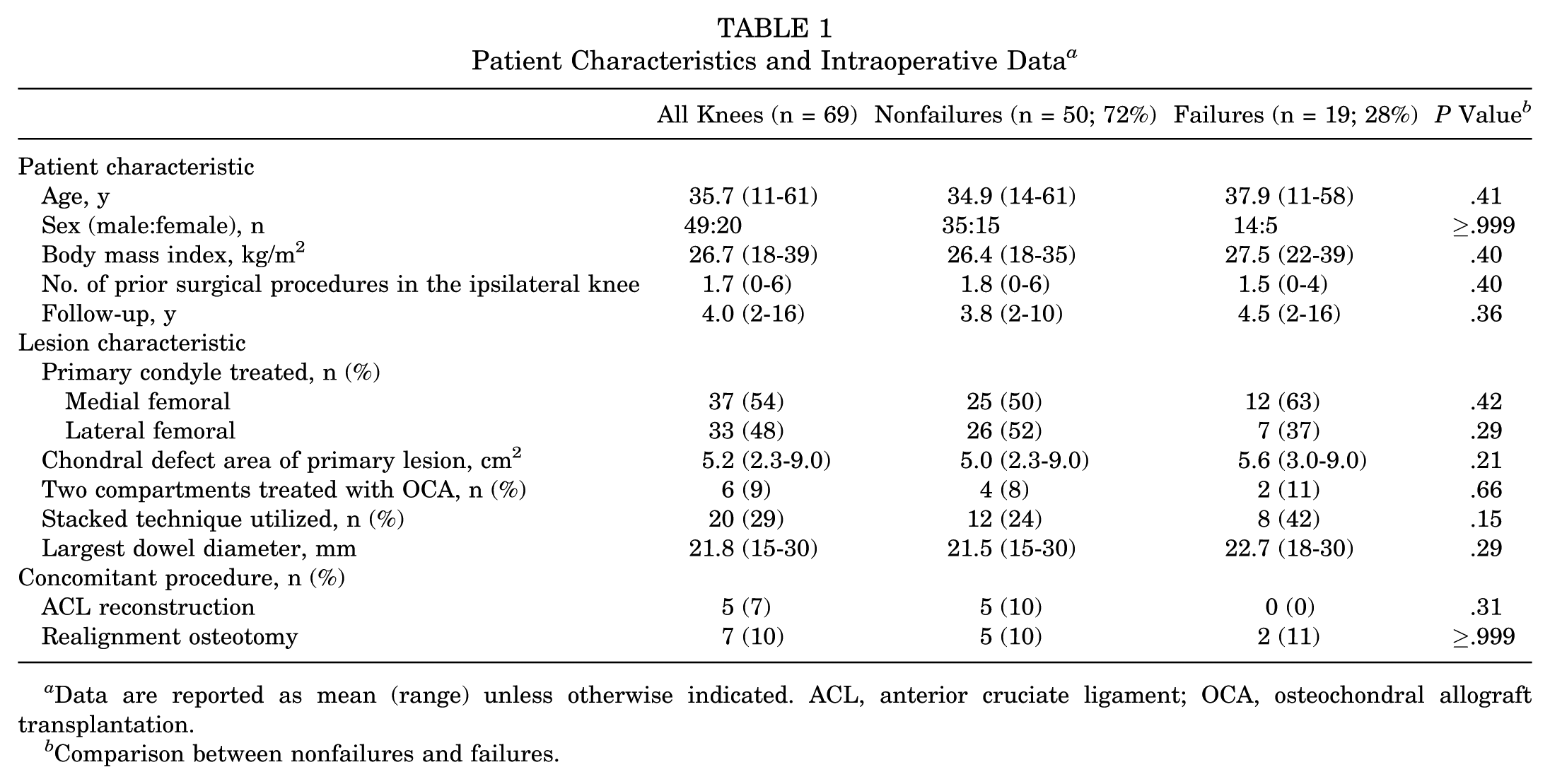
Data are reported as mean (range) unless otherwise indicated. ACL, anterior cruciate ligament; OCA, osteochondral allograft transplantation.
Comparison between nonfailures and failures.
Table 2 presents patient condyle and graft hemicondyle measurements. The mean AP and ML dimensions of the affected patient condyle among all knees were 65.0 mm and 30.9 mm, respectively. The mean AP and ML dimensions among all hemicondyle osteochondral allografts was 69.0 mm and 31.3 mm, respectively. Overall, the mean absolute AP mismatch between graft and patient was 6.7 mm (range, 0-20 mm; P < .01). In contrast, the mean absolute ML mismatch between graft and patient was 2.3 mm (range, 0-10 mm; P = .33). Chondral lesions were treated with grafts from the same condyle in 43 knees (62%) (eg, medial femoral hemicondyle graft for medial femoral condyle chondral lesion). The mean absolute AP mismatch for chondral defects treated with grafts from the same condyle was 6.4 mm (range, 0-18 mm), as compared with 7.2 mm (range, 0-20 mm) for chondral defects transplanted with grafts from the opposite condyle (P = .50).
Patient Condyle and Graft Hemicondyle Osteochondral Allograft Measurements a
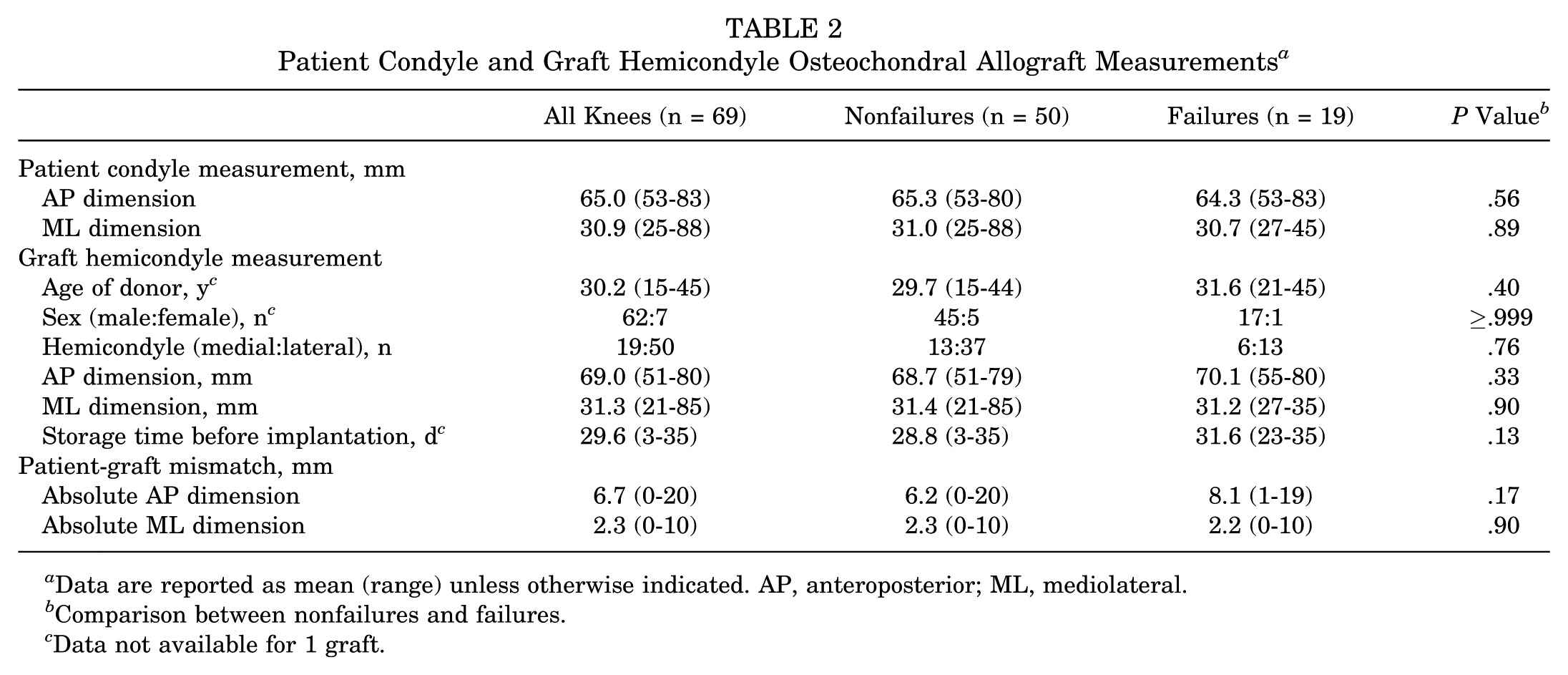
Data are reported as mean (range) unless otherwise indicated. AP, anteroposterior; ML, mediolateral.
Comparison between nonfailures and failures.
Data not available for 1 graft.
Reoperations and Failures
In total, 25 (36%) knees underwent reoperation after OCA. Of these, 6 knees underwent procedures that did not require allograft removal or were unrelated to the index OCA. These procedures included arthroscopic meniscectomy (n = 3), synovectomy (n = 6), and removal of hardware (n = 5). Nineteen failures were documented, with a mean time to failure of 2.6 years (range, 0.8-6.0 years). OCA survivorship was 87% at 2 years and 61% at 5 years (Figure 2). Comparisons of patient demographics, lesion characteristics, and treatment characteristics demonstrated no significant differences between nonfailures and failures (Table 1). The stacked technique for ovoid condylar lesions was used for 24% and 42% of nonfailures and failures, respectively (P = .15), and there was no significant difference in the diameter of the largest dowel transplanted between groups (P = .29). The mean absolute AP mismatches of nonfailures and failures were 6.2 mm and 8.1 mm, respectively, with no significant difference between groups (P = .17) (Figure 3). Additionally, there were no significant differences between nonfailures and failures in the AP and ML dimensions of the patient condyles or hemicondyle grafts, donor age or sex, and graft storage time (Table 2). Failures rates did not differ between knees treated with hemicondyle grafts from the same condyle and the opposite condyle (P = .78). Multivariate logistic regression further demonstrated that the magnitude of AP mismatch was not associated with graft failure (P = .14) while adjusting for patient age and number of prior surgical procedures in the ipsilateral knee (Table 3).
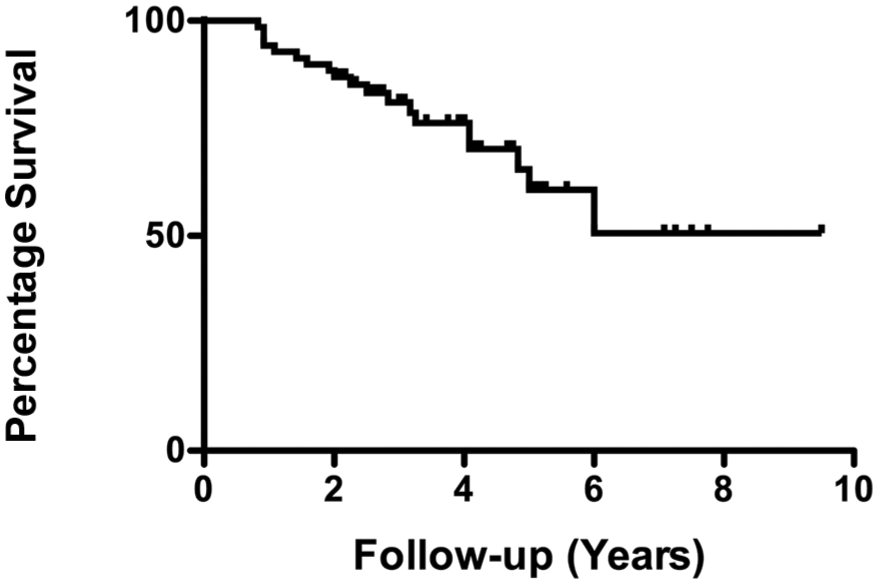
Kaplan-Meier survivorship of osteochondral allograft transplantation among all knees (N = 69).
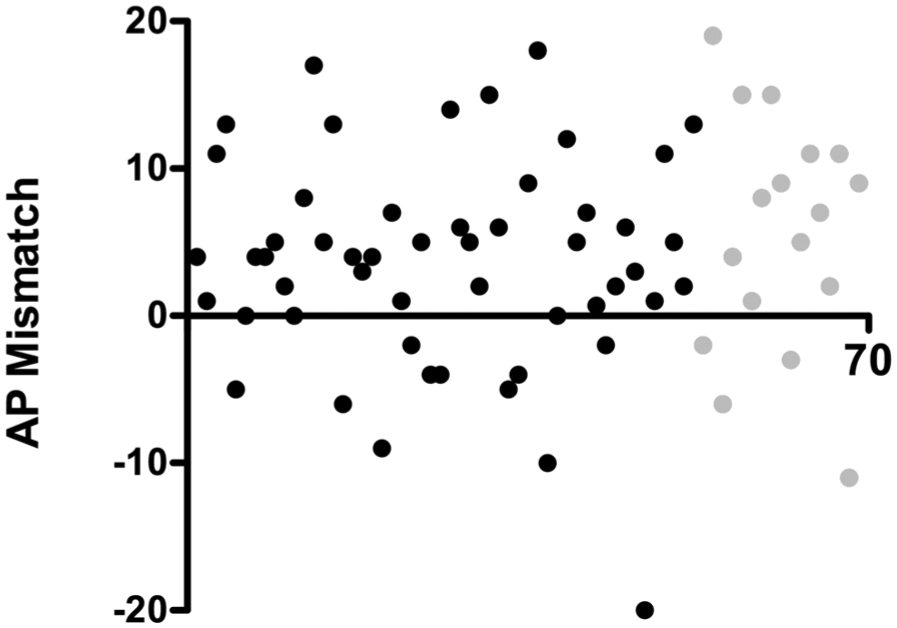
Scatter plot of anteroposterior (AP) mismatch between graft and recipient condyles for all knees (N = 69). Light grey indicates knees that had failed at latest follow-up.
Multivariate Logistic Regression of Patient- and Graft-Related Factors Associated With OCA Failure a
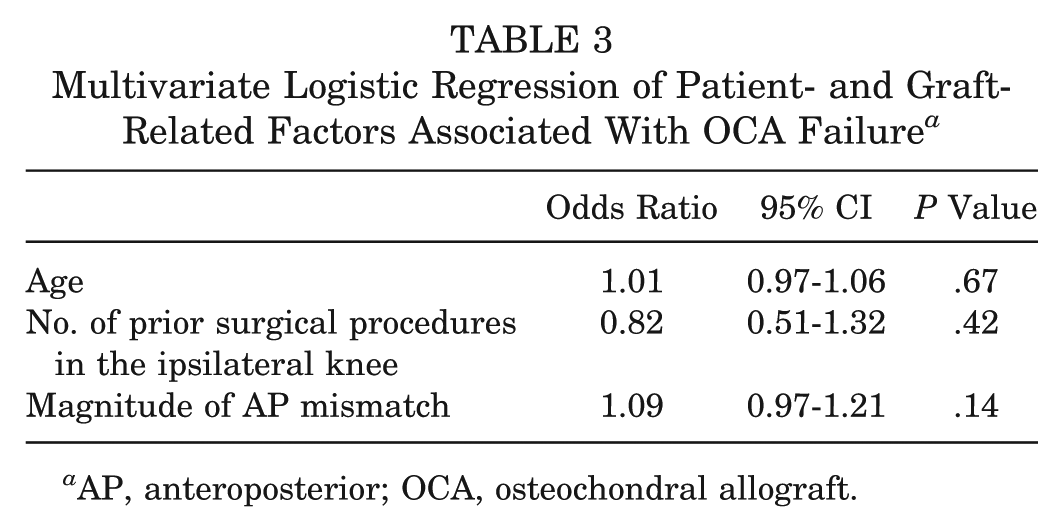
AP, anteroposterior; OCA, osteochondral allograft.
Outcome Scores
Postoperative SF-36 (pain, physical functioning, and role limitations), IKDC, and KOS-ADL scores improved significantly from preoperative scores among all patients (P < .01 for all) (Table 4). The mean score improvements for the SF-36 pain, physical functioning, and role limitations domains were 21.2, 20.0, and 39.8, respectively. Postoperatively, patients achieved a minimal clinically important difference (MCID) of 17.5 on the SF-36 pain, physical functioning, and role limitations domains at rates of 54%, 45%, and 63%, respectively. 10 The mean score improvements in the IKDC and KOS-ADL were 18.1 and 17.8, respectively. Postoperatively, patients achieved MCIDs of 17 and 10 on the IKDC and KOS-ADL at rates of 50% and 63%, respectively (Wang D, Chang B, Coxe FR, et al. “Preoperative Outcome Scores are Predictive of Achieving the Minimal Clinically Important Difference After Treatment of Focal Cartilage Defects of the Knee with Osteochondral Grafts.” Presented at the American Orthopaedic Society for Sports Medicine, 2018). Pre- to postoperative Marx Activity Rating Scale scores decreased significantly among all patients (P = .01).
Pre- and Postoperative Outcome Scores at Final Follow-up a
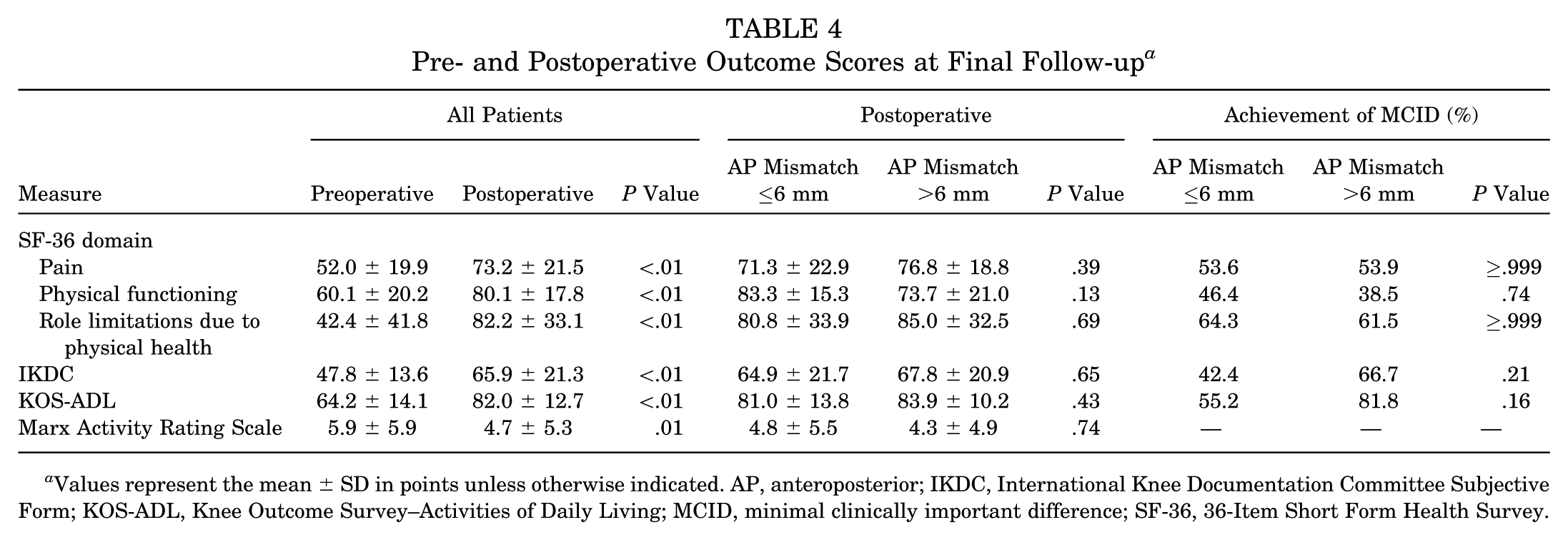
Values represent the mean ± SD in points unless otherwise indicated. AP, anteroposterior; IKDC, International Knee Documentation Committee Subjective Form; KOS-ADL, Knee Outcome Survey–Activities of Daily Living; MCID, minimal clinically important difference; SF-36, 36-Item Short Form Health Survey.
Among all knees, 27 (39%) had an absolute AP mismatch >6 mm between graft and recipient condyles. Comparison of postoperative outcome scores grouped by knees with an AP mismatch ≤6 mm versus >6 mm demonstrated no significant differences (Table 4). Additionally, there was no correlation between an AP mismatch ≤6 or >6 mm and achievement of the MCID on the SF-36 domains (pain, P ≥ .999; physical functioning, P = .74; role limitations, P ≥ .999), IKDC (P = .21), or KOS-ADL (P = .16).
Discussion
In this study of 67 knees treated with OCA, the absolute AP mismatch between graft and patient averaged 6.7 mm and ranged from 0 to 20 mm. At midterm follow-up, there was no significant difference in the average absolute AP mismatch between failures and nonfailures, and multivariate regression demonstrated that magnitude of AP mismatch was not associated with graft failure. Overall, patients reported significant improvements in the SF-36 domains (pain, physical functioning, and role limitations), IKDC, and KOS-ADL, with no correlation between magnitude of AP mismatch and postoperative outcome scores. These results suggest that AP length mismatch within the ranges reported here is not a contraindication for graft acceptance.
Management of articular cartilage defects of the knee remains a difficult clinical problem, especially in young, active patients. OCA has consistently shown excellent long-term results among patients, including high-level athletes, with large chondral defects.2,4,6,11,20,32,35 In the United States, OCA has become more popular as a treatment option in recent years, with an estimated 31% increase in the use of OCA from 2005 to 2009. 27 Despite the excellent results of OCA, there are significant technical and logistic challenges inherent to the technique. Perhaps the most formidable of these is the practice of procuring an appropriately sized allograft that matches the recipient condyle. The cylindrical grafts used in OCA of the femoral condyles necessitate minimal articular step-off to maintain normal or near-normal contact pressures, and an elevation of only 0.5 to 1 mm over the adjacent host cartilage can increase contact pressures on the graft up to 50%.16,17 Increased edge loading of the graft may contribute to early clinical failure. It has long been believed (although not proven) that donor-host matching helps prevent graft-recipient articular incongruity, and many surgeons seek hemicondyle grafts matched to the host laterality, condyle, and AP and ML dimensions. 3 However, absolute size matching restricts the number of compatible osteochondral allografts, thereby delaying treatment and potentially resulting in progression of lesion size. Furthermore, because donor chondrocyte viability gradually declines after graft harvest, 39 up to 13% of harvested grafts are unused and discarded before a suitable host is identified. 28
Recent anatomic studies argued that such precise matching may be unnecessary and that suitable allograft dowels may be harvested from nonmatched donor hemicondyles.3,30,33 There are considerable disparities in the characterization of the normal anatomy of the distal femur, with differences in sphericity and radius of curvature of different locations on the articulating portions of the condyles.8,18,31,34 Matching AP and ML diameter, as commonly practiced for OCA by surgeons and commercial vendors, seems likely insufficient to account for the complex 3-dimensional variations in condylar surface anatomy. We have believed for some time that any graft appropriately contoured to fill a defect with minimal articular step-off would produce results similar to those of size-matched grafts. Currently, the only criterion that we use to accept donor allografts for OCA is for the ML dimension of the hemicondyle to be equal to or larger than the ML dimension of the recipient condyle, which ensures that an adequately sized dowel can be harvested. In our experience, although AP dimension is correlated with the radius of curvature for a given condyle, any AP mismatch, indicating a corresponding mismatch in the radius of curvature, is unlikely to result in significant articular incongruity after implantation, particularly with use of smaller-diameter dowels or when 2 adjacent dowels are implanted with a stacked technique. In this study, the failure group did not have larger dowel sizes than the nonfailure group, and the stacked technique was utilized more frequently in the failure group (42% vs 24%), although not statistically significant. This may indicate a clinically important increased risk of failures with the stacked graft technique that this study did not have the statistical power to detect. Other factors, such as the angle and depth of the harvested osteochondral plug versus that of its recipient socket, are likely more important in resurfacing a defect with minimal step-off.
The results of the present study support the preferred approach of the senior authors. A recent study by Wang et al 37 reported no difference in graft failure and patient-reported outcomes between patients treated with condyle-specific matched and unmatched OCA. Similarly, in this study, we found no association between AP mismatch and graft failure when controlling for age and number of prior ipsilateral knee procedures. The failure rate of OCA in this patient cohort is consistent with the failure rates reported in prior studies that used size-matched donor grafts.1,4,12 Most important, patient-reported outcome measures improved significantly over the course of follow-up, despite a wide range of AP mismatch between graft and patient. Patients on average reported a decrease in postoperative Marx activity scores, which is consistent with other reports in the literature.19,36,37
There are several limitations to this study. As with any retrospective cohort study, there was no process for randomization in treatment or comparison with a predetermined control group. However, the magnitude of AP mismatch was governed solely by allograft availability rather than surgeon preference, which provided for some degree of randomization in the magnitude of mismatch. This study was subject to selection bias, as all patients were treated by 2 experienced surgeons at a single institution performing a high volume of OCAs, thereby reducing the generalizability of these findings to other settings. Although the average difference in AP mismatch between failures and nonfailures (1.9 mm) was less than the statistically significant difference that could be detected according to our power analysis (3.8 mm), indicating potential type II error, these values are well within the margin of error for measurement of AP length of the gross specimen and on MRI. Additionally, we were unable to quantify the degree of articular congruity intra- or postoperatively. Although we made every effort to minimize incongruity intraoperatively, we were unable to directly correlate this with AP mismatch, which would have strengthened our conclusions. The majority of patients did not have preoperative long-leg standing radiographs (ordered per the surgeon’s discretion), which precluded a more accurate quantification of lower-leg alignment in this study. Preexisting level of osteoarthritis, which may influence the risk of graft failure and postoperative patient-reported outcomes, was not factored into the analysis. Finally, our study population was not strictly homogeneous, with 29% who had undergone previous surgery and 10% who received a concurrent tibial or femoral osteotomy. Nevertheless, the role of specific previous or concurrent procedures on the final outcome is unknown, and prior published studies reported good outcomes after previous or concurrent osteotomies.9,14
In conclusion, magnitude of graft-recipient AP mismatch was not associated with OCA failure or patient-reported outcome scores at midterm follow-up. While commercial allograft vendors continue to provide the AP and ML dimensions of the hemicondyle grafts for surgeons to perform graft-recipient size matching, these results suggest that any AP length mismatch within the limits measured here is not a contraindication for graft acceptance.
Footnotes
Presented as a poster at the annual meeting of the AOSSM, San Diego, California, USA, July 2018.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.J.W. receives intellectual property royalties from Arthrex, Inc, and is a paid consultant for Arthrex, Inc, and JRF Ortho. S.A.R. is a paid consultant for JRF Ortho and receives royalties from Zimmer Biomet. K.J.J. has received education payments from Arthrex, Inc, honoraria from MTF, and hospitality payments from Aesculap Biologics.