
Abstract
Background:
The arthroscopic Latarjet-Bristow procedure is emerging as a reliable alternative to the open procedure. The reduced soft tissue damage with potential advantages of early pain control and functional recovery is attractive. However, the operation is technically more demanding, and there are concerns regarding the potential for increased recurrence and complication rates.
Purpose:
To evaluate the available literature focusing on the reported functional outcomes and complications of the arthroscopic Latarjet procedure and compare them with the open procedure.
Study Design:
Systematic review and meta-analysis.
Methods:
A comprehensive systematic review was performed with the keywords “arthroscopy,” “arthroscopic,” “Latarjet,” and “Bristow,” with no limit regarding the year of publication. The review was limited to the English-language articles, and each article was evaluated with a modified MINORS (methodological index for nonrandomized studies) scoring system.
Results:
Fourteen studies met the inclusion criteria and were included in the review. Overall, 813 patients met inclusion criteria, with a mean follow-up of 24.5 months. The mean Walch-Duplay and Rowe scores were 89.6 and 90.2, respectively. The overall complication rate was 16.5%; intraoperative conversion to open surgery, 2%; recurrence, 2.5%; and revision surgery, 5.6%. When only comparative studies were considered, the overall complication rates were 23.7% (arthroscopically) and 15.3% (open). The recurrence and revision surgery rates were 6.5% and 5.7% in the study group, while the corresponding values in the control group were 4% and 2.9%. The mean MINORS score was 14.5 (11.6 for noncomparative studies and 19 for comparative studies).
Conclusion:
The arthroscopic Latarjet-Bristow procedure is reliable. Outcomes are satisfactory, with less pain and faster recovery in the first postoperative week. However, the procedure is technically demanding, and higher rates of complications and reoperations should be expected. Finally, the arthroscopic operation is much more expensive in terms of implanted materials than the open procedure.
Shoulder dislocation is the most common dislocation among the major joints. 31 Surgical treatment is generally advocated to prevent recurrence and additional anatomic lesions. Despite improvements in techniques and instrumentation, the results of arthroscopic soft tissue repairs have not yet equaled those obtained with open techniques in some reported studies.16,24,29 High failure rates have been reported after arthroscopic repair in cases of bony deficiency, humeral avulsion of the glenohumeral ligaments, contact sports, and revision of previous soft tissue reconstructions.7,17,18,27 The Latarjet-Bristow procedure has risen to a possible gold standard in those situations, with a reported recurrence rate varying from 0% to 8%. 3 However, some concerns are still present regarding potential damage to the subscapularis muscle and around the accuracy of bone block positioning. Improper placement of the coracoid graft and screws has been reported in up to 50%. 35 Improper graft and screw placement has a dramatic effect on final outcomes, since it can lead to either early osteoarthritis, when the bone block overhangs the glenoid rim, or recurrence of instability, when it is placed too medial or proximal. 1 The arthroscopic Latarjet procedure was introduced to improve graft positioning, to reduce surgical dissection, and to allow easy identification and treatment of associated lesions (eg, labral and rotator cuff tears). Although the first arthroscopic Latarjet study showed promising results with a 0% rate of recurrence,22,23 skepticism remains regarding the increased operative time with the additional intraoperative complications, increased costs, and question of whether there are functional advantages over the traditional mini-open approach. Some authors claimed that complete anterior capsulectomy and extensive split of the subscapularis fibers laterally to the insertion on the lesser tuberosity (which is required in the arthroscopic approach) are actually more invasive than the traditional open operation. 36 The aim of the present systematic review and meta-analysis was to critically evaluate the available literature to report functional outcomes and complications of the arthroscopic Latarjet-Bristow procedure. It was hypothesized that this operation yields outcomes and complication rates similar to those of the traditional open procedure. In addition, the available literature was assessed through the MINORS (methodological index for nonrandomized studies) score, which was designed for nonrandomized surgical studies.
Methods
A comprehensive literature search was performed on September 22, 2017, with the following databases: PubMed, EMBASE, and Ovid (MEDLINE). The search terms included “arthroscopy,” “arthroscopic,” “Latarjet,” and “Bristow” with no limit regarding the year of publication. The inclusion criteria comprised therapeutic studies written in English. Although randomized controlled trials and prospective case series are the most relevant designs, the majority of the available literature consists of lower-level studies. Therefore, no limitation was set on the level of evidence, follow-up duration, or number of patients enrolled. Prospective and retrospective studies reporting clinical outcomes and complications were included, whereas reviews, technical notes, and case reports were excluded. Two independent surgeons screened all titles and abstracts, and the full text of any relevant abstract was retrieved. In addition, the reference lists of all the retrieved full texts were checked manually for any additional relevant study that may have been missed with the first search. The initial search resulted in 367 articles; at the end of the screening, 14 studies were available for review of outcomes and complications and methodological assessment (Figure 1).
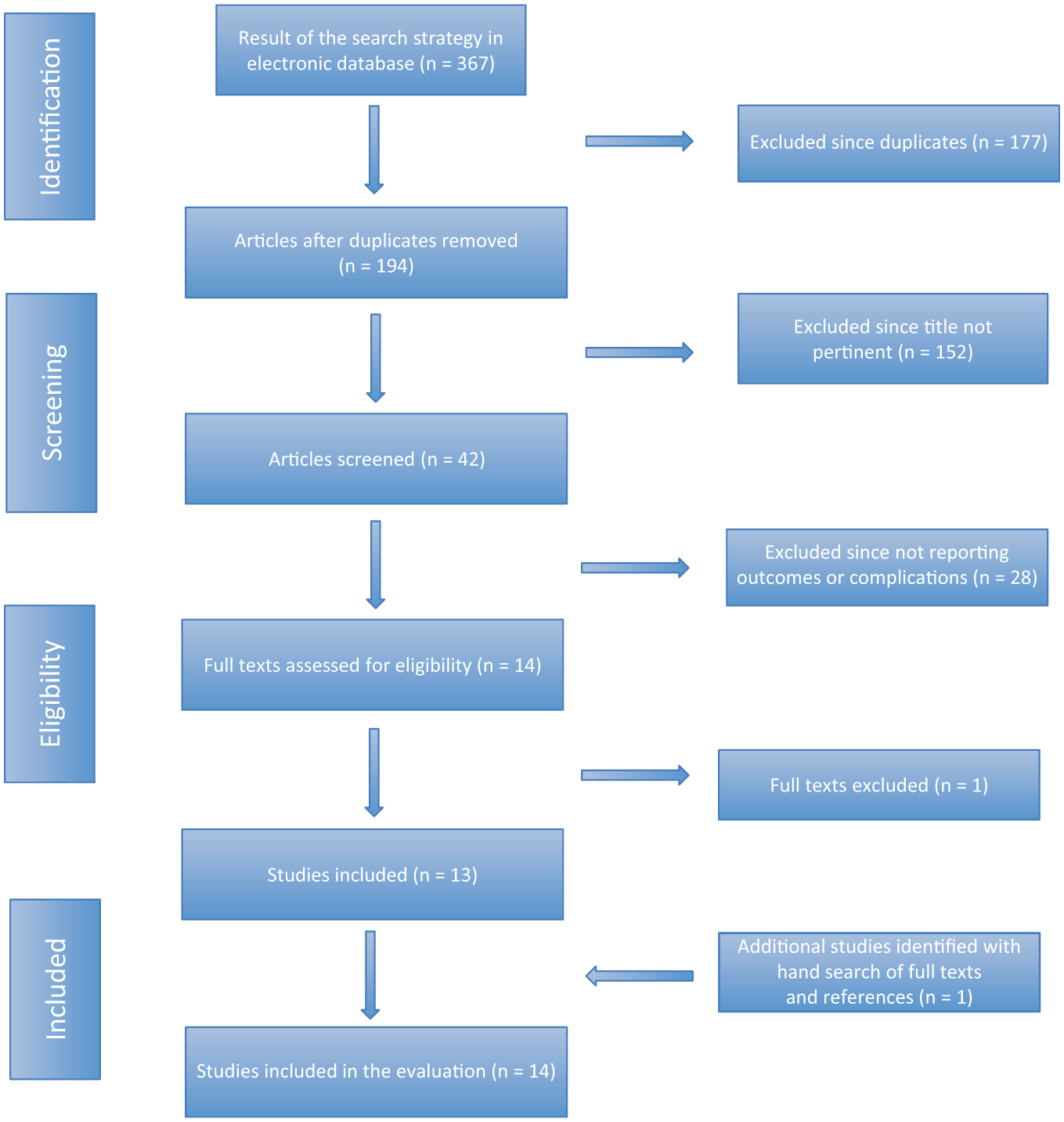
PRISMA (Preferred Reporting Items for Systemic Reviews and Meta-Analyses) flow diagram showing the systematic review of the literature for the arthroscopic Latarjet procedure.
Although the study by Ranne et al 33 was lacking on clinical outcomes, it was included in the review because of the important information that it provided regarding recurrence rate, reoperation rate, and complications. The study by Metais et al 26 included 2 study groups (arthroscopic Latarjet with screws and arthroscopic Latarjet with an Endobutton device), so these were considered independent studies. The evaluation was completed with the MINORS instrument. The MINORS scoring system was designed to assess the methodological quality of comparative and noncomparative nonrandomized surgical studies. 34 It consists of 8 items for noncomparative studies with 4 additional items for comparative studies. The items are scored 0 when information is not reported, 1 when it is reported but inadequate, and 2 when it is reported and adequate. Therefore, the maximum ideal score is 16 for noncomparative studies and 24 for comparative studies, while the worst score is 0.
Data Synthesis and Statistical Analysis
Review Manager software (v 5.3; Cochrane Collaboration) was used for the meta-analysis. Extracted data were entered into Review Manager by the first independent author and checked by the second independent author. The effect sizes were computed by a random effects model according to the heterogeneity among groups. Dichotomous effect sizes (imaging and clinical complications) were expressed as event rates. A 95% CI was determined for each effect size.
Heterogeneity—defined as variability among studies secondary to true differences among studies, instead of sampling error—was assessed with the Cochran Q test (χ2) and the Higgins I2 value. An I2 value was interpreted as follows: 0%-25%, low heterogeneity; 25%-75%, moderate heterogeneity; and 75%-100%, high heterogeneity. All results are presented as forest plots (Figures 2 and 3).

Forest plot of the comparison of imaging complications between the arthroscopic group and the open group. M-H, Mantel-Haenszel.

Forest plot of the comparison of clinical complications between the arthroscopic group and the open group. M-H, Mantel-Haenszel.
Sensitivity Analysis
To explore potential sources of heterogeneity and assess the robustness of the results, a sensitivity analysis was conducted by excluding 1 study in each round and evaluating the influence of any single study on the primary meta-analysis estimate.
Results
Study Characteristics
Patient demographic data are summarized in Table 1.
Characteristics of Included Studies and Patients a
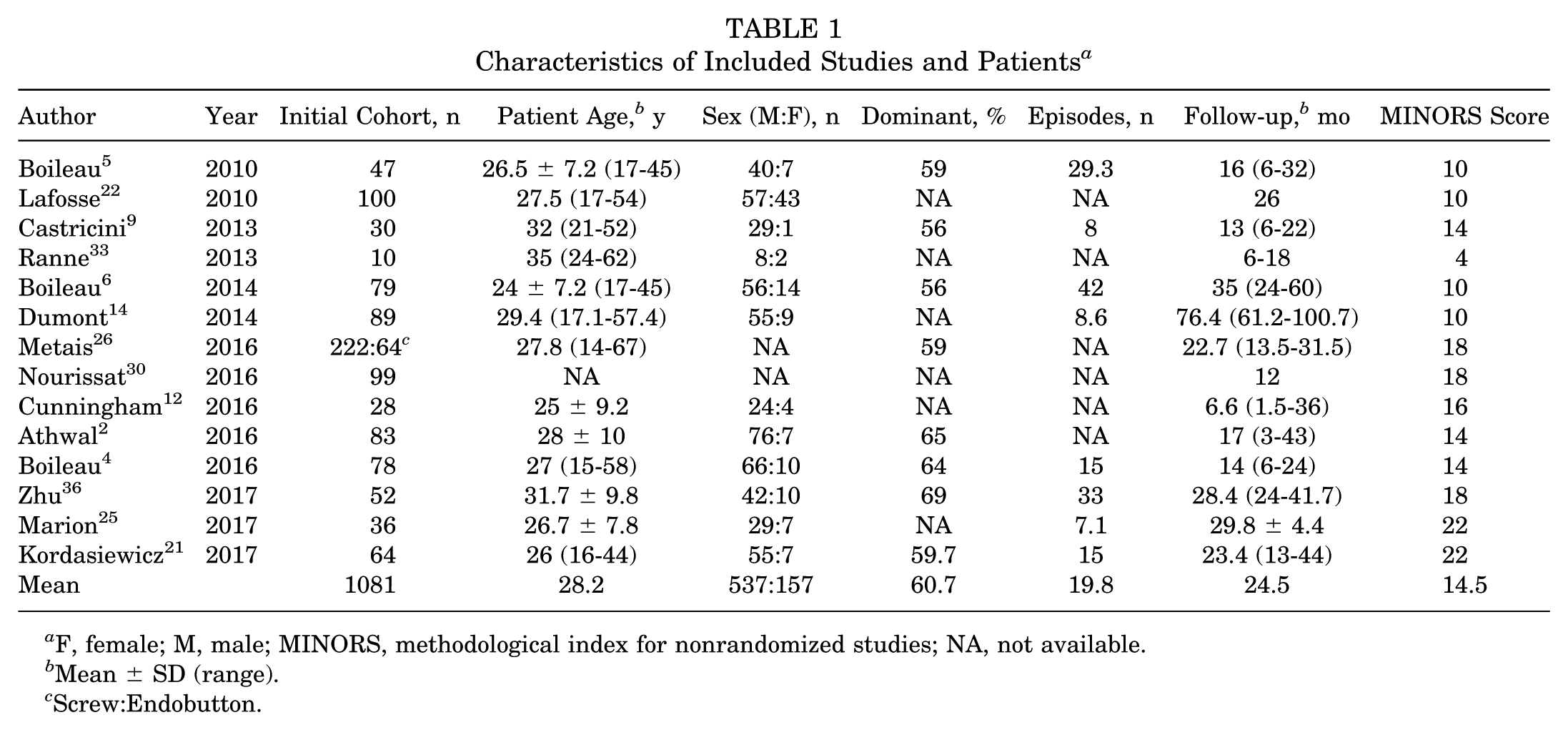
F, female; M, male; MINORS, methodological index for nonrandomized studies; NA, not available.
Mean ± SD (range).
Screw:Endobutton.
The initial cohort included 1081 patients after the arthroscopic Latarjet or Bristow procedure. Ten patients were converted to open surgery during the index procedure. Additionally, 258 patients were lost at follow-up, thus leaving 813 patients for clinical evaluation. The male:female ratio was 537:157, with the dominant arm being involved in 60.7% of cases. The mean number of instability episodes (dislocations and subluxations) before surgery was 19.8. The coracoid bone block was fixed with screws in all studies with the exception of 1 by Boileau et al 4 and 1 of the 2 cohorts of the study by Metais et al, 26 where an Endobutton system was used.
Outcome and complications are summarized in Table 2.
Outcomes and Complication Rates of the Included Studies a
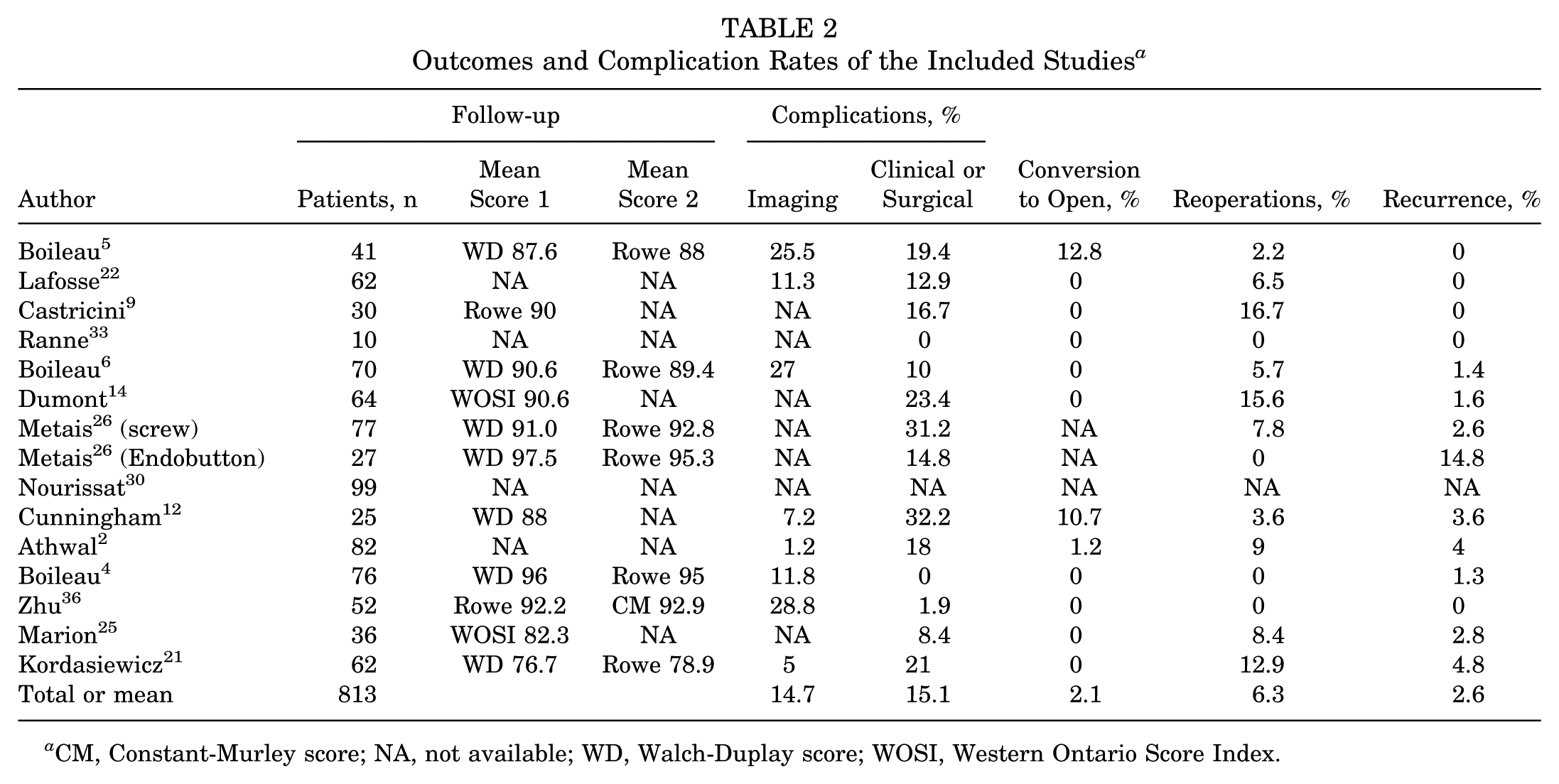
CM, Constant-Murley score; NA, not available; WD, Walch-Duplay score; WOSI, Western Ontario Score Index.
At a mean follow-up of 24.5 months, 781 patients were available for clinical evaluation. Outcomes were assessed with the Walch-Duplay (WD) score,4-6,12,21,26 Rowe score,4-6,9,12,21,26,36 Constant-Murley score, 36 and Western Ontario Score Index.14,25,30 Two studies reported complications but not clinical outcomes.2,22 The mean WD score was 89.6; Rowe score, 90.2; Constant-Murley score, 92.9; and Western Ontario Score Index, 86.4.
Complications
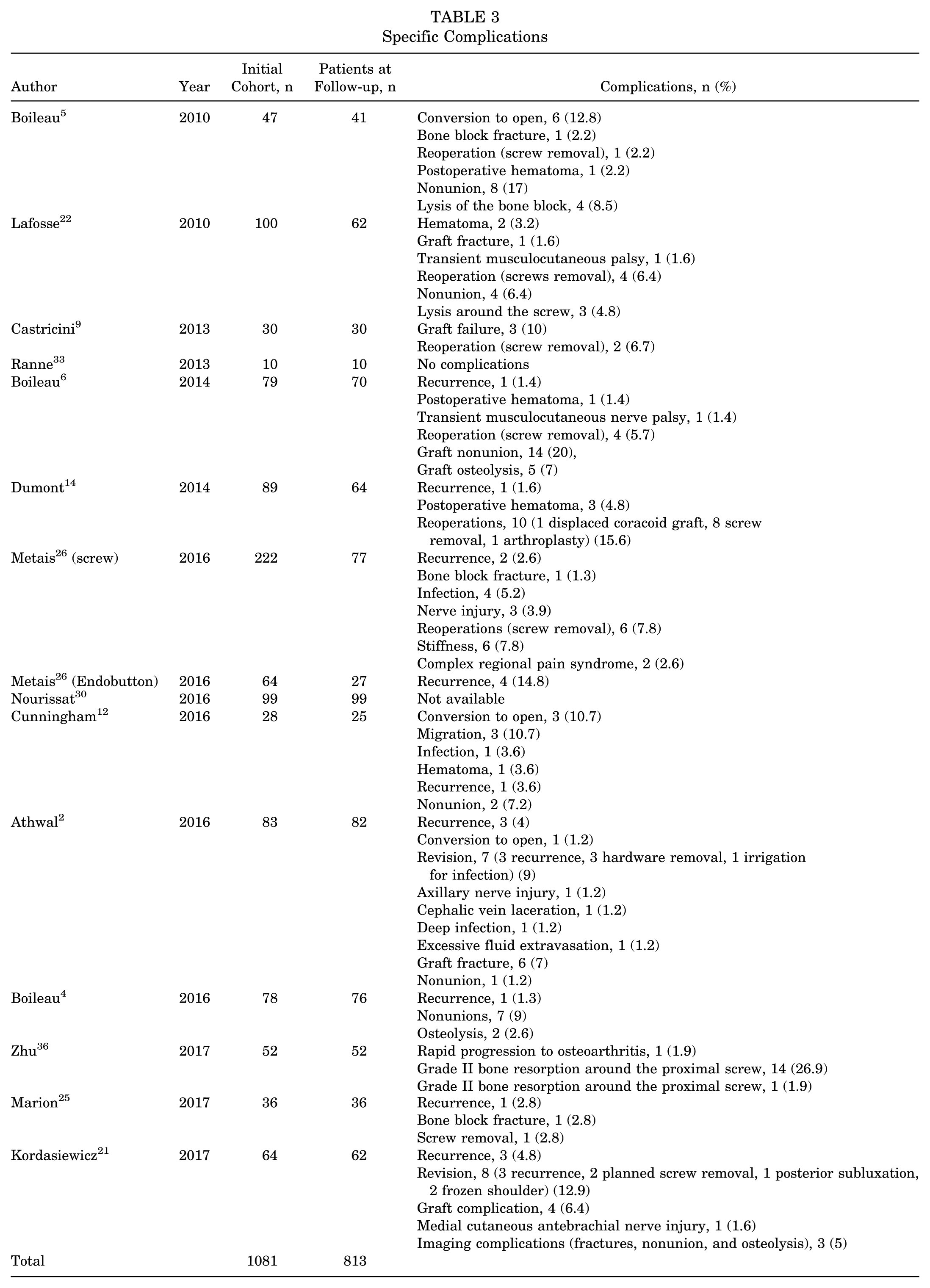
Complication rates are reported in Table 2, while specific complications are reported in Table 3. Complications were considered as follows: imaging complications (lysis and nonunion) and clinical/surgical complications (conversion to open surgery, recurrence of instability, revision procedures, and local and general complications). When in reference to the same patient, recurrence of instability or a postoperative complication that led to revision surgery was recorded, but this was considered a single complication. The imaging complication rate (lysis or nonunion) was 14.7%. The clinical/surgical complication rate was 15.1%; rate of intraoperative conversion to open surgery, 2.1%; recurrence rate, 2.6%; and reoperation rate, 6.3%.
Specific Complications
Methodological Evaluation
We identified 10 case series and 4 case-control studies. The overall mean MINORS score was 14.5 (range, 4-22). For noncomparative studies, the mean MINORS score was 11.6 (range, 4-18); for comparative studies, 19 (range, 16-22).
Arthroscopic vs Open Latarjet
Four studies compared the outcomes and complications of the arthroscopic and open Latarjet procedures12,21,25,26 (Metais et al 26 had 2 study groups) (Tables 4 and 5).
Patient Demographics in the Studies Comparing Arthroscopic and Open Latarjet Procedures a
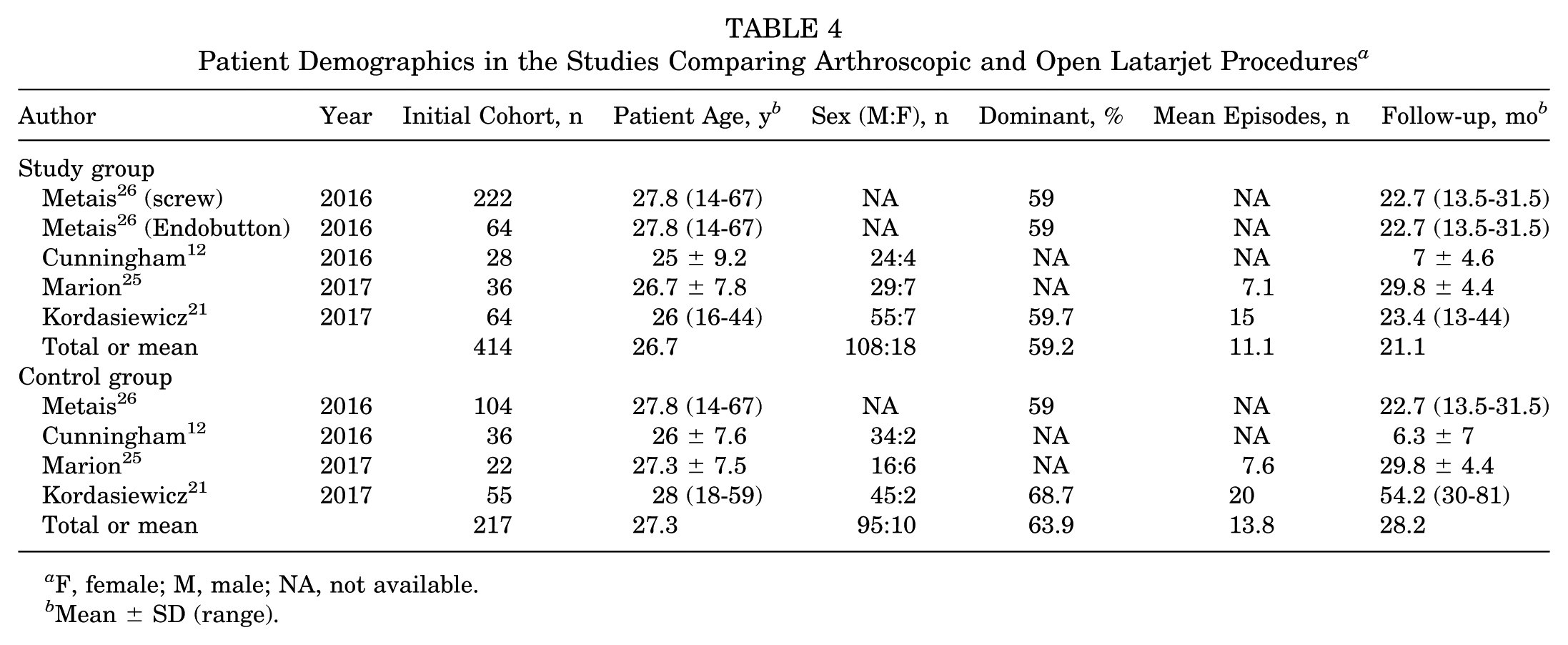
F, female; M, male; NA, not available.
Mean ± SD (range).
Outcomes and Complication Rates of the Studies Comparing Arthroscopic and Open Latarjet Procedures a
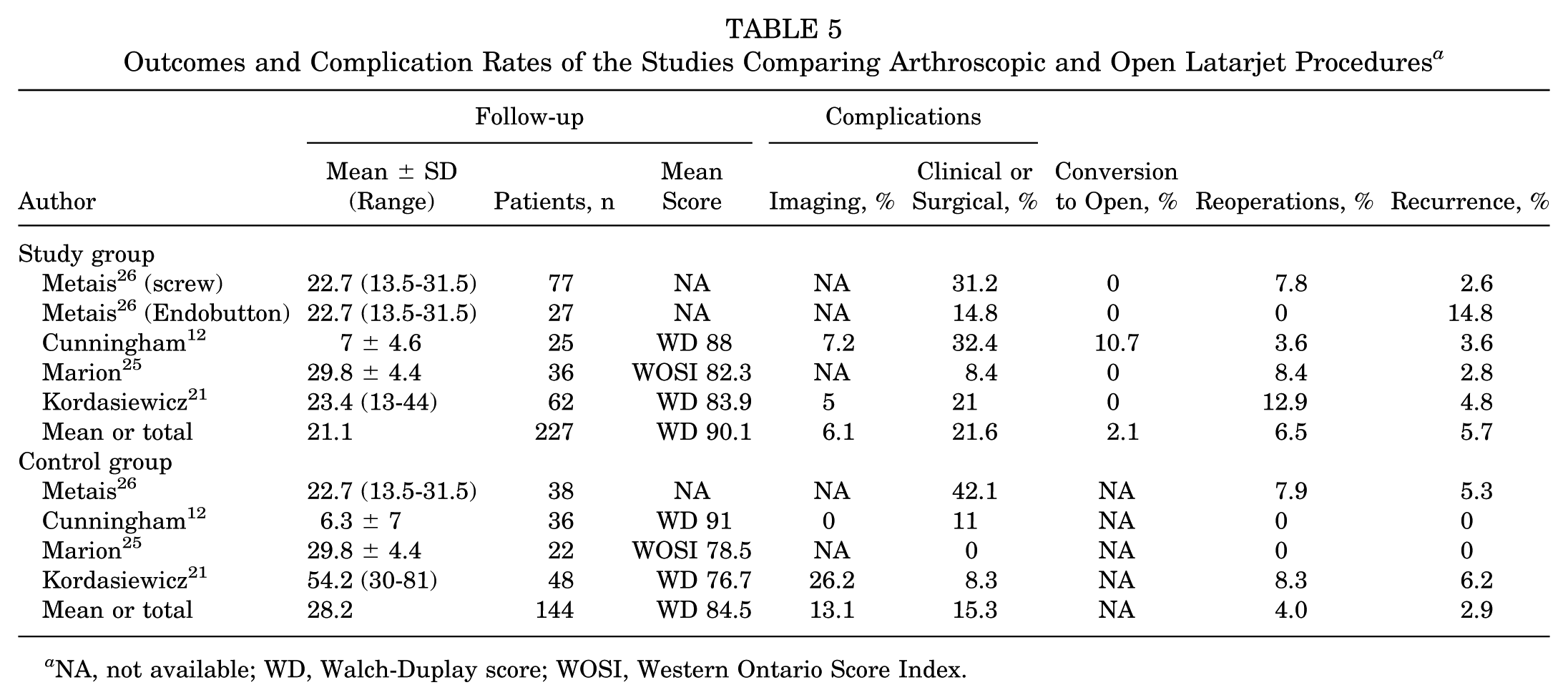
NA, not available; WD, Walch-Duplay score; WOSI, Western Ontario Score Index.
The initial cohort in the study group (arthroscopic) consisted of 414 patients, while the cohort in the control group (open) comprised 217 patients. In the study group, 227 patients were available for evaluation at a mean follow-up of 21.1 months. The mean age at the time of index procedure was 26.7 years, and the male:female ratio was 108:18. The dominant arm was involved in 59.2% of cases, and the mean number of instability episodes was 11.1. In the control group, 144 patients were reviewed at a mean follow-up of 28.2 months. The mean age at the time of index procedure was 27.3 years, and the male:female ratio was 95:10. The dominant arm was involved in 63.9% of cases, and the mean number of instability episodes was 13.8. The mean WD score was 90.1 in the study group and 84.5 in the control group. The rates of imaging complications were 6.1% and 13.1%, and the rates of clinical/surgical complications were 21.6% and 15.3%, respectively. A conversion to an open procedure was necessary in 2.1% of arthroscopic cases. Recurrence and revision surgery rates were 6.5% and 5.7% in the study group, as opposed to 4% and 2.9% in the control group, respectively.
Imaging Complications
Only 2 studies compared rates of imaging complications between the arthroscopic group and the open group in terms of the Latarjet procedure, including 171 patients. There was no significant difference in the risk of complications between the arthroscopic and open Latarjet groups (risk ratio, 0.90; 95% CI, 0.33-31.31; P = .95). A high level of heterogeneity among the studies existed (P = .03, I2 = 80%).
Clinical/Surgical Complications
Only 5 studies compared rates of clinical complications between the arthroscopic group and the open group in terms of the Latarjet procedure, including 409 patients. There was no significant difference in the risk of complications between the arthroscopic and open Latarjet groups (risk ratio, 1.04; 95% CI, 0.33-3.23; P = .95). A high level of heterogeneity among the studies existed (P < .0001, I2 = 83%).
Sensitivity Analysis
To evaluate the stability of the results of the meta-analysis, sensitivity analyses were performed through sequentially omitted individual studies. All the results were not materially changed, which suggested the robustness of the results.
Discussion
This study highlights several important findings regarding the arthroscopic Latarjet procedure. A key finding is its reliability. Functional outcomes are excellent, with a mean WD score of 89.6 and Rowe score of 90.2 at final follow-up. Even when compared with the open technique, the arthroscopic approach yielded positive outcomes, with mean WD scores of 90.1 and 84.5, respectively. The difference seems to be more relevant in the first postoperative days (within 7 days), with reduced pain 30 and consumption of analgesics. 25 Another important finding is related to the complication rate. In the present review, some parameters were considered: rate of conversion to open technique, recurrence rate, reoperation rate, and overall complication rate. The imaging complication rate included osteolysis and nonunion of the grafts. The clinical/surgical complication rate included local and general complications, reoperations, and recurrences. Reported complications included hematomas, musculocutaneous nerve problems, glenohumeral joint stiffness, screw migration, graft rupture, delay in wound healing, and infection. The reported rate of conversion to open surgery was 2.1% among arthroscopic cases, with the majority being the first cases of each study. This finding was shown to be related to the learning curve of such a technically demanding procedure. The imaging complication rate was 14.7%, whereas the clinical/surgical complication rate was 15.1%; the recurrence rate, 2.6%; and the reoperation rate, 6.3%. When only comparative studies were considered, the imaging and clinical complication rates were 6.1% and 21.6% (arthroscopic) and 13.1% and 15.3% (open), respectively. Recurrence rate and revision surgery rates were 6.5% and 5.7% in the arthroscopic cohort while the corresponding values in the open cohort were 4% and 2.9%.
The Latarjet-Bristow procedure has emerged in the past few decades as a potential gold standard treatment for instability cases with severe bone loss, contact sport athletes, and revision instability cases. Satisfactory results with low recurrence rates were shown after the Latarjet procedure in these circumstances.7,11 However, some surgeons are still concerned about the effect of the Latarjet technique on the local anatomy and function, since it is a nonanatomic procedure.13,15 More recent studies showed that the procedure has a limited effect on shoulder function 10 but leads to anatomic alterations as a consequence of the pectoralis minor detachment, coracoid transposition, and soft tissue dissection of the open approach. The arthroscopic Latarjet procedure was first introduced by Lafosse et al 23 to decrease this anatomic damage. After the initial arthroscopic Latarjet series, several authors proposed surgical technique variations and reported promising outcomes and an improvement in complications. However, there are still some concerns regarding the complexity of the arthroscopic Latarjet technique. Many surgeons still find the open Latarjet procedure to be challenging and fraught with complications, and the arthroscopic technique is more challenging.
First of all, the operative time for the arthroscopic Latarjet procedure has been reported to be longer than that of the open Latarjet technique. Casabianca et al 8 reported a mean operative time of 161 ± 34.8 minutes. Similar data were reported by Cunningham et al 12 (146 minutes for the arthroscopic group and 81 minutes for the open group), although the operative time decreased with experience and learning curve to approximately that of open surgery. Castricini et al 9 also highlighted the importance of the learning curve to reduce operative time and decrease the rate of complications. Therefore, less experienced surgeons should carefully select their patients; the arthroscopic approach should be avoided for patients who have increased risk of cerebral ischemia induced by prolonged hypotension. 20
Another concern regarding the arthroscopic approach is related to the placement of the coracoid graft. It is now clear that lateral overhang of the coracoid graft leads to postoperative arthritis, while a medialized coracoid is associated with recurrent instability.19,28 The analysis of the literature is encouraging on this issue. Marion et al 25 reported a correct positioning of the graft to the anterior aspect of the glenoid with the arthroscopic technique. In addition, they found that the position of the bone block was significantly more flush to the glenoid edge and inferior in the arthroscopic group than in the open group. Similarly, Boileau et al 4 showed that their arthroscopically placed grafts were congruent with the glenoid articular surface in 96% of cases, with only 3 patients having a lateral overhang of the bone block. Casabianca et al 8 demonstrated that their coracoid blocks were positioned flush in 32% of cases, congruent in 38%, medial in 30%, and too medial in 6%. No lateral overhang was reported.
Another crucial aspect is the healing of the coracoid graft. Boileau et al 4 showed a union rate of 91% of cases and a fibrous union in 9% on a computed tomography scan evaluation at 6 months after arthroscopic Latarjet surgery. Graft osteolysis was reported for 2 patients. The authors concluded that smoking was the only significant risk factor for nonunion of the graft. Zhu et al 36 reported a variable rate of bone block resorption in a computed tomography scan evaluation at postoperative 1 year—specifically, 82.7% for the arthroscopic cases, which was lower than the 90.5% reported for the open technique. 37 The authors suggested that the difference could have been due to the better blood supply from the conjoint tendon and the better mechanotransduction in the distal part of the coracoid in arthroscopic procedures. The difference of the healing rate between open and arthroscopic techniques was confirmed in the study by Kordasiewicz et al. 21 They found healing problems in 26.2% of open cases and 5% of arthroscopic cases, suggesting that the difference could have been related to the reduced damage to graft healing potential with the arthroscopic approach. On the contrary, partial graft osteolysis was significantly more frequent after arthroscopy (53.3%) than after the open technique (23.8%).
The last notable aspect is related to the costs and reimbursement of both procedures. Randelli et al 32 calculated the direct costs of the arthroscopic Latarjet procedure to be $2741, while the corresponding costs for the open operation were $1221. The cost comparisons are particularly relevant in those countries where a policy of cost reduction has been adopted.
The present study has some notable limitations. First, although several databases were accessed with different combinations of appropriate keywords, it is possible that some articles may not have been included in our search. Second, the majority of the available studies are case series with no control group; this could reduce the scientific relevance of the reported data. Third, when considering complications, we defined clinical/surgical complications and imaging complications. In some studies, these data were reported as numbers of cases and in other studies, as percentages. When they were reported as number of cases, the percentage was then calculated from the total number of patients at follow-up rather than from the initial cohort. This may have overestimated the percentage in some studies. Finally, it should be highlighted that, to date, the outcomes and complications of the arthroscopic Latarjet procedure have been reported only by master surgeons. This aspect could be a bias; therefore, other shoulder surgeons should confirm these promising results to draw more definitive conclusions. Nonetheless, the present review concludes that the arthroscopic Latarjet technique yields satisfactory functional outcomes with recurrence and reoperation rates comparable with those of the open technique. However, the complication rate is higher for the arthroscopic Latarjet procedure, which is reflective of the more technically demanding arthroscopic procedure with a prolonged learning curve. These aspects should be kept in mind when selecting candidates for arthroscopic Latarjet surgery.
Conclusion
The arthroscopic Latarjet-Bristow procedure is reliable. Postoperative pain seems to be lower after the arthroscopic Latarjet technique than after the open Latarjet surgery, presumably as a consequence of reduced soft tissue damage. Midterm functional outcomes are similar between the groups as well as rates of reoperation and recurrence. Conversely, the complication rate is higher and operative time longer after the arthroscopic technique; however, these can both be reduced with the surgeon’s experience. The last important aspect is the economic costs of arthroscopic procedures, which are much higher than those of the open Latarjet procedure. This issue can become relevant in the future, since most countries have adopted a cost reduction policy.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.