
Abstract
Background:
Iliopsoas fractional lengthening (IFL) continues to be a controversial procedure in hip arthroscopy.
Hypothesis:
Patients who underwent arthroscopic surgery for femoroacetabular impingement (FAI) and a labral tear either with or without IFL would experience favorable outcomes, and there would be no difference in postoperative patient-reported outcomes (PROs) between the 2 groups at minimum 2-year follow-up.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data from July 2009 and April 2015 were retrospectively reviewed. Patients were eligible if they had hip arthroscopy for both FAI and labral tear treatment with IFL and without IFL. IFL was indicated for painful internal snapping. Minimum postoperative follow-up was set to 2 years. The authors calculated the modified Harris Hip Score, International Hip Outcome Tool–12, Hip Outcome Score–Activity of Daily Living Score, Hip Outcome Score–Sports Specific Subscale, Non-Arthritic Hip Score, visual analog scale for pain, patient satisfaction, minimal clinically important difference (MCID), and the percentage of patients who achieved patient acceptable symptomatic state (PASS). Revision surgeries and conversions to total hip arthroplasty (THA) were documented.
Results:
351 hips (307 patients) met the necessary inclusion criteria in the IFL cohort, with a mean ± SD follow-up time of 42.5 ± 18.1 months. For the control cohort, 392 hips (354 patients) were included, with a mean ± SD follow-up time of 43.9 ± 19.6 months. Both groups showed significant postoperative improvement in 2-year follow-up PROs. The group with iliopsoas lengthening showed comparable results to the control group with respect to PRO improvement, MCID, PASS, and rates of revision or THA conversion.
Conclusion:
This comparative cohort study demonstrated that treatment of painful internal snapping syndrome with arthroscopic IFL, in the setting of FAI and a labral tear, is a safe procedure with good short- to mid-term follow-up results and associated improvement in PROs. Patients who underwent IFL showed similar outcomes compared with a control group treated for FAI and labral tear without IFL. In appropriately selected patients, arthroscopic IFL did not adversely affect clinical outcomes compared with patients who did not need IFL.
As described by Nunziata and Blumenfeld et al, 37 internal coxa saltans is not a new concept. Symptomatic iliopsoas impingement is defined as painful and sometimes audible iliopsoas tendon snapping over the femoral head and/or iliopectineal line,2,44-46 with a prevalence of 10% in the general population. 9
Symptomatic patients can manage their pain with properly structured nonoperative treatments, which include physical therapy programs, activity modification, nonsteroidal inflammatory drugs, and even ultrasound-guided injections.6,9,39 However, surgical intervention may be necessary for select cases where painful internal snapping or iliopsoas impingement is unresponsive to the aforementioned nonoperative approaches. 3
Many new options for minimally invasive surgical treatment have recently been discovered for hip disorders.11,16,17,27,28,40,42 A multitude of arthroscopic techniques have been described for iliopsoas fractional lengthening (IFL)3,22,28,35 and have been shown to effectively alleviate the pain associated with painful internal snapping hip19,22,36 with fewer complications, decreased failure rates, and decreased postoperative pain when compared with open procedures. 31
Transcapsular fractional lengthening from the central or peripheral compartment and extracapsular tenotomy at the tendon’s insertion on the lesser trochanter are 2 common arthroscopic surgical management options for painful internal snapping or iliopsoas impingement.19,22,31,35,36 The transcapsular technique is performed through an anterior hip capsulotomy and only the tendon fibers are completely transected, leaving the muscle fibers intact. This allows a relative lengthening of the iliopsoas muscle-tendon unit. 22 In the extracapsular approach, the lesser trochanter and the iliopsoas tendon are identified. A complete release is performed, which results in more muscle-tendon unit retraction.28,35
Given advancements in hip arthroscopy, researchers have discovered that iliopsoas impingement is commonly associated with characteristic anterior labral tears at the 3-o’clock position (right hip).7,19,25 El Bitar et al 22 published their 2-year follow-up results after arthroscopic IFL for painful internal snapping hip syndrome and reported that 81.8% of cases yielded good to excellent results with resolved symptoms. As well, good outcomes have previously been reported in recreational and competitive athletes. 4
Despite these outcomes and technical advantages, several concerns remain regarding arthroscopic IFL.22,31 Muscle atrophy, 50 poor hip flexion strength, 8 potential instability, 33 and even catastrophic complications like intra-abdominal fluid extravasation 32 have been reported after arthroscopic IFL, making iliopsoas impingement treatment relatively controversial.
The purpose of this study was to analyze, compare, and report the outcomes and results of 2 cohorts of patients who underwent arthroscopic hip surgery for femoroacetabular impingement (FAI) and a labral tear, one cohort with IFL and a second without. We hypothesized that no statistical differences would be found between the groups.
Methods
Patient Selection Criteria
This study received institutional review board approval (IRB ID: 5276), and data were reviewed retrospectively from prospectively collected databases at the involved institutions. All surgeries were performed by sports medicine fellowship–trained surgeons with specific expertise in hip arthroscopy between July 2009 and April 2015. To remove bias from the study, the primary surgeon was removed from all data during data analysis. Patients were determined eligible for this study if they had undergone hip arthroscopy with or without IFL during the aforementioned study period, if they had received concomitant treatment for labral tears and FAI syndrome, and if minimum 2-year postoperative measures were available for the following: modified Harris Hip Score (mHHS), International Hip Outcome Tool–12 (iHOT-12) score, Hip Outcome Score–Activity of Daily Living (HOS-ADL), Hip Outcome Score–Sports Specific Subscale (HOS-SSS), and Non-Arthritic Hip Score (NAHS). The exclusion criteria for this study were preoperative Tönnis osteoarthritis grade greater than 1, labral debridement, acetabular cartilage grade greater than 3, and having had any previous ipsilateral hip surgeries or conditions such as Legg-Calvé-Perthes disease and slipped capital femoral epiphysis. Visual analog scale for pain (VAS), patient satisfaction, minimal clinically important difference (MCID), 43 and patient acceptable symptomatic state (PASS) of the mHHS were calculated.34,41 Revision surgeries and conversions to total hip arthroplasty (THA) were documented. Statistical significance was set to P = .05.
Clinical Evaluation
All study patients were examined by 1 of the 3 senior authors (A.J.K., B.A.L., B.G.D.). Physical examination was conducted to evaluate range of motion, along with other factors that contribute to hip pain. Internal snapping hip syndrome was defined as mechanical symptoms such as painful snapping or popping. On the physical examination, the snapping was reproduced with a circumduction maneuver by moving the hip from flexion-external rotation to extension-internal rotation. To help with diagnosing labral tears and FAI, we performed anterior, lateral, and posterior impingement tests. In addition, all patients underwent preoperative radiographic evaluation assessed by the senior authors. The radiograph protocol of all involved institutions included Dunn view, anteroposterior pelvis in both supine and upright positions, and the false profile view. Radiographic images were used to calculate Tönnis angle, lateral center-edge angle, and crossover sign. The Tönnis scale was used to determine the degree of osteoarthritis. 48 Before surgery, all patients underwent magnetic resonance arthrograms to ensure that their diagnosis of a labral tear and FAI was indeed correct.
Indications for Hip Arthroscopy
Before undergoing surgical treatment, all patients were asked to adhere to nonoperative treatment for their hip pain, including physical therapy, anti-inflammatory drugs, and rest for at least 12 weeks. If patients still had problematic pain symptoms after documented nonoperative treatment, they were scheduled for arthroscopic surgeries by the primary surgeons. Reproducible painful internal snapping that did not improve after the nonsurgical treatment program was the main indication for IFL.
Surgical Techniques
The primary surgeons performed hip arthroscopies with the patient in the modified supine position. Portals to access the joint capsule were created, including standard anterolateral, midanterior, and distal anterolateral accessory portal as needed. Diagnostic arthroscopy was conducted to appraise the qualities of acetabular and femoral cartilage surfaces. Although internal snapping assessment under direct visualization is not part of our surgical routine, it is important to recognize the “iliopsoas impingement sign,” described by Domb et al, 19 as an inflamed appearance of the iliopsoas tendon and labrum at the 3-o’clock position (right hip) without frank tear. When indicated, supplementary procedures were performed during the hip arthroscopy. For example, the ligamentum teres was treated with debridement by use of a radiofrequency tool to address any tearing. Acetabular and femoral head deformities were addressed with bony reshaping of impinging lesions.
Since there were 2 cohorts, one in which patients received an IFL and the other in which patients did not, every patient in the appropriately named cohort received an IFL procedure. Patients who had an IFL procedure reported a history of painful internal snapping.
The actual IFL procedure involved releasing the tendinous portion with electrocautery or beaver blade while the hip was in traction, at the level of the joint line. A detailed description of the technique itself has already been published by one of the senior authors.19,22 Labral tears were identified and either repaired or reconstructed. Each treatment was selected for each case based on a previously published algorithm on labral tear treatment. 16 Similarly, in cases of capsular instability, joint capsules were closed via an inferior shift plication suture technique, also published by one of the senior authors.12,18 After surgery, follow-up outcomes were prospectively collected at each annual follow-up appointment.
Statistical Analysis
An a priori power analysis was completed to determine the number of patients needed in the IFL and non-IFL groups to realize a minimum of 80% power using a 1:1 matching ratio. 14 On the basis of an expected mean difference in the mHHS of 10 and a standard deviation of 20 (Cohen d = 1.0), 15 it was determined that a total number of 64 patients would be required for each group. A cutoff value was selected because a difference of 10 points was suggested as the MCID.30,34
All statistical analyses were performed with Microsoft Excel. When the normality and variances were analyzed for comparisons of continuous data, the Shapiro-Wilk test and F test were used, respectively. After assumptions of normality and equal variance were met, paired 2-tailed t tests were performed, where the threshold for statistical significance was set to .05. Pearson chi-square and Fisher exact tests were used to compare categorical sets of data. Simple descriptive statistics including standard deviations, proportions, means, and ranges were calculated using the aforementioned Microsoft Excel program and were reported when necessary.
Preoperative scores and rates of revision to THA were available for only some of the IFL and non-IFL patients. As a result, delta values were calculated only for those patients with both preoperative and postoperative scores.
Results
During the study period, 910 hips in 850 patients received an IFL between all involved institutions. Of those, 438 hips (390 patients) met the inclusion criteria, and 351 hips (307 patients) (80.1%) had the necessary follow-up (Figure 1). For the non-IFL cohort, 885 hips in 802 patients did not receive an IFL and 468 hips in 420 of these individuals met the inclusion criteria. Of these 468 hips, 392 hips (354 patients) (83.4%) had the necessary follow-up (Figure 2). Preoperative scores were available for 304 hips (260 patients) in the IFL group and 304 hips (266 patients) in the non-IFL group.
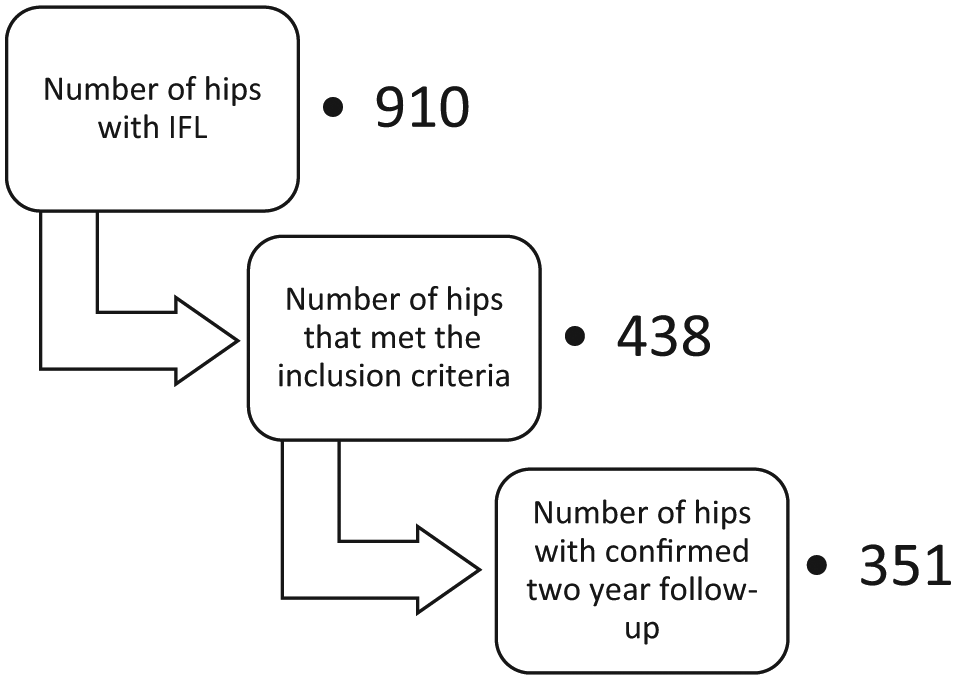
Patients with iliopsoas fractional lengthening (IFL).
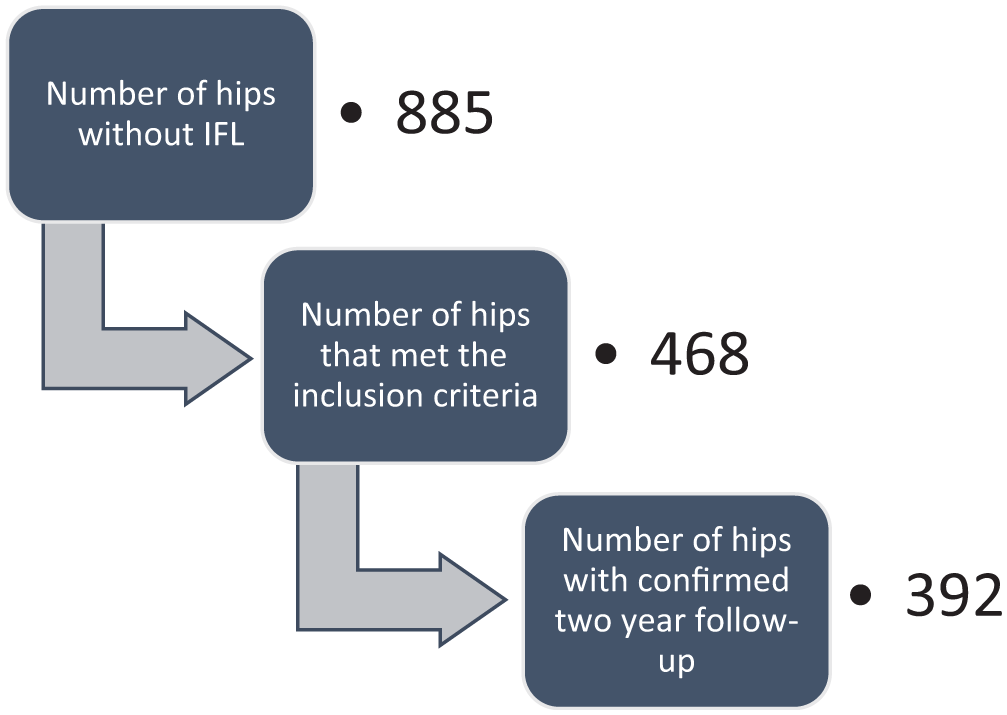
Patients without iliopsoas fractional lengthening (IFL).
Comparing the characteristics of the patients with and without IFL proved useful in verifying the similarities between the 2 cohorts (Table 1). Significant differences were found in sex and age. Body mass index and radiograph measurements (alpha angle and lateral center-edge angle) between groups yielded no significant differences. Follow-up time also showed no significant differences (Table 1).
Characteristics of Patients With and Without Iliopsoas Fractional Lengthening (IFL) a
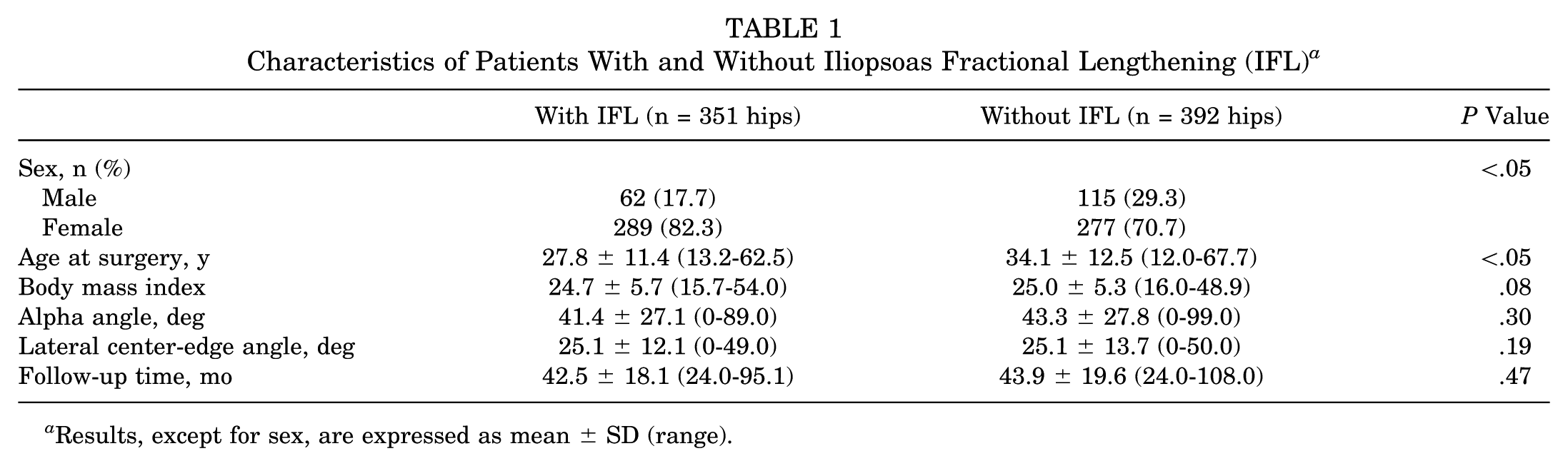
Results, except for sex, are expressed as mean ± SD (range).
Comparisons of Intraoperative Findings Between Groups
Intraoperatively, all primary surgeons noted the degree of chondral damage during diagnostic arthroscopy. Significant differences were noted between the groups with and without IFL in terms of acetabular labrum articular disruption and acetabular Outerbridge grades 1 and 2, as well as femoral head Outerbridge grades 0 and 2. No patients in either cohort were found to have acetabular or femoral head Outerbridge grades of 3 or 4 (Table 2).
Intraoperative Findings Noted During Diagnostic Arthroscopy in Patients With and Without IFL a
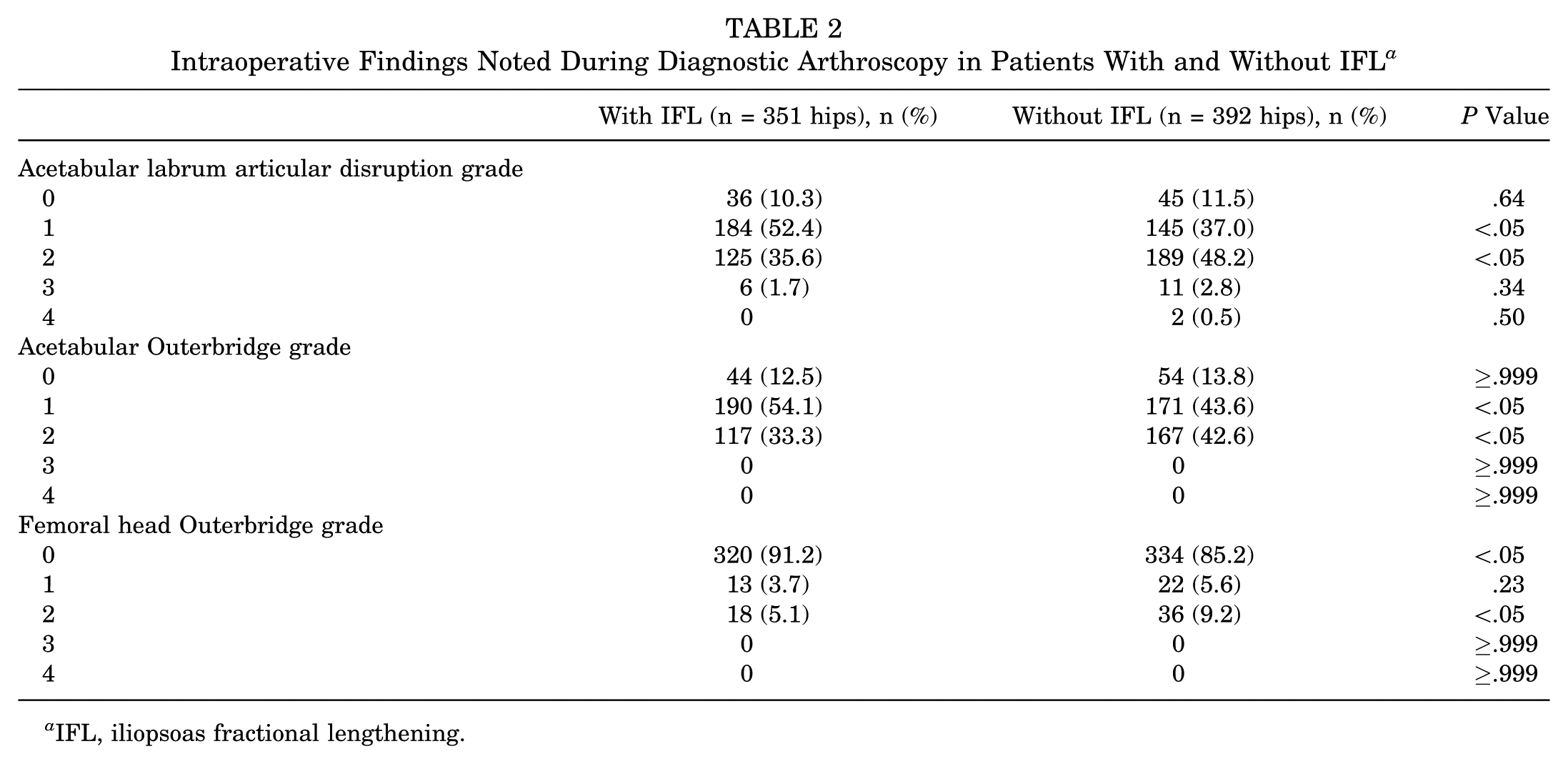
IFL, iliopsoas fractional lengthening.
Comparisons of Intraoperative Procedures Between Groups
All concomitant intraoperative procedures are listed in Table 3. All patients, from both groups, underwent labral repair or reconstruction. Femoroplasties and acetabuloplasties were also common, with 275 (78.3%) hips in the IFL group receiving a femoroplasty and 304 (77.6%) hips in the non-IFL group receiving said procedure. Also, 285 (81.2%) hips with IFL received an acetabuloplasty compared with 345 (88.0%) hips without IFL. Capsular closure or plication was used more commonly in the IFL group than in the non-IFL group.
Intraoperative Procedures Noted During Hip Arthroscopy in Patients With and Without IFL a
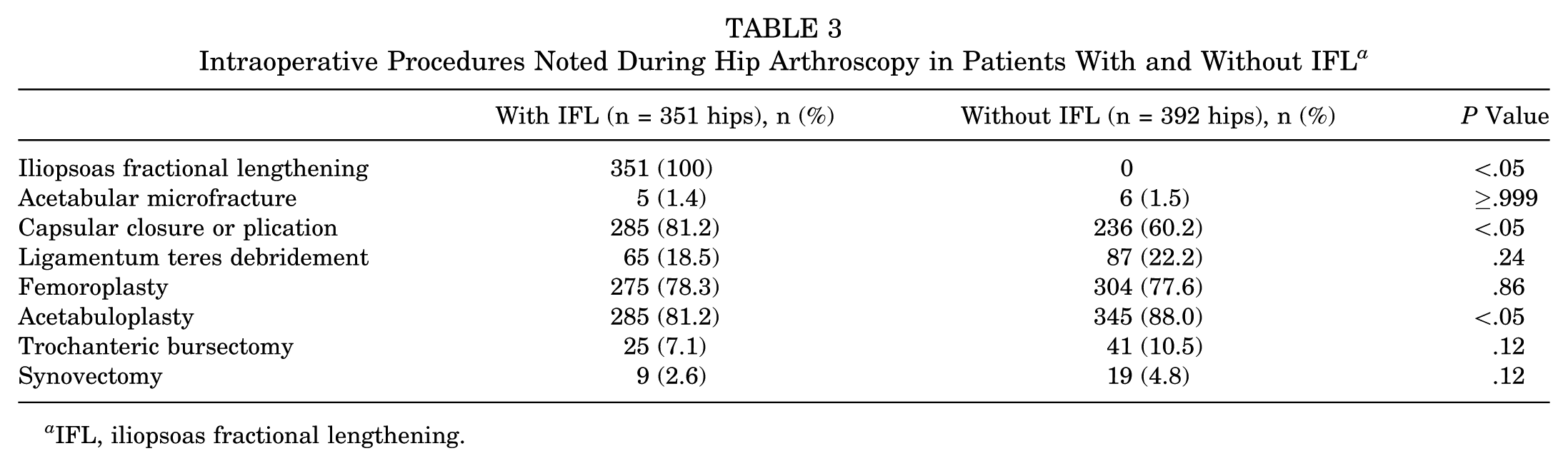
IFL, iliopsoas fractional lengthening.
Comparison of Follow-up Data
Table 4 depicts the follow-up scores compared between groups. No differences between cohorts were found for any outcome measure, including mHHS, iHOT-12, and HOS-SSS.
Follow-up Scores for Patient-Reported Outcomes in Patients With and Without IFL a
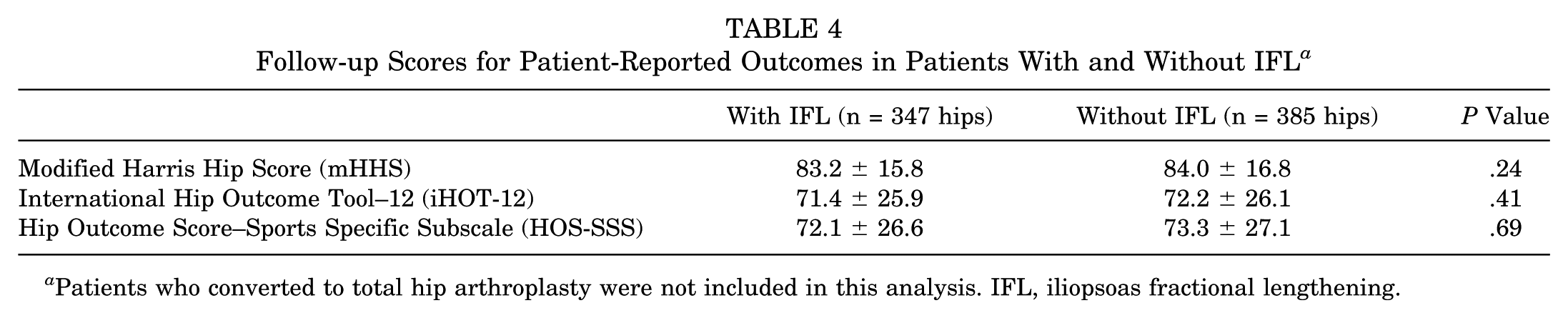
Patients who converted to total hip arthroplasty were not included in this analysis. IFL, iliopsoas fractional lengthening.
Delta values between preoperative and minimum 2-year follow-up scores were tabulated for both groups (Figure 3), and all improvements proved significant (P < .05). No differences in the deltas were found between the 2 groups.
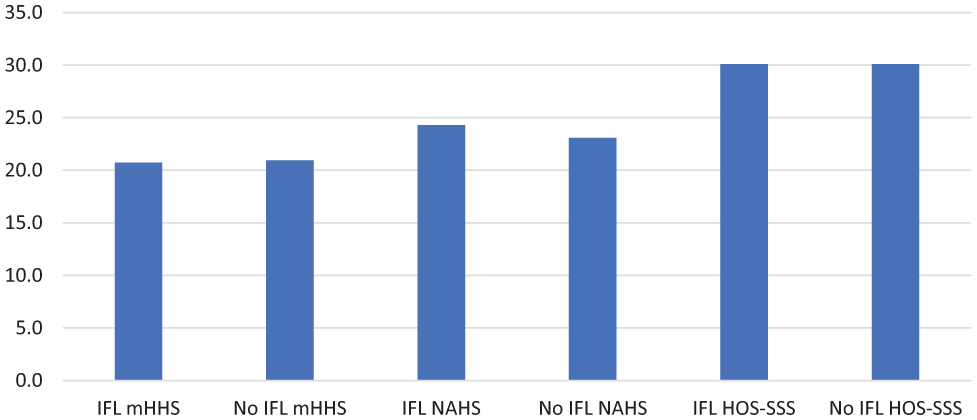
Improvement (delta values) from preoperative to postoperative patient-reported outcomes for the IFL group and the non-IFL group. IFL, iliopsoas fractional lengthening; mHHS, modified Harris Hip Score; HOS-SSS, Hip Outcome Score–Sports Specific Subscale; NAHS, Non-Arthritic Hip Score.
In the IFL group, 236 hips (77.6%) reached the PASS with mHHS 74 or higher, compared with 229 hips (75.3%) without IFL (P = .57). Furthermore, the mean change in mHHS was 20.7 in the IFL group and 20.9 in the non-IFL group. In the IFL group, 230 (75.7%) hips reached MCID, which was not significantly different (P = .71) from the 225 (74.0%) hips that reached MCID in the non-IFL group.
Revisions and Conversions to THA
Table 5 summarizes the rates of revision in the 2 patient cohorts. No differences were found with regard to revision rate and conversion rate to THA. However, time to revision was significantly different between the 2 groups.
Comparisons of Patients With and Without IFL for Rates of Revision, Time to Revision, Rates of Conversion to THA, and Time to THA a
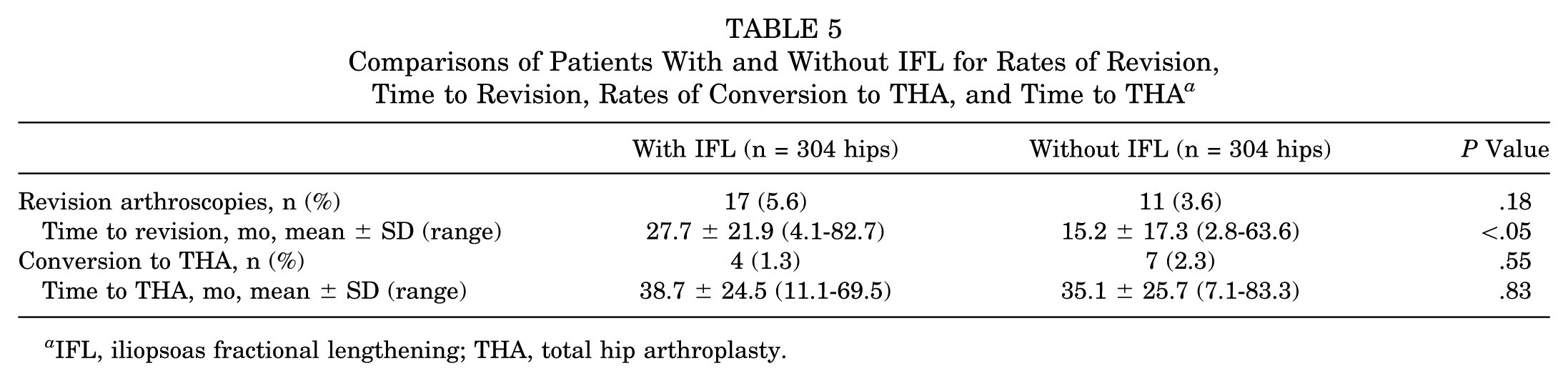
IFL, iliopsoas fractional lengthening; THA, total hip arthroplasty.
Discussion
This study evaluated the outcomes of a cohort of 351 hips (307 patients) undergoing arthroscopy for FAI correction, labral treatment, and IFL for painful internal snapping hip and compared their outcomes to a cohort of 392 hips (354 patients) without internal snapping hip that also underwent hip arthroscopy for FAI correction and labral treatment with no IFL. With a minimum follow-up of 2 years, both groups showed favorable results with significant improvements in all PROs and low rates of revision or THA. The cohorts had comparable postoperative PROs, VAS scores, patient satisfaction, MCID, and PASS. Between the 2 groups in the present study, no inferior outcomes were found in the patients with painful internal snapping who underwent arthroscopic hip surgery.
Previous literature has established iliopsoas lengthening as effective in eliminating painful internal snapping.13,28,31 El Bitar et al 22 published their findings whereby 55 patients underwent arthroscopic IFL for internal snapping of the hip with 2-year follow-up. The authors found that 45 of the patients (81.8%) reported resolution of painful snapping with significant improvement (P < .01) in all postoperative PROs (mHHS, NAHS, HOS-ADL, and HOS-SSS). The authors also reported mean improvements of 21.3 points for mHHS, 25.9 points for NAHS, and 30.6 points for HOS-SSS, similar to our findings (mHHS, 20.7; NAHS, 24.3; HOS-SSS, 30.1) and also similar to other authors’ results. 36
Interestingly, sex distribution was significantly different (P < .05) between the groups in the current study. In the IFL group, 82.3% of the patients were female, compared with 70.7% in the non-IFL group. Females may have a higher incidence of internal snapping or iliopsoas impingement and therefore would represent a higher proportion of the IFL group. In a systematic review, Khan et al 31 found that 82.5% of the patients who underwent arthroscopic iliopsoas tenotomy were women. As Hoskins et al 26 mentioned, women may be predisposed to developing this condition.
Patients were significantly younger in the IFL group than in the non-IFL group (P < .05). Similar results have been reported by other authors,1,10,13,19,23 suggesting that iliopsoas injury tends to affect a much younger population.
Capsular management was another variable that was significantly different (P < .05) between groups. In the IFL group, capsular closure or plication was performed in 81.2% of cases; however, in the non-IFL group, capsular closure or plication was accomplished in only 60.2% of total cases. Meticulous capsular management, with closure or plication, could be imperative to achieving good to excellent short-term outcomes. By capsular closure, we mean side-to-side stitches allowing repair and restoration of normal capsular structure, whereas plication implies not only closure but also imbrication and inferior shift of the capsule, increasing the tightness of the capsule in both extension and external rotation. 18 Previous studies5,11,18,21,29,49 have reported good results with different techniques for appropriate capsular management. Patients with dysplasia or generalized ligamentous laxity are usually considered potentially high-risk patients after arthroscopic hip surgery.24,25,38,51 If arthroscopic IFL is performed in such high-risk patients with a propensity for instability, then capsular plication, shift, or even newer techniques may be used 20 to preserve or augment the static stabilizers of the hip. 47 Furthermore, if the capsulotomy is extended medially for the IFL, it is imperative that it be closed. When arthroscopic iliopsoas tenotomy is performed in these potentially high-risk patients, capsular plication or shift techniques with labral preservation have been suggested. 20 Spiker et al, 47 in an attempt to avoid instability risk, proposed an arthroscopic psoas tunnel deepening to alleviate iliopsoas symptoms while preserving capsule integrity. We have theorized that this is because the iliopsoas becomes hyperactive in the unstable hip, in a vain attempt to stabilize the hip. When the static stabilizers are restored, the iliopsoas is no longer needed as a stabilizer and can be safely lengthened to address painful snapping. 10 These considerations may explain the higher rate of capsular plication in the IFL group.
The strength of the current study is that it was a multicenter endeavor, which increases the generalizability of the results. The inclusion of multiple validated functional hip outcome scores, a minimum of 2-year follow-up, and the inclusion of a representative number of patients also drastically increase generalizability of the results. The PRO scores that were used were designed specifically to detect outcomes in active patients with nonarthritic hips. 22 To our knowledge, this study has the highest number of patients who received arthroscopic IFL with reported outcomes and has an 80.13% follow-up rate.
Patients with FAI, labral tear, and painful internal snapping who do not improve after nonsurgical measures are candidates for IFL as an additional procedure during hip arthroscopy. A randomized study is currently in the planning stages at our institutions to evaluate this with a higher level of evidence.
It is unclear, based on the current literature, whether IFL leads to significant and/or permanent loss of hip flexor strength. Those who may be most at risk to develop iliopsoas-related issues may also be the ones at greatest risk for poor outcomes with arthroscopic IFL. Prospective randomized research is the only way to directly address this issue.
Limitations of this study must be acknowledged. First, it is a nonrandomized study. Second, the 2 cohorts are not matched and have inherent differences, as one group had painful snapping and one did not. Third, this study includes retrospective analysis of registry data, and a longer follow-up is needed to determine the long-term durability of these results. Fourth, preoperative scores and rates of revision to THA were available for only some of the IFL and non-IFL patients. As a result, delta values were calculated only for those patients with both preoperative and postoperative scores. Fifth, surgeon practice and bias may differ between the involved surgeons and institutions. Sixth, hip flexion weakness and resolution of snapping symptoms after IFL were not consistently documented. To address this, a study is currently underway at our institutions to evaluate the objective strength of hip flexion after hip arthroscopy with and without IFL.
Conclusion
This comparative cohort study demonstrated that treatment of painful internal snapping syndrome with arthroscopic IFL, in the setting of FAI and a labral tear, is a safe procedure with good short- to mid-term follow-up results and associated improvement in PROs. Patients who underwent IFL showed similar outcomes compared with a control group treated for FAI and labral tear without IFL. In appropriately selected patients, arthroscopic IFL did not adversely affect clinical outcomes compared with patients who did not need IFL.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G.D. reports personal fees and other from Arthrex, Pacira, and Stryker and personal fees from Orthomerica, DJO Global, Amplitude, and Medacta outside the submitted work. B.G.D. is a board member for the American Hip Institute, which funds research and is the institute where our studies are performed. B.G.D. is also a board member at the AANA Learning Center Committee and Arthroscopy Journal. A.J.K. has received consulting fees from Arthrex and DePuy. He also reports receiving personal and nonpersonal fees from the Musculoskeletal Transplant Foundation. B.A.L. receives personal fees as a consultant and nonpersonal fees from Smith & Nephew. D.E.H. has received education and hospitality payments from Arthrex and Smith & Nephew.