
Abstract
Background:
Cam-type femoroacetabular impingement (FAI) is a causative factor for hip pain and early hip osteoarthritis. Although cam FAI can alter hip joint biomechanics, it is unclear what role muscle forces play and how they affect the hip joint loading.
Purpose/Hypothesis:
The purpose was to examine the muscle contributions and hip contact forces in individuals with symptomatic cam FAI during level walking. Patients with symptomatic cam FAI would demonstrate different muscle and hip contact forces during gait.
Study Design:
Controlled laboratory study.
Methods:
Eighteen patients with symptomatic cam FAI were matched for age and body mass index with 18 control participants. Each participant’s walking kinematics and kinetics were recorded throughout a gait cycle (ipsilateral foot-strike to ipsilateral foot-off) by use of a motion capture system and force plates. Muscle and hip contact forces were subsequently computed by use of a musculoskeletal modeling program and static optimization methods.
Results:
The FAI group walked slower and with shorter steps, demonstrating reduced joint motions and moments during contralateral foot-strike, compared with the control group. The FAI group showed reduced psoas major (median, 1.1 newtons per bodyweight [N/BW]; interquartile range [IQR], 1.0-1.5 N/BW) and iliacus forces (median, 1.2 N/BW; IQR, 1.0-1.6 N/BW), during contralateral foot-strike, compared with the control group (median, 1.6 N/BW; IQR, 1.3-1.6 N/BW, P = .004; and median, 1.5 N/BW; IQR, 1.3-1.6 N/BW, P = .03, respectively), which resulted in lower hip contact forces in the anterior (P = .026), superior (P = .02), and medial directions (P = .038). The 3 vectors produced a resultant peak force at the anterosuperior aspect of the acetabulum for both groups, with the FAI group demonstrating a substantially lower magnitude.
Conclusion:
FAI participants altered their walking kinematics and kinetics, especially during contralateral foot-strike, as a protective mechanism, which resulted in reduced psoas major and iliacus muscle force and anterosuperior hip contact force estimations.
Clinical Relevance:
Limited hip mobility not only is attributed to bone-on-bone impingement, caused by cam morphology, but could be attributed to musculature as well. Not only would the psoas major and iliacus be able to protect the hip joint during flexion-extension, athletic conditioning could further strengthen core muscles for improved hip mobility and pelvic balance.
Cam-type femoroacetabular impingement (FAI) is widely recognized as a causative factor for groin pain, athletic hip injuries, and early adult hip osteoarthritis.25,26 The morphology itself appears as an aspherical bony extension at the anterolateral and anterosuperior femoral head on clinical imaging (ie, elevated alpha angles),57,58,64 leading to a reduced anterior head-neck offset. 28 In addition to the alpha angles that quantify the cam morphology, clinical symptoms and reduced functional range of motion (ROM) have been attributed to secondary anatomic characteristics.7,33,53,54,59
Individuals with symptomatic cam FAI previously demonstrated altered kinematics and kinetics compared with control participants during walking,21,35,37,63 squatting,6,41 and stair climbing. 62 Specifically during level walking, symptomatic individuals walked with reduced sagittal hip ROM, frontal hip and pelvic ROM, and internal hip rotation as well as with reduced flexion and external rotation moments. Recently, individuals with symptomatic cam FAI also demonstrated weaker muscle strength during maximum isometric voluntary contractions in abduction, adduction, flexion, and external rotation, suggesting that differences during activities of daily living were influenced by altered neuromuscular activation.15,20,37 Although dynamic muscle activity in individuals with FAI has been investigated only when subjects performed squatting activities, 42 no significant differences were observed with respect to the control population.
Previous biomechanical studies focused on analyses of joint kinematics and kinetics associated with FAI; however, limited literature is available regarding muscle strength or, more important, the contributions of muscle forces toward hip joint loading, during an activity of daily living. Therefore, the purpose of this study was to examine muscle contributions and hip contact forces in individuals with symptomatic cam FAI during level walking. We hypothesized that patients with symptomatic cam FAI would demonstrate different muscle and hip contact forces during level walking.
Methods
Study Design
This controlled laboratory study involved a case-control comparative analysis, which compared a patient cohort (individuals with symptomatic cam FAI) and a healthy cohort (asymptomatic individuals with no cam morphology). All participants provided informed consent, and the study was approved by the hospital and institution research ethics boards (OHSN-REB Protocol #2009537-01H).
Participants
A total of 36 male participants were included in this study. Eighteen patients (FAI group) initially visited the senior orthopaedic surgeon’s clinical practice (P.E.B.) with persisting unilateral clinical signs of hip pain and positive impingement tests; 18 control participants (CON group) were recruited as volunteers from the general population. Each participant underwent pelvic computed tomography (CT) imaging (Acquilion, Toshiba Medical Systems Corporation; or Discover CT750, GE Healthcare) to confirm that the affected, symptomatic hip of each patient with FAI had a cam morphology, as defined by an axial 3:00 or radial 1:30 alpha angle larger than 50.5° and 60° in the clock-face position,57,58,64 respectively, and to confirm that each CON participant did not have cam morphology. Alpha angles in the axial 3:00 and radial 1:30 planes were measured by a senior musculoskeletal radiologist. Participants were excluded if they had any other hip abnormality (eg, slipped capital femoral epiphysis, Legg-Calvé-Perthes disease, dysplasia, overcoverage), a body mass index (BMI) greater than 30 kg/m2, or a history of previous lower limb surgeries, severe traumas, or musculoskeletal disorders. The FAI and CON groups were matched for sex and BMI (Table 1), and the analysis compared the symptomatic hip for each FAI patient versus the hip with the lowest (combined axial and radial) alpha angles for each CON participant (Figure 1, A and B).
Participant Characteristics and Cam Morphology Parameters a
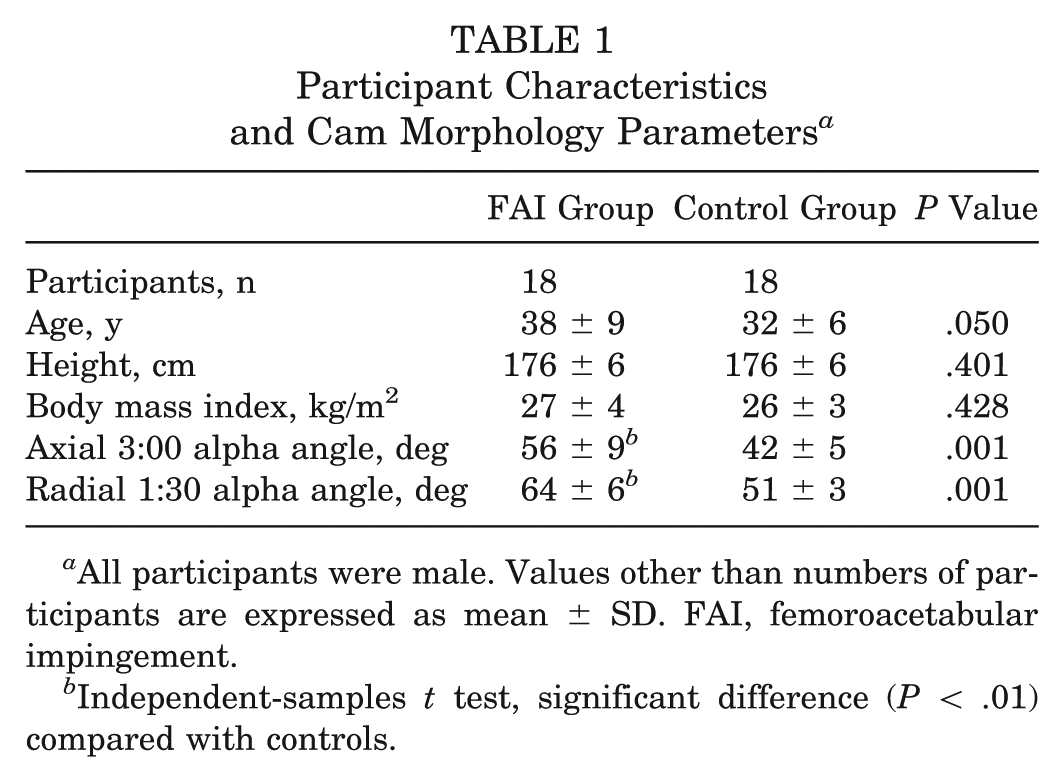
All participants were male. Values other than numbers of participants are expressed as mean ± SD. FAI, femoroacetabular impingement.
Independent-samples t test, significant difference (P < .01) compared with controls.
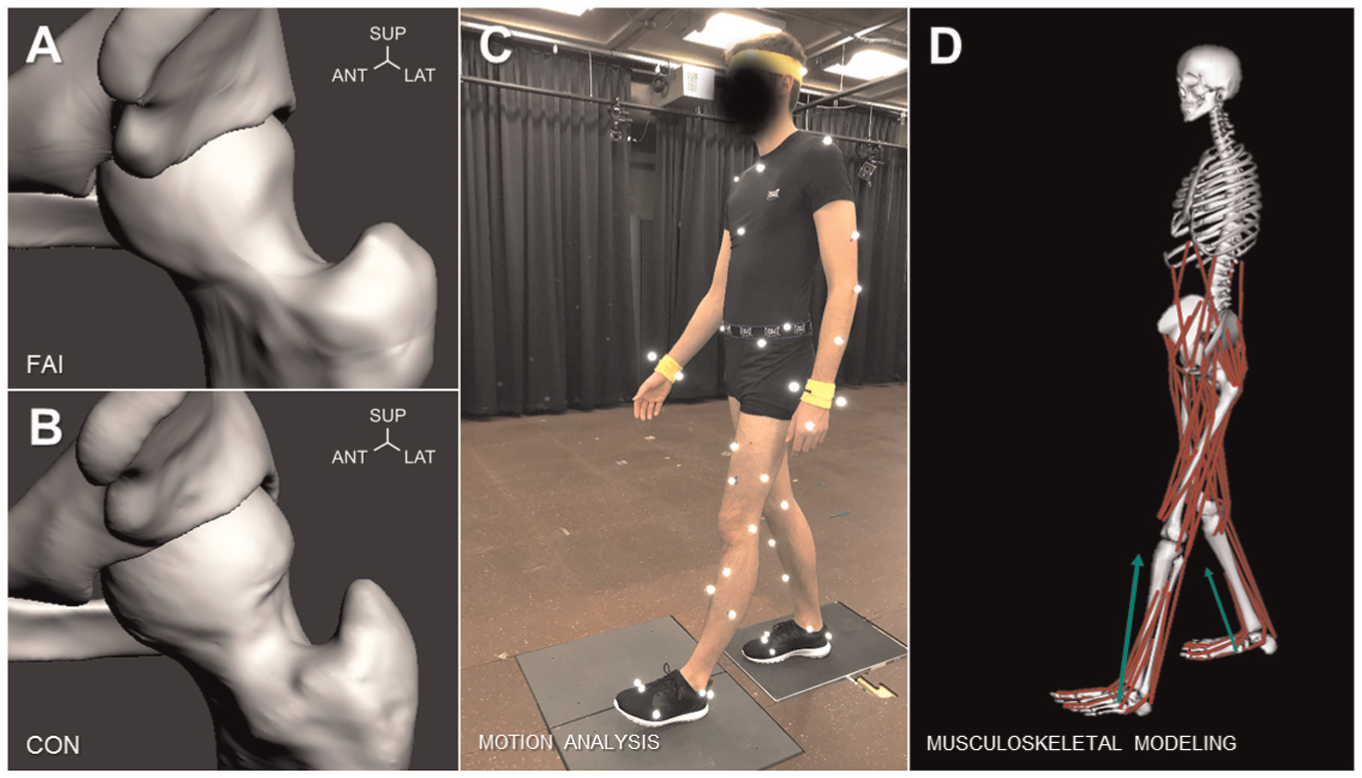
(A) Patients with symptomatic cam femoroacetabular impingement (FAI), depicted with an anterosuperior cam deformity, were compared with (B) healthy control participants (CON), who had no such deformity. (C) Each participant performed walking trials in the motion capture laboratory, where the ipsilateral foot-strike to foot-off kinematics and kinetics were captured. (D) A musculoskeletal model (consisting of the lower limb and torso segments) was used to determine the resultant muscle and hip contact forces. Ant, anterior; Lat, lateral; Sup, superior.
Motion Analysis
Before CT imaging, radiopaque surface markers were placed on each participant’s left and right anterior superior iliac spines and left and right posterior superior iliac spines in order to register the location of the surface markers with respect to the bony landmarks. 48 After imaging, the radiopaque markers were replaced with retro-reflective markers according to a customized marker set. 47 At the motion capture laboratory, each participant was asked to repeat 5 level walking trials,22,43 at a self-selected pace, where kinematics were captured with a 10–infrared camera system (Vicon MX-13; frequency = 200 Hz) and kinetics were captured by use of 2 fixed force plates (models FP4060-08, Bertec Corporation; frequency = 1000 Hz). The gait analysis was limited to the ipsilateral foot-strike to foot-off of the affected side, as forces at the hip are relevant during the stance phase (Figure 1C). Walking speed, step length, and cadence were determined by use of motion analysis software (Nexus 1.8.5; Vicon). The 3-dimensional marker trajectories and the ground-reaction forces were filtered (zero-lag, fourth-order Butterworth filter, cutoff frequency 6 Hz), and all gait variables were time-normalized to the stance cycle. Hip joint moments were normalized by bodyweight (BW), and walking speed and step length were further normalized to the participant’s leg length (LL). 34
Musculoskeletal Modeling
Muscle and hip contact forces were calculated in a musculoskeletal simulation program (OpenSim 3.1; SimTK) using a well-established musculoskeletal model (Gait2392). 19 The model was selected because it is conventionally used for lower limb studies27,67 to estimate joint contact forces11,12 and muscle activation patterns. 31 The model entails the lower limb and torso segments, modeling the hip and lumbar joints as ball-and-socket joints, the knee as a custom joint, 69 and the ankle as a hinge joint (Figure 1D). The pelvis reference system of the model presents a 13° offset in the sagittal plane, with respect to the recommended International Society of Biomechanics (ISB) reference system,36,68 which should be taken into consideration when pelvic and sagittal hip flexion-extension angles are compared with previous FAI studies in the literature (without adjustment of the estimations obtained from OpenSim).
From CT imaging, each participant’s pelvic width, depth, and height were measured and used to linearly scale the dimensions of the musculoskeletal model, accounting for the distance between virtual and experimental markers. The virtual marker positions were adjusted by registering their locations to their experimental coordinates, after static joint angles were estimated through inverse kinematics. The maximum isometric forces of the muscles in the musculoskeletal model were customized, and the participants’ anthropometric measurements were used to calculate the following scaling factor:
where Mexp and Hexp denoted the experimental mass and height, respectively. 32 The Mmod and Hmod measurements referred to original values of the musculoskeletal model’s mass and height parameters (Mmod = 74.2 kg, Hmod = 1.67 m).
After each model was scaled, a series of inverse kinematics, inverse dynamics, static optimization, and joint reaction analyses were performed. 18 Static optimization implemented a quadratic cost function to determine the muscle forces (92 muscles),4,17 which included the muscles of interest: rectus femoris, sartorius, tensor fasciae latae, gluteus medius, gluteus minimus, gluteus maximus, semitendinosus, biceps femoris, psoas major, iliacus, and adductors. Muscle contraction dynamics (ie, force-length-velocity relationship) were neglected, as they were shown to not influence muscle predictions during walking. 4 Static optimization was effective for muscle force estimations as it did not require modeling muscle dynamics and had previously demonstrated similar results with other rigorous and computationally demanding algorithms during walking (ie, dynamic optimization algorithms).4,46 Hip contact forces were calculated as 3-dimensional vectors acting on the acetabulum and expressed in the pelvic coordinate system. Both hip contact and muscle forces were normalized by BW.
Statistical Analysis
Between-group differences for demographics, anatomic variables, and gait parameters were examined using independent-samples t tests. Hip contact and muscle forces were compared using a Mann-Whitney U test for nonparametric distributions, given that some of the variables failed the Lilliefors normality test (confidence interval = 95%). Effect size was calculated with Pearson’s correlation coefficient r, the nonparametric equivalent of Cohen’s d, 61 and was considered as either small (r = 0.1), medium (r = 0.3), or large (r = 0.5). A sample size calculator (G*Power 3.1.9.3; Heinrich-Heine-Universität, Düsseldorf, Germany) determined that the acceptable sample size per group was 18 (total N = 36), to seek 80% statistical power and detect a moderate to large effect size.
Results
Gait Parameters
The patients with FAI walked with a slower walking speed (1.44 ± 0.16 m/s/LL) and smaller step length (0.77 ± 0.07 m/LL) in comparison with the CON participants (1.63 ± 0.17 m/s/LL, P = .001, and 0.85 ± 0.07 m/LL, P = .004, respectively) (Table 2). The FAI group demonstrated slightly reduced functional ROM and joint moments in all planes (Figure 2), showing significantly lower frontal adduction angle (–4.8°± 3.8°) and sagittal hip extension moment (0.08 ± 0.02 Nm/BW) during contralateral foot-strike (terminal stance phase of gait), compared with the CON group (–7.5°± 2.9°, P = .03, and 0.1 ± 0.01 Nm/BW, P = .002, respectively).
Summary of Cadence, Walking Speed, and Step Length Parameters of Each Group a
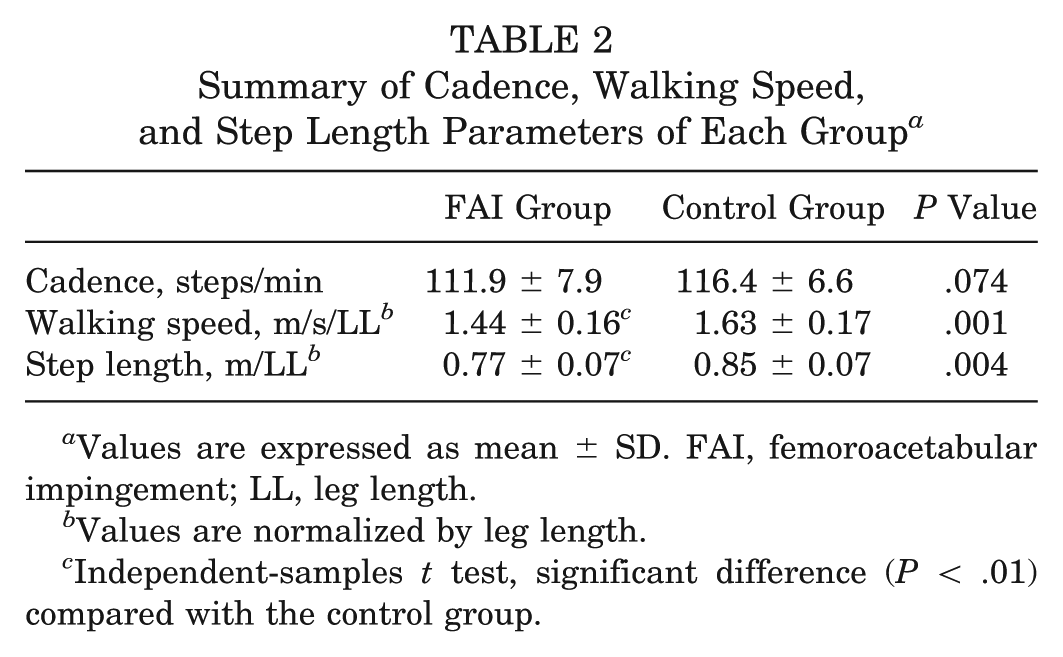
Values are expressed as mean ± SD. FAI, femoroacetabular impingement; LL, leg length.
Values are normalized by leg length.
Independent-samples t test, significant difference (P < .01) compared with the control group.
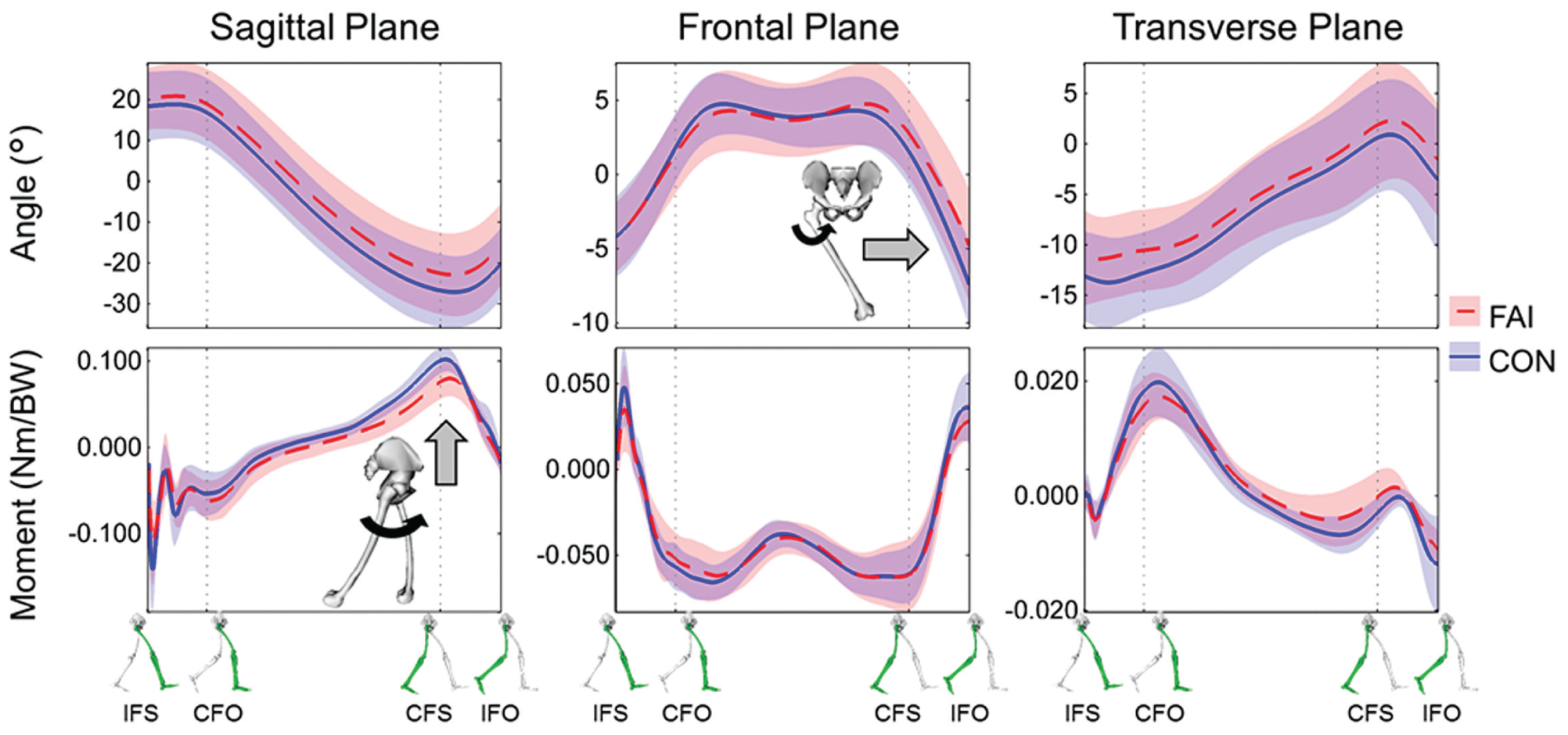
Hip joint angles (top row) and moments (bottom row) in each of the sagittal (left), frontal (center), and transverse planes (right), during the gait cycle, for the femoroacetabular impingement (FAI) (red/dashed) and control (CON) groups (blue/solid). Plotted lines and bands denote the mean and standard deviation, respectively. Hip joint moments were normalized by bodyweight (BW), and the full stance phase was represented at ipsilateral foot-strike (IFS), contralateral foot-off (CFO), contralateral foot-strike (CFS), and ipsilateral foot-off (IFO). Gray arrow denotes the statistical difference in adduction and extension moment.
Muscle and Hip Contact Forces
Both groups had similar extensor, abductor, and adductor muscle forces (Figure 3), while the FAI group demonstrated significantly reduced psoas major (median, 1.1 N/BW; interquartile range [IQR], 1.0-1.5 N/BW) and iliacus forces (median, 1.2 N/BW; IQR, 1.0-1.6 N/BW) during contralateral foot-strike (terminal stance of gait) compared with the CON group (median, 1.6 N/BW; IQR, 1.3-1.6 N/BW, P = .004, r = 0.48; and median, 1.5 N/BW; IQR, 1.3-1.6 N/BW, P = .03, r = 0.35, respectively).
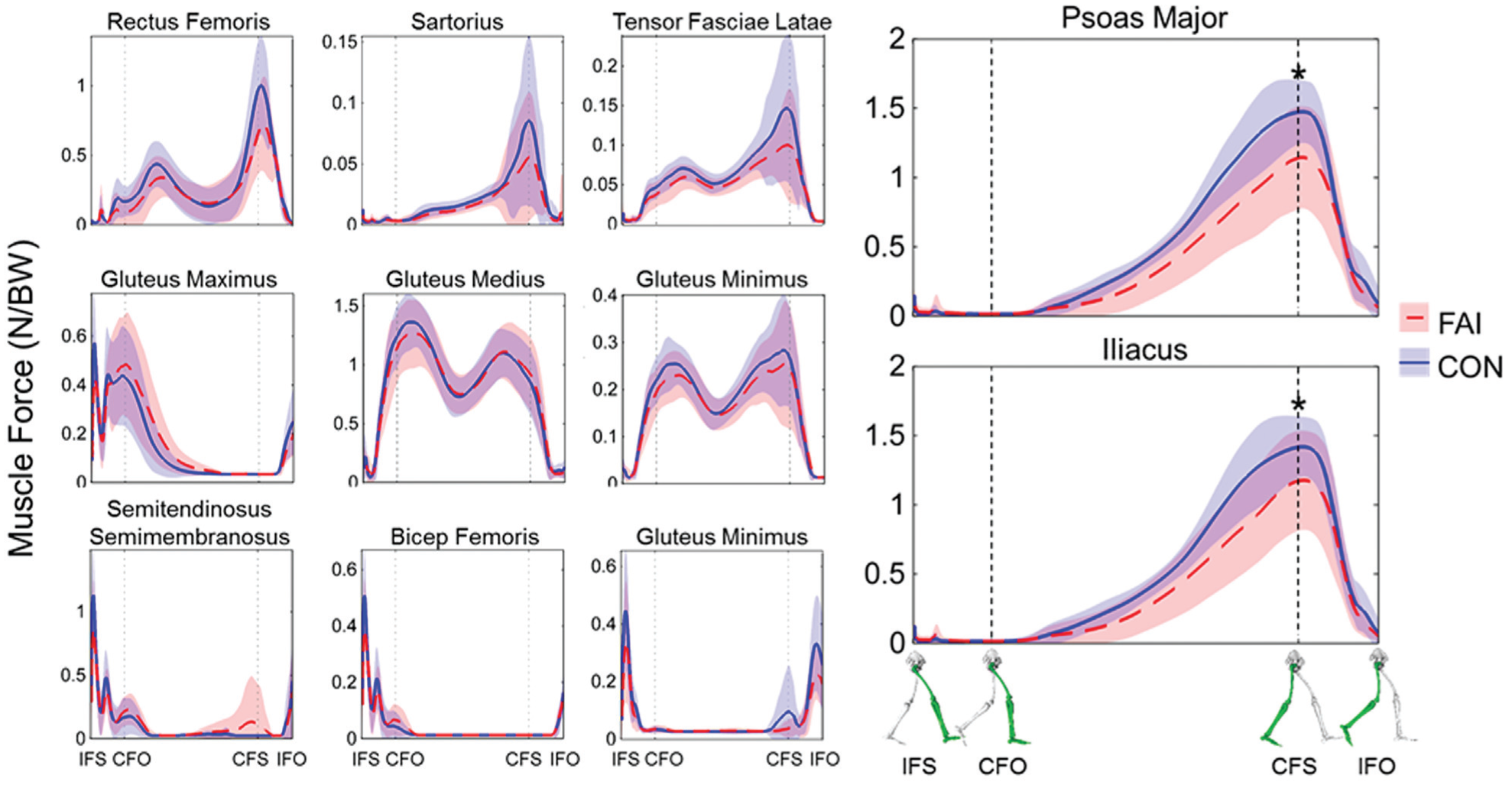
Muscle forces during the gait cycle, for the femoroacetabular impingement (FAI) (red/dashed) and control (CON) groups (blue/solid). Muscle forces were normalized by bodyweight (BW) and determined from static optimization. The full stance phase was represented at ipsilateral foot-strike (IFS), contralateral foot-off (CFO), contralateral foot-strike (CFS), and ipsilateral foot-off (IFO). Plotted lines and bands denote the mean and standard deviation, respectively. The FAI group demonstrated significantly lower psoas major (top right) and iliacus muscle forces (bottom right) during the contralateral foot-strike, denoted by an asterisk.
The FAI group walked with lower hip contact forces in the anterior (median, 2.7 N/BW; IQR, 2.2-3.9 N/BW), superior (median, 3.7 N/BW; IQR, 3.5-4.2 N/BW), and medial directions (median, 0.5 N/BW; IQR, 0.3-0.6 N/BW) compared with the CON group, during contralateral foot-strike, in each of the anterior (median, 4.0 N/BW; IQR, 2.8-4.4 N/BW; P = .026, r = 0.37), superior (median, 4.2 N/BW; IQR, 3.9-4.9 N/BW; P = .02, r = 0.39), and medial directions (median, 0.6 N/BW; IQR, 0.5-0.7 N/BW; P = .038, r = 0.36) (Figure 4A). The combination of the 3 vectors produced a resultant peak force at the anterosuperior aspect of the acetabulum for both groups (1:30 clock-face orientation) during the contralateral foot-strike, with the FAI group demonstrating a substantially lower resultant magnitude (Figure 4B).
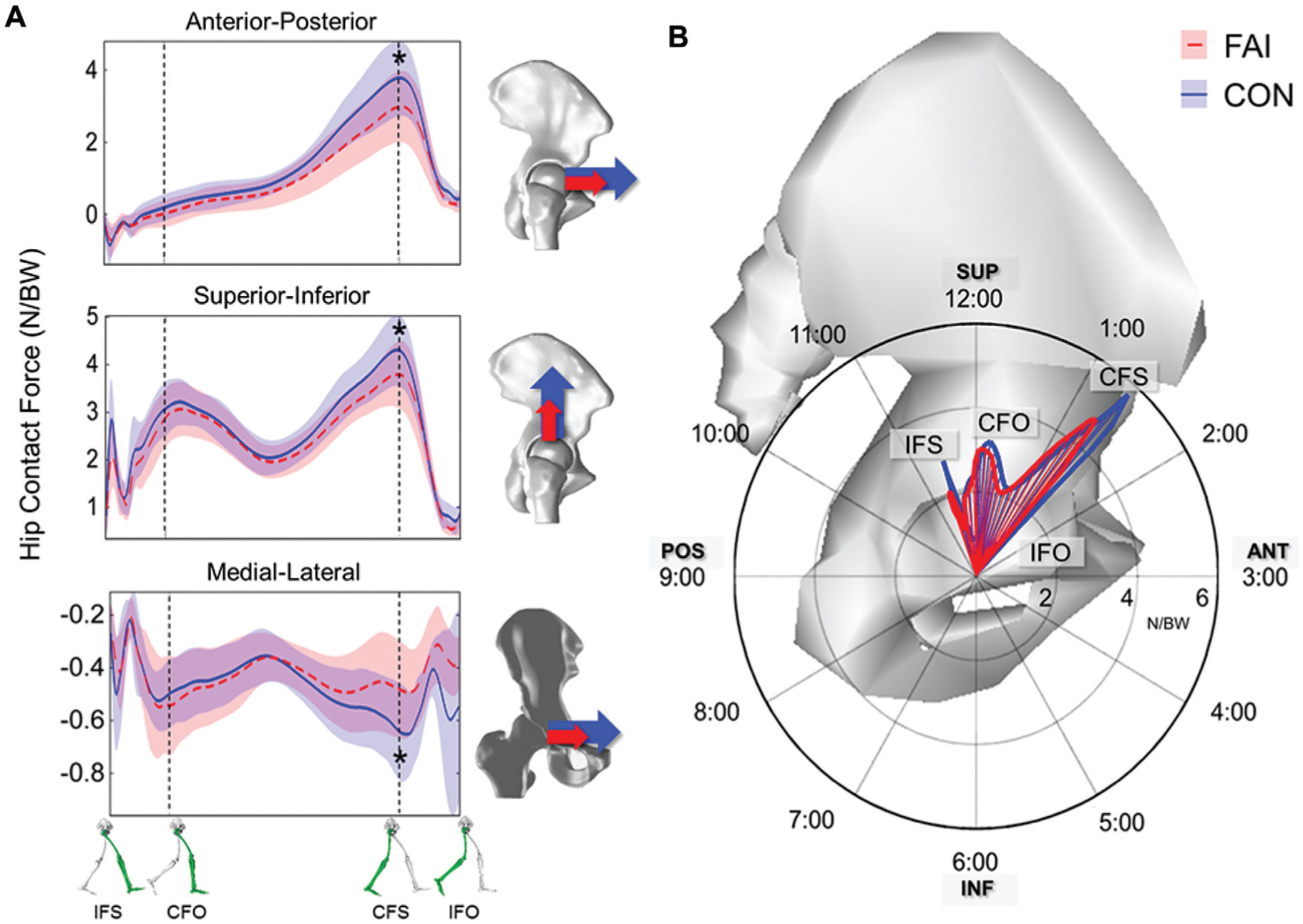
(A) Hip contact forces during the gait cycle for the femoroacetabular impingement (FAI) (red/dashed) and control (CON) groups (blue/solid) in all 3 planes. The full stance phase was represented at ipsilateral foot-strike (IFS), contralateral foot-off (CFO), contralateral foot-strike (CFS), and ipsilateral foot-off (IFO). Plotted lines and bands denote the mean and standard deviation, respectively. The FAI group demonstrated significantly lower forces during the contralateral foot-strike, denoted by an asterisk. (B) The resultant average hip contact forces during the gait cycle, depicted in the sagittal plane of a right hip. Hip contact forces were normalized by bodyweight (BW) and reported with a “butterfly” graph, showing magnitude (radar graph) and direction (acetabular clock-face orientation) with respect to the pelvic coordinate system. Ant, anterior; Inf, inferior; Pos, posterior; Sup, superior.
Discussion
In this study, we investigated whether symptomatic patients with cam FAI demonstrated different muscle and hip contact forces during level walking compared with a control group. We found that the FAI subjects altered their walking kinematics and kinetics, resulting in reduced psoas major and iliacus muscle forces and anterosuperior hip contact force estimations. Because cam morphology does not likely induce impingement during activities of daily living involving lower amplitudes of motion (ie, level walking), muscle and hip contact forces estimated via musculoskeletal modeling are crucial to help elucidate alterations in kinematics and kinetics. Furthermore, the differences in joint loading may provide a better strategy for athletic conditioning, training programs, or nonsurgical management.5,10,45 As Mayne and associates 49 recently pointed out, knowledge pertaining to hip muscle strength associated with FAI patients is very limited. Although previous studies reported joint kinematics and kinetics associated with cam FAI, none of the studies determined hip contact forces from musculoskeletal modeling in order to compare joint loading between a cohort of FAI and CON participants.
In this study, individuals with FAI walked with lower peak hip extension, abduction, and internal rotation angles, aligning well with previous findings.35,37,63 Many earlier studies of FAI assumed that limited ROM was attributed to bone-on-bone impingement, caused by the cam morphology. 39 Although the squatting motion may be more prone to impingement and reduced hip flexion,6,40,41 bone-on-bone impingement is less likely to occur during level walking. This further suggests that there may be other parameters, in addition to the bony deformity, that alter walking biomechanics of FAI participants. Moreover, our FAI group’s reduced step length, walking speed, and hip extension could be associated with a protective mechanism. All participants were instructed to walk at their self-selected pace; however, any apprehension to pain would have reduced muscle forces and, consequently, joint contact forces.2,50,52 Lewis and associates 44 previously noted that reducing hip extension may be beneficial for individuals with anterior hip pain, instability, or labral tears. In our study, participants completed their walking trials at their own self-selected pace and confirmed that they did not experience any difficulty or pain. Interestingly, 4 FAI participants in this study had indications of cartilage damage at the time of their surgery, which could have been further associated with their reduced walking speed and ROM.24,66
Although the iliacus and psoas major muscles contributed substantially to the hip contact forces, with respect to other muscles, the FAI group showed lower peak forces during contralateral foot-strike, resulting in lower hip contact forces. Both muscles (iliacus and psoas major) function primarily as hip flexors and structurally combine at the iliopsoas tendon, which tensions directly over the anterior capsulolabral complex,1,45 from the pectineal eminence of the pelvis to the lesser trochanter of the femur. During hip extension, the iliopsoas tendon and the adjacent medial branch of the capsular iliofemoral ligament prevent anterior subluxation, generating a flexion moment. The tension at the hip capsule interface may be further aggravated by the cam morphology, which is exposed more anteriorly with hip extension (Figure 5). Domb and associates 23 reported that varus hips with iliopsoas impingement sustained labral damage, where a tighter psoas tendon induced adverse stresses to the anterior capsulolabral complex during hip extension.1,37,44 This was more evident as our FAI group not only walked with a reduced hip extension but also showed a lower extension moment. The resultant hip contact forces were directed toward the anterosuperior acetabulum, from the femur onto the pelvis (in the pelvic reference system), which would be consistent with locations of chondrolabral damage in patients with FAI noted during intraoperative and imaging observations.8,9,25 This certainly supports the concept that not only extreme ROMs but also day-to-day activities contribute to hip damage in patients with cam FAI.
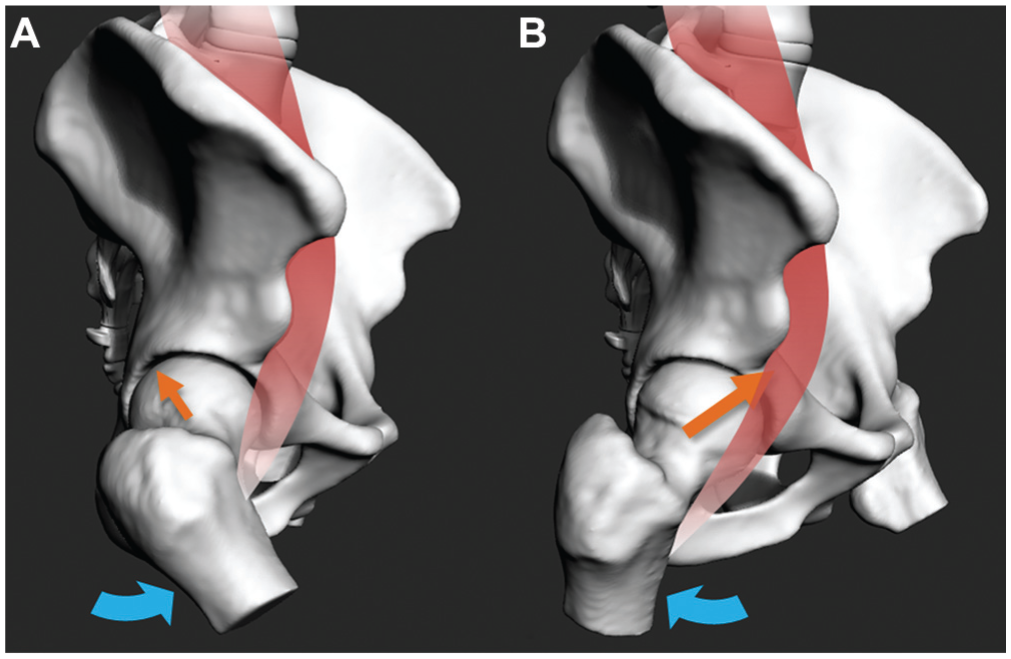
Sagittal views of the right hip during walking: (A) heel-strike, with the iliopsoas slackened and further away from the anterior femoral head, and (B) contralateral foot-strike, with the tighter iliopsoas closer to the anterior femoral head. Peak hip contact force vectors (straight arrows) occurred during the terminal stance phase of gait, with the hip extended. The participants with femoroacetabular impingement walked with smaller extension angles and flexion moments, resulting in reduced hip contact forces.
Resultant subject-specific hip contact forces and kinematics are necessary inputs for finite element simulations to examine hip joint stresses. In a recent finite element study that examined hip joint stresses caused by cam FAI, subject-specific hip contact forces were applied on segmented 3-D models and showed that elevated hip joint stresses not only were dependent on the cam morphology but also were attributed to secondary subject-specific characteristics (eg, joint loading direction, anatomic geometry, bone material properties). 56 Moreover, the finite element models that simulated symptomatic cam FAI had characteristic smaller femoral neck-shaft angles7,33,53,54,59 compared with asymptomatic and control individuals. It was also recently observed that symptomatic individuals indicated higher spinopelvic incidence angles, secondary to the cam morphology and varus neck parameters, which contributed to lower sagittal hip motions. 55 Anatomically, the combination of the varus neck and large pelvic incidence angle could result in different force vector direction of the iliopsoas tendon, psoas major, and capsular ligaments, where even a more superiorly positioned lesser trochanter would shorten the iliopsoas, resulting in anterior hip pain.7,13,23 This could suggest why individuals with FAI reduced their step lengths and walking speeds. In efforts to alleviate pain, clinicians who provide nonsurgical treatment of FAI should further emphasize core stability and muscle strengthening (iliopsoas, flexors, gluteal muscles) to alter sagittal plane moment arms and determine whether symptoms improve. 55 Similarly, asymptomatic cam individuals and postoperative cam patients may benefit from early targeted muscle strengthening. Not only would the psoas major and iliacus muscles function to protect the hip joint during flexion-extension,45,50 but proper athletic conditioning could further strengthen core muscles for improved hip mobility and pelvic balance.5,10,29,38 In the early stages of symptomatic FAI, it would be crucial to strategize effective nonsurgical management in efforts to optimize muscle strengthening regimens and delay the progression of clinical signs.
Limitations
First, our cohort consisted of only males. During the recruitment stage, very few female patients with clinical symptoms visited the clinical practice. As such, it was difficult to balance the participant groups with female participants without introducing additional sex-, age-, and BMI-related variances. 65 Symptomatic cam FAI is more prevalent in young, athletic males 30 ; however, study of statistical associations between sex, activity level, and symptoms is warranted in the future. Also, our symptomatic group was slightly older than the control group. Although age can influence walking and hip motions,3,65 several of our older FAI participants not only demonstrated higher amplitudes of hip motions and hip contact forces but also had faster walking speeds than control participants. Second, magnetic resonance imaging data of the entire lower limbs were not available; hence, the musculoskeletal model used in this study was based on cadaveric measurements and did not reflect detailed subject-specific anatomic features. Nonetheless, the current simulations were comparable to data from instrumented prostheses, where hip contact forces also reached up to 5 BW during similar walking speeds 12 ; this further reflects the importance of accounting for muscle contributions in joint loading.16,17,60 Third, the model was used within a consistent framework to compare a pathological group (FAI) with a healthy group (controls). Muscle forces were calculated through use of static optimization, which may not be able to model the muscle co-contraction mechanisms altered by a joint injury. However, static optimization provided muscle activations consistent with electromyographic measurements during various walking speeds 51 and did not require the additional measurements of muscle activities that typical electromyography-driven models would require. 14 Moreover, quadratic cost functions in static optimization have been used previously to estimate muscle forces 17 while also demonstrating similar results to computationally demanding algorithms. 4 Fourth, in addition to the comparative framework of our study design, inclusion of an asymptomatic group of FAI participants (with cam deformities but no clinical signs or pain) through a randomized controlled trial would provide further insights into differences in muscles contributions and hip joint loading.
Conclusion
This study provided insights into the link between cam FAI and hip contact forces. The FAI group’s altered gait mechanics (especially in hip extension) demonstrated a protective mechanism, to reduce psoas major and iliacus muscle forces, and resulted in lower hip contact forces.
Footnotes
Acknowledgements
The authors thank Kawan Rakhra, MD, FRCPC (The Ottawa Hospital, Canada) for his insight into the CT measurements, and Kevin Dwyer, MSc, and Danilo Catelli, MSc (Human Movement Biomechanics Laboratory, Canada), for their help and support during data collection.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from Canadian Institutes of Health Research (P.E.B. and M.L.) and Natural Sciences and Engineering Research Council of Canada (M.L.). The authors acknowledge funding contributions from the Han K. Uhthoff Graduate Fellowship (K.C.G.N.), Vanier Canada Graduate Scholarship (G.M.), and Imperial College Research Fellowship (L.M.).