
Abstract
Background:
The early recognition and management of patients with hip lesions, such as femoroacetabular impingement (FAI) and early hip osteoarthritis (OA), may preempt significant hip morbidity. The identification of reliable biomarkers may help guide decision making in an efficient and cost-effective manner.
Purpose:
To determine the biomarkers that have been associated with FAI as well as identify serum, synovial, and urinary analytes that have shown clinical utility in the prediction or identification of hip OA.
Study Design:
Systematic review and meta-analysis.
Methods:
The terms “hip arthroscopy,” “femoroacetabular impingement,” “labral tear,” “osteoarthritis,” and “biomarker” were searched in PubMed, Web of Science, Scopus, Cochrane Library, and Google Scholar, yielding 276 articles. After screening, 7 articles were included. Pooled estimates were calculated utilizing a fixed-effects inverse-variance model weighted for individual study size.
Results:
A total of 1747 patients with a mean age of 37.5 ± 4.5 years (76.4% female) were identified. Forty-three unique biomarkers were assessed. Although general proinflammatory cytokines IL-1 and TNF-α exhibited inconsistent trends in arthritic hips, IL-6 demonstrated a consistent increase (+84.8% [95% CI, 81.9%-87.6%]; P < .05). A significant difference was found in levels of the fibronectin-aggrecan complex (FAC) in patients with OA compared with controls (0.08 ± 0.40 vs 1.15 ± 0.35 μg/mL, respectively; P < .001). It was the only specific analyte to show a significant difference between those with and without OA. In the setting of FAI, cartilage oligomeric matrix protein (COMP) was significantly increased in athletes after adjusting for concurrent knee and hip OA. A statistically significant difference was present in FAI-positive hips (9.0 ± 0.1 [95% CI, 8.8-9.3]) compared with controls (8.4 ± 0.1 [95% CI, 8.2-8.4]) (P < .05). Other biomarkers, such as CXCL3, which exhibited statistically significant differences compared with controls, did not control for underlying factors such as age and concomitant lesions.
Conclusion:
COMP and FAC are specific biomarkers with potential utility in the diagnosis and management of FAI and hip OA, given their ability to differentiate between controls and patients with hip lesions. Further research is necessary to identify their ability in determining disease severity, predicting the response to treatment, and establishing an association with the risk of long-term OA.
Keywords
Femoroacetabular impingement (FAI) occurs because of abnormal contact between the proximal femur and acetabulum during hip joint motion and may subsequently lead to labral tears, accelerated cartilage damage, and joint degeneration.3,16,17,21,26 Surgical management involves the arthroscopic resection of bony overgrowth unless contraindications exist that necessitate a mini-open or surgical dislocation approach.18,21 Radiographic markers assessing the severity of hip osteoarthritis (OA), such as Tönnis grade ≥2, are associated with a higher risk of conversion to total hip arthroplasty.4,6
A rapidly growing body of evidence indicates that primary hip OA, which was previously believed to be a natural result of aging, is caused by FAI.10,12,13,27 The prevalence of radiographic findings of cam FAI in the asymptomatic general public is 23.1%, while this value is as high as 54.8% in athletes. 8 This evidence is further supported by a 20-year longitudinal study that determined subclinical FAI deformities are independent risk factors for radiographically confirmed OA, independent of age, body mass index, and joint space width.10-12,27
In an effort to curtail the profound economic and health-related effects of hip OA, which exceeds $100 billion on an annual basis, multiple studies have examined the utility of serum and synovial biomarkers to assess disease severity as well as the progression or subsequent risk of OA. Patients with no evidence of OA who fail nonoperative management may undergo joint preservation surgery in comparison with those with severe arthritis who undergo total hip arthroplasty as an option. However, for patients with hip pain and mild radiographic evidence of degenerative changes, treatment options may be less clear for the clinician.
The preoperative identification of patients who would benefit from joint-preserving procedures may be accomplished by identifying the inflammatory state of their joint. 2 Additionally, the ability to detect the early stages of hip inflammation and cartilage breakdown in the setting of FAI may allow clinicians and surgeons to recommend appropriate treatments before disease progression. Although the current literature has shown serum biomarkers to be associated with the severity of knee OA, there are currently limited data indicating whether such trends apply to biomarkers of hip OA, a field that remains in its infancy. 20 If hip biomarker changes exhibit similar properties to that of the knee, research from these areas can be utilized to develop the knowledge in this field more rapidly.
The purpose of this systematic review and meta-analysis was to assess the biomarkers that have been associated with FAI and identify serum, synovial, or urinary markers that have shown clinical utility in the prediction or identification of hip OA.
Methods
Search Strategy
This systematic literature review was structured to adhere to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. An electronic search was conducted using 5 databases including PubMed, Web of Science, Scopus, Cochrane Library, and Google Scholar. Our search methodology included the following search terms in different combinations and variations thereof, with the use of Boolean operators, to ensure the inclusion of relevant articles: “hip arthrosc*,” “femoroacetabular impingement,” “FAI,” “osteoarthritis,” “labral tear,” and “biomarker.” Bibliographies of studies meeting the inclusion criteria were also reviewed.
Identification of Eligibility
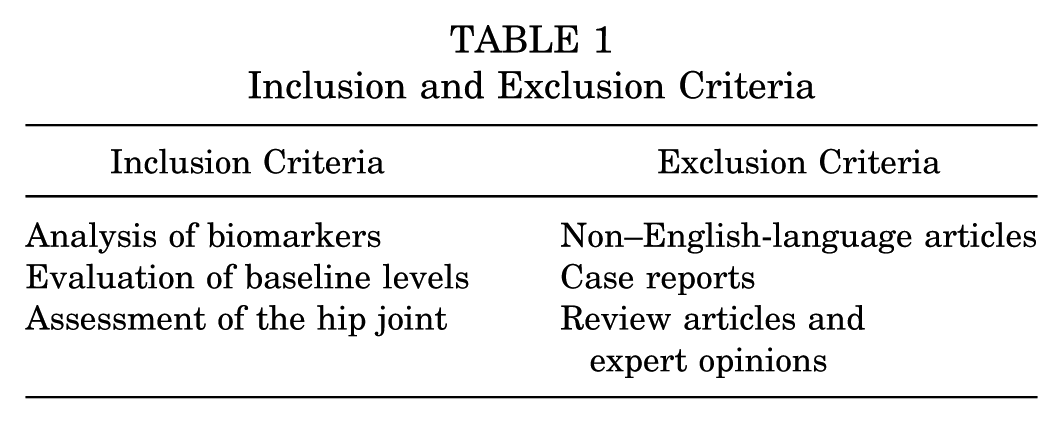
To be eligible for inclusion, a study must have assessed values of potential biomolecular analytes in patients with FAI, labral tears, or hip OA. Articles addressing circulating biomarkers after arthroscopic intervention while not reporting preoperative values were excluded. Case reports, review articles, and expert opinions (level 5) were excluded (Table 1).
Inclusion and Exclusion Criteria
Data Extraction, Statistical Analysis, and Quality Appraisal
The method of data extraction and computation followed the approach outlined by the Cochrane Handbook for Systematic Reviews of Interventions. Aggregate data from clinical studies were evaluated using a fixed-effects inverse-variance model. The quality of the included studies was calculated using the Coleman Methodology Score as determined by 2 reviewers (A.A.M., M.O.). A third tiebreaker (T.S.L.) was designated in the case of any disagreement.
Results
Eligibility
A total of 276 distinct publications were identified after a search through 5 electronic databases and the removal of 12 duplicates. Two hundred sixty-six articles were excluded based on the title or abstract of the article, while 3 were excluded after reading the full text. After applying the eligibility criteria, 269 total articles were excluded (Figure 1), and 7 articles were included (Table 2).
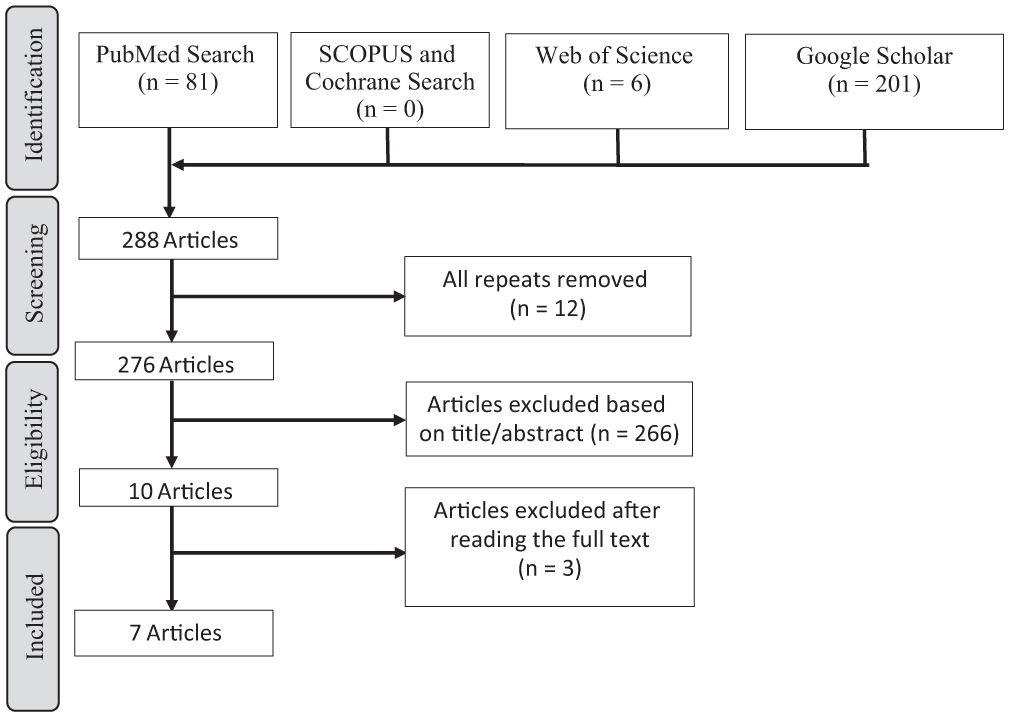
Study selection process (PRISMA [Preferred Reporting Items for Systematic Meta-Analyses] diagram).
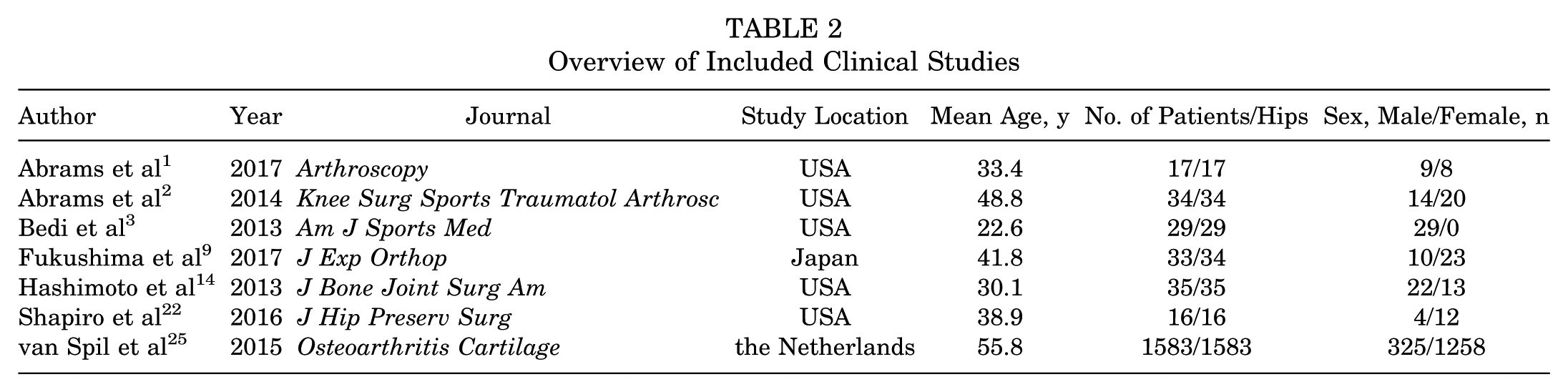
Overview of Included Clinical Studies
Patient Characteristics and Quality of Included Studies
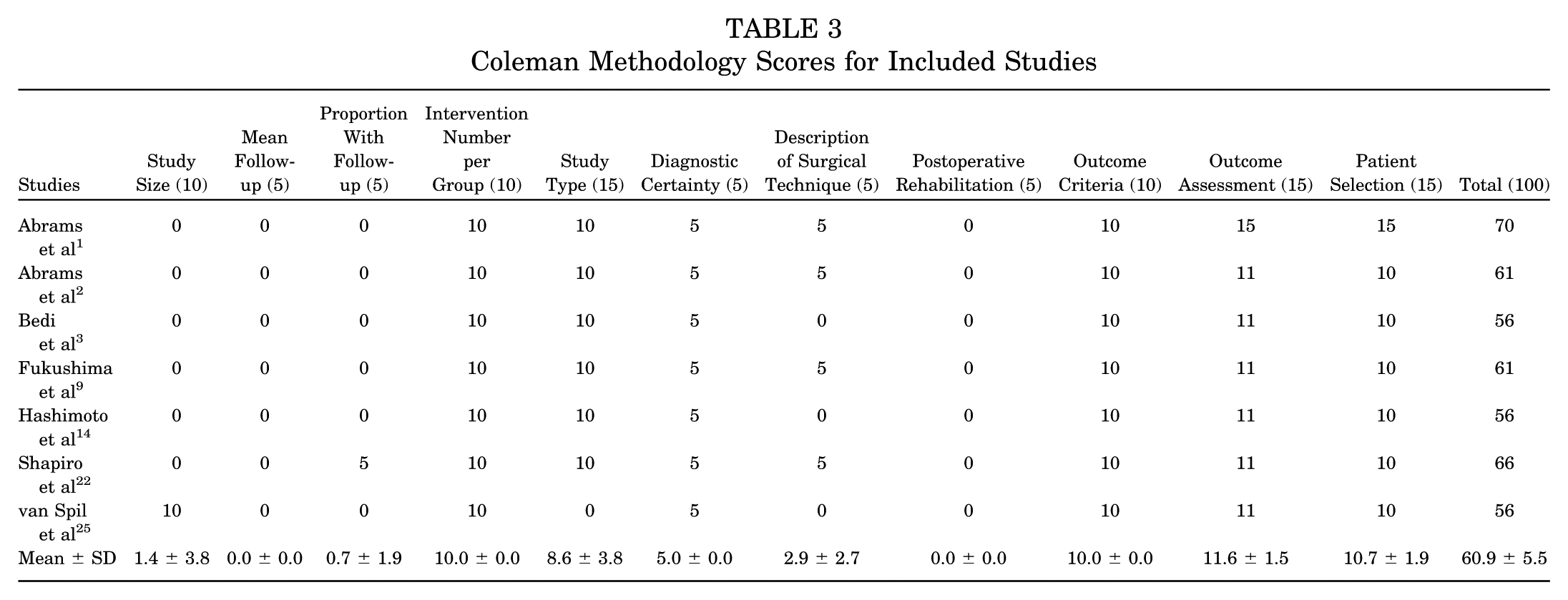
A total of 1747 patients were identified, with a mean age of 37.5 ± 4.5 years (76.4% female, 23.6% male). The mean modified Coleman Methodology Score was 60.9 ± 5.5 (Table 3). The included studies scored particularly well on diagnostic certainty in enrolled patients (5/5) and outcome criteria (10/10). The mean score for study size was poor (1.4/10), with 6 of 7 studies demonstrating an underpowered patient sample.
Coleman Methodology Scores for Included Studies
Overview of Assessed Biomarkers and OA
A total of 43 unique analytes were measured in 7 enrolled clinical studies (Table 4). The most commonly evaluated markers were general proinflammatory cytokines: IL-1 (4/7), IL-6 (3/7), and TNF-α (3/7) (Table 4). Although IL-1 and TNF-α exhibited inconsistent trends in arthritic versus nonarthritic groups, TNF-α demonstrated a significant increase when subchondral bone was exposed, as indicated by a grade 4 Outerbridge classification. 9 IL-6 demonstrated a consistent increase in OA, with a pooled estimate of +84.8% (95% CI, 81.9%-87.6%; P < .05). Of note, a biomarker identified as the fibronectin-aggrecan complex (FAC), a cartilage breakdown product, was found to be significantly higher in patients without OA (0.08 ± 0.40 vs 1.15 ± 0.35 μg/mL, respectively; P < .001) (Figure 2).
Assessed Biomarkers in 7 Clinical Studies a
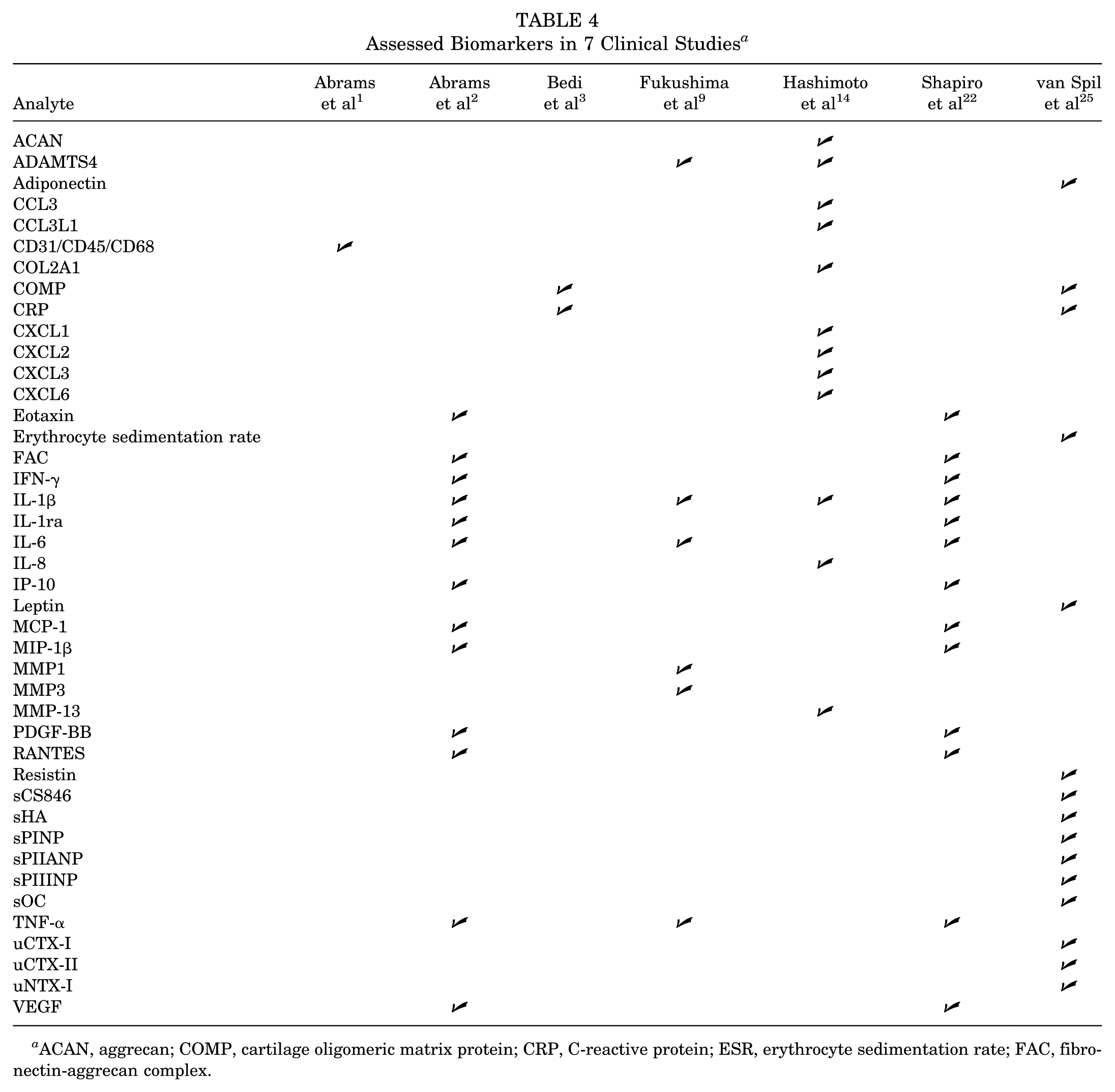
ACAN, aggrecan; COMP, cartilage oligomeric matrix protein; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; FAC, fibronectin-aggrecan complex.
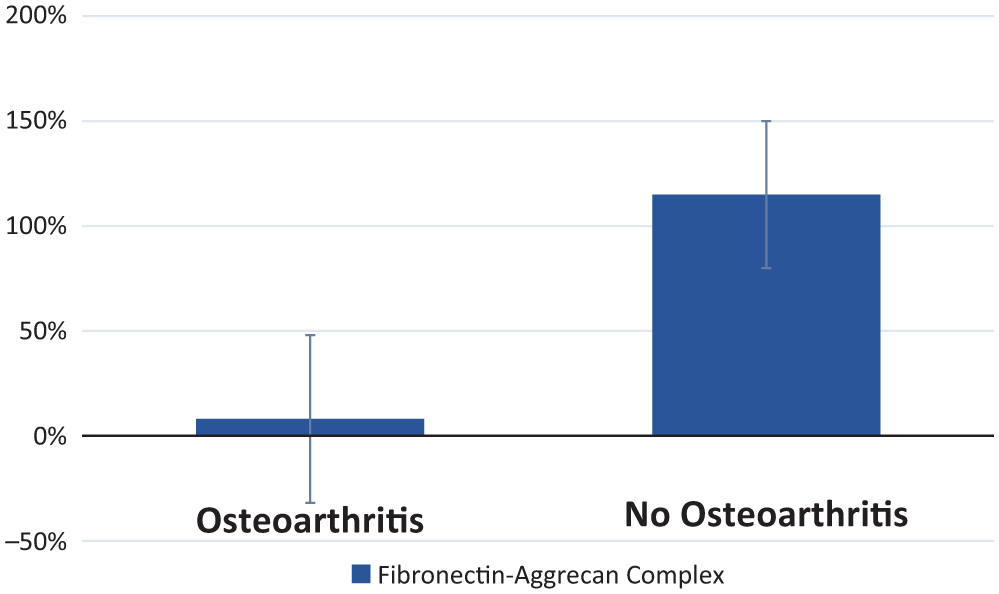
Change in fibronectin-aggrecan complex levels in arthritic hips.
FAC was the only analyte to show a significant difference between those with and without OA when analyzing 13 separate biomarkers (Table 5). Most importantly, age was not a significant predictor of FAC concentration (P > .05) and accounted for <1% of the FAC variance. 2 Notably, it was found that the presence of ≥2.18 µg/mL was 78% sensitive and 84% specific for predicting microfracture in the nonarthritic group, indicating near excellent accuracy with an area under the receiver operating characteristic curve of 0.87. 2 In a study that examined available hip and knee data but did not assess FAC, biomarker and adipokine associations with OA disappeared when controlling for demographics and higher baseline levels. 25
Association of Biomarker Levels With OA a
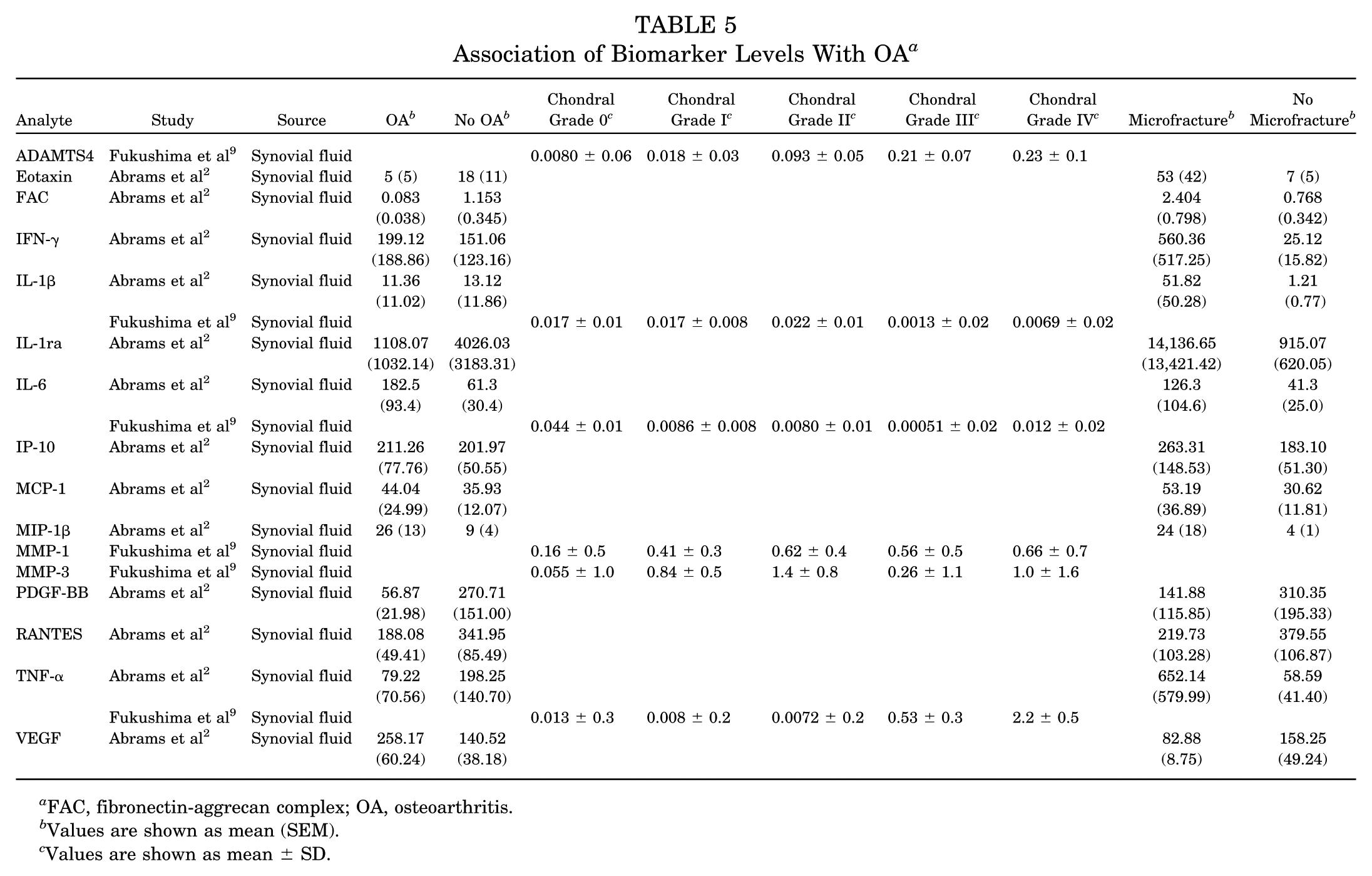
FAC, fibronectin-aggrecan complex; OA, osteoarthritis.
Values are shown as mean (SEM).
Values are shown as mean ± SD.
Microfracture
Patients undergoing microfracture demonstrated lower rates of tissue degradation as shown by lower levels of growth-related factors, including platelet-derived growth factor and vascular endothelial growth factor (Figure 3). 2 Additionally, FAC also exhibited significantly higher concentrations in patients without radiographic evidence of OA undergoing microfracture compared with those not undergoing microfracture (P < .05) (Figure 3). 2
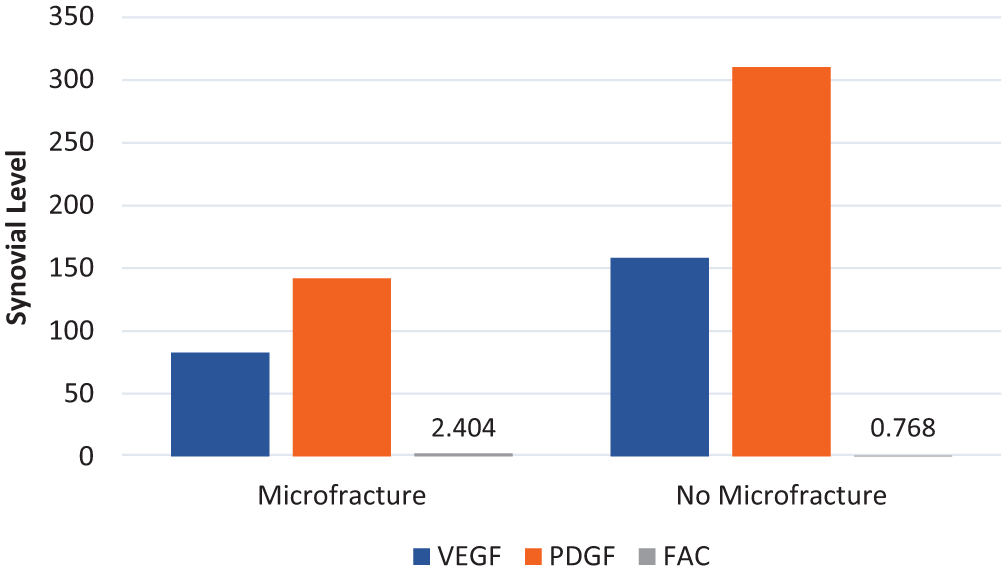
Difference in growth factors associated with microfracture, which is associated with higher levels of FAC. FAC, fibronectin-aggrecan complex; PDGF, platelet-derived growth factor; VEGF, vascular endothelial growth factor.
Femoroacetabular Impingement
Three studies looked at 18 analytes specifically in the setting of FAI (Table 6).3,14,25 Only 1 of these studies addressed FAI generally, 14 while 1 focused on impingement in the male athlete, 3 and another 25 only addressed cam impingement.
Analyte Levels in FAI a
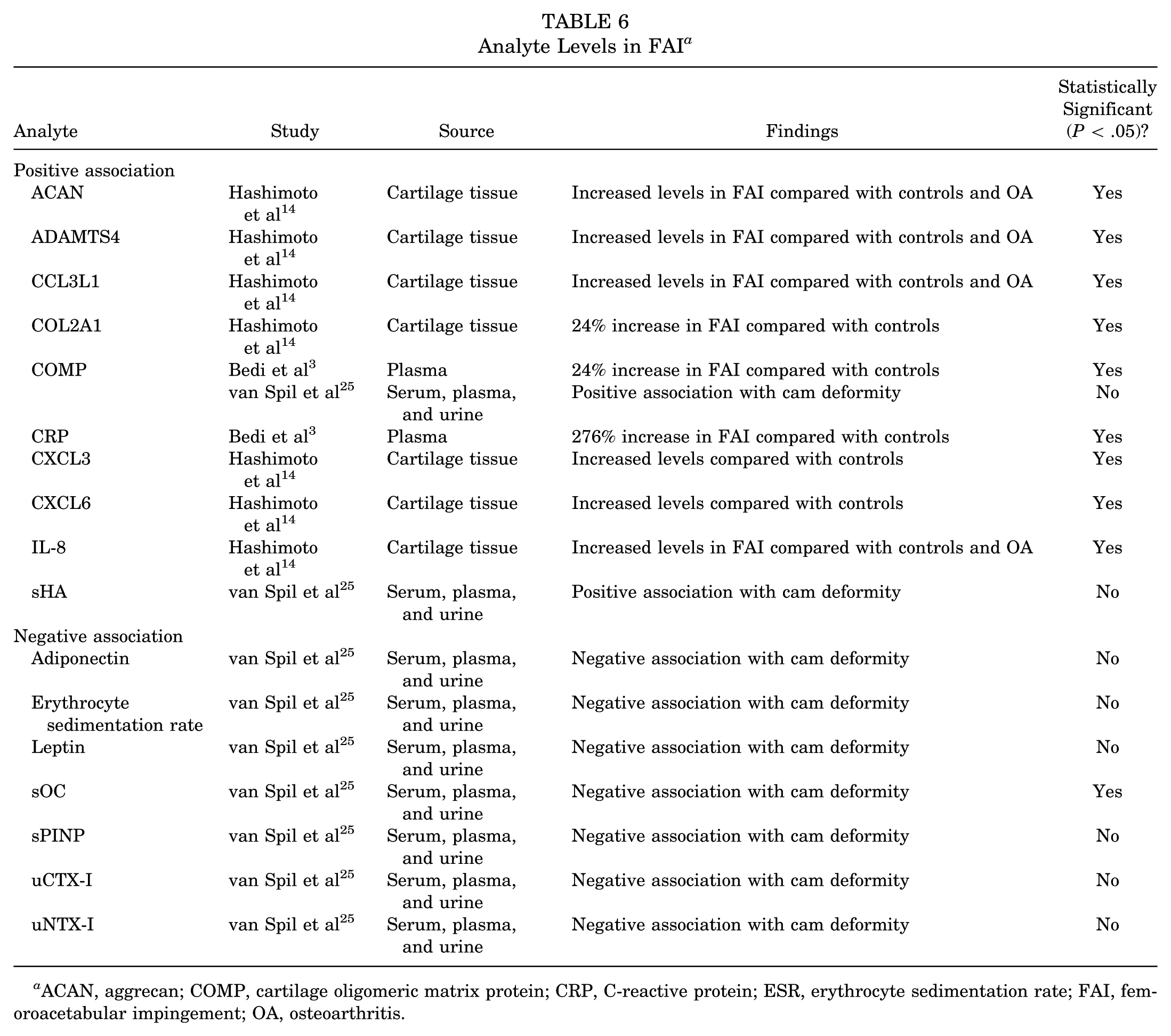
ACAN, aggrecan; COMP, cartilage oligomeric matrix protein; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; FAI, femoroacetabular impingement; OA, osteoarthritis.
Patients with FAI were found to have significantly higher levels of CXCL3, CXCL6, and COL2A1 when compared with controls (P ≤ .05) and significantly higher levels of IL-8, ADAMTS4, CCL3L1, and aggrecan (ACAN) compared with both controls and patients with OA (P ≤ .05). 14 However, these values did not control for underlying factors such as age and concomitant lesions.
A notable biomarker, cartilage oligomeric matrix protein (COMP), was significantly increased in athletes with all types of FAI compared with controls (P < .05).3,25 Additionally, it was positively associated with the presence of cam deformity even after adjusting for concurrent knee and hip OA. No other markers of cartilage metabolism were associated with cam deformity in this study (FAC was not assessed in this study). 25
The pooled estimate revealed a statistically significant difference, with FAI-positive hips demonstrating a serum COMP level of 9.0 ± 0.1 U/I (95% CI, 8.8-9.3) compared with controls (8.4 ± 0.1 U/I; 95% CI, 8.2-8.4) (P < .05) (Figure 4).
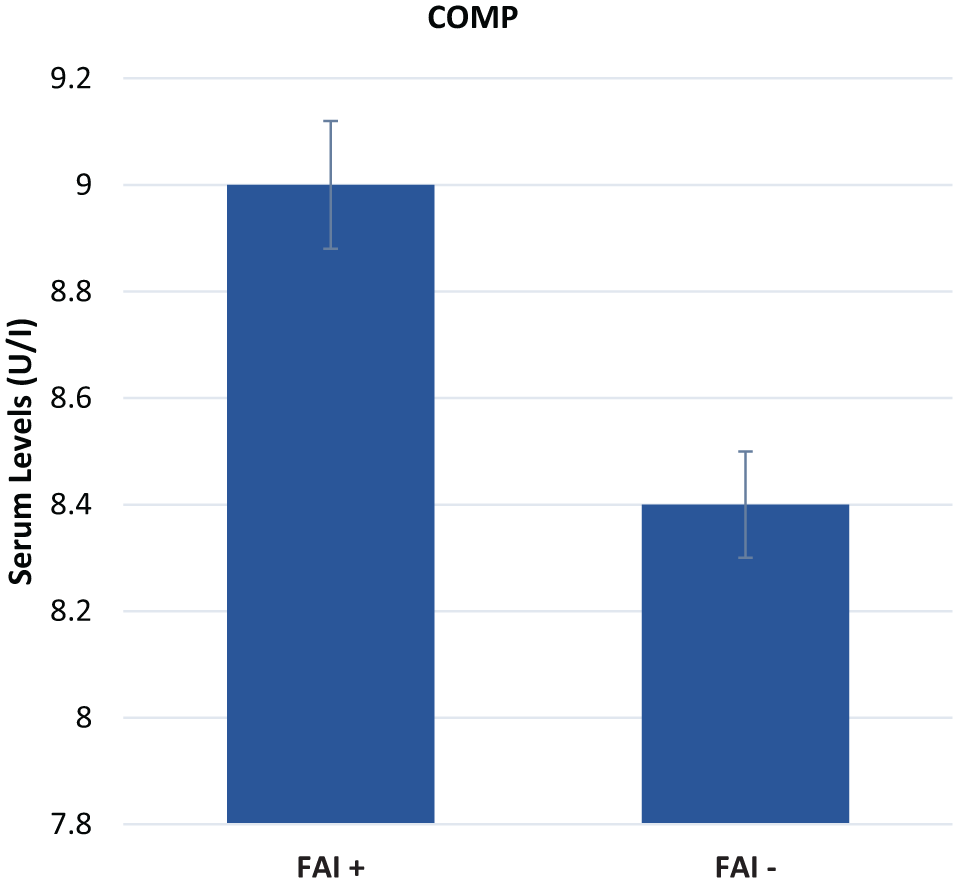
Statistically significant difference in serum cartilage oligomeric matrix protein (COMP) levels in femoroacetabular impingement (FAI)–positive versus FAI-negative hips.
Labral Tears
One study specifically assessed the difference in 6 analyte levels between patients with labral tears and those without (Table 7). 9 No significant difference was found in the levels of any of the 6 analytes between the labral tear and non–labral tear groups. Additionally, no analyte levels were found to have any significant difference between patients with hip instability and those without.
Analyte Levels Associated With Labral Tears and Hip Instability a
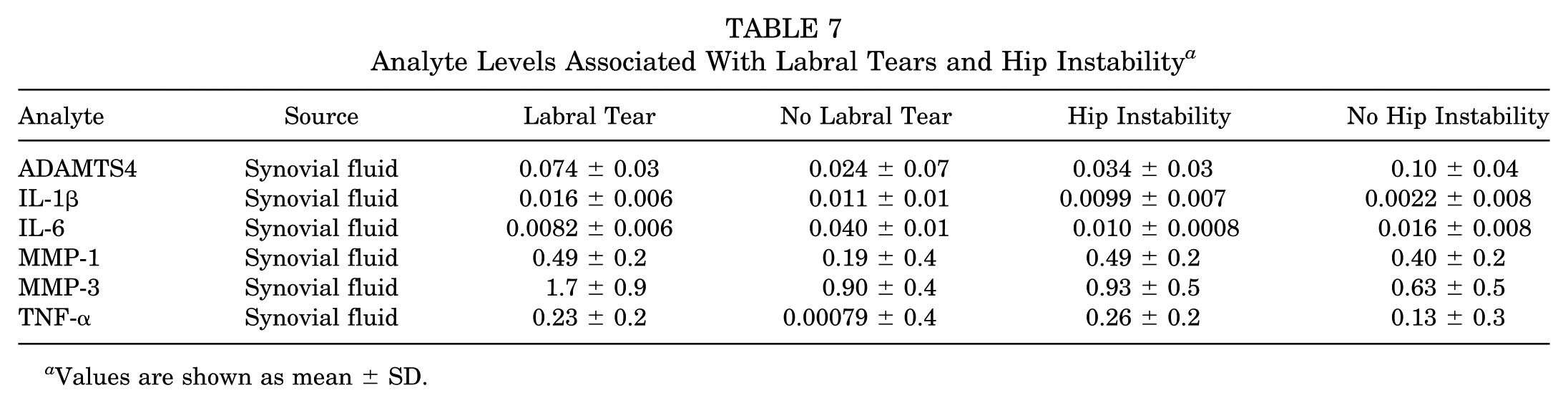
Values are shown as mean ± SD.
Synovitis
Two studies assessed the correlation between inflammation of the hip synovial membrane and analyte levels.1,9 Patients with diffuse synovitis exhibited significantly higher values of IL-1β, IL-6, TNF-α, and MMP-1. 9 No significant difference was found between the level of synovitis in patients with FAI compared with those with hip instability (P = .186). 1 Similarly, no significant correlation was found between the existence of a labral tear or instability and inflammation of the synovial membrane. 9 It was found, however, that patients undergoing microfracture for FAI had significantly higher inflammation than those not undergoing microfracture (P = .024). 1
Immunohistochemistry
A single study looked at the presence of inflammatory cells in patients with FAI compared with those with hip instability by evaluating CD45 (leukocyte antigen) and CD68 (macrophage) with immunohistochemistry. 1 The number of these cells was not significantly different between the 2 patient groups, nor was it significantly correlated with patient-reported outcomes. Patients with cam impingement (P = .045) as well as those undergoing microfracture (P = .035) expressed significantly more CD68+ cells.
Discussion
This systematic review and meta-analysis evaluated 7 clinical studies with a total of 1747 patients to determine if there are any known biomarkers that have been linked to FAI as well as to identify serum, synovial, or urinary markers that have shown clinical utility in the identification of hip OA. A total of 43 unique analytes, including serum, synovial, and urine biomarkers, were identified. Although general proinflammatory markers IL-1 and TNF-α exhibited inconsistent trends in arthritic hips, IL-6 demonstrated a consistent increase in OA (+84.8%; P < .05). Additionally, a cartilage breakdown product, FAC, was found to be significantly higher in patients without OA (0.08 vs 1.15, respectively; P < .001). It was the only specific analyte to show a significant difference between those with and without OA, with age accounting for <1% of variance and an area under the receiver operating characteristic curve of 0.87, demonstrating near excellent accuracy.
In the setting of FAI, COMP was significantly increased in athletes with all 3 lesion types compared with controls and was positively associated with the presence of cam deformity. This association persisted even after adjusting for concurrent knee and hip OA, whereas no other markers of cartilage metabolism were associated with cam deformity. 25 The pooled estimate revealed a statistically significant difference between patients with FAI and controls. An evaluation of COMP in FAI may be clinically useful and warrants further discussion.
Nonspecific markers such as C-reactive protein (CRP) have been evaluated as potential biomarkers for FAI. 3 The release of CRP is linked to increased inflammatory cytokine levels, and as a result, its levels can rise because of varying reasons such as trauma or infection 7 as with IL-1 and TNF-α. CRP would likely not be useful as a diagnostic biomarker for FAI because of the plethora of causes for high CRP levels. COMP, however, is an indicator of cartilage damage, and increasing levels of this molecule are reflective of disease severity. 5 Because COMP has the potential to indicate the progression of FAI, it may be useful to clinicians for determining whether to be more aggressive with surgical management. This evidence is also supported by the findings demonstrated by Clark et al 5 in which serum COMP levels correlated with knee OA severity as determined by the Kellgren-Lawrence grade (method of classifying the severity of knee OA), knee laterality, inclusion of hip OA, and total number of affected knee and hip joints. Young patients, who are predominant in the FAI population, are unlikely to have concomitant knee OA, further increasing the anticipated specificity of COMP.
Additionally, because FAI can lead to labral tears, accelerated cartilage damage, and consequent joint degeneration due to repetitive contact between the acetabulum and proximal femur, markers have been evaluated in association with labral tears and synovitis. However, an assessment of 6 analytes between the labral tear and non–labral tear groups showed no significant difference. 9 Similarly, no significant correlation was found between the existence of a labral tear or instability and inflammation of the synovial membrane. 9 Abrams et al 1 also investigated whether biomarkers would increase with hip instability. No significant difference was found between the level of synovitis in patients with FAI compared with those with hip instability (P = .186). Additionally, immunohistochemistry techniques did not show significant differences. Other biomarkers that showed a significant difference between FAI and OA compared with control groups, such as CXCL3, CXCL6, COL2A, ADAMTS4, CCL3L1, and ACAN, failed to control for underlying factors such as age and concomitant lesions 14 ; for these reasons, we cannot recommend clinical correlations until these are further studied. Multiple studies have investigated whether biomarkers would increase with hip instability.
Of particular importance in the progression to OA in patients with FAI is the increased expression of ACAN, disintegrin, and metalloproteinase. ADAMTS4 is a protein that when upregulated leads to an increase in proteases that degrade ACAN, which is a proteoglycan found in cartilage. 19 The increased production of ACAN is important in cartilage repair. 19 This is supported by the finding that FAC, another biomarker of cartilage breakdown, is significantly higher in nonarthritic hips undergoing arthroscopic surgery with microfracture compared with nonarthritic hips undergoing arthroscopic surgery without microfracture. 15 However, it is important to note that FAC was only found to be a significant biomarker by 1 study, which included 34 patients. 2 Although FAC exhibited a significant difference between those with and without OA (P < .001), the study attained an intermediate Coleman Methodology Score of 61, indicating sufficient study quality and methodology. As such, further research is necessary to determine whether FAC, which is currently a promising biomarker as proven by the aforementioned data, is a suitable biomarker that is useful in the designation of operative management.
Significance and Limitations
The early recognition and subsequent management of patients with hip lesions may preempt significant hip morbidity. Pain around the hip joint is increasingly challenging to diagnose, and in contrast to other joints, there are no systematic hip evaluation protocols to prevent a missed diagnosis.17,24 Furthermore, advanced imaging such as magnetic resonance imaging and 3-dimensional computed tomography to aid in the diagnosis of FAI after plain radiographs imposes significant costs.23,27 The introduction of a reliable biomarker can help guide decision making in an efficient and cost-effective manner. 21 Additionally, the validation of a biomarker can render it an efficient and low-cost predictor of the clinical response to nonoperative management or operative intervention. By analyzing its association with postoperative function, return-to-play rate, and duration, preoperative values can be used in evidence-based preoperative guidance.
Furthermore, 3 of the 7 studies included intra-articular injections per the reported methodology.1,9,10 Performing such injections may alter biomarker levels as well as inflammatory states. The current literature does not show whether intra-articular injections discordantly alter biomarker levels in arthritic and nonarthritic groups. We must also note that further studies are necessary as the data present a significant sex bias, with 76.2% of patients being female. Additionally, correlating imaging findings with biomarkers across patient groups may provide novel data regarding the utility of biomarkers as patients progress to hip OA.
To the authors’ knowledge, this is the first focused systematic review of biomarkers in FAI and hip OA to identify which biomolecules demonstrate clinical utility. We have determined that a considerable gap remains in the current peer-reviewed literature for how biomarkers can be used to the physician’s advantage as a clinical diagnostic and decision-making tool for FAI and hip OA as many of the investigated biomarkers are of a nonspecific nature. This review, however, has its limitations. Only 7 studies met the inclusion criteria of addressing biomarkers in the nonarthritic hip. While this may be a limitation of our study, it is also an indication of the lack of research on this topic as well as an area for future study.
Conclusion
This study has identified COMP and FAC as biomarkers with potential utility in the diagnosis and clinical management of FAI and hip OA, respectively, given their ability to differentiate between control groups and patients with hip lesions. However, while these biomarkers have been identified, their applicability as a diagnostic tool in assessing disease severity, predicting clinical responses, and predicting long-term OA remains unknown. If biomarkers are to be used as a tool for determining care management for patients, it is imperative that further research be done to identify thresholds of serum or synovial levels that can be beneficial in identifying nonoperative treatment versus operative management because of the severity of hip lesions.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: R.W.W. has received education and hospitality support from Arthrex, hospitality support from Medical Device Business Services, and education and hospitality support from Smith & Nephew. J.T.R. has received education, hospitality, and other financial support from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.