
Abstract
Background:
Surgical treatment to repair partial anterior cruciate ligament (ACL) injury without reconstruction has demonstrated inconsistent clinical success.
Purpose:
To examine the long-term clinical outcomes of primary ACL repair combined with biologic healing augmentation in patients with symptomatic partial ACL tears.
Study Design:
Case series; Level of evidence, 4.
Methods:
50 patients (mean age, 29.5 years) with a partial ACL tear and symptomatic knee instability were treated with primary ligament repair in conjunction with marrow stimulation and followed prospectively for a mean duration of 10.2 years (range, 5.3-14.3 years). Comparative analysis of preinjury, preoperative, and postoperative scores using patient-reported assessment instruments was performed to examine clinical outcomes. Correlation of final outcome scores with patient age, type of ACL tear, side-to-side difference in ligamentous laxity, and body mass index (BMI) was performed through use of Spearman rank analysis.
Results:
44 patients were available for assessment at final follow-up. The median Tegner Activity Scale score of 7 at final follow-up was the same as the preinjury median score of 7 (P = .128). The mean Marx Activity Scale, International Knee Documentation Committee (IKDC) Subjective, and Lysholm Knee Questionnaire scores were 10.8, 90.4, and 96.2, respectively, at final follow-up. Mean final Knee injury and Osteoarthritis Outcome Score (KOOS) subset assessments of Pain, Symptoms, Activities of Daily Living, Sports, and Quality of Life were 98.6, 97.5, 99.7, 94.3, and 95.6, respectively. Secondary ACL insufficiency occurred in 27% of patients. Clinical outcome scores were similar for all scoring instruments between patients treated for an associated diagnosis of meniscal or articular cartilage injury. No significant correlations of age, BMI, ACL tear type, or laxity and final IKDC Subjective, Lysholm, or KOOS scores were found. Analysis revealed a negative correlation of patient age and Tegner score at preinjury (rs = −0.333, P = .022) and at final follow-up (rs = −0.376, P = .013). The mean side-to-side difference in ligamentous laxity of 3.4 mm at short-term follow-up in those patients who developed secondary ACL insufficiency over the duration of follow-up was significantly greater than the mean of 0.9 mm in those who did not (P = .010).
Conclusion:
Primary ACL repair combined with biologic healing augmentation to treat select cases of knee instability secondary to incomplete ACL rupture demonstrated good to excellent long-term outcomes in this cohort for those patients who did not experience secondary ACL insufficiency, with high rates of restoration of knee stability and return to preinjury athletic activities. The rate of secondary treatment for recurrent ACL insufficiency over the course of long-term follow-up was greater than would be expected for primary ACL reconstruction. Greater side-to-side differences in objective findings of ligamentous laxity were identified at shorter term follow-up in the patients who later went on to experience symptomatic secondary ACL insufficiency, compared with those who maintained stability long term.
Keywords
The anterior cruciate ligament (ACL) provides crucial stabilizing function for the knee joint, and surgical treatment of ACL injury is often performed to restore knee stability, with the goal of enabling return to activities at the desired level of function. Surgical reconstruction procedures using autograft or allograft tissues have been used with success over many decades to treat symptomatic knee instability secondary to ACL insufficiency. This treatment, while successful, does not perfectly restore kinematics of the knee joint and has not been shown to prevent the development of degenerative cartilage changes.29,46 Additionally, complications are associated with reconstruction procedures related to autograft harvest, hardware failure, fracture, and bone tunnel widening with potential for pathologic cystic dilatation. 38
Although reconstruction has been a standard method of treatment for symptomatic ACL insufficiency, irrespective of ACL tear pattern, reconstruction of partially torn ligament fibers may sacrifice native tissue that has important proprioceptive and biomechanical function. Primary repair of the ACL has been described previously, and this method of treatment has demonstrated clinical outcomes of variable success.23,39,43,45,47
Growth factors and cellular elements contained within marrow have the potential to assist with repair of damaged ACL tissue12,25,44 and, when combined with surgical apposition of torn ligament fibers in cases of partial injury, may promote the generation of healthy repair tissue with retained proprioceptive and mechanical properties better able to restore native joint kinematics. Short-term clinical outcomes and return to sport have been examined previously in a cohort of patients who underwent treatment of partial ACL tears that entailed primary repair and biologic healing augmentation, with good to excellent results achieved. 18
The purpose of this study is to examine the long-term clinical outcomes of primary ACL repair combined with biologic healing augmentation in patients with symptomatic partial ACL tears.
Methods
Patients who underwent primary ligament repair with biologic healing augmentation to treat partial ACL tears at our institution between 2004 and 2012 were prospectively followed. Shorter term clinical follow-up for a subset of this cohort has been published previously. 18 Inclusion criteria consisted of an acute sports-related ACL tear diagnosed within 4 weeks of injury, in patients with symptomatic instability, examination findings of positive or glide jerk test, increased anterior laxity with Lachman testing that demonstrated 3- to 5-mm side-to-side difference in maximum anterior tibial translation, magnetic resonance imaging (MRI) findings consistent with an acute partial ACL injury, and follow-up for a minimum of 5 years. Appropriateness for treatment by primary repair with biologic healing stimulation was confirmed by arthroscopic findings of incomplete ACL tear based on visualization and probing of the anteromedial (AM) and posterolateral (PL) ACL bundles at the time of surgery. ACL tears were categorized into 4 groups: type 1 was considered to be a partial (<100%) lesion of the AM bundle with an intact PL bundle, type 2 was a partial (<100%) lesion of the PL bundle with an intact AM bundle, type 3 consisted of a partial lesion of both the AM and PL bundles, and type 4 was a complete ACL tear. Incomplete tears of the ACL consistent with type 1, 2, or 3 lesions were considered for treatment with primary repair and biologic healing augmentation. For type 3 lesions, the study included those cases in which 50% or less of both bundles were torn. Exclusion criteria consisted of ACL lesions in which the ligamentous fibers could not be reapproximated with suture, International Cartilage Repair Society grade 4 injury to articular cartilage, posterior cruciate ligament injury, lateral collateral ligament injury, grade 3 (complete disruption) medial collateral ligament (MCL) injury, significant malalignment, contralateral knee injury, and inability of the patient to adhere to the postoperative rehabilitation protocol.
All procedures were performed by the senior author (A.G.) and were completed within 4 weeks of injury. Nonoperative and operative treatment protocols were discussed with each patient before treatment. Standard methods to reconstruct the ACL were specifically discussed, in addition to the treatment method of primary repair with biologic healing stimulation. Those patients who chose not to participate underwent standard ACL reconstruction with hamstring autograft. Patients were followed prospectively via scoring instruments consisting of the Tegner Activity Scale, the Marx Activity Rating Scale, the Lysholm Knee Questionnaire, the International Knee Documentation Committee (IKDC) Subjective score, and the Knee injury and Osteoarthritis Outcome Score (KOOS) subsets of Pain, Symptoms, Activities of Daily Living (ADL), and Quality of Life (QOL). An independent examiner evaluated anterior knee laxity postoperatively at short-term follow-up and long-term final follow-up with a Rolimeter by measuring the side-to-side difference of anterior tibial translation in millimeters, using a manual maximum test. 17 Postoperative complications, recurrent instability, and reinjury were tracked over the duration of follow-up. Patients who experienced recurrent instability or reinjury consistent with ACL insufficiency were treated with a standard ACL reconstruction procedure. Data obtained from the most recent clinical evaluation before treatment for secondary ACL insufficiency were used in cases of treatment failure. The study protocol was approved by the local institutional ethics committee.
Surgical Technique
Patients were positioned supine in a manner typical of knee arthroscopy and standard ACL reconstruction and were given a spinal or general anesthetic. While the patient was under anesthesia, the knee was examined to confirm knee instability consistent with ACL insufficiency. A diagnostic arthroscopy was performed to examine the ACL and to confirm a partial tear amenable to the primary repair technique. Lachman and jerk tests were performed under direct visualization. Associated partial-thickness chondral injuries were treated with chondroplasty as needed, and meniscal injuries were treated with partial meniscectomy or all-inside suture repair, depending on the pattern of injury.
ACL repair was performed by passing polydioxanone No. 1 sutures (Ethicon) through the distal and proximal remnant ACL tissue at the site of tear by use of a suture passing device, and the torn ligament fibers were reapproximated and secured with a Duncan loop. Two or 3 sutures were used in each case to ensure taut reapproximation of ligament fibers and to eliminate gapping between the proximal and distal fibers. A 45° microfracture awl was then used to create 1.5 mm–diameter holes, 3 mm deep and 3 to 4 mm apart, at the lateral aspect of the intercondylar notch, about the anatomic femoral footprint of the native ACL. Care was taken to avoid injury to residual ACL tissue.
Primary repair procedures that entailed repair of more than 50% of an ACL bundle were treated with a biologic gel consisting of activated platelet-rich plasma (PRP) and bone marrow aspirate concentrate (BMAC) to improve sequestration of the repair site from circulating intra-articular plasmin and catabolic factors (Angel; Cytomedix). Approximately 5 mL of PRP/BMAC was activated by use of batroxobin enzyme (Plateltex Act; Plateltex S.R.O.) to create an adhesive gel. After primary ACL repair and marrow stimulation, fluid was removed from the articular space, and the activated PRP/BMAC gel was applied to the repaired ligament under dry arthroscopy. Primary ligament repair with biologic healing augmentation is depicted in Figure 1.
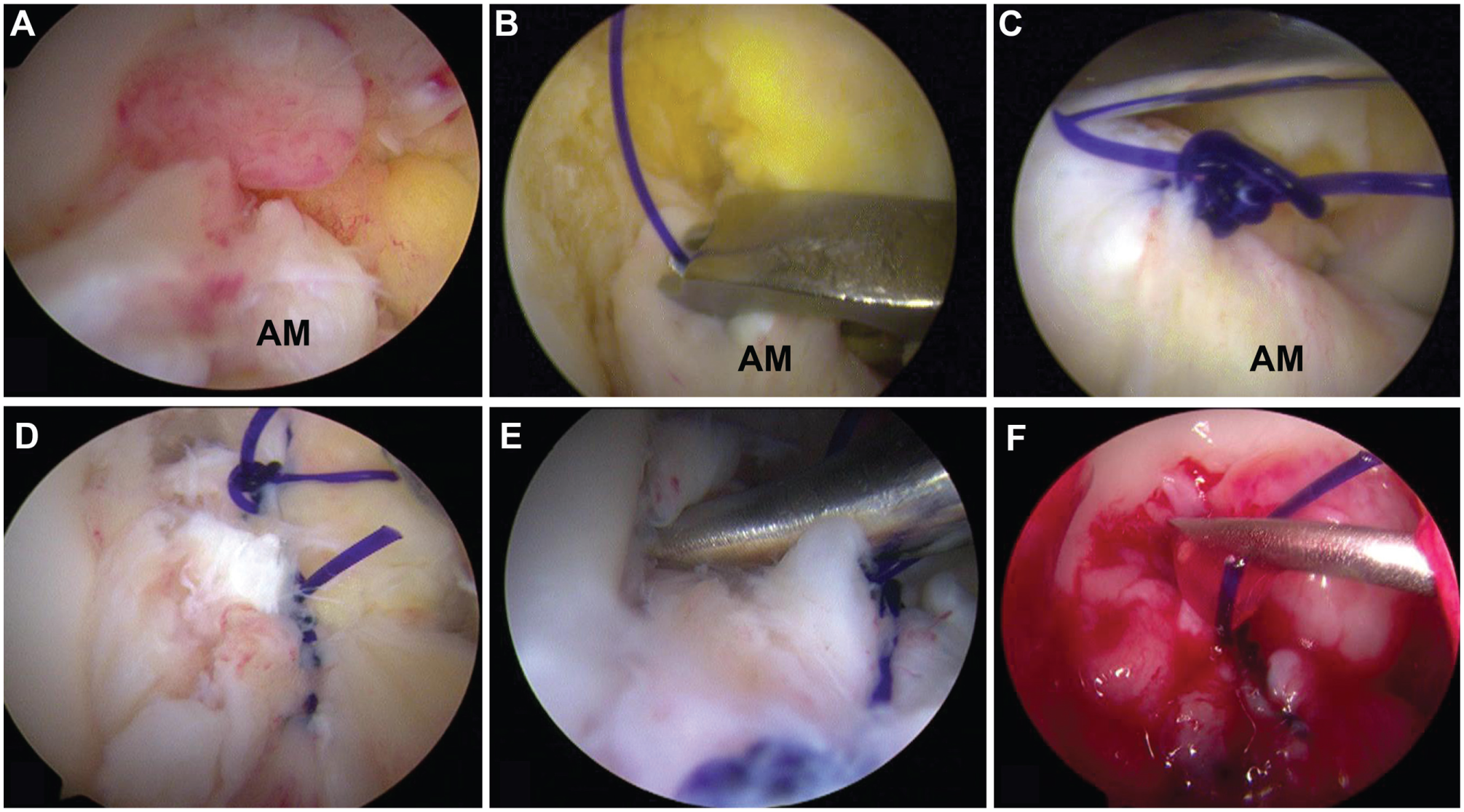
(A) Partial tear of the anterior cruciate ligament (ACL) anteromedial (AM) bundle. (B) Arthroscopic passage of No. 1 PDS suture through torn ACL. (C) Arthroscopic tensioning of suture by use of a knot pusher. (D) Torn ACL fibers reapproximated by suture fixation. (E) Microfracture awl used to perform marrow stimulation about anatomic footprint of ACL on lateral aspect of intercondylar notch. (F) Application of clot-activated platelet-rich plasma/bone marrow aspirate concentrate gel to site of ACL repair.
Rehabilitation Protocol
All patients followed the same rehabilitation protocol postoperatively. The knee was kept in a position of extension within a brace for a period of 3 weeks, and partial weightbearing was allowed with the assistance of crutches. Progression to weightbearing as tolerated was allowed after 3 weeks. Continuous passive motion (CPM) was started on postoperative day 1, for a duration of 4 to 6 hours per day, and was set initially at 20° to 60°. CPM was gradually increased daily, with 90° of flexion expected by 2 weeks postoperatively, followed by passive flexion exercises to increase flexion to 120°. Full active range of motion was allowed 6 weeks postoperatively. Straight-line running began 3 months postoperatively, with high-intensity exercise restricted until at least 4 to 5 months postoperatively, depending on patient activities and readiness.
Statistical Analysis
Data analysis was performed with SPSS software (version 22.0; IBM). Shapiro-Wilk tests and quantile-quantile plots were used to assess normality of continuous variables. Continuous variables were expressed as mean or median values followed by the SD, range, or interquartile range (IQR) where appropriate. Hypotheses testing regarding differences in continuous variables between preinjury, preoperative, and postoperative continuous variables was performed with the Student t test. The independent-samples t test was performed to examine differences in continuous data between participants grouped by sex, by those who did or did not undergo an associated procedure, by method of biologic augmentation, and by success or failure of procedure. One-way analysis of variance was performed to examine differences between groups after categorization of ACL injury type and categorization of associated lesions as meniscal, chondral, or combined (meniscal and chondral), with post hoc Tukey analysis performed where appropriate for multiple comparisons. Difference in the frequency of ACL tear type was examined within groupings through use of the 1-sample chi-square test and between groupings through use of the Fisher exact test. Spearman rank correlation coefficient was calculated to examine associations between outcome scores and age at surgery, body mass index (BMI), ACL tear type, and objective findings of laxity. The Kaplan-Meier survival function was used to examine survival rates. Two-tailed comparative analysis was used, and the level of statistical significance was considered to be P < .05.
Results
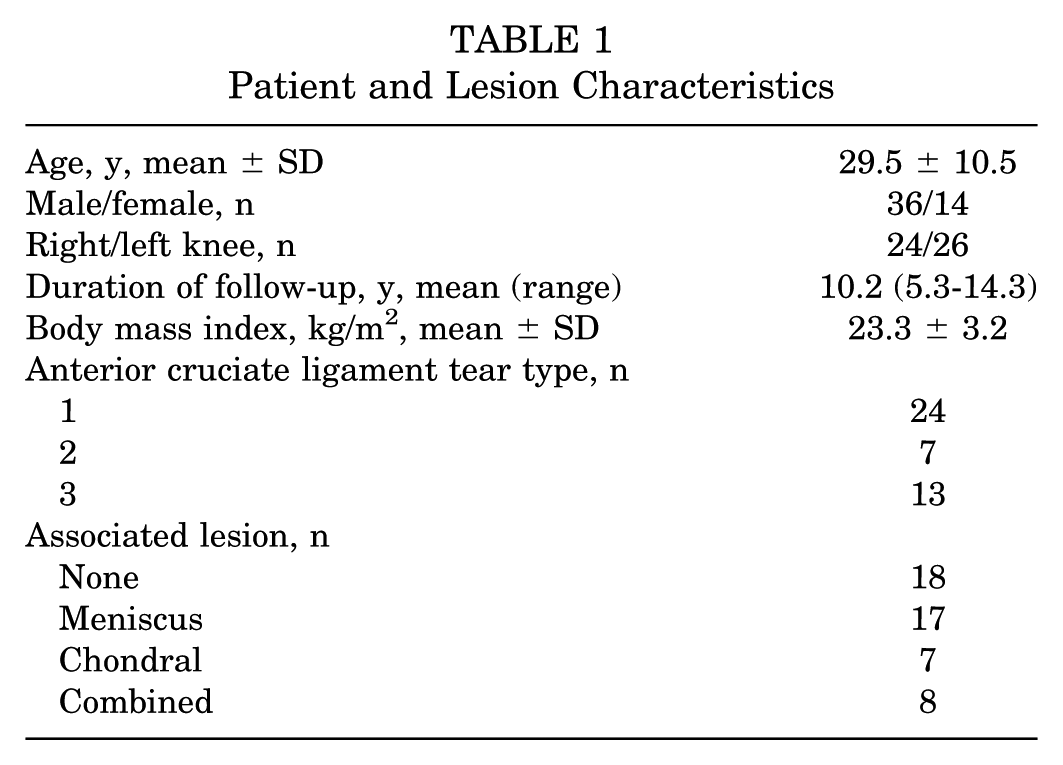
Fifty patients enrolled during the study period met the inclusion and exclusion criteria; their mean age was 29.5 years and mean BMI was 23.3 kg/m2. Six patients were lost to follow-up. Eleven patients experienced a significant reinjury during sporting activity that led to secondary ACL insufficiency, and 1 patient had symptomatic secondary knee instability without experiencing a discrete traumatic event. Mean duration of follow-up was 10.2 years (range, 5.3-14.3 years). The study group consisted of 36 males and 14 females (24 right knees and 26 left knees). Patient characteristics and associated lesions are presented in Table 1.
Patient and Lesion Characteristics
The median preinjury Tegner score of 7 (IQR, 2) was not statistically different from the median Tegner score of 7 (IQR, 1) at final follow-up (P = .128), and the mean final Marx score of 10.8 ± 4.0 was not statistically different from the preinjury mean of 10.8 ± 4.4 (P > .999) (Figure 2). The mean IKDC Subjective score of 90.4 ± 13.3 at final follow-up was decreased compared with the mean preinjury score of 99.7 ± 1.5 (P < .001). The mean Lysholm, KOOS Pain, KOOS Symptoms, KOOS ADL, KOOS Sports, and KOOS QOL scores at final follow-up were 96.2 ± 5.8, 98.6 ± 2.3, 97.5 ± 4.7, 99.7 ± 0.8, 94.3 ± 10.5, and 95.6 ± 8.5, respectively (Figure 3). Final outcome scores were not different between male and female patients and are detailed in Appendix Table A1 (available in the online version of this article). Mean side-to-side difference in anterior tibial translation as measured by Rolimeter testing was 1.4 ± 2.4 mm at short-term follow-up examination and 0.9 ± 0.9 mm at final follow-up examination.
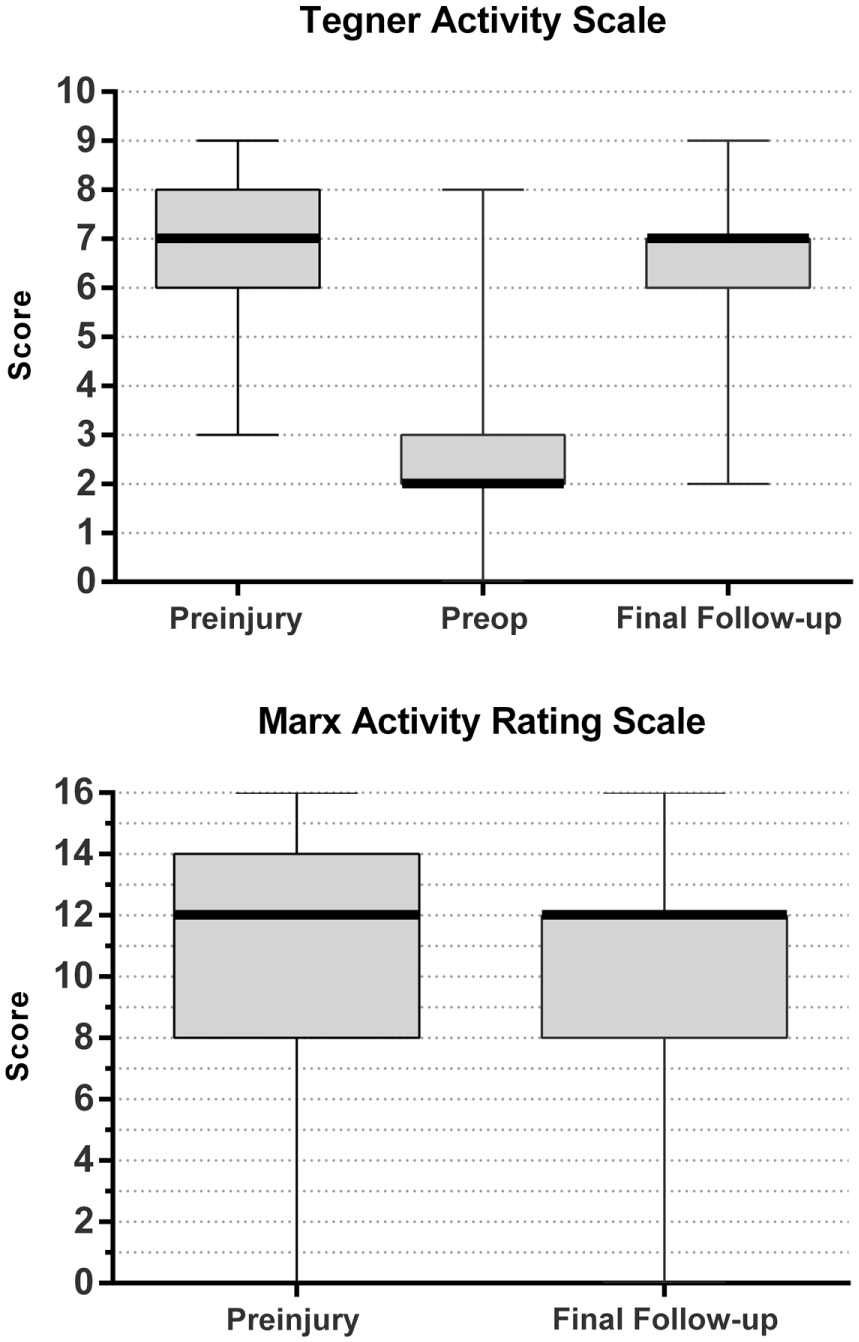
Box plots of Tegner Activity Scale and Marx Activity Rating Scale assessments comparing pretreatment scores and scores at final follow-up after treatment of partial anterior cruciate ligament tear with primary ligament repair and biologic healing augmentation. Plots depict minimum, 25th percentile, median, 75th percentile, and maximum scores. Median Tegner and Marx scores at final follow-up were not statistically different from preinjury scores (P = .128 and P > .999, respectively).
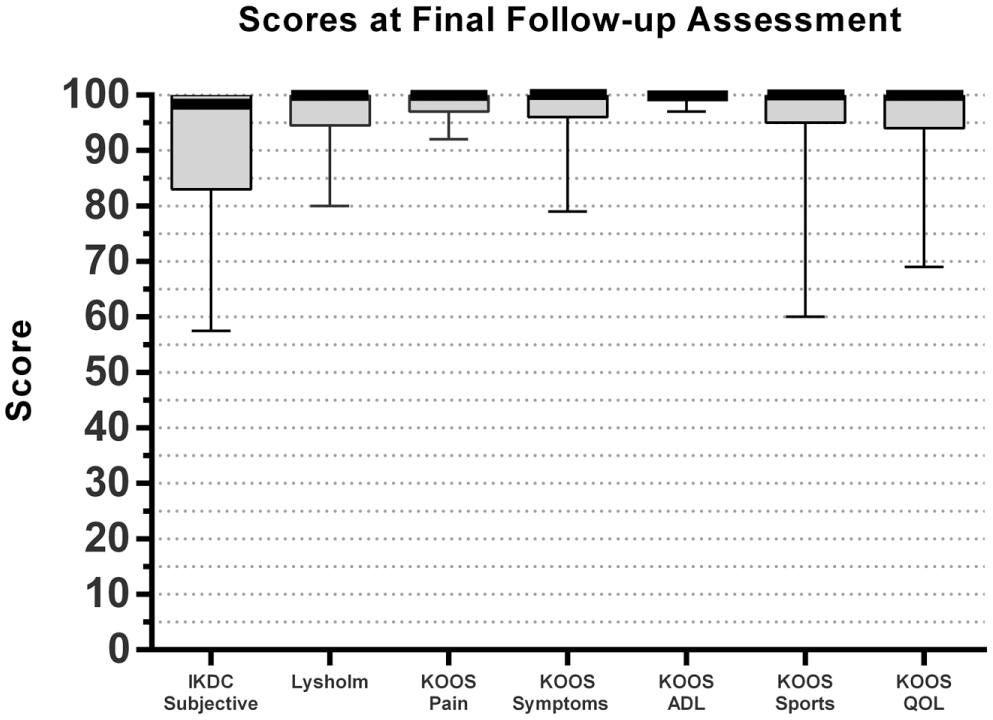
Box plots of International Knee Documentation Committee (IKDC) Subjective scores, Lysholm Knee Questionnaire scores, and Knee injury and Osteoarthritis Outcome Score (KOOS) subsets of Pain, Symptoms, Activities of Daily Living (ADL), Sports, and Quality of Life (QOL) at final follow-up after treatment of partial anterior cruciate ligament tear with primary ligament repair and biologic healing augmentation. Plots depict minimum, 25th percentile, median, 75th percentile, and maximum scores.
No significant differences in clinical outcome scores were found between those patients who did or did not undergo treatment of an associated lesion at the time of primary ACL repair and biologic healing augmentation (Appendix Table A2, part A). No significant differences in outcomes were identified when associated treatments were grouped according to meniscal, chondral, or combined injury (Appendix Table A2, part B), and no differences in final outcome were identified when patients were categorized by the type of ACL tear (Table 2). When patients were grouped according to treatment by biologic augmentation using solely marrow stimulation (n = 40) or biologic augmentation using marrow stimulation in conjunction with activated PRP/BMAC (n = 3), no differences in final outcome scores were identified (Appendix Table A3).
Clinical Outcome Scores at Final Follow-up After Treatment, by Anterior Cruciate Ligament Tear Type a
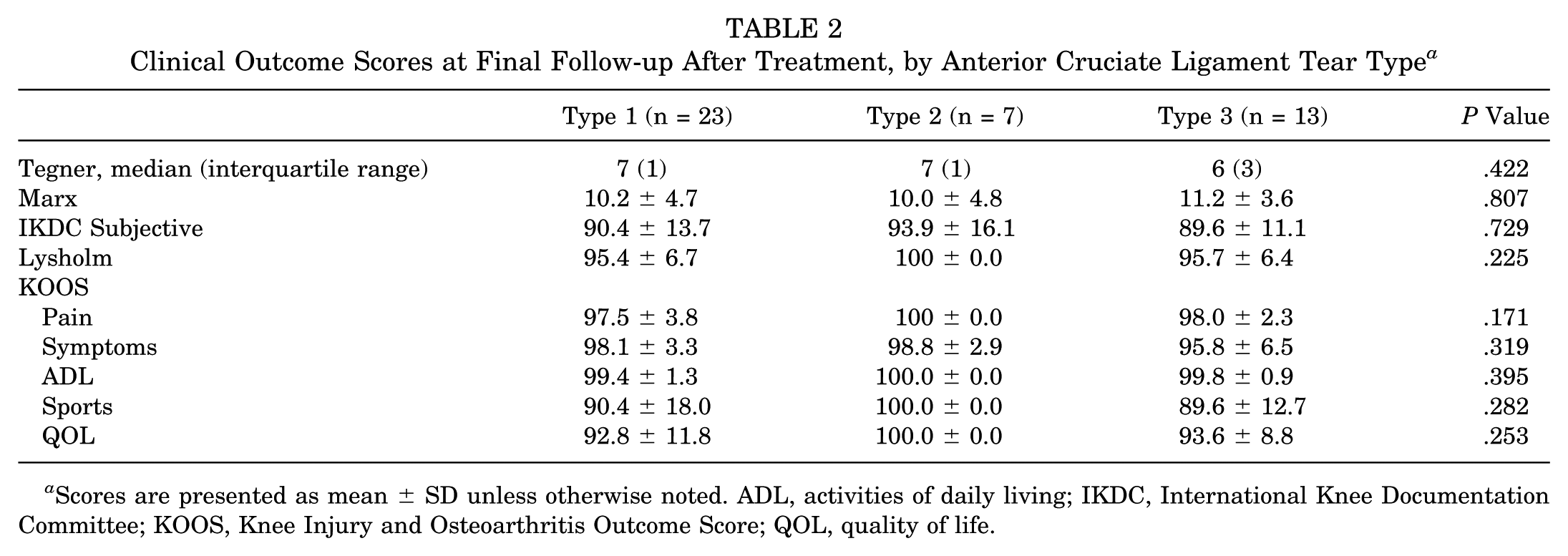
Scores are presented as mean ± SD unless otherwise noted. ADL, activities of daily living; IKDC, International Knee Documentation Committee; KOOS, Knee Injury and Osteoarthritis Outcome Score; QOL, quality of life.
Correlation analysis using Spearman rank correlation coefficient did not identify any significant associations between scores at final follow-up and age at time of surgery, BMI, type of ACL tear, or side-to-side difference in laxity with regard to IKDC Subjective, Lysholm, or KOOS scores (Appendix Table A4). A negative correlation was found for age and Tegner scores preinjury and at final follow-up (rs = −0.333, P = .022, and rs = −0.376, P = .013, respectively). A negative correlation was found for final Marx score and side-to-side difference in knee laxity (rs = −0.350, P = .049).
Survival rate of primary ACL repair with biologic augmentation using Kaplan-Meier analysis determined the survival rate to be 80.2% at 5 years, 72.7% at 10 years, and 72.7% at 14 years (Figure 4).
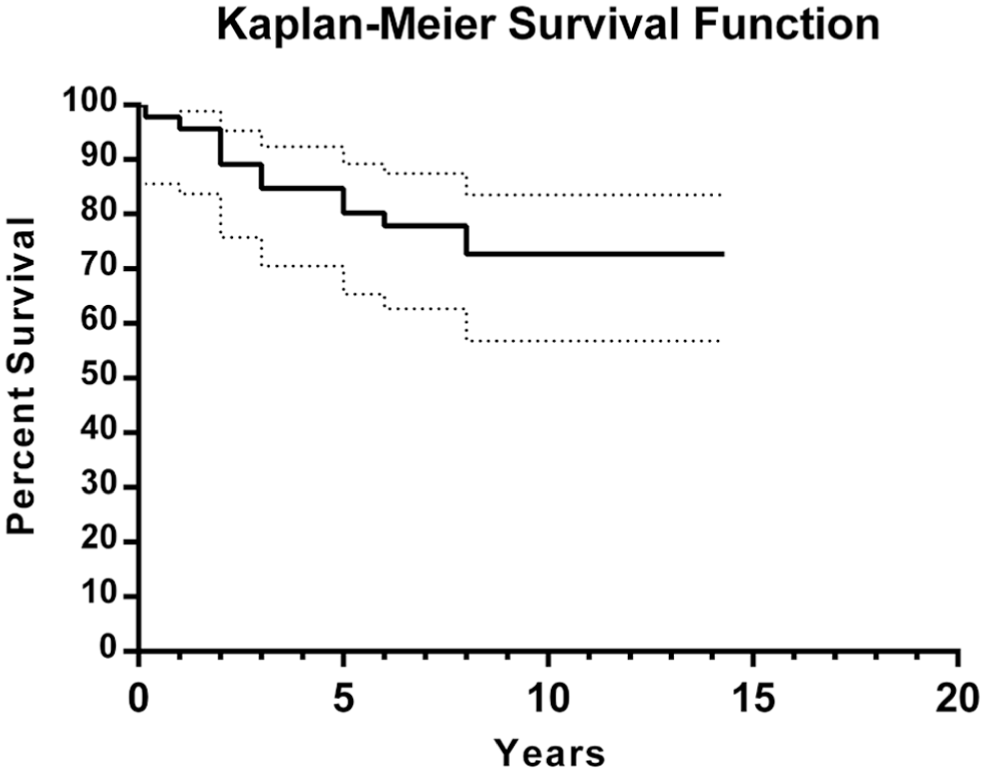
Kaplan-Meier survival plot with 95% CIs after treatment of anterior cruciate ligament tear with primary repair and biologic healing augmentation.
Twelve patients had secondary ACL insufficiency; in 11 of these patients a specific traumatic event was associated with secondary insufficiency, and 1 patient had symptomatic laxity without a discrete inciting event (Table 3). The mean age was 23.6 years at the time of surgery in the group that experienced secondary ACL insufficiency, which was significantly lower than the mean age of 31.7 years in the group that did not (P = .025). The ACL tear type was determined to be type 1 in 9 of the 12 patients who developed secondary ACL insufficiency, type 2 in 1 patient, and type 3 in 2 patients. A significantly higher percentage (73%) of patients in the secondary ACL insufficiency group were classified as having a type 1 tear compared with type 2 or 3 (P = .020). No difference was found in distribution of ACL tear type between those patients who did or did not develop secondary ACL insufficiency (P = .504) (Table 4). Side-to-side difference in mean ligamentous laxity as measured by Rolimeter testing at short-term examination (mean, 2 years) was significantly increased in those who went on to experience secondary ACL insufficiency compared with those who did not (3.4 mm vs 0.9 mm, P = .010). Traumatic reinjury events occurred during either high-impact or contact sporting activity. One case of traumatic reinjury occurred 2 months after the primary ACL repair procedure, without short- to medium-term follow-up scores available. The mean duration of short- to medium-term follow-up for the remaining patients with secondary ACL insufficiency before reconstructive ACL surgery was 2 years (range, 1-4 years). The median Tegner score at short- to medium-term follow-up before secondary ACL insufficiency was 7 (IQR, 2), which was not significantly different from the median Tegner score of 7 (IQR, 2) before patients underwent the initial procedure of primary ligament repair with biologic healing augmentation (P = .210). Similarly, no significant difference was found in the mean Marx score of 10.0 ± 4.5 at short- to medium-term assessment, before secondary insufficiency, compared with the mean score of 10.4 ± 4.3 before patients underwent the initial primary repair procedure (P = .838). Regarding IKDC Subjective scores before secondary ACL insufficiency, the mean score of 75.8 ± 15.9 was decreased at short- to medium-term follow-up compared with the mean preinjury score of 99.7 ± 0.6 (P = .002). The mean Lysholm score before secondary ACL insufficiency was 91.8 ± 7.1.
Characteristics of Patients With Recurrent ACL Insufficiency After Primary Ligament Repair With Biologic Healing Augmentation a
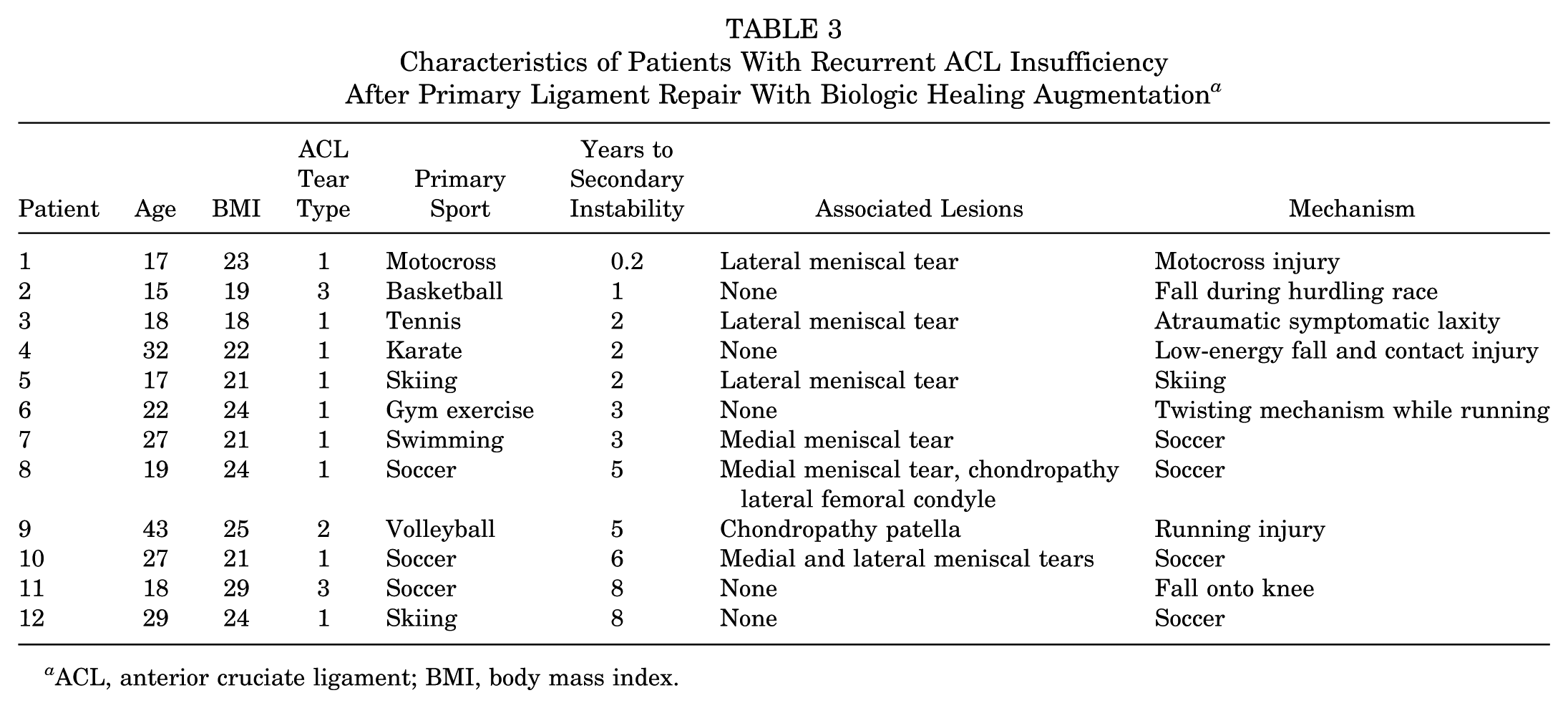
ACL, anterior cruciate ligament; BMI, body mass index.
Comparison of Anterior Cruciate Ligament (ACL) Tear Types
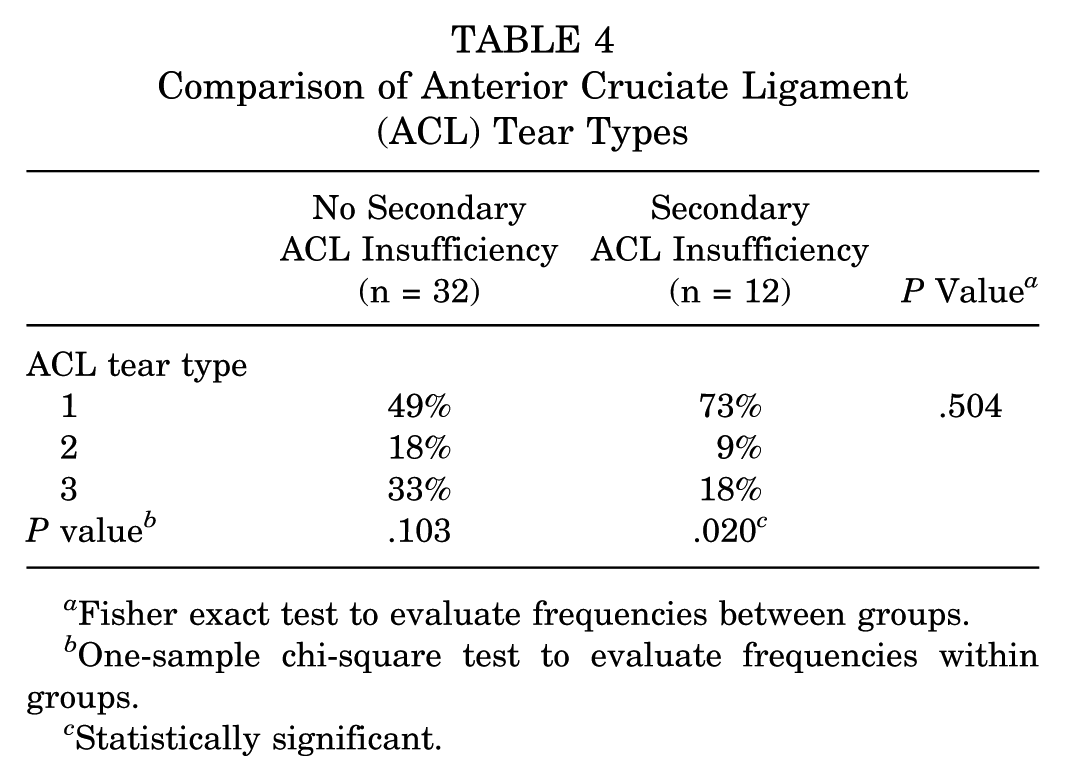
Fisher exact test to evaluate frequencies between groups.
One-sample chi-square test to evaluate frequencies within groups.
Statistically significant.
Discussion
Analysis of patients with partial ACL tear treated with primary repair and biologic healing augmentation in this cohort has demonstrated that restoration of knee stability and return to preinjury activity levels were achieved in the majority of patients at long-term follow-up. Eighty-eight percent of the patients were available for assessment at long-term follow-up, and functional knee stability was restored and maintained in 73% of cases. Comparable outcomes and similar rates of return to preinjury status were identified in those who were treated for associated conditions at the time of ACL repair. Patient age, BMI, ACL tear type, and ligamentous laxity did not correlate with clinical outcomes, although increased mean ligamentous laxity was found at short-term examination in those who went on to develop symptomatic secondary ACL insufficiency compared with those who did not. For those patients who were treated with ligament reconstruction due to secondary ACL insufficiency over the study period, successful clinical outcomes with high rates of return to sport were achieved at short- to medium-term follow-up, before the recurrent instability.
For those patients with an intact ACL repair at long-term follow-up assessment, final outcome according to IKDC Subjective, Lysholm, and KOOS scoring instruments was good to excellent, and Tegner and Marx scales demonstrated final scores that were comparable with preinjury functional status. Associated conditions treated concurrently with the ACL repair and biologic healing augmentation consisted of meniscal or chondral injury in 63% of these patients. Final outcomes were comparable between those who did or did not undergo treatment of an associated condition; when patients were categorized according to type of associated lesion, successful outcomes were comparable between those patients with meniscal, chondral, or combined lesions. Patient age ranged from 12 to 54 years and BMI ranged from 17.7 to 35.5 kg/m2 at the time of surgery. Rank correlation analysis using Spearman rho did not identify any significant associations between final outcome and patient age, BMI, ACL tear type, or objective measurement of laxity.
Several factors contribute to the reduced healing capability of the ACL after disruption of the ligament fibers. Although cellular constituents within injured ACL tissue have been demonstrated to contain mesenchymal stem cell (MSC) type cells that may assist with repair processes, 44 outgrowth of such cells, as well as their migratory and proliferative capacity, has been demonstrated to be inferior to other ligament tissue, such as the MCL.2,31,50 Furthermore, in the case of an intra-articular ligament such as the ACL, synovial fluid and the presence of plasmin within the joint space are likely important contributing factors to the suboptimal healing of ACL tissue after the separation of injured ligament fibers, because fibrin clot formation is impaired.3,35 The primary goal of the suture repair of torn and separated ACL fibers is to reapproximate this tissue and minimize gapping to allow for repair and regeneration to proceed unhindered. The postoperative rehabilitation protocol is designed to protect this initial repair, as it is not expected that the mechanical strength of sutured ligament is capable of providing significant long-term stability.
Tear pattern is an important consideration, as partial tears to the ACL have been associated with higher rates of return to sport than complete tears in those who forgo reconstruction. 7 An important point for those considering treatment of partial ACL tears is that certain patterns of partial injury, particularly those involving greater than 50% of the ligament, are likely to progress to a complete tear and worsening knee instability over time. 33 The natural history of conservatively treated tears is an important consideration. For lower grade injury, nonoperative treatment is associated with symptomatic instability after rehabilitation therapy. 15 Clancy et al 10 evaluated patients who underwent nonoperative treatment and had a positive Lachman test with either an absent or a mildly positive pivot shift; the investigators demonstrated that half of the patients had only fair clinical outcomes or experienced failure. Much of the clinical research on the outcomes of nonoperative management, however, was completed in the 1980s and was not of sufficient quality to reliably determine the most appropriate treatment algorithms. 27 Treatment of symptomatic partial ACL tears has been advocated to reduce the likelihood of secondary instability events that are associated with meniscal or chondral injury. 12 Animal research has demonstrated the potential for rapid degeneration of residual ligament fibers after transection of the ACL, and this is an important time-related consideration if primary repair is to be attempted. 1
Systematic reviews have reported various rates of return to previous levels of activity after ACL reconstruction, with rates ranging from 65% to 85%,4,34 and literature specifically analyzing return to competitive or elite sports has described rates ranging from 55% to 83%.4,26 A review of long-term outcomes of ACL reconstruction after 10 years reported a pooled graft rupture rate of 6%, with a cumulative failure rate, including clinical failures, of 12%. 11 Other literature that has specifically examined outcomes at medium- to long-term follow-up has reported similar graft failure rates, ranging from 4% to 12%.21,26,36,49 In the current cohort of patients who underwent primary ACL repair with biologic healing augmentation, 76% of patients returned to preinjury activity levels, which is comparable with rates expected with standard ACL reconstruction. Regarding secondary ACL insufficiency, however, 27% of patients underwent a reconstructive procedure to treat recurrent instability over the duration of follow-up, which is a higher rate than is typically reported after standard ACL reconstruction and is clinically concerning if there is an increased rate of instability episodes that is sufficient to increase the risk of meniscal or chondral injury. Of the patients with recurrent ACL insufficiency, 11 of 12 cases were associated with a specific traumatic event, and there was a single case of symptomatic knee instability that was treated with standard ACL reconstruction without a specific injurious event identified. Importantly, for those patients who did undergo standard reconstruction to treat a retear that occurred after primary repair, restoration of functional status and successful short- and medium-term outcomes were reported before the reinjury event. However, because MRI was not performed for every patient in this cohort to evaluate ligament repair tissue, some of these patients may have been functionally coping despite unrecognized ligamentous insufficiency.
Studies of long-term outcomes for patients who undergo ACL reconstruction have demonstrated that risk of subsequent meniscal injury and symptomatic joint laxity may be reduced, and activity levels may be superior, compared with those not undergoing reconstruction. Importantly, however, many outcome scores are comparable and there is no difference in radiographic findings demonstrating osteoarthritic changes.9,34 Progressive degenerative changes after ACL injury have been identified in series of prospective patient follow-up, irrespective of whether the injured ligament is reconstructed or treated nonoperatively, and controversy remains as to the role of reconstruction as a protective treatment to alter this natural history.29,46 Depending on patient expectations and activity level, nonoperative treatment can play a role for some patients with lower demands.16,40 Nonoperative treatment in patients with higher demands tends to be associated with symptomatic knee instability that affects return to sport and functionality with regard to participating in physical activities comfortably. 8 Additional considerations related to surgical reconstruction of the ACL are sensory deficits resulting from injury to the infrapatellar nerve and postoperative pain associated with the donor site. 24 An important goal in treatment of ACL injury with primary repair and biologic healing augmentation is to preserve the structure and function of the native ligament, which intuitively has greater capacity to restore natural joint kinematics, potentially reducing the incidence of secondary injuries to anatomic structures such as menisci or articular cartilage. Furthermore, complications typically associated with standard reconstruction techniques are minimized.
Procedures to reconstruct the ACL are associated with a number of complications that are avoided with the treatment method of primary repair and biologic healing augmentation. Autograft harvest can entail morbidities associated with sensory nerve injury, strength deficit, or increased postoperative discomfort. Reconstruction procedures using bone–patellar tendon–bone autograft have been associated with increased incidence of anterior knee pain, which has been associated with the development of knee extension deficit and weakness of the extensor mechanism.20,32 Furthermore, deficits of knee extension and strength after ACL reconstruction have been shown to negatively affect return to sport. 19 Arthrofibrosis is an important potential complication after reconstruction that has been demonstrated to result in reduced range of motion, which in severe cases may lead to extensive functional limitation. 13 Techniques of ACL reconstruction necessitate the creation of bone tunnels that may result in a variable degree of tunnel widening or even cystic dilatation. The difficulty in achieving exact anatomic positioning of the re-created ligament footprint contributes to pathologic changes in tunnel morphology, particularly in the early postoperative period. 48 Tunnel location and knee position during graft tensioning are also factors that have been shown to increase risk of postoperative extension deficit. 6 Moreover, hardware complications are associated with fixation devices used for ACL reconstruction. Metal interference screws create artifact on computed tomography imaging and MRI, and this may impair assessment of knee injury postoperatively. Interference screws composed of nonmetallic materials may fragment or migrate, potentially leading to loose intra-articular foreign bodies. 38
As a component of the treatment of primary ACL repair, microfracture was performed within the intercondylar notch about the anatomic ACL footprint to release marrow elements, and in a few cases biologic gel consisting of activated PRP/BMAC was added to the repair site. Recent investigations have identified pericytes as the primary cellular component of MSC preparations. Reduced in vitro manipulation of these cells improves the in vivo cell viability, longevity, trophic factor secretion, and ability to recruit resident cells. 28 Local administration of these multipotent cells about the ACL repair site is a method to optimize the availability and biologic reparative activities of these cells. Animal models have demonstrated positive effects of growth factors on ligament healing processes, including promoting neovascularization and the synthesis of collagenous and noncollagenous proteins that contribute to repair and remodeling of injured ligamentous tissue.5,22,25,30 Although biologic augmentation of injured ACL in humans through use of growth factors and cellular treatments has been shown to be associated with high rates of return to sport,12,37 much debate surrounds the benefits of such procedures, and further high-quality randomized studies are necessary to clearly elucidate the specific benefits and indications for such treatments, given the wide spectrum of injury patterns that may lead to functional deficit. 14 Regarding biologic healing augmentation in the current study, no differences in final outcome were demonstrated in those patients who underwent marrow stimulation alone compared with those who underwent marrow stimulation in addition to application of activated PRP/BMAC, although only a few patients were treated with the latter technique.
Steadman et al 41 published outcomes of a series of patients with ACL tear treated with a healing response technique. Over the course of 69 months, 23% of patients experienced reinjury that required ACL reconstruction, and the investigators reported high rates of patient satisfaction and return to previous levels of physical activity. This initial work in skeletally immature patients was followed by a study of healing response treatment in older patients with proximal ACL tears. In that study, 9% of patients underwent ACL reconstruction after a mean follow-up duration of 7.6 years to treat recurrent instability. 42 This healing response technique was later examined by Wasmaier et al, 47 who reported an unsatisfactory revision rate of 36% to treat symptomatic instability, which was comparable with the rate found for patients who were treated conservatively, after a mean follow-up duration of 4 years. These series have notable differences in regard to reinjury rate, which may be related to variables such as the pattern of ligament injury or patient activity levels.
Regarding the current study, clinical outcome analysis of part of this patient cohort at shorter term follow-up demonstrated an 81% rate of return to preinjury activity levels. 18 At this earlier follow-up assessment, no ACL reconstructions were performed to treat reinjury. After a mean follow-up of 10 years, ACL reconstruction to treat secondary ACL insufficiency was performed in 27% of patients. Kaplan-Meier survival analysis indicated a survival rate of 80.2% after 5 years and a rate of 72.7% at 10 years that remained unchanged at 14 years. The current long-term analysis has not demonstrated a statistically significant difference in outcome scores for those patients treated for associated lesions, and this is consistent with the findings at shorter term follow-up after a mean of 25 months.
Comparing the long-term outcomes of the patients in the current study to the smaller initial cohort examined after a short-term mean follow-up of 25.3 months 18 shows that good to excellent functional status was maintained over time in the majority of those treated. The proportions of ACL tear types were similar between the studies, with type 1 tear the most common, followed by type 3. In the current study, a number of cases of secondary ACL insufficiency occurred after the earlier follow-up period at short- to medium-term. It is particularly notable that while the correlations of outcome scores with ACL tear type and objective laxity findings were not significant, there was an increased mean side-to-side difference in laxity of 3.4 mm at short-term examination in those who went on to develop secondary ACL insufficiency compared with 0.9 mm in those who did not. Regarding the type of ACL tear treated in those who did or did not experience secondary ligamentous insufficiency, no difference was found in the distribution of tear types between these two groups. Another important consideration is that the mean age at the time of surgery was significantly lower in the group who went on to experience secondary ACL insufficiency over the duration of long-term follow-up, although age is a variable which typically affects activity levels that change over time.
Several limitations of this study should be considered. The study did not include a control group to compare outcomes of those who underwent primary ACL and biologic healing augmentation with those who underwent nonoperative management. Although this would have provided valuable comparative data, it was considered to be of ethical concern to offer nonoperative management to patients experiencing symptomatic knee instability secondary to ACL injury, given that available literature describes a high failure rate for nonoperative management. Regarding the specific location of suture repair along the length of the injured ACL, no comparative analysis was conducted to examine whether success of the repair varied depending on location. Although no differences were identified between patient outcomes based on treatment of associated lesions and ACL tear type, the smaller sample sizes in these subcategories may have affected the analysis. Regarding the constituency of the biologic preparations, the content of the PRP/BMAC isolates may have had unexpected variability, as samples were not subject to laboratory analysis. Analysis of postoperative imaging was not included in the study protocol; therefore, the prevalence of posttraumatic osteoarthritis is unknown.
Treatment of symptomatic knee instability secondary to ACL injury by method of primary repair or healing augmentation using marrow elements has had variable outcomes according to the few studies that have examined these treatments. The long-term follow-up of patients in our study who were treated with primary ACL repair in conjunction with biologic healing augmentation has demonstrated that high rates of return to physical activities and good to excellent long-term outcomes are achievable for a majority of those treated for partial ACL injury. Secondary ACL insufficiency in this cohort was primarily attributed to a significant reinjury event during high-impact activity or contact sports and tended to occur in younger patients, although it was not feasible to examine the specific reinjury events in detail. Although the incidence of recurrent ACL insufficiency in our cohort was greater than typically reported in the literature for primary ACL reconstruction, several notable complications of reconstruction are avoided with the technique of primary ACL repair and biologic healing augmentation.
Conclusion
Primary ACL repair combined with biologic healing augmentation to treat select cases of knee instability secondary to incomplete ACL rupture has demonstrated good to excellent long-term outcomes in this cohort for those patients who did not experience secondary ACL insufficiency, with high rates of restoration of knee stability and return to preinjury athletic activities. The rate of secondary treatment for recurrent ACL insufficiency over the course of long-term follow-up was greater than would be expected for primary ACL reconstruction. Greater side-to-side differences in objective findings of ligamentous laxity were identified at shorter term follow-up in those who later went on to experience symptomatic secondary ACL insufficiency, compared with those who maintained stability long term.
Supplemental Material
DS_10.1177_0363546518805740 – Supplemental material for Long-term Outcomes of Primary Repair of the Anterior Cruciate Ligament Combined With Biologic Healing Augmentation to Treat Incomplete Tears
Supplemental material, DS_10.1177_0363546518805740 for Long-term Outcomes of Primary Repair of the Anterior Cruciate Ligament Combined With Biologic Healing Augmentation to Treat Incomplete Tears by Alberto Gobbi and Graeme P. Whyte in The American Journal of Sports Medicine
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.