
Abstract
Background:
Ulnar collateral ligament (UCL) reconstruction is commonly performed among overhead throwing athletes. Previous studies demonstrated relatively high rates of return to sport after primary reconstruction. Outcomes after revision UCL reconstruction have not been widely studied.
Purpose:
To report the rate of return to sport after revision UCL reconstruction among elite-level baseball players.
Study Design:
Systematic review.
Methods:
A systematic review of the literature following the PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) guidelines was performed for high-level baseball players undergoing revision UCL reconstruction. Study bias was assessed with the Methodological Index for Non-Randomized Studies scoring system. The primary outcome measure was whether the study participants were able to return to sport after revision UCL reconstruction. Secondary outcome measures included career length after revision and pitching performance statistics. Data were summarized with ranges, tables, and weighted averages. A subjective analysis was performed.
Results:
A total of 5 studies met inclusion criteria. The rate of return to sport at preinjury level was 62.8%. Among Major League Baseball pitchers, the rate of return to sport at the preinjury level was 68.8%. The rate of return to sport at the same level or lower (Major League Baseball, minor league, collegiate) was 78.1%. Time to return to sport ranged from 1.3 to 1.7 years. Mean earned run average after revision ranged from 4.87 to 5.04. Mean number of innings pitched per season after revision ranged from 36.95 to 50.5.
Conclusion:
This systematic review demonstrated a limited rate of return to preinjury level of sport among elite-level baseball players who underwent revision UCL reconstruction. Pitching durability and career longevity were inferior to results that were reported for players who underwent primary UCL reconstruction alone. This study suggests that outcomes after revision UCL reconstruction are not reliable and elite-level players should be counseled accordingly.
Medial ulnar collateral ligament (UCL) injuries are common among overhead throwing athletes. These injuries can cause pain and instability during the throwing motion, altering an athlete’s performance. High-demand baseball pitchers are particularly prone to UCL injury and make up a large portion of patients undergoing UCL reconstruction. 15 In a survey of >5000 professional baseball players, 10% were found to have undergone at least 1 UCL reconstruction. Of the Major League Baseball (MLB) pitchers included in the survey, 25% reported that they had undergone the procedure. 4
Multiple large studies reported fairly low revision rates after UCL reconstruction. Cain et al, 2 in a retrospective study including 942 patients, reported a 1% revision rate after 2 years of follow-up. After 10 years of follow-up, Osbahr et al 13 reported a 2% revision rate among 313 patients. However, studies restricted to professional cohorts reported higher revision rates.3,8,11,17 In a retrospective study involving 271 MLB pitchers, Wilson et al 17 reported a revision rate of 15%.
In a population whose livelihood depends on the ability to maintain a high performance level for a sport, the ability to return to that sport after injury is exceedingly important. Previous analyses demonstrated relatively high rates of return to sport after primary UCL reconstruction,6,15,16 but to our knowledge, there is no existing review evaluating the literature on return-to-sport rates after revision UCL reconstruction. The purpose of this systematic review is to synthesize the existing evidence regarding return-to-sport rates among elite-level baseball players after revision UCL reconstruction. Our hypothesis is that elite-level baseball players will have a lower rate of return to sport after revision UCL reconstruction than after primary reconstruction.
Methods
Study Design and Literature Search
A systematic review of the literature regarding revision medial UCL reconstruction was conducted following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. An electronic search of the literature was performed with the PubMed (MEDLINE) and Cochrane databases. The following search term was used: “(medial ulnar collateral ligament OR ulnar collateral ligament OR UCL) AND (reconstruction OR Tommy John surgery) AND (return to sport OR return to play OR sports re-entry OR return to activity).” Additionally, the reference section of each full-text article obtained was reviewed for additional inclusions to the study not identified in the electronic search.
Studies were included if they were reported in English and evaluated return to sport after revision medial UCL reconstruction. Studies were excluded if they were literature reviews, expert opinions, case reports, or studies that did not report on rates of return to sport. In the initial search, 551 unique abstracts were identified, of which 72 relevant full-text articles were assessed for eligibility. Of the 72 full-text articles, 67 were excluded because return to sport was not reported, return-to-sport data were reported only for primary UCL reconstruction, or the article was a review. Therefore, 5 studies were included in the final analysis (Figure 1). The Methodological Index for Non-Randomized Studies (MINORS) scoring system was used to assess study bias. Each study was assigned a score based on a system ranging from 0% (high bias) to 100% (low bias). The articles selected for review were evaluated by 2 authors (G.G., B.M.G.). Articles in question of inclusion or exclusion were discussed between authors until consensus was achieved.
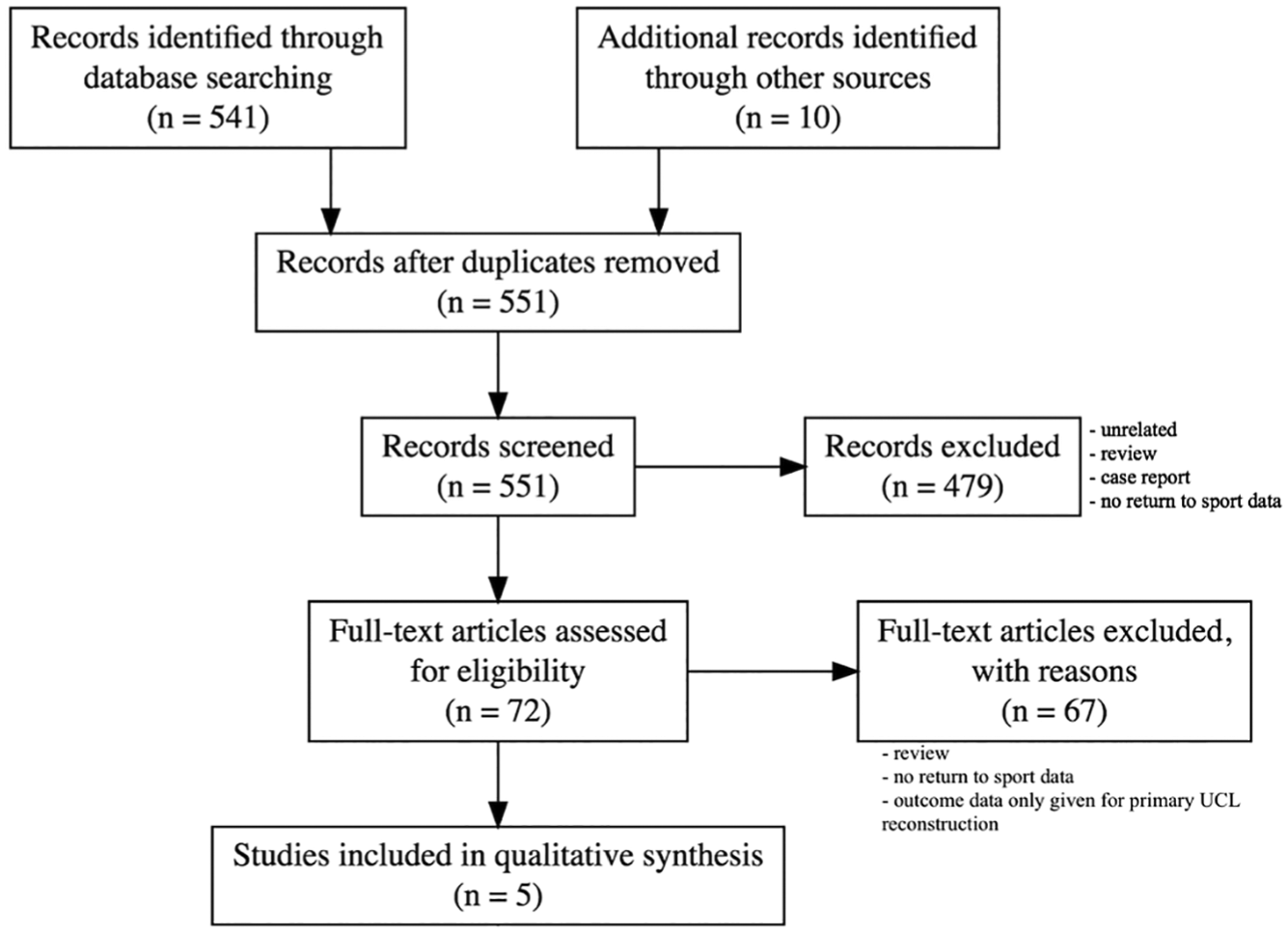
PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) flowchart. UCL, ulnar collateral ligament.
Data Extraction and Analysis
The following data were extracted from each article: study design, level of evidence, patient demographics (number, age, sex), duration of clinical follow-up, rate of return to sport, pitching performance statistics, reoperations, and complications. The primary outcome measure was whether the study participant was able to return to sport after revision UCL reconstruction. Secondary outcome measures included career length after revision and pitching performance statistics.
Given the significant heterogeneity, methodological variability, low levels of evidence, and retrospective nature of the included studies, the pooling of results for meta-analysis was avoided. Instead, a subjective analysis was performed, and outcomes that were reported in at least 3 studies were summarized with tables that included ranges, SDs, and weighted means, when possible. 1
Results
Five studies with a total of 199 patients were analyzed in this systematic review. The studies had evidence levels of 3 (n = 2) and 4 (n = 3). All studies had a MINORS score ≥75%. All patients were male baseball players, the majority of which played at the professional level (98%). All patients were pitchers, with the exception of 1 catcher. The mean age at the time of revision ranged from 20.1 to 29.8 years. The mean time from primary UCL reconstruction to revision ranged from 3 to 5 years (Table 1).
Summary of Included Studies and Patient Demographics a
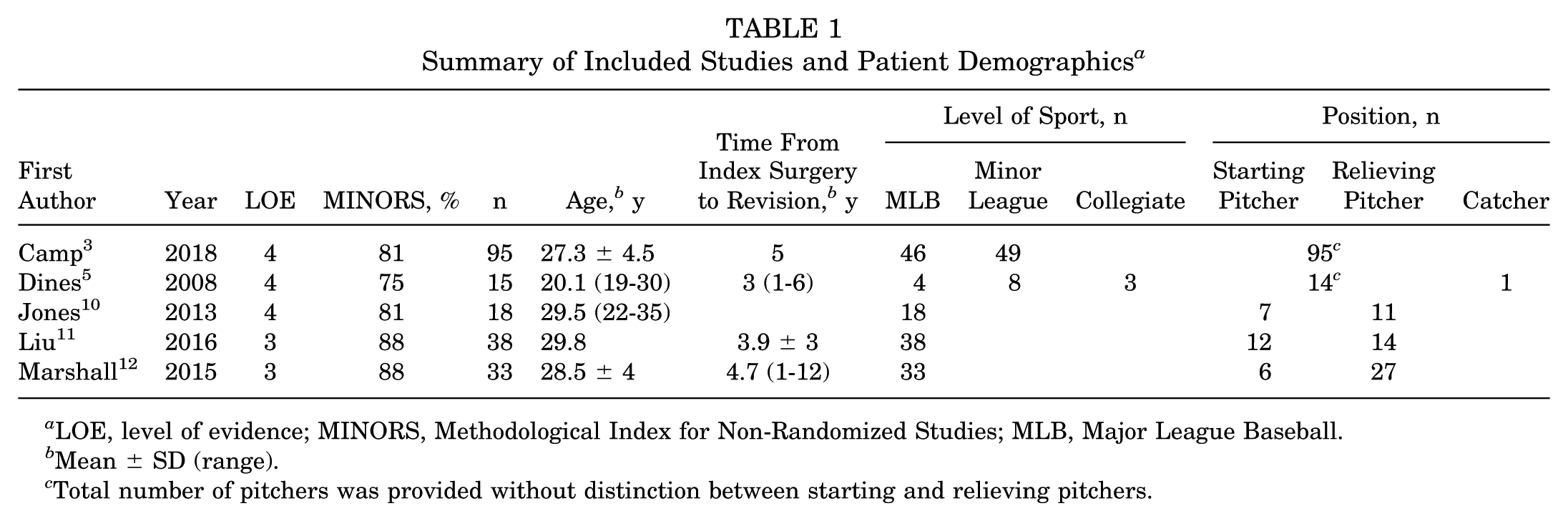
LOE, level of evidence; MINORS, Methodological Index for Non-Randomized Studies; MLB, Major League Baseball.
Mean ± SD (range).
Total number of pitchers was provided without distinction between starting and relieving pitchers.
The rate of return to sport at the preinjury level was reported in all 5 studies (mean, 62.8%). Patients were considered to have returned to their previous levels of play if they participated in at least 1 game at that level. Four studies with MLB cohorts reported rates of return to at least 1 game at the MLB level (mean, 68.8%). The rate of return to sport at any level (MLB, minor league, or collegiate) was reported in 4 studies (mean, 78.1%). Mean time to return to sport was reported in 3 studies and ranged from 1.3 to 1.7 years. The mean career length after revision was reported in 3 studies and ranged from 2.6 to 3.2 years (Table 2).
Return to Sport Data a

MLB, Major League Baseball; RTS, return to sport.
Mean ± SD (range).
Pitching statistics were reported in 3 studies: all 3 reported mean number of innings pitched per season and ERA (earned run average); all 3 reported mean values after revision UCL reconstruction; and 2 reported presurgical means. The range of mean innings pitched per season after revision was 36.95 to 50.5; prerevision means were 67.18 and 83.97. The range of mean ERA was 4.87 to 5.04; prerevision means were 4.14 and 4.74 (Table 3).
Pitching Statistics a
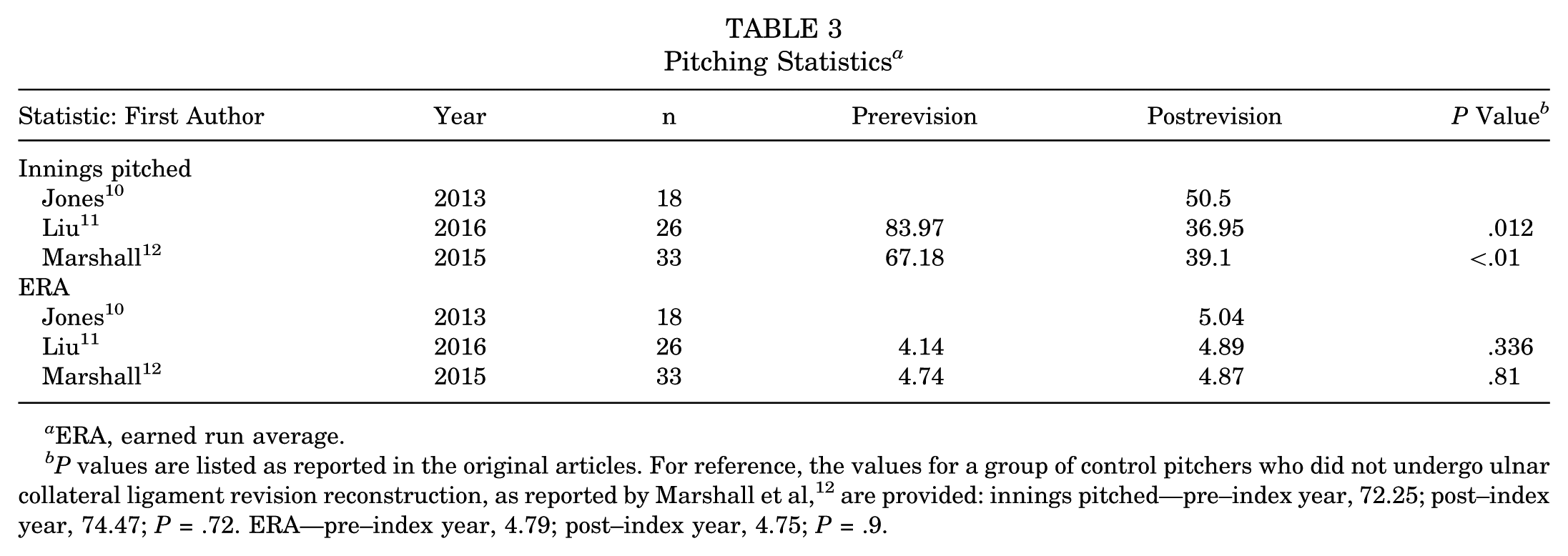
ERA, earned run average.
P values are listed as reported in the original articles. For reference, the values for a group of control pitchers who did not undergo ulnar collateral ligament revision reconstruction, as reported by Marshall et al, 12 are provided: innings pitched—pre–index year, 72.25; post–index year, 74.47; P = .72. ERA—pre–index year, 4.79; post–index year, 4.75; P = .9.
Discussion
Recent analyses demonstrated high rates of return to sport at the preinjury level after primary UCL reconstruction. In a meta-analysis of 14 studies, Somerson et al 15 found an 83.2% rate of return to sport at the preinjury level. Similarly, in a meta-analysis of 22 studies, Peters et al 14 found a 79% rate of return to prior level of sport. In contrast, our analysis found a mean rate of 62.8% return to sport at the preinjury level after revision UCL reconstruction. When restricted to MLB players, the rate was slightly higher (68.8%). The mean rate of return to sport at the same or lower level of play was 78.1%. The mean time to return to sport ranged from 1.3 to 1.7 years. The mean career length after revision ranged from 2.6 to 3.2 years.
In addition to lower rates of return to sport, studies evaluating players who had undergone revision reconstruction reported declines in the performance levels of those able to return. Liu et al, 11 in a retrospective review of 31 MLB pitchers, reported significant declines in innings pitched and total pitches per season in the 3 years after revision as compared with the 3 years prior. Similarly, in a review of 33 MLB pitchers, Marshall et al 12 reported a significant decrease in number of innings pitched after revision, in contrast to the significantly improved statistics seen among matched control pitchers during the same time frame (decreases in walks and increases in strikeouts). Jones et al, 10 in a study including 18 MLB pitchers, found that starting pitchers were able to resume only 35% of their preinjury workload. Of the 3 studies included in our review that reported pitching statistics, 2 demonstrated no significant improvements in any performance measure.10,11 These findings lie in stark contrast to the favorable outcomes reported by Erickson et al 8 in their retrospective review of 179 MLB pitchers who had undergone primary UCL reconstruction. The players included in this study demonstrated significant improvement in pitching performance after surgery. Specifically, the authors reported a significant decrease in number of losses, number of walks, number of hits allowed, and ERA after surgery. Compared with matched controls during the same time frame, pitchers who had undergone primary UCL reconstruction had significantly fewer losses per season, fewer walks, and a lower ERA.
Revision studies also demonstrated decreased professional longevity among pitchers after surgery. Liu et al 11 reported that only 29% of pitchers continued to play at the MLB level for >2 seasons. Marshall et al 12 reported that MLB pitchers who had undergone revision UCL reconstruction ended their careers almost 1 year earlier than their matched controls. In contrast, Erickson et al 8 reported a longer mean career length after primary UCL reconstruction (3.9 seasons) than the mean career length after the index year in matched controls (3.5 seasons).
Specific risk factors associated with these poor outcomes have not been identified. Regarding primary UCL reconstruction, Gibson et al 9 found that pitching in a starting role in MLB was associated with an increased incidence of UCL insufficiency requiring reconstruction. Jones et al 10 suggested that overuse of the throwing arm may similarly contribute to less favorable outcomes among players who have undergone revision. Their study demonstrated a decreased postsurgical pitching workload among starting and relief pitchers, as measured by number of innings pitched per season. This decreased workload was demonstrated to a higher degree among the starting pitchers, who were able to resume only 35% of their previous workload, in comparison with the relief pitchers, who were able to resume 50% of their prior workload. The authors reasoned that starting pitchers average more innings per season than relievers and thus place a greater demand on the elbow. Additionally, the authors found that the 2 starting pitchers who switched to relief roles after surgery demonstrated more favorable statistics, pitching 63% and 125% of their prior workloads. Liu et al 11 reported that only 25% of starting pitchers were able to participate in at least 10 games at the MLB level after revision, as opposed to 57% of relief pitchers. Only 1 starting pitcher was able to continue in the starting position for >2 seasons. However, in a study comparing the number of innings pitched by MLB pitchers who had undergone primary UCL reconstruction alone with those who had required revision, Erickson et al 7 found that the number of pitches thrown in the first full season after primary surgery was not associated with increased risk of undergoing revision. But as our review demonstrated a mean range of 3 and 5 years between index and revision reconstruction, a study spanning a longer period might be necessary to fully evaluate the association between number of pitches and revision UCL reconstruction.3,5,11,12
This study had several limitations. Our review was limited by low levels of evidence, low patient counts (reflecting the relative rarity of the procedure), and a lack of procedural and rehabilitation information. Few studies detailed the surgical techniques or rehabilitation programs implemented; thus, we were unable to analyze whether differences in surgical technique or rehabilitation measures had an effect on rate of return to sport among high-level baseball players. Future studies may wish to evaluate these measures to better guide the treatment of professional athletes with recurrent UCL insufficiency after primary reconstruction.
Conclusion
This systematic review demonstrated a limited rate of return to preinjury level of sport among elite-level baseball players who underwent revision UCL reconstruction. Pitching durability and career longevity were inferior to results that were reported for players who underwent primary UCL reconstruction alone. This study suggests that outcomes after revision UCL reconstruction are not reliable and elite-level players should be counseled accordingly.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.M.G. has received education payments from Arthrex and education, travel, and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.