
Abstract
Background:
The prolonged tendon-healing process, the high costs associated with treatment, the increase in the number of injuries over the past decades, and the lack of consensus on the optimal treatment of tendon injuries are a global problem. Restoring the normal tendon anatomy and decreasing the healing time are key factors for treatment advancement.
Hypothesis:
Application of a purified protein from natural latex (PPNL) accelerates the healing process, increasing collagen synthesis and decreasing metalloproteinases. PPNL associated with a simpler suture technique should decrease the healing time.
Study Design:
Controlled laboratory study.
Methods:
Injury, surgery, and treatment with PPNL were conducted with male Sprague-Dawley rats. Two suture techniques were used: U-suture, a simpler and lesser traumatic technique, and Kessler-Tajima, to avoid strangulation of the microcirculation. Achilles tendons were completely sectioned, and 100 µL of 0.1% PPNL was applied on the tendon during surgery. Tendon morphology, distribution, and quantity of collagen types I and III, as well as expression of TIMP-1, TIMP-2, MMP-2, and MMP-9 and ultrastructural aspects of cells and collagen fibrils, were assessed after 2 and 4 weeks.
Results:
PPNL treatment improved collagen type I synthesis and reduced MMP-2 expression. All groups showed a 6.8-times increase in tendon weight as compared with the control group after 2 weeks and a 5.2-times increase after 4 weeks. All groups showed an increase in diameter after 4 weeks, except for the ones treated with PPNL, which showed a slight reduction in diameter. The peak of concentration of collagen fibrils with a 80-nm diameter was 27.79% in the control group; all other experimental groups presented fibrils between 50 and 60 nm. However, the best results were observed with Kessler-Tajima suture associated with PPNL.
Conclusion/Clinical Relevance:
There are no known medicines or substances capable of aiding the tendon healing process besides surgery. The discovery of a substance able to improve this process and decrease its duration represents an important advancement in orthopaedic medicine.
The Achilles tendon originates from the merging of the soleus and gastrocnemius muscles and is inserted distally onto the calcaneus bone. 32 Tendons are fibrous connective tissues composed of cells within a complex extracellular matrix (ECM) rich in collagens, proteoglycans, glycoprotein, and water. 58 A normal tendon is basically composed of 2 types of cells: 90% to 95% is composed of tenoblasts and tenocytes, and the remaining 5% to 10% consists of chondrocytes at the bone attachment, synovial cells of the tendon sheath, and vascular cells. 53 Rupture of this tendon is a common injury that causes significant morbidity. Its incidence seems to have increased over the past several decades, and it is estimated that tendon injuries will continue to rise due to the increase in life expectancy and sports practice, placing an enormous financial strain on health care.1,48
Every year, >30 million musculoskeletal injuries are registered worldwide, and nearly half of them involve tendons and ligaments. The USA and EU associated expenditure exceeds US$180 billion per year. 20 There is no consensus in the literature on the optimal treatment for Achilles tendon ruptures, but they can be treated either nonoperatively or operatively with open or percutaneous repairs; however, some studies indicate surgery as the best option, mainly for athletes.14,35
Many types of sutures are acceptable, but here we chose the Kessler-Tajima (KT) to avoid strangulation of the microcirculation, 8 and the U-suture, which some studies showed as the simplest and least traumatic repair, leading to a more rapid healing of the tendon.8,17 Both sutures have only 2 suture arms spanning the repair site.
The basis for the KT suture concept lies on 2 longitudinal strands, 4 corner loops, and 2 transverse parts, all in continuity. This continuous configuration dictates that longitudinal loading of the tendon repair will also result in loading of the corner loops and the transverse suture strands. 60 The U-suture has just 2 longitudinal strands that join the 2 ruptured tendon parts; it is considered the simplest suture technique, and its name comes from the fact that it is presented in a U shape at the transverse section view after the stitch is drawn. 12
Apart from surgery, there is no known medicine or substance capable of aiding the tendon-healing process. Here, we applied a purified protein from natural latex (PPNL) extracted from Hevea brasiliensis, which previous studies showed to have good repair properties in several tissues. PPNL has been successfully used in dogs as a biomembrane in pericardium repair, 50 in alveolar bone regeneration, and after tooth extraction, demonstrating biocompatibility and gradual integration into the alveolar bone. 6 In humans, it has been used to treat tympanic membrane perforation. 44
More recent studies used the PPNL as a gel applied at the repair site. It was shown to restore morphology and function of the sciatic nerve7,15,41 and to correct defective bone in rats 25 and retinal neovascularization in rabbits, 51 without rejection or signs of infection. All these studies primarily demonstrated the biocompatibility of PPNL,6,40 an angiogenic effect, 39 and extracellular matrix formation, 40 which expedites and improves tissue healing. The present study, however, is the first study to assess the effects of PPNL on the tendon.
Matrix metalloproteases (MMPs) are the major enzymes involved in remodeling the ECM of tendons, and a balance between MMPs and tissue inhibitors of metalloproteases (TIMPs) is required to maintain ECM homeostasis. 38 MMP-2 and MMP-9 are MMPs with collagenolytic activity, and they are upregulated in the ruptured Achilles tendons 59 and inhibited by TIMP-1 and TIMP-2. 30
Thus, we assessed the influence of the type of suture on the tendon repair and whether PPNL improves tendon healing, evaluating collagen synthesis and arrangement, expression of TIMP-1, TIMP-2, MMP-2, and MMP-9, as well as the morphology and ultrastructural aspects of the Achilles tendon.
Methods
Animals
The subjects were male Sprague-Dawley rats (90 days old, ±350 g) from the animal house of the Department of Anatomy of the Institute of Biomedical Sciences (University of São Paulo), where they were maintained in plastic standard cages (5 rats in each cage) with free access to food and water and raised under a controlled room temperature (22°C ± 2°C) and a light-dark cycle of 12 hours.
All experimental groups were analyzed 2 and 4 weeks after surgery2,23,42 and organized into 9 groups: control, U-suture analyzed after 2 weeks (U2w), U-suture plus PPNL after 2 weeks (UP2w), KT after 2 weeks (K2w), KT plus PPNL after 2 weeks (KP2w), and the same conditions after 4 weeks (U4w, UP4w, K4w, and KP4w). Groups assigned to histology and scanning electron microscopy (SEM) were composed of 3 rats. Groups assigned to transmission electron microscopy (TEM) and Western blot were composed of 5 rats, totaling 288 rats.
This study was approved by the Ethics Committee in Animal Experimentation of the Institute of Biomedical Sciences (process 016/14).
Surgery
The rats were anesthetized with ketamine (Dopalen; Ceva) and xylazine (Anasedan; Ceva) at dosages of 75 and 10 mg/kg, respectively. 16 The surgery site was shaved and disinfected with a 10% iodopolividone aqueous solution (Vic Pharma). Achilles tendons were cross-sectioned 7 mm above the calcaneum bone with a 12-cm scissor. 43 The tendons were then sutured with either the U-suture or the KT suture (see the Appendix Figure A1, available in the online version of this article), followed by the suture of the skin. Groups treated with PPNL also used 1 of the 2 sutures and 100 µL of 0.1% PPNL carried in a vehicle of 1% hyaluronic acid hydrogel, which was pipetted on the tendons according to Dias et al. 15 After that, the skin was sutured. PPNL has the consistency of a thick gel, which prevents its spreading to the surrounding sites. Tendon and skin were sutured with a biodegradable catgut 5-0 (Technofio CS57MR15).
After surgery, the animals received 0.1 mL/100 g of an anti-inflammatory (Banamine; Intervet) and 0.1 mL/100 g of an antibiotic (Veterinary Pentabiotic; Fort Dodge). 25 Lidocaine hydrochloride (21.0 mg/mL) and benzethonium chloride spray (1.33 mg/mL) (Timeolate; Lifar) were applied daily for 1 week.
Surgery was performed on the left hindlimb of each rat, and only that limb was used in the analyses. In the control group, the left Achilles tendon was used.
Histological Procedures
The Achilles tendons were removed and immersed in 4% formaldehyde fixative solution (Synth 01P1005.01.AF) for 48 hours at room temperature. After tendons were dehydrated in a graded ethanol series (70°-100°, 30 minutes for each grade), they were diaphanized with xylene (Synth 00X1001.14.BJ) for 30 minutes, repeated 3 times. The tendons were embedded in paraffin, and sections of 7-µm thickness were mounted in glass slides and stained with hematoxylin-eosin and picrosirius red.
Conventional and polarized light microscopy was carried out on a light microscope (Nikon Eclipse E600) equipped with a camera (Nikon Digital Sight DS-Ri1). For the polarized light microscopy analyses, once the microscope was set up, all slides were analyzed at once to keep consistency throughout the experiment.
The microscope polarizer was initially adjusted to obtain a background image completely black; then, with NIS-Elements AR 3.2 software, the light intensity was set to 80 milliseconds.
Scanning Electron Microscopy
The Achilles tendons were removed after perfusion with a modified Karnovsky solution with 2.5% glutaraldehyde (Sigma-Aldrich V000383) and 2% formaldehyde (Synth 01P1005.01.AF) in 0.1M sodium phosphate buffer at pH 7.4 (monobasic sodium phosphate [Synth 00F1034.02.AH] plus bibasic sodium phosphate [Synth 01F1033.01.AF]). 61
The tendons were immersed in the same solution for 24 hours at 4°C, rinsed in 0.1M phosphate buffer solution at pH 7.4, and then cryofractured with liquid nitrogen and immersed in 1% osmium tetroxide (EMS 19100) for 2 hours at 4°C. The tendons were then dehydrated in a graded ethanol series (70°-100°, 15 minutes per grade). Tendons were dried in a Balzers CPD-030 critical point apparatus with liquid carbon dioxide, mounted in metal stubs, and coated with gold ions in a Balzers Union SCD-040 apparatus.
All analyses were done at the center of the injury. The cross cryofracture samples were analyzed in a rectangular area of 0.027 mm2 at 20,000× magnification, and the longitudinal cryofracture samples were analyzed in an area of 2.73 mm2 with 2000× of magnification.
The samples were analyzed in a scanning electron microscope (Jeol JSM-7401F) and Jeol Neoscope (JCM-5000) at the Analytical Center of the Institute of Chemistry (University of São Paulo).
Transmission Electron Microscopy
The Achilles tendons were removed after perfusion as described in the Scanning Electron Microscopy section. They were then immersed in the same solution for 3 hours at room temperature, rinsed in 0.1M phosphate buffer solution at pH 7.4, postfixed with 1% osmium tetroxide for 2 hours at 4°C, and immersed in 0.5% uranyl acetate (EMS 22400) overnight.
Tendons were dehydrated in a graded ethanol series (50°-100°, 30 minutes per grade), followed by 4 stages of dehydration in propylene oxide (EMS 20401) for 30 minutes each. The samples were then embedded in Spurr’s resin (EMS 14300) for ultrathin sections of 60-nm thickness, collected on copper grids (EMS G200-Cu), and counterstained with uranyl acetate–saturated solution for 5 minutes and 0.4% lead citrate solution for 3 minutes.49,62
Similar to the SEM analyses, the TEM analyses were done at the center of the injury. The cross-sectional samples were analyzed in a rectangular area of 5.19 mm2 with 50,000× of magnification and an area of 3.82 mm2 with 2000× of magnification for the longitudinal sections.
The samples were analyzed in a transmission electron microscope (Jeol JEM 1010) at 80 kV at the Microscopy Center of the Department of Development and Cell Biology of the Institute of Biomedical Sciences.
Western Blot
For protein extraction, 5 tendons from each group were macerated with liquid nitrogen with a volume of extraction buffer equivalent to 20-fold the tendon weight (4M guanidine hydrochloride [Sigma-Aldrich G4505], 0.05M sodium acetate buffer [pH 5.8; Synth A2034.01.AG], 0.05M ethylenediaminetetraacetic acid [Gibco 15576-028], 1mM phenylmethanesulfonyl fluoride [Sigma-Aldrich P7626]). 5 Samples were kept under stirring for 24 hours at 4°C, homogenized with a sonicator apparatus at 75% frequency, and centrifuged at 11,000 rpm for 10 minutes at 4°C.
Proteins in the supernatant were precipitated with 1M sodium acetate buffer (pH 7.4) and ethanol at a ratio of 9 (ethanol) to 0.5 (sodium acetate buffer) and 0.5 (supernatant) at 4°C for 24 hours. The samples were then centrifuged at 11,000 rpm for 10 minutes at 4°C, and the pellet was collected and homogenized with Tris-HCl (pH 6.8) under stirring for 5 minutes at 95°C. Proteins were quantified with the Bradford method. 10
After quantification, 30 µg of protein was pipetted with 4× Laemmli Sample Buffer (Bio-Rad 1610747) and 10% 2-mercaptoethanol (Sigma-Aldrich M3148) and then stirred for 5 minutes at 95°C. Proteins were subjected to electrophoresis on gradient SDS-polyacrylamide gel (6%-20%) and transferred to nitrocellulose membranes with a Trans-Blot Turbo Transfer System (Bio-Rad), which were blocked with 5% bovine serum albumin for 1 hour at room temperature.
Membranes were incubated with primary antibodies overnight at 4°C: collagen type I (Rhea Imuny IM-0283; 1:500), collagen type III (Cusabio CSB-MA000282; 1:1000), TIMP-1 (Cusabio CSB-PA004293; 1:500), TIMP-2 (Cusabio CSB-PA004294; 1:500), MMP-2 (Cusabio CSB-PA003258; 1:500), MMP-9 (Rhea Imuny IM-0671; 1:500), and β-tubulin (Aves Lab TUJ; 1:5000). Secondary antibodies were incubated at a concentration of 1:30,000 for 1 hour at room temperature. The densitometry analyses were performed with ImageJ software (v 1.52c; National Institutes of Health).
Statistical Analyses
After euthanasia, the rats’ tendons were removed and weighed on an analytical balance (Scientech SA120), except for the tendons assigned to electron microscopy (owing to perfusion).
Tendon diameters were measured from the cross-sectional histological images with 20× magnification with ImageJ 1.52c software. The diameters of collagen fibrils were determined from cross-sectional TEM images per the protocol of Starborg et al. 55 Density, frequency, and distribution of collagen fibrils were calculated in an area of 5.19 mm2. All measurements were determined with ImageJ 1.52c software, following the same protocol. Experimental groups were compared with the control group via 1-way analysis of variance, followed by Dunnet posttest when necessary.
Experimental groups were subjected to 3-way analysis of variance—suture type (U-suture and KT), PPNL application, and time—followed by Tukey posttest when necessary. Data are presented as mean ± SE. The assumptions of normality and homogeneity of variances were verified by the tests of Shapiro-Wilk and Cochran, respectively. The significance level adopted in all tests was 5%. Results were analyzed by the Statistical Center of the Institute of Biomedical Sciences.
Results
In the control group, longitudinal sections stained with hematoxylin-eosin and analyzed under light microscopy showed low overall cellularity with the cells linearly arranged and the predominance of collagen fibers in parallel—normal aspects of a dense regular connective tissue. The cross sections showed tendons with small diameters adjacent to neurovascular bundles separated by loose connective tissue (Figure 1, A and A′).
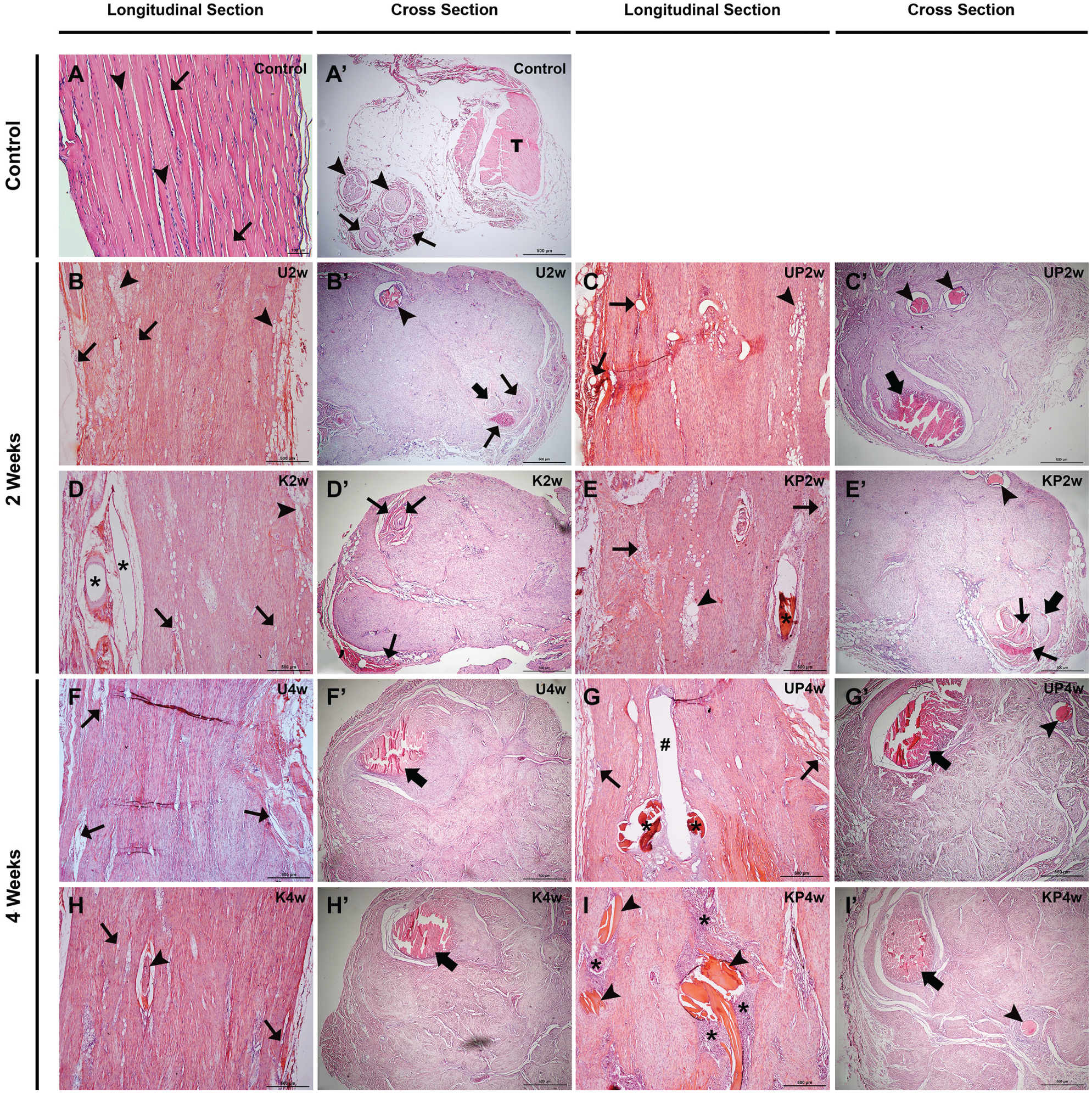
Light microscopy images. Stain: hematoxylin-eosin. Bar: 500 µm, ×40 (unless noted otherwise). Control group: (A) cell nuclei (arrowhead) and collagen fibers (small arrows), bar: 100 µm, ×100; (A′) Achilles tendon (T), nerves (arrowheads), and blood vessels (small arrows). U2w group: (B) adipocytes (arrowheads) and blood vessels (small arrows); (B′) catgut (arrowhead), nerve (larger arrow), and blood vessels (small arrows). UP2w group: (C) adipocytes (arrowhead) and blood vessels (small arrows); (C′) catgut (arrowheads) and catgut knot (large arrow). K2w group: (D) large blood vessels (asterisks), small blood vessels (small arrows), and adipocytes (arrowhead); (D′) blood vessels (small arrows). KP2w group: (E) adipocytes (arrowheads), catgut (asterisk), and blood vessels (small arrows); (E′) catgut (arrowhead), nerve (large arrow), and blood vessels (small arrows). U4w group: (F) blood vessels (small arrows); (F′) catgut knot (large arrow). UP4w group: (G) local area occupied by the catgut (#), catgut (asterisks), and blood vessels (small arrows); (G′) catgut knot (large arrow) and catgut (arrowhead). K4w group: (H) blood vessels (small arrows) and catgut (arrowhead); (H′) catgut knot (large arrow). KP4w group: (I) catgut (arrowheads) and cellular concentration (asterisks); (I′) catgut knot (large arrow) and catgut (arrowhead). K2w and K4w, Kessler-Tajima after 2 and 4 weeks; KP2w and KP4w, Kessler-Tajima plus purified protein from natural latex after 2 and 4 weeks; U2w and U4w, U-suture analyzed after 2 and 4 weeks; UP2w and UP4w, U-suture plus purified protein from natural latex after 2 and 4 weeks.
All experimental groups analyzed after 2 weeks of treatment showed a larger amount of disorganized cells, an increase in number of blood vessels, and adipocyte agglomerates in the ECM. Groups treated with PPNL, regardless of suture type, demonstrated a larger amount of adipocytes. These aspects were observed in the longitudinal sections and are shown in Figure 1, B-E. Cross-sectional samples revealed an increase in the tendon diameter, neurovascular bundles observed in the peripherical region, and the absence of loose connective tissue in between. Catgut suture not yet reabsorbed was also observed in all groups (Figure 1, B′-E′).
The 4-week treatment samples were similar to the 2-week groups, with smaller blood vessels and a smaller amount of adipocytes. Also, we observed a high cellular concentration surrounding catgut (Figure 1, F-I). Suture knots were seen in the cross sections regardless of the technique used. Interestingly, the U-suture knot was tied around the tendon, but during the healing process, it was engulfed by connective tissue and ended up very similar to the KT knot, which was tied between the tendon stumps (Figure 1, F′- I′).
Samples stained with picrosirius red under polarized light microscopy showed the distribution of thin collagen fibers, stained greenish, and thick collagen fibers, stained predominantly yellowish orange.
The control group, whether longitudinal or in cross section, demonstrated a predominance of thick collagen fibers; however, connective tissue around the tendon and neurovascular bundles had a mix of thin and thick collagen fibers (Figure 2, A and A′).
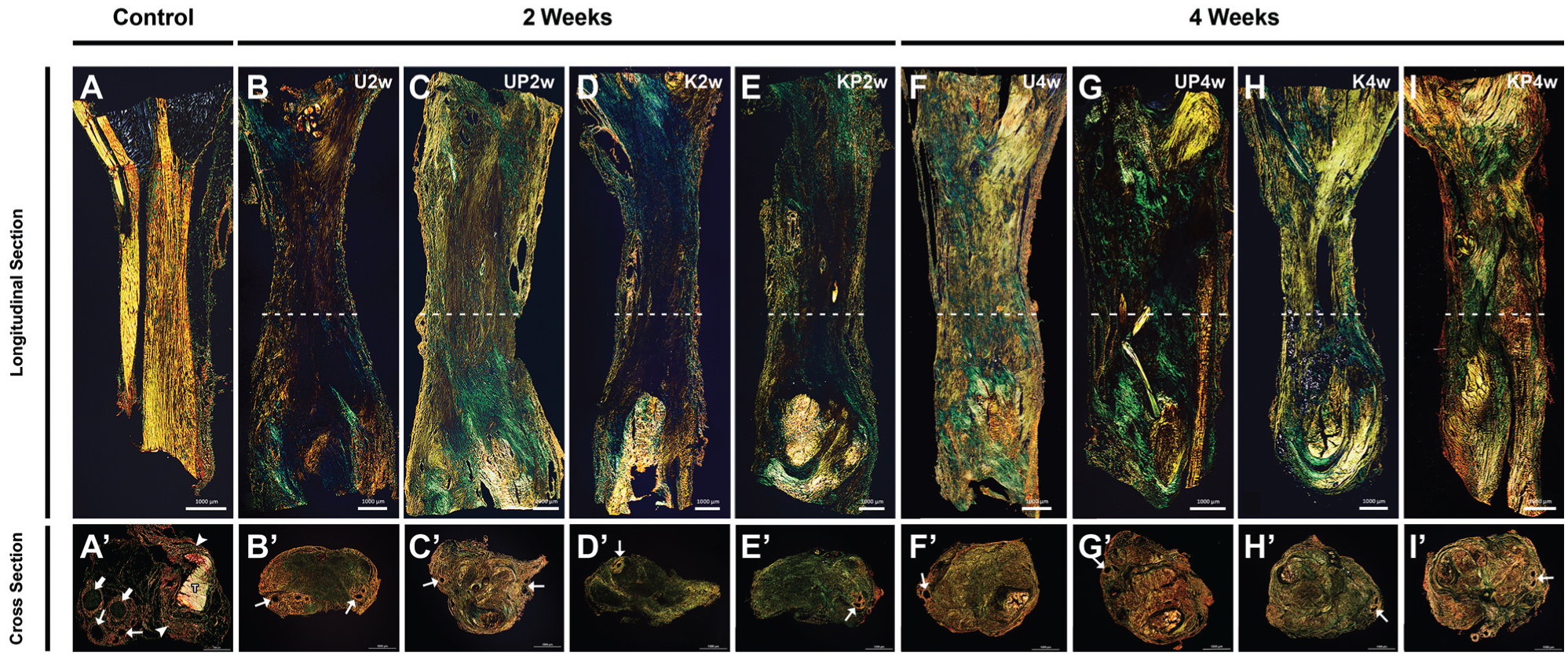
Polarized light microscopy images. Stain: Picrosirius red. Bars: 1000 µm, ×20. Collagen fibers: thin (greenish), thick (yellowish orange). (A-I) Longitudinal section. (B-I) Approximate section location (dashed line). (A′-I′) Cross section. (A′) Tendon (T), connective tissue around tendon (arrowheads), blood vessels (small arrows), and nerve (large arrow). (B′-I′) Show tendon and blood vessels (small arrows). K2w and K4w, Kessler-Tajima after 2 and 4 weeks; KP2w and KP4w, Kessler-Tajima plus purified protein from natural latex after 2 and 4 weeks; U2w and U4w, U-suture analyzed after 2 and 4 weeks; UP2w and UP4w, U-suture plus purified protein from natural latex after 2 and 4 weeks.
Longitudinal sections of the experimental groups—regardless of suture technique, treatment, or time—showed thin and thick collagen fibers distributed throughout the tissue, with no discernible pattern of organization (Figure 2, B-I). Cross sections demonstrated tendons with larger diameters when compared with those of the control group. All experimental groups lacked connective tissue between tendon and neurovascular bundles, suggesting the engulfment of the neurovascular bundles by the tendon. The U2w group presented an oval shape in the tendon cross-section, thin collagen fibers at the center of the tendon, and thick collagen fibers in the peripheral region (Figure 2B′), whereas the group treated with PPNL (UP2w group) had a rounded shape and a predominance of thick collagen fibers (Figure 2C′).
Both groups with the KT suture showed a predominance of thin collagen fibers and an oval shape (Figure 2, D′ and E′). Groups treated with PPNL were more rounded than the corresponding groups without treatment (Figure 2, B′-E′).
All groups analyzed at 4 weeks were rounded. Groups where the U-suture was used had more thick collagen fibers than did the groups sutured with KT, but all groups analyzed at 4 weeks had more thick collagen fibers than did the groups analyzed within 2 weeks (Figure 2, F′-I′).
Regarding weight and diameter, groups with the U-suture, regardless of PPNL treatment, presented a mean weight 7.1 times higher than that of the control group after 2 weeks. Similarly, groups with the KT suture, regardless of PPNL treatment, presented a mean weight 6.5 times higher than that of control after 2 weeks. After 4 weeks, the U-suture groups had a mean weight 5.4 times higher than that of the control group, while KT group’s mean weight was 5.1 higher.
Thus, in the later period, the U-suture and KT groups presented, on average, a 1.3-times reduction in weight. The control group was statistically different from all other groups (P < .001), and the 4-week groups were different from the 2-week groups regardless of suture technique applied and PPNL treatment (P < .001) (Figure 3A, Table 1).

Weight and diameter of the tendons. Values are presented as mean ± SE. (A) Tendon weight. ANOVA, Dunnet: control group is different from all other groups (P < .001). ANOVA, Tukey: 2-week groups are different from 4-week groups regardless of PPNL treatment and suture technique (*P < .001). (B) Tendon diameter. ANOVA, Dunnet: All groups are different from control group (P < .0001) except for the K2w group (*P > .05). ANOVA, Tukey: 2-week groups are different from 4-week groups regardless of PPNL treatment and suture technique (#P < .0001). K2w group is different from all 4-week groups (&P < .05). ANOVA, analysis of variance; PPNL, purified protein from natural latex. K2w and K4w, Kessler-Tajima after 2 and 4 weeks; KP2w and KP4w, Kessler-Tajima plus purified protein from natural latex after 2 and 4 weeks; U2w and U4w, U-suture analyzed after 2 and 4 weeks; UP2w and UP4w, U-suture plus purified protein from natural latex after 2 and 4 weeks.
Tendon Weight (in grams) a
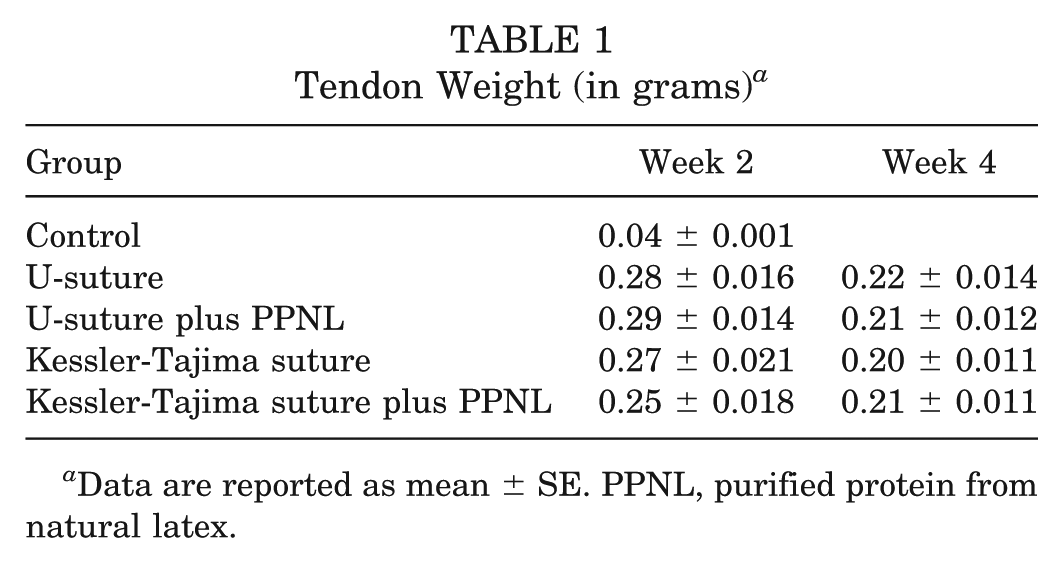
Data are reported as mean ± SE. PPNL, purified protein from natural latex.
Conversely, the tendon diameter increased with time. All experimental groups, other than K2w group, showed a larger diameter when compared with that of control; the K2w group presented no statistical difference (P = .08).
Interestingly, groups analyzed after 2 weeks, with PPNL application, showed a larger diameter than did groups without PPNL treatment; however, this situation was reversed after 4 weeks. Within 4 weeks, all groups showed a further increase in diameter, except for the ones treated with PPNL, which showed a slight reduction in diameter. A statistical difference was observed with respect to time of analysis: groups analyzed within 2 weeks were different from groups analyzed after 4 weeks, regardless of suture technique and PPNL treatment. All data are shown in Figure 3B and Table 2.
Tendon Diameter (in millimeters) a
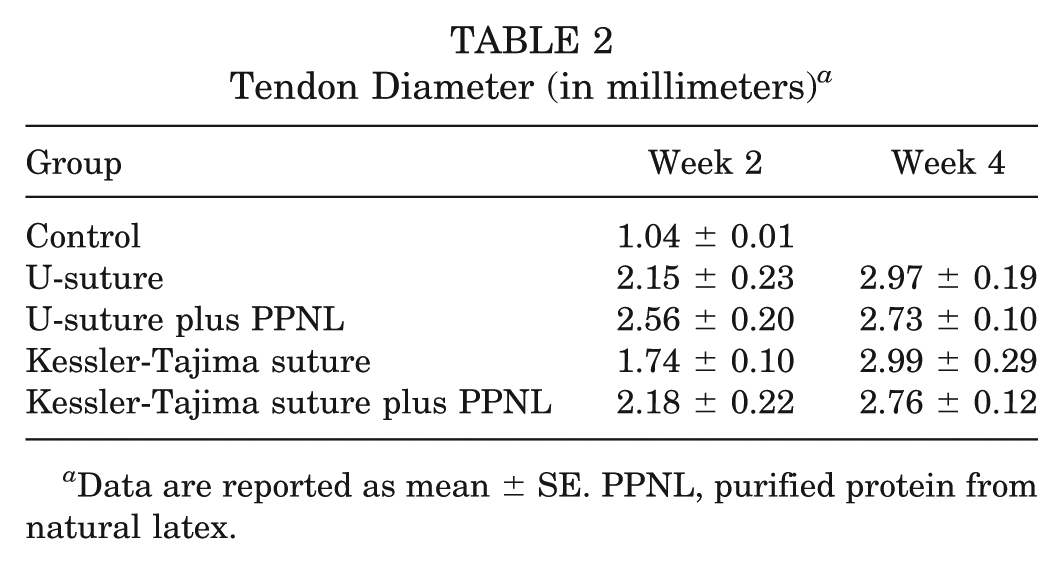
Data are reported as mean ± SE. PPNL, purified protein from natural latex.
Morphological aspects and collagen fiber organization were observed with SEM. The longitudinal cryofracture of the control group showed collagen fibers arranged in bundles; however, cross cryofracture revealed that collagen fibers were tightly close (Figure 4, A and A′).
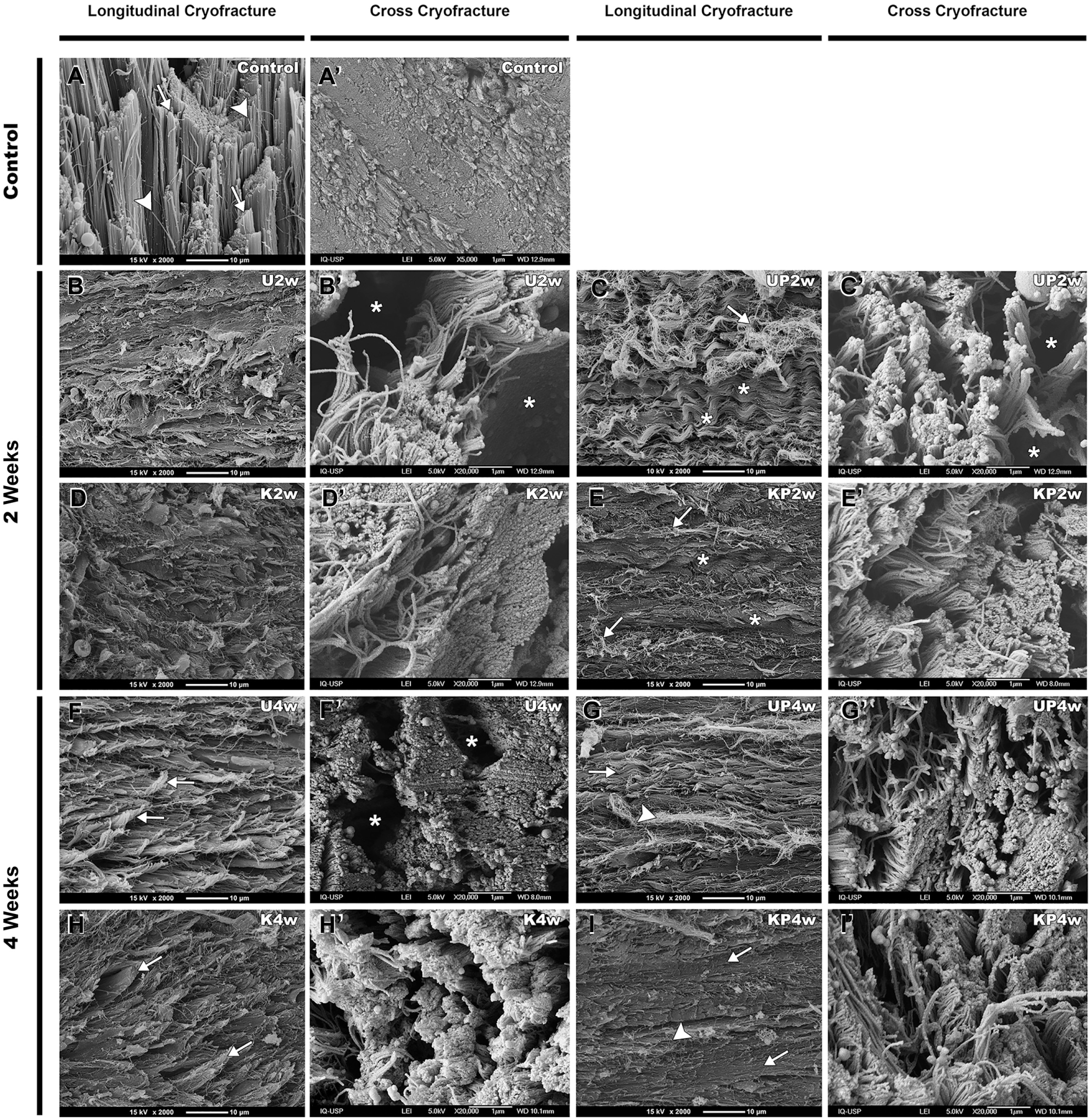
Electron micrograph (scanning electron microscope). Longitudinal cryofracture. Bars: 10 µm, ×2,000. Cross cryofracture images. Bars: 1 µm, ×20,000. (A) Collagen fiber (arrowheads), collagen fiber bundles (arrows). (A′) Cross cryofracture of the control group showing collagen fibers packed closely together. (B) Longitudinal cryofracture of the U2w group showing collagen fibers without arrangement. (B′) Collagen fiber bundles with spaces (asterisks) among them. (C) Thin collagen fibers (arrow) and collagen fibers with wavy aspect (asterisks). (C′) Small collagen fiber bundles with some spaces (asterisks) among them. (D) Longitudinal cryofracture of the K2w group showing collagen fibers without arrangement. (D′) Cross cryofracture of the K2w showing collagen fibers in different directions and smaller gaps among them. (E) Some thin collagen fibers (arrows) and wavy collagen fibers (asterisks). (E′) Cross cryofracture of the KP2w. (F) Collagen fibers (arrows) organized in parallel. (F′) Collagen fibers bundles with some spaces (asterisks) among them. (G) Collagen fibers organized in parallel showing some wavy fibers (arrow) and thin collagen fibers (arrowhead). (G′) Cross cryofracture of the UP4w. (H) Collagen fibers (arrows) organized in parallel. (H′) Cross cryofracture showing initial collagen fiber bundles. (I) Collagen fibers (arrows) organized in parallel, showing thin collagen fibers (arrowhead). (I′) Cross cryofracture of the KP4w. K2w and K4w, Kessler-Tajima after 2 and 4 weeks; KP2w and KP4w, Kessler-Tajima plus purified protein from natural latex after 2 and 4 weeks; U2w and U4w, U-suture analyzed after 2 and 4 weeks; UP2w and UP4w, U-suture plus purified protein from natural latex after 2 and 4 weeks.
The longitudinal cryofracture of the injury site of all experimental groups showed collagen fibers without a discernible pattern of organization and absence of bundles (Figure 4, B-E). Both PPNL-treated groups (UP2w and KP2w) demonstrated collagen fibers with a wavy aspect (Figure 4, C and E). Groups without PPNL treatment analyzed at 4 weeks (Figure 4, F and H) revealed a better arrangement of the fibers than that of the groups analyzed at 2 weeks. Groups treated with PPNL presented collagen fibers more closely packed. The KP4w group and the control group presented similar collagen fibril densities, as quantified by TEM, producing the appearance of a fibrous tissue without spaces (Figure 4, G and I).
Cross cryofracture of the experimental groups revealed an initial formation of collagen fiber bundles; however, in the U2w and U4w groups, these bundles were more interspaced (Figure 4, B′ and F′). This spacing decreased with PPNL treatment (Figure 4, C′ and G′). Groups with KT suture demonstrated similar patterns at 2 and 4 weeks regardless of PPNL treatment (Figure 4, D′, E′, H′, I′).
TEM was used to evaluate the ultrastructural characteristics of tendon collagen fibrils and cells. At low magnification, the longitudinal sections of the control group showed few cells surrounded by a dense collagen matrix (Figure 5A). All experimental groups demonstrated an increase in tenoblast quantity. These were rounded, elongated, or star-shaped cells with 1 common feature: the euchromatic nuclei (Figure 5, B-I).
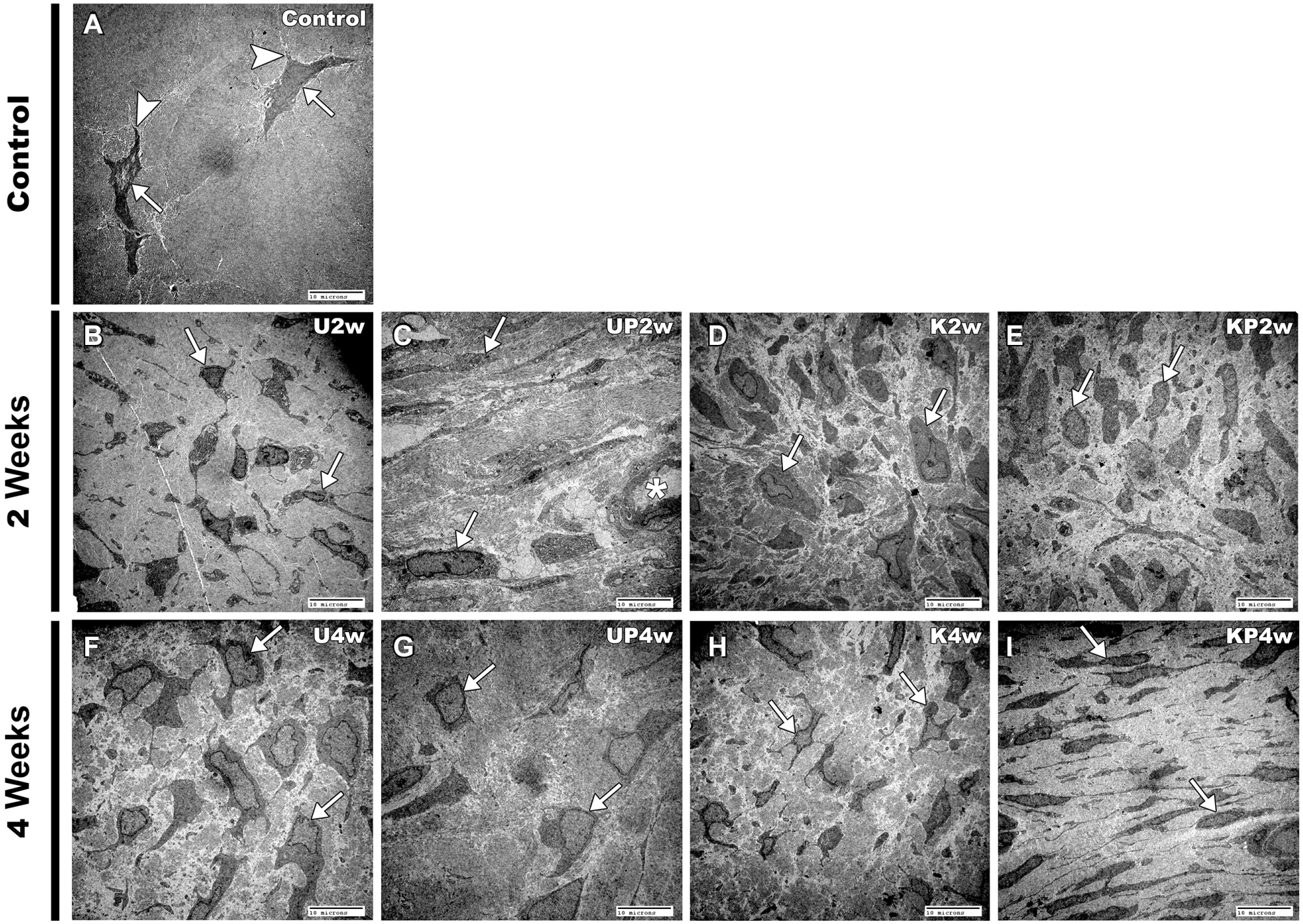
Electron micrograph (transmission electron microscope). Longitudinal sections. Bars: 10 µm, ×2,000. (A) Control group, tenocytes (arrows) and cellular processes (arrowheads). (B-E) 2-week groups. (F-I) 4-week groups. Arrows indicate tenoblasts; asterisk indicates blood vessel in panel C. K2w and K4w, Kessler-Tajima after 2 and 4 weeks; KP2w and KP4w, Kessler-Tajima plus purified protein from natural latex after 2 and 4 weeks; U2w and U4w, U-suture analyzed after 2 and 4 weeks; UP2w and UP4w, U-suture plus purified protein from natural latex after 2 and 4 weeks.
At high magnification, cross sections of the control group showed collagen fibrils with a mean diameter of 83.8 ± 1.3 nm. The U2w group presented a smaller diameter, 59.5 ± 1.3 nm, and the group treated with PPNL, UP2w, showed a diameter close to that of the control group, 74.3 ± 3.6 nm. The K2w and KP2w groups had diameters of 54.5 ± 2.0 nm and 52.0 ± 1.8 nm, respectively.
The U4w group demonstrated a diameter similar to that obtained after 2 weeks, 52.8 ± 3.7 nm; the diameter of the UP4w group was smaller than that of the UP2w group, 51.4 ± 1.2. K4w showed a diameter slightly larger, with 55.5 ± 1.3 nm, and KP4w diameters similar to those of controls, 80.7 ± 2.2 nm. The control group was statistically different from all groups except KP4w. Data are shown in Figure 6, A and B.
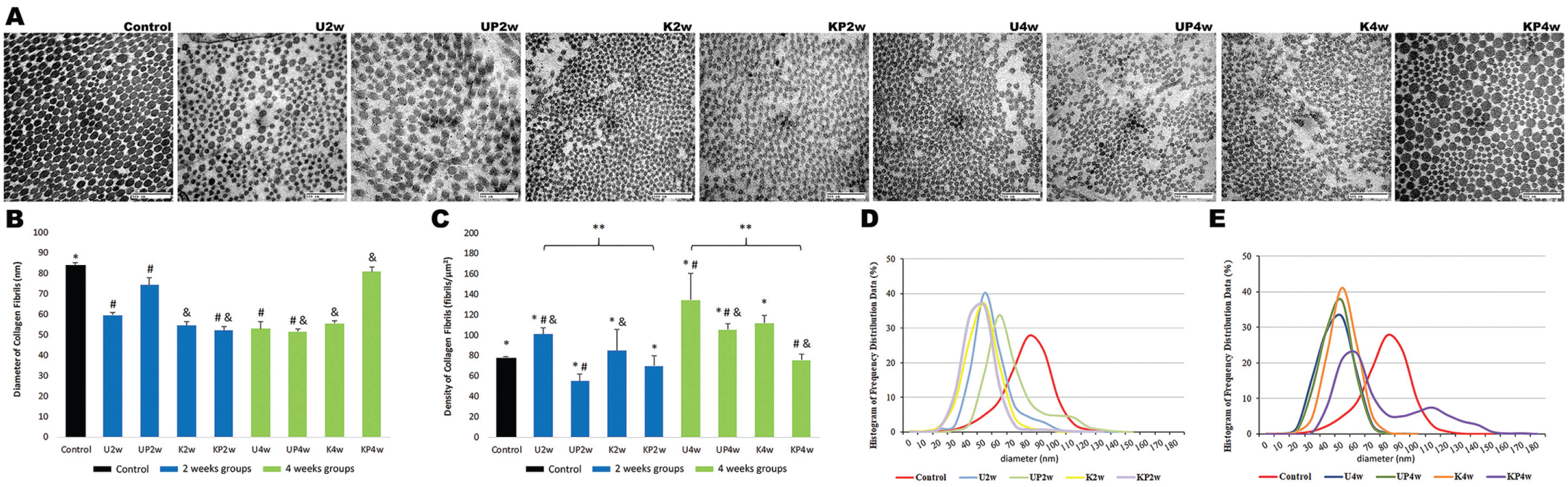
(A) Electron micrograph (transmission electron microscope) for all groups (cross sections). Bars: 500 nm, ×50,000. (B) Diameter of collagen fibrils. Values are presented as mean ± SE. ANOVA, Dunnet: control group is different from all other groups, *P < .05, except for KP4w group P > .05. ANOVA, Tukey, P < .05: #UP2w group significantly different from U2w, KP2w, U4w, and UP4w groups; &KP4w significantly different from K2w, KP2w, UP4w, and K4w groups. (C) Density of collagen fibrils. Values are presented as mean ± SE. ANOVA, Dunnet: control group significantly different from all groups, *P < .05, except for KP4w group, P > .05. ANOVA, Tukey, P < .05: **2-week groups significantly different from 4-week groups regardless of PPNL treatment and suture technique; #U4w significantly different from U2w, UP2w, UP4w, and KP4w; &K2w significantly different from U2w, UP4w, and KP4w. All PPNL-treated groups are different from groups without treatment regardless of suture technique and period, P < .001. Histogram of frequency and distribution data of control group and (D) 2-week groups and (E) 4-week groups. ANOVA, analysis of variance; PPNL, purified protein from natural latex. K2w and K4w, Kessler-Tajima after 2 and 4 weeks; KP2w and KP4w, Kessler-Tajima plus purified protein from natural latex after 2 and 4 weeks; U2w and U4w, U-suture analyzed after 2 and 4 weeks; UP2w and UP4w, U-suture plus purified protein from natural latex after 2 and 4 weeks.
The control group showed that the larger the diameter, the smaller the density, since fibril density is the number of fibrils per unit of cross-sectional area. Therefore, the control group had the larger collagen fibrils and, consequently, fewer fibrils per area. This group presented a mean density of 77.0 ± 2.1 fibrils/µm2, as compared with the U2w group (100.9 ± 6.3 fibrils/µm2), the UP2w group (54.8 ± 7.3 fibrils/µm2), the K2w group (84.9 ± 20.4 fibrils/µm2), and the KP2w group (69.6 ± 9.8 fibrils/µm2), with this last group being the second smallest in both diameter and density.
All experimental groups showed an increase in density at 4 weeks: U4w group, 134.6 ± 26.2 fibrils/µm2; UP4w group, 105.4 ± 5.7 fibrils/µm2; K4w group, 111.7 ± 7.4 fibrils/µm2; and KP4w group, 75.5 ± 5.6 fibrils/µm2. All these groups demonstrated density similar to that of control but had collagen fibrils with smaller diameters. The only exception was the KP4w group, which had a diameter and density similar to those of the control group; however, all PPNL-treated groups showed a smaller density than that of their corresponding groups without treatment. Detailed data are shown in Figure 6C.
The distribution of collagen fibrils was also analyzed. The control group showed the highest concentration of collagen fibrils at 80 nm (27.79%). The U2w, K2w, KP2w, U4w, UP4w, and K4w groups had a concentration of 37.61% at 50 nm, and the PPNL-treated groups UP2w and KP4w showed a peak concentration of 28.23% at 60 nm. However, the KP4w group presented a second peak concentration of 7.46% at 110 nm; this group was the only one with fibrils between 160 and 170 nm. All detailed data for each group are shown in Table 3 and Figure 6, D and E.
Distribution of the Collagen Fibrils by Diameter a
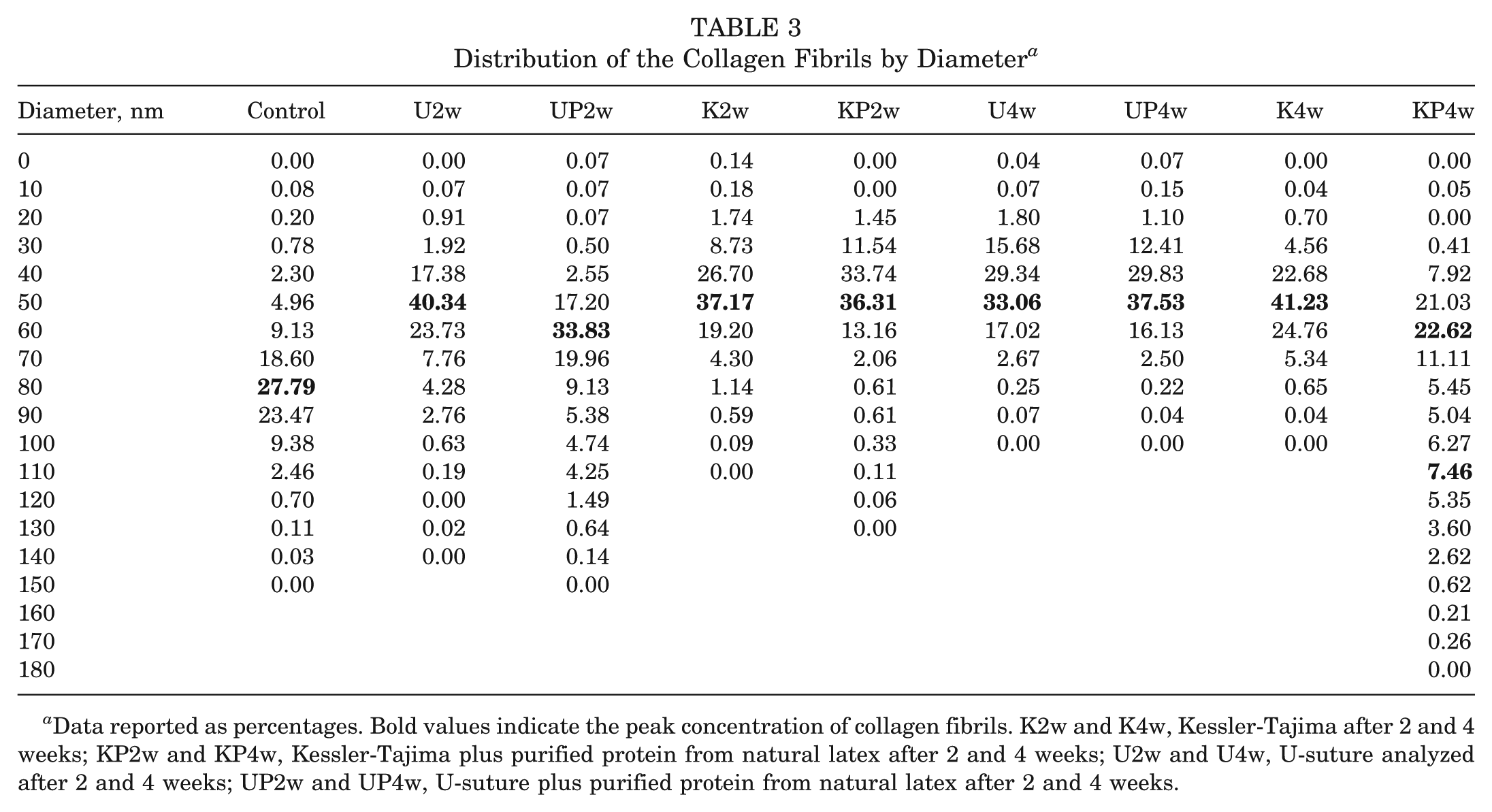
Data reported as percentages. Bold values indicate the peak concentration of collagen fibrils. K2w and K4w, Kessler-Tajima after 2 and 4 weeks; KP2w and KP4w, Kessler-Tajima plus purified protein from natural latex after 2 and 4 weeks; U2w and U4w, U-suture analyzed after 2 and 4 weeks; UP2w and UP4w, U-suture plus purified protein from natural latex after 2 and 4 weeks.
A semiquantitative analysis of collagen types I and III was conducted with Western blot. The control group did not differ from any other group, and all experimental groups analyzed within 2 weeks showed a similar collagen type I expression. Although the difference was not significant, the PPNL-treated groups expressed a larger amount of collagen type I than did the corresponding groups without treatment (Figure 7A). Collagen type III expression was equivalent in the control group and the other groups but was underexpressed in the groups with KT suture analyzed within 2 weeks. The peak expression was observed in the UP2w and U4w groups. All experimental groups had increased collagen type III expression when analyzed within 4 weeks, except for the UP2w and U4w groups, which remained at similar degrees (Figure 7B).
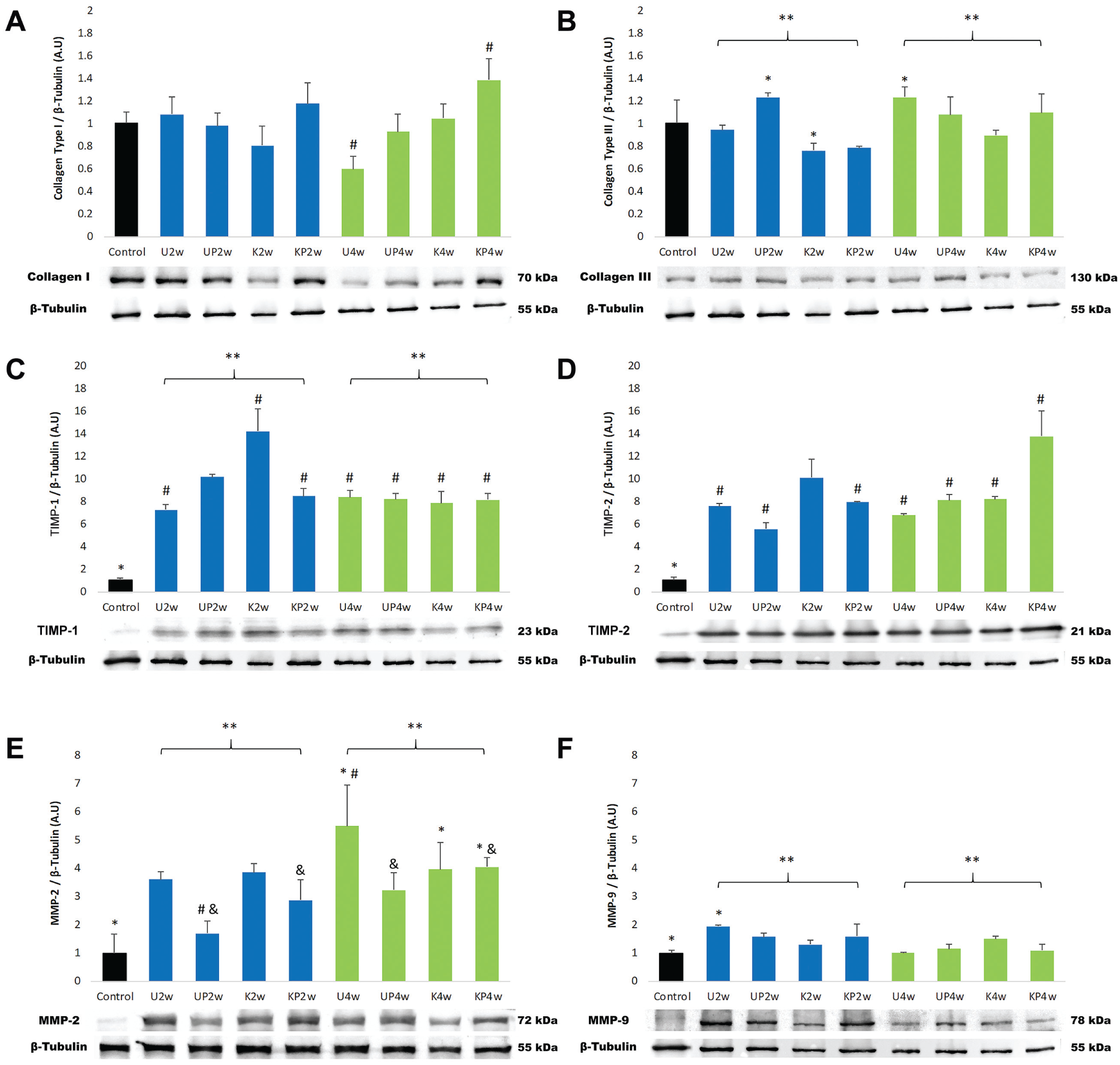
Protein expression by Western blot. Values are presented as mean ± SE. (A) Collagen type I. ANOVA, Dunnet: control group is not different from any other group, P > .05. ANOVA, Tukey, #P < .05: KP4w significantly different from U4w. (B) Collagen type III. ANOVA, Dunnet: Control group is not different from any other group, P > .05. ANOVA, Tukey, *P < .05: K2w significantly different from UP2w and U4w. **2-week groups significantly different from 4-week groups regardless of PPNL treatment and suture technique. (C) TIMP-1. ANOVA, Dunnet: control group is different from the other groups, *P < .05. ANOVA, Tukey, P < .05: #K2w significantly different from U2w, KP2w, U4w, UP4w, K4w, and KP4w. **2-week groups significantly different from 4-week groups. (D) TIMP-2. ANOVA, Dunnet: control group is different from other groups, *P < .05. ANOVA, Tukey P < .05: #KP4w significantly different from U2w, UP2w, KP2w, U4w, UP4w, and K4w. (E) MMP-2. ANOVA, Dunnet: control group significantly different from U4w, K4w, and KP4w, *P < .05. ANOVA, Tukey, P < .05: **2-week groups significantly different from 4-week groups. &PPNL-treated groups significantly different from groups without treatment, #P < .05 (F) MMP-9. ANOVA, Dunnet: control group significantly different from U2w group, *P < .05. ANOVA, Tukey, P < .05: **2-week groups significantly different from 4-week groups. ANOVA, analysis of variance; PPNL, purified protein from natural latex. K2w and K4w, Kessler-Tajima after 2 and 4 weeks; KP2w and KP4w, Kessler-Tajima plus purified protein from natural latex after 2 and 4 weeks; U2w and U4w, U-suture analyzed after 2 and 4 weeks; UP2w and UP4w, U-suture plus purified protein from natural latex after 2 and 4 weeks.
All experimental groups showed TIMP-1 expression about 9 times higher than that of control, except for the K2w group, whose expression was almost 14 times larger than that of control; however, TIMP-1 expression decreased at 4 weeks, and groups reached very similar values (Figure 7C). Similarly, TIMP-2 expression was about 14-fold in KP4w in relation to control and about 7-fold in all other groups. TIMP-2 expression was smaller in PPNL-treated groups analyzed within 2 weeks than in the corresponding groups without treatment. At 4 weeks, the U-suture groups showed similar expression, and in the KP4w group, expression was considerably larger (Figure 7D).
MMP-2 expression was larger in the fourth week but consistently smaller in PPNL-treated groups than in those without treatment, particularly for the U-suture groups. The control group was significantly different from the U4w, K4w, and KP4w groups (Figure 7E). Expression of MMP-9 was lower than that of MMP-2. Expression in the experimental groups analyzed after 2 weeks was 2-fold that of control and at 4 weeks, 1-fold that of control; only the U2w group was significantly different from control (Figure 7F).
Discussion
The main result of this study is that the KT suture associated with PPNL after 4 weeks restores the diameter and density patterns of the collagen fibrils and increases collagen type I synthesis. Moreover, the healthy tendon showed a small amount of cells and a high density of collagen fibers organized in parallel, while all other groups, after 2 and 4 weeks, demonstrated high cellularity. In the inflammatory stage, between the third and seventh day after the injury, cells began to migrate to the injured site. Initially, the cells played a phagocytic role. After the fifth day of migration, the tenoblasts began to synthesize collagen (mainly type III), proteoglycans, and other ECM elements that were initially organized randomly. At the end of the proliferation stage, the tissue was highly cellularized and contained a relative amount of water.26,36 This could explain the increase in the tendon diameter observed in this study.
This increase in mass consequently changed the length and diameter, leading to an initial increase in weight that began to decrease at the fourth week. 54 Our results showed an increase in the diameter at the fourth week, but PPNL-treated groups had a smaller diameter within this period.
In a research with 50 patients between 21 and 55 years old, Kangas and colleagues 28 explained that during the repair process, an elongation of the tendinous tissue occurs, regardless of whether it is immobilized or not, and that this phenomenon occurs within 6 weeks of the surgery, with a very small reduction or stabilization. The shortening occurs between 24 and 60 weeks.
The increase in mass and cross-sectional area of the tendon always occurs during the remodeling process, and during this stage the tissue is resized and reshaped. Consequently, one observes a decrease in cellularization. This process continues until the 10th week, when the tissue changes from cellular to fibrous, cellular metabolism remains high, and cellular and collagen fibers start to align.24,54 Regarding cellular metabolism, another study with human patients showed that it may remain elevated for up to a year after surgery and that the repair occurs from the center toward the periphery of the tissue. 18
Our results for the PPNL-treated groups analyzed within 2 weeks demonstrated the presence of adipocytes among collagen fibers, with the adipocytes diminishing considerably over time. This aspect may be initially explained by Bi and colleagues, 9 who discovered tendon stem/progenitor cells (TSPCs), a finding that is considered the most relevant in the subject in recent years.
Some in vitro and in vivo studies showed that mechanical loads at physiological levels promoted proliferation and differentiation of TSPCs in tenocytes, whereas excessive loading led to differentiation in nontenocyte cells, such as adipocytes, chondrocytes, and osteocytes.65,66 These results suggest that PPNL treatment somehow contributed to a greater mobility or muscular contraction capacity, thus leading to a higher tension on the tendon and the resulting cellular differentiation into adipocytes. However, this is speculation of ours that needs further evaluation.
SEM analyses demonstrated morphological aspects of the collagen fibers. Within the period evaluated, the control group differed from all experimental groups, and regardless of suture technique employed, the groups showed wavy collagen fibers. This wavy aspect appeared on injured tendons, or tendinopathy, accompanied by hypervascularization. 33 We identified all fibers present in the tendon as collagen fibers, since the volume of noncollagen fibers may be considered negligible. 52
In the control group, ultrastructural analysis with TEM showed the tenocytes surrounded by a dense collagen matrix. This cell type presents long cellular processes that protrude deeply into an ECM with well-organized collagen fibrils, but such projections are absent in injured tendons or in any type of tendinopathy. 47
Morphologically, tenocytes are elongated cells, but their shape can vary. Tenoblasts, predominant in all experimental groups, were observed in several shapes—rounded, elongated, or star shaped.19,29 However, in TEM, all experimental groups showed electron-dense heterochromatin adhered to the inner nuclear membrane and electron-lucent euchromatin dispersed throughout the nucleus. The heterochromatin is typically highly condensed, so gene transcription is hindered, whereas euchromatin is less condensed and more accessible to gene transcription; thus, this euchromatic aspect is prevalent in cells with high gene transcription. 56
Ultrastructural characteristics of collagen fibrils demonstrated a decrease in diameter in all experimental groups, with space among them, except for the KP4w group. These spaces were electron lucent in TEM. In the control group, collagen fibrils showed a distribution of 10- to 140-nm diameters; all experimental groups had a decrease in collagen fibrils between 70 and 140 nm. This result is consistent with 2 previous human studies, which indicated that ruptured and degenerated tendons were between 40 and 60 nm and 10 and 20 nm respectively, with a reduction in fibrils at 60 to 150 nm.27,37 However, the KP4w group presented collagen fibrils of several diameters, with 60 nm the most abundant, while the diameter was 80 nm in the control group. The KP4w group had 16.8% more fibrils between 110 and 170 nm than the control group. This group was the most similar to control, since PPNL treatment associated with KT suture after 4 weeks caused the mean diameter and density of collagen fibrils to return to control standards.
The interesting fact is that the UP2w group had collagen fibrils with a diameter similar to that of the control group, although statistically different; however, the diameter decreased over time, and at 4 weeks the opposite was found for KT groups where PPNL had been used. The KP4w group presented collagen fibrils with diameters and densities similar to those of control, with no statistical difference.
We are not able to speculate whether the diameter of collagen fibrils in the KP4w group would decrease, as observed in the UP2w group, had the experiment continued for a longer period. In addition, the distribution of thick and thin fibers, which can be associated with collagen types I and III, respectively, 21 were shown by polarized light microscopy.
This study demonstrated an increase in collagen type I synthesis in PPNL-treated groups at the fourth week. Collagen type I synthesis began on the third day and continued to increase, while collagen type III also began to be synthesized on the third day, reached its peak in the 14th day, and then started to drop. 45 Collagen type III increased with time in all experimental groups. The proliferative response of the tenocytes and tenoblasts to trauma induced the synthesis of both collagen types. 34 Synthesis of collagen type III is a normal physiological process in the tendon healing 31 and provides support for the synthesis of collagen type I. 22
Some healing modulators were analyzed that degrade ECM components, such as MMP-2 and MMP-9. Expression of MMP-2 was lower in all PPNL-treated groups than in groups without PPNL treatment; however, the expression of this metalloproteinase increased with time. MMP-9 remained similar to control with a slight decrease over the weeks.
MMP-2 levels increased from the third day of injury, remained elevated until the 28th day, and participated in the degradation and remodeling of collagen. Also, it broke down collagen fragments generated by the collagenase activity, cleaving intact collagen types I and III. MMP-9 reached its peak of expression between day 7 and day 14, and soon afterward it dropped to almost zero, participating only in the degradation.45,46,54 Moreover, some studies reported that MMP-9 may have a role in the inflammatory reaction and is expressed in macrophages.11,38
The balance between the activity of MMPs and TIMPs regulates the remodeling of the tendon, and an imbalance between these molecules leads to disorders. 30 Our study demonstrated a reduction in TIMP-1 expression over the weeks and a similar expression at both periods analyzed. The high expression of TIMPs can be considered a tissue response to an increase in the synthesis of MMPs, as an effort to reduce the catalytic activity in the tendon matrix. After 4 weeks, TIMP-1 expression seemed to vanish, suggesting that it inhibited the excessive degradation of ECM caused by MMP-2 acutely. 13 However, TIMP-2 has a chronic action, with elevated levels being observed up to 3 years after tendon rupture. 46
Although the PPNL mechanism of action is still poorly understood, it is speculated that an interaction with immune cells might be at play, 57 as demonstrated in studies that found an anti-inflammatory response with an increase in IL-10 and a decrease in IL-1β expression after PPNL use.3,4 Moreover, cardiac fibroblast studies suggested that IL-1β upregulation increases MMP-2 expression and that this activity may be regulated by the PKC-θ, PKC-ζ, and NF-κB pathways. 64 Hence, when MMP-2 expression was reduced with IL-1β, an increase in collagen synthesis was found. 63
In the present study, we observed in PPNL-treated groups, regardless of the suture technique, a decrease in MMP-2 expression and an increase in collagen synthesis, mainly type I. We speculate that PPNL action is mediated by immune cells; however, the PPNL anti-inflammatory effect did not alter MMP-9 levels. Furthermore, the downregulation effect of PPNL on IL-1β may also explain the presence of adipocytes in the 2-week PPNL-treated groups, since one of the functions of IL-1β is to inhibit the adipogenic differentiation of TSPCs. 67 However, the 4-week groups showed a lower number of adipocytes, suggesting that the IL-1β inhibitory effect on TSPC differentiation may occur in only the acute phase.
Conclusion
Based on our results, PPNL treatment improved the synthesis of collagen type I and reduced MMP-2 expression.
The KT suture associated with PPNL after 4 weeks showed better results regarding organization, distribution, diameter, and density of collagen fibrils. However, future biomechanical tests should be conducted to assess whether PPNL application associated with the KT suture increases tendon resistance, avoiding a rerupture.
Supplemental Material
DS_10.1177_0363546518822836 – Supplemental material for Application of a Purified Protein From Natural Latex and the Influence of Suture Type on Achilles Tendon Repair in Rats
Supplemental material, DS_10.1177_0363546518822836 for Application of a Purified Protein From Natural Latex and the Influence of Suture Type on Achilles Tendon Repair in Rats by Diego Pulzatto Cury, Bárbara Tavares Schäfer, Sonia Regina Yokomizo de Almeida, Marta Maria da Silva Righetti and Ii-sei Watanabe in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank Luciano César Pereira Campos Leonel, PhD, Maria Inês Nogueira, PhD, Maria Luiza M. Barreto-Chaves, PhD, Rosana Duarte Prisco, and Kelly Patrícia Nery Borges.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by FAPESP Fundação de Amparo à Pesquisa do Estado de São Paulo (São Paulo Research Foundation; grant 2015/24087-3) and CAPES Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (Coordination of Superior Level Staff Improvement). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.