
Abstract
Background:
The glenoid track concept has been widely used to assess the risk of instability caused by a bipolar lesion. The mean glenoid track width is reported to be 83% of the glenoid width. However, this width seems to be affected by the range of motion of the shoulder. By clarifying the relationship between the range of shoulder motion and the glenoid track width, a more precise determination of the glenoid track width for each individual could be possible.
Purpose:
To determine the relationship between the glenoid track width and the range of motion of healthy volunteers.
Study Design:
Descriptive laboratory study.
Methods:
Magnetic resonance imaging was taken in 41 shoulders of 21 healthy volunteers (mean age, 32 years) with the arm in maximum horizontal extension, with the arm kept in 90° of abduction and 90° of external rotation. Three-dimensional surface bone models of the glenoid and the humerus were created with image analysis software. The distance from the anterior rim of the glenoid to the medial margin of the footprint of the rotator cuff tendon was defined as the glenoid track width. Active and passive ranges of shoulder motion were measured in the supine and sitting positions. The correlations between the glenoid track width and the ranges of shoulder motion were investigated with Pearson correlation coefficients. Intra- and interobserver reliabilities based on the intraclass correlation coefficient were also analyzed to assess the reliability of the glenoid track measurement.
Results:
The intra- and interobserver reliabilities for the glenoid track measurement were excellent (0.988 and 0.988, respectively). Among all the measurements, the glenoid track width and the active range of motion in horizontal extension in the sitting position showed the greatest correlation coefficient (r = −0.623, P < .0001). A correlation between the glenoid track width and this angle was expressed as Y = −0.49X + 90, where X is the horizontal extension angle (degrees) and Y is the glenoid track width (percentage of glenoid width).
Conclusion:
The present data demonstrate that the greater the horizontal extension angle in abduction and external rotation, the smaller the glenoid track width. An individualized glenoid track width can be obtained by measuring the active horizontal extension angle with the arm in abduction and external rotation in the sitting position.
Clinical Relevance:
An individualized glenoid track width enables selection of a more precise surgical option by the on-track/off-track concept.
Keywords
Glenoid defects and Hill-Sachs lesions are common injuries associated with anterior shoulder instability. The incidence of “bipolar lesion,” which is the combination of glenoid defect and Hill-Sachs lesion, is reported to be 62% to 81% among patients with recurrent anterior dislocation of the shoulder4,6 (D. Kurokawa, personal communication, 2013). It is important for surgeons to assess which bipolar lesion needs to be treated in addition to the soft tissue repair. The concept of the glenoid track proposed by Yamamoto et al 11 has been widely used for the evaluation of a large Hill-Sachs lesion that needs to be treated. The glenoid track is a zone of contact between the glenoid and the humeral head with the arm along the posterior end range of motion (ROM; anterior apprehension position). If a Hill-Sachs lesion is located outside the glenoid track, there is a risk of dislocation.
The glenoid track width was reported to be 84% ± 14% of the glenoid width in a cadaveric study and 83% ± 12% in live shoulders7,11; 83% is widely used these days in various studies.2,5,9 It is speculated that the glenoid track width may change depending on the ROM of the shoulder. It is also speculated that in shoulders with a great amount of ROM, as compared with those with a small amount of ROM, the posterior rim of the glenoid overrides the greater tuberosity, pushing the cuff tendon more laterally on the footprint when the arm comes to the end-range position of abduction and external rotation. This means that the distance between the anterior rim of the glenoid and the medial margin of the footprint, which is defined as the glenoid track width, decreases in shoulders with a great amount of ROM. In contrast, in shoulders with a small amount of ROM, the glenoid track width increases. Therefore, if we use the fixed value of 83% for all patients with various degrees of ROM, we are unable to accurately assess the necessity of surgical treatment for bipolar lesions.
A previous biomechanical study with cadaveric shoulders demonstrated a linear relationship between the glenoid track width and the ROM in horizontal extension. 12 Given this previous study, we hypothesize that the glenoid track width would correlate with the ROM in horizontal extension in live participants. The purpose of this study was to prove our hypothesis.
Methods
We examined 41 shoulders of 21 healthy volunteers. There were 20 male and 21 female participants (mean age, 32 years). They had no history of shoulder pain. The shoulders with joint contracture or shoulder instability were excluded from this study. Informed consent was obtained from all participants prior to their enrollment. This study was approved by the ethical committee of our institute.
Step 1: Image Acquisition
We used a 0.2-T magnetic resonance imaging (MRI) system (Signa Profile HD; General Electric Healthcare) for the measurement of glenoid track width. This device had a wide gantry (diameter, 120 cm; height, 44 cm) and thus could obtain images with the arm in abduction. The 3-dimensional (3D) time-of-flight method was used (repetition time, 12 milliseconds; echo time, 6.6 milliseconds; 1.2-mm slice thickness; flip angle, 40°; field of view, 200 × 160 mm2: 160 × 128 matrix). With use of this method, 3D surface bone models were created. The MRI scans were taken with the participant in the supine position with the arm in maximum horizontal extension, keeping the arm in 90° of abduction and 90° of external rotation (Figure 1). A loop coil was set around the shoulder. A Styrofoam board (thickness, 90 mm) was placed on the back of a volunteer so that the shoulder could be extended horizontally without limitation. An empty space corresponding to the scapula was created to avoid limitation of the scapular motion or undue compression on the scapula.
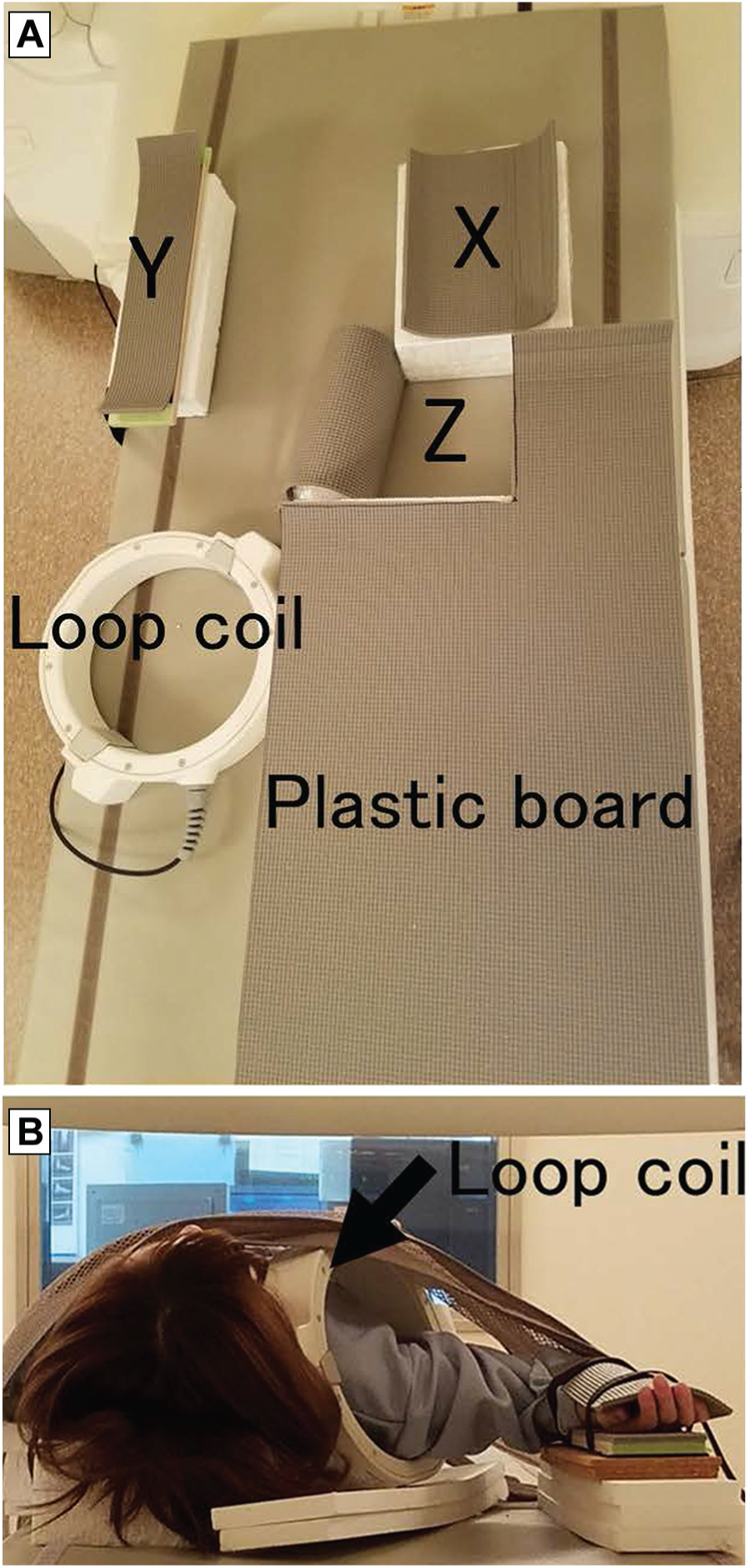
The shoulder positioning during magnetic resonance imaging examination. (A) Scans were taken in the supine position with the arm in maximum horizontal extension, with the arm kept in 90° of abduction and 90° of external rotation. A space was made under the scapula such that it was not compressed. X, head positioner; Y, forearm positioner; Z, space under the scapula. (B) Craniocaudal view.
Step 2: Measurement of the Glenoid Track Width
According to a previous study, the distance from the anterior rim of the glenoid to the medial margin of the footprint was measured and defined as the glenoid track width. 7 The 3D surface bone models of the proximal humerus and the glenoid were reconstructed from the segmented area of MRI scans with image analysis software (Amira, v 6.0; FEI Visualization Sciences Group). The plane approximating the anatomic neck of the humerus was created. The center of the humeral section was created by this plane (Figure 2A, point G). The center on the articular surface of the humeral head (Figure 2A, point C) was defined as an intersection between the articular surface and the line perpendicular to this plane passing through point G (Figure 2A). The anterior and posterior points of the 3D glenoid surface model were identified, as shown in Figure 2B. A superior-inferior line was created connecting the 12- and 6-o’clock positions of the glenoid. Then, the medial-lateral line perpendicular to the superior-inferior line with the maximum width was defined. The anterior and posterior intersections between the glenoid rim and the medial-lateral line were named points A and P, respectively. The length of the line connecting points A and P was measured as the glenoid width. The intersection between the humeral head and the line connecting points A and G was named point M (Figure 2C). Line CM passed through the footprint of the rotator cuff. The distance from point M to the medial margin of the footprint on line CM (point F) was measured as the glenoid tack width (Figure 2D). To assess the reliability of measuring the glenoid track width, 2 examiners (J.K., T.E.) measured the glenoid track width of 10 participants independently, and 1 examiner (J.K.) measured the glenoid track width twice with an interval of 1 hour to calculate intraclass correlation coefficient (ICC).
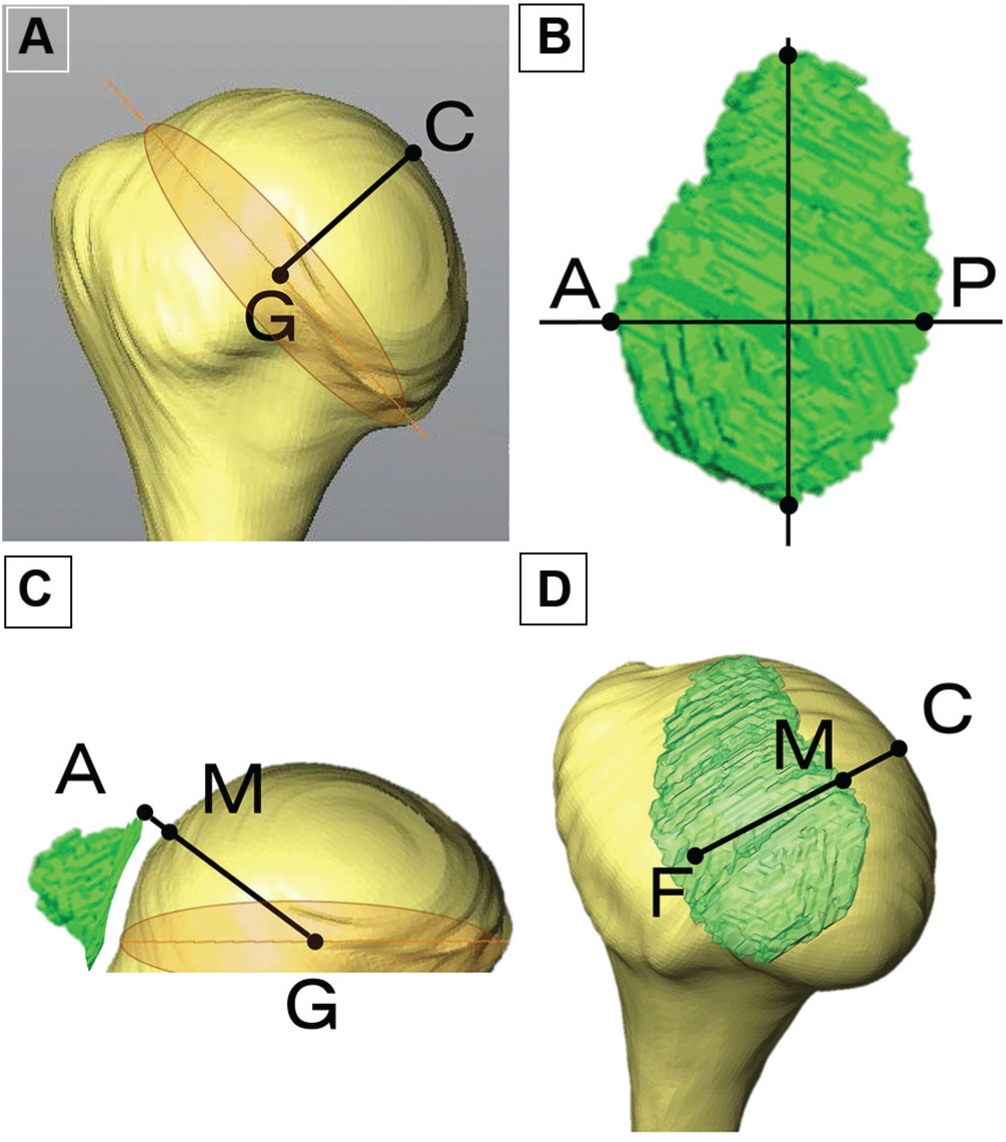
Measurement of the glenoid track width. (A) Definition of point C: the center of the humeral section created by this plane (point G). The center on the articular surface of the humeral head (point C) was defined as an intersection between the articular surface and the line perpendicular to this plane passing through point G. (B) Definition of the anterior and posterior points. A superior-inferior line connecting the 12- and 6-o’clock positions of the glenoid was drawn. Then, the medial-lateral line crossing perpendicular to the superior-inferior line with the maximum width was defined. The anterior and posterior intersections between the glenoid rim and the medial-lateral line were named points A and P, respectively. (C) Definition of the landmarks of the humeral head. The intersection between the humeral head and the line connecting points A and G was named point M. (D) Measurement of the glenoid track width. Line CM passed through the footprint of the rotator cuff. The distance from point M to the medial margin of the footprint on line CM (point F) was measured as the glenoid tack width.
Step 3: Measurement of Shoulder ROM
A single investigator (J.K.) measured shoulder ROM with a goniometer. Active and passive ROM were measured for each participant in the supine and sitting positions without specifically stabilizing the scapula of the participants. The measured shoulder motions were flexion, extension, abduction, internal and external rotations with the arm at 0° and 90° of abduction, and horizontal flexion and horizontal extension with the arm in neutral rotation and 90° of external rotation. In the present study, horizontal extension was defined as extension in the axial plane with the arm in 90° of abduction; and horizontal flexion was defined as flexion in the axial plane with the arm in 90° of abduction. Internal rotation with the arm at 0° of abduction was recorded as the level of the vertebral spine that the thumb could reach. The reliability of our measurements was assessed with use of the ICC in 10 participants by 2 examiners. We measured horizontal extension angle with the arm in 90° of abduction and 90° of external rotation. Measurements were recorded in degrees with a 1° increment. Each measurement was performed twice by 1 examiner (J.K.) and once by another examiner. The interval between the 2 measurements by J.K. was 30 minutes. From these measurements, we calculated the ICCs.
Statistical Analysis
Data were analyzed with JMP Pro 11 Software (SAS Institute). The relationship between the glenoid track width and the range of bilateral shoulder motions was correlated with the Pearson correlation coefficient. Statistical difference was set at P < .05. An ICC was used to assess the intra- and interobserver reliabilities of the measurement of the glenoid track width and shoulder ROM.
Results
Reliability of Measurements
For the measurement of ROM, the intra- and interobserver reliabilities were excellent, with ICCs of 0.978 (95% CI, 0.919-0.919) and 0.947 (95% CI, 0.808-0.987), respectively. Similarly, for the measurement of the glenoid track width, the intra- and interobserver reliabilities were also excellent: 0.988 (95% CI, 0.954-0.997) and 0.988 (95% CI, 0.954-0.997), respectively.
Range of Motion and Glenoid Track Width
Among measured ROMs, active horizontal extension with the arm in 90° of abduction and 90° of external rotation in the sitting position (r = −0.623, P = .0001) and the supine position (r = −0.527, P = .0004) and active abduction in the supine position (r = −0.646, P = .0001) showed significant correlation with the glenoid track width (Tables 1 and 2). The contralateral side showed the same trend. A correlation between the glenoid track width and the range of horizontal extension motion in the sitting position was expressed as the following mathematical formula: Y = −0.49X + 90, where X was the horizontal extension angle (degrees) and Y was the glenoid track width (percentage of glenoid width) (Figure 3). A correlation between the glenoid track width and the range of abduction motion in the supine position was expressed as the following mathematical formula: Y = −0.22X + 117, where X was the abduction angle (degrees) and Y was the glenoid track width (percentage of glenoid width) (Figure 4). Given these formulae, we present tables where we can find a corresponding value of the glenoid track width relative to horizontal extension (Table 3) and to abduction (Table 4).
Data of the Ranges of Shoulder Motion a
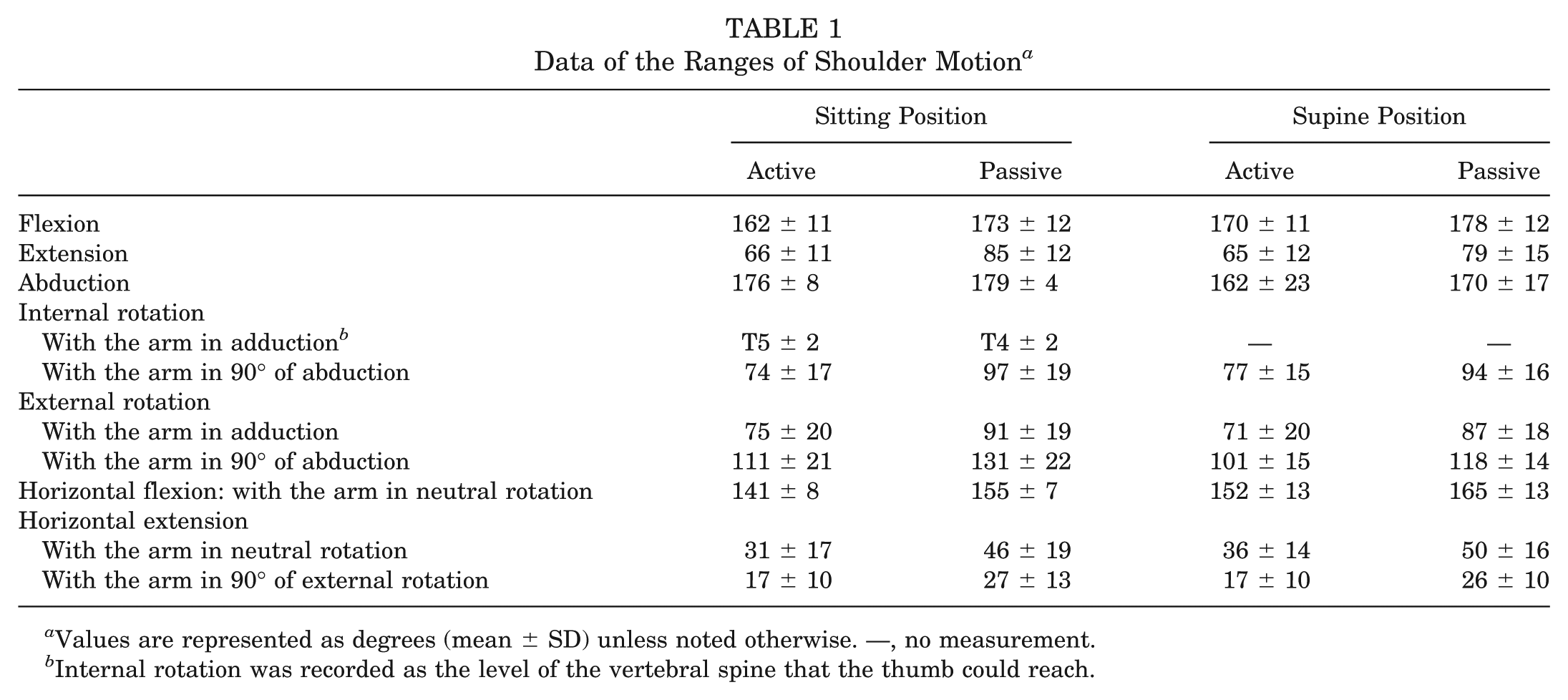
Values are represented as degrees (mean ± SD) unless noted otherwise. —, no measurement.
Internal rotation was recorded as the level of the vertebral spine that the thumb could reach.
Correlation Coefficients Between the Glenoid Track Width and the Ranges of Shoulder Motion a
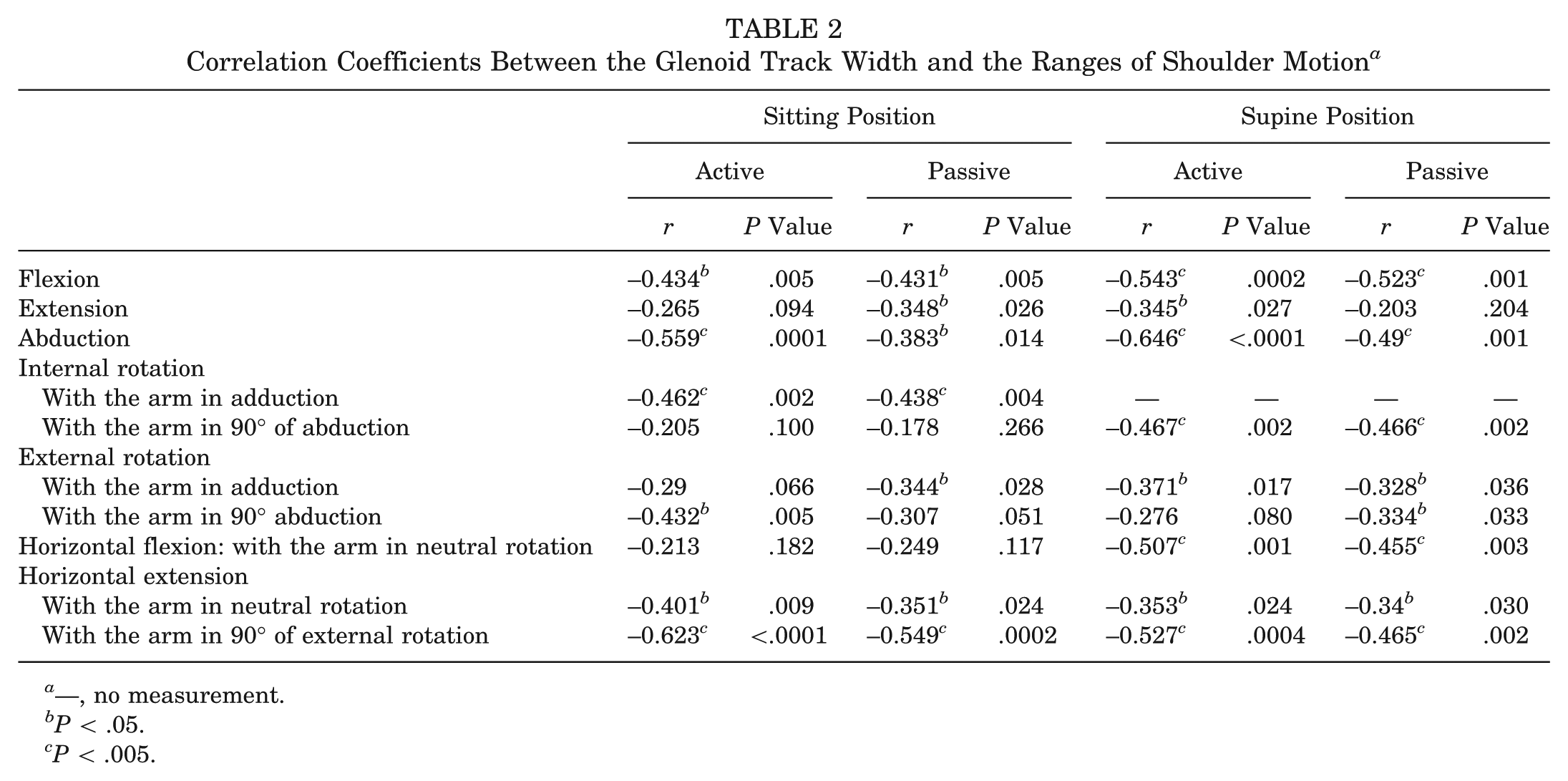
—, no measurement.
P < .05.
P < .005.
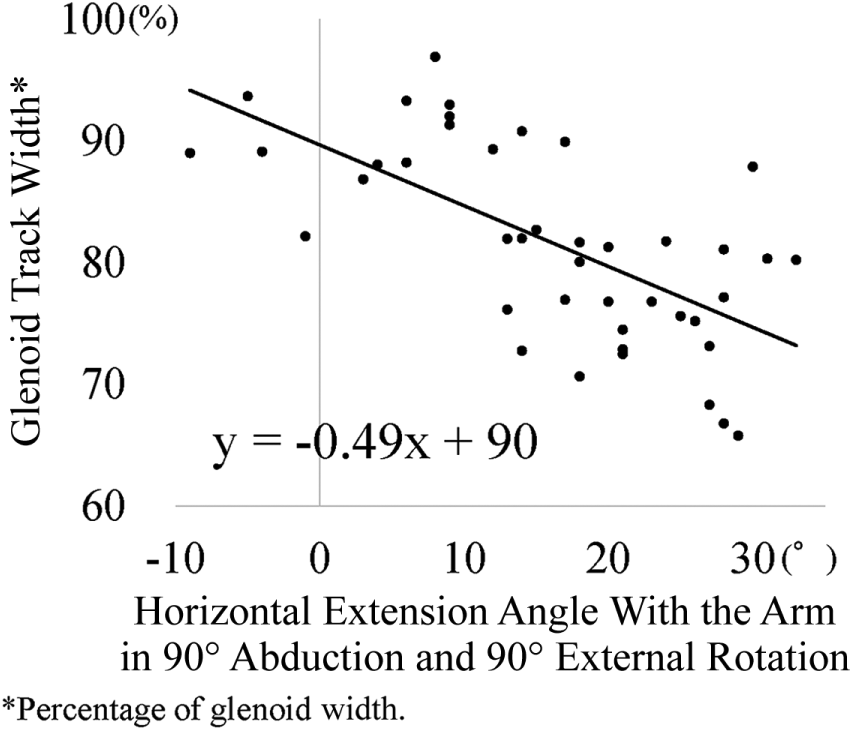
Relationship between the glenoid track width and active horizontal extension with the arm in abduction and external rotation in the sitting position.
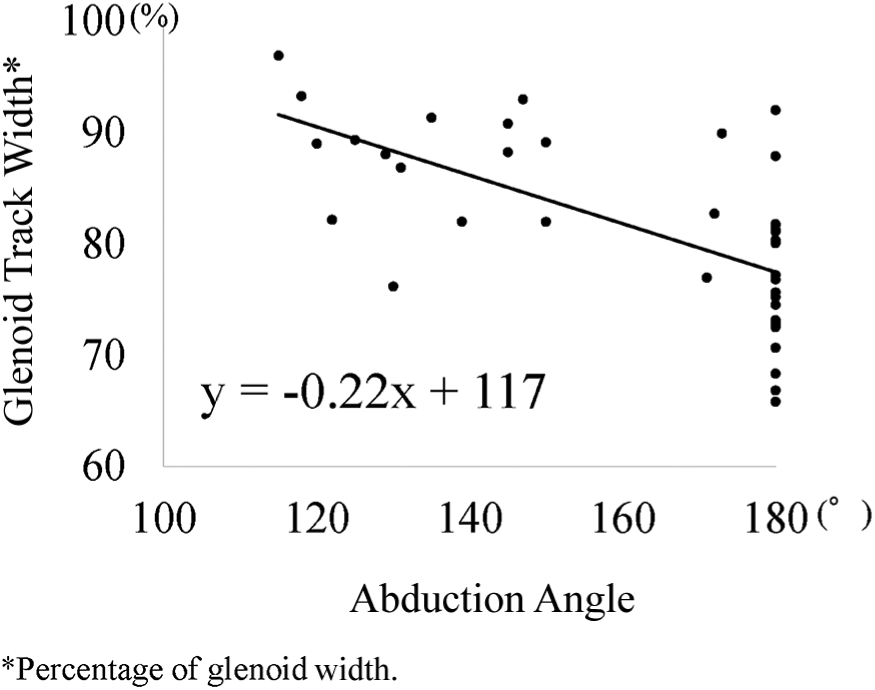
Relationship between the glenoid track width and active abduction in the supine position.
Glenoid Track Width in 5° Increments in Horizontal Extension

Minus value indicates horizontal flexion angle.
Percentage of the glenoid width.
Glenoid Track Width in 10° Increments of Abduction

Percentage of the glenoid width.
Discussion
The intra- and interobserver reliabilities of the measurement of the glenoid track width were excellent in the present study. Among the shoulder ROMs measured, active horizontal extension in the sitting position and active abduction in the supine position correlated moderately with the glenoid track width, with correlation coefficients >0.6. The greater the horizontal extension in the sitting position or the greater the abduction in the supine position, the smaller the glenoid track width. Similar to the previous cadaveric study, 12 the present study proved our hypothesis with healthy volunteers. The question is, which ROM should we use? Horizontal extension or abduction? As shown in Figure 4, more than half the shoulders reached the maximum abduction of 180°. This means if a patient has 180° of abduction, the glenoid track width could be any value between 66% and 92%. This seems to be a great limitation of using the abduction angle. In addition, most physicians usually examine patients with anterior shoulder instability in the sitting or standing position rather than in supine position. These are the reasons why we believe that the horizontal extension angle would be preferable to estimate the individualized value of the glenoid track width.
A correlation between the glenoid track width and the range of horizontal extension motion could be expressed as the following mathematical formula: Y = −0.49X + 90, where X is horizontal extension angle (degrees) and Y is the glenoid track width (percentage of glenoid width). Table 3 was made with this formula, where a corresponding glenoid track width would be easily found once we measured the angle of active horizontal extension in the sitting position. For example, while the glenoid track width is 85% of the glenoid width in a normal shoulder with 10° of horizontal extension, it could be 80% in a lax shoulder with 20° of horizontal extension, or it could be 90% in a stiff shoulder with 0° of horizontal extension.
In practice, we should measure the range of horizontal extension in the uninvolved shoulder, not the involved shoulder, because it may not be possible to measure it on the involved side owing to anterior apprehension. Our data showed that a correlation between the glenoid track width and the range of horizontal extension motion in the involved side was almost the same as that in the uninvolved side.
Theoretically, the glenoid track width is affected by the shoulder joint laxity because the glenoid track is defined as a zone of contact between the glenoid and the humeral head. It would be ideal to take a patient’s joint laxity into consideration with the glenoid track concept. We have used a constant value of 83% of the glenoid width for all patients because we did not know the correlation with the glenoid track width and joint laxity. In the present study, the ranges of shoulder motion were measured to evaluate shoulder joint laxity. Of course, laxity and ROM are different by definition, but laxity can be represented by certain ranges of motions, as shown in the Instability Severity Index Score.8,10 Since ROM was much easier to quantify than joint laxity, in this study we focused on the range of various motions to observe any correlations with the glenoid track width.
There were several limitation in this study. First, we used 3D magnetic resonance for the measurement of the glenoid track width. It was reported that 3D computed tomography (CT) is the best imaging modality to detect glenoid bone loss. 1 However, recent studies showed that 3D magnetic resonance was as accurate as 3D CT with an additional benefit of delineating the margin of the footprint better than 3D CT. 3 Second, 3D surface bone models of the glenoid were created without the labrum. As the labrum is detached from the anterior rim of the glenoid, this method is usually acceptable. However, in cases of a midsubstance tear of the capsule or humeral avulsion of the glenohumeral ligament, the labrum should be taken into consideration during assessment of the off-track lesion. Third, although the glenoid track width correlated with horizontal extension in the sitting position, the correlation coefficient was −0.623: a moderate correlation. Although using this correlation is better than using the fixed value of 83%, it still seems difficult to accurately assess the “true glenoid track width.” Last, our measurement method of range of active horizontal extension motion with use of a goniometer may not be as accurate as other quantitative methods, such as magnetic or gyro sensors. However, using ICCs, we confirmed that our measurement method was sufficiently reliable for our study.
Conclusion
Our data show that the greater the horizontal extension in abduction and external rotation in the sitting position, the smaller the glenoid track width. With this relationship in mind, we should be able to provide a tailor-made treatment for each patient whom we are going to treat.
Footnotes
Acknowledgements
We thank Dr. Takaya Sato for helping us assess the reliability of measuring the range of shoulder motion.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.