
Abstract
Background:
Hip arthroscopy for femoroacetabular impingement syndrome (FAIS) is a rapidly growing field in sports surgery; however, factors associated with poor outcomes and identification of predictor models of inferior clinical outcomes is unclear.
Purpose:
To analyze predictors of clinical failure and inferior clinical outcomes among patients undergoing hip arthroscopy for treatment of FAIS.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Data were collected and analyzed from consecutive patients who underwent primary hip arthroscopy with routine capsular closure for the treatment of FAIS from a single fellowship-trained surgeon between January 2012 and November 2015. Baseline data, postoperative patient-reported outcomes, and rates of clinical failure and inferior clinical outcomes were recorded at 2 years postoperatively. Clinical failure was defined by revision hip arthroscopy or conversion to total hip arthroplasty. Inferior clinical outcome was defined as not reaching the minimal clinically important difference (MCID) or patient acceptable symptomatic state for Hip Outcome Score–Activities of Daily Living. A multivariate logistic regression analysis was used to identify significant predictors of clinical failure and inferior clinical outcome.
Results:
Out of 1161 eligible patients, 935 (80.5%) completed 2-year postoperative patient-reported outcomes. The mean ± SD age and body mass index were 33.3 ± 12.3 years and 25.4 ± 8.2 kg/m2, respectively. The overall clinical failure rate was 3.6% (n = 34), including 23 cases (2.5%) of revision hip arthroscopy and 11 cases (1.2%) of conversion to total hip arthroplasty. Predictors of clinical failure were lower preoperative International Hip Outcome Tool score (P = .016), chronic preoperative pain (P = .001), and chondromalacia in the affected hip (P = .04). The inferior clinical outcome group, consisting of those who failed to reach the MCID for Hip Outcome Score–Activities of Daily Living, included 256 patients (27.4%). Predictors of inferior clinical outcomes were Tönnis grade >1 (P = .01), workers’ compensation (P < .001), and increased body mass index (P = .02).
Conclusion:
This study demonstrates that 73% of all patients treated for symptomatic FAIS with primary hip arthroscopy and routine capsular closure achieved the MCID. Clinical failure is predicted by a number of modifiable and nonmodifiable factors, including chronic preoperative pain and presence of chondromalacia. The current study updates the midterm failure rates and outcomes achievable with hip arthroscopy for FAIS.
Technical advances in hip arthroscopy have led to exponential growth in the treatment of femoroacetabular impingement syndrome (FAIS). 3 While originally treated with open hip surgery, osseous pathomorphology and chondrolabral pathology associated with FAIS is increasingly being treated successfully with hip arthroscopy. 6 Numerous studies reported that surgical correction of FAIS and treatment of chondrolabral injury yield reliable pain relief and improvement in hip function for the majority of patients in the short to midterm.10,11,13,14,31,36,41
Surgical techniques for hip arthroscopy are being increasingly recognized as an important determinant of surgical outcome. Management of the hip capsule during arthroscopic treatment of FAIS has evolved, and capsular plication is increasingly the standard for capsular management.1,10,23,44 Frank et al 10 demonstrated improved clinical outcomes with a lower revision rate when complete capsular closure was performed after hip arthroscopy for the treatment of FAIS. Similarly, Wylie et al 44 reported improvements in all patient-reported outcomes after revision hip arthroscopy and capsular closure among 33 previously symptomatic patients after index hip arthroscopy for FAIS correction in which capsular closure was not performed. Such prior studies highlight that previously published studies on hip arthroscopy survivorship may have been confounded by variable techniques for capsular management. Given the current understanding for the role of capsular management in hip arthroscopy, there is a need for a study that evaluates the medium-term outcomes and predictors of clinical failure for hip arthroscopy performed with capsulotomy followed by capsular plication.
The primary purpose of the current study was (1) to investigate the factors associated with clinical failure (defined by requiring revision arthroscopy or conversion to total hip replacement) after hip arthroscopy with capsular plication and (2) to identify factors associated with achieving a clinically significant outcome with this technique, defined as reaching the minimal clinically important difference (MCID) or patient acceptable symptomatic state for the Hip Outcome Score–Activities of Daily Living (HOS-ADL). We hypothesized that the use of modern surgical techniques would result in a lower clinical failure rate (previously reported figures of 5%-15%) and that the majority of patients would achieve clinically significant outcomes at medium-term follow-up.
Methods
Patient Selection
This study was approved by the institutional review board of the senior author’s (S.J.N.) institution (12022108-IRB01), and no funding was received. Prospective data on all patients who underwent hip arthroscopy for the treatment of FAIS by a single fellowship-trained surgeon (S.J.N.) were collected and analyzed in a clinical repository. All patients undergoing primary hip arthroscopy for the treatment of FAIS between January 1, 2012 (the initiation of the repository), and January 1, 2016, were included in this study. Inclusion criteria consisted of clinical and radiographic diagnosis of symptomatic FAIS, failure of nonoperative management (physical therapy, activity modification, oral nonsteroidal anti-inflammatory drugs, and, for some patients, fluoroscopically guided intra-articular cortisone injection), and hip arthroscopy to address FAIS, with a minimum of 2-year follow-up. Exclusion criteria included a history of ipsilateral or contralateral hip surgery, advanced osteoarthritis, reduced joint space (Tönnis grade >1), evidence of congenital hip disorders (slipped capital femoral epiphysis, developmental dysplasia of the hip [lateral center-edge angle <20°], and Perthes disease), and hip arthroscopy for an indication other than FAIS.
Surgical Technique
Patients underwent hip arthroscopy for the treatment of FAIS in the supine position as previously described.10,15,38 Diagnostic arthroscopy was performed, and labral tears were repaired when there was gross detachment from the acetabular rim. The peripheral compartment was then addressed with osteochondroplasty for cam lesions. A T-capsulotomy composed of transverse interportal capsulotomy with a vertical limb was utilized for visualization in all cases. As part of routine closure, the vertical limb was closed via plication, while the interportal limb was closed by approximating the medial and lateral edges of the interportal capsulotomy. All patients followed a standard rehabilitation protocol previously described. 22 Furthermore, all patients were instructed to take prophylactic nonsteroidal anti-inflammatory drugs postoperatively for the prevention of heterotopic ossification.
Radiographic Analysis
All patients had a series of preoperative and final follow-up radiographs. 42 Each series consisted of a standing anteroposterior pelvis radiograph, an anteroposterior hip radiograph, a false-profile hip radiograph, and a Dunn lateral hip radiograph. 8 The joint space width was measured in 3 positions on the anteroposterior hip radiograph, as was the acetabular inclination (Tönnis angle), femoral neck-shaft angle, crossover sign, and lateral center-edge angle of Wiberg.8,21 Alpha angle was measured on the Dunn lateral view of the hip. 29 The Tönnis grade was determined.21,40
Functional Outcome Evaluation
Preoperatively, the following data were collected from all patients: sex, age, operative extremity, body mass index (BMI), sports participation, acute versus insidious onset, duration of symptoms, and comorbidities. All patients completed preoperative and minimum 2-year postoperative hip-specific patient-reported outcome instruments, including the HOS-ADL 27 and the modified Harris Hip Score (mHHS).4,16 In addition, all patients graded their postoperative pain and satisfaction levels with a paper-based visual analog scale (0-10 cm). Patients were examined preoperatively and at final follow-up by a physician assistant (an independent examiner) for measures of hip flexion, hip internal rotation at 90° of flexion, and hip external rotation at 90° of flexion with visual estimation.
Determination of Clinical Failure and Inferior Outcomes
All complications were tracked throughout the study period. Clinical failure was defined according to previous literature standards as the need for ipsilateral revision hip arthroscopy or conversion to total hip arthroplasty (THA).7,14,24,28,32,33,35 During the study period, all revision procedures, performed by the senior surgeon or elsewhere, were tabulated to calculate a rate of revision surgery. Inferior clinical outcome was defined as failing to reach the MCID for the HOS-ADL at 2 years postoperatively. As described in the literature, the MCID was determined by calculating the half SD of the HOS-ADL mean of the study patients.20,25,30 The MCID was calculated to be 9.84. We sought to define clinical failure and inferior outcome, as both endpoints pose significant challenges to patients that can be difficult to treat.
Statistical Analysis
All data were screened to determine if they met all parametric statistical assumptions before analysis. Two binary logistic regression models were created: one for inferior clinical outcome (those who did not achieve the MCID) and another for clinical failure (required revision or conversion to THA). The process of creating the models is summarized in Figure 1. Pearson and Spearman coefficient analysis was carried out to identify correlations between (1) the MCID and clinical failures and (2) pre-, intra-, and postoperative variables to identify variables to fit in the exploratory analysis for the final logistic models. An exploratory factor analysis was performed on the variables with statistically significant correlations to the primary outcomes (MCID and THA/revisions) through a principal component (PC) extraction (ie, eigenvector decomposition) with a varimax rotation to reduce the redundancy in the predictor variables. The Kaiser-Meyer-Olkin test was used to determine if the predictor variables demonstrated adequate correlation for an exploratory factor analysis. A Kaiser-Meyer-Olkin value of 0.7 was found, which demonstrates that the data were appropriate for factor analysis, as this value exceeded a recommended value of 0.6 for exploratory factor analysis. 39 A scree plot was examined to determine the number of PCs to retain for analysis of the 2 separate models. Each extracted PC was used to calculate the percentage variance explained by dividing the eigenvalue of each PC by the sum of all eigenvalues. The contribution of each variable to the PC was determined with the factor loadings of each variable. Variables that demonstrated a factor loading greater than ±0.25 for a PC was retained as a predictor variable for the follow-up binary logistic regression analysis used to create both models. If the loading components in the analysis had >1 variable less than ±0.25, each variable in the component was placed into the model independently. A receiver operating characteristic (ROC) curve analysis was then used to identify the model with the best fit and, therefore, the variable with the best fit for the model. The final models for inferior clinical outcome and clinical failure were chosen per the highest area under the curve (AUC) in the ROC curve analysis.
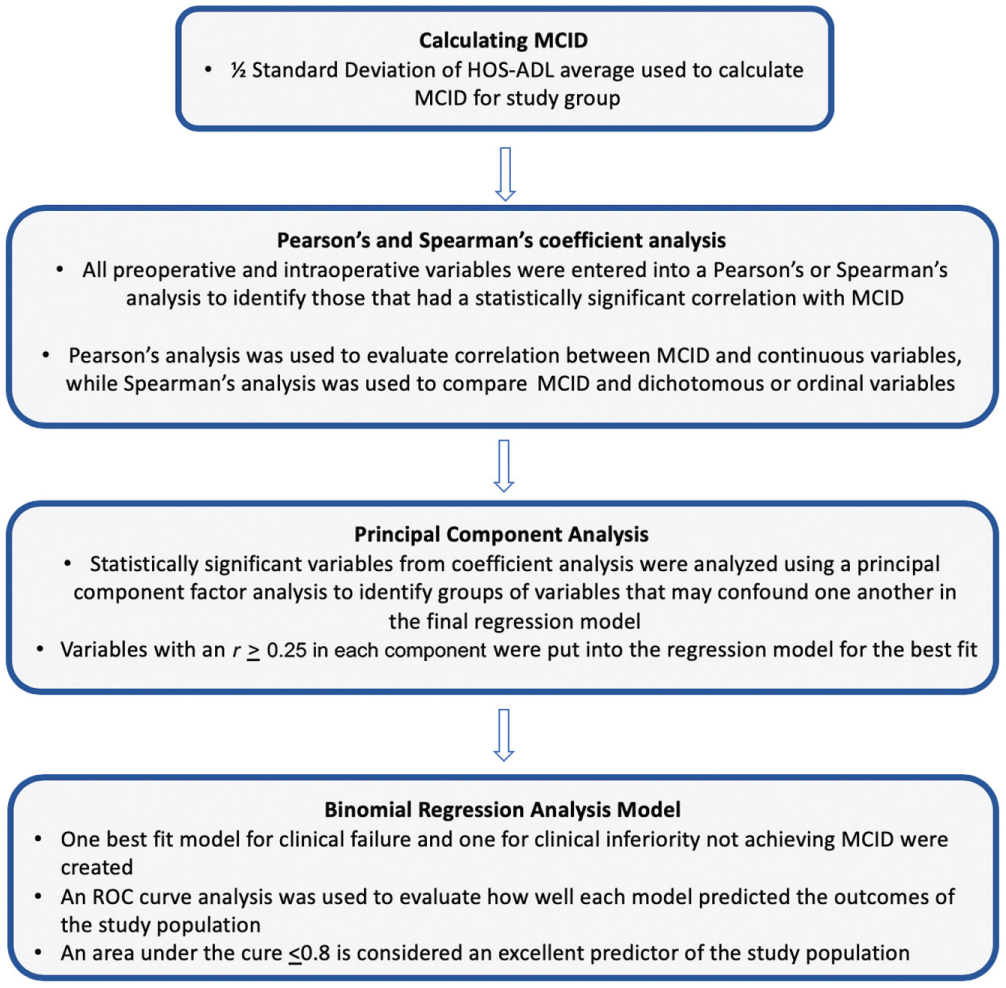
Statistical analysis flowchart. HOS-ADL, Hip Outcome Score–Activities of Daily Living; MCID, minimal clinically important difference; ROC, receiver operating characteristic.
Descriptive statistics for all continuous variables are reported as means and SDs, and frequency statistics were reported for all noncontinuous variables. Paired-samples t tests were used to compare preoperative and 2-year postoperative patient-reported outcome scores of patients with FAIS. Statistical significance for all analysis was set at α ≤ .05.
Results
From a total of 1336 hip arthroscopy procedures performed within the study period, 1161 patients were eligible and available for follow-up, with 935 (80.5%) completing patient-reported outcome surveys at a minimum of 2 years postoperatively (Figure 2). Table 1 presents patient characteristics, radiographic parameters, and FAIS-pertinent physical findings. The patient population had a mean ± SD age of 33.3 ± 12.3 years and a BMI of 25.4 ± 8.2 kg/m2. The majority of the patient study group was healthy, with 77.2% reporting being physically active and 48.4% running for sport. In sum, 918 (98.2%) of patients underwent labral repair, while 17 (1.8%) underwent labral debridement.
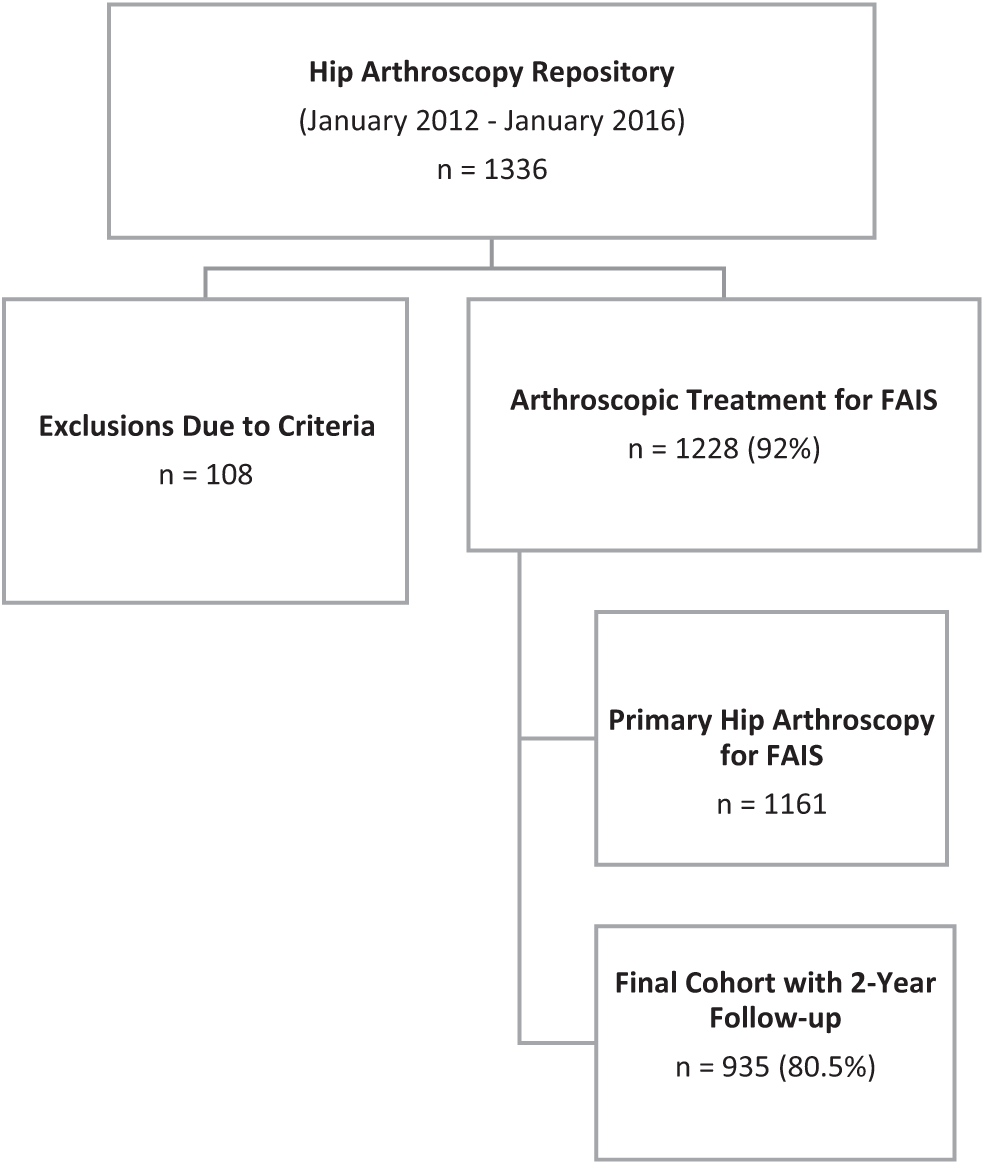
CONSORT (Consolidated Standards of Reporting Trials) flowchart of final cohort selection. FAIS, femoroacetabular impingement syndrome.
Patient Characteristics, Radiographic Parameters, and Physical Examination (N = 935) a
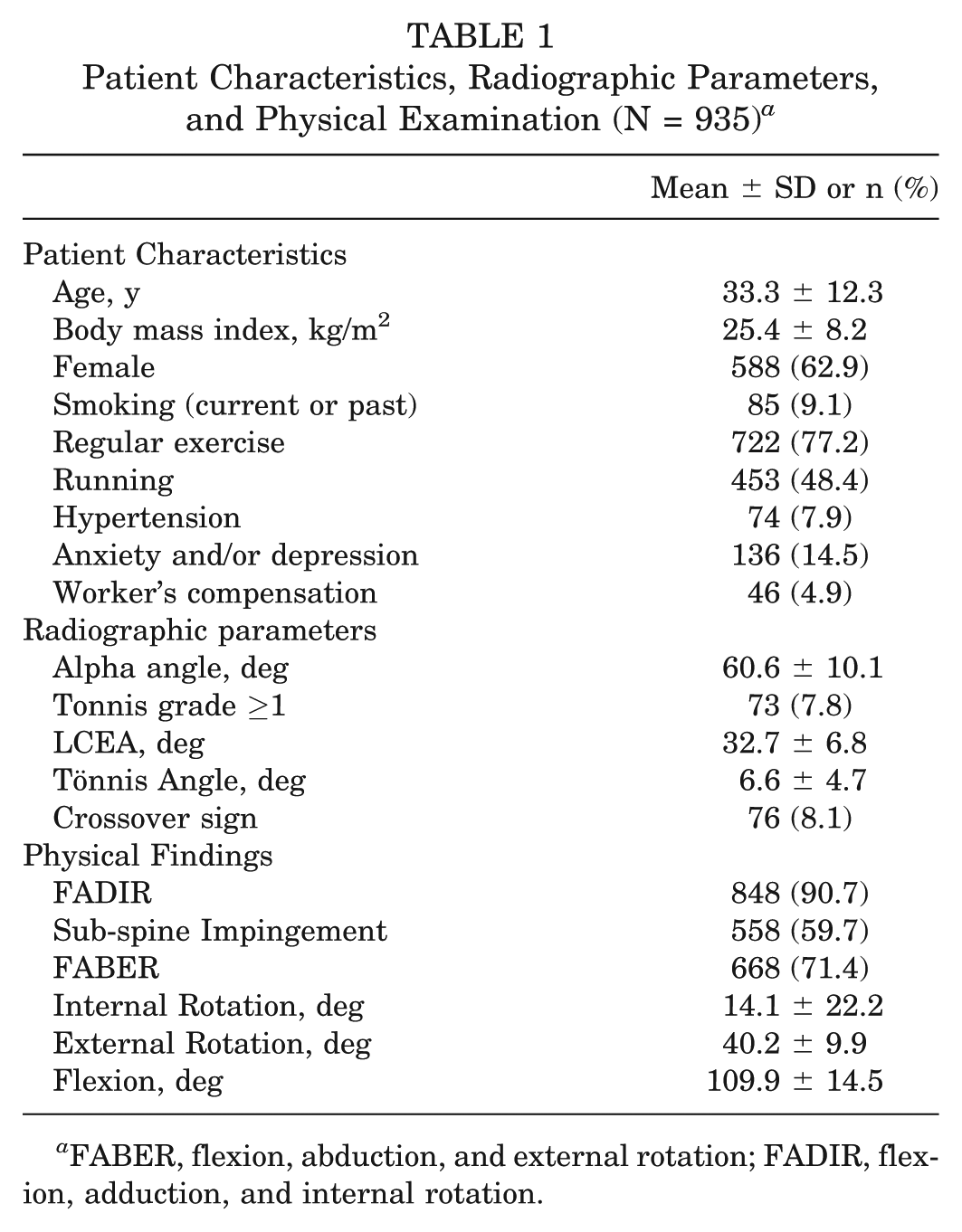
FABER, flexion, abduction, and external rotation; FADIR, flexion, adduction, and internal rotation.
Distribution of Outcome Scores
Independent t tests were used to compare mean scores for patients who did and did not have clinical failure (Table 2). Interestingly, there was a statistically significant difference in preoperative International Hip Outcome Tool (iHOT-12) score, being higher among patients with clinically significant outcome improvement versus those without (36.8 vs 27.3, respectively; P = .016). All postoperative patient-reported outcomes were higher among patients achieving clinically significant outcome improvement as compared those not achieving this improvement.
Comparison of Patient-Reported Outcomes in Clinical vs Nonclinical Failure a
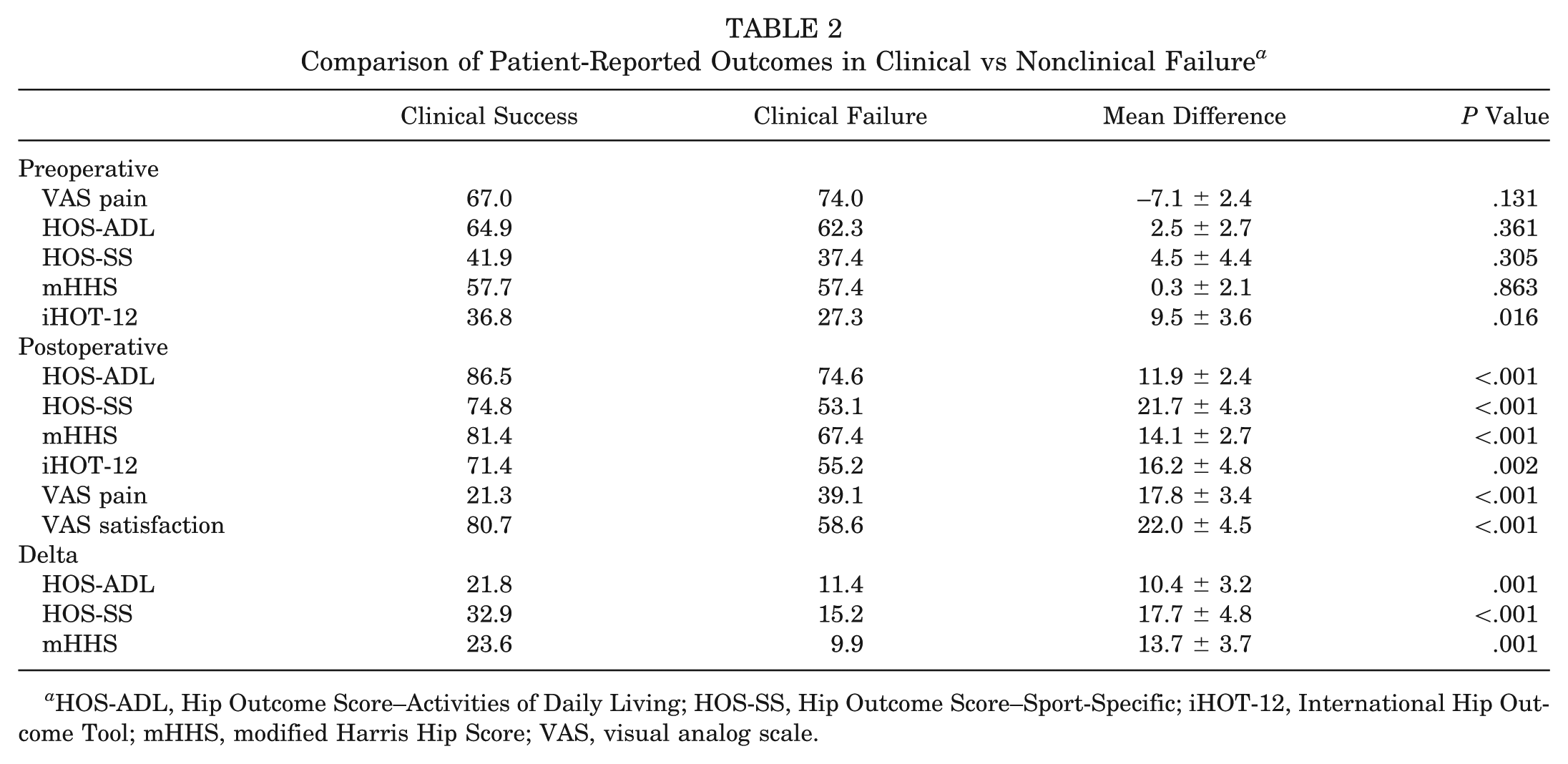
HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sport-Specific; iHOT-12, International Hip Outcome Tool; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Overall, 72.6% (n = 679) of the combined study population achieved the MCID (Table 3). Chi-square analysis of individuals achieving the MCID for the HOS-ADL demonstrated a statistically significant difference between patients with clinical success and those with clinical failures (P = .042). Only 59.5% (n = 22) of patients who had clinical failures achieved the MCID for the HOS-ADL, while 73.7% (n = 660) with clinical success achieved it.
Analysis of Achieving the MCID for the HOS-ADL a
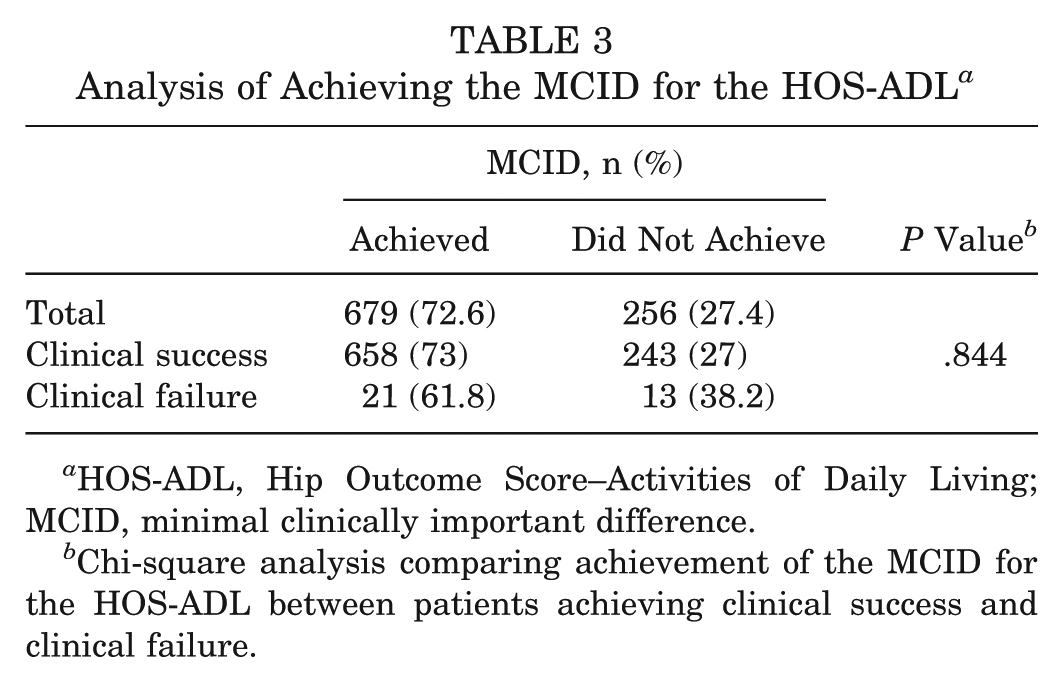
HOS-ADL, Hip Outcome Score–Activities of Daily Living; MCID, minimal clinically important difference.
Chi-square analysis comparing achievement of the MCID for the HOS-ADL between patients achieving clinical success and clinical failure.
Factors Associated With Clinical Failure
By final follow-up, 11 patients (1.2%) went on to THA because of recurrent symptoms and joint space loss. An additional 23 patients (2.5%) underwent revision hip arthroscopy: 2 for lysis of adhesions, 5 for excision of heterotopic ossification, 7 for residual FAIS femoral morphology (1 in combination with capsular insufficiency), and 9 for capsular insufficiency. Factor analysis consisted of 9 PCs that explained 60% of the variance of the predictor variables. For the rotated factor analysis, see Appendix 1 (available in the online version of this article). The variables retained for analysis were based on the PC loadings. The logistic regression model of the variables is reported in Table 4. Briefly, a lower preoperative iHOT-12 score, chronic preoperative pain (odds ratio [OR], 4.81; P = .001), and the presence of chondromalacia (OR, 1.59; P = .042) were the statistically significant variables from the factor analysis, while providing a model that had an excellent fit based on ROC curve analysis (AUC = 0.845) (Appendix 1, available online).
Binomial Logistic Regression Model for Clinical Failure: Total Hip Arthroplasty or Arthroscopy Revision a
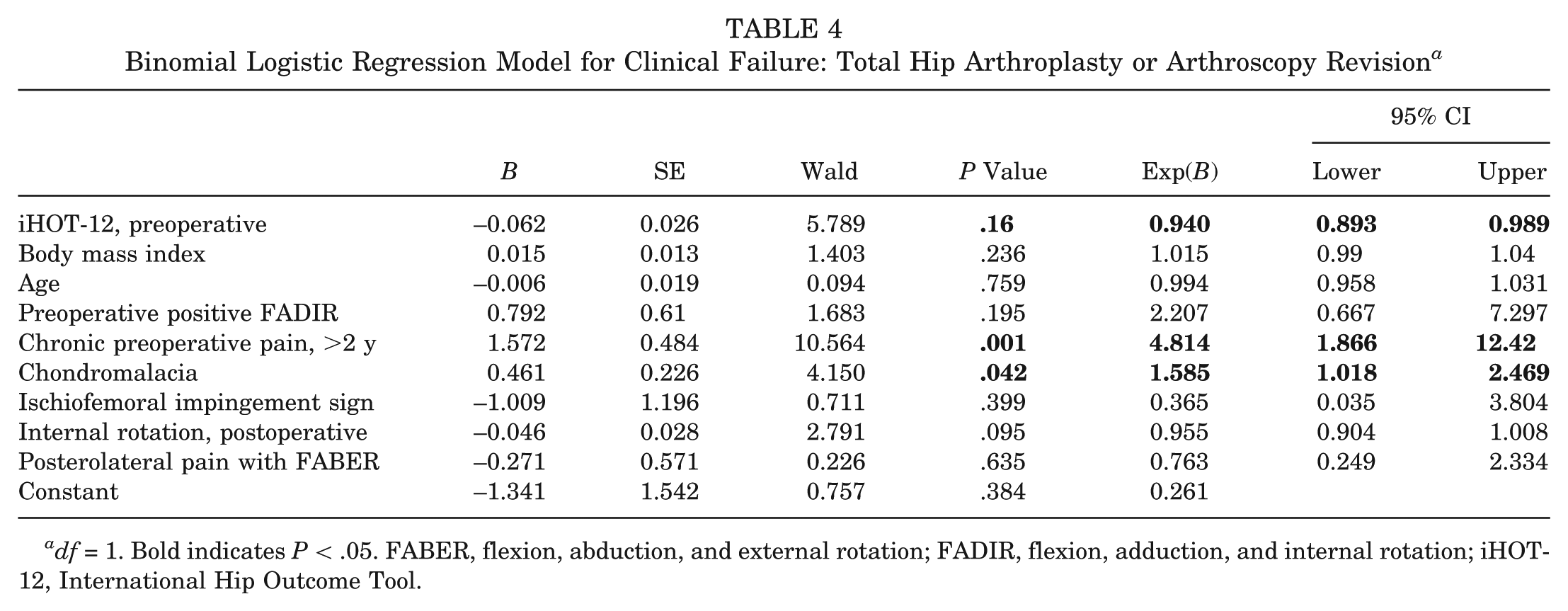
df = 1. Bold indicates P < .05. FABER, flexion, abduction, and external rotation; FADIR, flexion, adduction, and internal rotation; iHOT-12, International Hip Outcome Tool.
Factors Associated With Inferior Clinical Outcomes
The factor analysis for inferior clinical outcomes consisted of 8 PCs that explained 64% of the variance of the predictor variables. For the rotated factor analysis, see Appendix 2 (available online). The variables retained for analysis were based on the PC loadings (Table 5). Briefly, Tönnis grade (OR, 2.798; P = .01), workers’ compensation (OR, 1.2; P < .001), and BMI (OR, 1.065; P = .02) were all predictors of not achieving the MCID for the HOS-ADL, while providing a model that had an excellent fit based on ROC curve analysis (AUC = .796) (Appendix 2, available online).
Binomial Regression Model for Inferior Outcome: Did Not Reach MCID for the HOS-ADL a
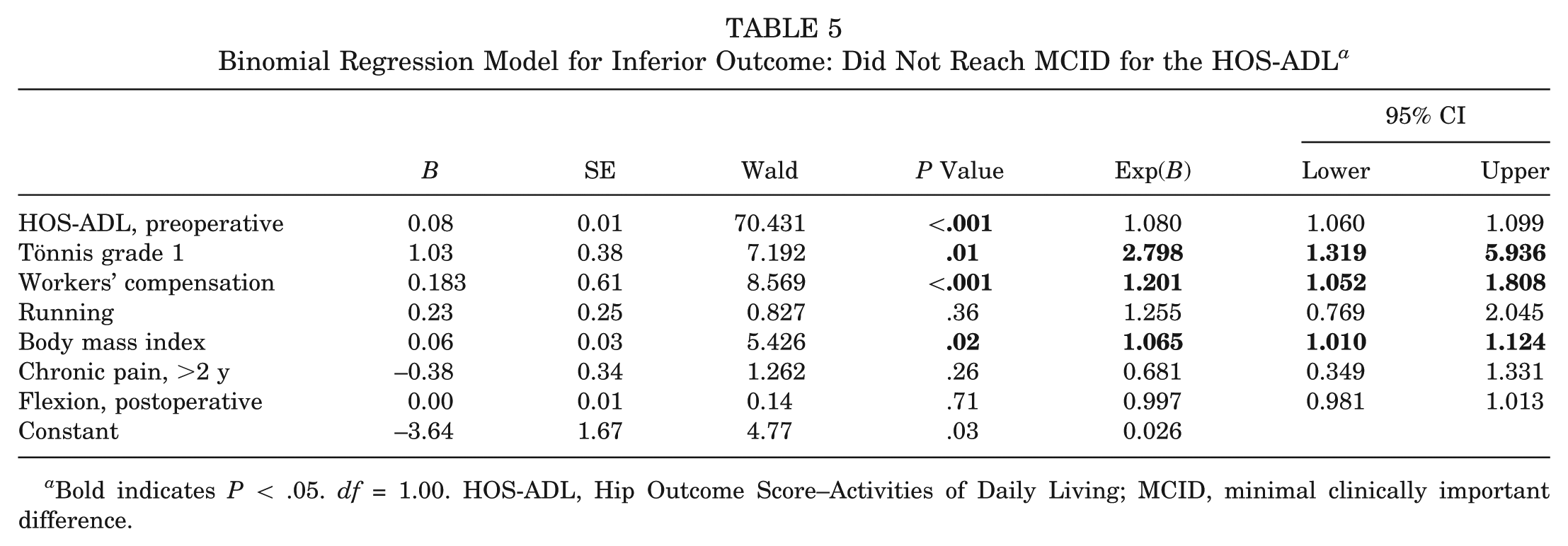
Bold indicates P < .05. df = 1.00. HOS-ADL, Hip Outcome Score–Activities of Daily Living; MCID, minimal clinically important difference.
Discussion
In this study, survivorship and clinically significant outcome were evaluated for patients undergoing hip arthroscopy for FAIS with modern techniques for capsular management. We found that the survivorship within the study patient population was higher than that in previously published series.2,5,12,19,35 The combined revision–conversion to THA rate was 3.6%, and factor analysis demonstrated that chronic preoperative pain and evidence of chondromalacia were predictive of clinical failure. Additionally, we found that the majority of patients achieved clinically significant outcomes. Patients with Tönnis grade ≥1, workers’ compensation, and higher BMI were less likely, however, to achieve clinically significant outcomes.
Understanding the reason for inferior outcomes and clinical failure helps to refine the indications for arthroscopic treatment of FAIS, to assist in shared decision making, and to set appropriate expectations. Clinical failure of primary hip arthroscopy was previously defined as revision hip arthroscopy26,33,35 or conversion to THA.14,18,28,32,37 Previous studies investigating the revision and conversion rates after primary hip arthroscopy for the treatment of FAIS documented rates between 1% and 50%.14,19,26,28,33 In the most complete systematic review of the literature, including >6000 patients in 90 clinical studies, Harris et al 14 found that the reoperation rate was 6.3% at a mean 16 months and that conversion to THA was the most common (2.9%) operation after hip arthroscopy. A strength of the current study is the consecutive nature of the prospective series. At a mean follow-up of 2.32 years, a 2.5% revision rate and a 1.2% conversion rate were observed.
The previously reported patient- and imaging-related factors associated with inferior outcomes and clinical failure are older patient age and preoperative osteoarthritis in the form of joint space loss or Tönnis grade.14,28,31,32,37 Malviya et al 26 recently reported on the National Health Service Database for all hip arthroscopy cases performed in England and found that age was a significant predictor of conversion to THA; however, as with many national database studies, their study was unable to account for confounding variables, such as preoperative joint space or Tönnis grade, in their logistic regression model. The current study demonstrated that Tönnis grade is a predictor of not achieving MCID but not of clinical failure. One possible reason that this study did not find Tönnis grade predictive of clinical failure is due to the younger age of our patient population (33.3 ± 12.3 years) versus the older population seen in other studies. 34 Furthermore, in our practice, the general exclusion criterion for undergoing surgery is Tönnis grade >1. This is interesting, as patients with a Tönnis grade ≥1 in our study were almost 3 times more likely to have inferior clinical outcomes versus patients with a Tönnis grade of 0.
One explanation for the low rates of revision and conversion to THA in the current study as compared with prior studies is the routine complete closure of the hip capsule at the conclusion of the arthroscopic procedure. As such, we had a low incidence of capsular insufficiency and hip microinstablity in our data set. Mounting biomechanical evidence suggests that capsulotomies lead to microinstability of the hip joint and that capsular repair restores the stability profile more closely to the intact hip.1,23 The biomechanical evidence has been corroborated in recent clinical studies. Frank et al 10 demonstrated that complete repair led to improved outcomes and decreased revision surgery rates as compared with partial capsular repair. Wylie et al 44 demonstrated 2-year improvements in patient-reported outcomes after revision hip arthroscopy with capsular repair in a population previously symptomatic from microinstability after primary hip arthroscopy with capsulotomy without subsequent capsular repair. In following with these prior reports, the current consecutive series of primary hip arthroscopies for the treatment of FAIS had a 100% rate of complete capsular closure. As stated previously, this study’s revision rate and conversion rate are 2.6% and 1.2%, respectively. In contrast, the aforementioned recent study by Chandrasekaran et al 7 —with a comparable patient population, a comparable surgical technique (aside from capsular management), and a comparable follow-up—had rates of revision and conversion to THA of 6.8% and 10.8%, respectively. The capsular repair rate in that study was 17.6%, and it is possible that this markedly lower capsular repair rate may contribute to the differences in revision rate and survivorship.
A previously unreported predictor of clinical failure after primary hip arthroscopy for the treatment of FAIS is the lack of preoperative athletic activity as defined by patient intake questionnaire. This study found that preoperative athletic activity in the form of recreational sports or higher-level athletics was possibly protective against revision surgery or conversion to THA. Another explanation for the association with athletic activity and hip functional outcome is the type of patient undergoing hip arthroscopy. Not all patients with hip pain or dysfunction are athletic, and some patients may prioritize pain relief, improvement in activities of daily living, or participation in athletic activities. While physical activity was not a direct predictor of clinical success, this study demonstrated that BMI was a predictor of clinical outcomes. This confirms the observation of Westermann et al 43 that BMI was an independent predictor of postoperative pain and hip function.
Limitations
The current study has several limitations that should be addressed. First, the predictive models for inferior clinical outcomes and clinical failures demonstrated an excellent fit based on the ROC curve analysis; however, it is possible that better models exist. A number of models were analyzed with the variables in the factor analysis, although confounders and other nonlinear associations possibly exist between the primary outcomes and variables not tested. Second, despite the consecutive nature and complete follow-up, the results are those of 1 high-volume, fellowship-trained hip arthroscopist. Hip arthroscopy has a well-documented and steep learning curve9,17; thus, the results of the current study should be extrapolated cautiously. Third, there is no current gold standard for defining an inferior outcome or clinical failure. Ideally, it would be defined for each patient after measurement and application of individual patient preferences in a transparent and formal shared decision-making framework. Future directions must include developing technology and approaches to efficiently communicate predicted individual patient outcomes to allow for personalized shared decision making. Last, we were not able to account for all patients lost to follow-up in our analysis, and it is possible that some patients may have undergone revision surgery or conversions to THA at other institutions. However, to the best of our knowledge, all required revisions were performed by the senior author, and we were notified of all patients undergoing conversion to THA.
Conclusion
This study demonstrates that 73% of all patients treated for symptomatic FAIS with primary hip arthroscopy and routine capsular closure achieved the MCID. Clinical failure is predicted by a number of modifiable and nonmodifiable factors, including chronic preoperative pain and the presence of chondromalacia. The current study updates the midterm failure rates and outcomes achievable with hip arthroscopy for FAIS.
Footnotes
Presented at the annual meeting of the AOSSM, Boston, Massachusetts, July 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.N. has received research support from Allosource, Arthrex Inc, Athletico, DJ Orthopaedics, Linvatec, Miomed, Smith & Nephew, and Stryker; consulting fees from Ossur and Stryker; and intellectual property royalties from Ossur. J.D.H. has received research support from DePuy and Smith & Nephew and consulting fees from NIA Magellan, Ossur, and Smith & Nephew and is a paid presenter or speaker from Ossur and Smith & Nephew. R.C.M. has received consulting fees from KNG Health Consulting and Stryker and research support from Zimmer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.