
Abstract
Background:
Mesenchymal stem cells (MSCs) can be isolated from various tissues and can present themselves as a promising cell source for cell-based therapies. Although adipose- and bone marrow–derived mesenchymal stem cells have already been used in a considerable number of clinical trials for osteoarthritis treatment, systematic analyses from single- to bulk-cell resolution as well as clinical outcomes of these 2 MSCs are still insufficient.
Purpose:
To explore the characteristics and differences of adipose-derived stem cells (ADSCs) and bone marrow MSCs (BMSCs) at single- and bulk-cell levels, to study the clinical outcomes of these 2 cells on the treatment of osteoarthritis, and to provide potential guidance on the more precise clinical application of these MSCs.
Study Design:
Controlled laboratory study and meta-analysis.
Methods:
Same donor–derived ADSCs and BMSCs were isolated and cultured. Single- and bulk-cell assays were used to identify the characteristics of these 2 cells. Meta-analysis of clinical trials was done to compare the clinical therapeutic effects in osteoarthritis treatment with ADSCs and BMSCs.
Results:
Single-cell RNA sequencing analysis showed that the population of ADSCs showed lower transcriptomic heterogeneity when compared with BMSCs. Additionally, as compared with BMSCs, ADSCs were less dependent on mitochondrial respiration for energy production. Furthermore, ADSCs had a lower expression level of human leukocyte antigen class I antigen and higher immunosuppression capacity when compared with the BMSC population. Meta-analysis of current clinical trials of osteoarthritis treatment with MSCs consistently showed that ADSCs are more stable than BMSCs in their therapeutic effect.
Conclusion:
These results provide basic biological insights into human ADSCs and BMSCs at the single-cell resolution. Findings indicated that ADSCs may be a more controllable stem cell source, may be more adaptable to surviving in the hypoxic articular cavity niche, and may exhibit superiority in regulating inflammation. Based on the meta-analysis results of the different characteristics of ADSCs and BMSCs, ADSCs were implicated as being a better cell source for osteoarthritis treatment.
Clinical Relevance:
These results guide a more precise clinical application of adipose and bone marrow mesenchymal stem cells.
Keywords
Cell therapies utilizing mesenchymal stem cells (MSCs) are being explored in a large number of clinical trials targeting a variety of diseases, such as osteoarthritis, cardiovascular diseases, and diabetes. MSCs were originally isolated from human bone marrow aspirates, 6 and a variety of connective tissues contain MSCs, such as umbilical cord blood, 19 white adipose tissue, 59 and skin. 47 A range of methods have been used to produce MSCs; however, no standard MSC preparation protocol has been developed in the absence of supporting clinical data.32,35 In the United States, it is only required that MSCs for clinical application be produced according to good manufacturing practice and have an approved investigational new drug application from the Food and Drug Administration. According to the definition given by the International Society for Cellular Therapy, 16 MSCs should meet the following criteria: (1) the ability to adhere to plastic under standard culture conditions; (2) positive expression of CD105, CD73, and CD90; (3) negative expression of CD45, CD34, CD14 or CD11b, CD79a or CD19, and human leukocyte antigen (HLA)–DR surface molecules; and (4) the capability to differentiate into the osteogenic, chondrogenic, and adipogenic lineages in vitro.
Evidence suggests that MSCs isolated from different tissues are not identical 25 even though they all meet the minimal criteria for defining MSCs. 16 Transcriptome patterns and in vivo differentiation potential of different isolates can also vary considerably. 44 Regardless of their potentially different behaviors, different kinds of MSCs are currently being used to treat the same diseases in animal studies and clinical trials.
Bone marrow MSCs (BMSCs) and adipose-derived stem cells (ADSCs) are the most frequently used MSCs in clinical trials because of their relative accessibility and widespread ethical acceptability. However, a series of comparative studies have demonstrated differences between ADSCs and BMSCs,9,15,21 and it is not clear how these influence clinical outcomes. Systematic evaluation of the relative therapeutic effects of ADSCs and BMSCs in treatments of the same conditions is required. Nevertheless, MSCs derived from the same tissue also showed different characteristics, 30 thus indicating the heterogeneity and possible instability of MSCs. Bulk cell–based analyses do not permit characterization of cell subpopulations, and it remains unclear how ADSCs and BMSCs differ at the single-cell level.
Single-cell RNA sequencing (scRNA-seq) has recently become a powerful method to investigate cell types in complex tissues and cellular heterogeneity under diverse conditions. By profiling the gene expression pattern of individual cells, scRNA-seq can provide a much higher-resolution view of cellular transcription as compared with pooled-cell RNA sequencing. scRNA-seq can assay heterogeneity in MSCs and provide a higher-resolution view of differences between ADSCs and BMSCs.
Here, we performed scRNA-seq on ADSCs and BMSCs derived from the same donor to achieve high-resolution comparative profiling of gene expression in these cells, followed by a literature search and meta-analysis of published studies on the therapeutic effect of ADSCs and BMSCs in the treatment of osteoarthritis. Our study indicates that a careful choice of MSCs is required for optimum treatment of specific conditions to achieve better therapeutic effects and clinical outcomes.
Methods
For full methods, see the Appendix (available in the online version of this article).
Human MSCs
Human MSCs were obtained from the subcutaneous fat and bone marrow of patients undergoing a specific surgical procedure. In this study, we used the direct plating method to isolate BMSCs and the enzyme digestion method to isolate ADSCs, both as previously described. 43
scRNA-seq
For the initial scRNA-seq experiments (Fluidigm C1), single-donor derived ADSCs and BMSCs of passage 3 were harvested and loaded onto a 17- to 25-μm RNA-sequencing microfluidic integrated fluidic circuit. cDNA libraries were prepared on the Fluidigm C1 system with the SMARTer Ultra Low RNA Kit (Clontech). The qualified library was then sequenced on the Illumina Hiseq 2500 platform.
The second scRNA-seq experiment was performed with the Chromium Single Cell Gene Expression Solution (10x Genomics). ADSCs and BMSCs of passage 3 derived from 3 patients were harvested, and scRNA-seq libraries were obtained following the 10x Genomics recommended protocol, with the reagents included in the Chromium Single Cell 3′ v 2 Reagent Kit. Libraries were sequenced on the HiSeq X Ten (Illumina) instrument.
Metabolic Analyses
Metabolic analysis of MSCs was performed in the Seahorse XF96 extracellular flux analyzer (Seahorse Bioscience) according to the manufacturer’s instructions.
Statistical Analyses
All quantitative data are presented as mean ± SD. Student t test was performed to assess the statistical significance of results between groups. Values of P < .05 were accepted as statistically significant.
Results
ADSCs Show Lower Transcriptomic Heterogeneity Than Do BMSCs at the Single-Cell Level
Same donor–derived ADSCs and BMSCs were isolated, cultured, and characterized by their cell surface marker expression and osteogenic, adipogenic, and chondrogenic differentiation potential 57 (Appendix Figure A1). To analyze the transcriptomic heterogeneity between these cell types, we performed scRNA-seq. A total of 83 transcriptomes of single ADSCs and 69 transcriptomes of BMSCs passed quality control.
To obtain an overall profile, we performed a principal component analysis. In the 3-dimensional principal component analysis plot, ADSCs and BMSCs were obviously separated (Figure 1, A and B). A comparative transcriptomic analysis between ADSCs and BMSCs identified 2861 genes that were highly expressed in ADSCs and 1172 genes that were highly expressed in BMSCs (Figure 1E, Appendix Tables A2 and A3). As MSCs are highly heterogeneous, 30 we calculated the cell-to-cell distance among single cells of ADSC and BMSC populations based on scRNA-seq data 24 to assess the cellular transcriptomic heterogeneity. The cell-to-cell distance of BMSCs was larger than that of ADSCs, suggesting that ADSCs show lower transcriptomic heterogeneity than BMSCs (Figure 1F).
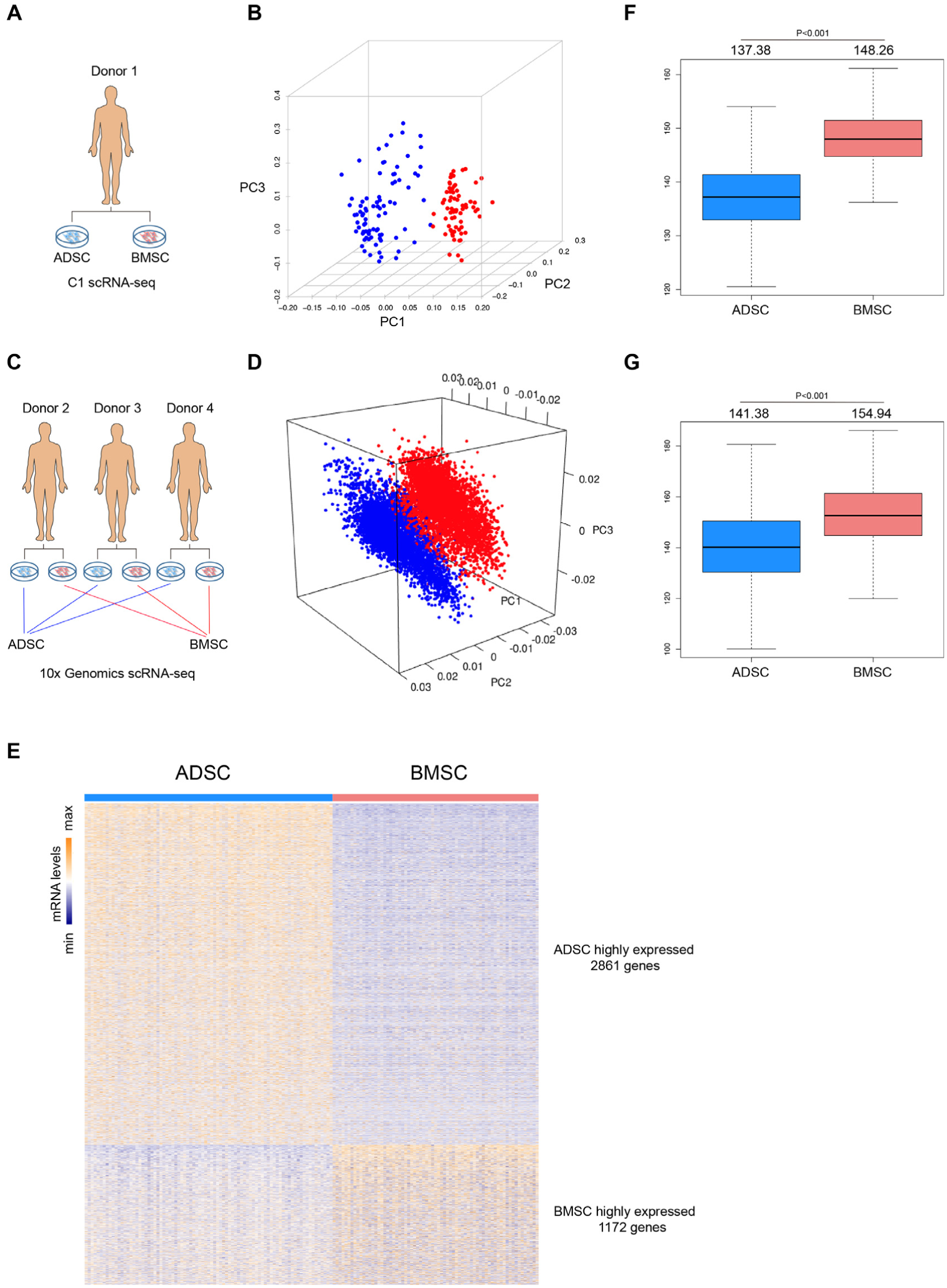
ADSCs show lower transcriptomic heterogeneity than BMSCs at single-cell resolution. (A) ADSC and BMSC culture process: Fluidigm C1. (B) Principal component (PC) analysis of 83 ADSCs (blue dots) and 69 BMSCs (red dots). (C) ADSC and BMSC culture process: 10x Genomics. (D) PC analysis of 3940 ADSCs (blue dots) and 4111 BMSCs (red dots). (E) Identification of genes highly expressed in ADSCs and BMSCs (P < .05, fold change >1.5). Each column represents a single cell. Boxplots depicting cell-to-cell distance in ADSC and BMSC populations based on (F) Fluidigm C1 and (G) 10x Genomics scRNA-seq data. Wilcoxon rank-sum test P values and median (line) values of cell-to-cell distance are shown. Boxes indicate interquartile range, and error bars indicate 1.5 times the first and third quartiles. ADSC, adipose-derived stem cell; BMSC, bone marrow mesenchymal stem cell; scRNA-seq, single-cell RNA sequencing.
To independently validate the results, we assessed a larger number of ADSCs and BMSCs from 3 donors with the 10x Genomics Chromium platform: 3940 ADSCs and 4111 BMSCs were captured and passed quality control. We found that despite the different cell donors and capture methods, these data largely recapitulated our initial findings (Figure 1, C, D, G). Taken together, these analyses indicated that ADSCs and BMSCs have a large difference in their transcriptomic profiles, and the transcriptome of ADSCs is more homogeneous than that of BMSCs.
ADSCs and BMSCs Show Different Metabolic Patterns and Stress Responses
To reveal the specific difference in transcriptomic profile, we inspected the differentially expressed genes of ADSCs and BMSCs. Among the top 100 highly expressed genes of BMSCs, we found 6 mitochondria-encoded genes, and almost all 69 BMSCs analyzed highly expressed these genes (Figure 2A). Although the high expression level of mitochondrial genes could be an indicator of unhealthy cells, the even expression patterns of housekeeping genes across all individual cells indicated a good cell status (Appendix Figure A2). Additionally, we found that nuclear-encoded genes for proteins in the mitochondrial respiratory electron transport chain were also highly expressed in BMSCs (Figure 2B, Appendix Figure A3). Transmission electron microscopy with these 2 cell preparations showed that the mitochondria of ADSCs were round, while they were significantly more elongated in BMSCs (Appendix Figure A4). These results suggest that ADSCs and BMSCs may adopt a different metabolic status under the same in vitro cell culture condition.
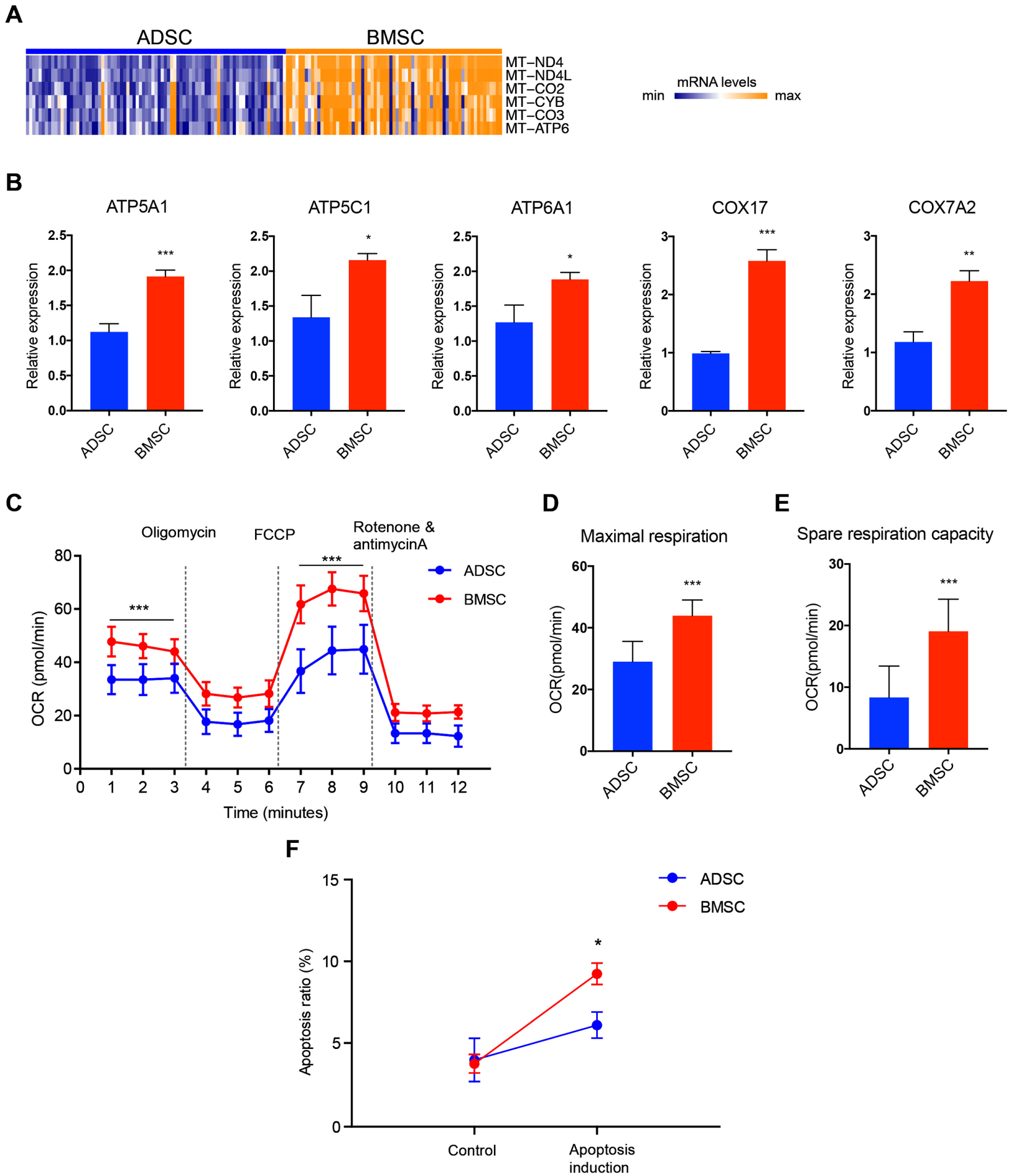
ADSCs and BMSCs show different metabolic patterns and stress responses. (A) Heat map displaying log2-normalized RPKM (reads per kilobase per million mapped reads) of mitochondrial genes reveals that BMSCs express a higher level of mitochondria-encoded genes than do ADSCs at single-cell resolution. Each column represents a single cell. (B) Expression of respiratory electron transport chain–related genes in ADSCs and BMSCs, quantified with real-time polymerase chain reaction. Results are normalized to the housekeeping gene ACTB and presented as mean ± SD (n = 3). (C) Oxygen consumption rate (OCR; pmol O2/min) of ADSCs and BMSCs (n = 6). (D) Maximal respiration (pmol O2/min) and (E) spare respiration capacity (pmol O2/min) of ADSCs and BMSCs (n = 6). (F) Change of apoptosis ratio of ADSCs and BMSCs after induction with hypoxia and serum-free condition for 24 hours. Cellular apoptosis after hypoxia and serum-free conditioning was measured by fluorescence-activated cell sorting analysis with annexin V and propidium iodide staining (n = 3). Results are presented as mean ± SD. *P < .05. **P < .01. ***P < .001. ADSC, adipose-derived stem cell; BMSC, bone marrow mesenchymal stem cell; FCCP, carbonyl cyanide-p-(trifluoromethoxy)phenylhydrazone (a decoupling agent for oxidative phosphorylation in mitochondria).
To further confirm the metabolic differences, we performed real-time cell metabolism assay with the Seahorse XF96 analyzer (Figure 2, C-E; Appendix Figure A5). These results demonstrated a higher level of oxygen consumption as well as maximal respiration and spare respiration capacity in BMSCs when compared with ADSCs. These findings indicated that BMSCs showed a more aerobic metabolic phenotype in comparison with ADSCs. Also, we constructed an in vitro hypoxia and serum deprivation–induced apoptosis model to detect how these 2 cells adapt to this stressed condition. 8 After 24 hours in this more stressed medium, annexin V and propidium iodide staining showed that the apoptosis rate of ADSCs was significantly lower than that of BMSCs (Figure 2F, Appendix Figure A6), suggesting that ADSCs may be more rapidly adapted to a hypoxic and serum-deprived environment.
ADSCs Have Intrinsically Lower Immunogenicity Than BMSCs
With their lack of HLA class II molecule and consequent relative insensitivity to costimulatory molecules, MSCs are thought to be “immune privileged,” and these attributes make them potentially exploitable as universal donor stem cells for therapeutic transplantation. 26 In fact, similar to other cells that do not express HLA class II molecule, MSCs are still being rejected after allogenic transplantation, especially when given in high doses,3,38,56 because of their HLA class I (HLA-I) expression. Higher cell surface HLA-I expression ultimately leads to graft rejection, while HLA-I downregulation helps cells evade immune defenses.22,29 Here we found that, as compared with ADSCs, BMSCs highly expressed HLA-I genes HLA-A, HLA-B, and HLA-C (Figure 3A). Real-time polymerase chain reaction was done to confirm this phenomenon (Figure 3, B-D), and cell surface HLA-I molecule expression level was assayed by flow cytometry with ADSCs and BMSCs derived from 3 donors. Results revealed that when compared with BMSCs, ADSCs expressed lower levels of cell surface HLA-I antigens under normal and inflammatory-simulated conditions (Figure 3, E-G).
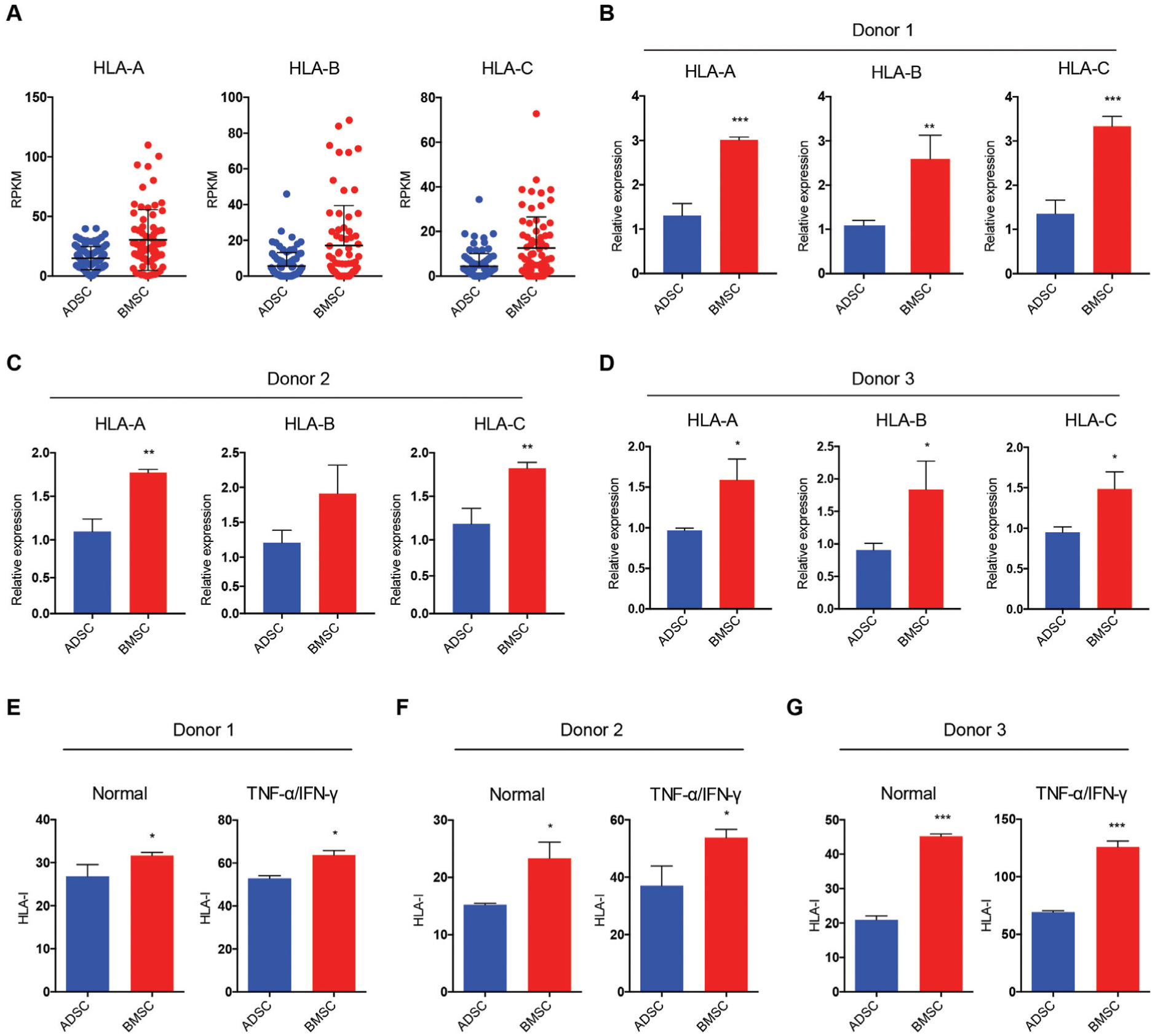
ADSCs show lower immunogenicity than do BMSCs. (A) The expression levels of HLA-A, HLA-B, and HLA-C in individual cells. Results are presented as mean ± SD. (B-D) Real-time polymerase chain reaction confirmation of scRNA-seq data in the expression levels of HLA-A, HLA-B, and HLA-C. Results are presented as mean ± SD (n = 3). (E-G) Cell surface HLA-I expression levels of ADSCs and BMSCs under normal and inflammation conditions, quantified with flow cytometry. The Y-axis represents the mean fluorescence intensity of the cell surface HLA-I molecule. Results are presented as mean ± SD (n = 3). *P < .05. **P < .01. ***P < .001. ADSC, adipose-derived stem cell; BMSC, bone marrow mesenchymal stem cell; HLA-I, human leukocyte antigen class I; RPKM, reads per kilobase per million mapped reads; scRNA-seq, single-cell RNA sequencing.
However, we found that BMSCs did not all equally express the high level of HLA-A, HLA-B, and HLA-C mRNA but instead were divided into BMSC HLA-Ihigh and HLA-Ilow subpopulations according to their mean level of HLA-A expression (Figure 3A). This division was consistent with the observation that BMSCs showed higher transcriptomic heterogeneity when compared with ADSCs. Gene ontology analysis further revealed that the BMSC HLA-Ihigh subpopulation also had more cell maturation–related genes being expressed, such as those for extracellular matrix organization and antigen processing and presentation (Figure 4A, Appendix Table A4), whereas genes in the BMSC HLA-Ilow subpopulation were related to cell proliferation (Figure 4B, Appendix Table A5). These results indicated that cells with low immunogenicity might have higher proliferation potential than those with higher immunogenicity.4,17
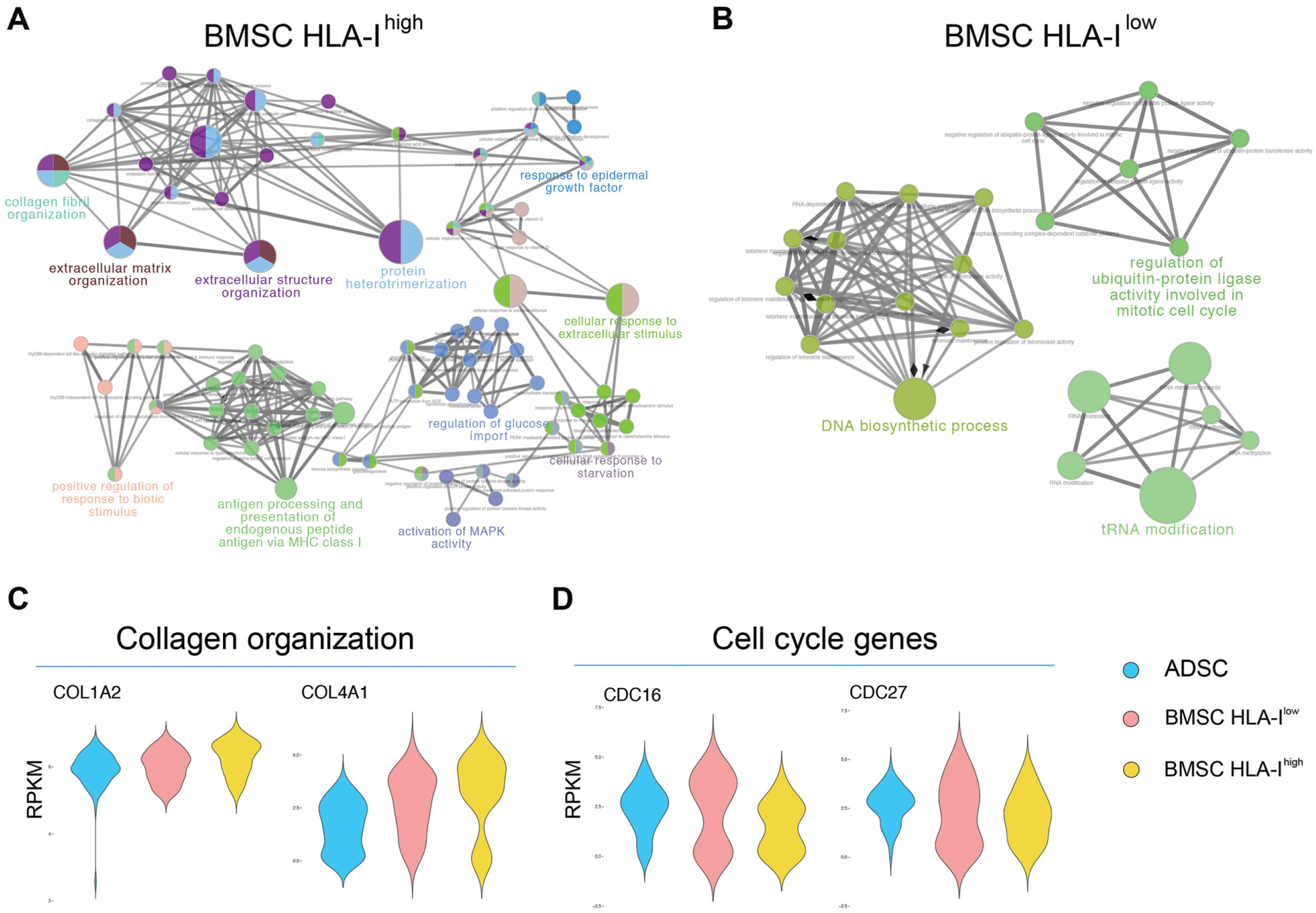
Characteristics of BMSC HLA-Ihigh and BMSC HLA-Ilow subpopulations. Gene ontology analysis of (A) BMSC HLA-Ihigh population and (B) BMSC HLA-Ilow population. Violin plots displaying the expression levels of (C) collagen organization and (D) cell cycle–related genes in ADSCs and BMSC HLA-Ihigh and HLA-Ilow cells. ADSC, adipose-derived stem cell; BMSC, bone marrow mesenchymal stem cell; HLA-I, human leukocyte antigen class I; RPKM, reads per kilobase per million mapped reads.
To analyze the relative state of ADSCs, we compared them with the BMSC HLA-Ihigh and BMSC HLA-Ilow subpopulations. ADSCs showed lower “collagen organization” but higher cell proliferation–related gene expression levels. This profile more closely resembled that of the BMSC HLA-Ilow subpopulation than the BMSC HLA-Ihigh subpopulation (Figure 4, C and D). Taken together, these findings indicated that at single-cell resolution, ADSCs were less immunogenic than BMSCs, and less immunogenic cells shared the transcriptomic similarities of higher proliferation potential and fewer extracellular matrix activities.
ADSCs Possess a Higher Immunosuppression Capacity Than BMSCs
In addition to their stem/progenitor properties, MSCs are active metabolically, secreting an array of cytokines (eg, IL-10, IDO, TGF-B1) that contribute to their immunomodulatory capacity. To test the immunomodulatory properties of ADSCs and BMSCs, cytokine expression analysis of each cell population was performed. Results showed large differences in cytokine expression pattern between ADSCs and BMSCs (Figure 5A). IL-33, a gene of an immune regulation–related cytokine, was highly expressed by ADSCs, and CXCL12, which contributes to hematopoietic stem cell microenvironment maintenance, was highly expressed by BMSCs.2,49
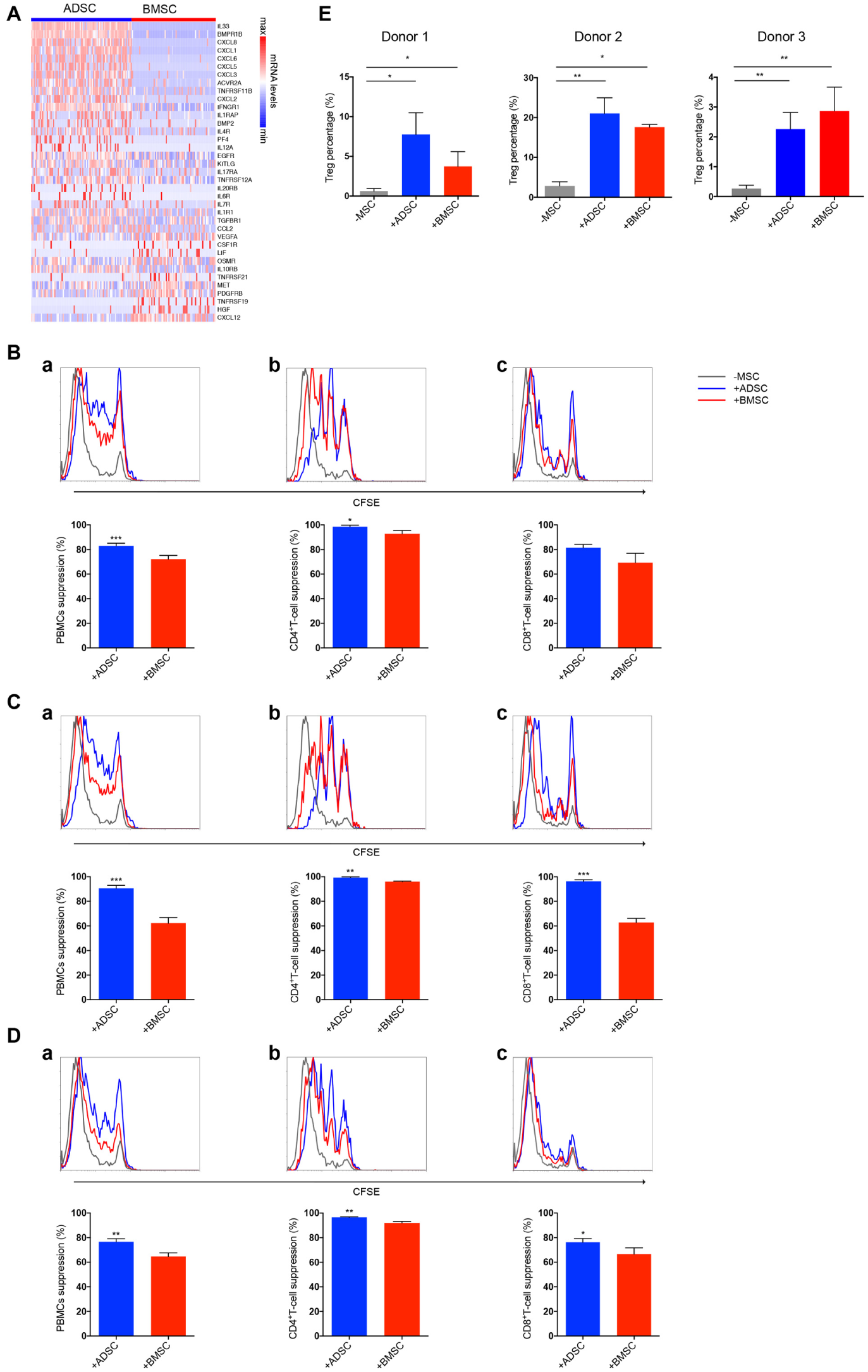
ADSCs possess higher immunosuppression capacity than do BMSCs. (A) Heat map displays log2-normalized RPKM (reads per kilobase per million mapped reads) of cytokine genes of ADSCs and BMSCs, with each column representing a single cell. PBMCs from 1 donor were cocultured with ADSCs or BMSCs from 3 donors: (B) donor 1, (C) donor, 2, (D) donor 3. The proliferation of (a) CFSE-labeled PBMCs, (b) CD4+, and (c) CD8+ T-cell subpopulations was induced with PHA, and the CFSE intensity was measured via flow cytometry (n ≥ 3). The top row of the figure is CFSE intensity, and the bottom is a bar plot of the suppression rate. (E) Induction of functional CD4+CD25+FoxP3+ T cells by coculture of ADSCs or BMSCs with PBMCs. Bar plots of expression of CD4, CD25, and FoxP3 on PBMCs on day 14. Results are presented as mean ± SD (n = 3). *P < .05. **P < .01. ***P < .001. ADSC, adipose-derived stem cell; +ADSC, PBMCs cocultured with ADSCs; BMSC, bone marrow mesenchymal stem cell; +BMSC, PBMCs cocultured with BMSCs; CFSE, carboxyfluorescein succinimidyl ester; –MSC, PBMCs only; PBMC, peripheral blood mononuclear cell; PHA, phytohaemagglutinin.
Given the different cytokine expression by ADSCs and BMSCs, it is possible that these 2 cells may possess different immunomodulation ability. To test this possibility, we investigated the capacity of ADSCs and BMSCs to inhibit proliferation of peripheral blood mononuclear cells. ADSCs showed a much higher ability to inhibit the proliferation of peripheral blood mononuclear cells stimulated with phytohaemagglutinin (+ADSCs vs +BMSCs: donor 1, 82.88 ± 2.23 vs 72.19 ± 3.00; donor 2, 90.57 ± 2.49 vs 62.30 ± 4.59; donor 3, 76.63 ± 2.49 vs 64.61 ± 5.17). The proliferation of activated CD4+ T cells and CD8+ T cells was also investigated. When compared with BMSCs, ADSCs exerted a stronger capacity to inhibit CD4+ T-cell proliferation (+ADSCs vs +BMSCs: donor 1, 98.51 ± 1.29 vs 92.80 ± 2.61; donor 2, 99.26 ± 0.74 vs 96.03 ± 0.43; donor 3, 96.53 ± 0.43 vs 92.06 ± 1.14) and CD8+ T-cell proliferation (+ADSCs vs +BMSCs: donor 1, 81.49 ± 2.64 vs 69.39 ± 7.58; donor 2, 96.28 ± 1.35 vs 62.28 ± 3.45; donor 3, 76.32 ± 2.93 vs 66.60 ± 5.10). These results suggested that ADSCs possess higher immunosuppressive performances, indicating that ADSCs may be a better candidate cell as an immunosuppressive cellular therapy product than BMSCs (Figure 5, B-D).
Furthermore, several studies documented the ability of MSCs to polarize T cells toward a regulatory phenotype that serves as an important mechanism to reduce inflammation.5,37 Since ADSCs highly express IL33, it is possible that ADSCs possess a stronger capacity to promote regulatory T (Treg) cell development, as IL33 can promote the proliferation of Treg. Therefore, we compared the capacity of ADSCs and BMSCs to promote Treg differentiation in a coculture analysis. However, no significant difference in the quantity of Treg was found between these groups (Figure 5E).
Clinical Outcome Profiling of ADSCs and BMSCs in Osteoarthritis Treatment
The number of registered stem cell clinical trials has continuously risen during the past decade (Figure 6A), indicating that the demand for MSC-based therapies has sharply increased. ADSCs and BMSCs are both used to treat diverse conditions, and both are popular for the treatment of osteoarthritis (Figure 6B and C; Appendix Tables A6 and A7). To determine whether there are any outcome differences between these MSC sources in the treatment of the same disease, a meta-analysis was performed with osteoarthritis as our target disease. A total of 3188 studies were identified in a computerized search, and 3163 records were excluded (437 articles were duplicates and 2726 articles did not meet our criteria per their titles or abstracts). We obtained the full text of the remaining 25 articles. Eleven of these were excluded for the following reasons: case report (n = 2), conference abstract (n = 5), incomplete data with no scale score (n = 2), and data replication in a longer follow-up (n = 2). Fourteen articles met our inclusion criteria † (Figure 6D). The characteristics of the included studies are summarized in Appendix Table A8 and Figure 6E.
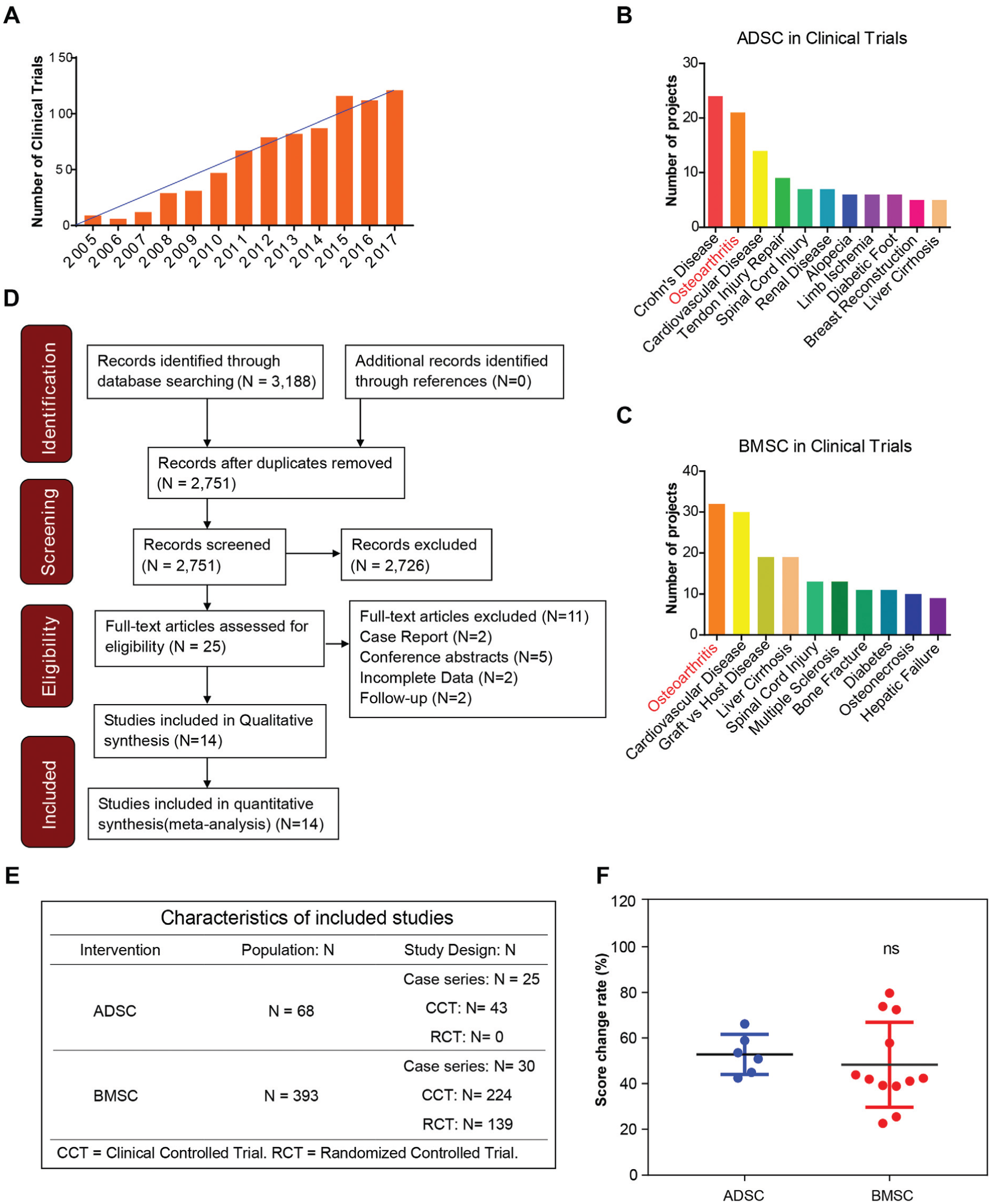
Clinical outcome profiling of ADSCs and BMSCs in osteoarthritis treatment. (A) Change in the number of registered clinical trials from 2005 to 2017. X-axis is time; Y-axis is the number of registered clinical trials. Data from ClinicalTrials.gov. (B) Top 10 indications being addressed with ADSCs in clinical trials, with data for 222 registered clinical trials. Data from ClinicalTrials.gov. (C) Top 10 indications being addressed with BMSCs in clinical trials, with data for 314 registered clinical trials. Data from ClinicalTrials.gov. (D) Flow diagram of included and excluded studies in this meta-analysis. (E) Characteristics of included studies. (F) Score change rate of osteoarthritis after treated by ADSCs or BMSCs. Each dot represents a group of patients treated by the same dose of mesenchymal stem cells in 1 research study. Results are presented as mean ± SD. ns (not significant), P > .05. ADSC, adipose-derived stem cell; BMSC, bone marrow mesenchymal stem cell.
In Appendix Table A8, full details of the 14 studies comprising 461 original patient records are given. These patients’ data were merged into a comparison of the disease severity score change rates achieved after ADSC or BMSC administration. These comparisons indicated no significant difference in the score change rate of osteoarthritis between the treatments, but ADSC treatments showed considerably less variable outcomes than BMSC treatments (ADSCs, 52.76 ± 3.603; BMSCs, 48.23 ± 5.374); the highest change rate of the BMSC group was 79.65%, while the lowest was only 22.57% (Figure 6F). Thus, the meta-analysis results indicated that the therapeutic effect of BMSCs was more variable, suggesting that ADSCs may be a more stable cell source for osteoarthritis treatment.
Discussion
It is well known that MSCs are heterogeneous on multiple levels.30,36 Our single-cell assay results demonstrated that BMSCs show higher transcriptomic heterogeneity than do ADSCs. As more homogeneous stem cells are required for more repeatable and reliable assays and clinical treatments, it is reasonable to suppose that ADSCs may be more suitable for certain cell transplantation treatments.
Unexpectedly, ADSCs and BMSCs showed quite marked differences in the metabolic pattern. Numerous studies showed that during stem cell differentiation, energy production shifts from glycolysis to the aerobic oxidation11,13,52,53; the morphology of the mitochondrion would also change during this process.52,58 According to these phenomena, our results in ADSC and BMSC metabolic profiles suggested that ADSCs may be superior to BMSCs at maintaining stemness and resisting differentiation when cultured in vitro. Such indications are supported by previous studies showing that ADSCs have higher proliferative activity and senescent tolerance than BMSCs.15,31,40 It also suggests that we could improve the quality of cultured MSCs in vitro by controlling and optimizing their pretransplantation metabolic patterns. In contrast to in vitro culture conditions, in vivo cell microenvironments can be relatively nutrient and oxygen deprived.10,12,23,39 The failure of transplanted cells to rapidly adapt to environmental changes may be one of the reasons for the low MSC survival rate.1,45,54 The better tolerance of ADSCs against apoptosis under hypoxic and serum deprivation conditions according to our results indicated that ADSCs might be better at preadapting to posttransplantation conditions.
MSCs have been popularly used for the treatment of various clinical diseases, as they are believed to be immune privileged. However, even though allogenic MSCs are more commonly used than autologous MSCs, given their quantity and accessibility, it has been reported that allogenic MSCs are not able to survive as long as autologous MSCs when injected in vivo. 4 This indicated that the immunogenicity of MSCs must be taken into consideration for clinical applications. It is especially important for patients who may need to receive multiple injections of allogenic MSCs, since the previously sensitized immune system rejects MSCs more rapidly. 56 In clinical practices, in vivo administrated MSCs normally enter the inflammatory environment of patients experiencing chronic inflammation or other conditions. In our study, to simulate a patient’s inflammatory condition, ADSCs and BMSCs were pretreated with cytokines IFN-γ and TNF-α for 24 hours. A flow cytometric assay was then performed where ADSCs demonstrated a lower immunogenicity level when compared with BMSCs. Therefore, ADSCs may be a more suitable choice for allogenic MSC-based therapies.
We evaluated the expression of cytokines in our scRNA-seq data and found that ADSCs highly expressed IL-33, a type 2 cytokine that can promote the proliferation of ST2L+ Treg cells. 49 Nevertheless, our functional analysis demonstrated that ADSCs and BMSCs show no significant difference in inducing the proliferation of Treg cells in peripheral blood mononuclear cells; a possible explanation may be that most of the Treg cells of peripheral blood mononuclear cells are ST2L negative and thus not affected by IL-33-expressed ADSCs. However, adipose tissues are rich in endogenous ST2L+ Treg 50 ; this suggests that in vivo transplanted ADSCs may be secreting IL-33 and acting on tissue endogenous immune cells to exert immunomodulatory function.
Our meta-analysis indicated that ADSCs show better stability in osteoarthritis treatment. This finding is supported by our single-cell analysis results clearly showing that ADSCs were more homogeneous than BMSCs. However, the meta-analysis has limitations: the number of cases included in it varied considerably (ADSCs vs BMSCs, n = 68 vs 393) (Figure 6E), which might render the results biased. Furthermore, the dose of MSCs given, the quality of the product, and the timing of MSC infusion all influenced trial results, adding to the difficulty in interpreting subsequent meta-analysis.
Another limitation of this study is the MSC culture methods. Because adipose and bone marrow are 2 tissues with different properties, the cell isolation process is different and unique to these 2 tissues. Adipose tissues were digested by collagenase to obtain ADSCs, while BMSCs were usually isolated through density-gradient centrifugation or direct plating. It is possible that the different isolation methods may influence the characteristics of these 2 cell types. In addition, a higher number of immune cells was observed in BMSCs at passage 0 after density-gradient centrifugation or direct plating when compared with ADSCs, and this coculture environment with immune cells at passage 0 may introduce BMSCs skewing toward an inflammatory direction. To avoid these problems, direct isolation of ADSCs and BMSCs by fluorescence-activated cell sorting should be studied in the future. Several studies have already revealed the in vivo identity of ADSCs, 46 and much more research still needs to be done on the in situ identity of BMSCs, making BMSC direct isolation from bone marrow possible.
In conclusion, our findings and strategies will promote the development of MSC biology, provide more knowledge on the selection of MSC sources for a particular treatment, and introduce new strategies for MSC-based precise medicine.
Supplemental Material
DS_10.1177_0363546519848678 – Supplemental material for Single-Cell Profiles and Clinically Useful Properties of Human Mesenchymal Stem Cells of Adipose and Bone Marrow Origin
Supplemental material, DS_10.1177_0363546519848678 for Single-Cell Profiles and Clinically Useful Properties of Human Mesenchymal Stem Cells of Adipose and Bone Marrow Origin by Wenyan Zhou, Junxin Lin, Kun Zhao, Kaixiu Jin, Qiulin He, Yejun Hu, Hongwei Ouyang, Gang Feng, Youzhi Cai, Chen Xia, Hua Liu, Weiliang Shen and Xueqing Hu in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank the Core Facilities of Zhejiang University School of Medicine for technical assistance, as well as Prof Junfeng Ji for his advice and Chengrui An for his help in data analysis. The authors thank Prof David Aront and Varitsara Bunpetch for their help in manuscript editing.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Key R&D Program of China (2017YFA0104900), the National Natural Sciences Foundation of China (31830029, 81630065, 81672162), and the Research Grant for the Application of Public Technology of Zhejiang province (2015C33180). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.