
Abstract
Background:
The benefits of platelet-rich plasma (PRP) for the treatment of rotator cuff tears remain inconclusive, as it is administered either as an adjuvant to surgical repair or as a primary infiltration without targeting the index lesion, which could dilute its effect.
Purpose:
To determine whether PRP infiltrations are superior to saline solution infiltrations (placebo) at improving healing, pain, and function when injected under ultrasound guidance within isolated interstitial supraspinatus tears.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
In this single-center, double-blinded, randomized controlled trial, 80 adults with symptomatic isolated interstitial tears of the supraspinatus, confirmed by magnetic resonance arthrography, were randomized to PRP or saline injections. Each patient received 2 injections with a 1-month interval. The primary outcome was the change in lesion volume, calculated on magnetic resonance arthrography, at 7 months. The secondary outcomes were improvements in shoulder pain and the Single Assessment Numerical Evaluation (SANE) score at >12 months.
Results:
Preoperative patient characteristics did not differ between the 2 groups. At 7 months, there were no significant differences between the PRP and control groups in terms of a decrease in lesion size (–0.3 ± 23.6 mm3 vs –8.1 ± 84.7 mm3, respectively; P = .175); reduction of pain on a visual analog scale (VAS) (–2.3 ± 3.0 vs –2.0 ± 3.0, respectively; P = .586); and improvement in SANE (16.7 ± 20.0 vs 14.9 ± 29.0, respectively; P = .650), Constant (8.6 ± 13.0 vs 10.7 ± 19.0, respectively; P = .596), and American Shoulder and Elbow Surgeons (19.5 ± 20.0 vs 21.9 ± 28.0, respectively; P = .665) scores. At >12 months, there were no significant differences between the PRP and control groups in terms of a reduction of pain on a VAS (–3.3 ± 2.6 vs –2.3 ± 3.2, respectively; P = .087) or improvement in the SANE score (24.4 ± 27.5 vs 23.4 ± 24.9, respectively; P = .846). At 19.5 ± 5.3 months, the incidence of adverse effects (pain >48 hours, frozen shoulder, extension of lesion) was significantly higher in the PRP group than the control group (54% vs 26%, respectively; P = .020).
Conclusion:
PRP injections within interstitial supraspinatus tears did not improve tendon healing or clinical scores compared with saline injections and were associated with more adverse events.
Registration:
NCT02672085 (ClinicalTrials.gov identifier).
Advances in imaging and arthroscopic techniques have improved the understanding and diagnosis of rotator cuff tears. Nonetheless, the true incidence of rotator cuff tears remains underestimated because of the prevalence of asymptomatic tendinopathies and partial-thickness tears,29,45 especially interstitial lesions that are more difficult to detect.25,46
There is no clear consensus at present on the strategies to manage rotator cuff tears. Initial treatments are often nonoperative and include various combinations of physical therapy, analgesics, nonsteroidal anti-inflammatory drugs, or local anesthetic and steroid injections.5,6,10,30,32 When nonoperative treatments fail, surgical repair may be attempted, 31 even if it requires extended rehabilitation and does not guarantee tendon healing in the long term. 15 Alternatively, platelet-rich plasma (PRP) can be injected to promote healing, as it involves fewer risks and faster rehabilitation. 27
Currently, PRP is a popular clinical strategy to stimulate regenerative tendon healing13,36 and has been reported to improve clinical outcomes in various tendinopathies of the elbow2,8,35 and knee joints.2,12 The benefits of PRP for the treatment of rotator cuff tears, however, remain inconclusive,13,48 as it is administered either as an adjuvant to surgical repair11,21-23,37,39,41,47 or as a primary infiltration without targeting the index lesion, 24 which could dilute its effect.
The aim of the present study was to determine whether PRP infiltrations are superior to saline solution infiltrations (placebo) at improving healing, pain, and function when injected under ultrasound guidance within isolated interstitial supraspinatus tears. Our main hypotheses were that, compared with saline solution, PRP offers a significantly greater (1) reduction in lesion volume at 7 months and (2) improvement in shoulder pain and the Single Assessment Numerical Evaluation (SANE) score at 12 months.
Methods
Trial Design
We conducted a single-center, double-blinded, randomized placebo-controlled efficacy trial with 2 parallel groups and a minimum follow-up of 12 months. The study protocol has been registered at ClinicalTrials.gov (NCT02672085) and approved by the medical ethics committee of Geneva University Hospital (HUG#15-081). All patients provided written informed consent for their participation and for the use of their data and images for research and publishing purposes.
Patients
From June 2015 to August 2016, we prospectively enrolled all adult patients with a diagnosed isolated interstitial supraspinatus tear and symptomatic shoulder pain for ≥6 months. We included patients suspected to have a supraspinatus tear based on the Jobe test, performed by an experienced surgeon (A.L.), and with an interstitial supraspinatus tear diagnosed on magnetic resonance arthrography (MRA), performed by an experienced radiologist (F.C.K.). We excluded patients who had (1) concomitant articular or bursal supraspinatus, infraspinatus, or subscapularis tendon tears; (2) a frozen shoulder, defined as a restriction of >20% in external rotation as well as active and passive elevation, despite a normal radiological appearance 17 ; (3) shoulder steroid infiltrations over the past 3 months; or (4) calcifying tendinopathies.
Interventions
All patients were treated from August 2015 to November 2016 at La Tour Hospital, with 2 infiltrations with an interval of 1 month, following the method described by Rha et al. 40 The intervention group received 2 leukocyte-poor PRP infiltrations, while the placebo group received 2 infiltrations of saline solution. Given the reported benefits of needling on tendon healing,26,40 recruitment issues associated with a lack of treatment in the placebo group were circumvented. 42
A blood sample of 8 mL was taken from all patients before surgery. In the intervention group, PRP was prepared using the RegenKit BCT (Regen Lab) according to the manufacturer’s instructions: (1) no use of buffering or activating agents, (2) one centrifugation for 5 minutes at 1500 revolutions per minute, (3) discarding of the first 2 mL of the platelet-poor supernatant, and (4) collection of 2 mL of the platelet-rich supernatant. The blood samples of patients assigned to the intervention group were centrifuged according to the manufacturer’s instructions (RegenKit BCT) to obtain 2 mL of PRP. The blood samples of the placebo group were discarded. Within 30 minutes of blood sample collection, PRP or the saline solution was injected within the interstitial lesion under ultrasound guidance, by the radiologist, until the lesion was filled.
For 7 months after the first infiltration, patients were allowed to take paracetamol or opioids for pain relief but not nonsteroidal anti-inflammatory drugs, to prevent a blockade of platelet function. They could perform daily activities and light sports below the pain threshold. To avoid bias, physical therapy was forbidden for 7 months after the intervention.
Randomization
Using permuted block randomization 44 with blocks of 4 or 6 patients in a 1:1 ratio, patients were assigned by another experienced radiologist (A.K.) either to the intervention group, which received leukocyte-poor PRP injections (n = 41), or to the placebo group, which received isotonic saline injections (n = 39).
Blinding
Syringes were masked with a covering sheath to ensure blinding to patients and medical staff. Ultrasound-guided infiltrations were injected by an experienced radiologist (F.C.K.), who was blinded to treatment allocation and used the same technique for all patients. The 2 radiologists (F.C.K. and A.K.), who independently performed postoperative radiographic readings, and the surgeon (A.L.), who collected clinical scores and performed follow-up visits, were all blinded to preoperative measurements, preoperative functional scores, and patient treatment allocation.
Outcomes
The primary outcome was the change in lesion volume, calculated on MRA, from before the first infiltration to 6 months after the second infiltration, allowing the critical period of 6 months necessary for adequate tendon healing. 4 MRA was performed using a 3-T machine (Achieva; Philips). Interstitial tendon tears were defined by a longitudinal hyperintense signal on a T2 fat-saturated sequence, without contrast agents. The lesion volume was estimated as half the product of maximal tear dimensions in the 3 axes, using OsiriX software (Figure 1). The final lesion volume recorded was the mean of measurements by the 2 independent radiologists (F.C.K. and A.K.). In case of a >50% difference in the lesion volume calculation, a consensus was sought in the presence of the orthopaedic surgeon (A.L.).
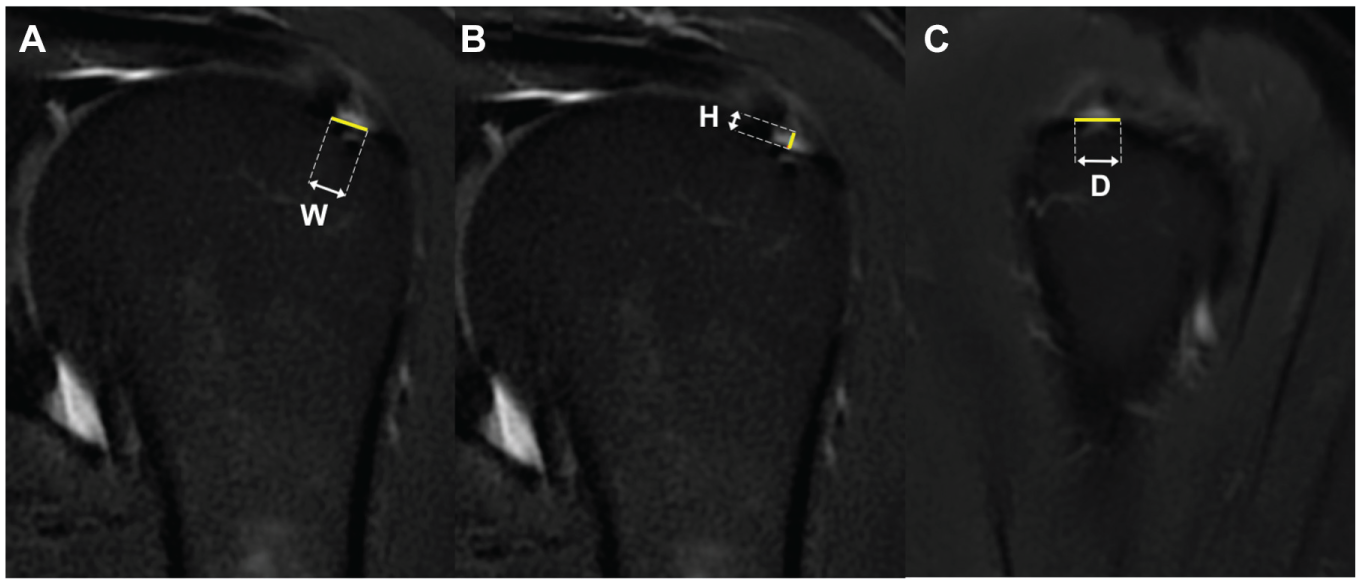
Interstitial supraspinatus tear measurement (T2 fat-saturated magnetic resonance arthrography). Coronal view showing (A) lesion width (W) and (B) lesion height (H). (C) Sagittal view showing lesion depth (D). The tear size volume was calculated as half of the product of maximal tear dimensions measured in the 3 axes.
The secondary outcomes were (1) improvement in pain on a visual analog scale (VAS); (2) improvement in function assessed by the SANE, Constant score, and American Shoulder and Elbow Surgeons (ASES) score; (3) adverse events (persistent pain >48 hours, tear extension to bursal or articular surface); and (4) additional treatments performed >7 months after the intervention (physical therapy, PRP or corticosteroid infiltration, surgical intervention). Follow-up information; pain on a VAS; and SANE, Constant, and ASES scores were collected at 7 months after the first injection, between October 2015 and May 2017. Pain on a VAS and the SANE score were collected again at a minimum of 12 months’ follow-up.
Statistical Analysis
Power calculations were based on a pilot study. 28 A clinically relevant difference of 50% between preoperative and postoperative tear volumes corresponded to 38 ± 59 mm3. Assuming that the lesion volume would decrease by ≥38 ± 59 mm3 in the PRP group and by 0 mm3 in the placebo group, with a power (beta) of 0.80 and level of significance (alpha) at .05, forty patients were required per group. Assuming that 5% of patients would be lost to follow-up, 42 patients were enrolled in each group.
Descriptive statistics were used to describe baseline patient characteristics. The Shapiro-Wilk test was used to assess the normality of distributions. For non-Gaussian continuous data, intergroup differences were evaluated using the Wilcoxon rank-sum test (Mann-Whitney U test), and intragroup differences between the 3 time points were evaluated using the Wilcoxon signed-rank test (paired Mann-Whitney U test). For categorical data, differences between the groups were evaluated using the Fisher exact test. Intraclass correlation coefficients (ICCs) were used to assess the level of agreement between the MRA readings of 2 independent readers (A.J.S., F.C.K.; before seeking a consensus in cases of discordant results). The ICC can be interpreted as follows: <0.40 poor; 0.40-0.59 fair; 0.60-0.74 good; and 0.75-1.00 excellent. 9 The coordinating researcher (A.J.S.), who performed statistical analyses, was blinded to the allocated treatment. Statistical analyses were conducted using R version 3.3.2 (R Foundation for Statistical Computing). P values <.05 were considered statistically significant.
Results
Of the 107 patients screened, 8 presented concomitant tears of the infraspinatus or subscapularis tendons, and 15 declined to participate, leaving 84 patients for a randomized intervention (Figure 2). In the intervention group, 1 patient was lost to follow-up, leaving 41 patients for analysis; in the placebo group, 2 patients withdrew from the study, and 1 patient was excluded because of a late diagnosis of a concomitant tear, leaving 39 patients for evaluation. Preoperative patient demographics, clinical characteristics, and lesion size did not differ between the 2 groups (Table 1). The interobserver agreement on lesion size was good (ICC, 0.68 [95% CI, 0.59-0.76]).
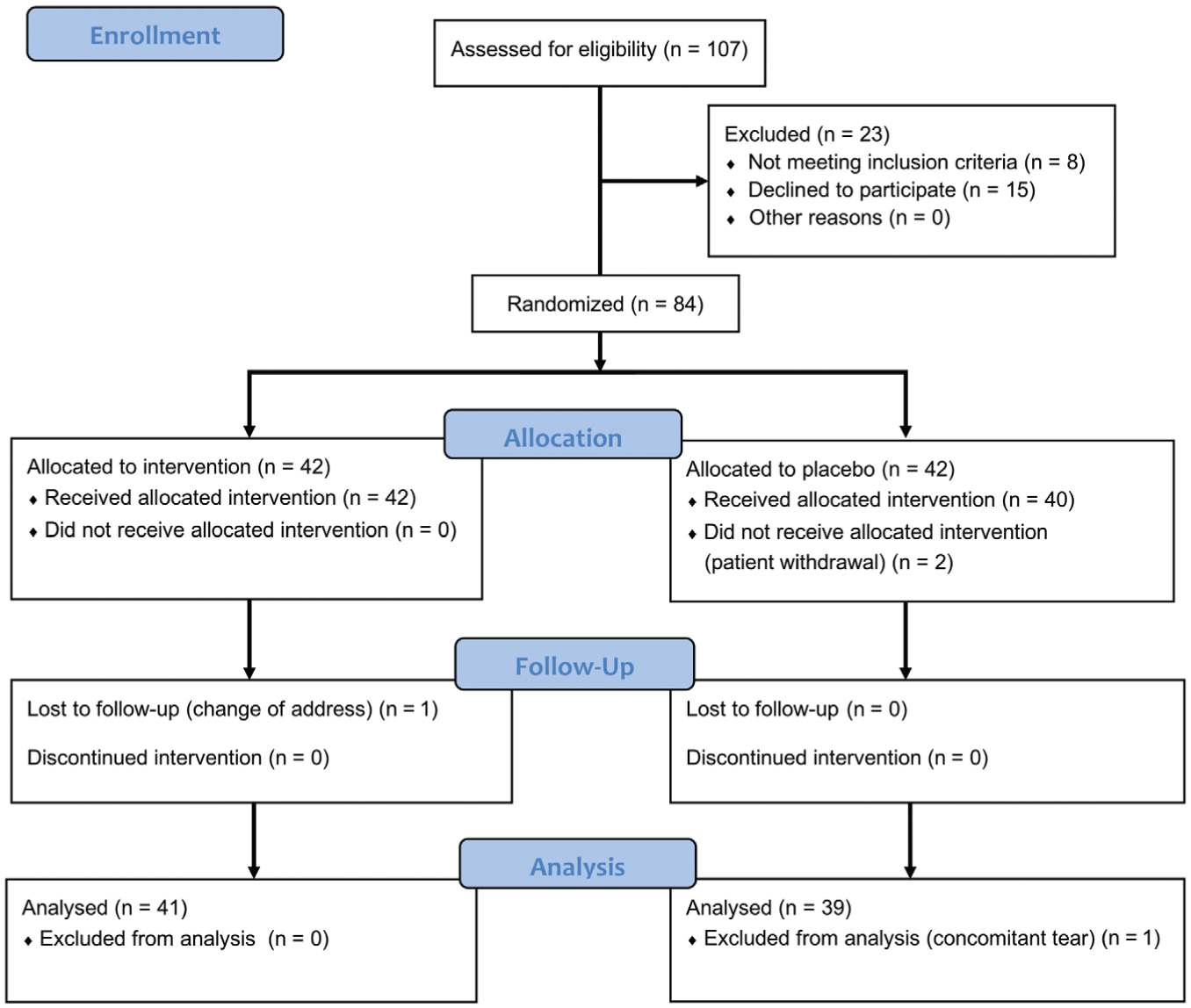
Flowchart of patient enrollment.
Demographics and Clinical Characteristics by Infiltration Type a
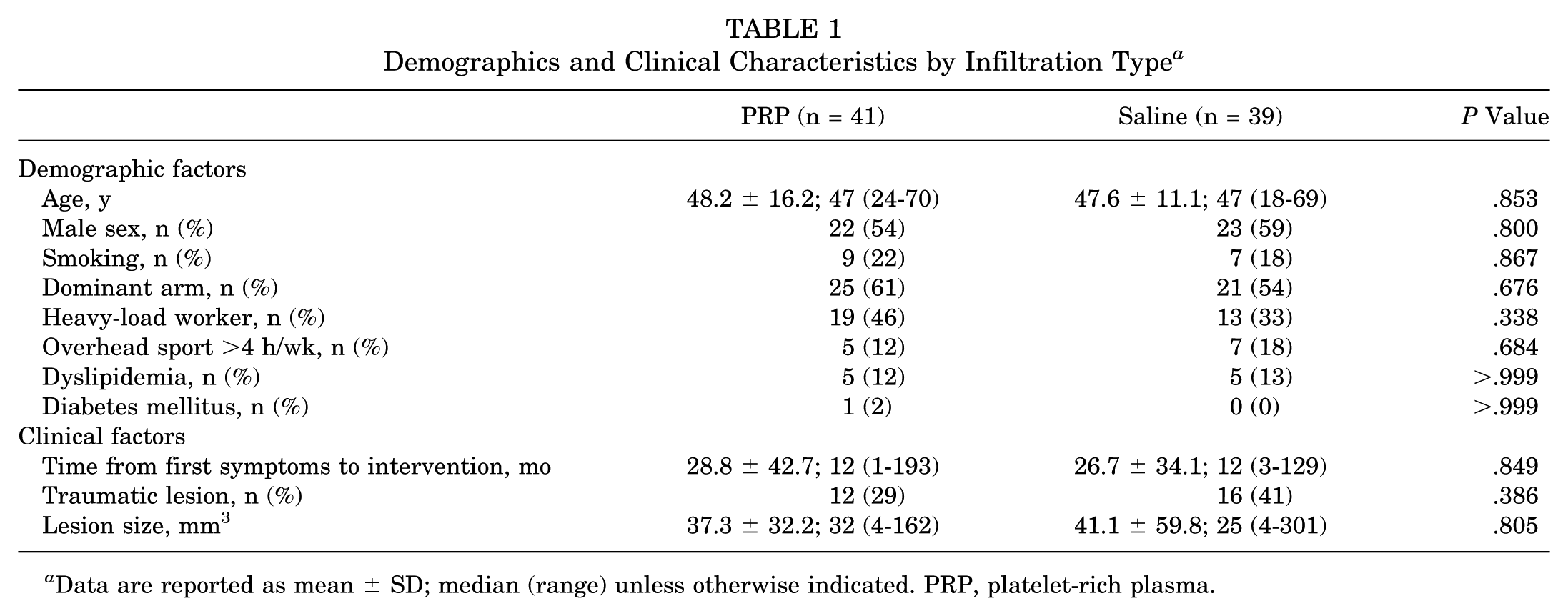
Data are reported as mean ± SD; median (range) unless otherwise indicated. PRP, platelet-rich plasma.
At 7 months, there were no significant differences between the PRP and control groups in terms of a reduction in lesion volume (–0.3 ± 23.6 mm3 vs –8.1 ± 84.7 mm3, respectively; P = .175) (Table 2 and Figure 3); reduction of pain on a VAS (–2.3 ± 3.0 vs –2.0 ± 3.0, respectively; P = .586); and improvement in SANE (16.7 ± 20.0 vs 14.9 ± 29.0, respectively; P = .650), Constant (8.6 ± 13.0 vs 10.7 ± 19.0, respectively; P = .596), and ASES (19.5 ± 20.0 vs 21.9 ± 28.0, respectively; P = .665) scores (Table 2 and Figure 4). At >12 months, there were no significant differences between the PRP and control groups in terms of a reduction of pain on a VAS (–3.3 ± 2.6 vs –2.3 ± 3.2, respectively; P = .087) or improvement in the SANE score (24.4 ± 27.5 vs 23.4 ± 24.9, respectively; P = .846).
Preintervention and Postintervention Outcomes by Infiltration Type a
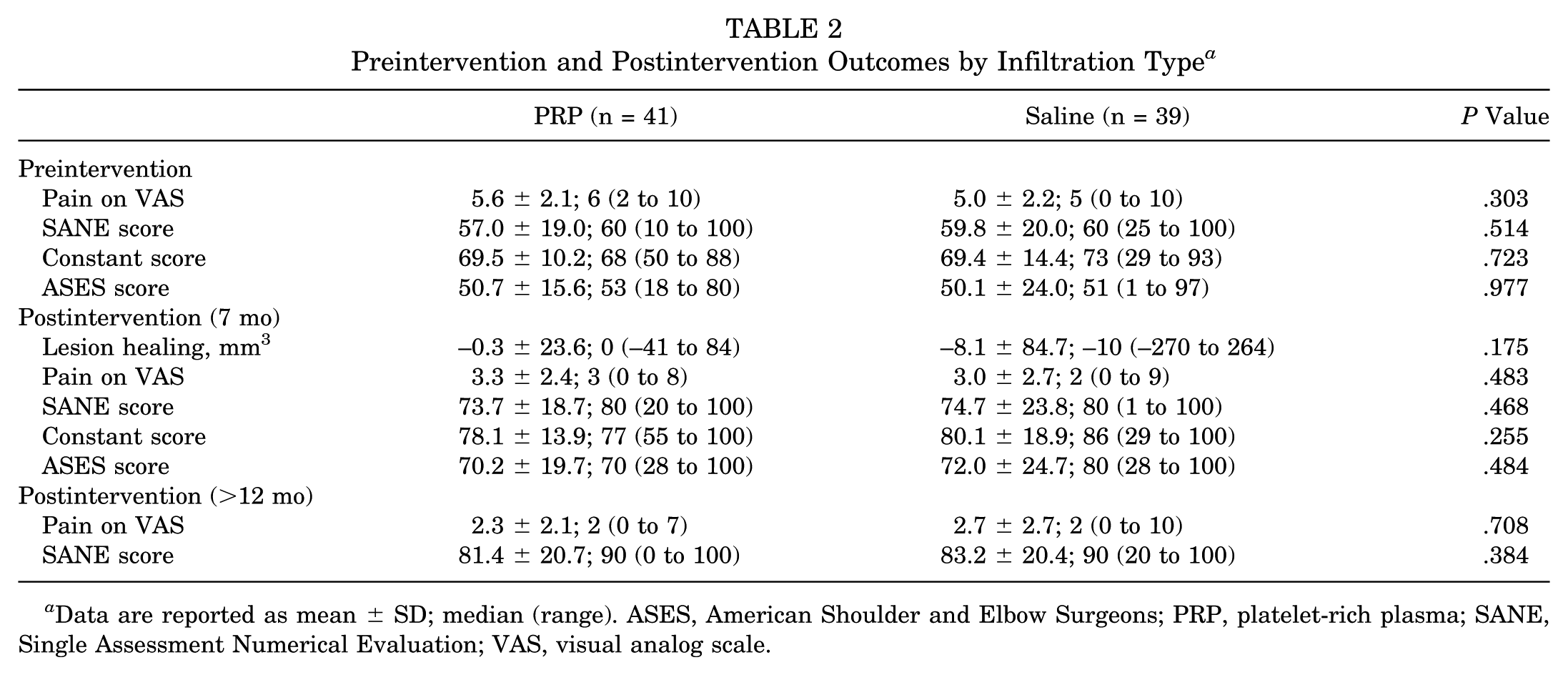
Data are reported as mean ± SD; median (range). ASES, American Shoulder and Elbow Surgeons; PRP, platelet-rich plasma; SANE, Single Assessment Numerical Evaluation; VAS, visual analog scale.
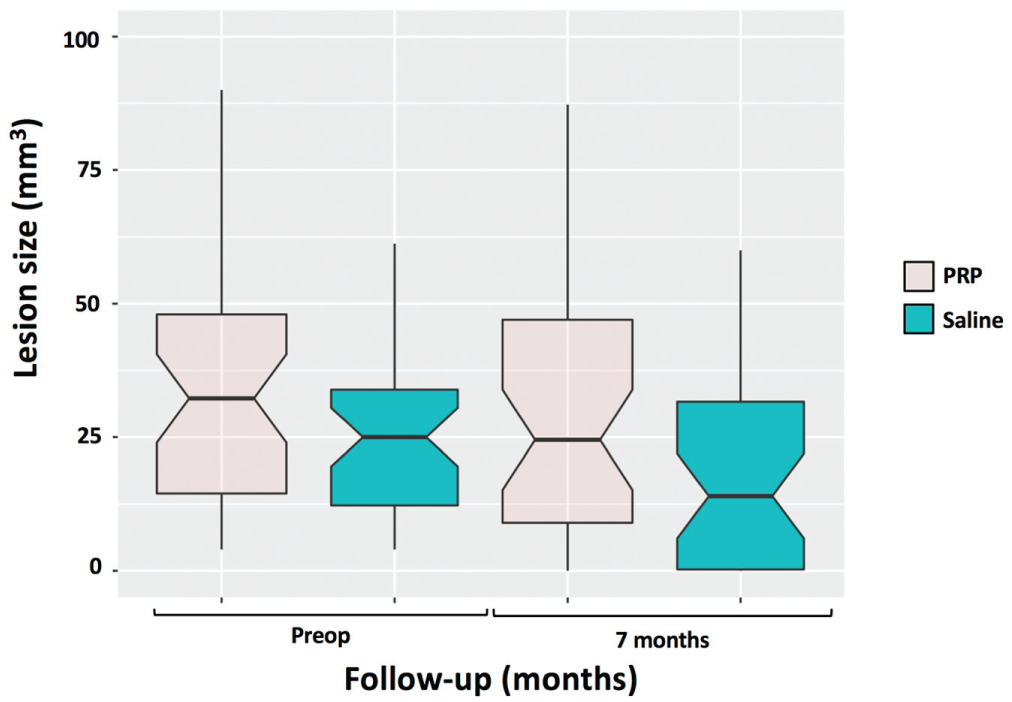
Boxplots showing preoperative and postoperative lesion sizes for the platelet-rich plasma (PRP) and saline groups. No significant differences were observed. Outliers are not illustrated.
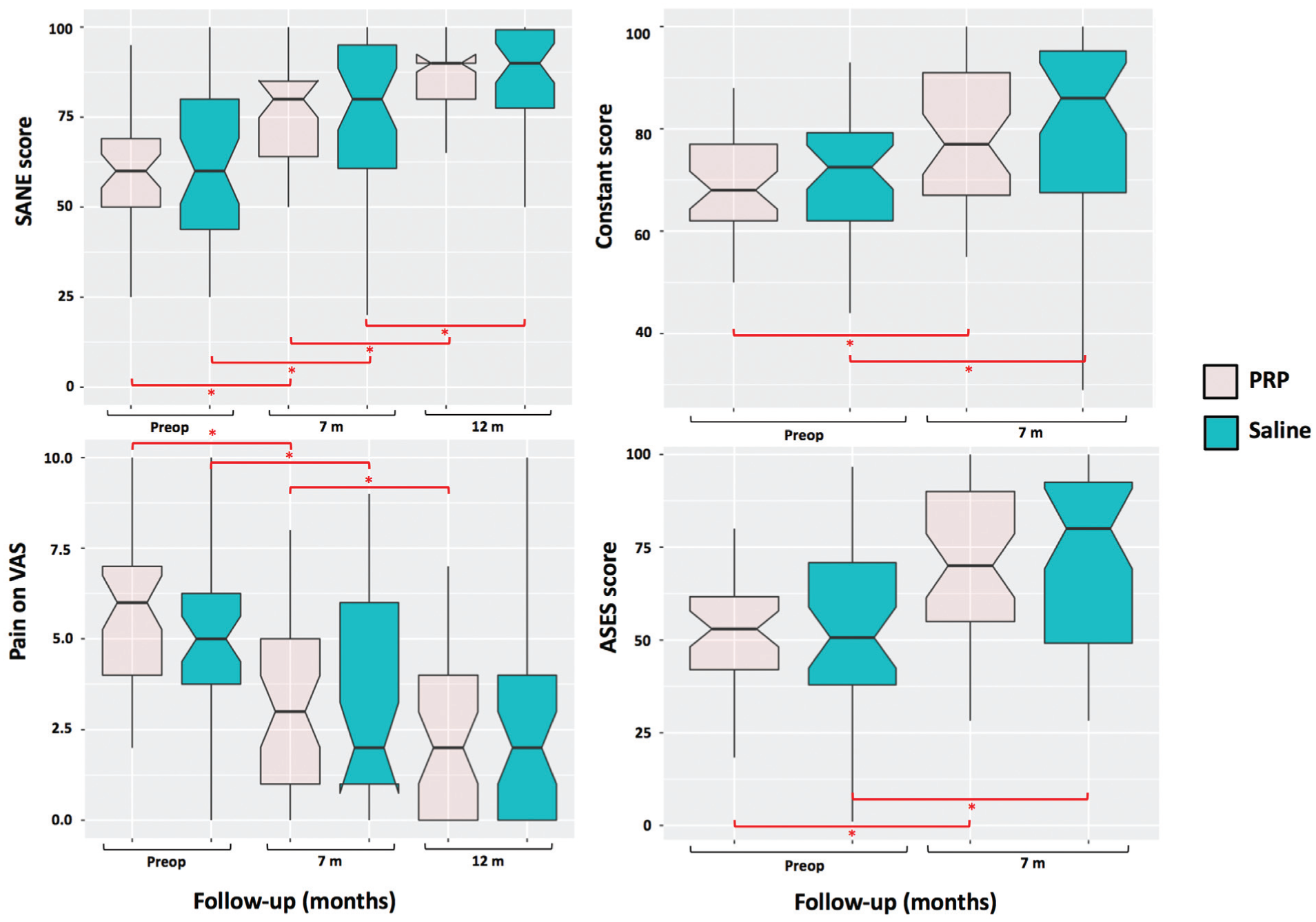
Boxplots showing preoperative and postoperative clinical scores for the platelet-rich plasma (PRP) and saline groups. Only significant P values are shown. Outliers are not illustrated. ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
At final follow-up of 19.5 ± 5.3 months (range, 12.0-28.0 months), the incidence of adverse effects (pain >48 hours, frozen shoulder, extension of lesion to bursal or articular surface) was significantly higher in the PRP group compared with the control group (54% vs 26%, respectively; P = .020) (Table 3). Seven patients (17%) in the PRP group underwent surgical repair of the rotator cuff compared with only 2 patients (5%) in the control group (P = .182).
Adverse Events and Additional Treatments by Infiltration Type a
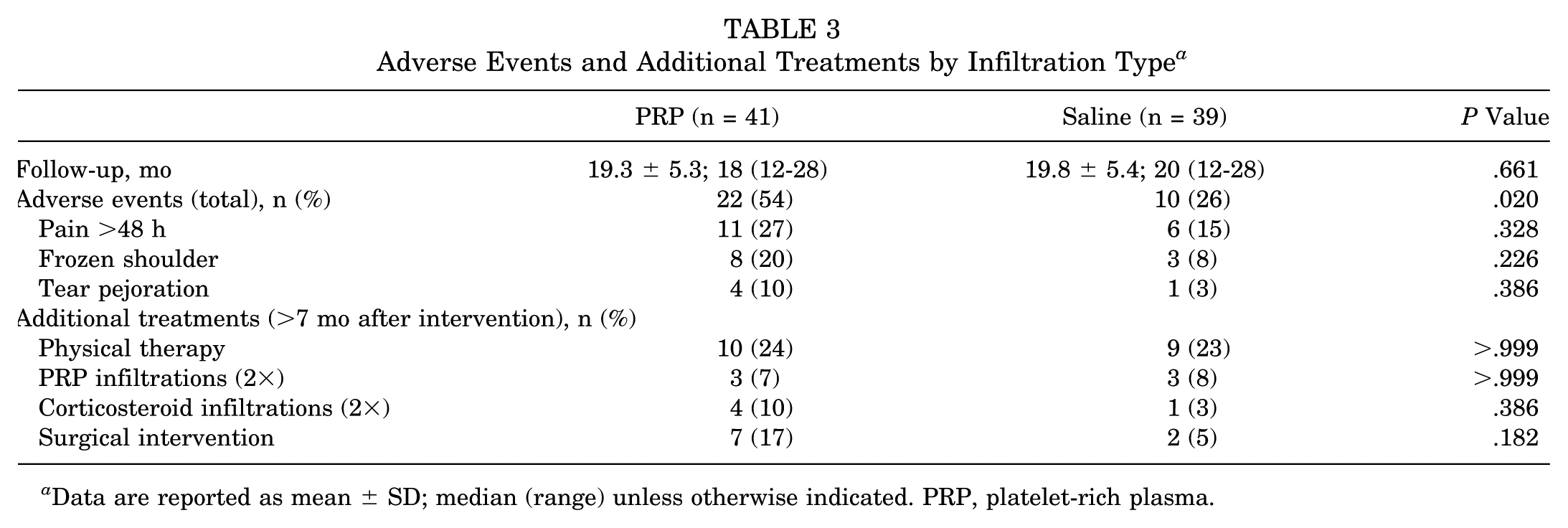
Data are reported as mean ± SD; median (range) unless otherwise indicated. PRP, platelet-rich plasma.
Discussion
The aim of the present study was to determine whether PRP infiltrations are superior to saline solution infiltrations (placebo) at improving healing, pain, and function when injected under ultrasound guidance within isolated interstitial supraspinatus tears. PRP is commonly injected at the tendon-bone interface, leading to considerable loss of PRP into the glenohumeral joint and subacromial space or dilution by arthroscopic lavage or hematoma.21-23,37 The authors believed that ultrasound-guided injections of PRP into the confined volume of interstitial lesions could enhance healing. Our results did not confirm our hypotheses that, compared with saline solution (placebo), ultrasound-guided PRP injections within interstitial lesions offer a significantly greater reduction in lesion volume and improvement in shoulder pain and function. Furthermore, the PRP group had a significantly higher incidence of adverse events than the saline group, suggesting that PRP injections may have direct or indirect deleterious effects.
Our findings indicated that both PRP and placebo treatments significantly improved clinical scores and tended to reduce the lesion size. This could be interpreted as a mere placebo effect in both groups but would not explain the reduction in lesion volume. It is therefore likely that tendon healing was induced either (1) spontaneously; (2) by dilation of the lesion after the interstitial injection; and/or (3) by needling itself, which is known to stimulate tissue regeneration by inducing bleeding18,19 as well as to improve function.26,40
Overall, laboratory studies have reported positive results for the use of PRP on rotator cuff tears,16,34 but these are not confirmed by clinical studies, which have reported conflicting conclusions based on PRP formulations, surgical techniques, and tear sizes.1,2,14,33-35,38,41 Systematic reviews on the effect of adjuvant PRP in rotator cuff repair have concluded that PRP has no overall significant effect on functional outcomes and repair integrity, except for small- to medium-sized tears, for which PRP treatment might be advantageous.3,7,41,47 To the authors’ knowledge, there are no published studies on the effects of PRP injected within interstitial tears of the supraspinatus, but 1 randomized controlled trial 20 and 1 comparative trial 48 evaluated the effects of PRP injections as nonoperative treatment for rotator cuff tears, and 2 randomized controlled trials24,40 assessed the effects of ultrasound-guided injections of PRP as nonoperative treatment for tendinopathies, tendinosis, or partial rotator cuff tears. In agreement with our findings, 3 of 4 studies20,24,48 concluded that, at 12 months, PRP had no healing or functional benefits over placebo or physical therapy. Rha et al, 40 however, reported a significant reduction in pain and function with ultrasound-guided PRP injections compared with dry needling at 6 months, although their findings are limited by a small cohort size (n = 39), short follow-up, difficulties in injecting PRP directly into the lesion site, and lack of blinding of the investigator who injected the treatment.
An important strength of our placebo-controlled efficacy study is that it was blinded for patients, treating physicians, and outcome assessors (including the statistician). Moreover, we had a high follow-up rate. Finally, to the authors’ knowledge, this study was the first to evaluate radiographic improvement in lesion volume, together with clinical progress on pain and functional scores. There are, however, some limitations worth discussing. First, we did not report the PRP composition, which is known to influence growth factors.39,43 Second, patients with deltoid muscle weakness were not excluded prospectively, although clinical and MRA assessments revealed no signs of axillary nerve deficiency or painful acromial impingement. Third, we included patients with small or large tears, which could influence the efficacy of PRP,3,7,41,47 although no difference in the tear size distribution was detected among the PRP and placebo groups. Last, we reported absolute changes in the lesion volume, while a relative reduction in lesion volume could also be of value.
Conclusion
Compared with saline injections (placebo), ultrasound-guided PRP injections within isolated interstitial supraspinatus tears were not superior in reducing the lesion volume or improving pain or clinical scores, and they were associated with more adverse events.
Footnotes
Acknowledgements
The authors are grateful to Hugo Bothorel and Aude Michelet for their assistance in statistical analyses and article preparation.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.