
Abstract
Background:
There is a paucity of literature regarding risk factors and mechanisms of Achilles tendon (AT) ruptures in the National Basketball Association (NBA).
Purpose:
To identify the risk factors and outcomes of AT ruptures in NBA athletes. Furthermore, using video analysis, to characterize the mechanisms of rupture by identifying the most common playing situations and lower extremity positions at the time of injury.
Study Design:
Descriptive epidemiology study.
Methods:
AT ruptures in the NBA that occurred between the seasons of 1969-1970 and 2017-2018 were identified. Player data collected included age, position, body mass index, total games started before and after injury, and Player Efficiency Rating. Injury-related variables collected included date of injury, laterality, minutes played before injury, operative versus nonoperative treatment, and time to return to play. Available video footage was analyzed for the mechanism and body position at the time of injury. Univariable and multivariable linear regression was used to compare changes in performance before and after AT rupture. Statistical significance was set at P < .05.
Results:
Forty-four ruptures were identified between 1970 and 2018. The mean age was 28.3 years, with players averaging 6.8 seasons before AT rupture. AT ruptures were most prevalent during early-season game play (27.3%), followed by preseason (18.2%) and late season (18.2%). More than a third (36.8%) of players either did not return to play or started in fewer than 10 games in the remainder of their career, with 21% of ruptures leading to retirement. The mean time to return to play was 10.5 months. The Player Efficiency Rating declined by an average of 2.9 points (range, –11.5 to +2.3) (P < .001). Analysis of available injury footage (n = 12) demonstrated all ruptures to be noncontact in nature, most commonly occurring just before takeoff as the player began to push off from a stopped position, with the foot in dorsiflexion, the knee in early flexion, and the hip in extension.
Conclusion:
In the NBA, a majority of AT ruptures occur early in the season, in veteran players, with almost half not returning to play or starting fewer than 10 games in the remainder of their career. The most common mechanism of injury is taking off from a stopped position just before toe-off in a dorsiflexed foot.
Keywords
Achilles tendon (AT) ruptures are common injuries affecting both recreational and competitive athletes, with an incidence of 18 per 100,000 person-years. 35 A study from Finland by Lantto et al 21 demonstrated a rising incidence of AT ruptures from an incidence of 2.1 per 100,000 patient-years in 1979 to 21.5 in 2011. AT ruptures most commonly occur during athletic competition, among both recreational and competitive athletes. 22 In Europe, AT ruptures occur most commonly during soccer (football), while in America, basketball is cited as the most common cause.22,24
In professional athletes, AT ruptures are devastating injuries, frequently season ending and occasionally career ending. Furthermore, professional athletes frequently experience AT ruptures at an earlier age than their counterparts due to the increased physical demands of elite athletes.1,21,31 Regardless of intervention, these injuries can derail a career, marking the importance of understanding how they occur and how they can be prevented.
Despite basketball being well documented as a major cause of AT ruptures in American recreational athletes, there remains a paucity of literature regarding the epidemiology and mechanism of AT ruptures in professional basketball players. The studies that do exist are limited by their small sample sizes and provide little information on in-game actions that put athletes at risk for AT ruptures.1,2,34 The purpose of this study was to characterize the epidemiology and outcomes of an AT rupture using publicly available archived data of National Basketball Association (NBA) athletes. Additionally, videos of athletes experiencing an AT rupture were analyzed to determine playing situations and lower extremity positions at the moment of injury to further characterize mechanisms of injury. We hypothesized that a player’s performance as measured by Player Efficiency Rating (PER) would decline after AT rupture, and that such an injury would shorten a player’s career.
Methods
AT ruptures in NBA basketball players were identified from 1970 to 2018 using publicly available data from injury reports, press releases, and player profiles, and confirmed by 3 authors (N.J.L., J.E.K., S.T.).5,12,13,30 Player data and performance statistics were collected using a publicly available database. 6 Variables collected included age, position, body mass index (BMI), draft pick, total games started, and PER. PER is a standardized measure of overall player performance commonly used in basketball (see the Appendix, available in the online version of this article).1,2,27,34,38 Injury variables included date of injury, laterality, minutes played before injury, operative versus nonoperative treatment, and time to return to play (RTP). In the present study, RTP was defined as minutes played in at least 1 game after AT rupture, as this suggests that the patient was healthy enough for competitive play and not just recreational or practice play. We also further characterized players that may have returned to play but had suboptimal recovery, which we defined as either a failure to return or a return with fewer than 10 career starts after AT rupture. This criterion was chosen as so few starts after return likely represents poor performance on RTP or persistent pain/disability preventing the player from making the starting lineup. The time of injury during the season was categorized as preseason, early season (first 27 games), midseason (second set of 27 games), late season (third set of 27 games), and postseason (playoffs and finals).
Publicly available videos were identified for 12 AT ruptures.12,13,30,39 Qualitative video analysis was performed individually by 2 authors (N.J.L., S.F.D.). Video analysis software was not used to perform any portion of the video analysis, and therefore quantitative measurements were not performed. The aforementioned authors determined whether AT ruptures were contact in nature, game activity at the time of injury (running takeoff/accelerating, beginning jump, landing from jump, pivot/cut), and various body part positions including foot position (eg, abduction, adduction, neutral, pronation, supination, dorsiflexion, plantarflexion), knee position in the sagittal plane, and hip position (extension vs flexion). The answers were reviewed and compared. Conflicting answers were resolved with a final review by a third author (N.Y.L.).
Univariable and multivariable linear regression were used to compare changes in PER after AT rupture and preinjury PER. To assess the interrater reliability between the independent raters’ video analyses, a Cohen kappa statistic was calculated for each question. Statistical analysis was performed in SAS statistical software v 9.4 (SAS Institute, Inc). Statistical significance was set at P < .05 a priori.
Results
Characteristics of Achilles Tendon Ruptures
Forty-four AT ruptures were identified among NBA players from 1970 to 2018. The mean age was 28.3 years (range, 22-36 years; SD = 3.7), with players averaging 6.8 seasons before AT rupture (range, 0-17 seasons; SD = 3.7) and 2.8 seasons after injury (range, 0-9 seasons; SD = 2.5) (P < .001). Fourteen players were guards (31.8%) and 30 were forwards (68.2%) (P = .006). The average BMI of athletes sustaining an AT rupture was 25.6 kg/m2 (range, 21.4-31.3; SD = 2.3) (Table 1).
Characteristics of NBA Athletes With an AT Rupture a
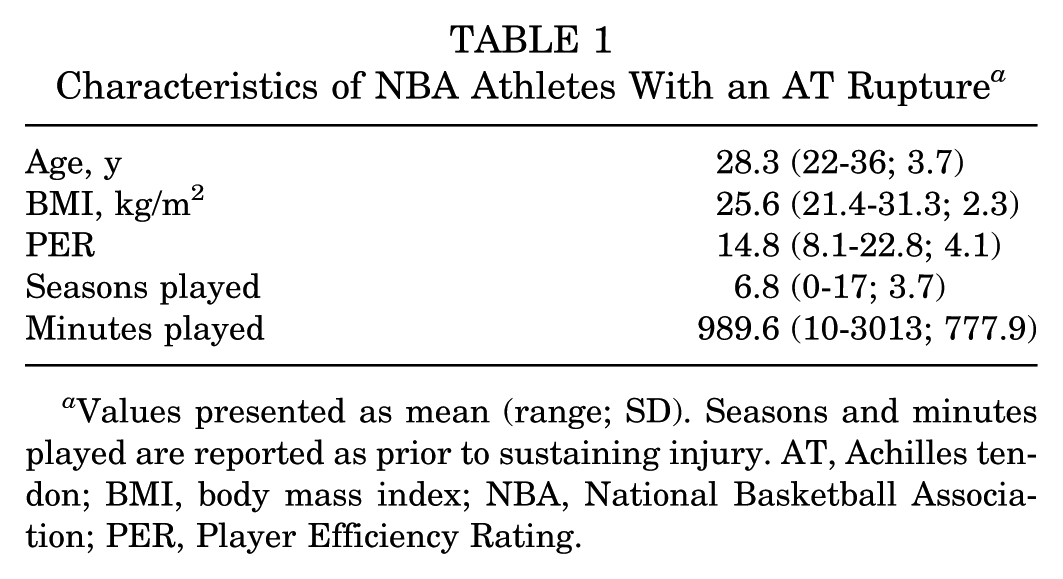
Values presented as mean (range; SD). Seasons and minutes played are reported as prior to sustaining injury. AT, Achilles tendon; BMI, body mass index; NBA, National Basketball Association; PER, Player Efficiency Rating.
Twenty-one injuries (50%) were left-sided and 21 injuries were right-sided (50%). Laterality was not available for 2 injuries. The setting of injury (game vs practice) was identified for 37 (84.1%) injuries. Of the 37 injuries, 29 (78.3%) occurred during a game, while 8 occurred during practice (21.7%). Over the study period, the frequency of AT ruptures peaked during early-season play with 12 of the 44 observed AT ruptures (27.3%) occurring during this segment of each season. Similar rises were observed, although to less of an extent, at the end of the seasons (last 27 games of each season) and during preseason play, with each of these aforementioned season segments accounting for 8 AT ruptures (18.2%) (Figure 1). During the injury season, players were active a mean of 989 minutes (20.6 games) before injury (range, 10-3013 minutes). During the game of injury, AT rupture occurred at a mean of 24.0 minutes (range, 1-47 minutes) into the game. Forty-three (97.7%) injuries were treated operatively.
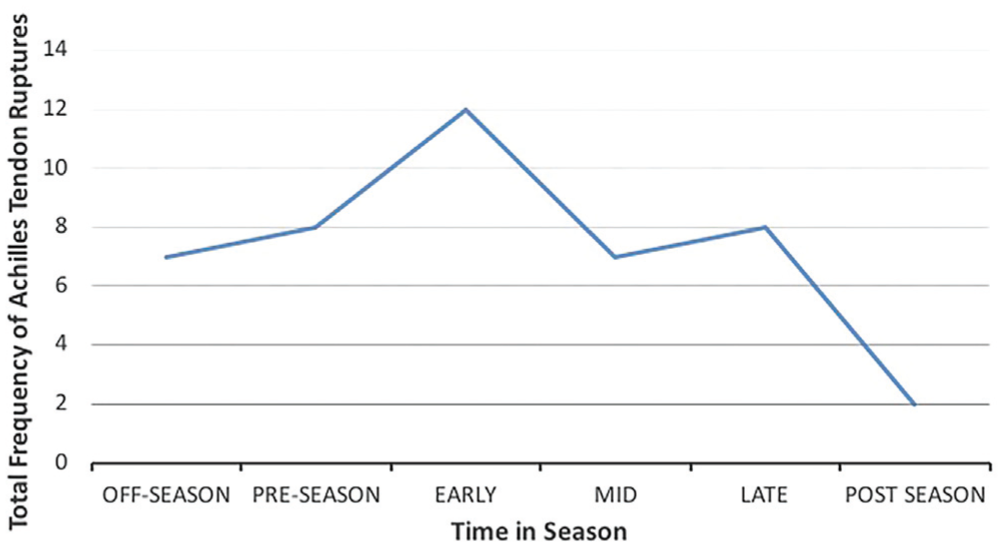
Season-related trends in the frequency of Achilles tendon ruptures in the National Basketball Association from 1969 to 2018.
Return to Play and Suboptimal Recovery
The mean time to RTP was 10.5 months (range, 5-16 months). Thirty-five players (79.5%) returned to play after Achilles tear, with 7 players (15.9%) only returning for 1 season, 28 players (63.6%) returning for 2 or more seasons, and the remaining 9 players (20.5%) retiring. The mean age of players who retired or played less than 1 season after injury was 27.8 years and did not differ from the mean age of those who returned and played more than 1 season (28.5 years) (P = .6). Among players who returned to play, 18 (51.4%) started fewer than 10 career games. Players who returned to play started significantly fewer games during the season in which the athlete returned to play (20.8 games) compared with the season before injury (49.4 games) (P < .01). A lower RTP rate was observed in players younger than 30 years of age (76.7% vs 85.7%, P = .753), in shooting or point guards (64.3% vs 86.7%, P = .516), in players with a BMI less than 25 (72.2% vs 84.6%, P = .129), and in players with a preinjury PER less than 15 (67.9% vs 100%, P = .949) (Table 2). However, none of these relationships reached statistical significance.
Rate of Return to Play After Achilles Tendon Rupture by Patient Characteristic a
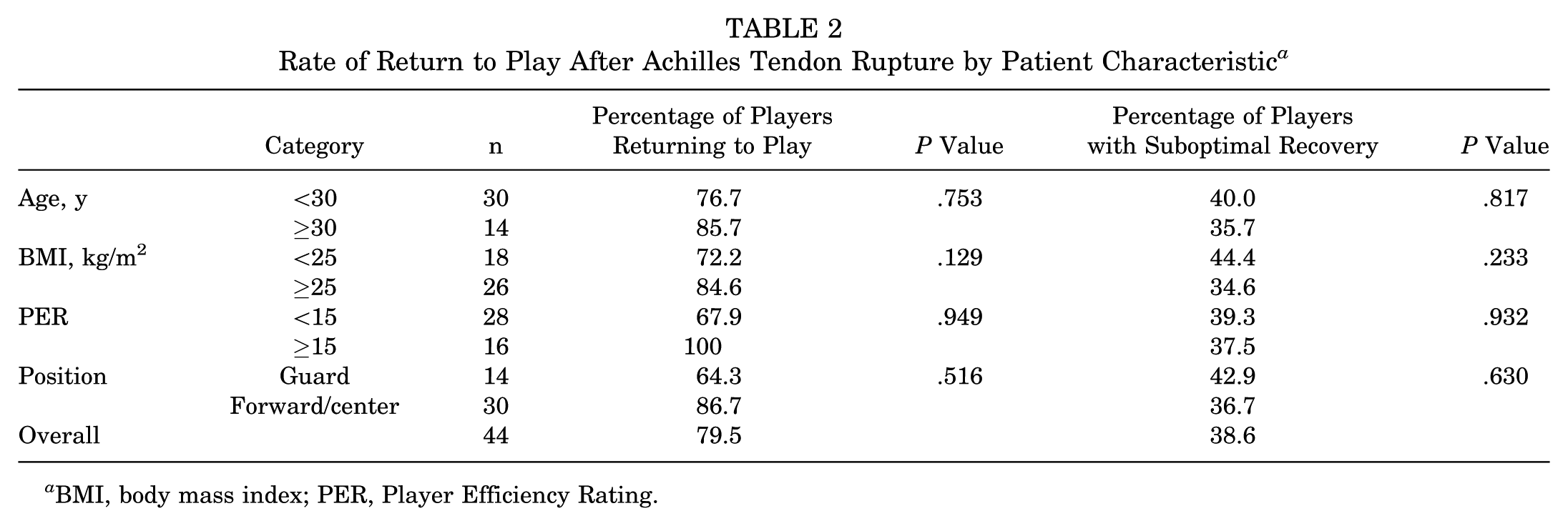
BMI, body mass index; PER, Player Efficiency Rating.
Suboptimal Recovery
Suboptimal recovery was defined as either failure to return or return with fewer than 10 career starts after AT. Seventeen players (38.6%) met this definition of suboptimal recovery after AT rupture. No statistically significant relationships were observed in players who experienced suboptimal recovery in regard to age, BMI, position, or preinjury performance (Table 2).
Performance After Injury
PER declined by an average of 2.9 points after AT rupture (range, –11.5 to +2.3 points) (Table 3). Players with preoperative PER less than 15 (league average) had greater declines in PER after Achilles rupture (P < .001). Injuries in guards (P = .086) and injuries in players age ≥30 years (P = .549) were not associated with greater declines in performance.
Change in Performance After AT Rupture in Returning Players, by Patient Characteristic a
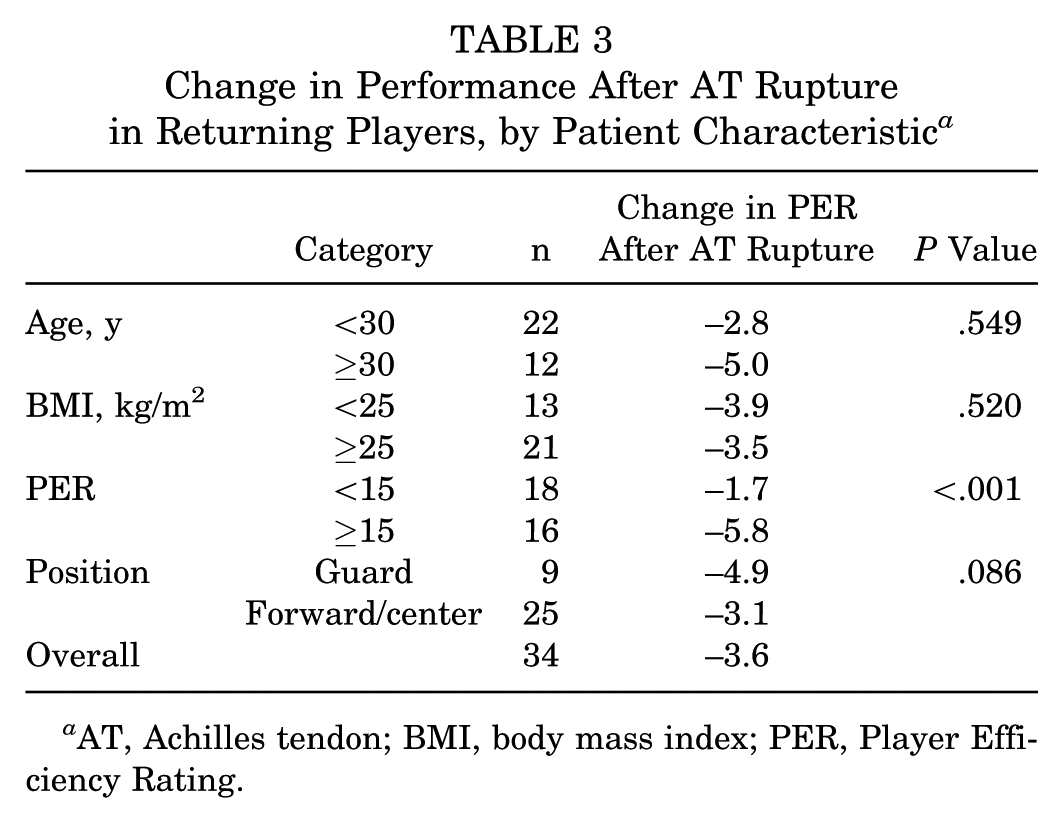
AT, Achilles tendon; BMI, body mass index; PER, Player Efficiency Rating.
Video Analysis
Videos for analysis were available for 12 injuries. There was substantial interrater agreement between the 2 raters when analyzing injury footage, with an overall Cohen kappa of 0.74 for all data and 0.82 regarding the activity at the time of injury (Table 4). All were noncontact injuries. The most common activity at injury was running takeoff/acceleration (67%, n = 8) (Figure 2), followed by pivoting (17%, n = 2) (Table 5). In the transverse and sagittal plane, the foot was most commonly neutral (67%, n = 8) and dorsiflexed (75%, n = 9), respectively. When examining triplanar foot/ankle movements, the foot was most commonly neutral, with only 17% (2/12) in supination and 8% (1/12) in pronation. In the sagittal plane, the knee was in early flexion (0°-45°) in 100% of the injuries, while the hip was most frequently in the extended position (83%, n = 10).
Interrater Reliability of Achilles Tendon Rupture Video Analysis
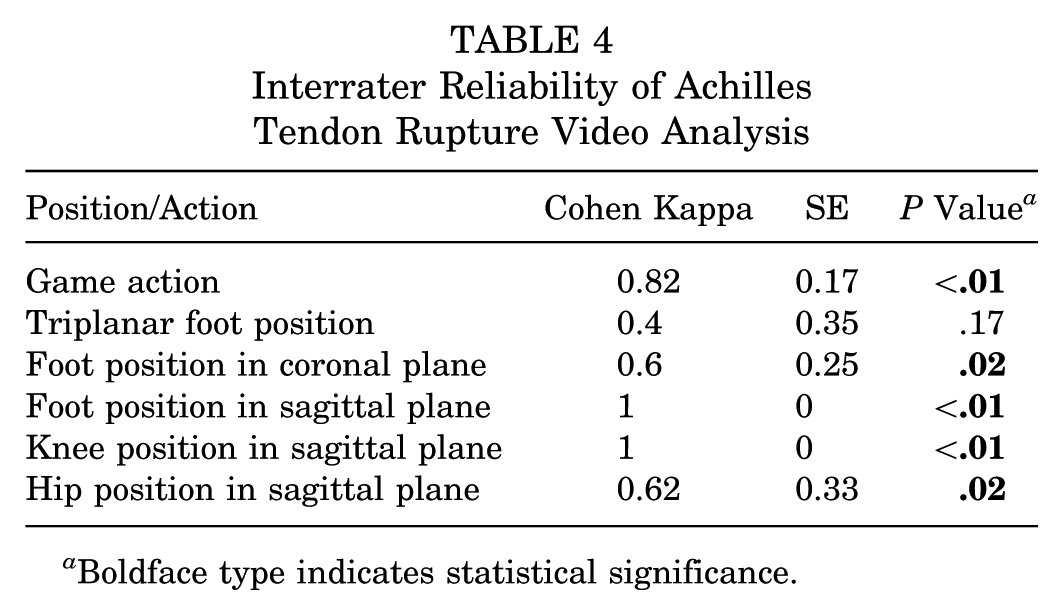
Boldface type indicates statistical significance.
Mechanism of AT Ruptures by Video Analysis a
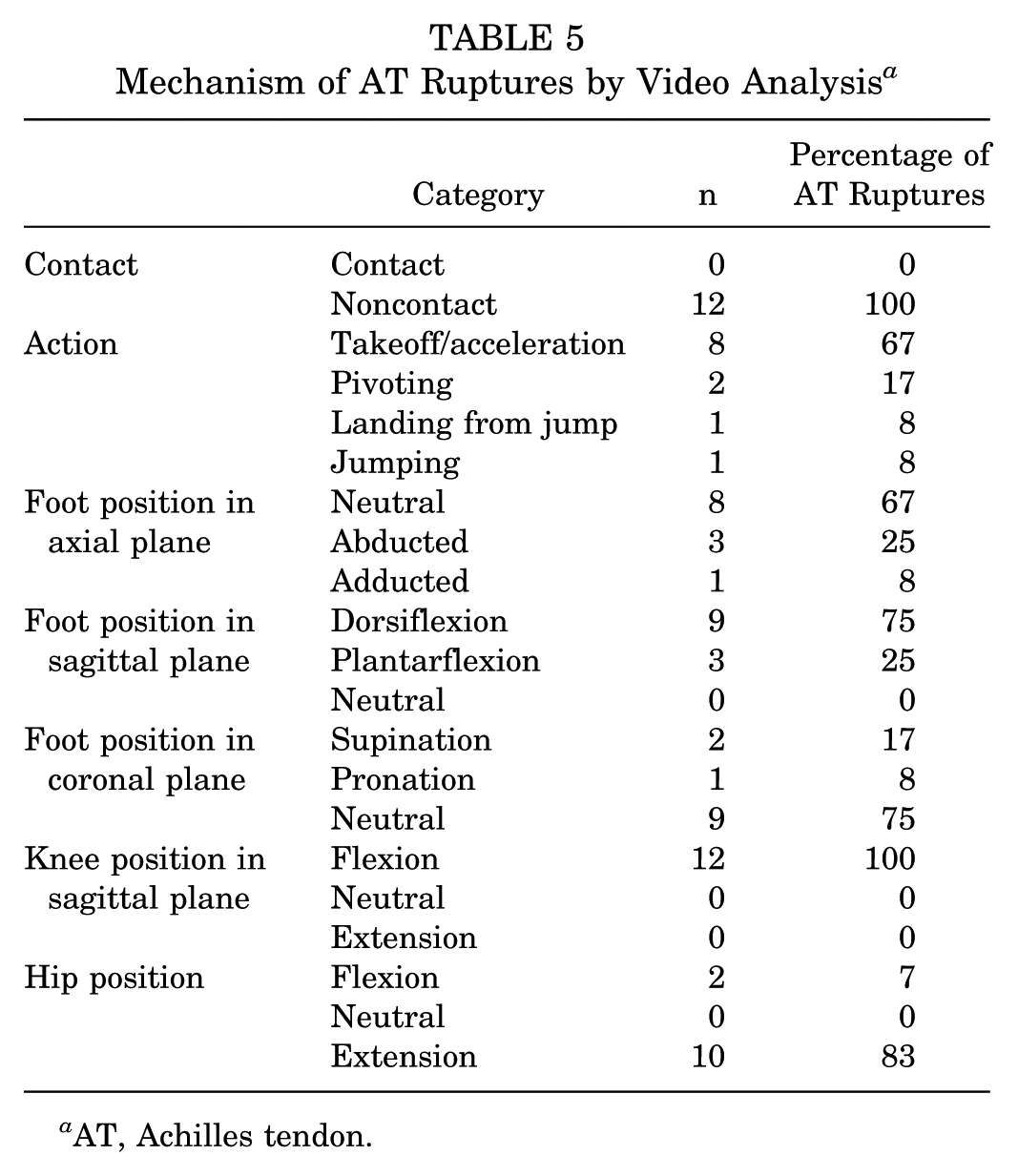
AT, Achilles tendon.

Video analysis demonstrating the most common mechanism of Achilles tendon rupture: takeoff, with the foot dorsiflexed, knee in early flexion, and hip in extension.
Discussion
The prognosis of AT ruptures in NBA players is guarded.2,27 We sought to further characterize the risk factors for AT ruptures in NBA athletes, as previous studies have been limited by small sample sizes and a lack of mechanistic data. We identified 44 NBA athletes who sustained an AT rupture. Of those sustaining an AT rupture, 36.8% of players did not return to play or started in fewer than 10 games in the remainder of their career. Athletes who returned to play missed on average 10.5 months and saw a significant decline in their performance. Players who had poorer performances before their injury, represented by their PER, saw a significantly larger decline in their performance compared with those who had a PER above the league average before injury. By studying the mechanism of injury using video footage, we discovered all AT ruptures to be noncontact injuries, with 67% of injuries occurring during takeoff as the player pushed off from a stopped position, with the AT eccentrically contracting, the foot in dorsiflexion, the knee in early flexion, and the hip in extension.
Despite the overall low frequency of AT ruptures, previous studies support our findings, demonstrating devastating outcomes in professional athletes. Trofa et al 34 investigated the difference in outcomes after AT rupture between professional athletes in the NBA, National Football League (NFL), and Major League Baseball, illustrating RTP rates of 68.0%, 65.6%, and 100%, respectively. Despite a slightly larger percentage of NBA athletes returning to play compared with those in the NFL, the performance of NBA athletes suffered the most, with the largest decline in games played, playing time, and PER upon RTP. The seriousness of AT rupture in NBA athletes is further emphasized by Minhas et al, 27 who compared performance and RTP after 7 different orthopaedic procedures in NBA athletes. The authors found that of all the procedures, athletes who suffered an AT rupture and underwent an AT repair not only had the lowest RTP rate (70.8%) but also experienced the largest decline in performance.
Compared with the outcomes after AT rupture observed by Amin et al 2 in a cohort of 18 NBA players, the players in the present study had a higher RTP rate (79.5% vs 61%) and less of a decline in performance, represented by their PER (−2.9 vs −4.38). Potential explanations for the decreased RTP observed may be due to the older age of the players in the study (29.7 vs 28.3 years) and the greater number of seasons played before injury (7.6 vs 6.8). Furthermore, the aforementioned study may be limited by the small patient cohort used for investigation (18 vs 44 players). Parekh et al 31 observed similar outcomes after AT rupture in NFL players. Athletes sustaining an AT rupture in the NFL had an average age of 29 years and a mean of 6 seasons played before injury. Compared with NBA athletes, the ramifications of AT ruptures were even worse with only 67.7% of players returning to play after injury, with more than a 50% decrease in performance upon RTP, represented by the athlete’s power rating. 31
To prevent AT rupture, it is important to identify athletes at risk and develop measures to decrease the prevalence of injury. Rupture of the AT tendon is thought to be a chronic degenerative issue that leads to eventual acute rupture. 7 Upon histological analysis of ATs that spontaneously rupture, up to 97% of the tendons have evidence of degenerative changes consistent with tendinosis, despite many patients denying prodromal symptoms. 16 Such findings may explain why in the general population AT ruptures are most common in the third and fourth decades of life. 33 Professional athletes competing at the highest level may potentially accelerate this process due to the large volume of training they undergo.26,35 In the present study, the average age of those sustaining AT ruptures was 28.3 years, almost 2 years older than the league average of 26.8 years, but much younger than the age of recreational athletes who sustain AT injuries. 11
Over the study period, the frequency of AT ruptures peaked during early-season play with 12 of the 44 observed AT ruptures (27.3%) occurring during this segment of each season, with similar rises (although to less of an extent) occurring during preseason play (18.2%, n = 18) and at the end of each season (18.2%, n = 18). This is the first known report to demonstrate an increased risk of AT rupture in the pre- and early season, which together accounted for 45.5% of all AT ruptures identified during the study period. A similar trend has been identified in collegiate basketball, with the largest injury incidence occurring in preseason (12.1 per 1000 athlete exposures [AEs]) compared with in-season (10.1 per 1000 AEs) and postseason injury incidences (6.4 per 1000 AEs). 8 Similar trends have been observed in other sports as well. Woods 37 analyzed preseason English professional football (soccer) injuries over 2 competitive seasons and found the incidence of AT injuries in preseason to be almost triple the in-season incidence, with 3.5 AT injuries per week of preseason compared with only 1 per week during the regular season. The second rise in injury prevalence observed in this study at the end of each season may be explained by athlete fatigue secondary to the large quantity of NBA regular season games played, with the typical season consisting of 82 regular season games, compared with just 16 and 32 games in the NFL and Major League Soccer seasons, respectively.25,29 Recent data by Lewis 23 in 2018 support this theory demonstrating the risk of injury in NBA athletes to increase 2.87% (P < .001) for each 96 minutes of game play and a 15.96% (P < .001) decrease in the risk of injury for each day of rest.
Multiple extrinsic factors may be responsible for the increased incidence of AT ruptures observed early in the season, which include the abrupt increase in training volume/intensity and the propensity to do repetitive drills and novel plyometric activities during preseason.14,20,35,37 This abrupt increase in training volume during preseason likely causes athletes to fatigue, which has been shown to cause impairments in timing and neuromuscular coordination, both of which are known risk factors for injury. 9 Additionally, a greater proportion of running takes place during preseason to condition athletes for season game play. Repeated days of heavy running has been shown to deplete muscle stores in the gastrocnemius, which assists the AT with shock absorption and locomotion. When this muscle becomes fatigued, increased stress is placed on the AT. 3 Numerous studies support this notion and suggest that the increased injury rates observed during preseason are correlated with the volume, duration, and frequency of running done by the athletes.19,37 These findings highlight the importance of insightful monitoring of preseason training volume, and the allowance for adequate neurological and physiological recovery.
Video analysis has been widely used to better understand the mechanisms of various injuries including ankle sprains and anterior cruciate ligament injuries at both the collegiate and the professional level across multiple sports.4,18,28 However, to date there is a paucity of data regarding the movements and mechanisms of AT rupture in athletes. Despite jumping being cited as a common mechanism of AT rupture, little objective data can be found in the literature to support this. Rather, this perception has been molded by the high incidence of AT rupture in sports that require frequent jumping.10,15,21,36 Video analysis of AT can be used to objectively identify injury mechanisms and extremity positions at the time of injury. An understanding of such information can subsequently be used to develop preventative training programs.
In the present study, all AT ruptures were noncontact injuries, with the most common action at the time of injury being a takeoff movement (67%), followed by pivoting (8%). The most common foot position at the time of injury was neutral in the transverse plane and dorsiflexed without any supination or pronation of the foot. Furthermore, the knee was most commonly in early flexion with the hip extended. The anatomic and biomechanical properties of the AT support such a mechanism. Just before takeoff, when the foot is planted in dorsiflexion, the calf musculature undergoes eccentric contraction to prevent falling over the planted foot. At this time, energy is stored in the AT as elastic energy, which ultimately assists in propulsion. As the triceps surae violently contracts, the foot is plantarflexed, allowing for takeoff during a sprint. It has been shown that the force delivered through the AT at this moment approaches 6 to 8 times one’s body weight, potentially exceeding the ultimate strength of the tendon and resulting in rupture.17,32
There are several limitations to this study. Its retrospective design prevents obtaining the athletes’ medical information as to the type of surgical treatment, the severity of tissue injury, or the duration and form of postoperative rehabilitation. Additionally, it is unclear if these athletes had other extrinsic risk factors for AT rupture such as anabolic steroid or fluoroquinolone use. Furthermore, since injury data were obtained from public records, they may not be 100% accurate, nor are we able to confirm that every athlete with an AT rupture during the study period was captured. However, similar methods have been used in numerous previous studies and are accepted in the sports medicine community.18,27,34 Limitations also exist in regard to the injury video analyses. Unfortunately, video footage could only be obtained for 27% (12/44) of the documented injuries, and the videos were of varying quality, as not all clips provided multiple camera angles or zoomed-in footage of the injury mechanism. Despite these limitations, this study provides valuable information to the sports medicine community as it investigates the largest cohort of professional basketball players sustaining AT ruptures to date, and this is the first paper to highlight the actions and body positions of athletes at the time of AT rupture.
In conclusion, we confirm the findings of previous smaller studies that highlight the guarded prognosis of AT rupture in professional athletes. NBA athletes were most at risk for rupture early in the season, with smaller peaks in the injury incidence observed during preseason and at the end of the season. Of the athletes who sustained an AT rupture, 36.4% retired or played in less than 1 season upon returning to play. Those who did return to play had a significant decline in their performance. Interestingly, those who performed at a higher level before injury were less likely to suffer as large of a decline compared with those with worse performance before injury. Finally, we demonstrated the most common mechanism of AT rupture in NBA athletes to be taking off from a stopped position with the foot in dorsiflexion, the knee in early flexion, and the hip in extension. There are currently no definitive guidelines or evidence-based therapy programs for AT injury prevention. It is therefore likely that there is variability in the approaches for prevention among sports medicine professionals. The lack of robust evidence for prevention of such an impactful injury as AT ruptures in athletes demonstrates the need for future studies on AT injury–specific prevention techniques and programs.
Supplemental Material
DS_10.1177_0363546519858609 – Supplemental material for Epidemiology and Video Analysis of Achilles Tendon Ruptures in the National Basketball Association
Supplemental material, DS_10.1177_0363546519858609 for Epidemiology and Video Analysis of Achilles Tendon Ruptures in the National Basketball Association by Nicholas J. Lemme, Neill Y. Li, Justin E. Kleiner, Sydney Tan, Steven F. DeFroda and Brett D. Owens in The American Journal of Sports Medicine
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.D.O. is an associate editor of The American Journal of Sports Medicine; has received consulting fees from CONMED Linvatec, DePuy Synthes, DePuy Orthopaedics, Flexion Therapeutics, Mitek, Musculoskeletal Transplant Foundation, and Vericel; and has received research support from Histogenics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.