
Abstract
Background:
Dorsiflexion closing wedge metatarsal osteotomy (DCWMO) has been considered the traditional treatment of Freiberg disease. Several case reports presented osteochondral autologous transplantation (OAT) as an alternative treatment.
Purpose/Hypothesis:
The purpose was to compare the results of DCWMO versus OAT for the treatment of Freiberg infraction in an athletic population. It was hypothesized that OAT was superior to DCWMO regarding functional outcomes, pain, and the time that the athletes returned to training and to previous sport level.
Study Design:
Randomized controlled trial; Level of evidence, 2.
Methods:
Between 2008 and 2013, 27 consecutive patients with Freiberg disease were randomly assigned to either the DCWMO group (14 patients) or the OAT group (13 patients). The primary outcomes collected were as follows: postoperative complications, range of motion of the metatarsophalangeal joint, length of the metatarsal, function of the foot (measured with the American Orthopaedic Foot and Ankle Society–lesser metatarsophalangeal-interphalangeal [AOFAS-LMI] score), and pain (assessed with the visual analog scale–foot and ankle score).
Results:
Mean follow-up was 46 months (range, 36-60 months). The mean ± SD AOFAS-LMI score in the DCWMO group was 63.4 ± 14.4 preoperatively, 81.8 ± 6.6 at 1 year postoperatively, and 84.4 ± 5.6 at 3 years postoperatively, while in the OAT group, it was 62.8 ± 14, 89.9 ± 7.1, and 92 ± 6.9, respectively (P < .001). The differences in the AOFAS-LMI scores favoring the OAT group at 1 and 3 years reached statistical but not clinical significance. The mean visual analog scale–foot and ankle score was improved significantly from 48.1 ± 11.5 to 91.8 ± 9.5 in the DCWMO group and from 49.9 ± 10.9 to 95.4 ± 4.4 in the OAT group. There was a shortening of the metatarsals by a mean 1.9 ± 0.5 mm in the DCWMO group, as opposed to a metatarsal lengthening of 0.2 ± 0.1 mm in the OAT group. In the OAT group, patients were able to start training at 6 ± 1 weeks (P < .001) and return to full sport action at 10 ± 2.5 weeks (P < .05), while in the DCWMO group, the time was 8 ± 1.5 and 13 ± 2.5 weeks, respectively.
Conclusion:
The authors concluded that OAT is equal to DCWMO. Acceptable clinical results were reported, as well as very low morbidity and early return to sport activities. That makes the OAT procedure a safe, effective, and optimal treatment for an athletic population experiencing Freiberg infraction.
Keywords
Freiberg disease or infraction is an osteochondrosis of the metatarsal heads, more commonly seen in the head of the second metatarsal. This condition was originally described in 1914 by A. H. Freiberg and was attributed to trauma. 10 Although a general consensus of the etiology has not been established, the following have been advocated as the potential causes: single or repetitive trauma, epiphysial ischemia caused by arterial spasm, and a combination of multiple factors, such as rigidity of central ray, shoes, hormonal abnormalities, growth disturbances, and family history.8,36
Nonoperative treatment is rooted in decreasing foot pressure and unloading the affected metatarsal. Stiff-soled shoes, casting, orthotics, and modified physical activities are employed to rest the joint, allowing for resolution of inflammation and mechanical irritation. 8
Surgical management is typically performed when nonoperative therapy fails. Dorsiflexion closing wedge osteotomy of the metatarsal head (DCWMO), which was initially presented by Gauthier and Elbaz, 11 has been widely used in the original or modified versions5,15,17,21 and has been considered the gold standard for the treatment of Freiberg disease. 15
Osteochondral autologous transplantation (OAT) is one of the well-accepted surgical options to treat osteochondral lesions of the knee and the ankle.12,13 Recently published case reports presented OAT for the treatment of Freiberg disease. Although the studies reported promising results, there are no comparative studies between the methods.7,14,28,29,36
The purpose of our study was to compare the results of DCWMO versus OAT for the treatment of Freiberg infraction in the athletic population. We hypothesized that OAT was superior to DCWMO regarding functional outcomes, pain, and time to return to training and previous sport level. To our knowledge, this is the only study in the literature that directly compared the 2 surgical methods.
Methods
This was a prospective randomized controlled single-surgeon study. Institutional research board approval was obtained before the initiation of the trial. All patients enrolled in the study signed an informed consent form. Each patient was assigned to either the DCWMO group or the OAT treatment group by means of a computer-generated random number.
Patients
Between 2008 and 2013, 27 consecutive patients with Freiberg disease were enrolled for this study. Chart numbers were randomly assigned to treatment groups: a patient was assigned to the DCWMO group if the chart number was odd and to the OAT group if it was even. Inclusion criteria included the following: adult patients (>16 years) participating in professional or recreational sports activities, pain on walking and during daily activities that affected the overall athletic performance, and failed nonoperative treatment after 6 months of implementation. Exclusion criteria comprised severe osteoarthritic changes of the metatarsophalangeal (MTP) joint and excessively altered anatomy of the foot that required additional operation (hallux valgus, pes cavus, pes planus).
Methods of Assessment
The primary outcomes collected in the present study were as follows: postoperative complications, range of motion (ROM) of the MTP joint, length of the metatarsal, time to return to training and previous sport level, and function of the foot. Functional outcome was measured with the American Orthopaedic Foot and Ankle Society–lesser MTP-interphalangeal (AOFAS-LMI) score (range, 0-100 points) preoperatively and at 12 and 36 months postoperatively. 22 Pain was assessed with the visual analog scale–foot and ankle score (range, 0-100 points). 32 Anteroposterior and lateral radiographs in the standing position and magnetic resonance imaging scan were used to analyze the sphericity and viability of the metatarsal head and the length of the metatarsal with bone union and graft incorporation postoperatively. Radiological staging of the cases was based on the Smillie classification system 34 : stage I—subtle fracture of the subchondral epiphysis; stage II—collapse of dorsal portion of metatarsal head flattening; stage III—further collapse, depression, and widening of the metatarsal head; stage IV—loose body formation and complete central separation of the articular fragment; stage V—end-stage degeneration, widening of the head, loss of joint space.
Patients were followed up at 2 weeks for wound check, at 6 weeks for radiographic assessment, and at 3 and 12 months and 3 years for clinical assessment.
Surgical Technique
Both techniques were performed with the patient in the supine position after intravenous administration of 1.5 g of cefuroxime (Glaxo-Smith-Kline) before inflation of a thigh tourniquet to 300 mm Hg. A longitudinal dorsal incision was made over the affected MTP joint. Capsulotomy was performed longitudinally just medial to the extensor tendons, and the extensor digitorum longus and brevis tendons were retracted laterally. The hyperplastic synovium was removed, and debridement of loose fragments was carried out.
In the DCWMO group, a dorsal closing wedge osteotomy performed. The osteotomy was intra-articular, and the entire dorsal articular defect was excised with an oscillating saw while the plantar articular hinge was preserved. The metatarsal head was rotated proximally and dorsally, bringing the healthy plantar part of the articular surface into articulation with the phalanx. The osteotomy site was fixed with 2-0 nonabsorbable sutures (FiberWire; Arthrex).
In the OAT group, the necrotic articular defect was entirely curetted to expose the underlying sclerotic bone. The OAT System (OATS; Arthrex) was used for the recipient site preparation and the osteochondral plug harvesting and transplantation. The diameters of the plug and the recipient socket were determined by measuring the size of the cartilage defect with sizers. An osteochondral plug was arthroscopically cored out from the lateral edge of the lateral trochlea of the ipsilateral knee or the anterior edge of the articular surface of the ipsilateral talus (Figure 1). The depth of the recipient socket was measured, and the osteochondral plug was trimmed accordingly and finally impacted with a larger tamp to be flush with the surrounding cartilage surface (Figure 2).
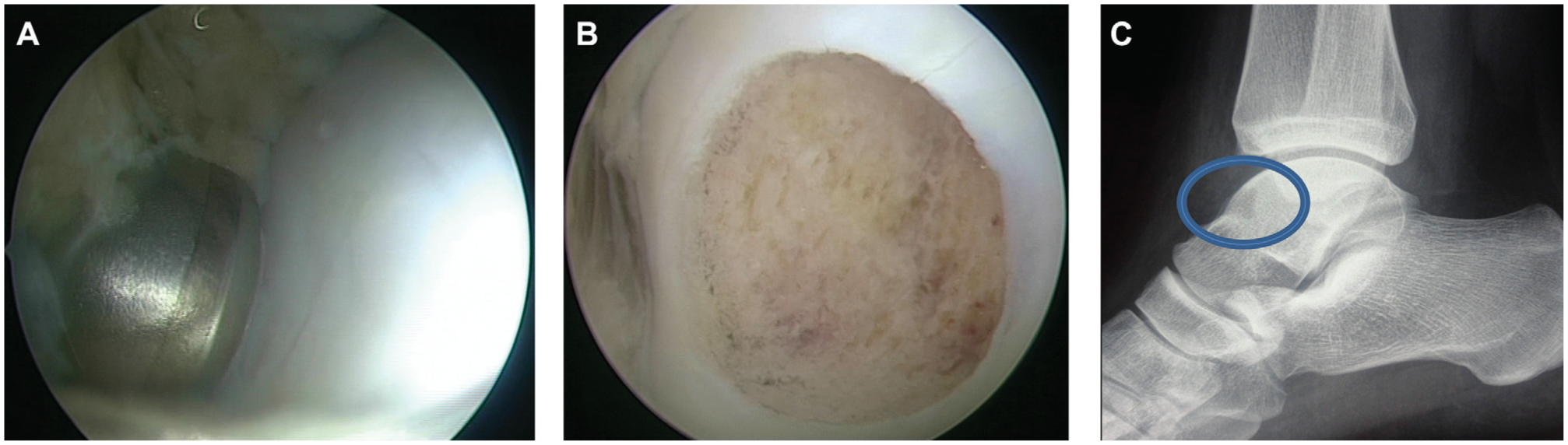
(A, B) Arthroscopic harvesting of an osteochondral graft from the anterior edge of the articular surface of the ipsilateral talus as viewed from the anteromedial portal. (C) Lateral radiograph of the ankle shows the donor site (circle) at the anterior edge of the talus.
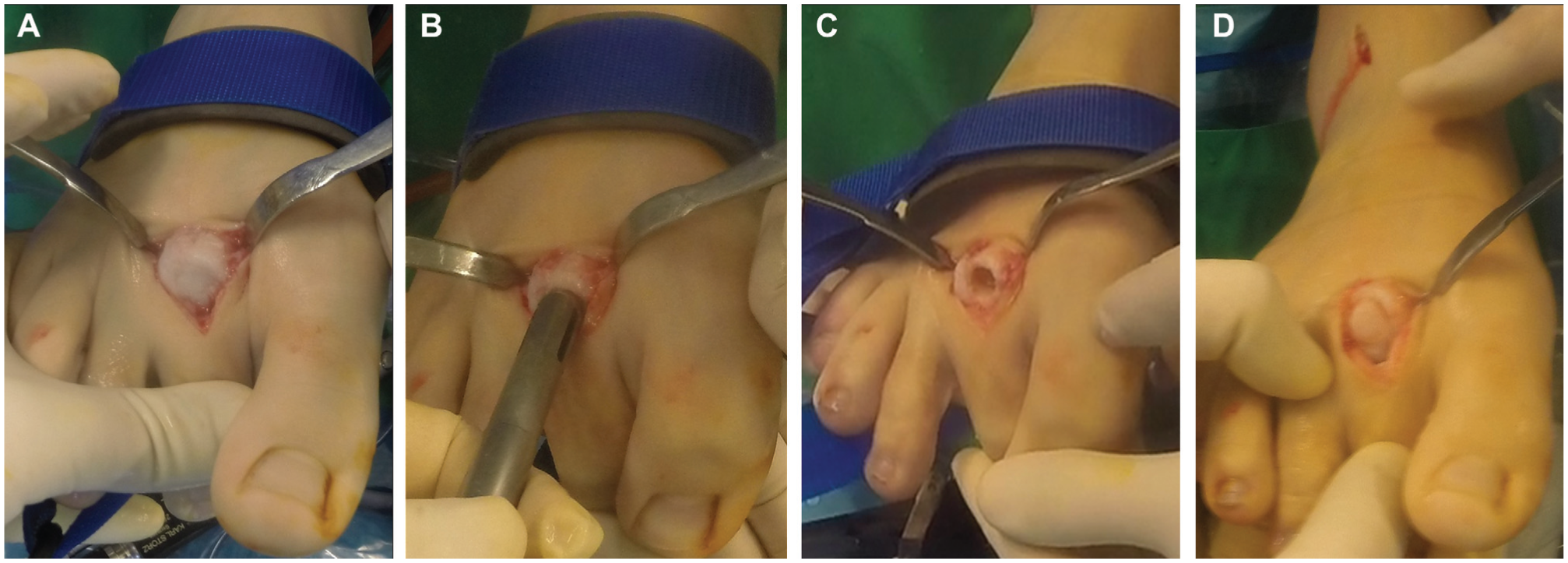
Surgical technique of OAT for the treatment of Freiberg infraction of the second metatarsal head. (A) The head of the second metatarsal is exposed through a dorsal approach, revealing a dorsal articular defect. (B, C) The recipient site is prepared with the OAT system. (D) The osteochondral plug is impacted flush with the surrounding cartilage surface of the second metatarsal head. OAT, osteochondral autologous transplantation.
At the end of both techniques, the joint capsule was roughly sutured and the skin incision closed with absorbable sutures.
Postoperative Management
No means of immobilization was applied postoperatively. All patients were allowed heel weightbearing for 4 weeks, and active toe flexion-extension exercises started from the first postoperative day. Full weightbearing gait was allowed at 4 weeks and running at 8 weeks.
Statistical Analysis
Statistical analysis with the unpaired Student t test and the Fisher exact test was implemented for quantitative and qualitative variables, respectively (SPSS, v 13.0; IBM). Statistical significance was defined at the 5% level (P < .05).
The preliminary sample size calculation suggested that, with a 5% probability of a type I error (P < .05) and a power of 80% (type II error, 0.20), a sample size of 24 patients (12 patients in each group) was necessary to detect the minimal clinically important differences 4 of 19 points in the AOFAS-LMI score between the groups.
Results
Between 2008 and 2013, 33 patients with Freiberg infraction syndrome were examined in the foot and ankle clinic. Twenty-eight patients were identified to be eligible, and all agreed to participate in the study. Finally, 27 patients were randomly assigned into 2 therapeutic groups (Figure 3). Fourteen patients were treated with DCWMO and 13 with OAT. Patient data are shown in Table 1.
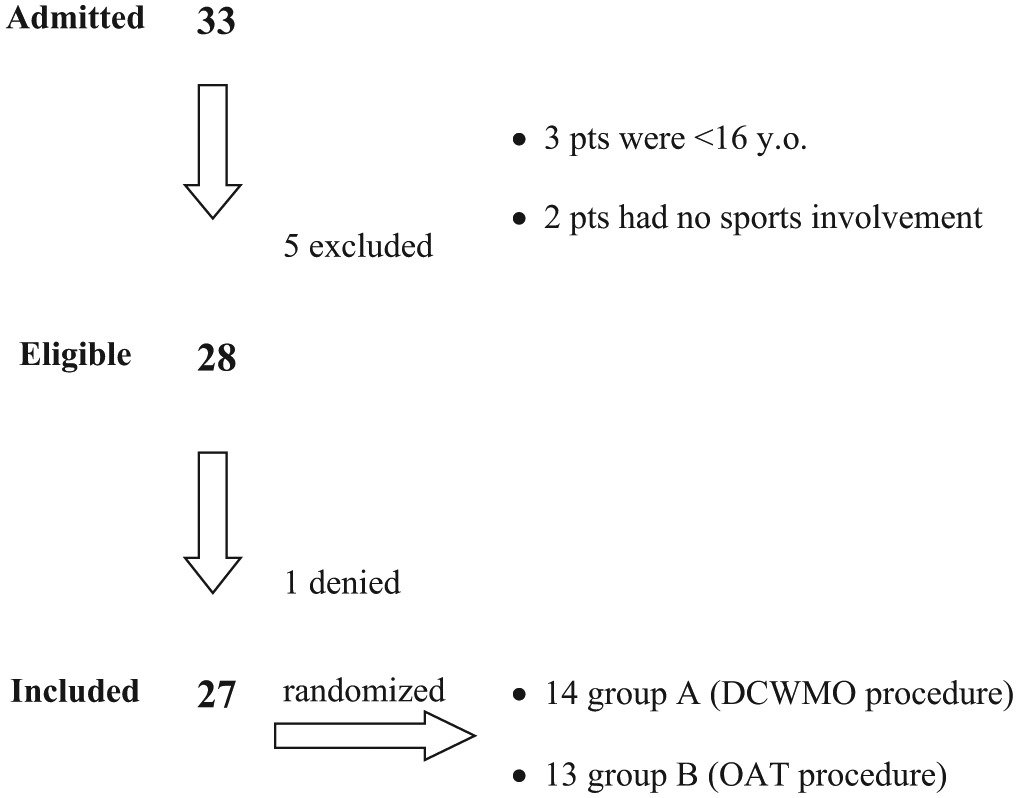
Flowchart of participants in the study. DCWMO, dorsiflexion closing wedge metatarsal osteotomy; OAT, osteochondral autologous transplantation.
Patient Data a
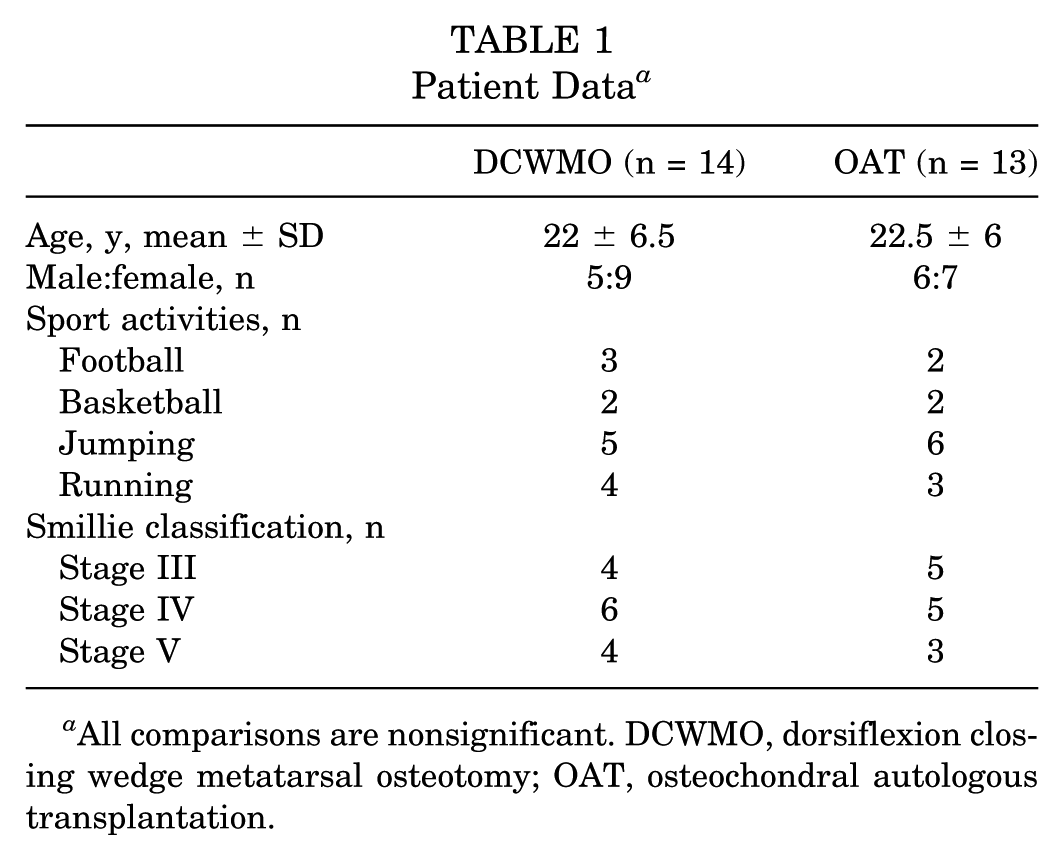
All comparisons are nonsignificant. DCWMO, dorsiflexion closing wedge metatarsal osteotomy; OAT, osteochondral autologous transplantation.
The period of follow-up was 46 months (range, 36-60 months) (Figures 4 and 5). The mean ± SD AOFAS-LMI score in the DCWMO group was 63.4 ± 14.4 preoperatively, 81.8 ± 6.6 at 1 year postoperatively, and 84.4 ± 5.6 at 3 years postoperatively, while in the OAT group, it was 62.8 ± 14, 89.9 ± 7.1, and 92 ± 6.9, respectively. There was a significant difference in favor of the OAT group between the postoperative values at 1 year (P = .001) and 3 years (P < .001). However, the differences in the AOFAS-LMI scores favoring the OAT group at 1 and 3 years reached statistical but not clinical significance. The mean visual analog scale–foot and ankle score improved significantly from 48.1 ± 11.5 to 91.8 ± 9.5 in the DCWMO group (P < .001) and from 49.9 ± 10.9 to 95.4 ± 4.4 in the OAT group (P < .001). However, no statistical significance was found between the postoperative values of the 2 groups (P = .02) (Table 2).
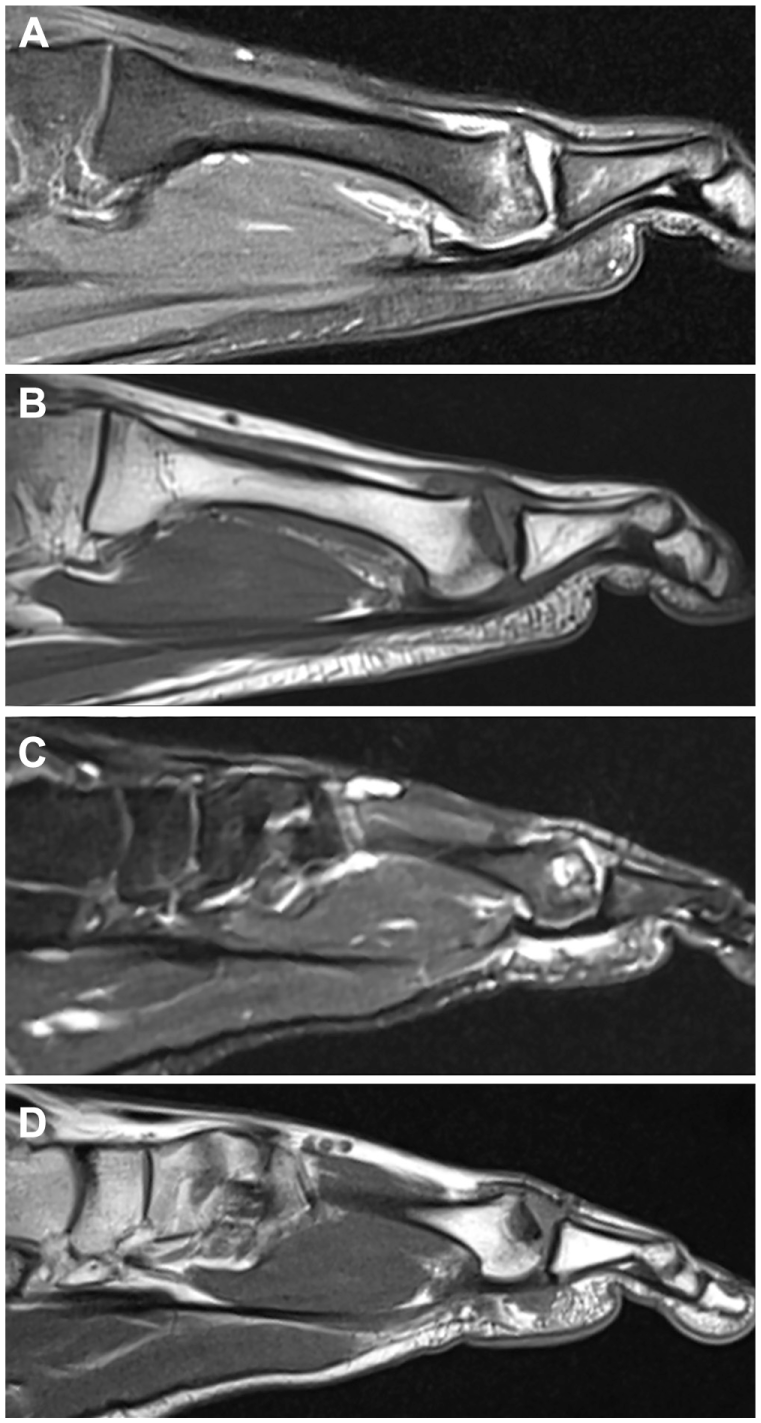
(A, B) Preoperative magnetic resonance imaging scan (sagittal T1 and T2 images) of a 24-year-old athlete shows stage III Freiberg infraction of the second metatarsal head. (C, D) Six-month postoperative scan shows a well-incorporated osteochondral autologous plug.
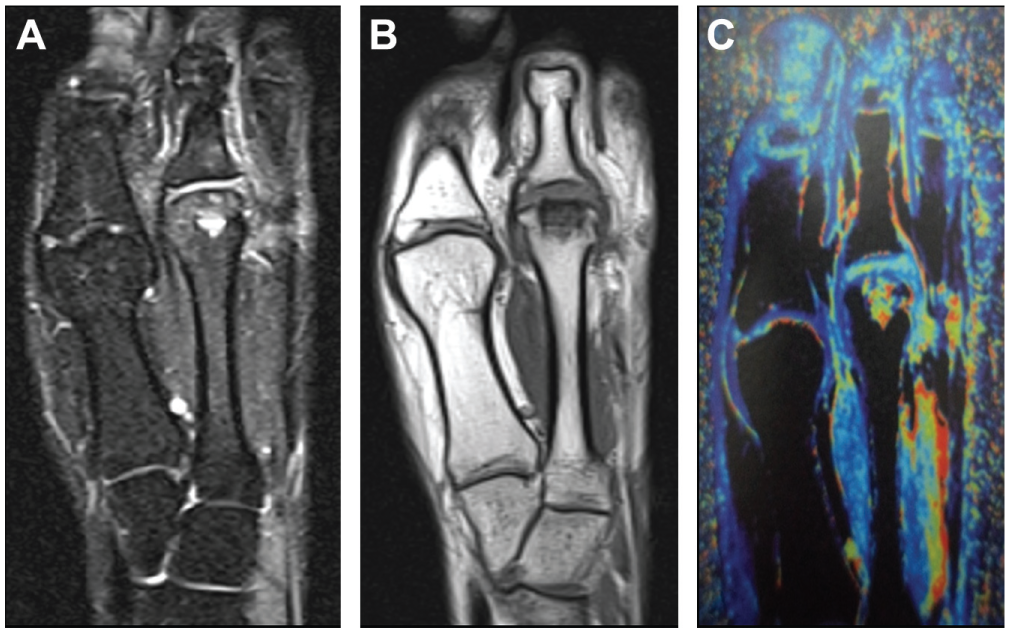
(A, B) Coronal views (T1, T2, and chromatographic) of a 6-month postoperative magnetic resonance imaging scan show a well-preserved shape of the articular surface and (C) satisfactory incorporation of the osteochondral graft with viability of the articular cartilage.
Results and Scoring Data a
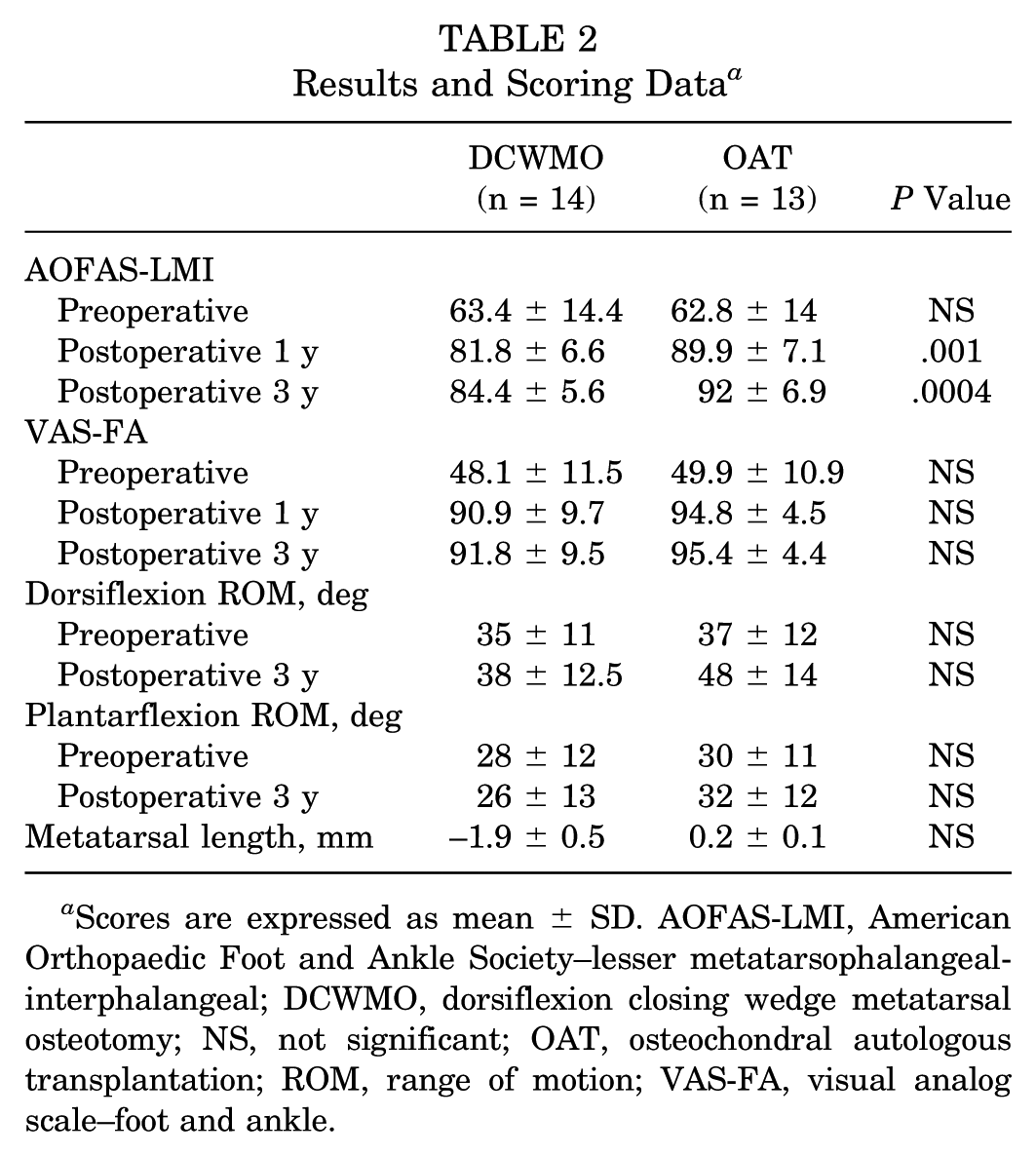
Scores are expressed as mean ± SD. AOFAS-LMI, American Orthopaedic Foot and Ankle Society–lesser metatarsophalangeal-interphalangeal; DCWMO, dorsiflexion closing wedge metatarsal osteotomy; NS, not significant; OAT, osteochondral autologous transplantation; ROM, range of motion; VAS-FA, visual analog scale–foot and ankle.
Bone union was achieved at 6 weeks for all patients of both groups (Figure 6). There was a shortening of the metatarsals by a mean 1.9 ± 0.5 mm in the osteotomy group, as opposed to a metatarsal lengthening of 0.2 ± 0.1 mm in the OAT group. In the DCWMO group, dorsiflexion increased from 35°± 11° to 38°± 12.5°, and plantar-flexion decreased slightly from 28°± 12° to 26°± 13°. In the OAT group, dorsiflexion increased from 37°± 12° to 48°± 14° and plantarflexion from 30°± 11° to 32°± 12°. No statistical difference was detected between the groups (Table 2).
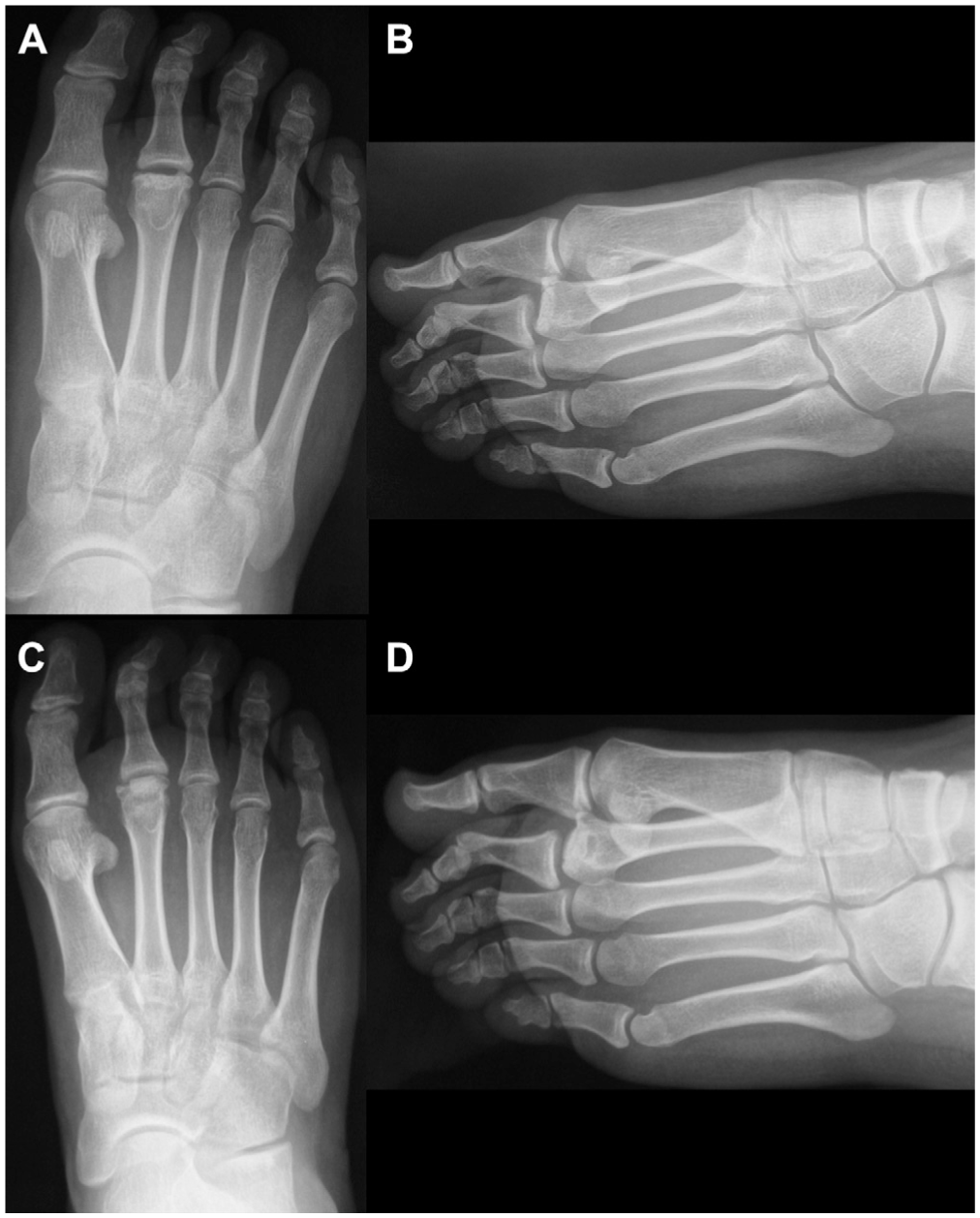
(A, B) Preoperative right foot anteroposterior and lateral radiographs of a 22-year-old soccer player show symptomatic Freiberg infraction of the second metatarsal head. (C, D) Four-month postoperative anteroposterior and lateral views show the reconstruction of the articular surface and the osteochondral graft in place.
Patients treated with the OAT procedure returned to sport activities earlier than the patients treated with metatarsal osteotomy. In the OAT group, patients were able to start training at 6 ± 1 weeks and to return to full sport action at 10 ± 2.5 weeks, while in the DCWMO group, the time was 8 ± 1.5 weeks and 13 ± 2.5 weeks, respectively. There was significant difference in favor of the OAT group in time to return to training (P < .001) and to previous sport level (P < .05) (Table 3).
Time to Return to Sport Activities: Results a
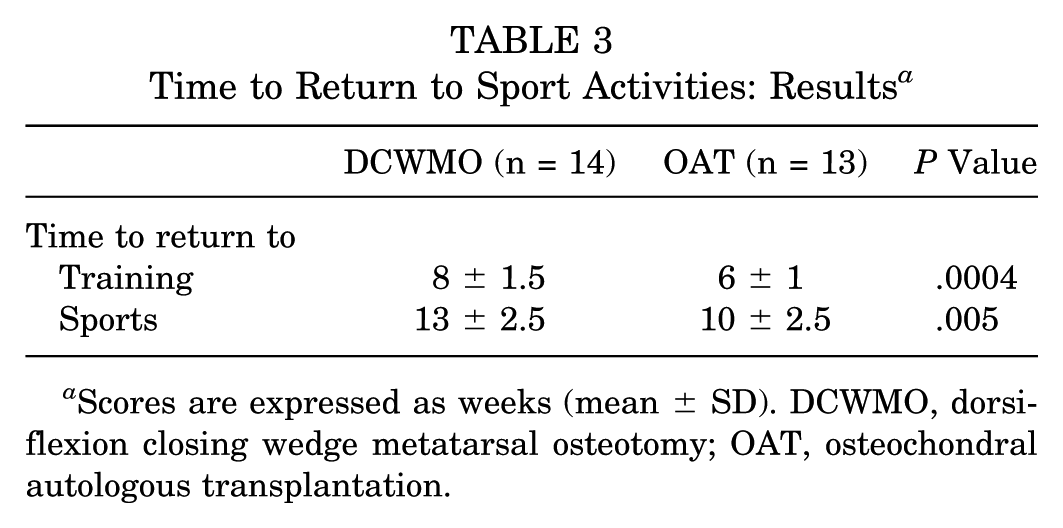
Scores are expressed as weeks (mean ± SD). DCWMO, dorsiflexion closing wedge metatarsal osteotomy; OAT, osteochondral autologous transplantation.
Two complications were encountered, both in the DCWMO group. One patient complained of residual ache and stiffness of the second MTP joint, but no further surgical treatment was required. The other patient, with DCWMO of the second metatarsal, complained of transfer metatarsalgia of the third and fourth MTP joints. After several courses of physical therapy without any improvement, a Weil osteotomy of the third and fourth metatarsal heads was performed uneventfully.
There was no donor site morbidity in the OAT group. Nine plugs were harvested from the anterior edge of the ipsilateral talus, and 4 plugs were cored out from the lateral trochlea of the ipsilateral knee.
Discussion
Surgical treatment of Freiberg disease is divided into 2 basic categories: joint-sparing and joint-destructive procedures.3,33 The first comprises procedures that attempt to alter the abnormal physiology and biomechanics that may predispose an individual to the disease. These alterations include core decompression with drilling 9 or microfracture,18,31 arthroscopic debridement and drilling, 27 corrective osteotomies,5,8,11,15,19,21,23,24 and autologous osteochondral transplantation.7,14,28,29 The second comprises procedures that excise the damaged part of the articular surface of the metatarsal head and include resection arthroplasty–open 16 or arthroscopic, 2 joint replacement arthroplasty, 6 and interpositional arthroplasty.25,26
Dorsal closing wedge osteotomy has been accepted as the gold standard treatment of Freiberg infraction.15,30 The objective for DCWMO is to redirect the intact and healthy plantar articular cartilage more dorsal to articulate with the proximal phalanx. The original procedure consisted of an intra-articular osteotomy with removal of a dorsal wedge of the unhealthy cartilage. 11 Kinnard and Lirette 21 modified the procedure by performing the closing wedge osteotomy over the extra-articular normal metaphyseal region at the margin of the joint. The lesion was not removed but merely rotated proximally away from the articulation between the metatarsal head and the proximal phalangeal base.17,23 A modified Weil osteotomy has also been used, where the wedge apex begins more proximally in the metatarsal metaphysis to allow easier fixation with a screw and, distally, the wedge opens to excise the avascular damaged bone completely.8,19
Intra-articular DCWMO enables less metatarsalgia than the extra-articular osteotomy, which often leads to excessive elevation of the metatarsal head. 5 We encountered only 1 case of transfer metatarsalgia. This was attributed to a 2.4-mm shortening of the second metatarsal. In this study, the mean shortening of 1.9 mm was consistent with the shortening of 1.8 to 2.5 mm reported in the literature.5,21,30 The reduced ROM of the MTP joint as correlated with the metatarsal osteotomy was not proved in the present study. Helix-Giordanino et al 15 reported a loss of 15°± 10.7° in plantarflexion and 10°± 8.5° in dorsiflexion, while Özkul et al 30 reported a mean plantarflexion restriction of 18° (range, 0°-35°) and a mean dorsiflexion restriction of 12° (range, 0°-25°). In the present study, there was only a slight decrease of plantarflexion, from 28°± 12° to 26°± 13°, while the dorsiflexion improved from 35°± 11° to 38°± 12.5°.
OAT has been a well-accepted treatment for articular cartilage lesions of the knee, ankle, and elbow joints.12,13,20,37 Hayashi et al 14 introduced in 2002 the use of the OAT procedure as a new technique to treat advanced-stage Freiberg disease. It was concluded that OAT was advantageous because it was nondestructive and could restore the congruity of the MTP joint. Since then, a number of case reports have reported acceptable clinical results, low morbidity, and early return to sport.7,28,29,36
Donor site morbidity was considered the most common complication of the OAT procedure. 1 However, we encountered no donor site problems in the present study. The congruity of the MTP joint was restored, and lengthening of the metatarsal by 0.2 ± 0.1 mm occurred as well. That led to improvement of the ROM of the MTP joint, as opposed to the stiffness that was frequently seen after DCWMO. The dorsiflexion increased from 37°± 12° to 48°± 14° and the plantarflexion from 30°± 11° to 32°± 12°.
Miyamoto et al 28 reported comparable results to the present study after following up 13 patients treated with OAT for advanced-stage Freiberg disease for a mean duration of 67.2 months. Significant improvement of the AOFAS score (from 66.9 ± 5.3 to 93 ± 7.6) and the visual analog scale score (from 72.7 ± 10.3 to 7.8 ± 7.2) was reported, while magnetic resonance imaging scan at 5 years postoperatively showed consolidation of the transplanted autograft and smooth configuration of the articular surface.
Athletes treated with osteochondral transplantation returned to both training and full sport activities 2 to 3 weeks earlier than the athletes who received metatarsal osteotomy for treatment. We attributed the earlier time to return to previous sport level to 2 reasons: (1) the increased ROM and improved congruity of the joint noted in the OAT group and (2) the large contact area of the cylindrical surface and the underlying interface between the osteochondral plug and the cancellous bone socket, both favorable for early bone-to-bone healing. These advantages allowed the athletes to accelerate their rehabilitation protocol and return to previous sport level earlier. Furthermore, the joint surface restored with hyaline cartilage was durable and capable of being preserved against repetitive mechanical stress and highly demanding sport activity. 36
There is a paucity of literature reporting on the treatment of Freiberg disease in athletes. Sproul et al 35 reported improvement of symptoms and a 20% decrease of ROM in 10 athletes (11 feet) treated with MTP joint debridement (10 feet) and MTP head resection (1 foot). Tsuda et al 36 used OAT for advanced-stage Freiberg disease in 3 adolescent athletes. Acceptable clinical results and early return to sport were reported despite the short-term follow-up.
We acknowledge several limitations in the study. The number of patients was rather small, and longer follow-up is necessary to draw definite conclusions. However, although Freiberg disease is a rare condition, an adequate number of patients were recruited to participate in the study. The prospective randomized single-surgeon nature of the study increased its strength.
Conclusion
We concluded that OAT is equal to the recognized gold standard treatment for Freiberg disease: dorsal closing wedge metatarsal osteotomy. Acceptable clinical results were reported, as well as very low morbidity and early return to previous sport level. That makes the OAT procedure a safe, effective, and optimal treatment for the athletic population experiencing Freiberg infraction.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.