
Abstract
Background:
Studies on the effect of partial- and full-thickness chondral damage of the hip on outcomes and the ability to achieve meaningful clinical outcomes are limited.
Purpose:
To determine the effect of full- and partial-thickness chondral injuries on 2-year outcomes in patients undergoing hip arthroscopic surgery for femoroacetabular impingement syndrome (FAIS) compared with patients without chondral damage, and to identify significant predictors of achieving the patient acceptable symptomatic state (PASS) and minimal clinically important difference (MCID).
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Data from consecutive patients with evidence of chondromalacia at the time of primary hip arthroscopic surgery with routine capsular closure for the treatment of FAIS by a single fellowship-trained surgeon between January 2012 and September 2016 were reviewed. Patients were divided into groups with partial-thickness (grade I-III) or full-thickness (grade IV) chondral defects and matched by age and body mass index (BMI) to patients without chondral injuries. Preoperative and postoperative outcomes were compared among the 3 groups, and a binary logistic regression analysis was utilized to identify significant predictors of achieving the MCID and PASS.
Results:
There were 634 patients included in the analysis, with a mean age of 34.5 ± 10.9 years and a mean BMI of 25.2 ± 4.7 kg/m2. A total of 493 (77.8%) patients had no evidence of chondral damage, 92 (14.5%) patients had partial-thickness chondral defects, and 49 (7.7%) patients had full-thickness chondral defects. There were statistically significant differences in the Hip Outcome Score (HOS)–Activities of Daily Living, HOS–Sports Subscale, modified Harris Hip Score, pain, and satisfaction (P < .01) among the 3 groups. Patients with grade IV chondromalacia experienced the poorest outcomes and lowest percentage of achieving the PASS. Predictors for achieving any PASS threshold included preoperative alpha angle (odds ratio [OR], 0.96; P = .016), absence of preoperative limping (OR, 7.25; P = .002), absence of preoperative chronic pain (OR, 5.83; P = .019), primary hip arthroscopic surgery (OR, 0.17; P = .050), patients who self-identified as runners (OR, 2.27; P = .037), and Tönnis grade 0 (OR, 2.86; P = .032). Male sex (OR, 2.49; P = .015) was the only predictor of achieving any MCID threshold.
Conclusion:
Patients with grade IV chondral defects experienced worse functional outcomes, lower satisfaction, and increased pain when compared with both patients without chondral damage or grade I-III chondromalacia at 2-year follow-up. Several predictors were associated with achieving clinically significant function in patients undergoing hip arthroscopic surgery for FAIS.
Keywords
The effect of hip chondral lesions at the time of hip arthroscopic surgery remains incompletely understood. 4 This is likely because of the multitude of concomitant factors that can negatively affect outcomes in patients with chondral damage, some of which include the location and extent of the chondral lesion, the geometry of the head-neck junction, the degree of head coverage, altered biomechanics, and demographic factors.29,42 Similar to other joints, cartilage defects in the hip constitute a significant challenge because of their unclear treatment algorithm and predisposition to joint degeneration if left untreated. 19 It has been reported that arthroscopic treatment of femoroacetabular impingement syndrome (FAIS) and labral tears in patients with mild osteoarthritis (Tönnis grade 1) can result in similar clinical improvements to those with no osteoarthritis (Tönnis grade 0). 9 This is of high clinical significance, given the limited survivorship and longevity of total hip arthroplasty in younger patients with higher activity demands.
Despite substantial biomechanical differences between the 2 joints, most current cartilage restoration procedures for the hip have been adopted from surgical techniques for the knee.2,10,34 A recent systematic review by Nakano et al 31 reported that there are more than 10 different techniques described for cartilage repair in the hip and that most of them have good short- to medium-term outcomes. However, there is limited literature evaluating differences in outcomes between patients with partial- versus full-thickness injuries. In addition, improvements in patient-reported outcome measures in those with chondral injuries are not always clinically significant and thus remain difficult to interpret.
For the abovementioned reasons, the purpose of the current study was to determine the effect of full- and partial-thickness chondral injuries on 2-year outcomes in patients undergoing hip arthroscopic surgery for FAIS when compared with patients without chondral damage. Additionally, we sought to identify significant predictors of achieving the patient acceptable symptomatic state (PASS) and minimal clinically important difference (MCID) in this specific patient population. Our hypothesis was that the presence of chondral injuries would negatively affect outcomes and decrease the likelihood of achieving clinically significant improvements in regard to the PASS and MCID.
Methods
Patient Enrollment
After institutional review board approval, data from patients undergoing hip arthroscopic surgery and labral repair for FAIS with evidence of a cartilage injury at the time of surgery between January 2012 and September 2016 were extracted. All clinical data were prospectively collected in a secure repository, and patient-reported outcomes were collected in a secure electronic outcome data collection database. Inclusion criteria consisted of a diagnosis of FAIS, based on established criteria, 13 in patients with failed nonoperative treatment (eg, physical therapy, lifestyle modification, nonsteroidal anti-inflammatory drugs, hip injections) who ultimately underwent hip arthroscopic surgery with intraoperative documentation of the cartilage status with a minimum 2-year follow-up. Exclusion criteria were patients with a history of pediatric deformities (congenital hip dislocation, slipped capital femoral epiphysis, or Perthes disease), osteoarthritis or a joint space narrowing <2 mm (Tönnis grade >1), hip dysplasia (lateral center edge angle [LCEA] <20°), a history of lower extremity surgery, and a history of contralateral hip arthroscopic surgery. The control group consisted of consecutive patients who met the same exclusion and inclusion criteria without intraoperative evidence of a cartilage injury. Grade I-III and grade IV chondromalacia groups were subsequently compared with the control group of patients without chondromalacia (matched by body mass index [BMI] and age).12,44 Patients with grade I-III chondromalacia were grouped together into the low-grade group, as these were considered to be patients with partial-thickness lesions, whereas those with grade IV chondromalacia were classified separately into the high-grade group, as they encompassed patients with full-thickness chondral lesions.
Chondral Grading System
The classification from Beck et al 1 was utilized to grade chondral injuries, given its high interobserver reliability for outcome reporting. 33 This classification is based on the type and depth of chondral damage as an isolated lesion in the acetabulum. It distinguishes 4 categories of lesions: grade I is chondromalacia or cartilage fibrillation; grade II is described as “debonding” or loss of chondral fixation but with an intact cartilage surface; grade III represents a loss of fixation, thinning of the cartilage, and formation of a chondral flap; and grade IV is a full-thickness injury. For the purpose of this study, chondral injuries were classified as Beck grades I, II, and III (partial thickness) or grade IV (full thickness) as described above. Chondral grading for all patients was performed intraoperatively by the senior author (S.J.N.).
Radiographic Assessment
Preoperative and postoperative weightbearing anteroposterior (AP) pelvis, false profile, and 45° Dunn views were obtained for all participants. The Tönnis grade, LCEA, and alpha angle were assessed on all AP pelvis radiographs. The LCEA was measured from the vertical to lateral edge of the acetabular rim. The anterior center edge angle (ACEA) was measured from the vertical to lateral edge of the acetabular rim in the false profile view. All patients underwent magnetic resonance imaging before surgery. All measurements and assessments were performed by a trained fourth-year medical student, a sports fellow, and a fellowship-trained orthopaedic surgeon (E.C.B., J.C., S.J.N.).
Operative Technique
All hip arthroscopic procedures were performed by a single fellowship-trained hip surgeon (S.J.N.) at a high-volume academic hospital whose technique has been previously described in the literature.11,15,41 A standard anterolateral portal was established under fluoroscopic guidance, and a subsequent modified midanterior portal was established via spinal needle localization under direct arthroscopic visualization. A 2-cm capsulotomy site was then created, connecting the anterior and anterolateral portals. Central compartment abnormalities were then addressed in a standard fashion, including labral repair or debridement and acetabular rim trimming if pincer morphology was present. Grade I-III chondral injuries were then debrided with a combination of mechanical shavers and radiofrequency probes, while all grade IV chondral injuries were treated with microfracture.
After completion of the procedures in the central compartment, traction was released, and the hip was flexed to 20° to access the peripheral compartment. Via the anterior portal, the arthroscope was placed into the peripheral compartment, and T-capsulotomy was performed between the 12- and 2-o’clock positions to the intertrochanteric line. A suture-passing device (SlingShot Suture Manager; Stryker) was used to reflect the capsule using No. 2 high–molecular weight polyethylene sutures (BioComposite Corkscrew; Arthrex) in the medial and lateral leaflets of the iliofemoral ligament and another in the lateral leaflet of the iliofemoral ligament. Both stitches were retrieved out of the anterolateral portal and tensioned with a hemostat against the skin. With the capsule reflected, osteochondroplasty of the cam deformity was performed. A dynamic examination and fluoroscopic imaging were used to confirm complete osteochondroplasty with appropriate head-neck offset restoration. Once the arthroscopic procedure was complete, full capsular closure via plication was performed to ensure normal biomechanical properties of the iliofemoral ligament. 32
Capsular plication was then performed in all patients using the same technique as follows. The suture-passing device loaded with suture was inserted through the cannula in the distal anterolateral accessory portal, and a full-thickness pass was made through the medial limb of the T-capsulotomy site, followed by a larger full-thickness bite in the lateral leaflet. Plication of the vertical limb was performed with the amount of leaflet overlap dependent on the degree of capsular laxity. Depending on the integrity of the iliofemoral ligament and size of the capsulotomy site, 2 to 4 interrupted sutures were used to close the vertical limb. The interportal limb was typically closed by approximation of the leaflets; however, the interportal capsule was tightened based on capsular redundancy by alternately advancing the location where sutures were passed through the acetabular leaflet of the interportal limb.
Postoperative Rehabilitation
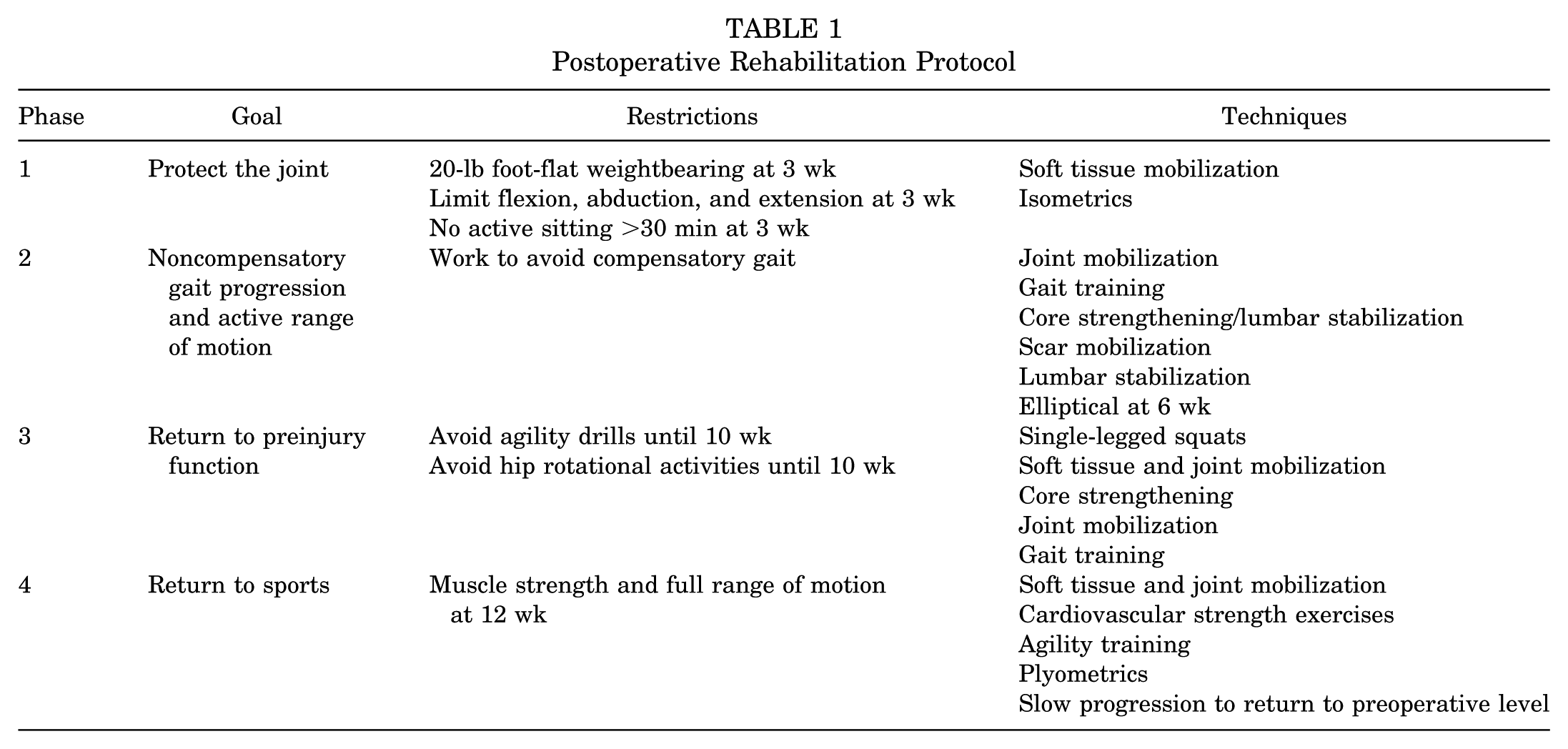
Rehabilitation started on postoperative day 1 for all patients as previously described and did not differ from therapy indicated for FAIS cases.25,30 Patients went through a 4-phase rehabilitation protocol that lasted a mean of 16 to 18 weeks (Table 1). Phase 1 prioritized joint protection and soft tissue mobilization techniques. The surgical limb was initially restricted to 20-lb foot-flat weightbearing during this phase. Patients were weaned off crutches if they demonstrated ambulatory capability without significant pain or compensatory movements at 3 weeks postoperatively. Patients with grade IV lesions were limited to 20-lb foot-flat weightbearing and used crutches for the first 6 to 8 weeks as a modification to this protocol. Patients advanced to phase 2 if they demonstrated full weightbearing capabilities. Phase 2 concentrated on normal gait maintenance, full range of motion restoration, improvement of neuromuscular control, and maintenance of pelvic and core stability. Patients progressed to phase 3 if gait was determined to be normal and pain-free with adequate neuromuscular control. Phase 3 included single-legged squats and strengthening, soft tissue and joint mobilization, and cardiovascular fitness. Phase 4 emphasized returning to the preinjury level of sports participation. Patients were cleared to return to sports if they were able to participate in sports without pain, had full dynamic functional control, and passed return-to-sports tests (including but not limited to resisted single-legged squats and lateral agility).
Postoperative Rehabilitation Protocol
Patient-Reported Clinical Function
To quantify the clinical significance of outcomes for athletes and nonathletes individually, we applied the principles of the MCID and PASS as defined for functional patient-reported outcome measures. Prior work has proposed that the MCID be considered a minimum target for outcome improvement, while the PASS can be considered to represent a satisfactory outcome that is acceptable to the patient. 35 The Hip Outcome Score (HOS)–Activities of Daily Living (ADL), HOS–Sports Subscale (SS), and modified Harris Hip Score (mHHS) values were assessed preoperatively and at 2-year postoperative time points (22-24 months). Patients also reported their visual analog scale scores for pain and satisfaction at the same time points. As previously described in the literature, the MCID for the HOS-ADL, HOS-SS, and mHHS was determined by calculating the 0.5 SD of the mean change of the respective outcome scoring tool in the study patients.20,27,37
The PASS for the HOS-ADL, HOS-SS, and mHHS at 2 years was calculated using an anchor-based method. To identify the satisfaction score associated with the PASS, patients were asked the following question: “Taking into account all the activities you have during your daily life, your level of pain, and also your functional impairment, do you consider that your current state is satisfactory?” The PASS was then identified using a receiver operating characteristic (ROC) curve analysis as conducted in prior studies (analysis provided in Appendix 1, available in the online version of this article).5,8 A sensitivity and specificity of 0.80 were used as cutoffs for determining the threshold cutoff scores.
Statistical Analysis
All data were confirmed to have met all parametric statistical assumptions before analysis. Two binary logistic regression models were created: 1 for achieving any MCID threshold and another for achieving any PASS threshold. The process of creating the models is summarized in Figure 1. Pearson and Spearman covariate analyses were performed between the MCID and PASS with preoperative, intraoperative, and postoperative variables to identify variables to fit in the exploratory analysis for the final logistic models. To identify predictors of achieving the MCID and PASS in patients with chondromalacia, an exploratory factor analysis was performed on the variables with statistically significant correlations to achieving an intermediate (achieving any MCID threshold) or high meaningful clinical outcome (achieving any PASS threshold) using principal component (PC) extraction (ie, eigenvector decomposition) with a varimax rotation to reduce redundancy in the predictor variables. A Kaiser-Meyer-Olkin value of 0.7 was found, which demonstrates that data were appropriate for factor analysis, as this value exceeded a recommended value of 0.6 for exploratory factor analysis. 43 A screen plot was examined to determine the number of PCs to retain for analysis. Each extracted PC was used to calculate the percentage of variance by dividing the eigenvalue of each PC by the sum of all eigenvalues. The contribution of each variable to the PC was determined using the factor loadings of each variable. A variable that demonstrated a factor loading of greater than ±0.25 for a PC was retained as a predictor variable for the follow-up binary logistic regression analysis used to predict high- versus low-functioning 2-year postoperative patient-reported outcome scores. Once a final model was created for the PASS and MCID, an ROC curve analysis was performed to determine how well each model represented the study group. 40
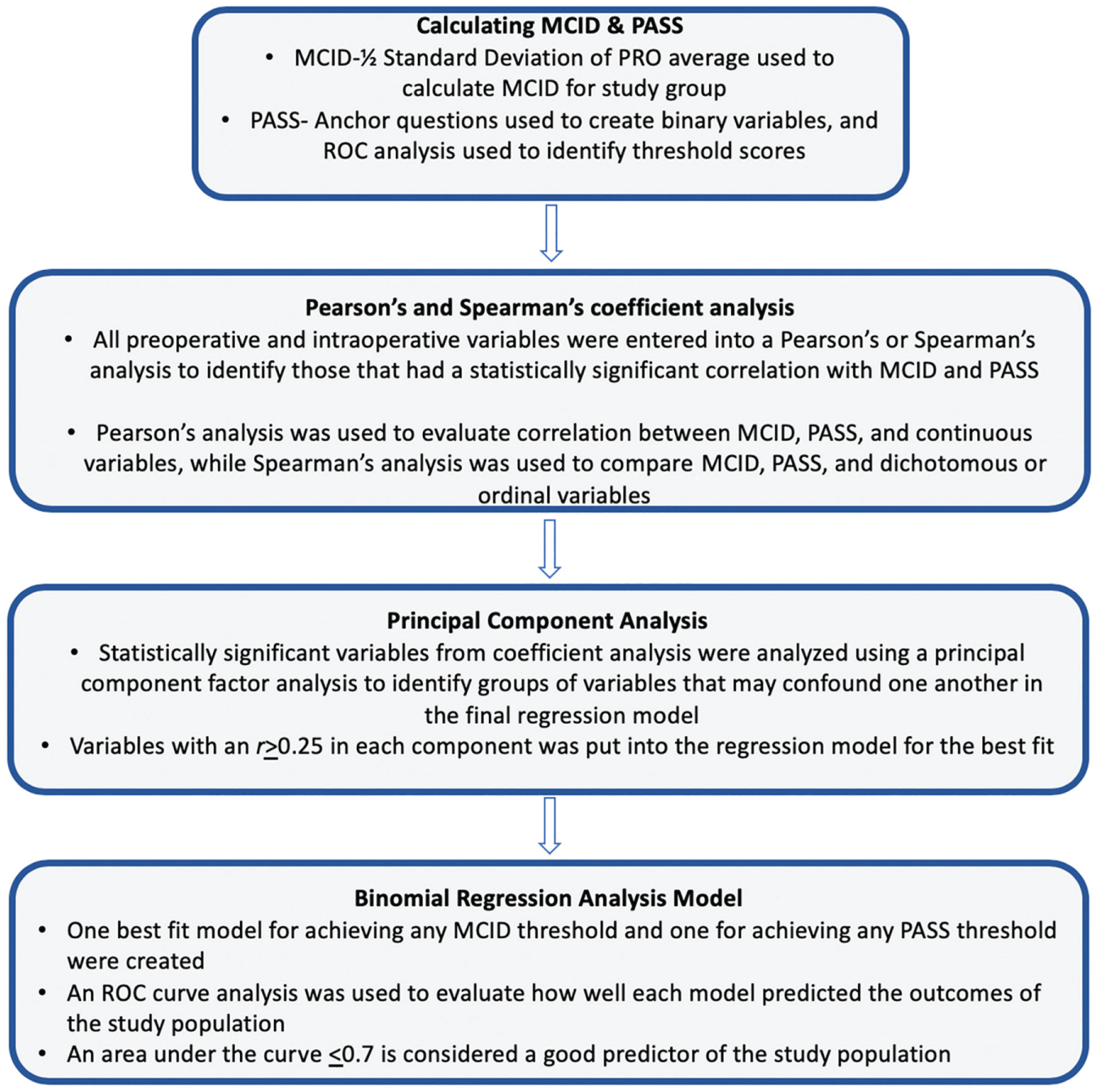
Flowchart of the statistical analysis used to build the predictive regression model. Briefly, a correlation analysis was used to filter variables correlated with clinical failure or inferior clinical outcomes, and then an exploratory factor analysis using principal components was performed to limit the collinearity of variables in the final model. MCID, minimal clinically important difference; PASS, patient acceptable symptomatic state; PRO, patient-reported outcome; ROC, receiver operating characteristic.
Descriptive statistics for all continuous variables were reported as mean ± SD, and statistics for all noncontinuous variables were reported as frequency and proportion. A paired-samples t test was used to compare preoperative and 2-year postoperative patient-reported outcome scores in patients with FAIS. Statistical significance for all analyses was set at α≤ .05. All statistical analyses were performed using SPSS statistical software (v 25.0; IBM).
Results
Patient Characteristics
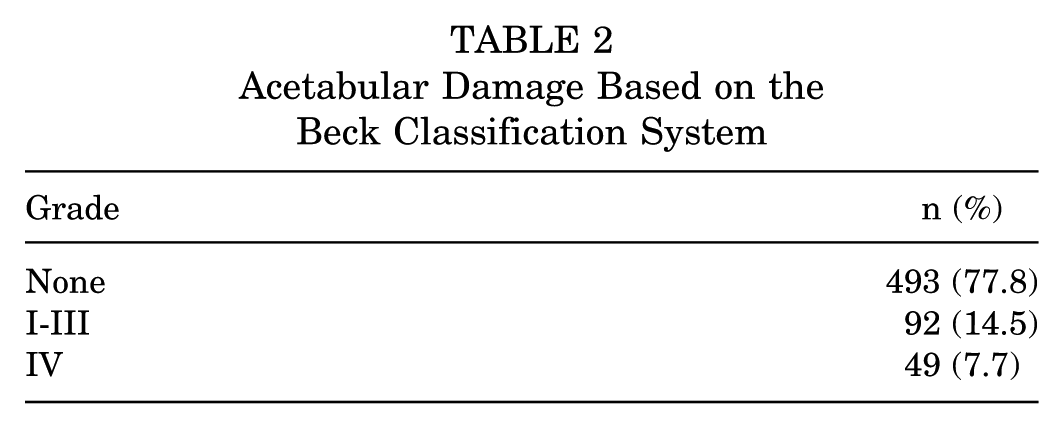
A total of 790 patients had a reported intraoperative cartilage status, of whom 634 (80.3%) had 2-year reported outcomes (mean follow-up, 27.8 ± 3.8 months) and were included in the final analysis (Figure 2). The majority of patients (77.8%) did not have evidence of cartilage damage, while 14.5% had grade I-III (partial thickness) chondral injuries, and 7.7% had grade IV (full thickness) chondral injuries (Table 2). Overall, there were more women (65.8%), with an overall mean age of 34.5 ± 10.9 years and a mean BMI of 25.2 ± 4.7 kg/m2. There were no statistically significant differences in the age or BMI between groups (P = .086 and P = .259, respectively). There was, however, a statistically significant difference in the frequency of male versus female patients with grade I-III (21.8% vs 10.8%, respectively; P < .001) and grade IV (10.6% vs 6.2%, respectively; P < .001) chondromalacia (Table 3). Of note, a total of 19 (3.0%) patients included in the study underwent labral debridement, 13 of whom did not have evidence of chondromalacia, 3 of whom had grade I-III chondromalacia, and 3 of whom had grade IV chondromalacia.
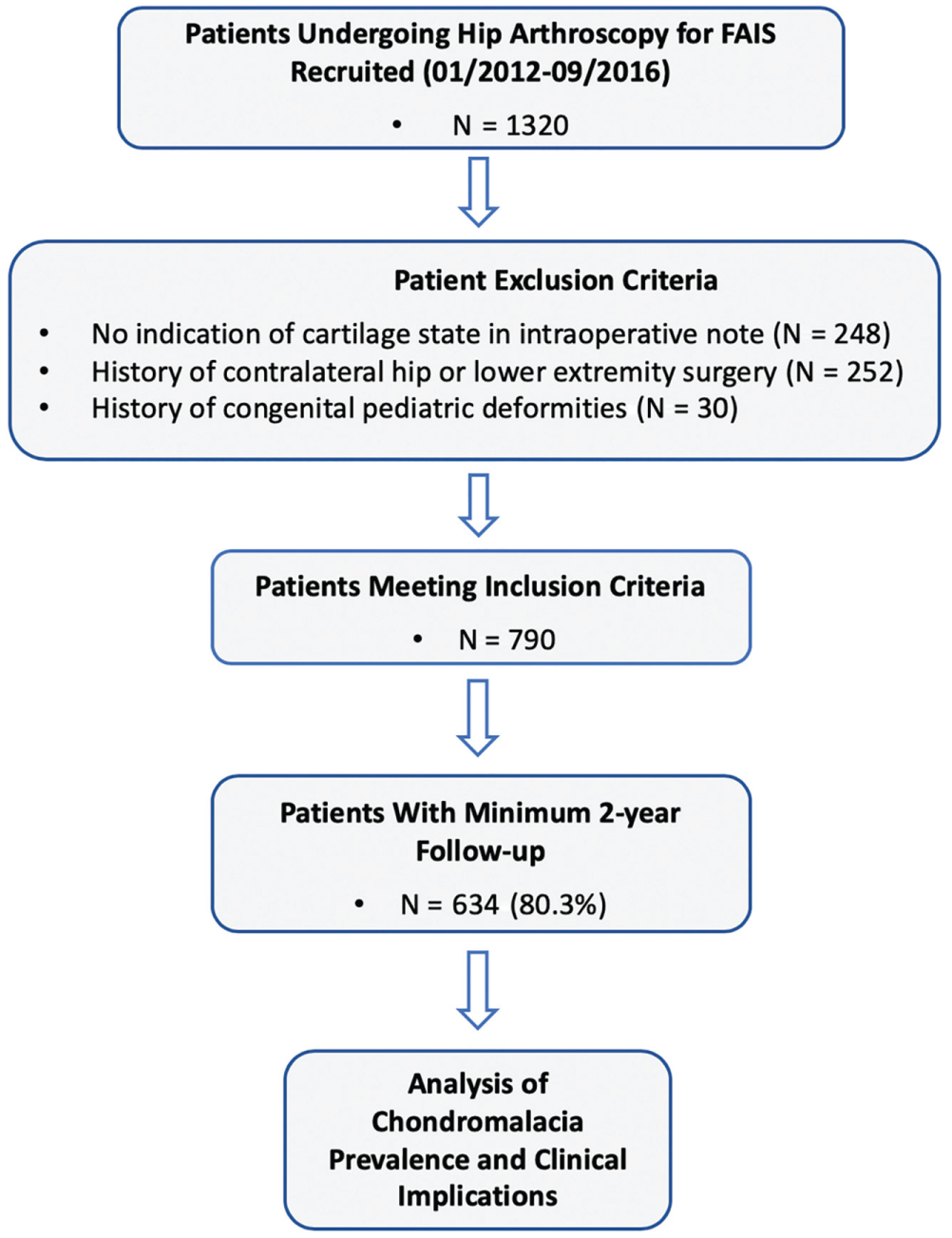
PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) diagram of the final cohort selection, showing a flowchart of the study population recruitment window as well as exclusion and inclusion criteria.
Acetabular Damage Based on the Beck Classification System
Patient Demographics by Chondromalacia Status a
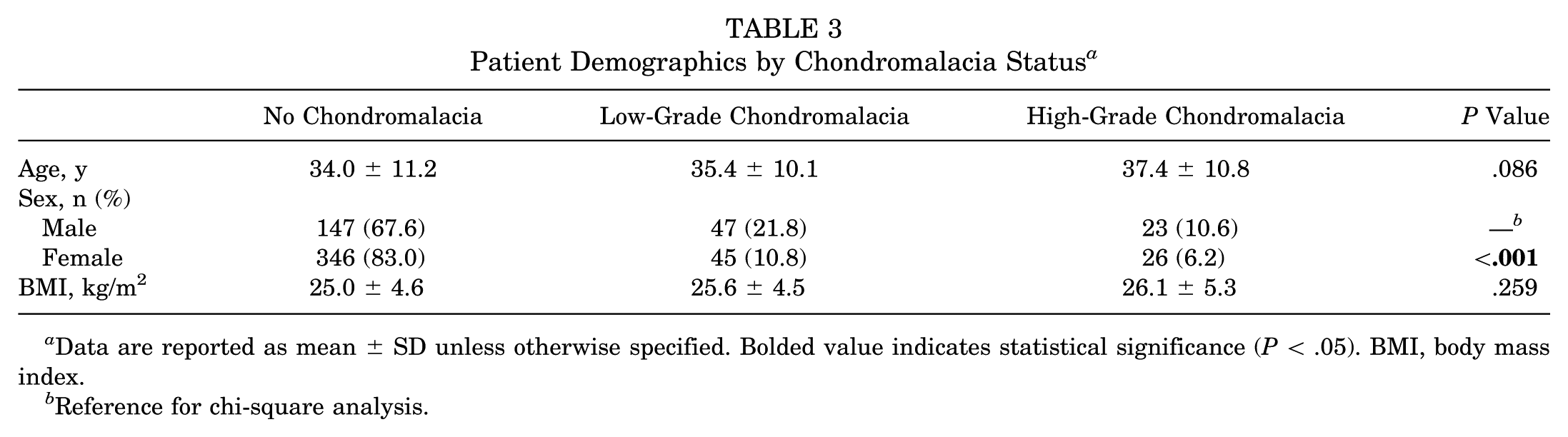
Data are reported as mean ± SD unless otherwise specified. Bolded value indicates statistical significance (P < .05). BMI, body mass index.
Reference for chi-square analysis.
Radiographic Analysis
Postoperatively, there was a statistically significant improvement in all measured variables including alpha angle (AP, false profile, and Dunn), LCEA, and ACEA (P < .001). An independent-samples t test was used to analyze differences in preoperative and postoperative radiographic findings between patients with and without chondromalacia. While there were statistically significant differences between the groups in regard to the preoperative alpha angle in the AP, false profile, and Dunn views, as well as the ACEA, there were no significant postoperative radiographic differences (Table 4).
Radiographic Measurements by Chondromalacia Status a
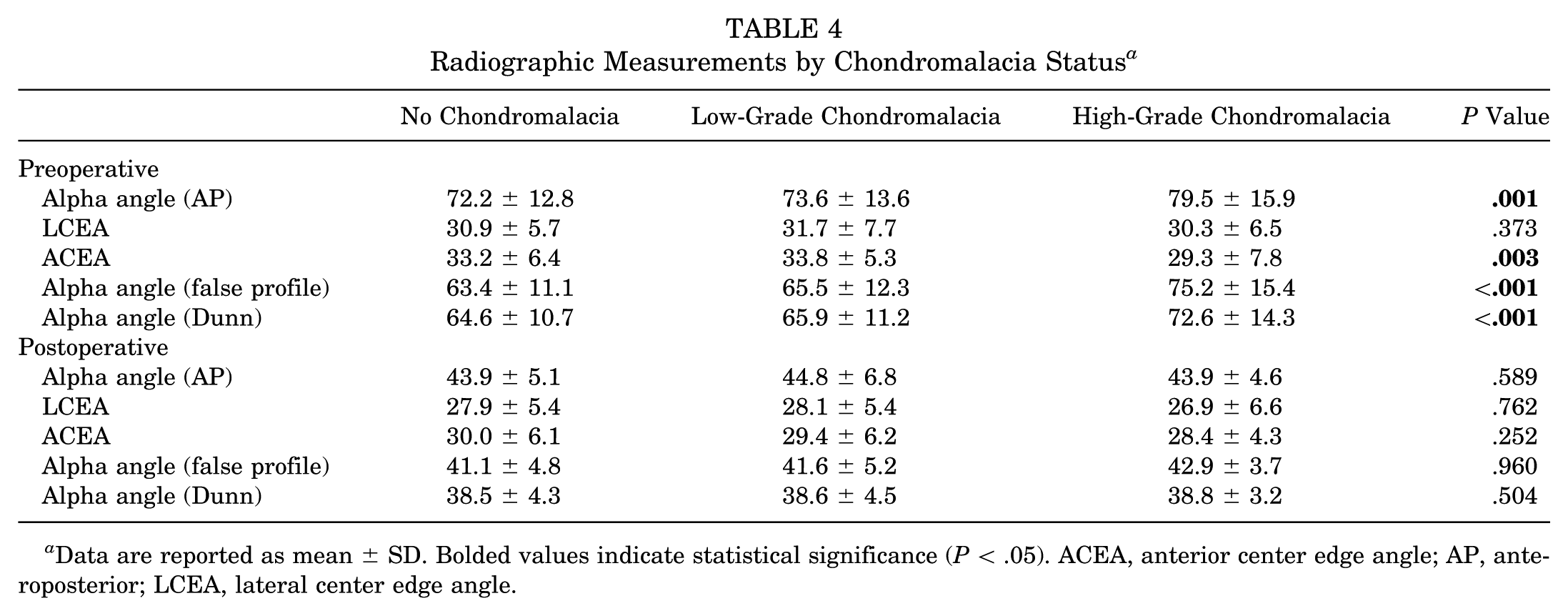
Data are reported as mean ± SD. Bolded values indicate statistical significance (P < .05). ACEA, anterior center edge angle; AP, anteroposterior; LCEA, lateral center edge angle.
Analysis of Chondral Damage
Analysis of baseline patient-reported outcome scores demonstrated no statistically significant differences between groups. However, a comparison of 2-year postoperative patient-reported outcomes demonstrated statistically significant differences in all outcome scores (Table 5). Patients with grade IV chondromalacia had the lowest 2-year outcome and satisfaction scores and the highest pain scores.
Patient-Reported Outcome Scores by Chondromalacia Status a
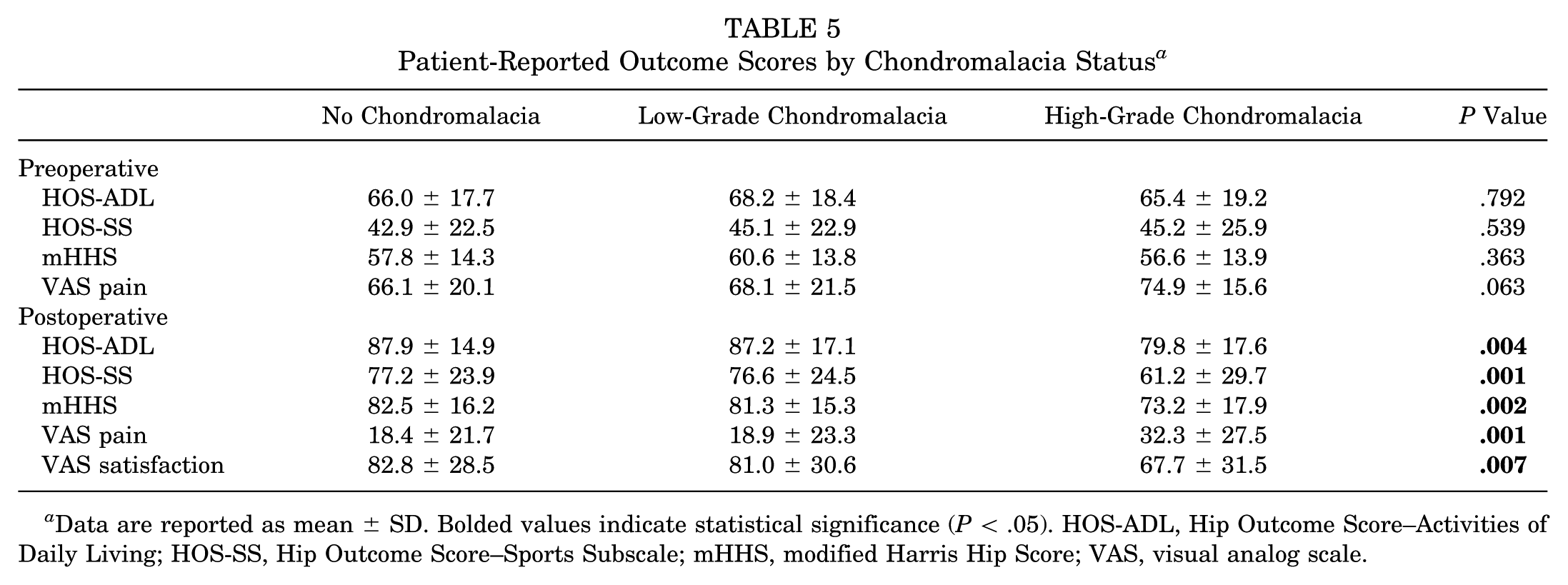
Data are reported as mean ± SD. Bolded values indicate statistical significance (P < .05). HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Analysis of Outcome Differences by Chondromalacia Severity
The threshold scores for the change in the HOS-ADL, HOS-SS, and mHHS to achieve the MCID were 15.4, 13.1, and 16.8, respectively. The threshold scores for the 2-year HOS-ADL, HOS-SS, and mHHS to achieve the PASS were 86.0, 69.1, and 80.2, respectively. There was a statistically significant difference between the number of patients achieving the MCID for the HOS-ADL (P = .044) and HOS-SS (P = .001) and the PASS for the HOS-ADL (P = .019), HOS-SS (P = .005), and mHHS (P = .022) when comparing all 3 groups (Table 6). Patients with grade IV chondromalacia had the lowest percentage of patients achieving both the PASS and the MCID for the HOS-ADL, HOS-SS, and mHHS when compared with patients with grade I-III chondromalacia and no chondromalacia.
Analysis of Achieving the PASS and MCID a
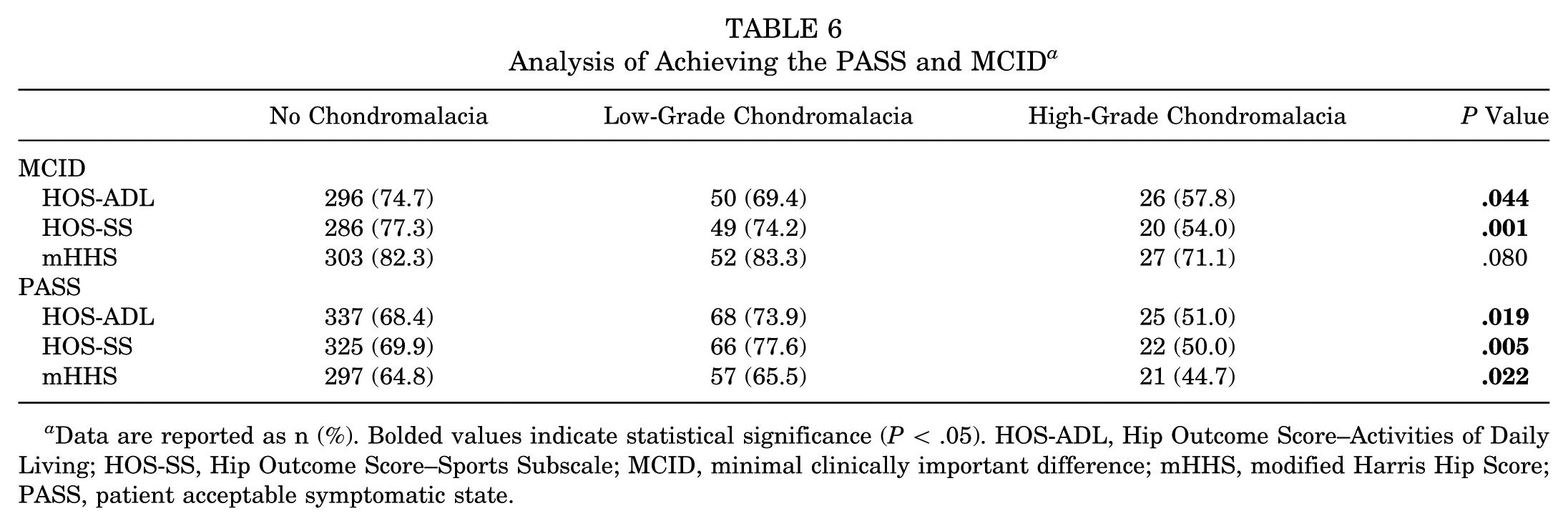
Data are reported as n (%). Bolded values indicate statistical significance (P < .05). HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, patient acceptable symptomatic state.
MCID and PASS Logistic Regression Analysis Models
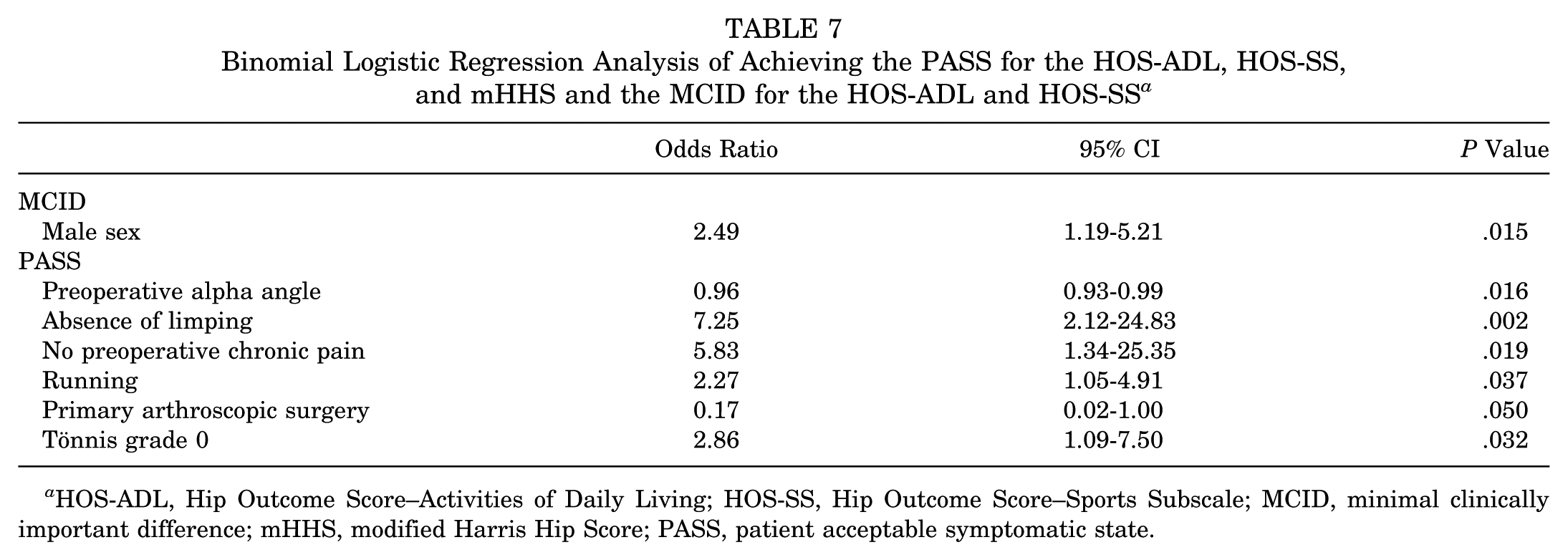
The factor analysis for achieving MCID consisted of 5 PCs that explained 67.9% of the variance of the predictor variables, while the analysis for achieving PASS consisted of 7 PCs that explained 68.7% of the variance of the predictor variables. The rotation factor analysis for each predictor variable can be found in Appendix 2, available online. The variables retained for analysis were based on the PC loadings that were statistically significant in the MCID and PASS logistic regression models and are reported in Table 7. Briefly, the only variable that was a statistically significant predictor of achieving the MCID was male sex (odds ratio [OR], 2.49; P = .015). The predictors for achieving the PASS included preoperative alpha angle (OR, 0.96; P = .016), no preoperative limping (OR, 7.25; P = .002), absence of preoperative chronic pain defined as ≥2 years (OR, 5.83; P = .019), no prior primary hip arthroscopic surgery (OR, 0.17; P = .050), running (OR, 2.27; P = .037), and Tönnis grade 0 (OR, 2.86; P = .032). Both the MCID and the PASS logistic models demonstrated a good fit with an area under the curve of 0.719 and 0.724, respectively, in the ROC curve analysis (Appendix 3, available online).
Binomial Logistic Regression Analysis of Achieving the PASS for the HOS-ADL, HOS-SS, and mHHS and the MCID for the HOS-ADL and HOS-SS a
HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, patient acceptable symptomatic state.
Clinical Failures
At 2-year follow-up, there were a total of 16 patients who experienced failure as defined by undergoing revision hip arthroscopic surgery or conversion to total hip arthroplasty. A total of 12 patients underwent revision hip arthroscopic surgery, 8 of whom had no evidence of chondromalacia, 2 of whom had grade I-III chondromalacia, and 2 of whom had grade IV chondromalacia. Furthermore, 7 patients underwent conversion to total hip arthroplasty (1 with prior revision), 2 of whom had no evidence of chondromalacia and 5 of whom had grade IV chondromalacia.
Discussion
The main findings of the current study were that patients with chondral damage at the time of hip arthroscopic surgery demonstrated significant improvements in clinical and functional outcomes, as well as satisfaction and pain scores, at a minimum of 2 years postoperatively compared with preoperative scores. Furthermore, when stratified by chondral damage, patients with partial-thickness chondral injuries demonstrated significantly better functional outcomes and improvements in pain and more frequently achieved clinically significant outcome improvement than those with full-thickness chondral injuries. Additionally, male sex was identified as a predictor of achieving the MCID, while preoperative alpha angle, absence of preoperative limping, primary hip arthroscopic surgery, absence of chronic preoperative pain, running for sport, and Tönnis grade 0 were identified as predictors for achieving the PASS.
Despite the sensitivity and specificity of preoperative imaging for patients undergoing hip arthroscopic surgery, previously undiagnosed cartilage defects are commonly found at the time of surgery.7,18,24,39 Kemp and colleagues 21 quantified the prevalence of chondral injuries (defined as Outerbridge grade ≥1) in patients undergoing hip arthroscopic surgery and determined it to be 40% in a total of 58 patients with FAIS. The current study found that the prevalence of chondral injuries was 22.2% in a total of 634 patients. The present study examined a cohort with more than 10 times the number of patients and may provide a better estimate of the incidence of chondral injuries at the time of hip arthroscopic surgery. Furthermore, it is possible that the prevalence of 40% determined by Kemp and colleagues was an overestimate in a smaller sample of patients or that their technique of a cartilage assessment differs from the one used in this study. Despite differing estimates, these numbers suggest that patients with FAIS have a relatively high prevalence of concomitant chondral injuries. Other studies have demonstrated a high frequency of chondral injuries among patients with FAIS. In a Danish registry with 686 FAIS procedures, Lund et al 28 reported a prevalence of 88% for chondral injuries. This higher prevalence could be related to the duration of symptoms, as Scandinavian countries may have more strict policies for surgical procedure indications, specifically after failing other nonoperative measures for a certain period of time. As the duration of symptoms is not stated in the abovementioned study, this cannot be concluded but should raise the question for future research.
The geometry of the femoral head and acetabulum articulation in patients with FAIS is thought to predispose patients to premature osteoarthritis through the gradual degeneration of articular cartilage,16,18,38 which likely begins with chondral damage. The current study suggests that chondral damage may be an independent risk factor for poorer functional and clinical outcomes. This finding is in accordance with previous literature that suggests that patients with mild chondral damage have inferior outcomes compared with patients without chondral damage. 21 Bhatia et al 3 reported on 308 patients with grade IV chondral defects identified at the time of hip arthroscopic surgery. The authors reported that full-thickness injuries were associated with a decreased joint space, increased time from symptom onset to arthroscopic surgery, male sex, and a larger alpha angle. Similarly, Suarez-Ahedo et al 42 suggested that greater chondrolabral damage was associated with male sex, more advanced age, anterior extension of the acetabular chondral lesion within the anterosuperior quadrant, labral detachment from the acetabular cartilage, and posterior extension of the labral tear. Although these studies identified factors associated with chondral damage, the current study provides clinical implications of such associations and demonstrates that full-thickness chondral lesions are not only associated with inferior outcomes but also with a less likelihood of achieving meaningful clinical differences.
In our specific study population of patients with grade I-IV chondromalacia who underwent femoral osteochondroplasty with modern capsular repair techniques, decreased joint space, sex, preoperative alpha angle, and duration of pain were all significant predictors of clinically significant outcome improvement. To our knowledge, factors associated with clinically significant outcome improvement in patients with FAIS and chondral injuries at the time of surgery have yet to be investigated. These data may provide further prognostic information to the treating surgeon to better counsel this complex patient population with advanced chondral disease choosing to undergo hip arthroscopic surgery on postoperative expectations. Specifically, treating surgeons may inform these patients that it is possible that they may not experience the same clinical improvement in the short term as a patient with FAIS without chondral disease.
Furthermore, when stratifying patients by the degree of chondromalacia severity, the current study found that patients with full-thickness chondral injuries experienced significantly less improvement than those with partial-thickness chondral injuries, despite undergoing similar rehabilitation protocols. This is in accordance with the results published by Kemp and colleagues, 21 which demonstrated that patients with severe chondral injuries had worse outcomes than those with mild chondral injuries with respect to the Hip Disability and Osteoarthritis Outcome Score (HOOS)–Stiffness, HOOS-Pain, HOOS–Activities of Daily Living, HOOS–Sport and Recreation, HOOS–Quality of Life, and International Hip Outcome Tool–33. This finding has also been demonstrated by Haviv et al, 17 who reported that patients with severe chondral injuries experience worse outcomes than patients with hips that have less chondral damage. While these studies have reported on outcome scores, they did not examine the effect of chondral injuries on achieving the MCID and PASS.
Nwachukwu and colleagues 36 have defined the HOS-ADL, HOS-SS, and mHHS threshold scores for achieving the MCID as 9.8, 12.1, and 9.5, respectively. While prior studies have used these scores as thresholds for comparing differences in achieving meaningful clinical outcomes in other populations with FAIS, a number of previous studies have demonstrated that threshold scores for achieving meaningful clinical threshold values vary based on disease.22,26 Furthermore, threshold scores and rates of achieving meaningful clinical outcomes may be influenced by differences in patient characteristics. The HOS-ADL, HOS-SS, and mHHS threshold scores for achieving the MCID in the current study were 15.4, 13.1, and 16.8, respectively, which were higher than those calculated by Nwachukwu and colleagues. This is likely because the current study calculated the difference of scores over a 2-year period instead of a 1-year period, and it included patients with chondral damage in the analysis, which highlights the importance of determining thresholds specific to inclusion and exclusion criteria of the study.
The current study adds to the existing literature by demonstrating a statistically significant difference in the frequency of clinically significant outcome improvement between patients with full- versus partial-thickness chondral damage. Specifically, those patients with more severe chondral lesions achieved the MCID for the HOS-ADL and HOS-SS, as well as the PASS for the HOS-ADL, HOS-SS, and mHHS, less often. It is possible that those with a more advanced degree of chondromalacia may not benefit to the same degree as patients with less advanced disease progression because of irreversible cartilage changes. Future studies are warranted to investigate the effect of chondral damage on adjacent hip structures in patients with FAIS and to better understand the role of microfracture in the treatment of these patients and its influence on outcomes.
Limitations
There are a number of limitations that need to be addressed. First, although the majority of baseline characteristics were statistically similar between patients with and without chondral damage, there was a significantly greater percentage of female patients in the group without chondral damage. However, as no associations between female sex, chondromalacia, and postoperative outcomes have been established, we do not believe this to be a confounding factor. Second, our study also utilized specific cartilage classification schemes, and we acknowledge that other classification methods exist. Depending on how other treating physicians choose to classify the degree of cartilage change in patients with FAIS, the findings of this study may not be applicable to their patient populations, given that a single surgeon graded all cartilage lesions. Additionally, as classification systems do not consider the severity of every clinical scenario, in the current study, Beck-classified grade III injuries (cleavage, loss of fixation to the subchondral bone, frayed edges, thinning of the cartilage, flap) were treated with microfracture if the cartilage flap was unstable. However, when chondral fraying was minimal at the chondrolabral junction, debridement was performed, and the labrum was fixed to the rim. Third, based on the intraoperative measurements recorded by the senior author, the analysis was limited to only chondral lesion depth based on the Beck classification and not lesion size. Although the overall study sample size was sufficiently powered, the grade IV group was small, which could have led to type I/II errors in the independent t test analysis of reported outcomes. Using the mean change in the HOS-ADL, HOS-SS, and mHHS, we performed a post hoc power analysis using a Cohen d (ie, observed effect size) equal to 0.04996, a probability level of .05, and sample sizes of 141 (grade I-III: n = 92; grade IV: n = 49) and 542 (no chondromalacia: n = 493; grade IV: n = 49) and calculated an observed power of 0.835 and 0.999, respectively. Finally, all patients with grade IV chondromalacia in the current study were treated with microfracture. Given that microfracture for cartilage defects of the knee has demonstrated inferior outcomes compared with other cartilage preservation techniques,6,14,23 future studies that include a control group of grade IV chondral lesions that did not undergo microfracture are needed to determine whether inferior outcomes seen in these patients are solely caused by the presence of a full-thickness cartilage injury or whether there is partial contribution from the microfracture procedure.
Conclusion
Patients with grade IV chondral defects experienced worse functional outcomes, lower satisfaction, and increased pain when compared with both patients without chondral damage and patients with grade I-III chondromalacia at 2-year follow-up. Several predictors were associated with achieving clinically significant function in patients undergoing hip arthroscopic surgery for FAIS.
Supplemental Material
DS_10.1177_0363546519865912 – Supplemental material for Prevalence and Clinical Implications of Chondral Injuries After Hip Arthroscopic Surgery for Femoroacetabular Impingement Syndrome
Supplemental material, DS_10.1177_0363546519865912 for Prevalence and Clinical Implications of Chondral Injuries After Hip Arthroscopic Surgery for Femoroacetabular Impingement Syndrome by Jorge Chahla, Edward C. Beck, Kelechi Okoroha, Jourdan M. Cancienne, Kyle N. Kunze and Shane J. Nho in The American Journal of Sports Medicine
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.N. has received research support from AlloSource, Arthrex, Athletico, DJ Orthopedics, Linvatec, MioMed, Smith & Nephew, and Stryker; education payments from Arthrex; royalties from Ossur; and consulting fees and hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.