
Abstract
Background:
The size of a glenoid bone defect is responsible for reduction in shoulder stability and is correlated with the number of instability events. Biomechanical studies have suggested that it should be considered concomitantly with the Hill-Sachs lesion as “bipolar” bone defects for assessing structural degradation, but the definitive number of instability events associated with the critical size has not been investigated.
Purpose:
To (1) confirm that the number of instability events is the predictor of a critical size of bipolar bone defects and (2) demonstrate the cutoff value of the number of instability events for these defects in rugby players with traumatic anterior shoulder instability.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
One-hundred forty-four rugby players with anterior shoulder instability underwent morphologic evaluation for glenoid and Hill-Sachs lesions by computed tomography and determination of the critical (a glenoid bone defect of ≥25% or an off-track Hill-Sachs lesion) and subcritical (a glenoid bone defect of ≥13.5%) size of bipolar bone defects. In the primary analysis, the prevalence of the critical and subcritical size of bipolar bone defects was investigated. In the secondary analysis, the authors explored the predictors for these bone defects and determined the cutoff value correlating with the critical and subcritical size of bipolar bone defects by applying receiver operating characteristic curves.
Results:
The primary analysis revealed that the prevalence of critical and subcritical size of bipolar bone defects was 20.8% and 61.8% of 144 shoulders, respectively. In the secondary analysis, multiple logistic regression analysis demonstrated that the total number of shoulder instability events and dominant shoulder were the significant factors associated with the critical and subcritical size of bipolar bone defects. The cutoff value for the number of instability events that correlated with critical bipolar bone defects was 6 for the dominant and 9 for the nondominant shoulder, whereas it was 4 for the dominant and 5 for the nondominant shoulder for subcritical bipolar bone defects.
Conclusion:
The number of shoulder instability events and the dominant shoulder were the predictors for the critical and subcritical size of bipolar bone defects for a shoulder with traumatic instability. Four injury events should herald caution when treating rugby players with shoulder instability.
Traumatic anterior shoulder instability recurs frequently in people who play competitive rugby (hereafter termed “rugby players”).3,7 Our previous observational studies have shown that more than half of nonoperative treatments lead to reinjury during a single season. 10 In addition, these shoulders have a tendency for reinjury after stabilization surgery.1,11 At least part of the reason appears to be that rugby players are exposed to frequent high-energy collisions, which is a possible risk factor for shoulder dislocation. 14
The degree of bone defect in the affected shoulder is a further risk factor for recurrence. 4 Cadaveric studies have indicated that a large bone defect itself impairs shoulder stability. A bone defect of ≥25% in the glenoid width is critical for shoulder instability, 20 and a large Hill-Sachs lesion is also critical if it engages readily with the anteroinferior edge of the glenoid margin. 19 Therefore, the concept of the Hill-Sachs “off-track” lesion proposed recently suggests that both of these lesions (ie, the glenoid bone defect and Hill-Sachs lesion) should be assessed concomitantly when considering the unstable shoulder in individual cases. 6
A large bone defect appears to result in poor postoperative clinical outcomes.9,15 Shaha et al 15 and Dickens et al 5 demonstrated that a glenoid bone defect of width ≥13.5% is subcritical for shoulder instability after surgical stabilization. In addition, these bone defects have been correlated with the number of instability events. 12 Overall, those studies have suggested that an unstable shoulder should be treated before it becomes a large bone defect. However, the definitive number of instability events over the critical size in rugby players has not been investigated.
We investigated the prevalence and predictors for the critical and subcritical size of bipolar bone defects as well as the cutoff value of the number of instability events that correlate with these lesions in a cohort of rugby players. We hypothesized that a definitive number of instability events is the predictor of a critical and subcritical size of bipolar bone defects in a shoulder with traumatic anterior instability.
Methods
Participants
The study details were explained to the participants, each of whom provided written consent to participate. This study protocol was approved by the ethics review board of our hospital (No. 16-025).
From 2011 to 2016, a consecutive series of 200 shoulders in 190 rugby players who suffered traumatic anterior shoulder instability were enrolled in the present study. The inclusion criteria were (1) a rugby player who wished to play again; (2) an injury involving acute or recurrent dislocation or subluxation, which was defined as a “shoulder instability event”; and (3) a rugby player who underwent complete examination by helical computed tomography (CT) in the affected shoulder before surgery.
We excluded rugby players who (1) suffered multidirectional shoulder instability, (2) played rugby recreationally, (3) played a sport other than rugby, or (4) had undergone any other type of shoulder surgery.
Of this cohort of 200 shoulders in 190 rugby players, 144 shoulders in 144 players met the inclusion criteria stated above.
Collection and Processing of Data
The following information was obtained from medical records and imaging analyses (see below): player’s age at the time of the CT examination, body mass index (BMI), number of dislocations and subluxations of the shoulder before the CT examination, competition category (professional, collegiate, high school), laxity of the shoulder joint, side of the dominant shoulder, position of the rugby player (forward or back), and degree of bipolar bone defects.
“Shoulder hyperlaxity” was defined as an external rotation of >90° in the unaffected shoulder when the rugby player’s arms were held at the side (reaching the frontal plane). 2 In addition, to investigate the mechanism of the first injury, we asked the rugby players to provide (if possible) a video recording of the injury events. The level of each rugby player was defined as playing in Division 1 (the highest league in each category, including international players) or Division 2 (lower-grade competition level). The detailed characteristics of the rugby players are summarized in Table 1.
Patient Characteristics (N = 144 Shoulders) a
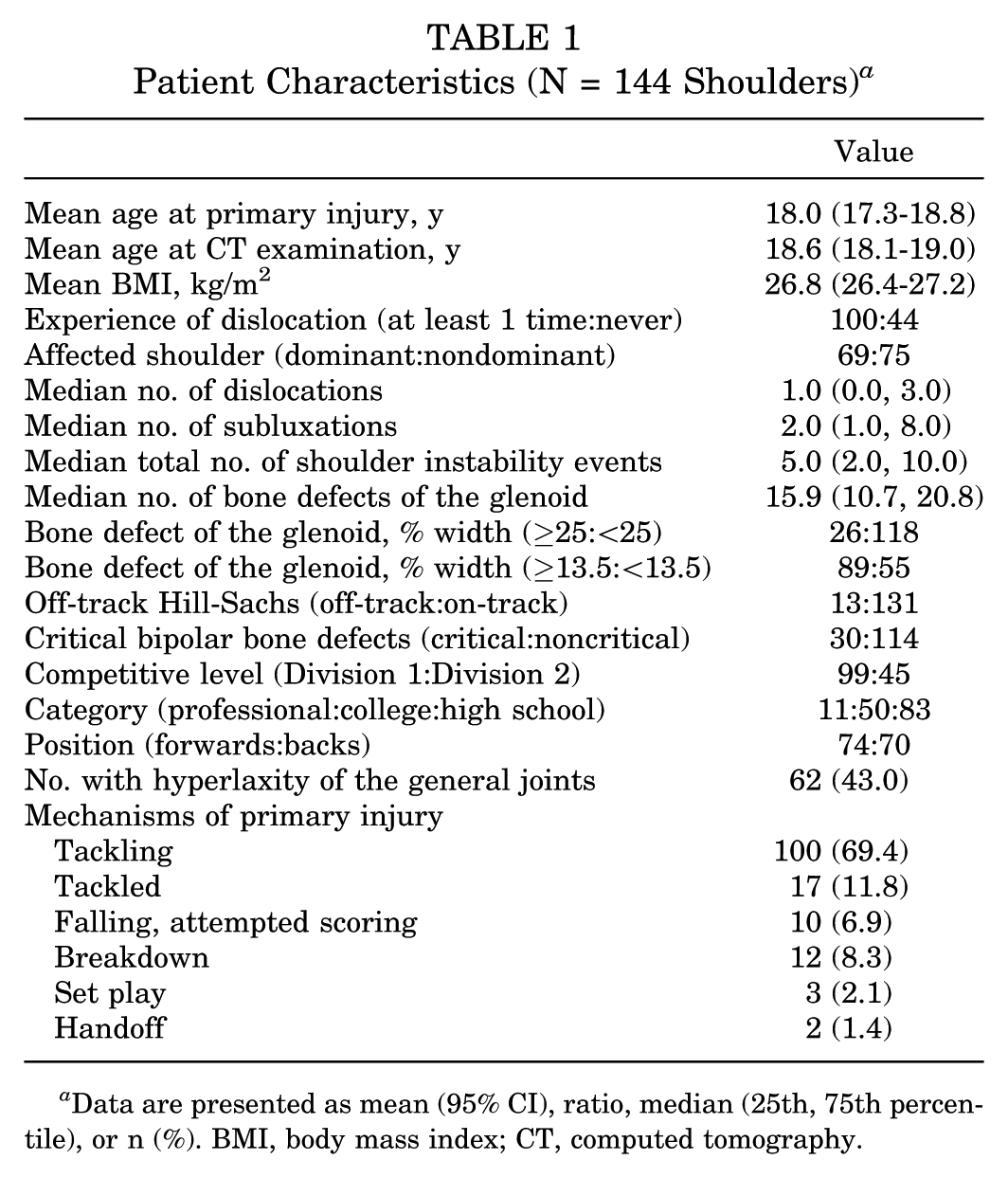
Data are presented as mean (95% CI), ratio, median (25th, 75th percentile), or n (%). BMI, body mass index; CT, computed tomography.
Analyses of CT Images
Before image analyses, an en face view of the glenoid lesion and Hill-Sachs lesion was prepared from reconstructed, 3-dimensional, helical CT images of each individual. According to previous reports,17,18 the percentage of the glenoid bone defect was calculated using the following equation:
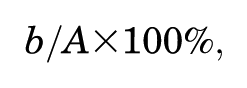
where A is the diameter of the assumed outer-fitting circle based on the inferior portion of the glenoid contour, and b is the width of the defect (Figure 1A). The Hill-Sachs lesion was evaluated according to the concept of “glenoid track” (83% of the diameter of the assumed outer-fitting circle of the glenoid). For shoulders involving any glenoid bone defect, the glenoid track was additionally subtracted from the width of the glenoid defect. 19 Then, we measured the Hill-Sachs interval (the distance from the rotator cuff attachments to the medial rim of the Hill-Sachs lesion) (Figure 1B). 6 Finally, if the glenoid track was less than the Hill-Sachs interval, the shoulder was considered to have an “off-track” Hill-Sachs lesion. All CT measurements were processed using Osirix (Pixmeo Sàrl).
Measurements of bone defects on unstable shoulder. (A) Measurement of a glenoid bone defect (% width), where b/A × 100 ≥ 25% indicates a critical defect, A is the diameter of a circle, and b is the width of the bone defect. (B) The Hill-Sachs interval is the distance from the rotator cuff attachment to the medial rim of the Hill-Sachs lesion (c).
Two researchers (Y.H., S.S.) evaluated 20 (14%) of the 144 shoulders randomly for the presence and size of glenoid bone defects and Hill-Sachs lesions to determine the accuracy of the measurements. The kappa coefficient was applied to assess the reliability for identifying the bone defects. The intraclass correlation coefficient (ICC) (2,1) was used to assess the interrater reliability for their measurements. The remainder of the shoulders (n = 124) were evaluated individually.
Definition of a Critical Bipolar Bone Defect
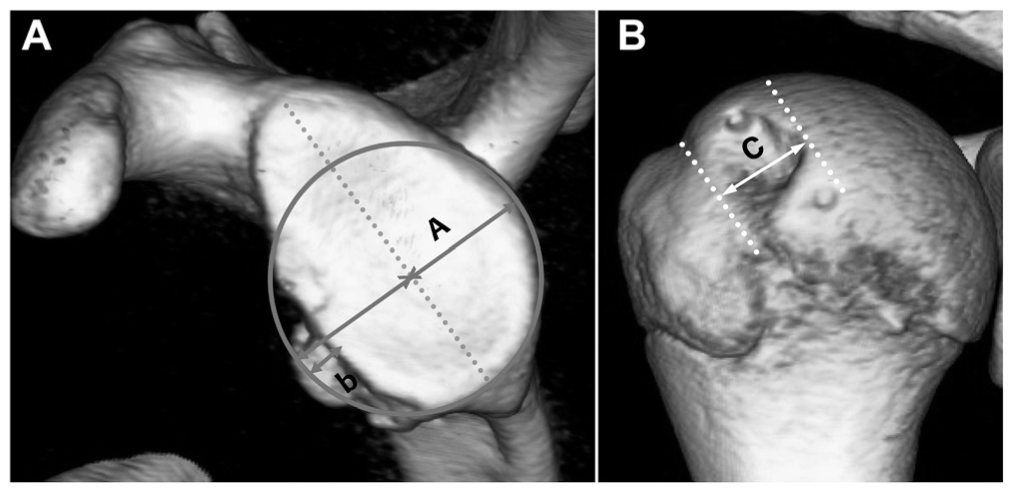
Based on a well-organized cadaveric study by Yamamoto and colleagues, 20 a “critical bipolar bone defect” was present if it displayed a glenoid bone defect ≥25% or an off-track Hill-Sachs lesion. According to clinical studies,5,15 a “subcritical bipolar bone defect” was defined as when a glenoid bone defect of ≥13.5% was present. These details are summarized in Figure 2.
Scatterplot with description of critical and subcritical bipolar bone defects. Filled circles, sample shoulders defined as “critical”; gray circles, sample shoulders defined as “subcritical”; open circles, sample shoulders defined as “safe.”
Statistical Analyses
When undertaking analyses, the age at the CT examination, BMI, and number of total injury events (dislocation + subluxation) were treated as continuous quantitative data. Other variables were defined as being positive or negative.
The primary analysis was carried out to investigate the prevalence of critical and subcritical bipolar bone defects in our cohort of rugby players. In the secondary analysis, we explored the predictors for these bone defects using univariate and multiple logistic regression analyses and confirmed that the number of instability events was correlated with critical and subcritical bipolar bone defects. In addition, receiver operating characteristic (ROC) curves were constructed to ascertain the highest sensitivity and specificity for the threshold of the number of instability events for the critical and subcritical size of bipolar bone defects. The highest sensitivity and specificity were defined as the optimal cutoff criteria. Confounders were selected as appropriate, and the multicollinearity of each independent variable was assessed by calculating each correlation before the analysis. The independent variables were age; BMI; competitive level; total number of instability events; and category, position, and laxity of the affected dominant shoulder. The goodness of fit for each final estimate was assessed using the Hosmer-Lemeshow test. 8 Statistical analyses were conducted using SAS v 9.4 (SAS Institute). P < .05 (2-sided) was considered significant.
Results
The interrater reliability evaluated using the kappa coefficient was 0.89 and 0.88 for identifying a glenoid bone defect and a Hill-Sachs lesion, respectively. The ICC (2,1) was 0.82 and 0.80 for measuring a glenoid bone defect and the Hill-Sachs lesion, respectively. These outcomes indicated that the accuracy for identifying and measuring the bone defects was acceptable.
Among our cohort of rugby players with shoulder instability, a glenoid bone defect was identified in 130 of 144 shoulders, and the prevalence was 90.3% (95% CI, 85.4-95.2). The size of the glenoid bone defect did not have a normal distribution, and the median value was 15.9% (interquartile range, 10.7-20.8). A Hill-Sachs lesions was observed in 120 of 144 shoulders, and the prevalence was 83.3% (95% CI, 77.2-89.5).
In the primary analysis, a critical size of bipolar bone defect was identified in 30 of 144 shoulders, for a prevalence of 20.8% (95% CI, 14.1-27.5). A subcritical size was detected in 89 shoulders, for a prevalence of 61.8% (95% CI, 53.8-69.8). A glenoid bone defect of ≥25% was identified in 26 shoulders, for a prevalence of 18.1% (95% CI, 11.7-24.4). An off-track Hill-Sachs lesion was detected in 13 of 144 shoulders, for a prevalence of 9.0% (95% CI, 4.3-13.8).
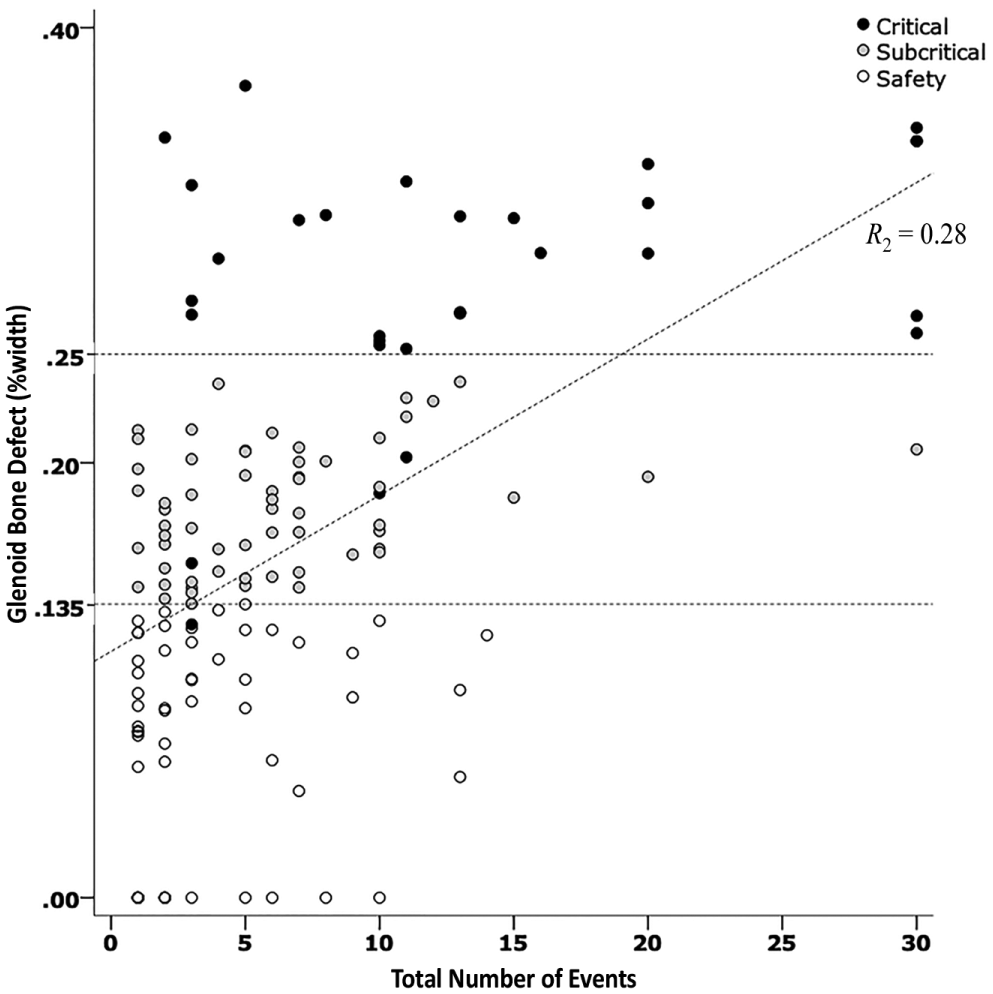
Before the secondary analysis, a correlation analysis was done. We found that the total number of instability events and glenoid bone defects was correlated significantly (r = 0.63; P < .01) (Appendix Figure A1, available in the online version of this article). The secondary analysis of the univariate and multiple logistic regression analyses demonstrated that 2 factors (the total number of shoulder instability events and the dominant shoulder) were significantly related to a critical bipolar bone defect (Appendix Table A1, available online), whereas the type of injury (ie, dislocation or subluxation) did not affect the outcome. ROC curves for the number of instability events were evaluated separately between the dominant and nondominant shoulder because these issues also appeared to be significant predictors of the outcome. For critical bipolar bone defects, the cutoff value of the number of instability events was 6 times in the dominant shoulder (sensitivity, 68.4%; specificity, 68.0%; P = .004; area under the curve [AUC], 0.78) and 9 times in the nondominant shoulder (sensitivity, 81.8%; specificity, 82.8%; P = .01; AUC, 0.85) (Figure 3). For subcritical bipolar bone defects, the cutoff value for the number of instability events was 4 times in the dominant shoulder (sensitivity, 67.3%; specificity, 65.0%; P = .02; AUC, 0.72) and 5 times in the nondominant shoulder (sensitivity, 70.0%; specificity, 65.7%; P = .04; AUC, 0.76) (Figure 4).
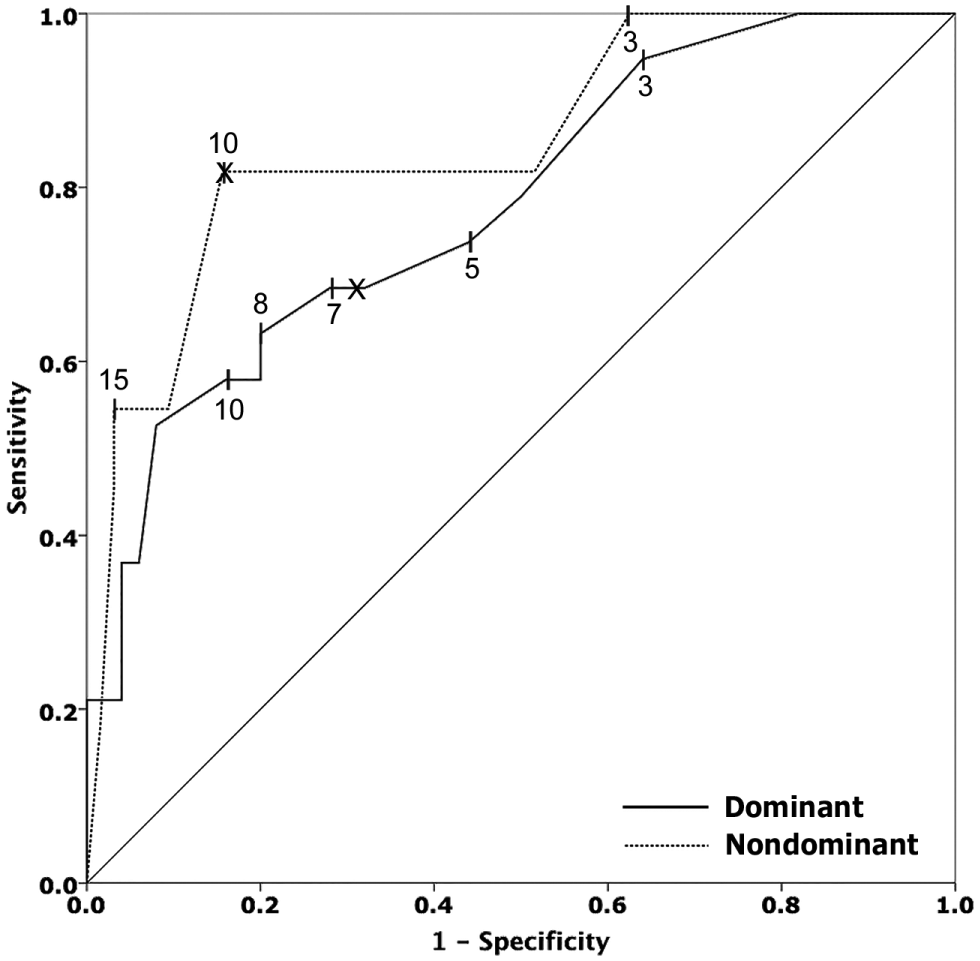
Receiver operating characteristic curve for a critical bipolar bone defect. Solid line, dominant shoulder (area under the curve = 0.78); dotted line, nondominant shoulder (area under the curve = 0.85).
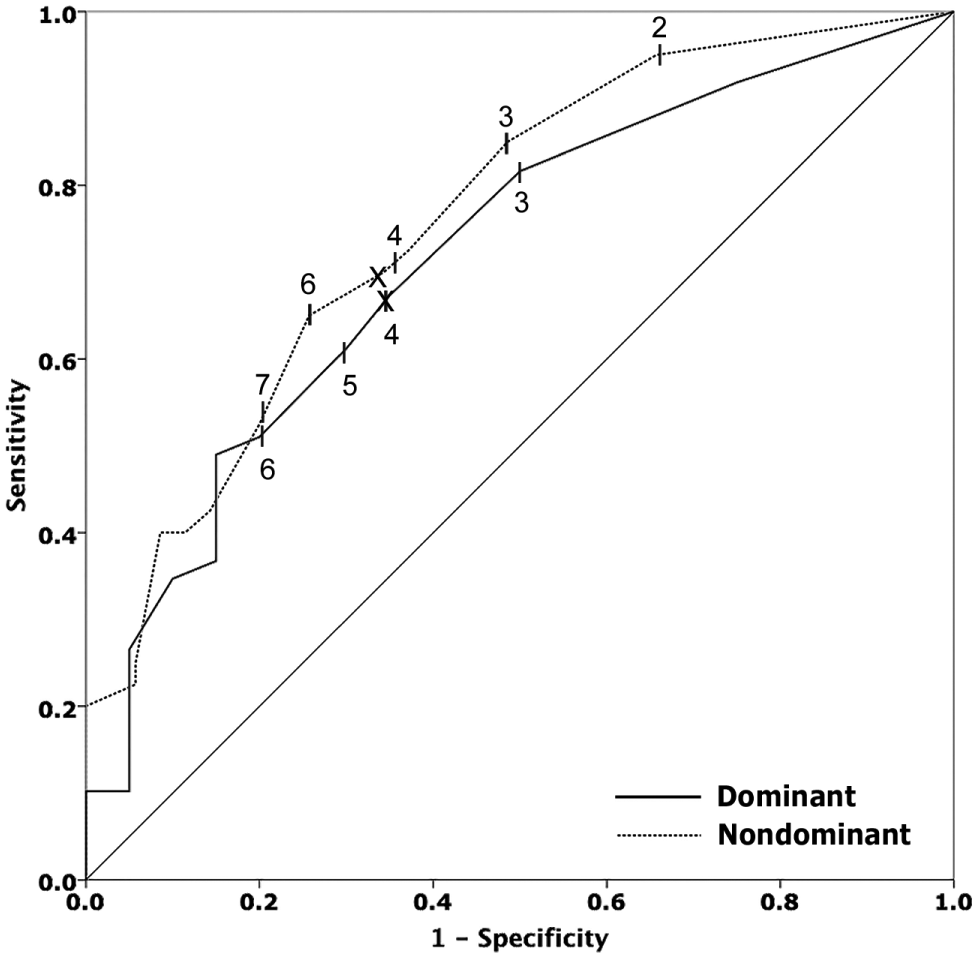
Receiver operating characteristic curve for a subcritical bipolar bone defect. Solid line, dominant shoulder (area under the curve = 0.72); dotted line, nondominant shoulder (area under the curve = 0.76).
Discussion
We found that ~20% of rugby players with shoulder instability had a critical size of bone defect. These data may imply that these players need bone recovery to restore stability during shoulder stabilization surgery (eg, transfer of the coracoid process). Our study also showed that ~60% of rugby players with shoulder instability had a subcritical size of bone defect. Studies have demonstrated the postoperative outcome to be insufficient in cohorts of rugby players,5,15 indicating that these rugby players also need augmentation surgery. Overall, our findings appear to suggest that more than half of rugby players with shoulder instability may be candidates for augmentation surgery.
In the secondary analysis, univariate and multiple logistic regression analyses showed that the number of shoulder instability events was correlated independently with the size of bipolar bone defects in rugby players who suffered traumatic anterior shoulder instability. It appears reasonable that injury recurrence would lead to certain degrees of structural degradation of the shoulder, which has been suggested previously.12,13 At the final estimate, we adopted the results of univariate analyses of the number of shoulder instability events for drawing the ROC curve in each side of the affected shoulder. We did this because the odds ratios, P values, and values of the Akaike information criterion of these shoulder instability events were not different from the results of multiple analysis (Appendix Table A2, available online). Finally, our results demonstrated that 4 injury events necessitated caution regarding the critical size of bipolar bone defects for rugby players with traumatic anterior shoulder instability. We believe these findings are important for people who play rugby as well as other sports involving collisions.
With regard to the difference in shoulder dislocations and shoulder subluxations, we combined these as a single total or considered them independently when conducting multiple regression analysis. The former was more suited for the final estimate, indicating that an influence on the defect size was not significantly different between dislocation and subluxation, data that are consistent with the work of Shin and coworkers. 16
We also found that the dominant shoulder, as the affected side, was correlated independently with the size of bipolar bone defects in our cohort. The reason why the dominant shoulder was a risk of a glenoid bone defect is not known, but it is possible that the dominant shoulder tends to experience greater force in rugby. The experimental work of Seminati and colleagues 14 appears to support our finding. They found that tackling with the dominant shoulder involved a greater mean peak impact force than with the nondominant shoulder. This finding may be applicable to other sports involving a dominant shoulder (eg, athletes in throwing events) and related studies should be undertaken.
The present study had 3 main limitations. First, this was a retrospective study with only a single observational period. Thus, a causal relationship between the degree of bone defect and actual reinjury events was difficult to demonstrate. Second, there may have been a recall bias regarding the number of reinjury events, which were self-assessed by the players and derived from medical records. Third, there may have been a selection bias for the sample of rugby players, most of whom were immature youths. Further studies are needed to resolve these limitations.
Conclusion
The present study demonstrated that the number of shoulder instability events and the dominant shoulder were the predictors for a critical and subcritical size of bipolar bone defects. Four injury events necessitated caution regarding the critical size of bipolar bone defects for rugby players with traumatic anterior shoulder instability. We should evaluate for a bipolar bone defect even if a small number of instability events has occurred.
Supplemental Material
DS_10.1177_0363546519869673 – Supplemental material for The Number of Injury Events Associated With the Critical Size of Bipolar Bone Defects in Rugby Players With Traumatic Anterior Shoulder Instability
Supplemental material, DS_10.1177_0363546519869673 for The Number of Injury Events Associated With the Critical Size of Bipolar Bone Defects in Rugby Players With Traumatic Anterior Shoulder Instability by Yoshinori Hasegawa, Takayuki Kawasaki, Shuko Nojiri, Shogo Sobue, Takefumi Kaketa, Yoshinori Gonda, Yoshiaki Itoigawa and Kazuo Kaneko in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.