
Abstract
Background:
Posterior glenoid bone deficiency is an increasingly recognized entity in the setting of recurrent posterior shoulder instability; however, little is known about the subject. Due to the paucity of literature on posterior bone loss, historical comparisons with anterior bone loss may not be fully accurate.
Purpose:
To systematically describe the morphology of posterior bone defects in the setting of recurrent posterior shoulder instability based on several quantitative parameters, including the mean location, orientation, and extent of bone loss on a clockface model, as well as the angle of the defect relative to the long axis of the glenoid.
Study Design:
Cross-sectional study; Level of evidence, 4.
Methods:
Three-dimensional reconstructed computed tomography scans of serially collected patients with a history of recurrent posterior shoulder instability were evaluated by 3 separate reviewers. The posterior glenoid bone defect was characterized using the following measures: (1) the mean lesion location and orientation based on a clockface model with 6 o’clock denoted as inferior and 9 o’clock as directly posterior for all patients; (2) the total extent of the posterior bone defect based on the clockface; and (3) the average angle of the bone loss relative to the long axis of the glenoid.
Results:
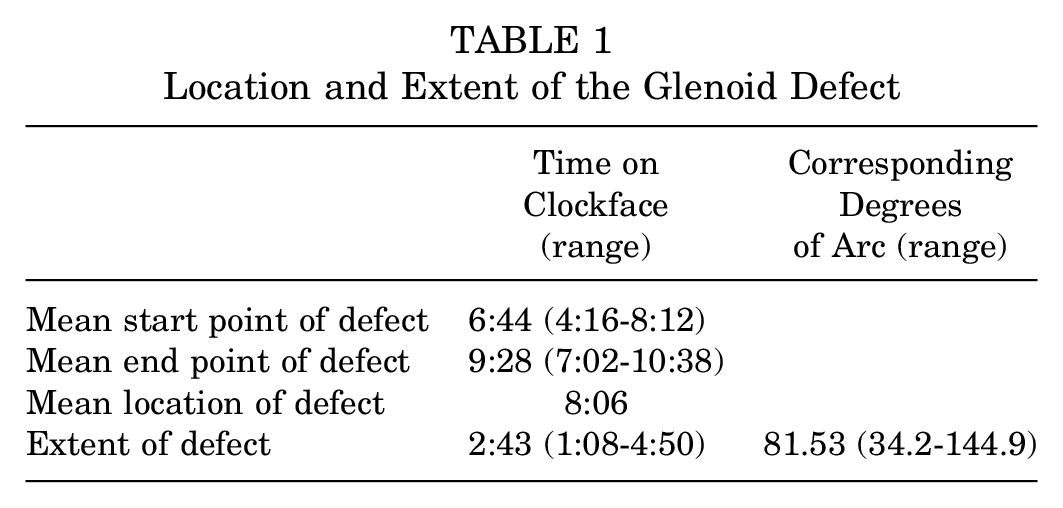
A total of 70 male patients and 1 female patient with a mean age of 29.3 years (range, 24.4-35.1 years) were included in the analysis. The mean clockface location of the posterior glenoid defect originated at 6:44 (range, 4:16-8:12) and extended to a mean of 9:28 (range, 7:02-10:38). The mean extent of the posterior glenoid defect was 2:43 (range, 1:08-4:50), which corresponds to a mean total bone loss arc of 81.5° (range, 34.2°-144.9°), nearly 1 quadrant of the glenoid. Posterior bone loss occurred in a posteroinferior direction at a mean angle of 30.7° (range, 8.0°-80.0°) relative to the long axis of the glenoid.
Conclusion:
Posterior bone defects in the setting of posterior shoulder instability most commonly occur in the posteroinferior quadrant of the glenoid and extend on average from 6:44 to 9:28 (81.5° total degrees of arc) on a clockface model. Posterior bone loss occurs at a mean of 30° off the long axis of the glenoid in a posteroinferior direction, which is historically different from anterior bone loss, which occurs parallel to the long axis of the glenoid. This study serves to highlight the location and orientation of bone loss that one can expect in a patient with recurrent posterior shoulder instability, although additional work is needed to assess why this develops.
Keywords
Anterior and posterior shoulder instability with associated bone loss are 2 distinct pathologic conditions with different patient presentations, symptoms, surgical techniques, and outcomes. 2 Posterior shoulder instability is much more infrequent compared with its anterior counterpart, historically representing 10% of all patients with shoulder instability.14,26 Furthermore, patients with posterior shoulder instability are 20 times less likely to have a dislocation compared with those patients who have anterior shoulder instability. 26 However, posterior shoulder instability is becoming more commonly recognized, and recent reports estimate it accounts for up to 24% of all shoulder instability events and may even be up to 40% in active populations. 19 Despite differences in pathology, posterior instability biomechanical models have been modeled after prior anterior shoulder instability models due to the paucity of basic science knowledge surrounding posterior shoulder instability with associated bone loss. 13
Evaluating critical bone loss in both clinical and biomechanical studies has proven essential in effective treatment preventing recurrence in anterior shoulder instability.10,18 Saito et al’s 15 landmark article demonstrated the most frequent location and extent of anterior bone loss when looking at both the orientation of the fragment in the plane of the trunk and the scapula. This clear defining of lesion location facilitated more accurate biomechanical evaluation and treatment studies to better clarify critical bone loss and effective treatment.22,23,25
Known factors that portend worse clinical outcomes in posterior capsulolabral repair include dominant shoulder surgery, female sex, use of 3 or fewer anchors, and smaller glenoid bone width. 1 However, the clinical implications of posterior bone loss quantity are still unclear. 7 Posterior bone loss biomechanical models have attempted to help define “critical” bone loss to prevent recurrence and poor outcomes. 13 Similar to anterior instability models, Nacca et al 13 found that 20% of vertically oriented defects increased posterior humeral head translation, which could not be restored by a reverse Bankart repair alone. However, this study used protocols and methodology consistent with anterior instability models, namely the vertical orientation of the bony defects, and thus the validity of the findings is unclear.
The purpose of this study was to systematically describe the morphology of posterior bone defects in the setting of recurrent posterior shoulder instability based on several quantitative parameters, including the mean location, orientation, and extent of bone loss on a clockface model, as well as the angle of the defect relative to the long axis of the glenoid. It was hypothesized that the median location of the lesion will be posteroinferior from 6 to 9 o’clock and oriented 45° off of the long axis compared with vertical models in line with the long axis seen in current biomechanical models. 13
Methods
A retrospective review of 71 serially collected patients with 3-dimensional (3D) reconstructed computed tomography (CT) scans for a diagnosis of traumatic posterior shoulder instability with associated bone loss were evaluated. Approval for this study was obtained from the Vail Health Institutional Review Board before patient imaging collection and review. A total of 70 male patients and 1 female patient with a mean age of 29.3 years (range, 24.4-35.1 years) were included in the analysis. Only those patients who had findings of posterior glenoid bone loss on 3D CT and a history consistent with recurrent posterior instability were included in the present study. Exclusion criteria for this study included the patient’s not having posterior bone loss, patient age greater than 40 years, the presence of glenohumeral osteoarthritis, a patient history of seizures or other neurological disorders, and a prior shoulder posterior stabilization procedure. Patients over the age of 40 were excluded from this study to minimize any chances that erosion would be due to any glenohumeral osteoarthritis.
3D CT
With the patient supine on the center of the gantry table and the arm in neutral rotation, CT images were obtained with a CT scanner (SOMATOM Plus 4; Siemens AG), with a spiral 2- or 3-mm slice thickness and a pitch of 1. Then, the 3D images of the glenoid were reconstructed using a 1-mm reconstruction with a surface-rendering method. 15
Quantitative Assessment of the Glenoid
A retrospective review of the collected images was conducted by 3 authors (T.J.D., L.A.P., B.T.G.). Three-dimensional reconstructed glenoids with an en face axial view were evaluated in a manner similar to that of prior established methods for anterior bone loss. 15 A best-fit circle was extrapolated for the inferior two-thirds of the glenoid according to prior established findings.5,9,10,20 The 12-o’clock position was identified by the bony landmark of the supraglenoid tubercle. A line drawn from the 12-o’clock position through the center of the circle and through the most inferior portion of the glenoid identified the 6-o’clock position (Figure 1).
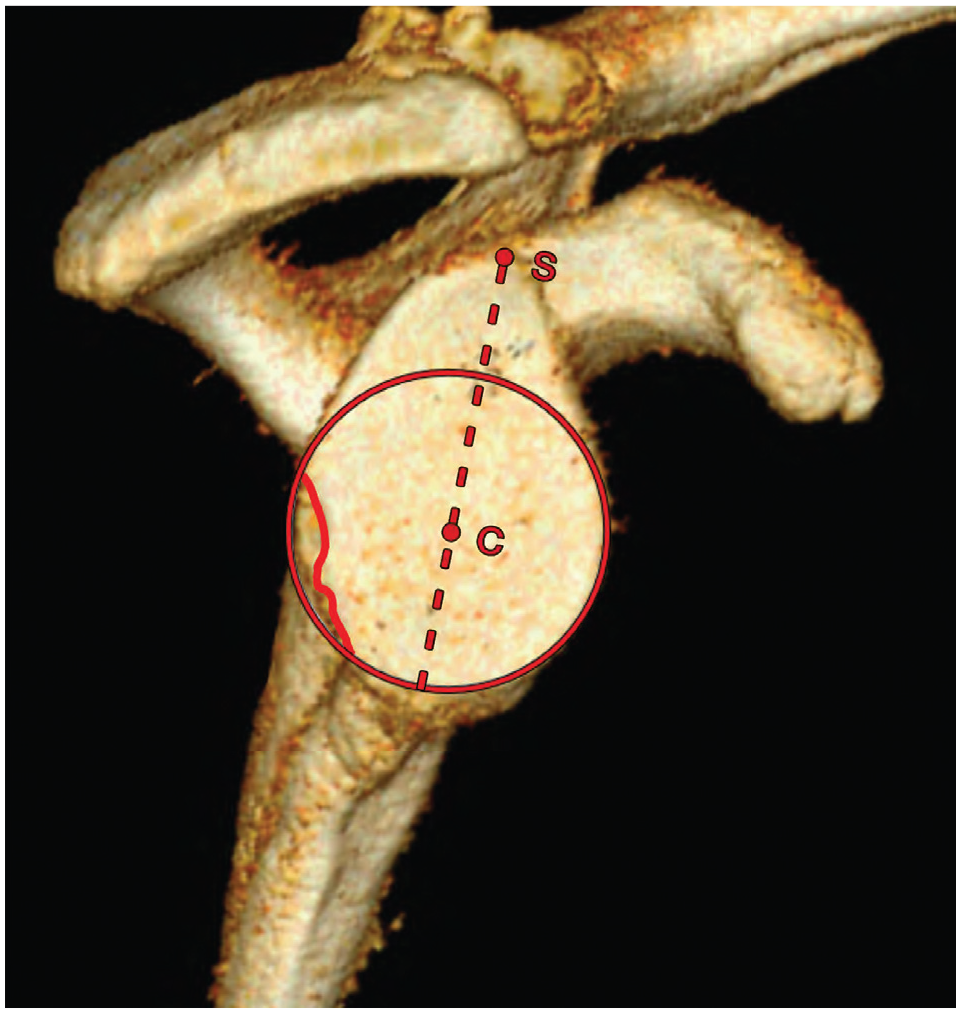
A 3-dimensional reconstructed glenoid with a best-fit circle superimposed on the inferior two-thirds of the en face image of the glenoid. The supraglenoid tubercle was identified, and a line drawn down the center of the circle helped mark the 12-o’clock position and 6-o’clock position. C, center of circle; S, supraglenoid tubercle.
For consistency, regardless of laterality, the 9-o’clock position was posterior and the 3-o’clock position was anterior (Figure 2A). For lesions that extended above the circle of the inferior two-thirds of the glenoid, a line was drawn from the center of the inferior two-thirds of the circle/bare spot and through the proximal aspect of the lesion to give the end clockface time. Location was tabulated in 2-minute intervals. The location, orientation, and extent of posterior glenoid bone deficiency of each patient were recorded. The location of the lesion was determined by the most superior and inferior aspects of where the lesion was located, and the extent was expressed in both time (ie, 6:00-9:00) and total angle (ie, 6:00-9:00 = 90°) (Figure 2B). The mean orientation of the defect was expressed similar to that as previously defined in the setting of anterior bone loss by Saito et al 15 : a line was created perpendicular to the defect margin and passed through the center of the circle to provide a mean time of orientation of the defect. To measure the angle at which bone loss occurred relative to the long axis of the glenoid, a best-fit line was superimposed over the location of the lesion, and the angle was determined by its intersection with the line drawn down the center of the circle originating at the supraglenoid tubercle (Figure 3). The same three authors independently measured all 71 3D CT reformatted images, identifying the location and extent of bone loss. Both extent of the lesion and location (start and stop points) were compared by the 3 authors to calculate interobserver reliability. A single author (T.J.D.) reevaluated and identified the location in a blinded fashion to the prior results, evaluating the extent of the posterior bone deficiency in 40 of the 71 glenoids 4 weeks after initial evaluation to verify intraobserver reliability.
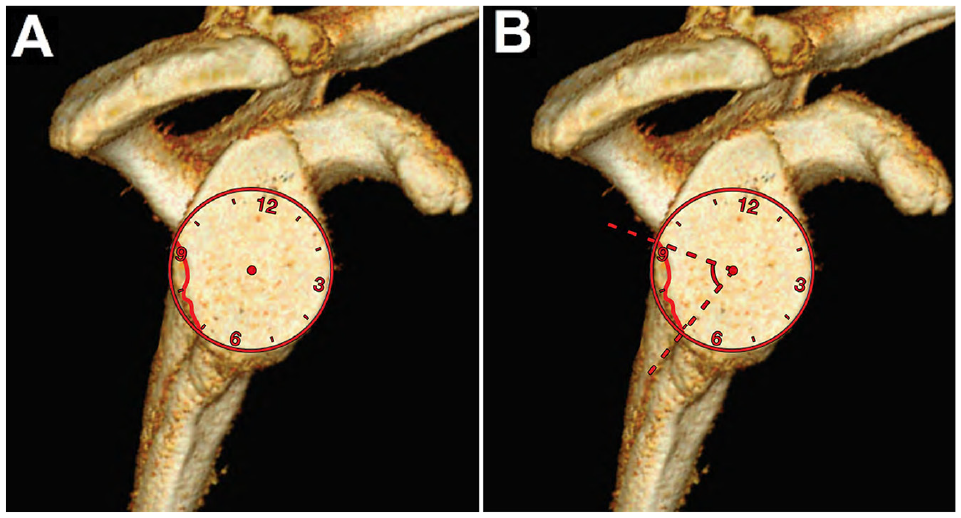
(A) A clockface was created utilizing the best-fit circle on the inferior two-thirds of the glenoid, with the 9-o’clock position representing posterior and the 3-o’clock position representing anterior. (B) The location of the defect was measured using the most superior and inferior aspects of the defect, and the extent was expressed in time and degrees.
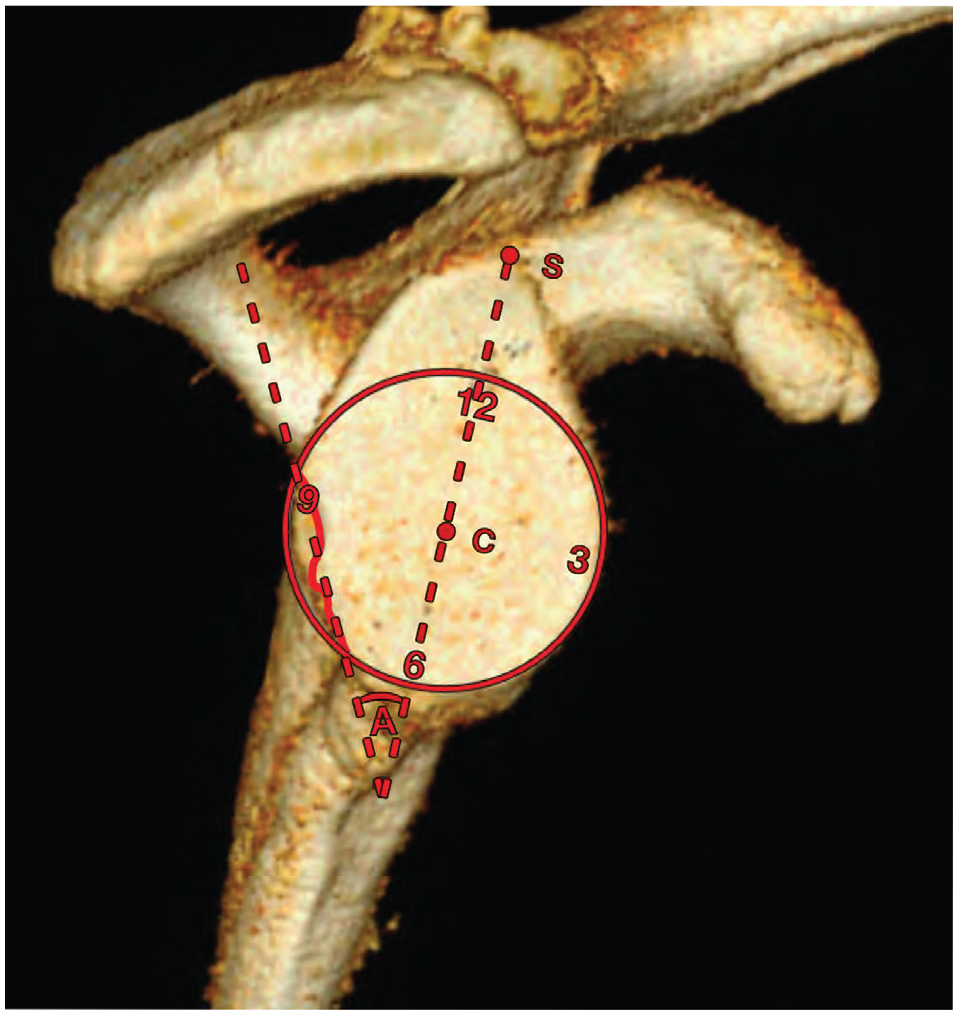
The angle to the long axis of the glenoid is found by measuring the angle created by the intersection of a best-fit line superimposed over the lesion and a line drawn down the center of the circle originating at the supraglenoid tubercle. A, angle of the posterior glenoid defect; C, center of the glenoid; S, supraglenoid tubercle.
Results
A total of 71 shoulders were reviewed of 70 males and 1 female, with a mean age of 29.3 years (range, 24.4-35.1 years). The mean clockface location of the posterior glenoid defect originated at 6:44 (range, 4:16-8:12) and extended to 9:28 (range, 7:02-10:38). This corresponded to a mean location of 8:06 on the superimposed clockface (Figure 4). The mean extent of the posterior glenoid defect on the clockface was 2:43 (range, 1:08-4:50), which corresponds to a mean total bone loss arc of 81.5° (range, 34.2°-144.9°). A summary of this study’s findings can be found in Table 1. Another novel finding of this study is that unlike anterior glenoid bone loss, which has been found to occur parallel to the long axis of the glenoid, posterior bone loss occurred at a mean angle of 30.7° (range, 8.0°-80.0°) relative to the long axis of the glenoid. The frequency of the posterior glenoid defect at every 10-minute interval (5° of arc) was 85% or greater between 7:30 and 9:00, and 90% or greater between 7:40 and 8:50 (Figure 5). The interobserver reliability of the measurements repeated by the 3 raters had an intraclass correlation coefficient (ICC) of 0.944 (95% CI, 0.909-0.968). When a single observer graded 40 (56.3%) of the glenoid 3D CT scans blinded for a second time 4 weeks after initial measurements were performed, the intraobserver reliability was calculated to have an ICC of 0.994.
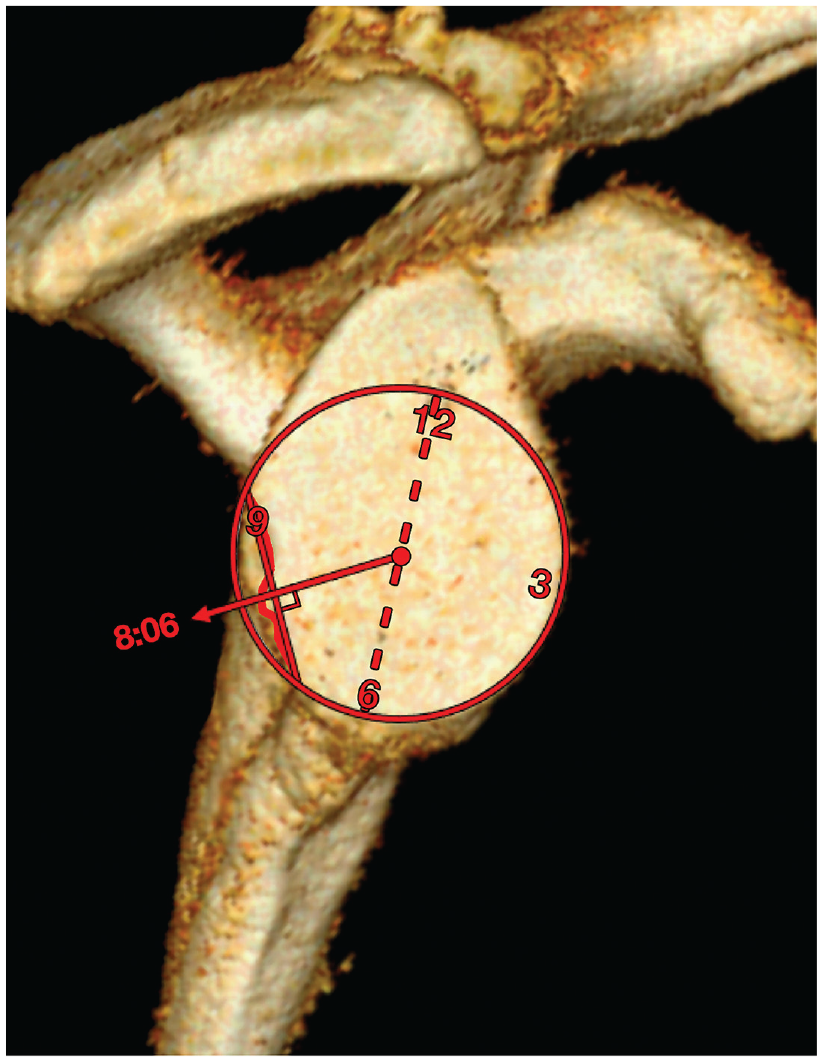
The mean orientation of the defect was pointing toward 8:06 on the clockface of the glenoid.
Location and Extent of the Glenoid Defect
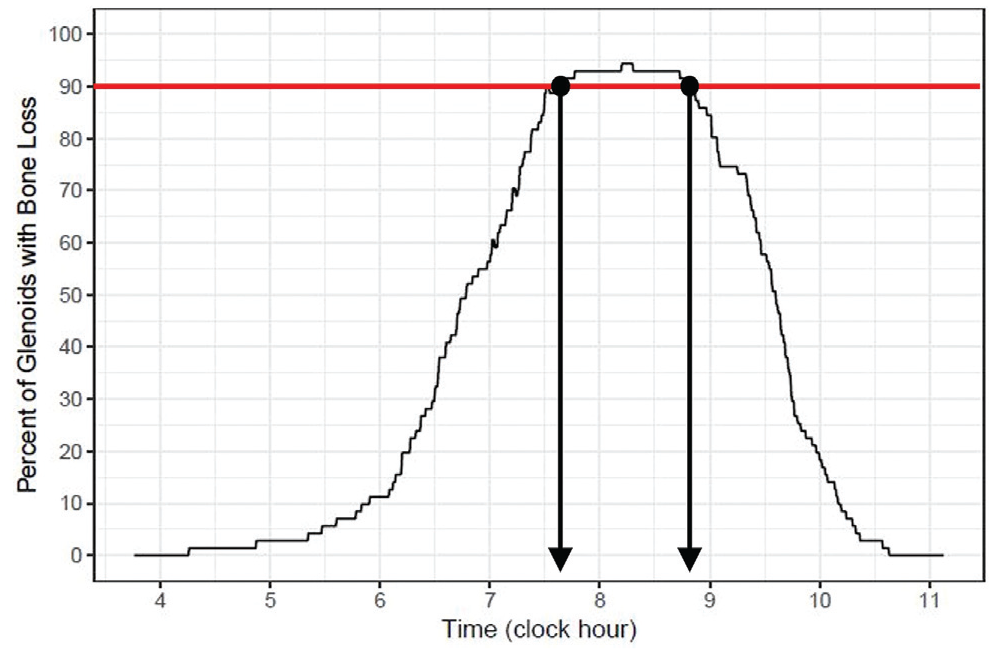
Frequency distribution of the glenoid defect. The frequency of the posterior glenoid defect at 10-minute intervals (5° of arc) was 90% or greater between 7:40 and 8:50.
Discussion
The primary finding of this study was that the posterior bony defect was most commonly oriented in a posteroinferior direction, thereby confirming our original hypothesis. Moreover, the bone loss that was assessed and characterized in this patient cohort occurred at a mean 30.7° posterior to the long axis of the glenoid. The present study is novel in that it is the first clinical study to quantify the location of posterior bone loss in the setting of posterior glenohumeral joint instability. The mean posterior bone loss defect extended from 6:44 to 9:28, with 90% of the defects observed demonstrating bone loss between 7:40 and 8:50. While some studies have investigated the average size of posterior glenoid defects,7,13 this study uniquely contributes to the knowledge of posterior bone loss location, which has implications on both clinical treatment and future research studies to more accurately evaluate stability in the setting of posterior bone loss.
Bone loss was evaluated using the best-fit circle technique as initially described by Burkhart et al 3 when evaluating glenoid bone loss arthroscopically. Furthermore, this study evaluates the bone loss location with the utilization of 3D CT reformats similar to that of Sugaya et al, 20 who evaluated anterior glenoid bone loss morphology. This method assumes that the inferior two-thirds of the glenoid approximates a circle 3 and is reliable in measuring glenoid bone loss.6,8,20 When the clockface was applied to the inferior two-thirds of the glenoid, high intra- and interobserver reliability was found. Furthermore, it is a practical and reproducible method to evaluate the location of the lesion in the en face axial view when evaluating 3D CT scan reformats.
In the setting of posterior shoulder instability, both acute and chronic, we found that the lesion is most commonly located in the posteroinferior quadrant of the glenoid, which is similar to the findings previously described by Weishaupt et al. 21 The authors found that 93% (14/15) of patients with recurrent atraumatic posterior shoulder instability had a deficiency of the posteroinferior glenoid rim, with a craniocaudal length of 12 mm predicting the highest sensitivity and specificity. The mean location in our series of 71 consecutive patients evaluated spanned from 6:44 to 9:28, with nearly all of the lesions contained between 7:40 and 8:50. Regardless of cause, knowledge of the exact location of the most commonly found posterior glenoid bone loss allows the surgeon to more accurately identify and then replicate posterior shoulder stabilization procedures.
Current biomechanical studies of posterior glenoid bone loss have yielded a basic understanding of posterior shoulder instability and the effects of soft tissue repair versus the addition of bone augmentation. The vast majority of current biomechanical models for posterior bone loss have been modeled off of studies evaluating the effects of anterior bone loss in the setting of anterior shoulder instability, with lesions created parallel to the long axis of the glenoid, as first described by Saito et al. 15 Yamamoto et al 24 studied the stabilizing effect of bone grafting over soft tissue repair with superior-inferior osteotomies made tangential to the long axis of the glenoid, helping explain the biomechanical importance of critical bone loss in anterior instability. Similarly, Nacca et al 13 in a recent biomechanical study of posterior bone loss found that >20% bone loss of the glenoid leads to persistent posterior shoulder instability in the setting of a soft tissue repair alone. However, in their methods, bone loss defects were created in a vertical fashion parallel to the long axis of the glenoid. This methodology conflicts with the findings of the present study, which demonstrated that a mean posterior glenoid lesion occurs 30.7° relative to the long axis of the glenoid. The findings of the present study dispute the proposed location of bone loss proposed by Nacca et al, which may alter the biomechanical properties of the glenohumeral joint when evaluating posterior shoulder instability. Our findings may account for the clinical results reported by Hines et al, 7 who found that clinical outcomes were affected less in the setting of posterior bone loss compared with those seen in anterior shoulder instability. Therefore, further biomechanical studies with accurate lesion location are required to accurately identify critical bone loss in the setting of posterior shoulder instability.
The literature regarding posterior shoulder instability with glenoid bone loss lacks uniformity in technique, thus making evaluation of outcomes difficult. For posterior bone block placement in particular, promising clinical results have been reported4,12; however, in the techniques they describe, the authors fail to specify the ideal location of the bone block placement. Posterior bone block augmentation has complication rates up to 36%, with many patients developing recurrent instability.4,11,16,17 Without the accurate identification of the ideal location for graft placement/greatest bone loss, these patients may be at increased risk of further instability. In this context, our findings precisely locate glenoid bone loss as well as provide angular orientation off of the long axis of the glenoid, both of which may aid in optimizing bone block placement procedures and thereby improve surgical outcomes.
We acknowledge some limitations to the present study. Due to this study’s being the first to describe posterior bone defect location and being descriptive in nature only, a power analysis was not performed. This study did not use chart review to correlate our imaging findings with patient demographics and presentation. Thus, we are unable to differentiate between glenoid dysplasia and glenoid bone loss as causes for instability. Also, we are unable to comment on the relationship between size or location of the defect and surgical procedures and outcomes. Glenoid retroversion and large reverse Hill-Sachs lesions have also been identified as osseous risk factors for recurrent posterior instability, but they were not measured in this study.
Conclusion
Posterior bone defects in the setting of posterior shoulder instability most commonly occur in the posteroinferior quadrant of the glenoid and extend on average from 6:44 to 9:28 (81.5°) on a clockface model. Posterior bone loss occurs at a mean of 30° off the long axis of the glenoid in a posteroinferior direction, which is historically different from anterior bone loss, which occurs parallel to the long axis of the glenoid. This study serves to highlight the location and orientation of bone loss that one can expect in a patient with recurrent posterior shoulder instability, although additional work is needed to assess why this develops.
Supplemental Material
AJSM_Supplement_to_the_ICMJE_Disclosure_Form_Revised_7.8.19 – Supplemental material for Location of the Glenoid Defect in Shoulders With Recurrent Posterior Glenohumeral Instability
Supplemental material, AJSM_Supplement_to_the_ICMJE_Disclosure_Form_Revised_7.8.19 for Location of the Glenoid Defect in Shoulders With Recurrent Posterior Glenohumeral Instability by Travis J. Dekker, Liam A. Peebles, Brandon T. Goldenberg, Peter J. Millett, James P. Bradley and Matthew T. Provencher in The American Journal of Sports Medicine
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: M.T.P. reports royalties, consulting fees, and hospitality fees from Arthrex, and personal fees from Joint Research Foundation. T.J.D. has received education payments from Smith & Nephew. P.J.M. reports consulting fees and royalties from Arthrex Inc, Medbridge, and Springer Publishing; holds stock in GameReady and VuMedi; and receives institutional funding from Smith & Nephew, Arthrex, Siemens, and Össur. J.P.B. reports personal fees from Arthrex, Inc outside the submitted work, and is president of the American Orthopaedic Society for Sports Medicine (2019-present). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.