
Abstract
Background:
There is evidence that tibial slope may play a role in revision risk after anterior cruciate ligament reconstruction (ACLR); however, prior studies are inconsistent.
Purpose:
To determine (1) whether there is a difference in lateral tibial posterior slope (LTPS) or medial tibial posterior slope (MTPS) between patients undergoing revised ACLR and those not requiring revision and (2) whether the medial-to-lateral slope difference is different between these 2 groups.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
We conducted a matched case-control study (2006-2015). Cases were patients aged ≤21 years who underwent revision surgery after primary unilateral ACLR; controls were patients aged ≤21 years without revision who were identified from the same source population. Controls were matched to cases by age, sex, body mass index, race, graft type, femoral fixation device, and post-ACLR follow-up time. Tibial slope measurements were made by a single blinded reviewer using magnetic resonance imaging. The Wilcoxon signed rank test and McNemar test were used for continuous and categorical variables, respectively.
Results:
No difference was observed between revised and nonrevised ACLR groups for LTPS (median: 6° vs 6°, P = .973) or MTPS (median: 4° vs 5°, P = .281). Furthermore, no difference was found for medial-to-lateral slope difference (median: −1 vs −1, P = .289). A greater proportion of patients with revised ACLR had an LTPS ≥12° (7.6% vs 3.8%) and ≥13° (4.7% vs 1.3%); however, this was not statistically significant after accounting for multiple testing.
Conclusion:
We failed to observe an association between revision ACLR surgery and LTPS, MTPS, or medial-to-lateral slope difference. However, there was a greater proportion of patients in the revision ACLR group with an LTPS ≥12°, suggesting that a minority of patients who have more extreme values of LTPS have a higher revision risk after primary ACLR. A future cohort study evaluating the angle that best differentiates patients at highest risk for revision is needed.
Anterior cruciate ligament reconstruction (ACLR) is one of the most common orthopaedic procedures performed in the United States and has been shown to restore knee stability and improve functional outcomes.3,7,47 However, failures do occur, with reported revision rates between 4% and 13%.28,53 Compared with knees with primary ACLR, those with revision ACLR can have increased cartilage and meniscal damage, as well as decreased clinical and functional outcomes.6,8,27 Risk for revision after primary ACLR is multifactorial.1,18,29,30,33,45 Posterior tibial slope has recently been cited as an anatomic factor that may influence the need for revision.
Changes in the slope of the tibial plateau affect the biomechanics of the knee and the forces seen by the knee ligaments. 2 Multiple studies have found an increased lateral tibial posterior slope (LTPS) on magnetic resonance imaging (MRI) to be a risk factor for primary ACL injury,4,11,13,15,23,51 with confirmation of these findings in a large systematic review 58 and meta-analysis. 54 Recent studies have indicated that an increased tibial slope may also be a factor associated with revision risk after ACLR,9,17,25,26,42,55 reporting a slope ≥12° to be associated with a higher risk of revision.25,42,44,55 Some of these studies measured tibial slope with lateral radiographs,25,42,55 which are limited in their ability to evaluate the complex 3-dimensional geometry of the tibial plateau.12,15,56 In studies that measured LTPS with MRI,9,17,26,43 results have been inconsistent, with an increase in LTPS ranging from 1° to 5° being associated with revision. One study found LTPS to play a role for female patients only, while another reported an association for ACLR performed through medial portal drilling only. 43 Some of this inconsistency in reporting across studies might be due to smaller sample sizes, with the largest including 57 cases of revision ACLR, 17 or to potential selection bias in identifying controls from a different source population than the cases. Given the variability in the literature, confirmation of these early reports on LTPS in a larger sample is needed.
A number of studies evaluating the medial tibial posterior slope (MTPS) found no association with primary ACL injury.13,15,23 Two studies that used MRI found a greater MTPS associated with revision risk after ACLR.17,26 These findings have yet to be confirmed in a younger cohort undergoing ACLR. An additional hypothesis to be investigated is the difference between MTPS/LTPS and revision risk, as a flatter MTPS with a greater LTPS may lead to rotational movement of the knee and increased strain on the ACL graft.11,13,48
The purpose of this study was to use the Kaiser Permanente ACLR registry to evaluate the following questions for patients aged ≤21 years: (1) Is there a difference in LTPS or MTPS between patients with revised and nonrevised ACLR? (2) Is the medial-to-lateral slope difference variant for revised or nonrevised ACLR? Our hypothesis was that there is a difference in LTPS, MTPS, and medial-to-lateral slope between patients with revised and nonrevised ACLR.
Methods
Study Design and Sample
To reduce the cost of measuring each patient’s slope, a matched case-control study5,49 was conducted. The study sample was identified with data from the Kaiser Permanente ACLR registry. This integrated health care system covers 12.3 million members throughout 8 geographic regions. 20 This patient population has largely been shown to be demographically and socioeconomically representative of the area that it covers.22,24
Cases and controls were selected from the same cohort of patients aged ≤21 years with a closed physis who underwent primary isolated ACLR (2006-2015). Double bundle surgery, bilateral surgery, and patients with a prior ACLR were excluded. Cases included all patients undergoing primary ACLR who subsequently underwent aseptic revision. Revision was defined as the aseptic failure of the primary graft where removal and replacement of the graft were required. The control group was matched to the case group on the basis of follow-up (defined for a case as the time from primary ACLR to revision surgery) in addition to other covariates (specified later), and it comprised patients undergoing primary ACLR who did not have revision surgery. Specifically, a patient who underwent revision 2 years after the primary ACLR was matched to a control patient who had not undergone revision at 2 years postoperatively, and a patient who underwent revision 4 years after the primary ACLR was matched to a control patient who had not undergone a revision at 4 years postoperatively.
Data Source
Data collection and data quality procedures for the registry have been previously described.32,37 In brief, this surveillance tool for all ACLR procedures performed within Kaiser Permanente collects a predefined set of information (patient, procedure, implant, surgeon, and hospital) with paper-based and electronic intraoperative forms that are completed at the point of care by the operating surgeon. Additional sources (ie, electronic medical records, claims files, and other data repositories within the institution) are used to extract supplemental data. 31 Once included into the registry, the patient is monitored longitudinally for postoperative complications, including revisions, which are then reviewed and validated by trained clinical content experts using the electronic medical record. All patients are followed indefinitely until death or if they leave the health care plan membership. Voluntary participation to the ACLR registry was 93% in 2011. 37
Exposure of Interest
LTPS and MTPS were the exposures of interest. Slopes were measured in whole degree intervals from MRI scans captured before the primary ACLR. Of the initial 732 patients who underwent ACLR (366 case-control pairs), MRI scans were unavailable for 51, leaving a final matched sample of 634 patients (317 case-control pairs). Slopes were evaluated continuously. Medial-to-lateral tibial slope difference was calculated as the difference between the MTPS and LTPS and evaluated continuously.
MRI Measurements
MRI was used to measure the both the LTPS and the MTPS based on the method described by Hashemi et al. 15 MRI images were viewed with Carestream VueMotion software (v 12.1.5.7529; Carestream Health, Inc), and graphic overlay software (PixelStick, v 2.10.1; Plum Amazing) was used for value measurements. Sagittal and axial images were viewed in linked panes and scrolled to identify the center of the lateral or medial tibial plateau on the axial image; measurements were then taken from the corresponding linked position on the sagittal images. The center of the tibial shaft was marked at 2 points, and a connecting line was used to define the tibial axis. The LTPS and MTPS were measured at the level of the cartilage based on a line that was 90° to the axis of the tibia (Figure 1). All measurements were performed by 1 clinical investigator (J.D.C.), who was blinded to the patients’ case-control status.
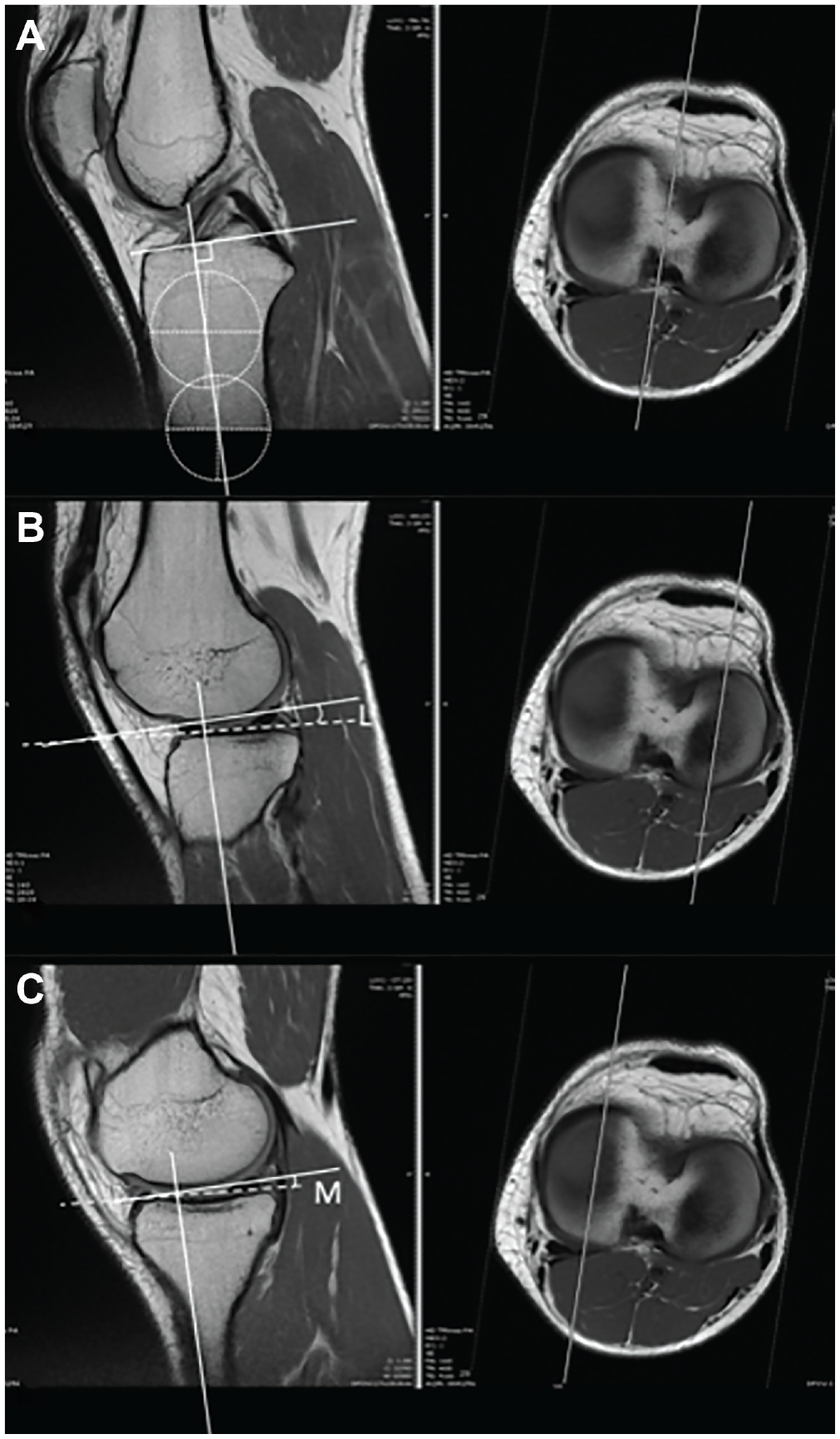
Measurement of the medial and lateral tibial posterior slope on magnetic resonance imaging. (A) Identification of the center of the tibia with the corresponding views on axial and sagittal imaging. Circles with crosshairs identify the center of the tibia at the lowest possible point at the base of the image and a second point below the metaphyseal flair. A corresponding line (solid white) connects these points; a 90° line is used for the reference. Slope measurement of (B) the lateral tibial plateau and (C) the medial tibial plateau is done using the linked sagittal (left) and axial (right) images. The sagittal position for measurement is at a point centered posteriorly on the plateau in the linked axial view. The slope is measured on the sagittal view with a line drawn between 2 points based at the tip of the cartilage and centered under the visible anterior and posterior portions of the respective menisci. The angle shown as L (lateral) and M (medial) are the measured values.
Covariates
In addition to follow-up time, the following were used to match controls to cases: age (continuous), body mass index (BMI; continuous), sex, race (Asian, black, Hispanic, other, and white), graft type (bone–patellar tendon–bone, hamstring, nonprocessed allograft, and processed allograft), and femoral fixation device type (combination, cross-pin, interference, and suspensory). Allografts chemically treated or irradiated were classified as processed, and allografts harvested aseptically were classified as nonprocessed. Combination fixation was defined as >1 fixation device used on the femoral side.
Statistical Analysis
Novel matching methods have been recently proposed to achieve finer covariate balance than propensity score matching methods.40,59 These newer methods ensure that after the match, the marginal distributions of nominal variables between the matched groups are identical or almost identical (eg, the same or almost the same number of males or females). We used the R package rcbalance 38 to perform our match via minimizing a distance defined through the Mahalanobis distance function. 41 Nonrevised controls were matched to revised cases on the covariates listed previously before the ascertainment of the slopes. To account for the follow-up time from primary ACLR to revision and enable a fair follow-up comparison between groups, a penalty was applied if a control with a shorter follow-up time was going to be matched with a case whose follow-up time was longer. 39 The Wilcoxon rank sum test was used for continuous covariates and the Fisher exact test for binary covariates to assess the final match balance between cases and controls. The LTPS, MTPS, and medial-to-lateral tibial slopes between revised and nonrevised ACLR were tested with the Wilcoxon signed rank test to account for matching in our study design. 57 An alpha of .05 (2-tailed) was used as the threshold for statistical significance.
We performed a secondary exploratory analysis evaluating whether a slope has a higher proportion of cases or controls with that degree measurement or greater. The frequency of specific LTPS and MTPS was tested with the McNemar test. 36 Based on the number of tests performed in this exploratory analysis, a sequential Bonferroni approach was applied to arrive at conclusions about statistical significance. 16
Results
There were 317 cases and 317 controls included in the study sample. Median time from primary ACLR to revision for the cases was 1.6 years (range, 0.2-8.6 years). Follow-up time to revision was part of the matching criteria so that a patient in the case group who, for example, had a revision at 2 years postoperatively was matched to a control patient who was revision-free at 2 years postoperatively, but the overall follow-up time of the control group was longer than the time to revision for the case group. Median follow-up for the control group was 4.4 years (range, 1.0-9.4 years). After the match was completed, all standardized absolute differences were less than the 0.10 threshold, and no P value indicated covariate imbalance (Figure 2). Mean BMI and age for revised ACLR were 24.5 kg/m2 (SD, 4.0) and 17.1 years (SD, 1.7). Revised ACLR was more common among male patients (53.6%) and white patients (46.7%), and was more often performed with an interference fixation device (44.2%) and a hamstring autograft (38.8%) (Table 1). Results were similar for nonrevised ACLR: mean BMI, 24.5 kg/m2 (SD, 4.0); mean age, 17.2 years (SD, 1.6); male, 51.4%; white, 48.6%; interference femoral fixation, 44.5%; and hamstring autograft, 39.8%.
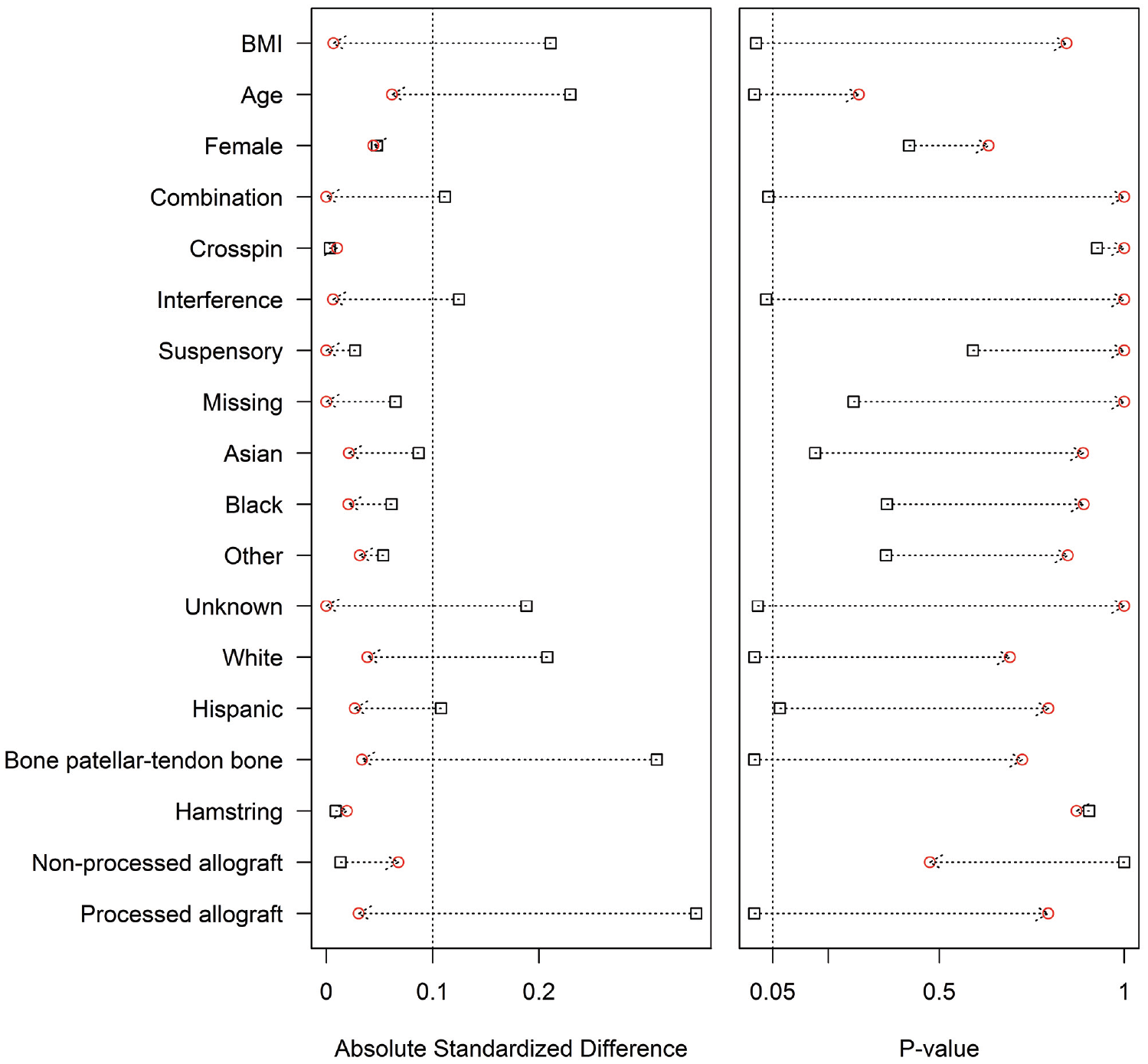
Absolute standardized difference and P value for covariates between cases and controls before matching (square) and after matching (circle). After the match, all standardized absolute differences were less than the 0.10 threshold, and no P value indicated covariate imbalance (P > .05). BMI, body mass index.
Patient, Graft, and Fixation Device Characteristics at the Time of the ACLR After Matching: Revised (n = 317) and Nonrevised (n = 317) a
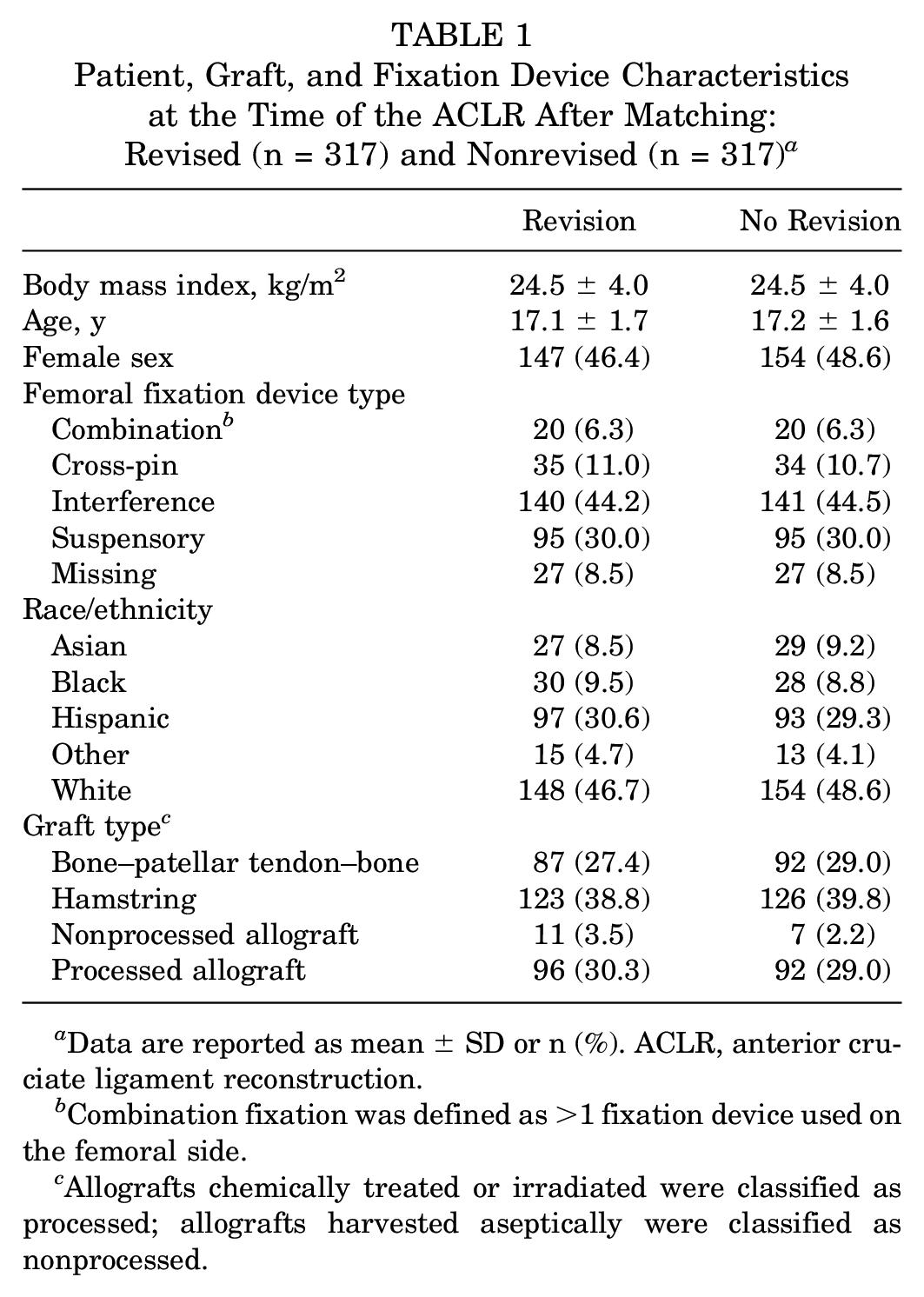
Data are reported as mean ± SD or n (%). ACLR, anterior cruciate ligament reconstruction.
Combination fixation was defined as >1 fixation device used on the femoral side.
Allografts chemically treated or irradiated were classified as processed; allografts harvested aseptically were classified as nonprocessed.
Figure 3 presents the distribution of LTPS, MTPS, and medial-to-lateral slope difference for the revised and nonrevised ACLR groups; distributions for LTPS and MTPS were right skewed for both groups. No difference was observed between revised and nonrevised ACLR groups in median LTPS (median, 6° vs 6°; P = .973) or MTPS (median, 4° vs 5°; P = .281) (Table 2). Furthermore, no difference was observed between cases and controls when the medial-to-lateral slope difference was evaluated (median, –1 vs –1; P = .289). When the MTPS and LTPS were compared, no difference was observed between the proportion of revised and nonrevised ACLR where the LTPS was less than the MTPS (20.2% vs 25.9%; P = .096), the LTPS was equal to the MTPS (15.1% vs 13.9%; P = .731), or the LTPS was greater than the MTPS (64.7% vs 60.3%; P = .261).
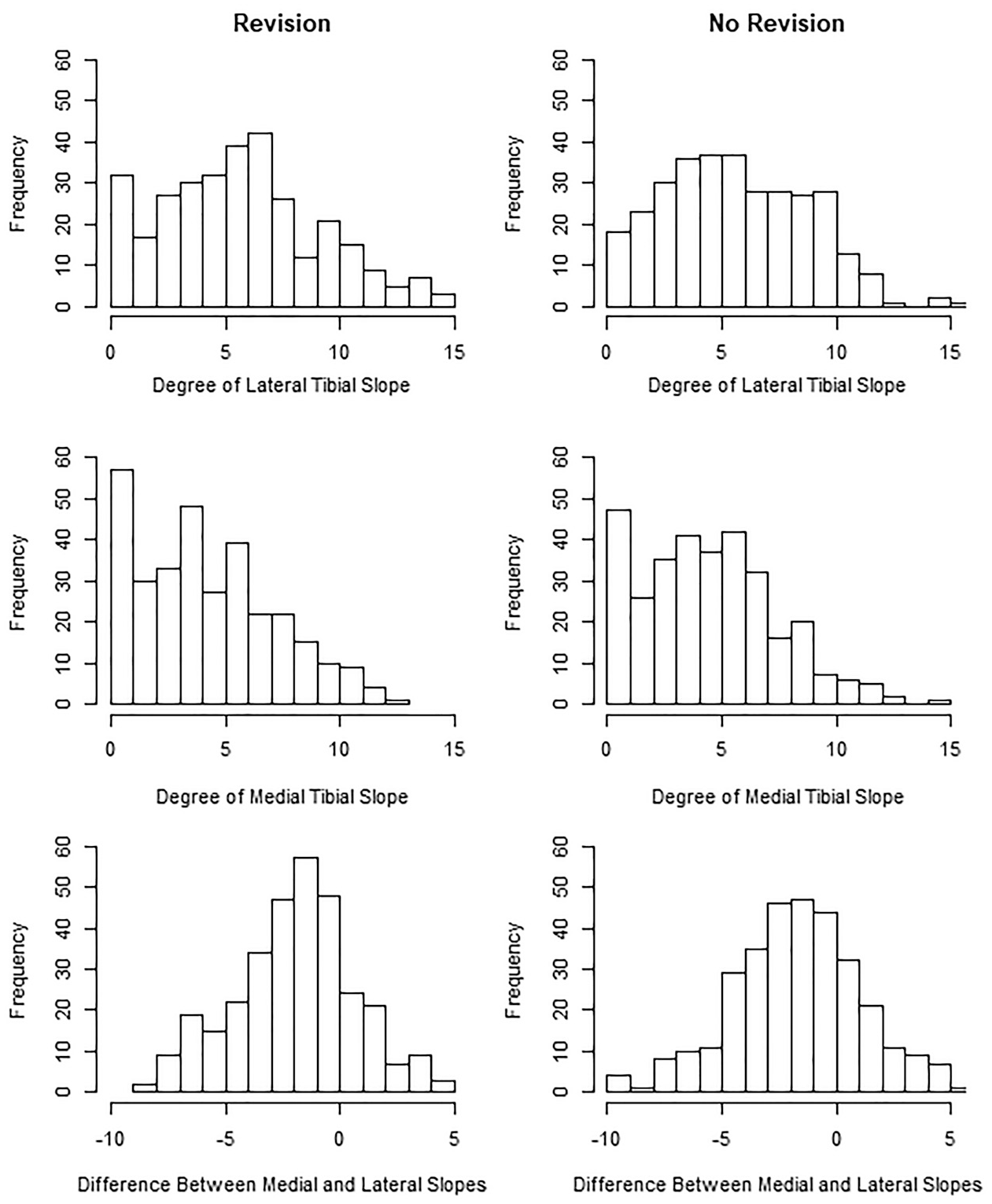
Distribution of the lateral tibial posterior slope (top panel), medial tibial posterior slope (middle panel), and medial-to-lateral slope difference (bottom panel) for 317 revision and 317 nonrevision anterior cruciate ligament reconstructions.
LTPS and MTPS Results for 317 Revised and 317 Nonrevised Anterior Cruciate Ligament Reconstructions a
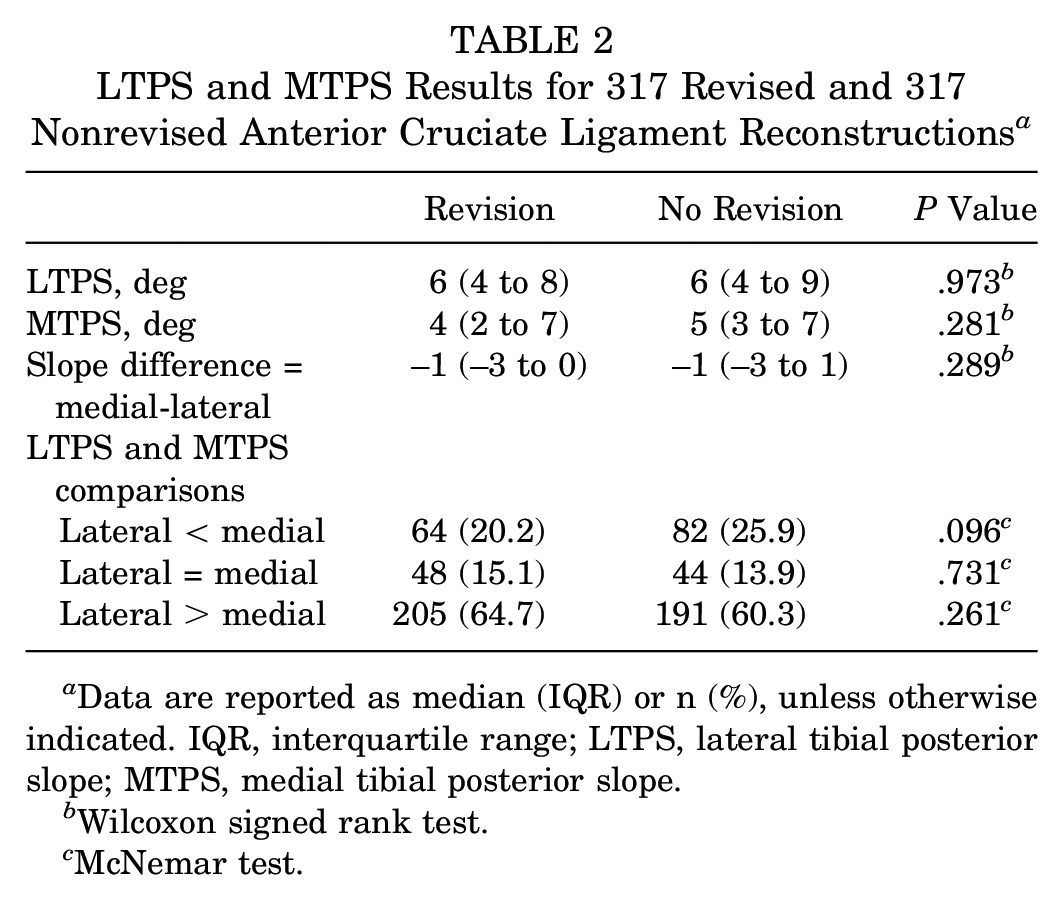
Data are reported as median (IQR) or n (%), unless otherwise indicated. IQR, interquartile range; LTPS, lateral tibial posterior slope; MTPS, medial tibial posterior slope.
Wilcoxon signed rank test.
McNemar test.
In a secondary exploratory analysis, when the 317 matched case-control pairs were directly investigated, there were 144 (45.4%) pairs where the revision patient had a greater LTPS than the nonrevision patient, 26 (8.2%) pairs where the LTPS was the same, and 147 (46.4%) pairs where the revision patient had a smaller LTPS than the nonrevision patient. Respective proportions for the MTPS were 131 (41.3%), 26 (8.2%), and 160 (50.5%), respectively, and for medial-to-lateral slope difference, 138 (43.5%), 35 (11.0%), and 144 (45.4%), respectively. When individual degree measurements of the LTPS were evaluated, the case group had a greater proportion with a slope ≥2° than the control group (94.3% vs 89.9%). The revision group had a greater proportion of patients with slopes ≥12° (7.6% vs 3.8%) and ≥13° (4.7% vs 1.3%) than the control group. However, these findings were not statistically significant after correcting for the number of tests performed (Table 3). No differences were observed between the revised and nonrevised ACLR groups and a specific MTPS (Appendix Table A1, available in the online version of this article) or medial-to-lateral slope difference (Appendix Table A2, available online).
LTPS Characteristics for 317 Revised and 317 Nonrevised Anterior Cruciate Ligament Reconstructions a
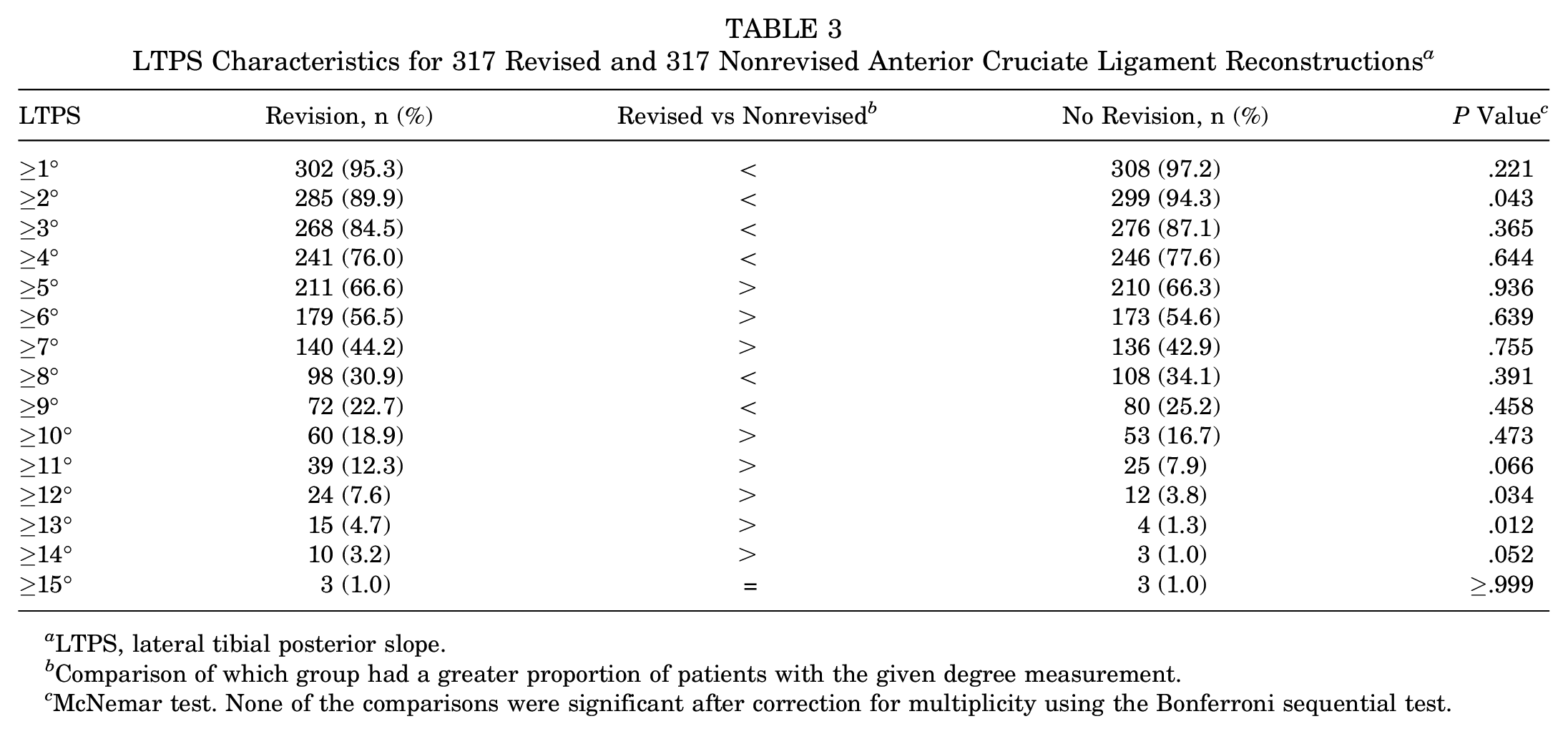
LTPS, lateral tibial posterior slope.
Comparison of which group had a greater proportion of patients with the given degree measurement.
McNemar test. None of the comparisons were significant after correction for multiplicity using the Bonferroni sequential test.
Discussion
Increased slope of the tibial plateau is associated with ACL injury, and recent research has focused on ascertaining its role in revision risk after ACLR.9,17,25,26,42,43,55 However, recent studies examining graft failure and revision after ACLR have reported inconsistent results, and none have specifically evaluated a skeletally mature young active population. Our matched case-control study included ACLR patients ≤21 years who underwent revision (n = 317) and who did not undergo revision (n = 317), matched on age, sex, BMI, race, graft type, femoral fixation type, and follow-up after the primary ACLR. In the current work, we failed to observe a difference in LTPS or MTPS between the revised and nonrevised ACLR groups when evaluated continuously or in the variation between the medial and lateral plateaus.
Our findings contrast with recent case-control studies that used MRI to measure LTPS. Jaecker et al 17 reported a 1° increase in LTPS to associate with a higher likelihood of revisions. Sauer et al 43 found an association between LTPS and graft failure in ACLR only when performed through the medial portal technique. We did not include tunnel drilling technique as part of the matching criteria; however, the distribution of patients who had transtibial versus anteromedial drilling was not different between the revised and nonrevised groups (data not shown). Christensen et al 9 and Li et al 26 reported a higher likelihood of revisions for every ≥2° and ≥5° increase in LTPS, respectively, suggesting that more severe angles of LTPS may have a role in revision risk after primary ACLR. Potential reasons for the differing results observed across these studies as well as ours include the following: (1) differences in definition of the case group, with some including revised ACLR only and others including graft failures with or without revision; (2) differences in identification of controls and the source population from which the control group was composed, potentially creating selection bias; (3) differences in follow-up time, with some studies having shorter follow-up for the control group than the case group, potentially creating misclassification bias since it is unknown whether these control patients would have eventually undergo revision ACLR given the same length of follow-up; (4) differences in the ages of the study populations; and (5) variation in sample sizes. In an effort to minimize potential biases, our study sample of >600 adolescent patients who underwent revised and nonrevised ACLR was identified with our integrated health care system’s ACLR registry, and exclusion criteria were applied before identification of a case group and selection of a control group. Furthermore, our match included follow-up time to ensure that a patient classified as a control really was revision-free at the same point during postoperative follow-up as the patient with a revision. While we failed to observe an association between LTPS and revision status, our exploratory analysis suggested that greater degrees of LTPS may have an effect on revision after ACLR.
A 12° rule has been suggested from prior studies evaluating posterior tibial slope via lateral radiographs. 44 Webb et al 55 initially reported that patients with a posterior tibial slope ≥12° had the greatest risk for further injury after ACLR, although they failed to find a difference in mean posterior tibial slope when comparing patients with intact ACLR grafts and those with ruptured grafts. Using data from the same series, Salmon et al 42 found that only 22% of adolescent patients (≤18 years of age) with a tibial slope ≥12° had an intact graft at 20-year follow-up; no difference in graft revision was found between adult patients with and without a posterior tibial slope ≥12°. Lee et al 25 further confirmed the 12° rule. Limitations have been reported in the use of radiographs for measurement of tibial slope based on the complex geometry of the tibial plateau, 15 including a significant effect of minor rotation on the perception of posterior tibial slope, 56 as well as a limited ability to estimate tibial axis based on knee radiographs. 12 In our exploratory analysis, we did find that there were twice as many revision ACLRs than nonrevision ACLRs with a slope ≥12°, although this was not statistically significant after correcting for multiplicity. Given our matched case-control study design and variable timing of the outcome investigated, we were unable to evaluate which degree measurement may best identify patients at higher risk for revision surgery through a receiver operating characteristic curve analysis. This is a limitation of our study. A future cohort study including an entire ACLR population, rather than selected case-control groups, is needed.
Our ACLR revision findings are in line with prior studies reporting no association between MTPS and ACL injury.15,50,52 This is in contrast to 2 prior case-control studies reporting MTPS to be associated with revision surgery.17,26 Biomechanical studies suggest that an increased LTPS as compared with a more level MTPS may lead to a possible simulated pivot shift with the knee in extension11,48 and therefore an increased force on the ACL.14,35,46 While this concept is biomechanically logical, our clinical study failed to observe a difference in the medial-to-lateral tibial slope between revised and nonrevised ACLR.
Our study has several limitations. First, this is a case-control study; causality cannot be determined. We used our institution’s ACLR registry, which has a predefined set of variables that are prospectively captured through validated algorithms, leading to high internal validity. Furthermore, the registry includes a diverse patient population that is representative of the geographic regions served by the health care system, with various surgeons who have differing levels of training and expertise, thereby increasing the generalizability of the findings. However, our data were limited to information captured by the registry. Although we carefully matched controls to cases based on a number of factors previously identified to affect ACLR revision, ¶ as well as follow-up time after the primary ACLR, so that a case patient who underwent revision surgery was matched to a control patient who was revision-free at the same time point after the primary ACLR, there is potential for residual confounding. We did not include activity at the time of injury or meniscal injuries/procedures during the primary ACLR as part of the matching criteria; however, the distributions for these variables were not different between the revised and nonrevised groups. We were not able to account for additional variables, such as nonanatomic reconstruction, rehabilitation, time of return to activity, or sports activity level, although we do not have a reason to believe that these variables would differ depending on tibial slope. Second, cases were identified from patients who underwent revision surgery after primary ACLR; that is, patients who experienced a clinical failure but did not undergo subsequent revision surgery were not included in the case group. Inferences regarding tibial slope and clinical failure cannot be made. In addition, patient-reported outcome measures, postoperative radiographic findings, and functional performance tests are not collected by the registry and therefore could not be compared between cases and controls. Third, there was no standardized protocol for MRI acquisition. Tibial rotation can affect LTPS measurements in radiographs. 56 This has not been evaluated with regard to MRI measurement, but it may lead to measurement variation. While MRI can accurately identify the center of the lateral tibial condyle, the rotation of the tibia and the plane of MRI acquisition can affect the point of the tibial plateau from which the measurements are taken, with some being more medial and others more lateral. During MRI review, we found that varying lengths of tibia included in the image affected slope measurement. When the length of tibia included in the image is limited, identification of the true axis of the tibia is more difficult and may affect measurement values. However, the reviewer performing MRI measurements (J.D.C.) was blinded to a patient’s case-control status, and we have no reason to believe that cases were more or less likely than the matched controls to have less tibial length included in their MRI.
Conclusion
In this study of 317 matched revised and nonrevised ACLR among patients aged ≤21 years, we were unable to identify an association between revision surgery and LTPS, MTPS, or medial-to-lateral slope difference. In fact, in our revised and unrevised ACLR groups, the medians for both slope measurements were equal to or almost equal to each other. Rather, greater measurements of LTPS may be associated with revision after ACLR. This suggests that slope of the tibial plateau may not be a risk factor for revision for the majority of patients undergoing ACLR but rather for only a minority with more extreme measurements of LTPS. A future cohort study to confirm our exploratory findings and identify whether there is an angle that best differentiates patients at highest risk for revision is needed.
Supplemental Material
DS_10.1177_0363546519878436 – Supplemental material for The Association Between Tibial Slope and Revision Anterior Cruciate Ligament Reconstruction in Patients ≤21 Years Old: A Matched Case-Control Study Including 317 Revisions
Supplemental material, DS_10.1177_0363546519878436 for The Association Between Tibial Slope and Revision Anterior Cruciate Ligament Reconstruction in Patients ≤21 Years Old: A Matched Case-Control Study Including 317 Revisions by Joseph D. Cooper, Wei Wang, Heather A. Prentice, Tadashi T. Funahashi and Gregory B. Maletis in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors acknowledge the Kaiser Permanente orthopaedic surgeons who contribute to the Kaiser Permanente ACLRR, as well as the surgical outcomes and analysis department staff, which coordinates registry operations. The authors also acknowledge William E. Burfeind, MAS, and Tom S. Huon, BS, for their ongoing support of the Kaiser Permanente ACLRR database and quality control management.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.