
Abstract
Background:
Identification of factors predictive of outcome and change is important to improve treatment for patellofemoral pain (PFP). Few studies have examined the predictive value of psychological factors in PFP, although they have been reported to be important predictors in other musculoskeletal pain conditions.
Purpose:
To evaluate predictors of pain, function, and change 1 year after an exercise-based intervention in PFP.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
In sum, 112 patients were recruited to a randomized controlled trial; 98 attended 1-year follow-up. There were no between-group differences in the trial; thus, the material was analyzed as 1 cohort. Nine baseline factors—sex, bilateral pain, worst pain, pain duration, Anterior Knee Pain Scale (AKPS), kinesiophobia, anxiety and depression, self-efficacy, and number of pain sites throughout the body—were investigated for their predictive ability on outcome at 1 year (AKPS, worst pain) and for change at 1 year (global change score, change in AKPS, and change in worst pain). Multivariable linear regression models with stepwise backward removal method were used to find predictors of poor outcome.
Results:
Number of pain sites at baseline was a significant predictor of worse outcome for AKPS (B = −2.7; 95% CI, –4.0 to −1.3; P < .01), worst pain (B = 0.5; 95% CI, 0.2-0.8; P < .01), global change (B = −0.8; 95% CI, –1.2 to −0.5; P < .01), change in AKPS (B = −2.7; 95% CI, –4.0 to −1.3; P < .01), and change in worst pain (B = 0.5, 95% CI, 0.2-0.8; P < .01) at 1 year. Baseline scores for AKPS and worst pain predicted respective 1-year levels and change scores (P < .01). Lower self-efficacy and male sex predicted less global change (P < .01). Longer pain duration predicted final score and change score for worst pain (P < .01). The predictive models had reasonable fit with adjusted R2 from 0.22 to 0.35.
Conclusion:
Higher number of pain sites throughout the body was a consistent predictor of poor outcome and less change at 1 year. Baseline levels for AKPS and worst pain predicted respective final scores and change scores.
Registration:
NCT02114294 (ClinicalTrials.gov identifier).
Patellofemoral pain (PFP) is defined as pain around or behind the patella that is provoked by activities loading the patellofemoral joint in the absence of other distinct pathology. 14 PFP is common, with annual prevalence estimates of 23% in the general population and 29% in adolescents. 40 Women are affected approximately twice as commonly as men. 40 Newer surveys suggest higher degrees of chronicity than previously thought, with the majority of patients still reporting pain at 2- to 8-year follow-up.30,39,40
Previous studies have identified some factors predictive of poor outcome in patients with PFP. A recent systematic review found that longer pain duration (>4 months) was the most reported prognostic factor of a poor outcome. 34 In addition, more intense self-reported symptoms at baseline, as evidenced by low Anterior Knee Pain Scale (AKPS) score, was a consistent predictor of poor outcome in a recent long-term analysis. 30 Other factors have been shown to predict poorer outcome, but these predictors are not consistent among studies.34,38,39 Generally, strength of the evidence is reduced by methodological limitations in original studies (most commonly related to small samples). 34
Psychological factors have been found to predict poorer outcomes in other musculoskeletal conditions.1,2,18,20,22,32,48,49 Existing studies suggest that psychological factors such as anxiety, depression, catastrophizing, and kinesiophobia may be important in PFP. 33 Two studies reported correlations between concurrent improvements in catastrophizing and kinesiophobia and improvements in pain and function,16,37 but to our knowledge, the prognostic value of baseline psychological measures on outcomes of pain and function has not previously been examined in PFP.
The aim of the present study was to evaluate predictors of outcomes for function (AKPS), pain, and measures of change after 1 year for patients with PFP who participated in a randomized controlled trial (RCT) comparing 3 exercise-based interventions.
Methods
Study Design
A post hoc analysis was performed with data from a previously reported 1-year follow-up of a single-blind, single-center randomized controlled trial. The trial has been reported, including the protocol.24,25 Patients (N = 112) were randomly assigned to a 6-week intervention consisting of patient education combined with isolated hip exercise (n = 39), traditional knee-based exercise (n = 37), or free training (n = 36); 98 patients completed 1-year follow-up. The trial was registered with the ClinicalTrials.gov database (NCT02114294). The Ethics Committee Health Region South-East, Norway, granted ethical approval (2013/1860/REKsør-øst). Patients provided informed consent.
Participants
Patients were recruited from referrals by primary care physicians or other medical specialists (eg, orthopaedic surgeons, rheumatologists) to the Department of Physical Medicine and Rehabilitation, Sørlandet Hospital, between September 2014 and September 2017.
Patients were eligible for inclusion if they were 16 to 40 years of age with a minimum 3-month history of PFP (pain ≥3 of 10) reproduced by at least 2 activities (stair ascent or descent, hopping, running, prolonged sitting, squatting, or kneeling) and present on at least 1 clinical test (compression of the patella, palpation of the patellar facets). In patients with bilateral pain, the worst knee was included.
Exclusion criteria were as follows: (1) clinical, radiographic, or magnetic resonance imaging findings indicative of other significant specific pathology, including meniscal, ligament, or cartilage injury, as well as osteoarthritis, apophysitis, significant knee joint effusion, or recurrent patellar subluxation or dislocation; (2) significant pain from hip or back hindering the ability to perform the prescribed exercises; (3) previous surgery to the knee joint; (4) nonsteroidal anti-inflammatory drug or cortisone use over an extended period; (5) previous trauma to the knee joint with an effect on the presenting clinical condition; (6) physiotherapy or other similar exercises for PFP syndrome within the previous 3 months.
Interventions
All patients received the same patient education and were randomized to isolated hip exercise, traditional knee-based exercise, or free training for 6 weeks. 24 The patients in the hip and knee groups performed exercises 3 times weekly (1 session under guidance from the physiotherapist and 2 home sessions).
Outcome and Predictor Variables
Data measured at baseline and 1 year were used for this post hoc analysis. Participants filled out the self-report questionnaires without assistance. Observers blinded to group assignment collected all outcomes.
Demographic measures were collected for all patients, including age, sex, body mass index, education, work/sick leave, pain duration, and presence of unilateral or bilateral pain.
The main outcome of the study was the AKPS. This is a self-report questionnaire consisting of 13 questions pertaining to symptoms of anterior knee pain. 28 The total score ranges from 0 to 100 (no symptoms).
Secondary outcomes were pain intensity and global change. Pain intensity was measured by a visual analog scale (range, 0-10 [most pain]). Usual pain and worst pain during the past week were measured. A global change score consisting of an 18-point Likert scale from −9 (maximum deterioration) to +9 (maximum improvement) was used to determine patients’ global assessment of change from baseline. 5
Psychological predictors included kinesiophobia, self-efficacy, and anxiety and depression. The Tampa Scale for Kinesiophobia (TSK) is a 13-item, self-report questionnaire used to assess fear of movement/reinjury (range, 13-52 [most]). 23 The Knee Self-Efficacy Scale (K-SES) was used to assess self-efficacy (range, 0-10 [highest]). 44 Questions pertain to how certain respondents feel about performing various activities now and in the future. The 10-question Hopkins Symptom Checklist (HSCL-10) assesses symptoms of anxiety and depression (range, 1-4 [most symptoms]).15,42
Number of pain sites during the past week was assessed with an adaptation of the Standardized Nordic Questionnaire. Patients record presence of pain (yes/no) in 9 body areas (head, neck, shoulder, elbow, hand, upper back, hip, knee, and ankle).27,29 Only 1 point is scored per bodily area; thus, the score does not differentiate between bilateral and unilateral pain.
Statistical Analysis
All statistical analyses were performed with SPSS (v 23; IBM Corporation). All data were checked for normality and outliers via stem-and-leaf plot and Q-Q plot. Scatter plots were used to inspect correlation data for outliers.
Missing Values
Missing values for AKPS, HSCL-10, K-SES, and TSK were handled as follows: If <25% of items were missing, the values were substituted with the arithmetic mean of values from the available items. 8 If ≥25% of items were missing, the outcome was regarded as missing for the patient. If an item was missing for the Nordic Questionnaire, the total score was regarded as missing.
Predictive Models
Outcomes were AKPS, worst pain, and global change score at 1 year. At 1 year, there were no significant between-group differences in either primary or secondary outcomes measures in the RCT (data not shown). Thus, for the current study, the data were analyzed as a single cohort. 35 Selection of potential predictors was based on findings in previous studies and clinical judgment. 43 We limited the number of variables in the model to 9 based on our sample size of 98. 21 On the basis of this, we chose the following 9 baseline measures as potential predictors of outcome, which were entered in each model: sex, bilateral pain, worst pain, pain duration (categories: 3-6, >6-12, >12-24, >24 months), AKPS, TSK, HSCL-10, K-SES, and number of pain sites. Treatment group was not included as a variable, as there were no between-group differences in the outcomes in question. 35 Multivariable models were also tested without the baseline variable for AKPS and worst pain for their 1-year outcomes.
Multivariable linear regression models were then constructed with the outcome in question as the dependent variable and potential predictors as independent variables. 41 A backward stepwise elimination (P≤ .10) was used to identify a group of factors that were associated with outcome at 1 year. The final model is presented with the constant (Y-intercept), the unstandardized regression coefficients (B), and their 95% CIs. P < .05 was used to define statistical significance in the final model. The amount of variance accounted for by the final model is expressed as adjusted R2. Models were checked for collinearity through the variance inflation factor.
Results
Of the 317 patients evaluated for inclusion, 47 did not meet inclusion criteria; 87 met exclusion criteria; and 71 declined to participate. Ultimately, 112 patients were randomized to 1 of 3 arms of the intervention, and 98 (88%) completed 1-year follow-up and were included in the present analysis (see flowchart; Figure 1). All groups showed statistically significant improvement from baseline to 1 year for pain and function. The intention-to-treat analysis in the main study did not find any between-group differences for any outcomes at 1 year. Thus, for the current post hoc analysis, we treated the whole group of patients as 1 cohort. Baseline values for the cohort are presented in Table 1. There were few missing data, except for the Nordic pain questionnaire (number of pain sites), in which 6 (5%) total scores were incomplete and treated as missing.
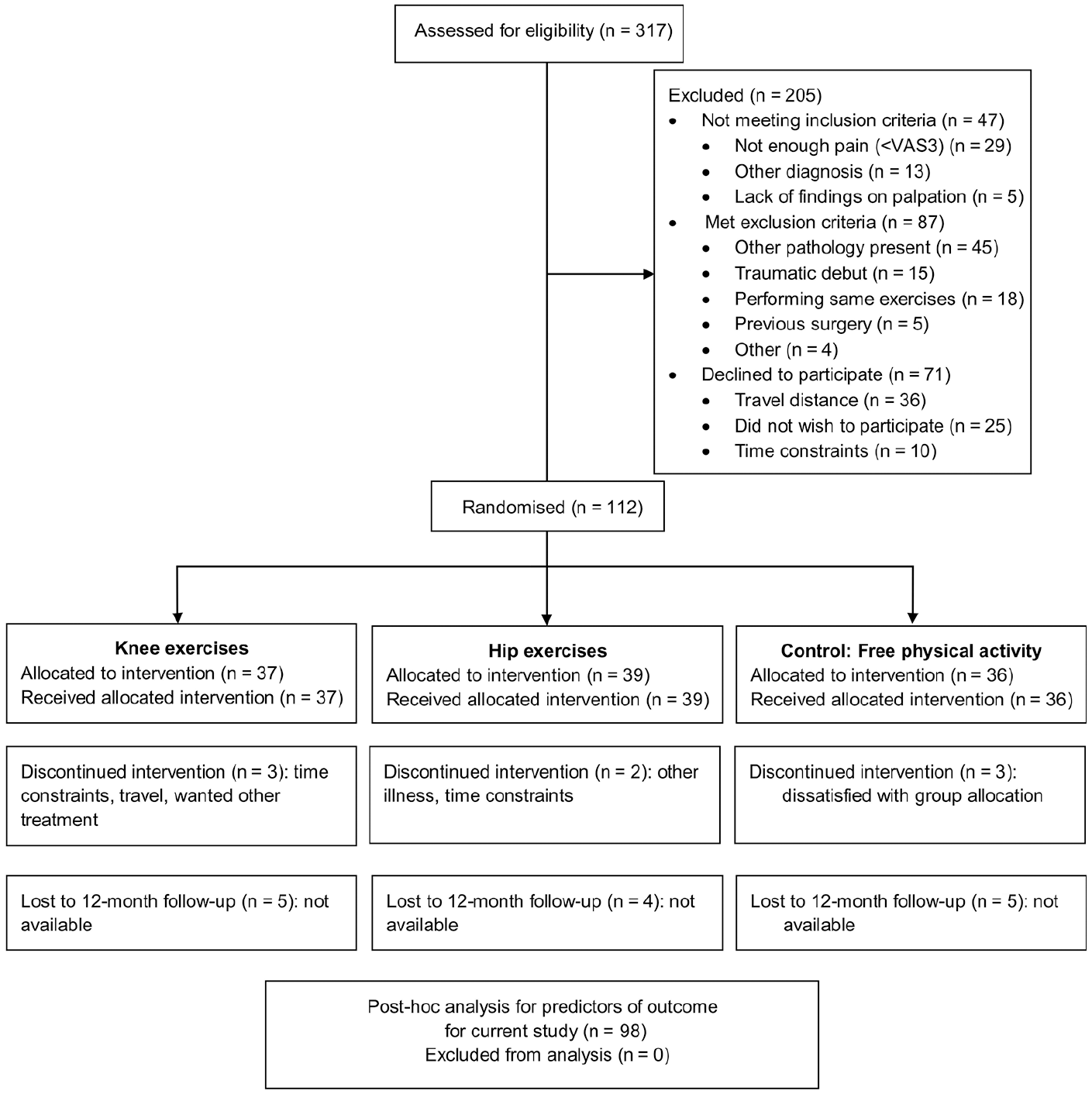
CONSORT (Consolidated Standards of Reporting Trials) flowchart. VAS, visual analog scale.
Baseline Characteristics a (N = 112)
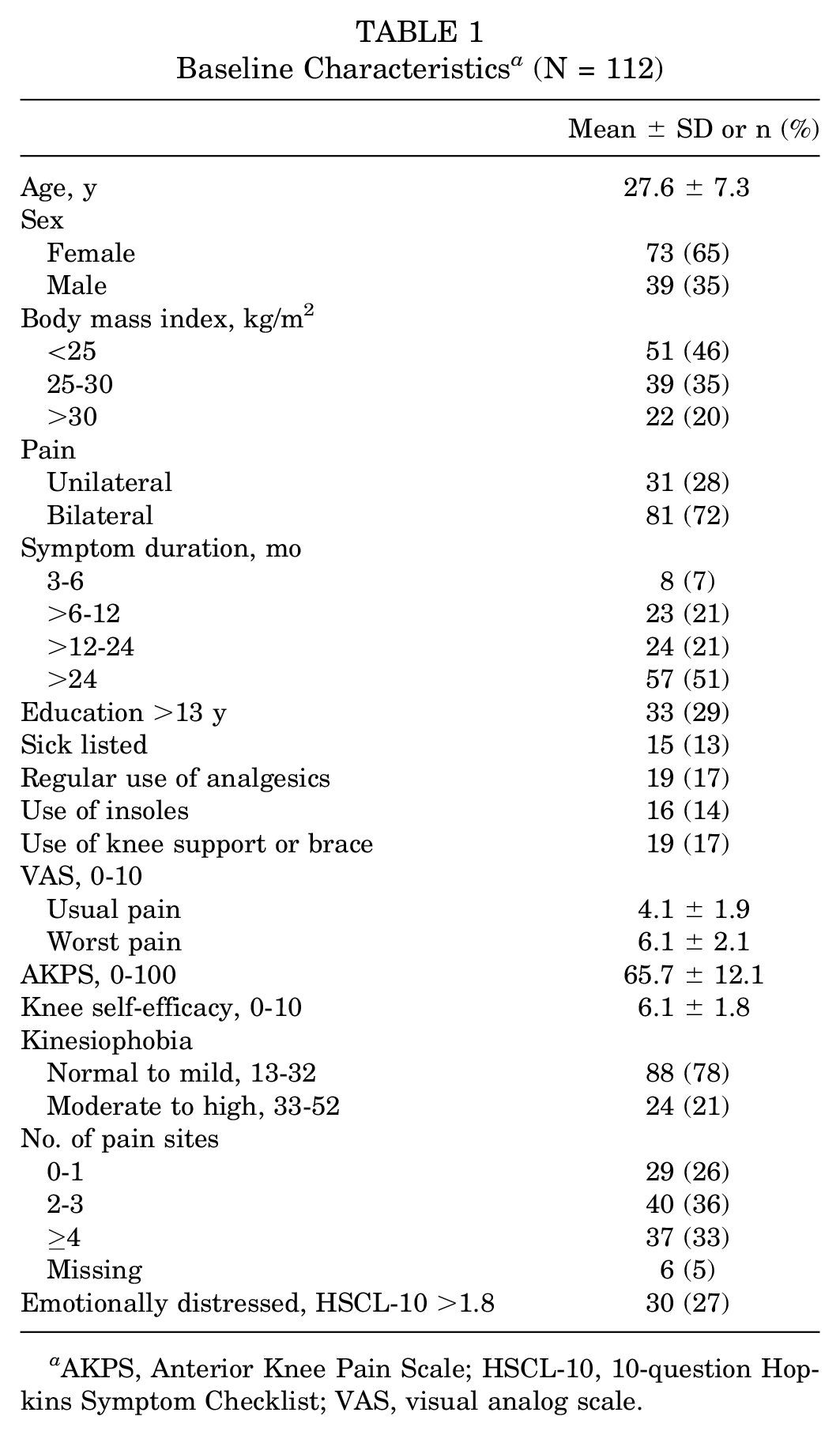
AKPS, Anterior Knee Pain Scale; HSCL-10, 10-question Hopkins Symptom Checklist; VAS, visual analog scale.
Anterior Knee Pain Scale
Lower AKPS baseline and higher number of pain sites were significant predictors of lower AKPS at 1 year, accounting for 35% of the variance (Table 2).
Multivariable Linear Regression for the Dependent Variable AKPS at 1 Year a
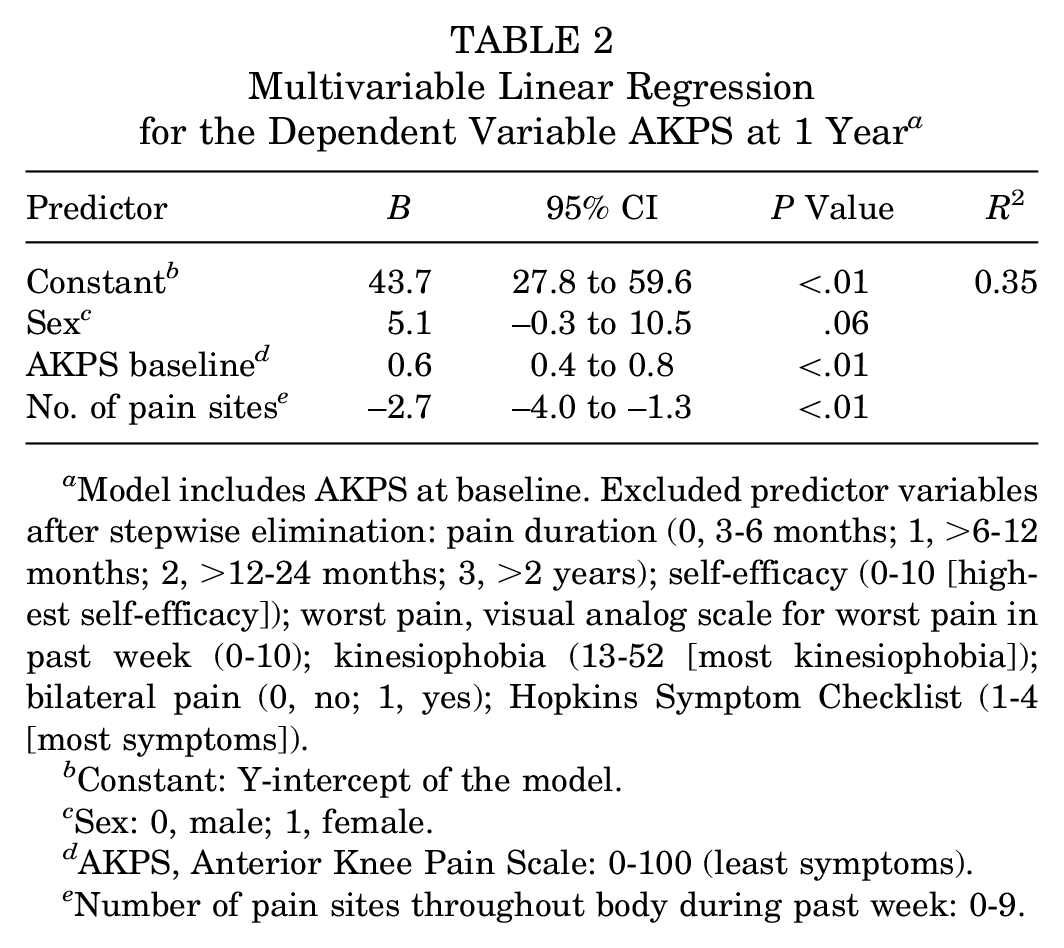
Model includes AKPS at baseline. Excluded predictor variables after stepwise elimination: pain duration (0, 3-6 months; 1, >6-12 months; 2, >12-24 months; 3, >2 years); self-efficacy (0-10 [highest self-efficacy]); worst pain, visual analog scale for worst pain in past week (0-10); kinesiophobia (13-52 [most kinesiophobia]); bilateral pain (0, no; 1, yes); Hopkins Symptom Checklist (1-4 [most symptoms]).
Constant: Y-intercept of the model.
Sex: 0, male; 1, female.
AKPS, Anterior Knee Pain Scale: 0-100 (least symptoms).
Number of pain sites throughout body during past week: 0-9.
Worst Pain
Higher baseline pain levels, longer pain duration, and higher number of pain sites predicted higher levels of pain at 1 year, accounting for 26% of the variance (Table 3).
Multivariable Linear Regression for the Dependent Variable Worst Pain at 1 Year a
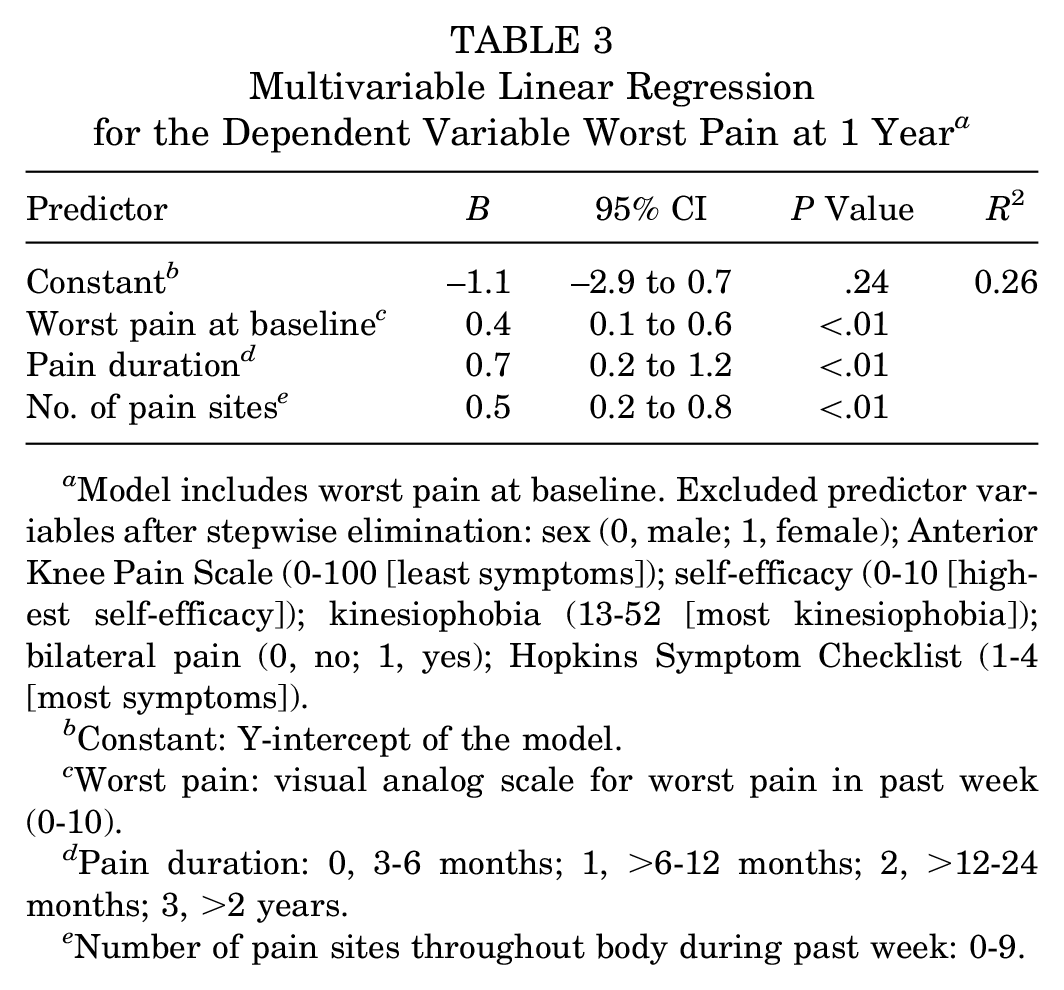
Model includes worst pain at baseline. Excluded predictor variables after stepwise elimination: sex (0, male; 1, female); Anterior Knee Pain Scale (0-100 [least symptoms]); self-efficacy (0-10 [highest self-efficacy]); kinesiophobia (13-52 [most kinesiophobia]); bilateral pain (0, no; 1, yes); Hopkins Symptom Checklist (1-4 [most symptoms]).
Constant: Y-intercept of the model.
Worst pain: visual analog scale for worst pain in past week (0-10).
Pain duration: 0, 3-6 months; 1, >6-12 months; 2, >12-24 months; 3, >2 years.
Number of pain sites throughout body during past week: 0-9.
Change Scores
For the outcome global change, the variables female sex, lower AKPS at baseline, higher self-efficacy, and lower number of pain sites were significant predictors of higher change scores at 1 year. The model accounted for 28% of the variance. Table 4 shows results for multivariable linear regressions for global change scores at 1 year.
Multivariable Linear Regressions for Global Change Scores at 1 Year a
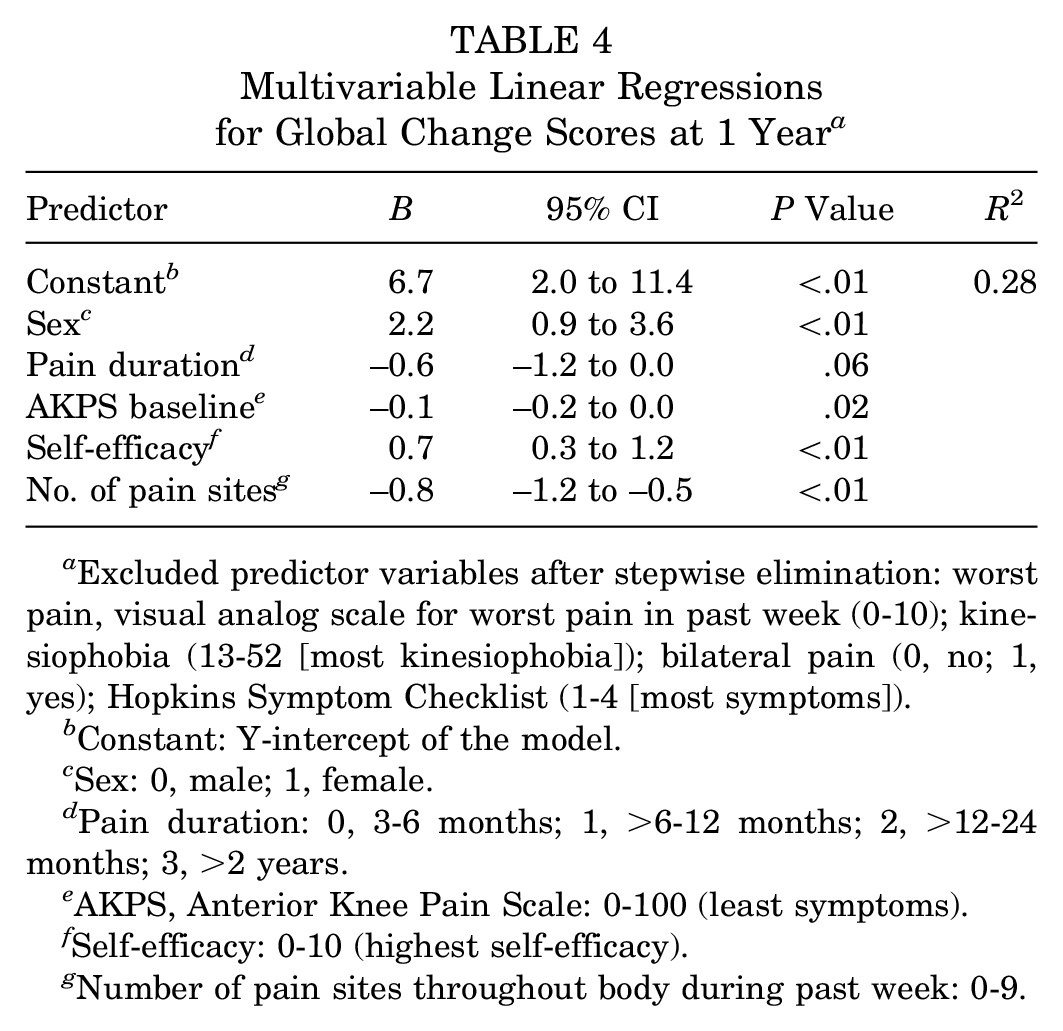
Excluded predictor variables after stepwise elimination: worst pain, visual analog scale for worst pain in past week (0-10); kinesiophobia (13-52 [most kinesiophobia]); bilateral pain (0, no; 1, yes); Hopkins Symptom Checklist (1-4 [most symptoms]).
Constant: Y-intercept of the model.
Sex: 0, male; 1, female.
Pain duration: 0, 3-6 months; 1, >6-12 months; 2, >12-24 months; 3, >2 years.
AKPS, Anterior Knee Pain Scale: 0-100 (least symptoms).
Self-efficacy: 0-10 (highest self-efficacy).
Number of pain sites throughout body during past week: 0-9.
For the outcome change in AKPS at 1 year, the variables lower AKPS at baseline and lower number of pain sites were significant predictors of higher change scores in AKPS at 1 year. This model accounted for 22% of the variance (Table 5).
Multivariable Linear Regressions for Change in AKPS at 1 Year a
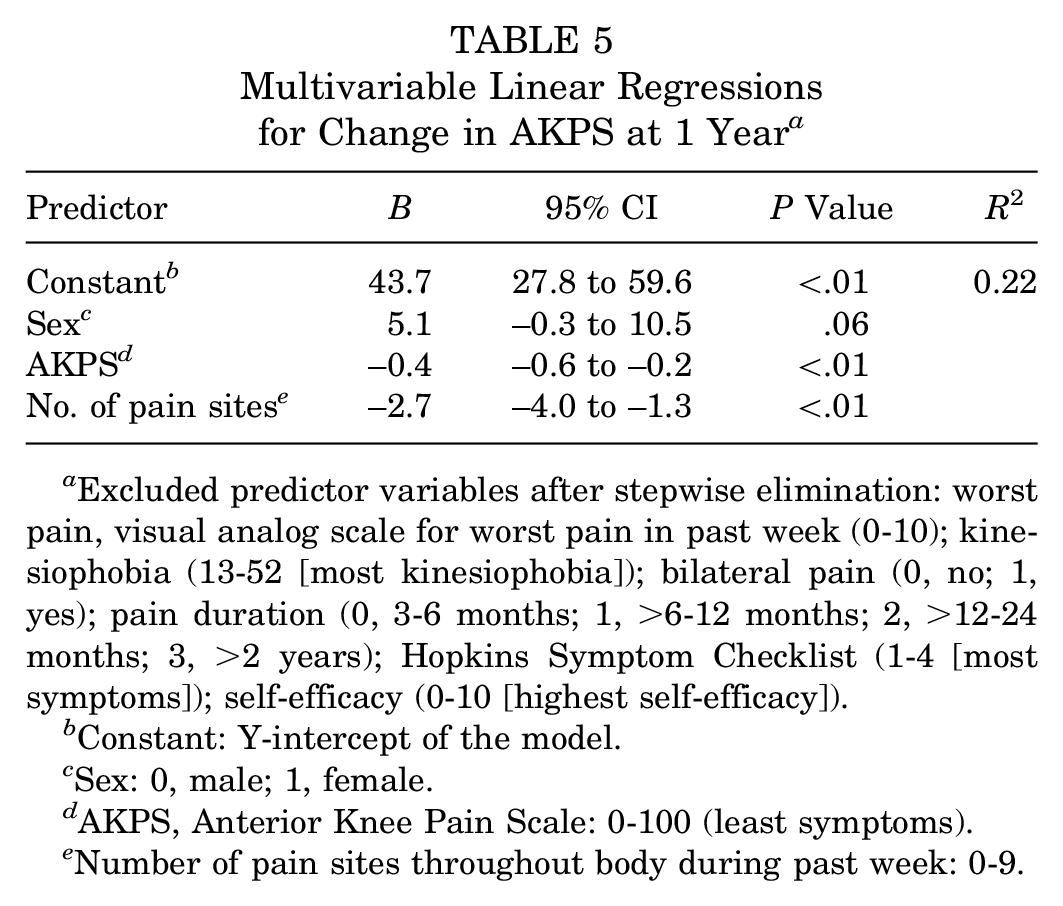
Excluded predictor variables after stepwise elimination: worst pain, visual analog scale for worst pain in past week (0-10); kinesiophobia (13-52 [most kinesiophobia]); bilateral pain (0, no; 1, yes); pain duration (0, 3-6 months; 1, >6-12 months; 2, >12-24 months; 3, >2 years); Hopkins Symptom Checklist (1-4 [most symptoms]); self-efficacy (0-10 [highest self-efficacy]).
Constant: Y-intercept of the model.
Sex: 0, male; 1, female.
AKPS, Anterior Knee Pain Scale: 0-100 (least symptoms).
Number of pain sites throughout body during past week: 0-9.
For the outcome change in worst pain at 1 year, the variables higher baseline pain levels, shorter pain duration, and lower number of pain sites predicted largest reduction in worst pain at 1 year. This model accounted for 30% of the variance (Table 6).
Multivariable Linear Regressions for Change in Worst Pain at 1 Year a
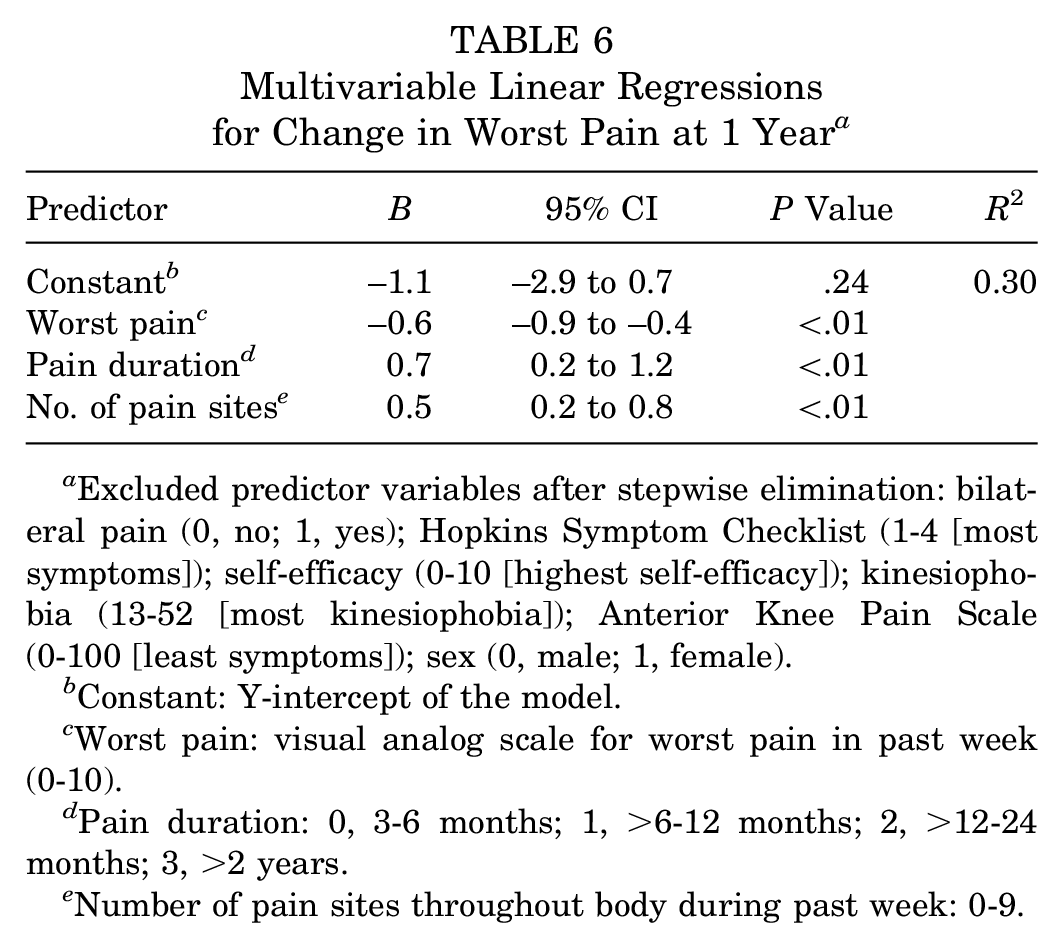
Excluded predictor variables after stepwise elimination: bilateral pain (0, no; 1, yes); Hopkins Symptom Checklist (1-4 [most symptoms]); self-efficacy (0-10 [highest self-efficacy]); kinesiophobia (13-52 [most kinesiophobia]); Anterior Knee Pain Scale (0-100 [least symptoms]); sex (0, male; 1, female).
Constant: Y-intercept of the model.
Worst pain: visual analog scale for worst pain in past week (0-10).
Pain duration: 0, 3-6 months; 1, >6-12 months; 2, >12-24 months; 3, >2 years.
Number of pain sites throughout body during past week: 0-9.
Alternative Models
We also tested predictive models for AKPS and worst pain at 1 year that excluded their baseline values. For the AKPS model with the baseline AKPS value removed, the variables longer pain duration, lower self-efficacy, and higher number of pain sites were significant predictors for lower AKPS at 1 year, accounting for 31% of the variance. For the worst pain model excluding baseline levels of worst pain, we found that longer pain duration, lower baseline AKPS, and higher number of pain sites predicted higher pain levels at 1 year, accounting for 24% of the variance.
Predictive models in which number of pain sites was excluded as a variable found HSCL-10 replacing it, although as a weaker predictor than number of pain sites, with a lower R2 for all models (for HSCL-10 in all models,P≥ .04 and R2 = 0.11-0.26).
Discussion
The most consistent predictor of outcome at 1 year in patients with PFP was number of pain sites at baseline. Higher number of pain sites was a significant predictor of poorer outcomes in all multivariable models. For the outcomes AKPS and worst pain, their baseline values were significant predictors of outcome at 1 year. Low self-efficacy, longer pain duration, and male sex were also significant predictors of poorer outcomes at 1 year, although these results were found in only 1 analysis.
Comparison With Previous Studies
Number of Pain Sites
Previous studies identified widespread pain as a predictor of poor prognosis in other musculoskeletal conditions1,20 and in knee pain in general practice. 46 Large epidemiologic surveys have found number of pain sites to be associated with lower function, 27 number of nonmuskuloskeletal symptoms, 45 and a predictor of long-term work disability. 26 Fibromyalgia survey criteria, in which number of pain sites is a central factor, have been identified as a strong predictor of poor outcome after total hip or knee joint replacement 7 and for postsurgical opiate use after total hip or knee joint replacement, 6 regardless of whether the patient fulfilled diagnostic criteria for fibromyalgia. Our finding that higher number of pain sites predicted poorer outcome for pain and function and poorer response to treatment (lower change scores) is consistent with these previous studies.
Pain Duration
Lankhorst et al, 30 Collins et al,11,12 and Rathleff et al 39 found longer pain duration to be predictive of poorer outcome in the long and short term in patients with PFP. The recent systematic review by Matthews et al 34 found longer duration of PFP symptoms (>4 months) to be the most reported prognostic factor of a poor outcome. Our results partially support this finding, with pain duration being a significant predictor for worst pain and change in worst pain. It is important to point out that none of the patients in our cohort reported pain duration <4 months, which might affect the predictive value of pain duration.
Psychological Factors
We found self-efficacy to be one of several predictors of global change and of AKPS when baseline AKPS levels were excluded from the model. Self-efficacy has not previously been examined as a predictor of PFP outcomes. A recent systematic review found that catastrophic thinking and poor coping strategies predicted higher pain levels after total knee replacement but kinesiophobia did not. 2 This is in keeping with our results, in which self-efficacy, but not kinesiophobia, was a predictor for global change score.
Domenech et al 16 and Piva et al 37 found that changes in kinesiophobia were strongly associated with changes in pain and function after treatment for PFP, but neither reported on the predictive value of baseline levels of kinesiophobia on final outcomes or change, as examined in this study. In the current study, baseline kinesiophobia was not predictive of any of the outcomes examined. We did not examine associations between concurrent changes in the various measures.
In the current study, alternative multivariable models were also constructed in which number of pain sites was excluded as an independent variable. Within these models, we found that HSCL-10 replaced number of pain sites in the final models, although as a weaker predictor than number of pain sites and with a lower R2 for all models. Although this finding has not previously been reported in PFP, it is consistent with previous findings indicating that anxiety and depression are predictors of poorer outcomes in back pain and in general musculoskeletal pain1,22 and are associated with widespread pain.9,13
Sex
Sex is a variable that has been examined in previous PFP studies. Given the sex differences in PFP prevalence, with women being more commonly affected than men, it has been hypothesized that female sex might predict worse outcome. Previous studies have not reported sex as predictive for outcome, 34 although Lankhorst et al 31 found a positive trend for females responding better to exercise therapy. Our analysis found female sex to be a significant predictor of higher global change score.
Directionality of Baseline Values on Final Outcome vs Change
Our findings that baseline measures of pain and function (AKPS) predict final outcomes are in agreement with previous studies.12,30 It should be noted that the directionality of predictive value of baseline levels for final outcome was opposite to that of predictive value for change. That is, having more symptoms at baseline predicted more symptoms at follow-up but also higher change scores (more improvement) for the outcomes.
The differences in directionality of predictors on either final outcomes or change in scores are intuitive from a statistical standpoint but still important to point out. It means that the predictive value of baseline levels of scores depends on whether we wish to predict final outcome or change scores.
In contrast, higher number of pain sites, longer pain duration, and lower self-efficacy were predictors for worse final outcome and less change.
Strengths and Weaknesses of the Study
Although this study is larger than most comparable predictor studies within PFP, 34 the limited sample size may affect the robustness of our results. The data extraction for this predictive analysis is based on an RCT in which the original study was not designed for prognostic analyses, which is a weakness when compared with prespecified analyses in a larger study designed for the purpose of prognosis. Data were analyzed as a single cohort, as there were no between-group differences in the 1-year outcomes of the RCT. 35 This is advantageous in increasing the sample size but allows for no analysis regarding which factors predict response to a specific treatment. Our cohort did not include any patients with pain duration <4 months, which may limit generalizability of the results to populations with shorter duration at baseline. Furthermore, the relatively strict inclusion criteria used in the main RCT may limit the generalizability of the results. The inherent clinimetric limitations of self-report measures should also be pointed out. Transformations of pain, feelings, or thoughts to numbers are unlikely to be linear as the scales imply, and results based on such analyses should be interpreted with caution. 4
Implications for Future Research and Clinical Practice
The most consistent predictor of pain, function, and change in PFP at 1 year was number of pain sites. This is consistent with previous studies within other musculoskeletal pain conditions1,6,7,22,46 but has not been examined in PFP previously. The meaning of multiple pain sites is unclear. Widespread pain is closely associated with various psychological factors9,13 and has been suggested as an indicator of central sensitization.6,7,19,36 Psychological factors, widespread pain, and sensitization are predictive of outcomes in other musculoskeletal pain conditions.1,2,6,7,20,22,26,46 Our findings suggest that they may be important to consider within PFP, as with other chronic musculoskeletal pain conditions. The recognition of multiple pain sites and self-efficacy as prognostic factors in a clinical setting suggests that we should broaden our perspective. The current recommendations3,10 are mainly based on biomechanical considerations. As such, we recommend the use of a biopsychosocial model in approaching PFP clinically and in future research.17,33,47
Our findings that baseline levels of worst pain, function (AKPS), and pain duration predict outcomes are consistent with previous studies. 34 The recognition of these risk factors for poorer outcome may be useful in a clinical setting—for example, in informing patients regarding realistic outcome expectations. The finding of sex as a predictor of outcome is not consistent with previous studies and should be examined further.
Conclusion
Number of pain sites was the most consistent predictor of pain, function, and change scores 1 year after an education- and exercise-based intervention for PFP. This finding has not previously been reported in PFP but is consistent with previous research for other musculoskeletal conditions. Baseline levels for AKPS and worst pain predicted respective final scores and change scores.
Footnotes
Acknowledgements
The authors thank the physiotherapists at the Department of Physical Medicine and Rehabilitation, Sørlandet Hospital Kristiansand, for performing the interventions and outcome measures in this trial.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Research Department of Sørlandet Hospital. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Submitted May 16, 2019; accepted September 30, 2019.