
Abstract
Background:
Recently, a cell identity assay has been introduced to evaluate the identity of cultured chondrocytes before autologous chondrocyte implantation (ACI), which was shown to be associated with graft survival after ACI.
Purpose:
To identify the influence of several patient- and lesion-specific factors on cell identity and viability assays.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 187 patients with second-generation ACI were included in this study. Patient and lesion characteristics, cell viability, cell identity, and biopsy specimen weight were recorded for each patient. A binomial logistic regression model was utilized to determine patient-specific predictive factors for cell product quality.
Results:
The implanted ACI cell products showed a cell viability of 93% ± 2.4% (mean ± SD; range, 84-98) with an identity score of 5.8 ± 2.1 (range, –0.08 to 9.46). Patients with multiple previous surgical procedures on the index knee had significantly lower cell identity scores when compared with patients without previous surgery (odds ratio = 0.31; 95% CI, 0.16-0.59; P < .001). Patients without surgical history had significantly higher cell identity scores than patients with 1 and ≥2 previous surgical procedures on the index knee (6.32 vs 5.32 vs 5.05; P = .006 and P < .001, respectively). Cell viability was not predicted by any preoperative variable (P > .05). Cell identity and viability were not associated with each other or with biopsy specimen weight (P > .05).
Conclusion:
Cartilage biopsy specimens from patients with ≥1 previous surgical procedures resulted in implants with lower cell identity scores when compared with patients without previous operations. None of the other patient- or lesion-specific factors were correlated, specifically biopsy specimen weight.
Keywords
First described by Brittberg et al, 6 autologous chondrocyte implantation (ACI) has become a well-established surgical treatment option for symptomatic focal chondral defects, with a large body of literature reporting on its efficacy, safety, and long-term survival. # Over the years, ACI techniques have evolved, but its principle as a 2-stage procedure has remained the same. 29 During the first stage, 100 to 300 mg of full-thickness articular cartilage is arthroscopically harvested from low-weightbearing areas of the femoral condyle, trochlea, or intercondylar notch. The biopsy tissue is processed and cultured in vitro for at least 2 weeks. The second stage requires careful debridement of the chondral defect, creating vertical walls without damaging the subchondral plate, and subsequent implantation of the cultured chondrocytes.
In addition to meticulous surgical technique, high cell quality is deemed important for a successful outcome after ACI. A recent study correlated a quality assay of the cultured chondrocytes with clinical outcome and quality of repair tissue in patients with symptomatic cartilage defects.1,17,23 Separately, assessing preoperative cell product quality, Pestka et al 20 showed that patients <20 years old have significantly higher expression rates of cartilage-specific markers when compared with older patients. In a study by Hindle et al, 10 intraoperative trauma to the ACI product, such as grasping, dropping, crushing, and cutting the ACI sample to size, was associated with chondrocyte death and consequently inferior cell viability and quality. In 2010, in addition to the expression rate of chondrocyte-specific protein markers and cell viability, cell identity was established as an indicator of cell product quality. 24 After evaluating the protein expression of histological samples of ACI biopsy specimens, Rapko et al 24 found that synovial tissue from the synovial membrane, 2 tissue fragments, 8 and individual synovial cells within the synovial fluid 27 were common contaminants of these biopsy specimens, leading to inferior purity of the final cell product.
Based on the synovial marker microfibril-associated glycoprotein 2 (MAGP2; official symbol, MFAP5) and cartilage marker cartilage link protein (CRTL1; official symbol, HAPLN1), the cell identity assay distinguishes between chondrocyte and synovial gene expression, essentially establishing a parameter of the purity of the culture. 24 Consequently, the cell therapy manufacturer Vericel Corporation assesses all cartilage biopsy samples with the cell identity assay before release. In a recently published study by Ackermann et al 1 investigating the relationship of cell identity and patient outcome, the authors reported that a superior cell identity—thus, an increased chondrocyte: synoviocyte gene expression ratio—was associated with improved repair tissue quality and 5-year graft survival in patients who underwent ACI for the treatment of chondral defects in the knee. Despite ACI product quality being variable among individuals, high ACI product quality is desired, and thus preoperative factors influencing cell viability and cell identity are of deep interest to enhance outcome after ACI.
We therefore sought to assess the potential influence of preoperative patient-, lesion-, and biopsy specimen–associated parameters on cell identity (chondrocyte:synoviocyte gene expression ratio) and viability determining final ACI product quality. It was hypothesized that previous surgical procedures on the index knee are associated with inferior cell identity assay scores, as the procedures can introduce a significant amount of free tissue fragments into the knee joint and consequently increase contamination with synoviocytes.
Methods
Patients treated with second-generation ACI for focal chondral defects in the knee by a single surgeon between October 2010 and June 2017 were enrolled for this study. Surgical treatment was indicated in patients after failed nonoperative treatment, including physical therapy and injection. Contraindications for the treatment with ACI were inflammatory joint disease, osteoarthritis, metabolic or crystal disorders, or obesity.
The following were recorded for each patient: sex, age at the time of surgery, body mass index, smoking status, workers’ compensation status, defect location, defect number, lesion size, concomitant procedures, whether the patient had multiple previous surgical procedures on the index knee (before cartilage biopsy), whether the patient experienced symptoms for >12 months, ACI biopsy specimen weight, cell identity assay score, and viability. Most biopsy specimens were harvested from the intercondylar notch (>95%). Even in prior ACL reconstruction, the biopsy specimen was usually harvested from the notch, but the medial instead of lateral notch in case of prior notchplasty.
Viability Assay
The percentage viability of autologous cells was indirectly determined by cell membrane integrity by adding trypan blue dye to a cell suspension. Equal volumes of cell suspension and trypan blue dye are incubated for approximately 3 minutes at room temperature. After that, the hemacytometer is loaded to determine the total number of cells and the number of nonviable cells. Nonviable cells will take up the trypan blue dye owing to the lack of cell membrane integrity and therefore appear blue under the microscope. Viable cells, however, will not take up the trypan blue dye, as their membrane is still intact. The number of viable cells (total cells minus nonviable cells) divided by the total number of cells multiplied by 100 gives the percentage viability for each chamber of the hemacytometer. The results from both chambers of the hemacytometer are averaged together to determine the final viability result.
Cell Identity Assay
The ACI lot release cell identity assay for cultured human chondrocytes is based on the work of Rapko and colleagues. 24 The assay is based on the discrimination of cultured human chondrocytes and human synovial synoviocytes, as the latter cell type frequently contaminates articular cartilage biopsy specimens during the first stage of an ACI procedure. A quantitative polymerase chain reaction (PCR) assay was established that measures HAPLN1 and MFAP5 mRNA expression in an ACI sample, as HAPLN1 was found to be a reliable protein marker for chondrocytes while MFAP5 was linked to synovial fibroblastic activity.
The first step for this assay requires the isolation of RNA by lysing and homogenizing the sample in a denaturing buffer that inactivates RNases isolates the RNA from the ACI product sample. The sample is then washed 3 times with ethanol to help the RNA bind to the silica-based membrane of the spin column and remove contaminants from the membrane. With a Nanodrop spectrophotometer, the RNA is eluted with RNase-free water and quantified. After use of a cDNA reverse transcription kit to synthesize cDNA from the single-stranded RNA, real-time PCR is performed for the relevant markers MFAP5 and HAPLN1. A 13-µL sample volume is needed for the PCR that is performed with 36 cycles of amplification on an ABI 7500 system in “fast” mode. To initially denature the sample, the PCR cycle is run at 95°C for 20 seconds, followed by 36 cycles of 95°C for 3 seconds and 60°C for 30 seconds.
Conclusively, the d5L number (cell identity assay score) is the difference in threshold cycles between MFAP5 and HAPLN1 when cycle time quantitation is compared. A cell identity assay score ≥–2.10 indicates a chondrocyte culture and qualifies to be shipped and ultimately implanted in the patient’s knee.
Statistical Analysis
Patients’ sociodemographic, lesion, and biopsy sample characteristics were determined with descriptive statistics. Based on the cohort’s mean cell identity/viability score, outcome was defined as whether a patient had an identity/viability score above or below the cohort’s mean. Thus, outcome was defined categorically with 0 representing below-average identity/viability scores and 1 representing above average. Binomial logistic regression models were utilized to determine the predictive value of preoperative variables for patients’ cell identity assay scores and cell viability. Variable selection was based on bivariate regression analysis. Associations displaying significance at a level of P < .15 were included in the logistic regression models. Categorical variables were coded as dummy variables for bivariate and logistic regression models (eg, for sex, 0 = male and 1 = female). In a cell identity subanalysis, patients without surgical history were compared with patients with 1 and ≥2 previous surgical procedures on the index knee, by utilizing the Kruskal-Wallis test and post hoc analysis. All statistical analyses were performed in SPSS for Mac (v 23.0; IBM). Final significance was set at P < .05.
Results
A total of 187 consecutive patients were treated with ACI for focal symptomatic cartilage lesions within the knee joint during the study period and were ultimately enrolled in this study. The implanted final ACI products showed a cell viability of 93% ± 2.4% (mean ± SD) with a cell identity score of 5.8 ± 2.1; thus, cell viability and identity scores were below average in 106 (56.7%) and 86 (46%) patients, respectively. Patient-, lesion-, and biopsy specimen–associated parameters are presented in Table 1.
Patient Demographics, Lesion Type, and Biopsy Specimen Characteristics for Patients With Below- and Above-Average Cell Viability and Cell Identity Scores a
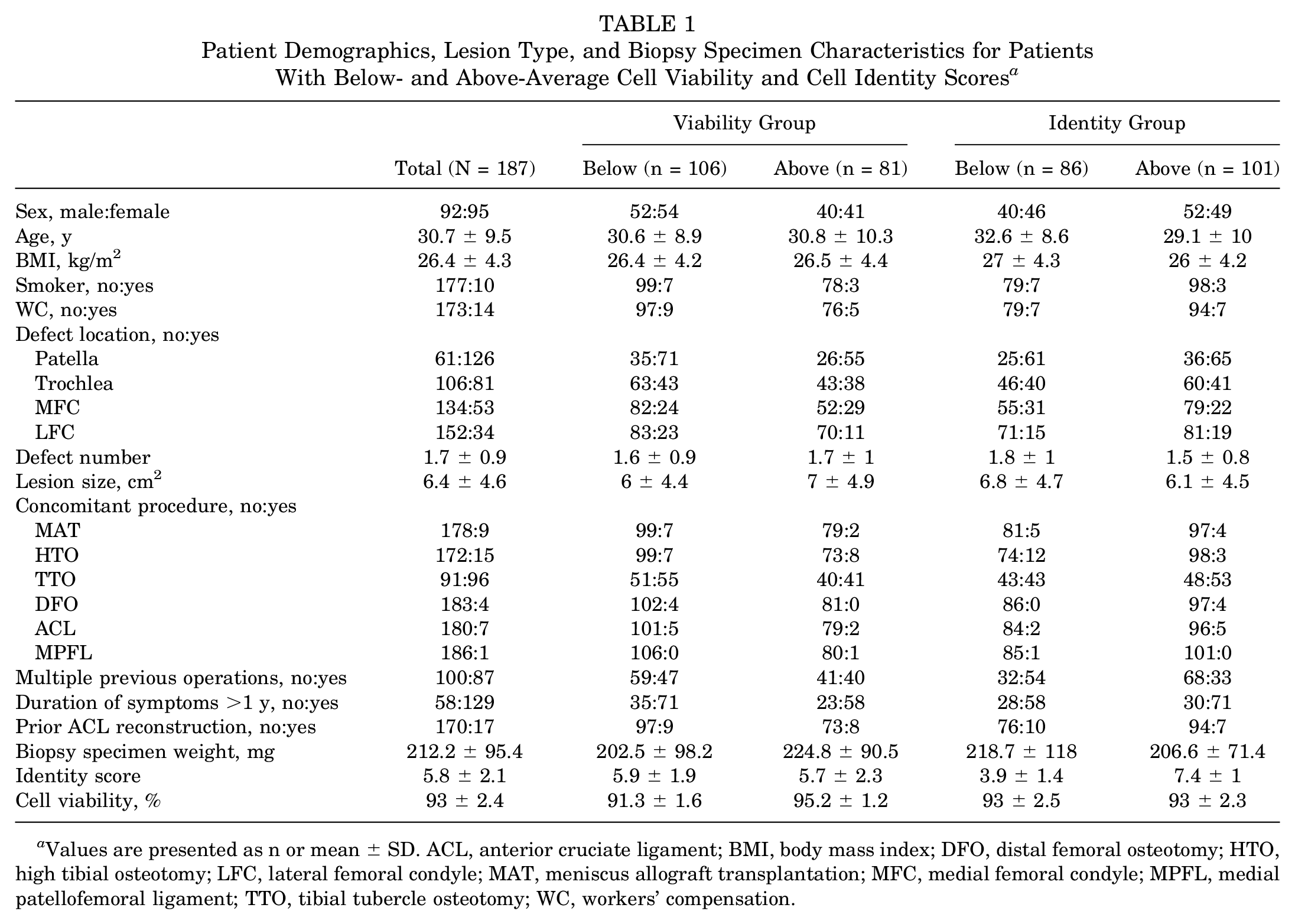
Values are presented as n or mean ± SD. ACL, anterior cruciate ligament; BMI, body mass index; DFO, distal femoral osteotomy; HTO, high tibial osteotomy; LFC, lateral femoral condyle; MAT, meniscus allograft transplantation; MFC, medial femoral condyle; MPFL, medial patellofemoral ligament; TTO, tibial tubercle osteotomy; WC, workers’ compensation.
Based on variable selection with bivariate correlation models (Table 2), logistic regression analysis revealed that “multiple previous operations” was the only significant predictive factor for patients’ cell identity assay scores. Patients who had multiple previous operations on the index knee were 0.31 times as likely to have an identity score that was above the cohort’s average as compared with patients without previous surgical procedures (odds ratio = 0.31; 95% CI, 0.16-0.59; P < .001) (Table 3). Patients who did not undergo previous surgery had significantly higher cell identity scores (6.32 ± 1.96) as compared with patients with 1 (5.32 ± 2.05; P = .006) or ≥2 (5.05 ± 2.17; P < .001) surgical procedures. There were no significant differences between patients with 1 and ≥2 surgical procedures (P = .614) (Figure 1). Cell viability was not significantly predicted by any of the preoperative patient-specific variables, nor was it correlated with cell identity (P > .05) (Tables 2 and 4).
Bivariate Correlations Between Patient Demographics, Lesion Type, Biopsy Sample Weight, and Cell Viability and Identity Groups a
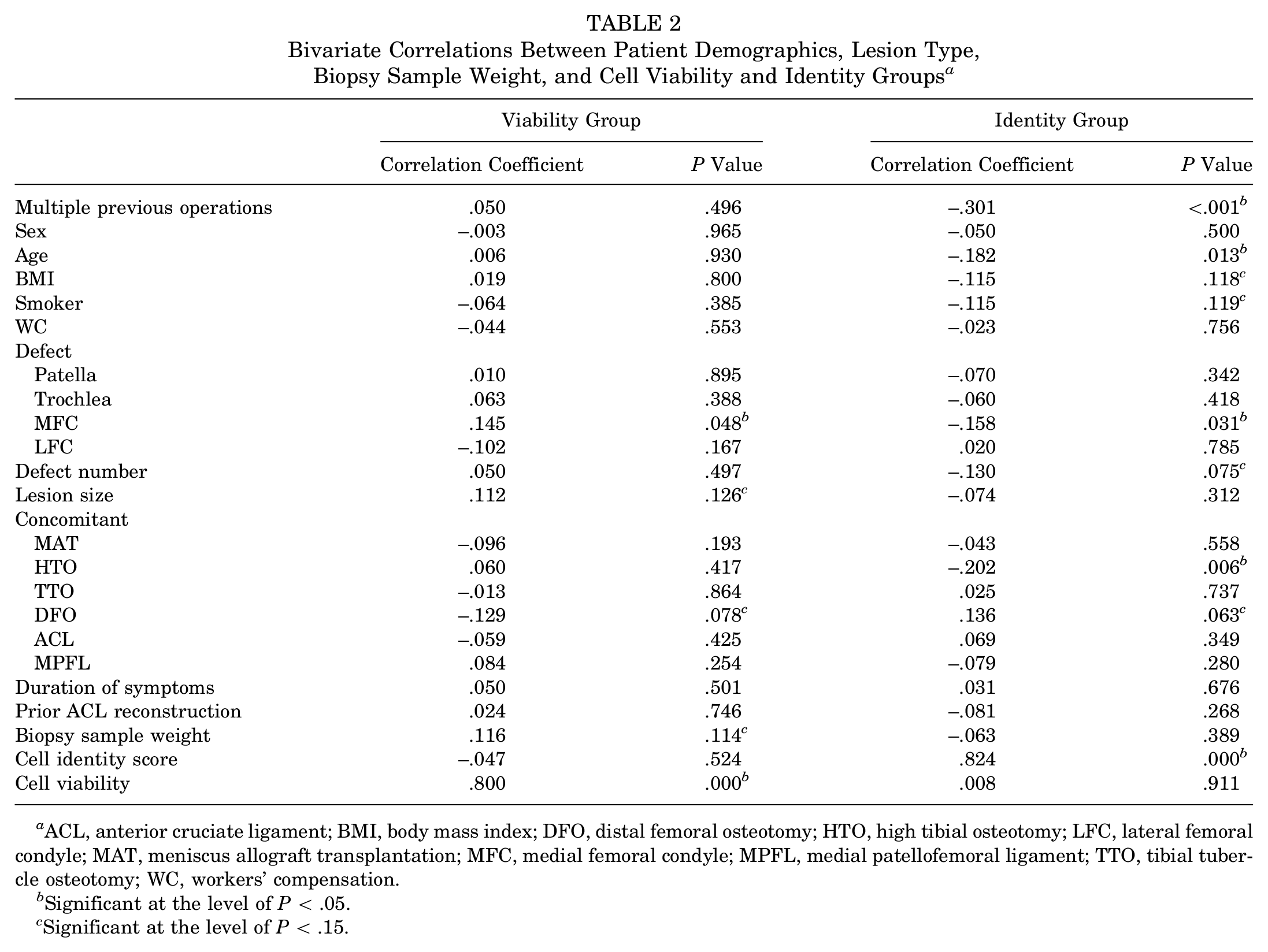
ACL, anterior cruciate ligament; BMI, body mass index; DFO, distal femoral osteotomy; HTO, high tibial osteotomy; LFC, lateral femoral condyle; MAT, meniscus allograft transplantation; MFC, medial femoral condyle; MPFL, medial patellofemoral ligament; TTO, tibial tubercle osteotomy; WC, workers’ compensation.
Significant at the level of P < .05.
Significant at the level of P < .15.
Logistic Regression Model Presenting Multiple Previous Operations as the Only Predictive Variable Associated With Cell Identity a
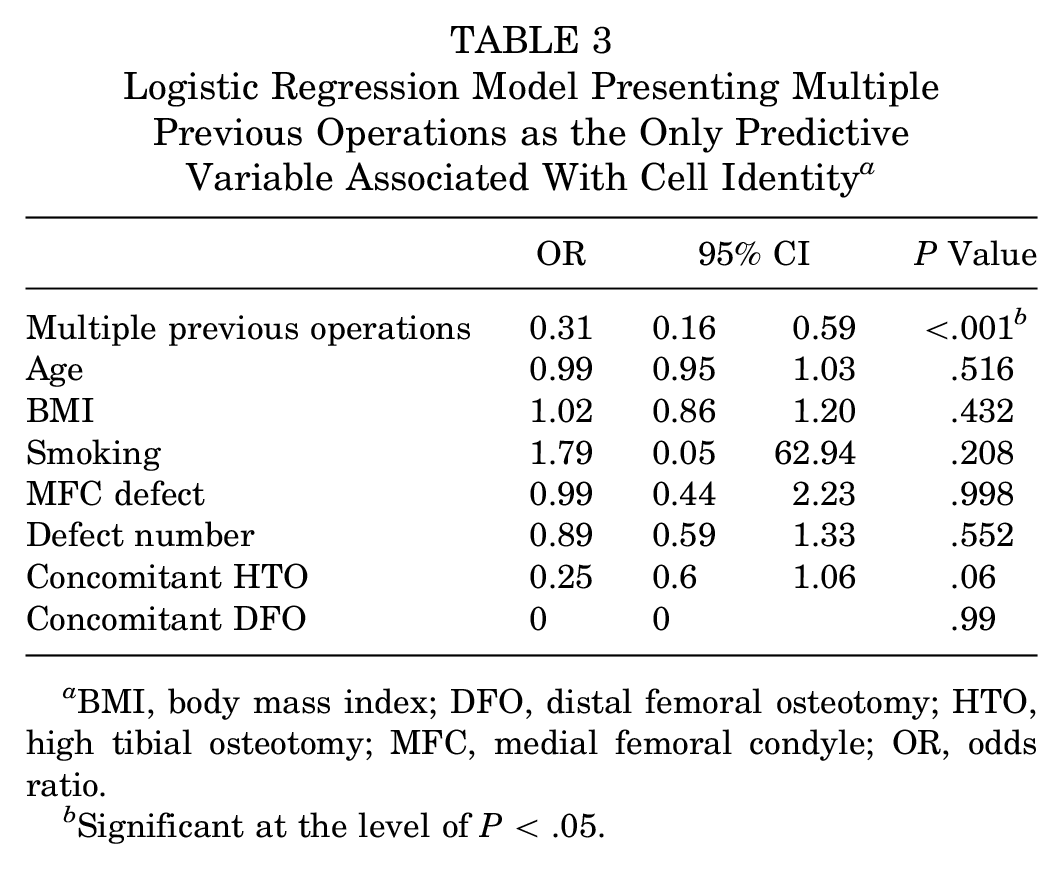
BMI, body mass index; DFO, distal femoral osteotomy; HTO, high tibial osteotomy; MFC, medial femoral condyle; OR, odds ratio.
Significant at the level of P < .05.
Logistic Regression Model Showing No Predictive Correlation Between Patient-, Lesion-, or Biopsy Specimen–Associated Parameters and Cell Viability a
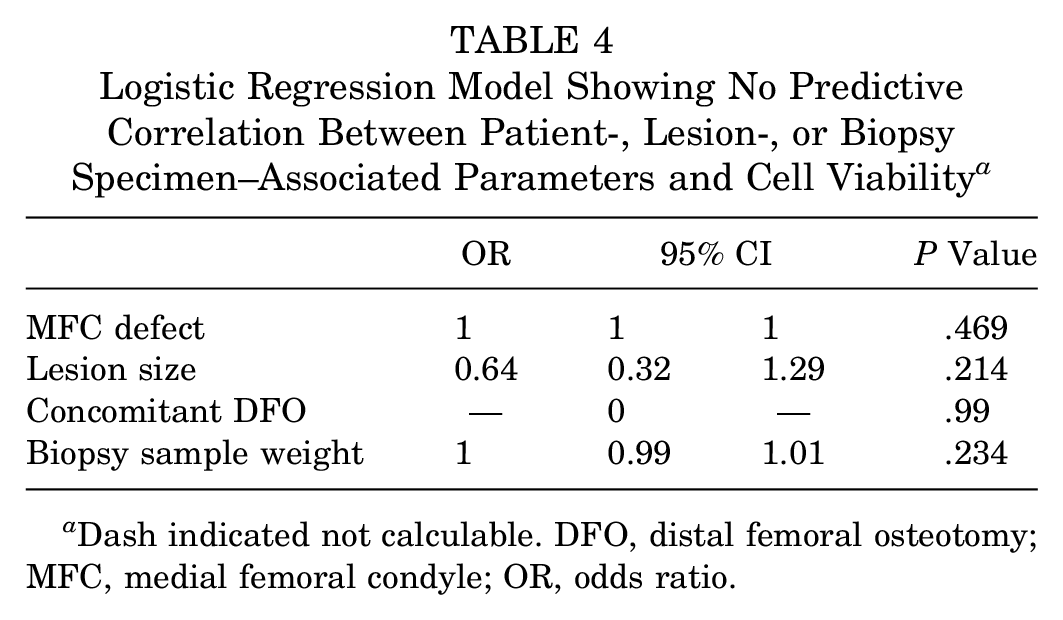
Dash indicated not calculable. DFO, distal femoral osteotomy; MFC, medial femoral condyle; OR, odds ratio.
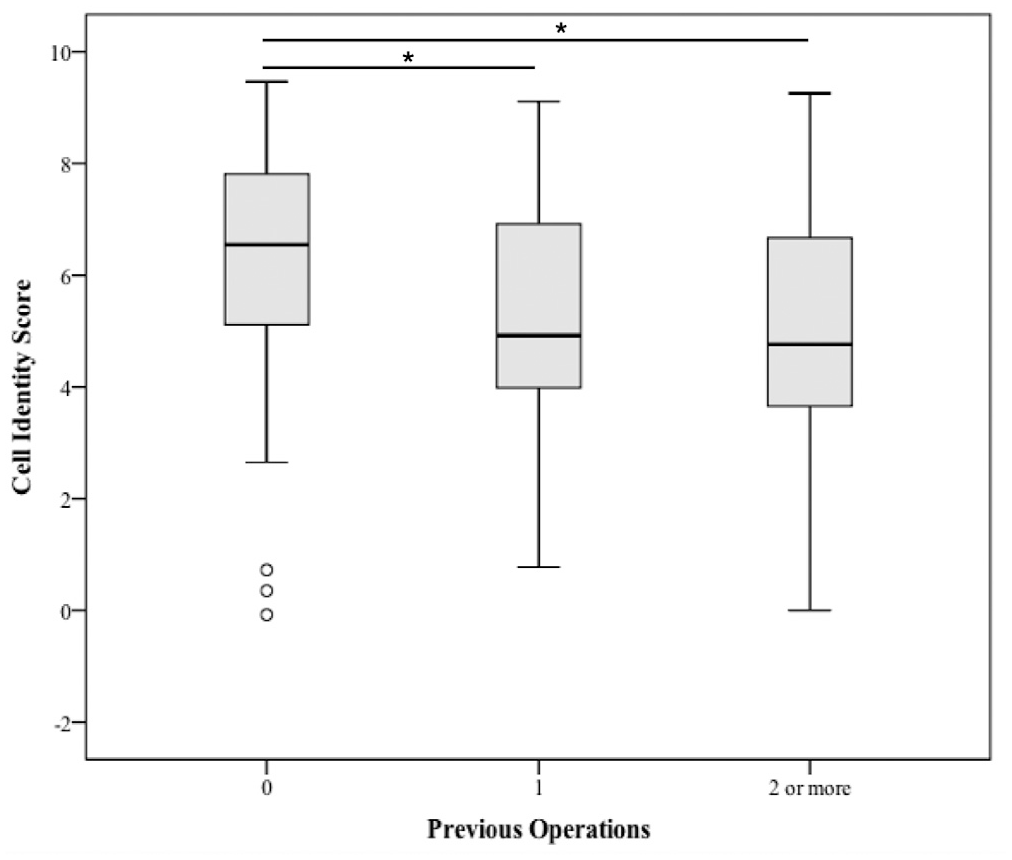
Patients who did not undergo previous surgery on the index knee had significantly higher cell identity scores than patients with ≥1 previous surgical procedures. Values are presented as median (line), interquartile range (box), 95% CI (error bars), and outliers (circles). *P < .05.
Discussion
The key finding of this study was that prior surgery on the index knee negatively influenced the cell identity assay score. Biopsy specimens from patients without previous surgery were >3 times likely to have a cell identity score above average as compared with patients with previous surgery. Even patients with a single intervention before the cartilage biopsy had significantly lower cell identity scores than patients without surgical history. Other factors—most important, biopsy specimen weight (within the ranges seen in this patient cohort)—were not found to influence either cell viability or cell identity score.
While numerous factors—such as age, female sex, lower preoperative patient-reported scores, workers’ compensation status, longer duration of symptoms, defect number/location/size, and prior cartilage repair procedures—have all been associated with less favorable results after ACI,9,13-15 recent research has focused on cell quality and its influence on clinical outcomes. In a recent study, Ackermann et al 1 investigated the influence of cell identity and viability on patient-reported outcome measures, graft survival, and repair tissue appearance on magnetic resonance imaging after ACI. They reported that high cell identity scores were significantly associated with both better structural repair quality on magnetic resonance imaging (per the MOCART [magnetic resonance observation of cartilage repair tissue] score) and higher ACI graft survivorship at 5-year follow-up. In their study, patients with an identity score >5.8 had a cumulative survivorship of 95.8% at 5 years, as opposed to 64.7% survival in patients with a lower identity score. In fact, cell identity score and smoking were shown to be the only independent predictors of ACI graft survival.
Niemeyer et al 17 analyzed the influence of collagen type II, CD44, and aggrecan expression and cell viability on clinical outcomes of patients after ACI. At 6, 12, and 24 months postoperatively, collagen type II expression, CD44 expression, and cell viability were significantly associated with clinical outcomes as measured with International Knee Documentation Committee scores. The authors hypothesized that early collagen type II expression was related to improved clinical results and that it therefore might be beneficial to stimulate collagen type II expression in vitro before implantation. Collagen type II is cartilage specific and has been used as a marker to demonstrate chondrocyte expansion and proliferation. 21 Based on the results of Ackermann et al 1 and Niemeyer et al, it can be argued that a high preoperative cell identity score (higher chondrocyte:synoviocyte gene expression ratio) could result in higher collagen type II expression of the implant, thus ultimately improving clinical outcomes and graft survival after ACI.
Pestka et al 20 investigated the influence of preoperative factors on cell quality, defined as the expression of CD44, aggrecan, and collagen type II, as well as cell density and viability. They reported that among age, sex, lesion size and location, number of defects, and grade of joint degeneration, only patient age <20 years resulted in significantly higher cell quality.
The current study confirmed our hypothesis that patients with multiple previous surgical procedures have decreased cell product quality. This is of consequence, as previous surgical interventions may spread synovial tissue onto the articular surface, thus contaminating the ACI biopsy specimens and leading to inferior purity of the final cell product. 24 This finding might stimulate research into mechanical cleaning of the biopsy site before harvest or the biopsy specimen once received in the laboratory to reduce contamination with synoviocytes. Conversely, it can be theorized that “multiple previous surgical procedures” is a surrogate marker and simply implies a worse overall biological environment in the knee as the mechanism for decreased cartilage quality rather than prior surgery per se. The current study, however, investigated the association of a patient’s duration of symptoms with one’s cell quality in the final ACI product. It can be assumed that patients with chronic symptoms have an inferior biological environment within the affected knee, yet there was no significant association between duration of symptoms and cell identity or viability. Moreover, multiple previous surgical procedures would suggest even more chronic and unresolved inflammation within the knee joint when compared with a single previous procedure. However, a single prior surgical procedure already significantly reduced cell identity, whereas multiple procedures did not further reduce cell quality. While we acknowledge the fact that multiple previous surgical procedures might correlate with an even less favorable biological environment within the index knee, we believe that the reduction in cell quality after a single previous procedure is more suggestive of the contamination with synovial tissue as the mechanism for a negatively affected cell culture identity in patients with a history of surgery.
Consequently, this might be beneficial information in surgical decision making and preoperative counseling in selecting the appropriate cartilage repair procedure. In fact, given the results of the current study in conjunction with those reported by Ackermann et al, 1 it is advisable to obtain a cartilage biopsy specimen as early as possible in a patient’s surgical treatment for a given knee injury if cartilage repair with ACI is considered a potential treatment option. In other words, it is consequential that patients who undergo primary knee surgery with the potential of future cartilage repair also undergo concomitant cartilage biopsy, as such specimens can be stored for many years until implantation. This may improve the outcome after ACI in patients with previous surgery. Given previous reported results (ie, patients aged <20 years have superior cell quality), the current study can also set the framework for selecting biopsy samples of appropriate patients for allogenic chondrocyte implantation in the future. 7
Last, within the range evaluated in the present study, biopsy specimen weight seemed to have no influence on cell quality of the final product, suggesting that only small amounts of cartilage (within the manufacturer’s suggested range of 100-300 mg) are required to achieve favorable cell quality.
In summary, multiple previous operations negatively affect chondrocyte culture, likely attributed to contamination with synovial tissue, thus reducing the cell identity score. Cell viability was not correlated with patient-, defect-, or biopsy specimen–associated factors.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.B.M. has received grants from Vericel and JRF Ortho. A.H.G. as received grants and personal fees from Vericel, Aastrom, Genzyme, Sanofi, and JRF Ortho; personal fees from Moximed, Geistlich, Aesculap, and Nutech/Organogenesis; personal fees and other from Smith & Nephew and Lifenet; and other from Fidia and Stryker. J.A. has received grants from Vericel and JRF Ortho. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Submitted June 28, 2019; accepted October 29, 2019.