
Abstract
Background:
Minimal clinically important difference (MCID), substantial clinical benefit (SCB), and patient acceptable symptomatic state (PASS) have gained prominence as important variables in the orthopaedic outcomes literature. In hip preservation surgery, much attention has been given to defining early clinically meaningful outcome; however, it is unknown what represents meaningful patient-reported outcome improvement in the medium to long term.
Purpose:
(1) To define MCID, PASS, and SCB at a minimum 5 years after hip arthroscopy for femoroacetabular impingement syndrome (FAIS) and (2) to evaluate the time-dependent nature of MCID, PASS, and SCB.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients undergoing primary hip arthroscopy for FAIS between January 2012 and March 2014 were included. Clinical and demographic data were collected in an institutional hip preservation registry. MCID, PASS, and SCB were calculated for each outcome score including the Hip Outcome Score–Activities of Daily Living subscale (HOS-ADL), Hip Outcome Score–Sport-Specific subscale (HOS-SS), modified Harris Hip Score (mHHS), and International Hip Outcome Tool (iHOT-12) at 1, 2, and 5 years. MCID was calculated by use of a distribution-based method, whereas PASS and SCB were calculated by use of an anchor method.
Results:
The study included 283 patients with a mean ± SD age of 34.2 ± 11.9 years. The mean changes in 1-year, 2-year, and 5-year scores, respectively, required to achieve MCID were as follows: HOS-ADL (8.8, 9.7, 10.2); HOS-SS (13.9, 14.3, 15.2); mHHS (6.9, 9.2, 11.4); and iHOT-12 (15.1, 13.9, 15.1). The threshold scores for achieving PASS were as follows: HOS-ADL (89.7, 88.2, 99.2); HOS-SS (72.2, 76.4, 80.9); mHHS (84.8, 83.3, 83.6); and iHOT-12 (69.1, 72.2, 74.3). Last, the threshold scores for achieving SCB scores were as follows: HOS-ADL (89.7, 91.9, 94.6); HOS-SS (78.1, 77.9, 85.8); mHHS (86.9, 85.8, 94.4); and iHOT-12 (72.6, 76.8, 87.5). More patients achieved MCID, SCB, and PASS at 2-year compared with 1-year follow-up; however, by 5 years, fewer patients had achieved clinically meaningful outcome (minimum 1-, 2-, and 5-year follow-up, respectively: MCID, 82.6%, 87.3%, 79.3%; PASS, 67.6%, 74.9%, 67.5%; SCB, 62.3%, 67.2%, 56.6%).
Conclusion:
The greatest proportion of patients achieved MCID, PASS, and SCB at 2-year follow-up after arthroscopic treatment of FAIS compared with 1- and 5-year time points. Improvements were maintained out to 5-year follow-up, although the proportion of patients achieving clinical significance was slightly decreased.
Interest has increased in defining clinically meaningful outcomes in orthopaedic surgery. Minimal clinically important difference (MCID), patient acceptable symptomatic state (PASS), and substantial clinical benefit (SCB) are increasingly being reported as measures of clinically meaningful outcome. 3 MCID represents the smallest change that is clinically meaningful and detectable to a patient. 16 SCB, however, represents outcome improvement that is not only detectable to the patient, but that the patient finds to be considerable. 12 MCID and SCB have been posited to represent a spectrum of clinical outcome improvement, with MCID representing the lower bound and SCB the upper bound of outcome improvement. However, although MCID and SCB exist within a functional outcome domain, PASS exists within the satisfaction domain and seeks to quantify the health state that patients find satisfactory. 5
Although MCID, SCB, and PASS are increasingly reported in the orthopaedic literature, a particular focus on these outcome endpoints is found in the field of hip preservation surgery. Because of the significant variability in outcome assessment for hip preservation surgery, there has been a shift toward defining clinically meaningful outcome after the arthroscopic treatment of femoroacetabular impingement syndrome (FAIS). Previous clinical investigators have defined MCID, SCB, and PASS at discrete time points after the arthroscopic treatment of FAIS. Nwachukwu et al 31 defined SCB and MCID for hip arthroscopy at 1-year time points, and Chahal et al 5 defined PASS at a similar time point. Flores et al 10 performed a prospective cohort analysis to determine when the MCID was achieved after hip arthroscopy. Those authors evaluated MCID at various time points up to 2-year follow-up. To our knowledge, no previous study has provided a psychometric analysis for meaningful outcome in hip preservation surgery beyond 2-year follow-up. Additionally, limited understanding is available regarding the medium- to long-term patient-reported outcomes in patients undergoing hip arthroscopy with modern surgical techniques and comprehensive capsular management.35,38
Given the paucity of evidence on medium- to long-term clinically meaningful outcome after orthopaedic procedures, specifically arthroscopic hip preservation surgery, we sought to address this deficiency in the available literature. The primary purpose of the present study was to define MCID, PASS, and SCB at a minimum 5 years after hip arthroscopy for FAIS. Secondarily, we sought to evaluate the time-dependent nature of MCID, PASS, and SCB. We hypothesized that the rates of achieving meaningful outcome changes over time—specifically MCID, SCB, and PASS—would trend upward at 1-year, 2-year, and 5-year follow-up points.
Methods
Patient Selection
This study was approved by the institutional review board of the senior author’s (S.J.N.) institution (12022108-IRB01-CR06). Prospective data on all patients undergoing hip arthroscopy for treatment of FAIS by a single, fellowship-trained surgeon (S.J.N.) were collected and analyzed in a clinical repository. All patients undergoing primary hip arthroscopy for the treatment of FAIS between January 1, 2012, and March 1, 2014, were included in this study. Inclusion criteria consisted of clinical and radiographic diagnosis of symptomatic FAIS, 13 failure of nonoperative management (physical therapy, activity modification, oral anti-inflammatory agents, and intra-articular cortisone injection), and a minimum 5-year follow-up. Exclusion criteria consisted of hip arthroscopy for an indication other than FAIS, previous ipsilateral hip surgery, signs of osteoarthritis (Tönnis grade >1), hip dysplasia (lateral center-edge angle of Wiberg [LCEA] <20°), 1 or a history of pediatric hip disorders (slipped capital femoral epiphysis, developmental hip dysplasia, avascular necrosis, etc).
Radiographic Analysis
All patients had a series of preoperative and postoperative radiographs at 1-month follow-up. 42 Each series consisted of a standing anteroposterior pelvic radiograph, an anteroposterior hip radiograph, a false-profile hip radiograph, and a 45° Dunn lateral hip radiograph. 6 Measurements of interest included alpha angle, Tönnis angle, Tönnis grade, LCEA, and anterior center-edge angle (ACEA).28,18,41 All radiographic measurements were made by the senior author (S.J.N.) and confirmed by an orthopaedic fellow (B.U.N.).
Surgical Technique
All hip arthroscopies were performed by a single fellowship-trained hip surgeon at a high-volume academic hospital using a technique that has been well-described in the literature.11,14,39 Briefly, a standard anterolateral portal was established under fluoroscopic guidance, and an anterior portal was established under direct visualization. The modified midanterior portal was established via spinal needle localization under direct arthroscopic visualization. A 2- to 4-cm capsulotomy connecting the anterior to anterolateral portal was performed. Any central compartment pathological condition was then addressed in a standard fashion, including labral repair and acetabular rim trimming if pincer morphology was present.
After completion of the procedures in the central compartment, traction was released, and the hip was flexed to 20° to access the peripheral compartment. Via the anterior portal, the arthroscope was placed into the peripheral compartment, and a T-capsulotomy was performed between the 12-o’clock and 2-o’clock positions to the intertrochanteric line. The capsule was then reflected, and any necessary osteochondroplasty of the cam deformity was performed. Dynamic examination and fluoroscopic imaging were used to confirm that there was no further impingement and that head-neck offset was restored. Once the arthroscopic procedure was complete, a complete capsular closure was performed. The vertical T-limb of the T-capsulotomy was closed first, beginning at the base of the iliofemoral ligament; after this, the interportal capsulotomy was closed.
Functional Outcome Evaluation
Patients completed preoperative and 1-year, 2-year, and 5-year postoperative, hip-specific, patient-reported outcome instruments including the Hip Outcome Score–Activities of Daily Living subscale (HOS-ADL), 21 the Hip Outcome Score–Sport-Specific subscale (HOS-SS), 23 the modified Harris Hip Score (mHHS),4,15 and the International Hip Outcome Tool (iHOT-12). 30 In addition, patients graded their pain level and satisfaction level from 1 to 100 with a visual analog scale (VAS). A minimum of 5-year follow-up on the HOS-ADL, HOS-SS, and anchor questions was required for a patient to be included in the study. Because the algorithm of the survey platform leads patients to address the HOS-ADL, HOS-SS, and anchor questions first, the vast majority of patients who completed these components would have completed the mHHS, iHOT-12, and VAS pain and satisfaction as well.
To quantify the clinical significance of meaningful outcome achievement, MCID, SCB, and PASS were calculated for HOS-ADL, HOS-SS, mHHS, and iHOT-12. MCID can be calculated by use of anchor or distribution-based methods, each with its own set of limitations. The anchor-based method is limited and not suitable for patients undergoing hip arthroscopy for FAIS, where most patients will report improvement and few will remain unchanged. The anchor-based method is also inherently limited by the number of patients who answer anchor-based questions. 7 MCID was calculated via the distribution method using half the standard deviation for each hip outcome tool for the overall cohort.16,20,30,34 MCID was calculated separately at 1-year, 2-year, and 5-year follow-up points. Patients were classified as achieving MCID if the MCID was achieved on any of the included outcome measures.
PASS was calculated by use of an anchor-based method. 5 At 1-, 2- and 5-year time points, patients were asked the following anchor question: “Taking into account all the activities you have during your daily life, your level of pain, and also your functional impairment, do you consider that your current state is satisfactory?” PASS values were then identified via a receiver operating characteristic (ROC) curve analysis as done in previous studies (see Appendix 1, available in the online version of this article).5,8,30 A sensitivity and specificity value of 0.80 was used as a cutoff for determining acceptable threshold scores. Patients were classified as achieving PASS if PASS was achieved on any of the included outcome measures.
SCB was similarly calculated through use of an anchor-based method. 31 At 1-, 2-, and 5-year time points, patients were asked the following anchor question: “Since your surgery, has there been any change in your daily functioning and nonsporting activities related to your treated hip?” Patients responding with “A very great deal better,” “A great deal better,” or “A good deal better” were classified as the “much improved group”; patients responding with “Almost the same, hardly any better,” “No change,” or “Almost the same, hardly any worse” were classified as the “no change group.” Using a method similar to previous studies, we applied ROC curve analysis to identify an absolute score that best differentiated outcome in these 2 groups; this value was defined as SCB. 31 Pain and physical function–related questions are both acceptable anchor questions for psychometric analysis to identify clinically meaningful improvements in function.26,29,31 The ROC curve analysis is provided in Appendix 2 (available online). As with previous psychometric studies in the orthopaedic literature, an area under the curve greater than 0.8 was considered acceptably predictive.2,31 Patients were classified as achieving SCB if SCB was achieved on any of the included outcome measures.
Statistical Analysis
All data were screened to determine whether they met all parametric statistical assumptions before analysis. Descriptive statistics for all continuous variables were reported as means ± standard deviations. Frequency statistics were reported for all noncontinuous variables. Paired-samples t tests were used to compare preoperative and 2-year postoperative patient-reported outcome scores in patients with FAIS. Chi-square analysis was used to identify statistically significant changes in the proportion of patients achieving MCID, PASS, and SCB over the different time points. Statistical significance for all analysis was set at α < .05. All statistical analysis was performed through use of SPSS (version 25; SPSS Inc).
Results
Of the 402 patients in the patient database within the time frame of the study, 283 (70.4%) met the inclusion criteria and were included in the final analysis (Figure 1). The study group had a mean ± SD age and body mass index of 34.2 ± 11.9 years and 26.1 ± 14.2 kg/m2, respectively (Table 1). Of the 283 patients, 63.3% were female, and 69.7% reported engaging in any form of physical exercise or competitive sports. The majority of patients had femoroplasty (96%), acetabular trimming (85.5%), and labral repair (100%).
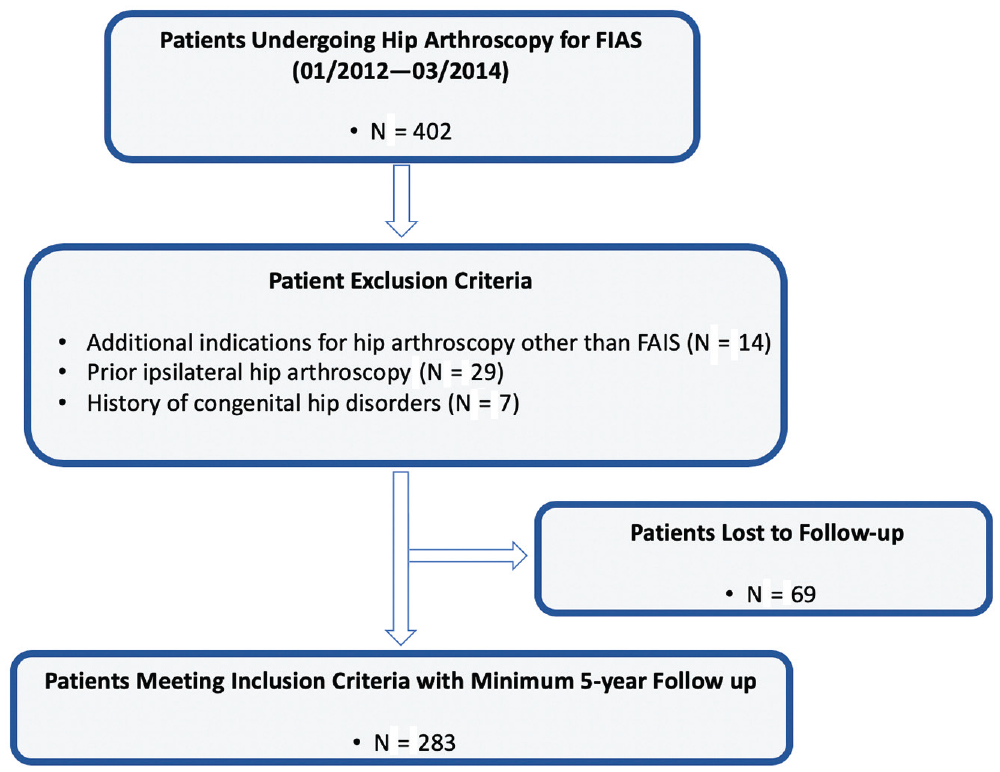
Flowchart indicating the number of patients excluded from the study, those lost to follow-up, and those meeting inclusion criteria who were included in the final analysis. FAIS, femoroacetabular impingement syndrome.
Patient Characteristics a
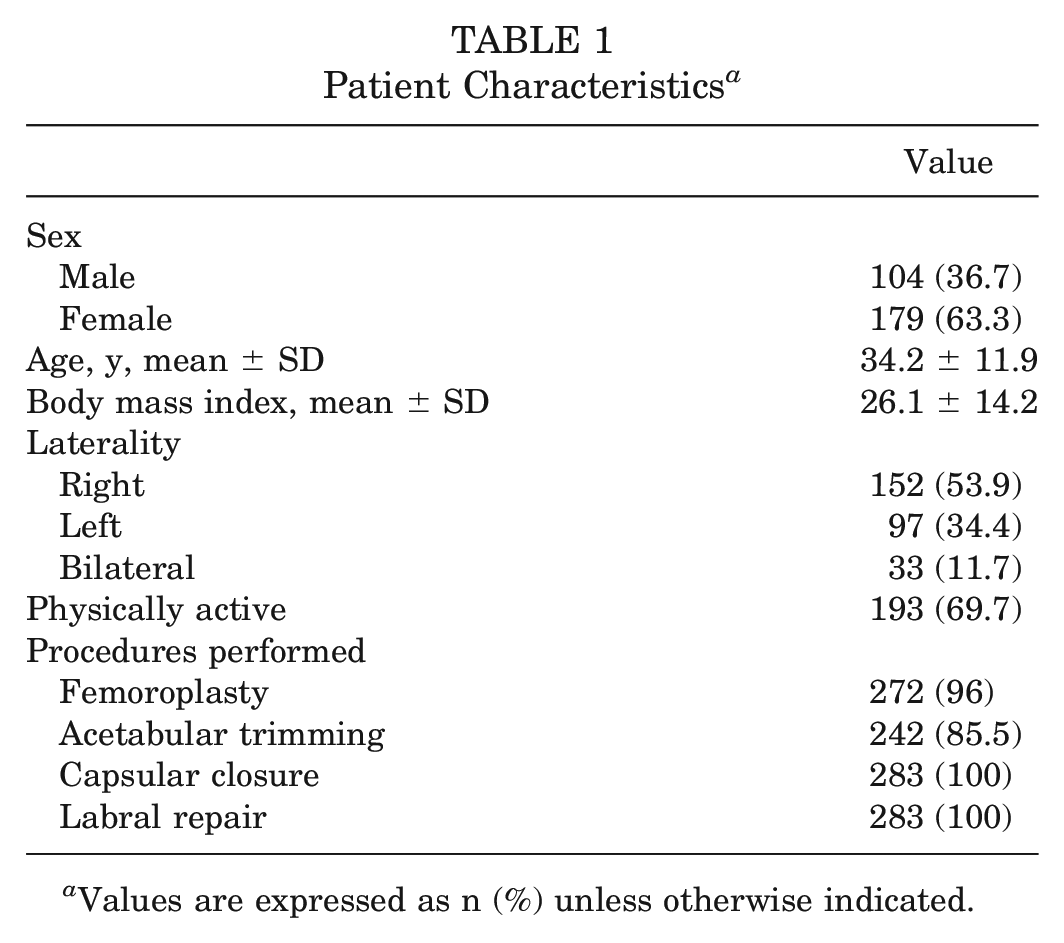
Values are expressed as n (%) unless otherwise indicated.
Radiographic Analysis
Alpha angles (measures in all radiographic views), LCEA, and ACEA all had a statistically significant decrease from preoperative to postoperative points (Table 2). Most patients did not have any prearthritic changes at the time of surgery (Tönnis grade 0; n = 243 [87.7%]).
Radiographic Parameters a
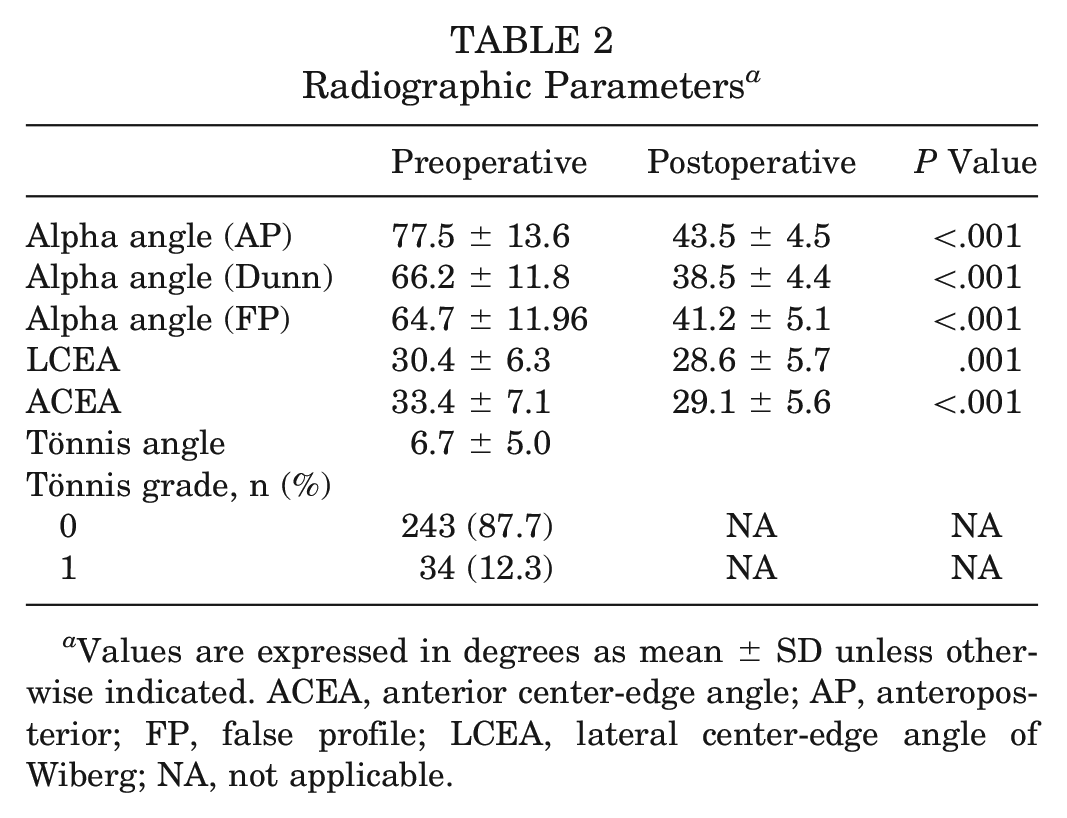
Values are expressed in degrees as mean ± SD unless otherwise indicated. ACEA, anterior center-edge angle; AP, anteroposterior; FP, false profile; LCEA, lateral center-edge angle of Wiberg; NA, not applicable.
Patient-Reported Outcomes
A statistically significant increase was noted in all mean postoperative patient-reported outcome scores when all postoperative time points were compared with preoperative scores (Figure 2, Table 3). Similarly, the VAS pain score was statistically improved (decreased) at minimum 1-, 2-, and 5-year follow-up compared with preoperative assessment. The VAS satisfaction scores for minimum 1-, 2-, and 5-year follow-up were 78.3 ± 48.7, 79.1 ± 27.8, and 72.6 ± 32.9, respectively.
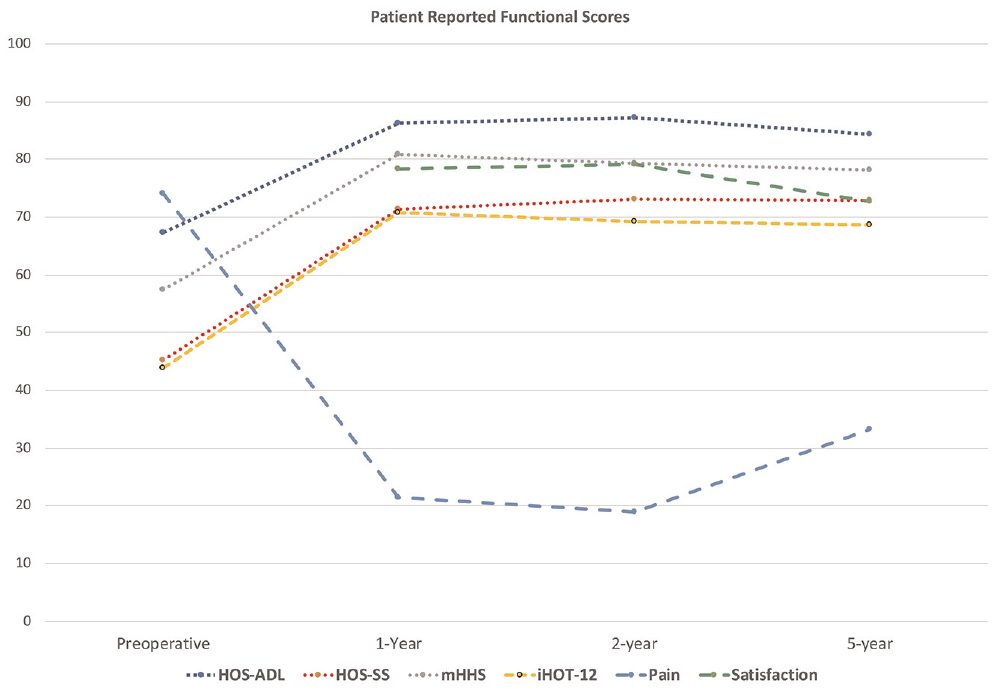
Linear graph describing the changes in Hip Outcome Score–Activities of Daily Living subscale (HOS-ADL), Hip Outcome Score–Sport-Specific subscale (HOS-SS), modified Harris Hip Score (mHHS), International Hip Outcome Tool (iHOT-12) score, and visual analog scale scores for pain and satisfaction over the 1-, 2-, and 5-year time points.
Comparison of Preoperative Scores Versus Minimum 1-, 2-, and 5-Year Follow-up Outcome Scores a
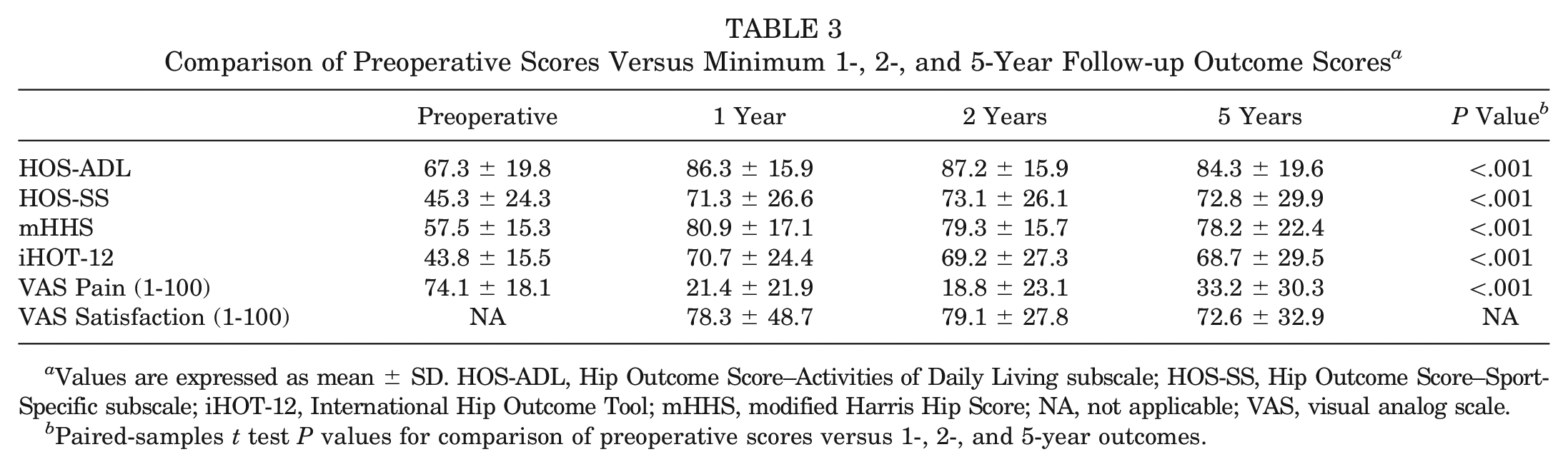
Values are expressed as mean ± SD. HOS-ADL, Hip Outcome Score–Activities of Daily Living subscale; HOS-SS, Hip Outcome Score–Sport-Specific subscale; iHOT-12, International Hip Outcome Tool; mHHS, modified Harris Hip Score; NA, not applicable; VAS, visual analog scale.
Paired-samples t test P values for comparison of preoperative scores versus 1-, 2-, and 5-year outcomes.
MCID, PASS, and SCB Analysis
The calculated MCID, PASS, and SCB values for HOS-ADL, HOS-SS, mHHS, and iHOT-12 for 5 years are summarized in Table 4. On all outcome tools except for the iHOT-12, the score required to achieve MCID increased over time.
MCID, PASS, and SCB Threshold Scores a
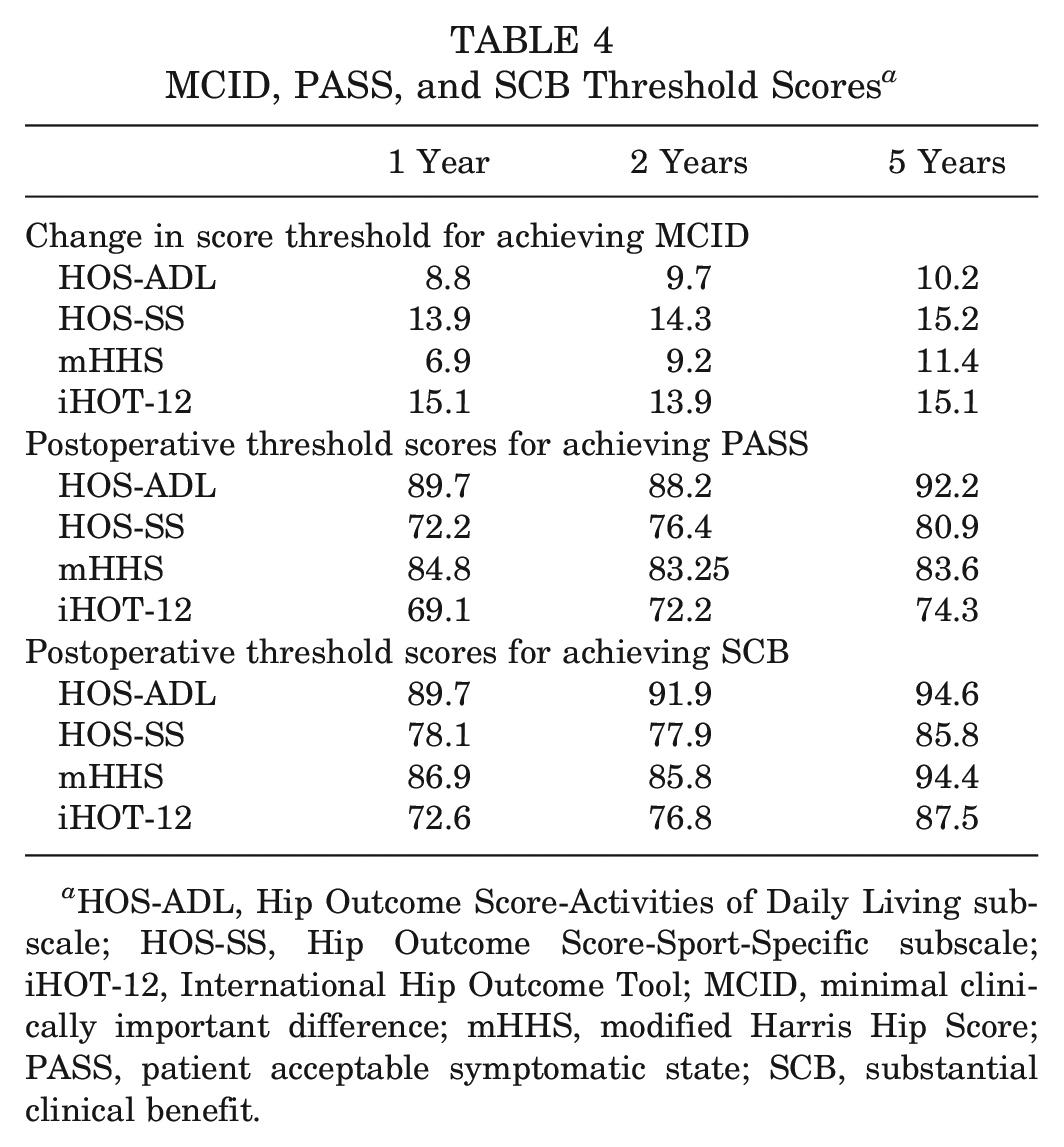
HOS-ADL, Hip Outcome Score-Activities of Daily Living subscale; HOS-SS, Hip Outcome Score-Sport-Specific subscale; iHOT-12, International Hip Outcome Tool; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, patient acceptable symptomatic state; SCB, substantial clinical benefit.
When the follow-up time points were compared, the highest proportion of patients achieved MCID, SCB, and PASS at minimum 2-year postoperative follow-up (87.3%, 74.9%, and 67.2%, respectively) (Table 5). Although more patients achieved MCID, SCB, and PASS at 2-year follow-up, by 5 years fewer patients were found to have achieved clinically meaningful outcome.
Frequency of Patients Achieving Any MCID, PASS, or SCB Threshold at Minimum 1-, 2-, and 5-Year Follow-up a
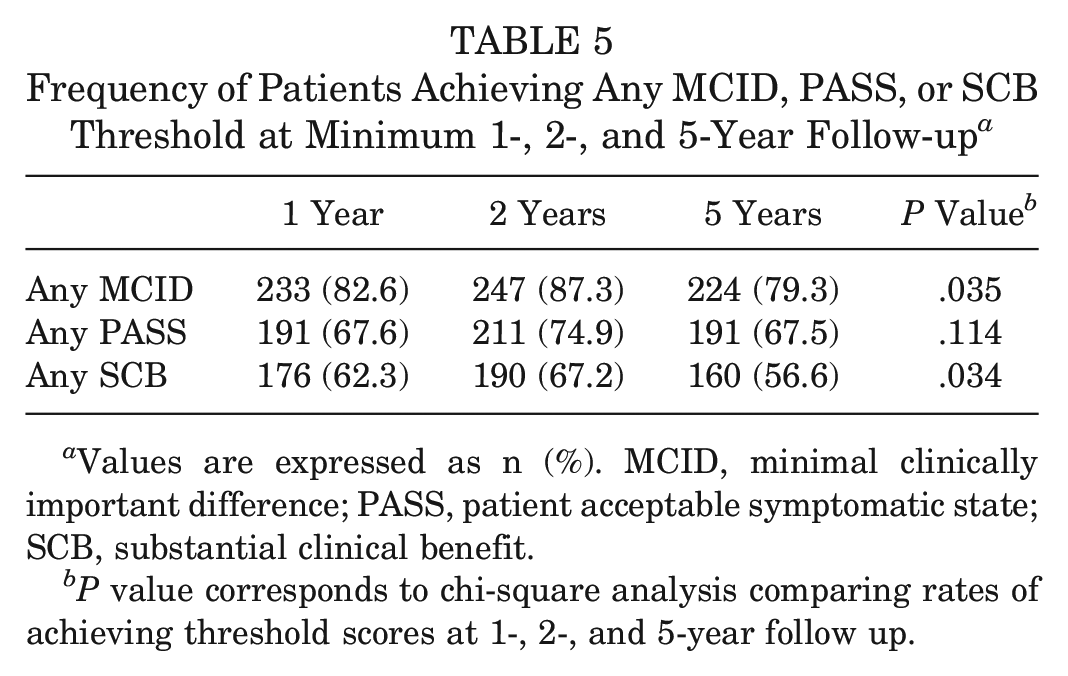
Values are expressed as n (%). MCID, minimal clinically important difference; PASS, patient acceptable symptomatic state; SCB, substantial clinical benefit.
P value corresponds to chi-square analysis comparing rates of achieving threshold scores at 1-, 2-, and 5-year follow up.
Discussion
In this study, we defined MCID, PASS, and SCB on the mHHS, HOS-ADL, HOS-SS, and iHOT-12 at minimum 1-, 2-, and 5-year follow-up. MCID values ranged from 6.9 to 15.2, PASS values ranged from 69.1 to 92.2, and SCB values ranged from 72.6 to 94.6. Across all outcome tools, the values required to achieve MCID, SCB, and PASS were highest at 5-year follow-up, and the lowest proportion of patients achieved clinically meaningful outcome at this time point. Interestingly, patients most consistently achieved clinically meaningful outcome at 2-year follow-up. However, by 5-year follow-up, 79.3% of patients achieved MCID, thereby suggesting some decline between 2 and 5 years. Additionally, our findings suggest that the requirements for clinically meaningful outcome may increase over time, with patients needing higher scores at 5-year follow-up to maintain clinically meaningful outcome.
Previous work has sought to both define and evaluate psychometric measures for commonly used hip outcome tools in various patient populations to better quantify what represents clinically meaningful outcome in patients who undergo hip preservation surgery. A few previous studies have looked at MCID, PASS, and SCB values for common hip outcome tools.22,30,32 None of these previous studies, however, looked at these measures prospectively at multiple time points, and no previous study has looked at the MCID, PASS, and SCB at minimum 5-year follow-up. The 1- and 2-year MCID, PASS, and SCB reported in the current study are similar to values reported in other studies, thereby confirming the appropriateness of our analysis.27,30-33,40 It is worth noting that meaningful clinical threshold values vary based on disease and population17,19; as such, we sought to calculate 1- and 2-year MCID, SCB, and PASS de novo in addition to our primary 5-year analysis.
Our study findings suggest that there is a time-dependent nature to achieving clinically meaningful outcome improvement. Nwachukwu et al 29 found that the majority of patients achieved MCID and SCB by 6 months postoperatively; however, the proportion of patients achieving clinically meaningful outcome improvement continued to increase out to 2 years postoperatively. The current study confirms the analysis by Nwachukwu et al and provides insight into clinically meaningful outcome beyond 2-year follow-up. Specific to MCID, we found that the net values remained relatively constant across multiple time points, all within 0 to 1.36 points of each other with the exception of the mHHS. This finding demonstrates that the minimum threshold for outcome is relatively constant even at 5 years after hip arthroscopy. Similar trends, however, were not consistently demonstrated for PASS and MCID; by 5-year follow-up, the values required to achieve clinically meaningful outcome showed quantifiably larger absolute increases. Interestingly, we also found that although a large proportion of patients still achieved clinically meaningful outcome improvement, there was a slight decline in the overall percentage of patients with meaningful outcome improvement at 5-year follow-up compared with 2-year follow-up. The reason for this finding is unclear; however, it may result from the fact that values required to achieve MCID, SCB, and PASS at the 5-year time point were higher than at previous time points. It is also possible that by 5-year follow-up, patient expectations for outcome improvement were greatly increased such that larger absolute values were needed to generate the same consideration of clinically meaningful outcome. Additionally, it is possible that by 5-year follow-up, outcome score changes were less reflective of postoperative outcome than at 2-year follow-up. As such, the decreased proportion of patients achieving clinically meaningful outcome at 5-year follow-up may represent an expected age-related decline in patient-reported outcomes, a phenomenon that has been well-established in the literature.9,24,25,43
The current study is one of the first to thoroughly assess clinically meaningful outcome improvement at 5 years after hip arthroscopy and to demonstrate the implications of measuring meaningful improvement over time. One of the major findings of this study was that patient-reported outcome improvement after hip arthroscopy for FAIS was maintained out to 5-year follow-up. Although the proportion of patients maintaining outcome improvement declined somewhat, the majority of patients still reported clinically meaningful outcome improvement. Specifically, by 5-year follow-up, 79% of patients had achieved MCID. Given that hip arthroscopy is a relatively novel and evolving surgical procedure, there is a paucity of medium- to long-term outcome studies. 35 A few previous studies have looked at the 5-year results of hip arthroscopy; however, these studies primarily focused on the survivorship of hip preservation surgery and statistically significant outcome improvement.36,37 As such, our findings have important implications for demonstrating the midterm clinical effect of hip arthroscopy. On a larger scale, our study highlights an opportunity for the assessment of what defines clinically meaningful outcome for other orthopaedic procedures.
This study has certain limitations that are worth noting. The reported psychometric values defined were based on a single cohort of patients at a large, tertiary care institution who underwent surgery by a single, high-volume surgeon. Therefore, it is possible that these values may not be generalizable to a larger population. Additionally, our study findings are limited to patient-reported outcome measures. We did not specifically seek to analyze survivorship or other functional outcome, such as return to sports. Finally, our study population consists primarily of young patients with minimal hip joint degeneration. This is representative of the senior author’s patient mix and may not represent the population with hip arthroscopy at large.
Conclusion
The greatest proportion of patients achieved clinically meaningful outcome improvement at 2-year follow-up after arthroscopic treatment of FAIS. Improvements were maintained out to 5-year follow-up, although there was a slight decrease in the proportion of patients achieving clinical significance.
Supplemental Material
DS_10.1177_0363546520902736 – Supplemental material for Defining the Clinically Meaningful Outcomes for Arthroscopic Treatment of Femoroacetabular Impingement Syndrome at Minimum 5-Year Follow-up
Supplemental material, DS_10.1177_0363546520902736 for Defining the Clinically Meaningful Outcomes for Arthroscopic Treatment of Femoroacetabular Impingement Syndrome at Minimum 5-Year Follow-up by Benedict U. Nwachukwu, Edward C. Beck, Kyle N. Kunze, Jorge Chahla, Jonathan Rasio and Shane J. Nho in The American Journal of Sports Medicine
Footnotes
Submitted July 15, 2019; accepted December 3, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.N. has received nonfinancial support from Allosource, Arthrex, Athletico, DJ Orthopaedics, Linvatec, Miomed, Smith & Nephew, and Stryker; personal fees from Ossur; hospitality payments from Stryker, Wright Medical Technology, and Zimmer Biomet; and indirect education payment from Smith & Nephew. J.C. has received indirect education support from Smith & Nephew and education and hospitality payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.