
Abstract
Background:
In young athletes, patient-reported activity level is frequently used to determine return to the same level of sport after treatment.
Purpose:
To evaluate the validity and score distributions of the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) compared with the Tegner Activity Level Scale (Tegner) in pediatric athletes.
Study Design:
Cohort study (Diagnosis); Level of evidence, 2.
Methods:
A retrospective review of 517 consecutive youth athletes who came to a sports medicine specialty clinic for a knee evaluation was performed. Patients completed the HSS Pedi-FABS, Tegner, and a sports participation survey before evaluation. Scores were compared with reported hours, days, and weeks of participation in sports as well as level of competition. Floor or ceiling effects were identified, and finally, the means and distributions of scores in the 8 most common primary sports were analyzed.
Results:
A total of 398 participants (54.0% female) with an average age of 14.5 years (range, 10.0-18.8 years) were included in the study. The HSS Pedi-FABS demonstrated correlations with hours per week (r = 0.302; P < .001), days per week (r = 0.278; P < .001), and weeks per year (r = 0.136; P = .014) playing a primary sport. The Tegner only demonstrated a correlation with days per week (r = 0.211; P = .001). Additionally, club/select-level athletes scored higher than junior high/high school–level athletes on the HSS Pedi-FABS (23.8 vs 21.0; P = .004), but no difference was observed with the Tegner. No floor or ceiling effect was observed for the HSS Pedi-FABS, but a ceiling effect was present for the Tegner (32.8%). The HSS Pedi-FABS demonstrated a varied score distribution between the 8 most common primary sports (P < .001), with soccer players scoring the highest, on average (23.5).
Conclusion:
The HSS Pedi-FABS, compared with the Tegner, demonstrated more correlations with an athlete’s participation in sport with no floor or ceiling effect and had a wide distribution of scores even among same-sport athletes. The HSS Pedi-FABS may be a more valuable activity measure than the Tegner in pediatric athletes.
Reported estimates of the number of active youth athletes in America range from 30 to 60 million.1,9 The U.S. Department of Health and Human Services reported that an average of 8.6 million people per year sustained a sport or recreation-related injury from 2011 through 2014, with the highest rate of injury observed among children aged 5 to 14 years. 29 One key factor for improving outcomes in the treatment of youth sports injuries is the use of patient-reported outcome measures (PROMs). The use of PROMs has the potential to identify issues that are often overlooked in routine medical care by facilitating a systematic and comprehensive approach to patient assessment. 18 Thus, it is necessary that the content of a PROM is relevant, appropriate, able to discern differences, and reliable for the patient population in which it will be used.
Various activity measures, in the form of PROMs, exist, but few are validated for use in pediatric patients.15,32,36 As a result, the pediatric literature often utilizes PROMs that were designed and validated for use in adult populations. 26 The inherent differences across athletic endeavors add complexity to the selection of appropriate PROMs. 13 Additionally, because of higher levels of preinjury function, ceiling effects may prevent the use of many PROMs in these populations.16,21 To accurately assess return to preinjury activity level, a measure often used to determine successful treatment of an athlete, standardized pediatric-specific outcome measures that are able to accommodate high levels of function and activity are required. 7
Tegner and Lysholm 34 described one of the first patient-reported activity scales in 1985, the Tegner Activity Level Scale (Tegner). The scale was initially designed for use in patients with anterior cruciate ligament ruptures but has since been studied in various conditions along with healthy populations.4 -6,25 The scale has become widely used, but there is little evidence supporting its use in pediatric patients or in athletes. 30 Additionally, while the measure may be appropriately used to categorize a respondent’s activity, it is frequently used incorrectly to measure activity level.2,31,39 In 2013, the Hospital for Special Surgery developed the Pediatric Functional Activity Brief Scale (HSS Pedi-FABS). 10 The HSS Pedi-FABS is an 8-item multiple-choice questionnaire validated in children aged 10 to 18 years that generates a score from 0 to 30 corresponding to how active the respondent was in the month prior. The questionnaire was further validated in 2014 through correlation with standardized physical fitness metrics in healthy adolescents, and normative data were published in 2018.11,12 However, literature assessing the use of an activity measure designed specifically for use in the pediatric athlete population remains sparse. Additionally, the score distribution of the HSS Pedi-FABS for different sports remains largely unknown and could add value to the current understanding of activity level in pediatric athletes.
The purpose of this study was to evaluate the validity of the HSS Pedi-FABS compared with the Tegner in a large population of pediatric athletes and to determine the distribution of scores across different sports.
Methods
Institutional review board approval was obtained before the initiation of this study.
Study Population
This study analyzed the completed medical records of 517 patients who initially came to a single pediatric sports medicine specialty clinic for evaluation of a knee complaint or injury between October 2016 and June 2017. Patients were included in the study if they were 10 to 18 years of age, completed the HSS Pedi-FABS, and had a reported status as an athlete at their baseline visit. Nonathletes were excluded from this study, as the focus was to obtain data across a pediatric population participating in sports.
Data Acquisition
All data reviewed were prospectively collected in a standardized manner using discrete data fields. Patient data were obtained by direct chart review of electronic medical records stored in EPIC. Data obtained included sex, age, race, and other information on patient characteristics. Patients prospectively self-reported their primary sport; hours per day, days per week, and weeks per year of participation in sports; and highest level of competition on standardized intake forms before being evaluated by a provider. Sports with similar functional and physical requirements were grouped, such as baseball, T-ball, and softball. The HSS Pedi-FABS and Tegner were administered on electronic tablets using Oberd, an electronic data collection system designed for physicians and hospitals (Universal Research Solutions, LLC). According to previous studies, PROMs administered on paper have been shown to be quantitatively comparable with measures administered on an electronic device.14,24 Likewise, the HSS Pedi-FABS shows high agreement between paper and electronic versions when using Oberd in this patient population. 27
Statistical Analysis
Means and standard deviations were used to describe continuous variables, such as HSS Pedi-FABS and Tegner scores, and a Student t test or analysis of variance with Tukey post hoc test was used to compare those variables. Transformations of variables were used to ensure that normality assumptions were satisfied. When necessary, a nonparametric test, such as a Mann-Whitney U test, was used. An evaluation of a floor or ceiling effect was performed and considered to be present if more than 15% of respondents scored the lowest or highest possible scores, respectively. 23 Terwee et al 35 explained that if 15% of respondents score the highest or lowest possible score, it is likely that extreme items are missing in the lower or upper end of the scale, indicating limited content validity. Last, Spearman correlation coefficient was used to assess the linear association between participation and scoring data. Statistical significance was set at P < .05.
Results
Patient Characteristics
Of the 517 patients reviewed, 119 did not fit the inclusion criteria. Of these, 36 were nonathletes, 52 had incomplete HSS Pedi-FABS results, 26 were outside the age range, and 5 were duplicate records. Of the 398 patients who fit the inclusion criteria, 215 (54.0%) were female and 183 (46.0%) were male. The average age of the population was 14.5 years (range, 10.0-18.8 years). A total of 193 (48.7%) patients reported involvement in multiple sports, and 203 (51.3%) reported involvement in a single sport (these data were not available for 2 patients). The most commonly reported primary sports were soccer and basketball (Table 1). No significant differences were found in mean HSS Pedi-FABS or Tegner scores by age, sex, or race.
Patient Characteristics a
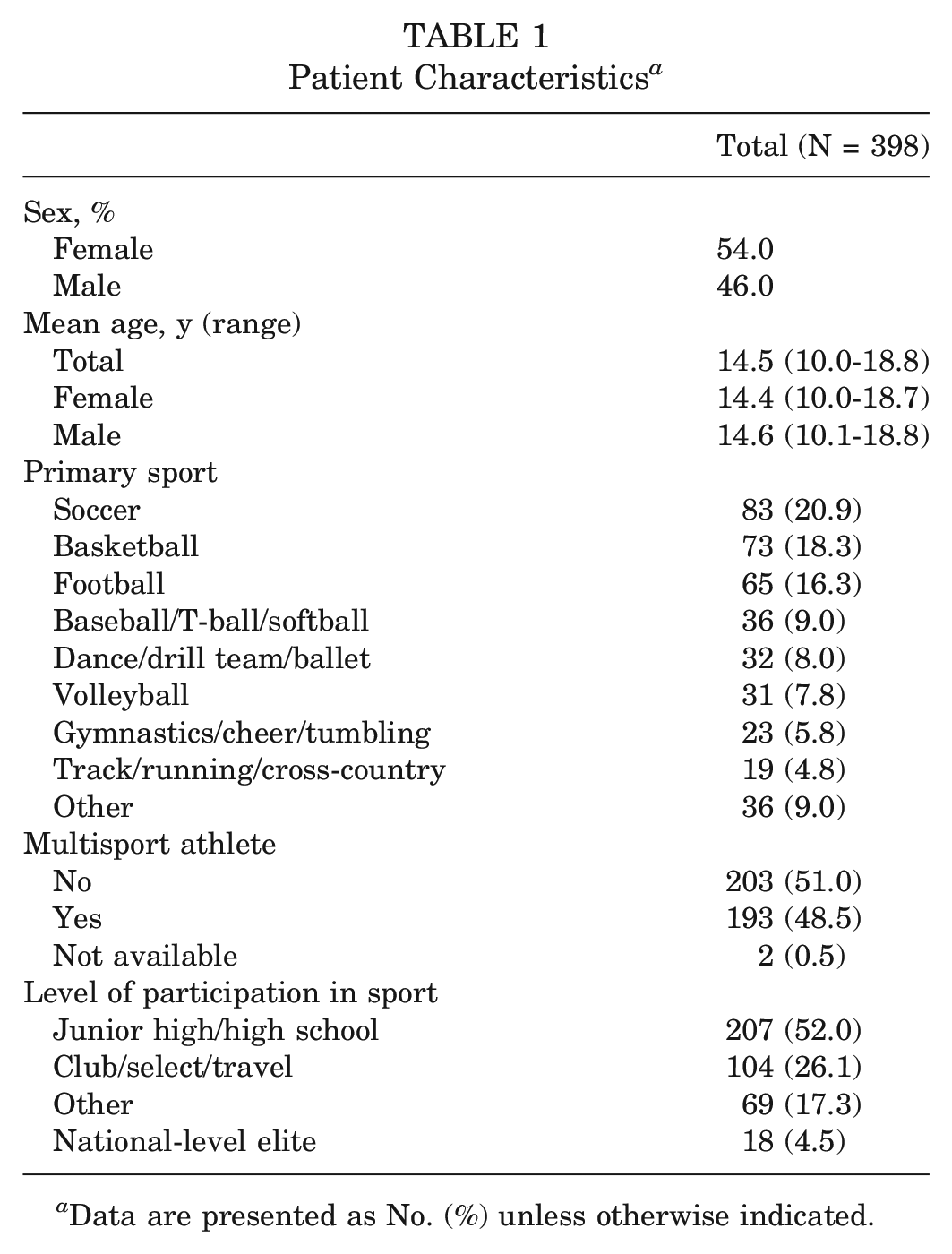
Data are presented as No. (%) unless otherwise indicated.
Validity of the HSS Pedi-FABS Compared With the Tegner
Significant correlations were found between the HSS Pedi-FABS score and patient-reported hours per week (r = 0.302; P < .001), days per week (r = 0.278; P < .001), and weeks per year (r = 0.136; P = .014) playing a primary sport. For the Tegner, a significant correlation was found only with days per week (r = 0.211; P = .001) (Table 2).
Spearman Correlation Between Reported Sport Participation and PROM Scores a
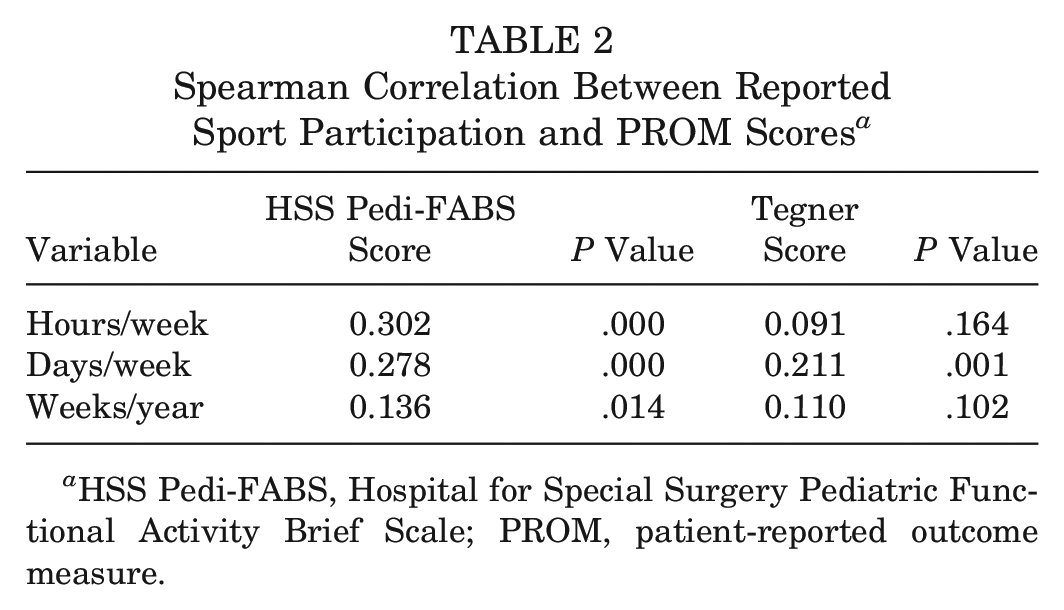
HSS Pedi-FABS, Hospital for Special Surgery Pediatric Functional Activity Brief Scale; PROM, patient-reported outcome measure.
According to self-reported level of competition, no differences were noted between the Tegner and level of competition. On the contrary, athletes who played at a club/select/travel level exhibited higher scores on the HSS Pedi-FABS than the junior high/high school–level athletes (23.8 vs 21.0; P = .004). However, when comparing scores for “national-level elite” athletes with the scores for athletes at the club/select/travel or junior high/high school, there was no significant difference in HSS Pedi-FABS scores or Tegner scores. On average, multisport athletes scored higher on the HSS Pedi-FABS than single-sport athletes (22.1 vs 20.4; P = .029), but no differences were seen in Tegner scores.
No correlation was found between the HSS Pedi-FABS and the Tegner (r = 0.088; P = .140). Further, it was noted that mean HSS Pedi-FABS scores were similar (range, 19.0-23.0) for each Tegner score >5, which is where the Tegner becomes entirely determined by participation in sport. In this pediatric athlete cohort, more than two-thirds of patients (72.8%) received either a 9 or 10 on the Tegner. No floor or ceiling effect was observed for HSS Pedi-FABS, but a ceiling effect was present for the Tegner (32.8% receiving the highest score) (Figure 1).
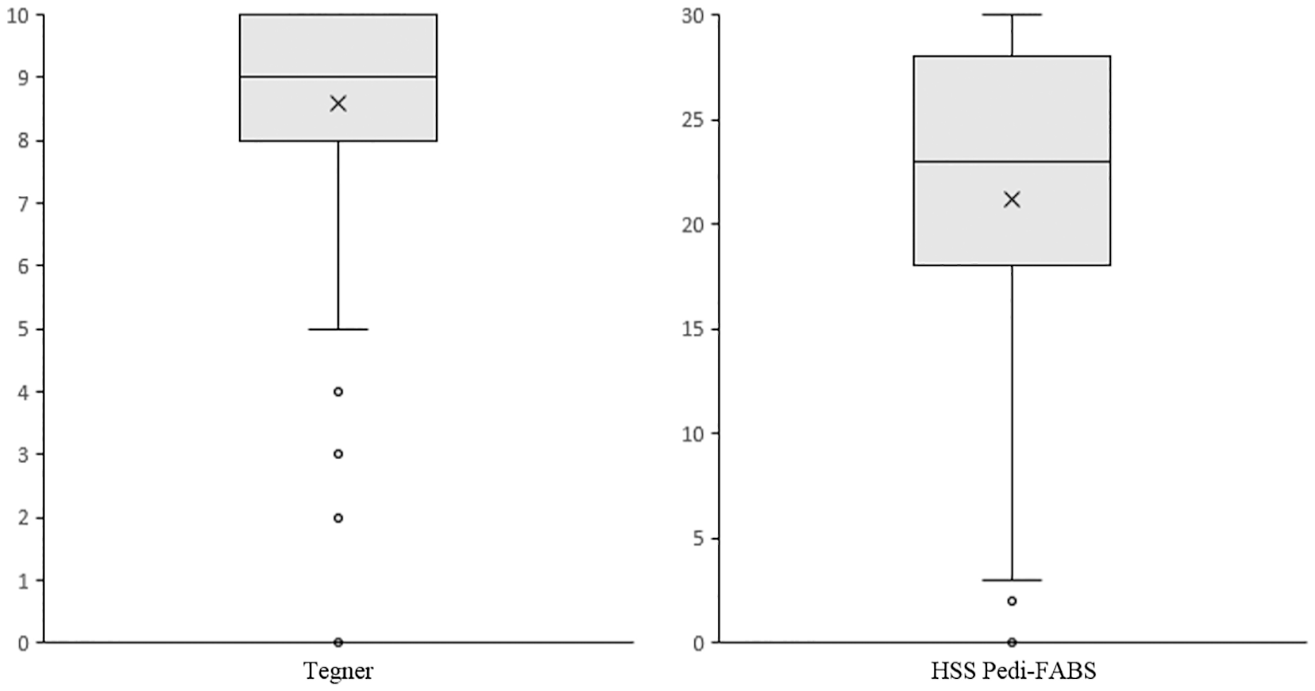
Box-and-whisker plots of the Tegner and Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) score distributions. Means are indicated with an X.
HSS Pedi-FABS Scores Across Common Sports
Of the 8 most commonly reported primary sports, soccer players scored the highest mean scores (23.5 ± 1.4) on the HSS Pedi-FABS. Dance/drill team/ballet (17.9 ± 2.1) and track and field/running/cross-country (17.5 ± 2.6) athletes had the lowest reported scores. The HSS Pedi-FABS showed a significant difference in mean scores across the 8 most common primary sports (P = .001). Participants whose primary sport was soccer scored significantly higher than those in dance/drill team/ballet (23.5 vs 17.9; P = .006) and track and field/running/cross-country (23.5 vs 17.5; P = .028). Additionally, there was a robust distribution of HSS Pedi-FABS scores for each common primary sport, with no floor or ceiling effect found in any individual sport. The distribution of scores varied from sport to sport (Figure 2).
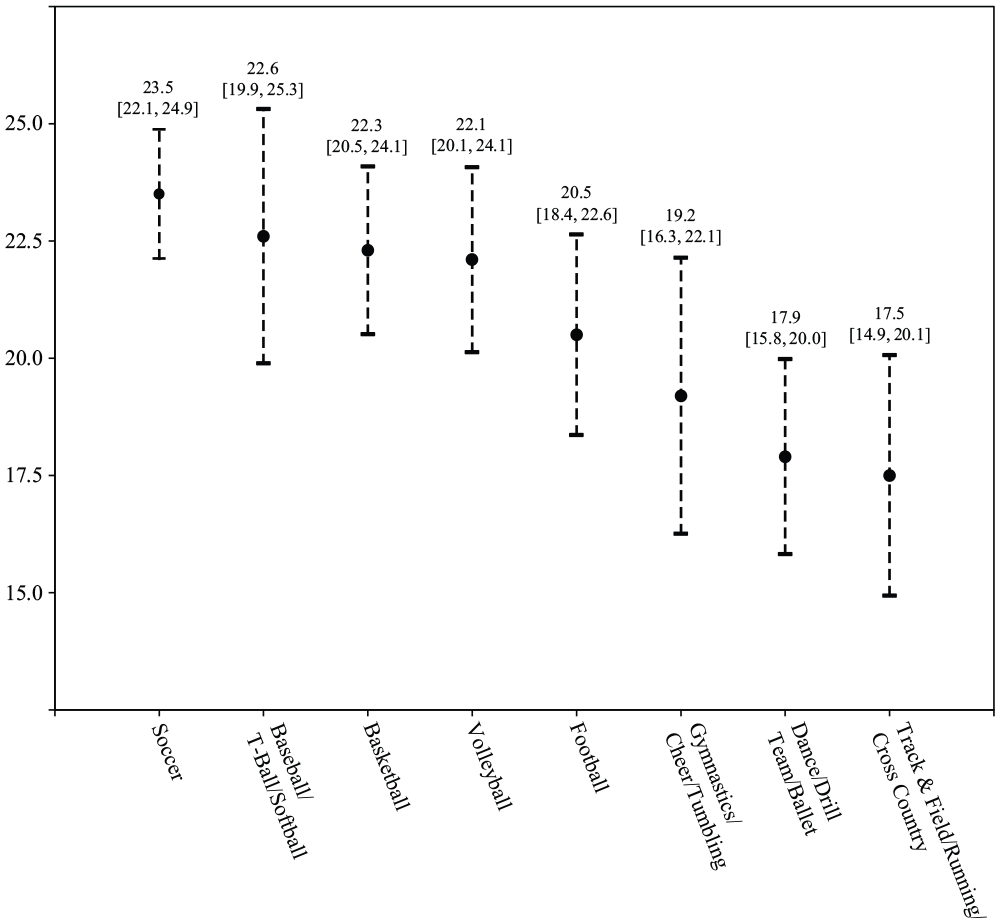
Graph displaying the means and 95% CIs of Hospital for Special Surgery Pediatric Functional Activity Brief Scale scores across the 8 most common primary sports.
Discussion
PROMs have been widely used and assessed in research over the past 4 decades. 20 PROMs can be used to measure how patients function or feel with respect to their health, quality of life, mental well-being, or health care experience. 19 Such measures are increasingly recognized as a primary means of assessing the success and effect of health care treatments.3,38 With the rise in youth sports participation, PROMs that measure activity level have become an important tool in sports medicine and research. However, many of the PROMs often used in pediatric orthopaedic publications were not developed for or extensively validated for use in children. 37 Our study revealed that the HSS Pedi-FABS, an activity measure developed for use in pediatric patients, is more valid in regard to frequency and level of activity than the Tegner, a measure designed for the adult population, when used in a large population of youth athletes.
As knee injuries are the most common sports injuries, patients presenting to the clinic for an evaluation of the knee were used in this study.8,22,33 The Tegner was first designed for use in adolescents and adults with knee injuries, but it has become commonly used to evaluate the treatment of knee injuries in pediatric populations. While the Tegner is used to accurately categorize activity in adults and adolescents, this study showed that it cannot effectively differentiate the activity level of pediatric athletes. Iversen et al 17 reported that 87% of children had difficulty distinguishing the various levels used in the Tegner, as various sports are repeated. For example, soccer and football are repeated in both Tegner level 9 and level 10; relying on the ability of the respondent to select a level with no provided directions yielded inconsistent results.
Almost three-fourths of the patient population in this study reported a 9 or 10 on the Tegner, with a third reporting a 10. This observed ceiling effect may be attributed to the fact that soccer and football were among the most commonly reported primary sports in the study population, but it may also be a result of the lack of clarity described by Iversen et al. Additionally, the Tegner demonstrated no correlation with reported level of competition. When using the Tegner, every competitive soccer and football player classifies as a 9 or 10, regardless of whether the athlete plays at a youth or collegiate level. The HSS Pedi-FABS, on the contrary, did not demonstrate a floor or ceiling effect and in general showed a correlation with level of competition. However, likely because of the low number included in the study, an increase in scores was not found for national-level elite athletes. Additionally, the HSS Pedi-FABS demonstrated greater correlation with reported time spent participating in sports than the Tegner, indicating its validity when used in a population of youth athletes. Whereas the Tegner relies most heavily on reported sport, the HSS Pedi-FABS relies on level and frequency of performing specific activities, as an activity measure should.
Sanders et al 28 reported that the style, level, and intensity of physical exertion for football players are dependent on a player’s position. Thus, as level and position may affect the physical demand of a sport, an activity measure used in a population of athletes must be able to account for such factors. Each sport demonstrated a wide distribution of HSS Pedi-FABS scores, indicating the utility of the scale for differentiation between various levels of activity, even in same-sport athletes. By design, the Tegner is unable to do this. However, the average HSS Pedi-FABS score and distribution of scores varied from sport to sport. For example, the distribution of scores in soccer is observed to be right shifted compared with the distribution of dance and track scores. This may be attributed to the HSS Pedi-FABS focusing on physical activity generally associated with field/court sports, such as cutting and pivoting. Thus, the HSS Pedi-FABS may not effectively address the activity level of highly competitive athletes who participate in sports such as track, dance, golf, gymnastics, and swimming. However, because of the clinical relevance of assessing running/cutting activity, especially in pediatric orthopaedic sports medicine, the design of the questionnaire remains useful.
The HSS Pedi-FABS was originally designed in 2013 with the intention of being a comprehensive and concise measure of activity for children and adolescents regardless of athletic activity or medical condition. 10 The newly designed questionnaire demonstrated internal consistency and test-retest reliability. Additionally, the measure provided a means to longitudinally assess activity level based on changes in a patient’s condition rather than changes in age or physique. Further, in 2014 Fabricant et al 11 demonstrated that scores on the HSS Pedi-FABS correlated with an aerobic endurance test and identified a cutoff score of 14 to classify youth at risk of poor aerobic capacity. Fabricant et al 12 further assessed the HSS Pedi-FABS in 2018 by conducting a nationwide survey of children aged 10 to 18 years to generate normative data for the activity measure. It was demonstrated that both athletes and nonathletes showed a relatively normal distribution of scores, with athletes showing higher scores in general. However, in the same paper in which Iversen et al 17 critiqued the design of the Tegner, it was also reported that 27% of respondents had difficulty distinguishing between “endurance” and “duration,” 2 important aspects of the HSS Pedi-FABS. Our study further supported the use of the activity measure in a population of youth athletes by finding positive correlations between patient scores and reported participation in sport, while also comparing the measure with the Tegner, a historically designed activity scale. Additionally, our study analyzed the distribution of HSS Pedi-FABS scores by an athlete’s primary sport, something that has not been reported in the literature.
A limitation of this study is its retrospective design. However, as the data used in the study were all prospectively collected and documented in a standardized manner, many limitations associated with a retrospective study were avoided. Additionally, as the population presented to a single specialty sports medicine clinic for an evaluation of the knee, the generalizability of the results may be limited. Last, there were limitations in identifying whether the participants in the study were actively in season in their respective primary sports. Future work using accelerometers to objectively measure the activity level of athletes in season will be helpful in further validating the use of the HSS Pedi-FABS in athletes.
Conclusion
The HSS Pedi-FABS demonstrated higher validity compared with the Tegner when used in a population of youth athletes. The HSS Pedi-FABS showed additional correlations with reported hours per week and weeks per year of participation in sport and demonstrated the ability to differentiate higher-level athletes from lower-level athletes. Additionally, while the Tegner demonstrates a notable ceiling effect in this patient population, no floor or ceiling effect was found with the HSS Pedi-FABS. Further, there was a robust distribution of HSS Pedi-FABS scores even among athletes of the same sport. When using an activity measure to evaluate outcomes of treatment, especially in sports-related injuries, using the HSS Pedi-FABS may provide a more comprehensive analysis of activity level than the Tegner.
Footnotes
Acknowledgements
The authors acknowledge Chan-Hee Jo, PhD, Texas Scottish Rite Hospital for Children, Dallas, TX, USA.
Submitted August 28, 2019; accepted December 4, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.L.W. has received education payments from Pylant Medical–Arthrex and royalties from Elsevier. H.B.E. has received hospitality payments from Arthrex and Smith & Nephew; compensation for services other than consulting from Smith & Nephew and Synthes GMBH; and royalties from Elsevier. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.