
Abstract
Background:
The relationship between the medial patellofemoral ligament (MPFL) and the distal femoral physis has been reported in multiple studies.
Purpose:
To determine the distance from the MPFL central origin on the distal femur to the medial distal femoral physis in skeletally immature participants.
Study Design:
Systematic review.
Methods:
A systematic review was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Multiple databases were searched for studies investigating the anatomic origin of the MPFL on the distal femur and its relationship to the medial distal femoral physis in skeletally immature participants. Study methodological quality was analyzed with the Anatomical Quality Assessment tool, with studies categorized as low risk, high risk, or unclear risk of bias. Continuous variable data were reported as mean ± SD. Categorical variable data were reported as frequency with percentage.
Results:
Seven articles were analyzed (298 femurs, 53.7% male patients; mean age, 11.7 ± 3.4 years). There was low risk of bias based on the Anatomical Quality Assessment tool. The distance from the MPFL origin to the distal femoral physis ranged from 3.7 mm proximal to the physis to 10.0 mm distal to the physis in individual studies. Six of 7 studies reported that the MPFL origin on the distal femur lies distal to the medial distal femoral physis in the majority of specimens. The MPFL originated distal to the medial distal femoral physis in 92.8% of participants at a mean distance of 6.9 ± 2.4 mm.
Conclusion:
The medial patellofemoral ligament originates distal to the medial distal femoral physis in the majority of cases at a mean proximal-to-distal distance of 7 mm distal to the physis. However, this is variable in the literature owing to study design and patient age and sex.
Patellar instability is a common injury, with an annual incidence of 5.8 per 100,000 in the total population. 10 This increases to 43 per 100,000 in children <16 years of age, with adolescent female athletes at the highest risk.10,26 Recurrent dislocations can be disabling for competitive athletes and lead to a failure of nonoperative management in up to 31% of cases.14,28 Risk factors for recurrent dislocations include female sex, family history of patellar instability, personal history of dislocation or subluxation, trochlear dysplasia, patella alta, and increased Q angle.3,14,17,19,27
The medial patellofemoral ligament (MPFL) is an important checkrein to lateral subluxation or dislocation of the patella. Although there are other dynamic and static stabilizers, the MPFL serves as the primary restraint during the first 30° of knee flexion and has been shown to contribute up to 60% of the resistance to lateral patellar translation.5,13 As such, injury to the MPFL can also lead to increased rates of recurrent patellar dislocations. 27 Anatomic MPFL reconstruction with or without bony realignment has become an increasingly common treatment option for recurrent patellar instability in patients after failed nonoperative treatment. Failure to place the femoral tunnel in an anatomic location can have negative consequences, with increased contact pressures in the patellofemoral joint.1,8 To guide this anatomic placement, Schӧttle et al 29 described the radiographic landmarks for the origin of the MPFL on the distal femur using lateral radiographs of skeletally mature patients.
The close proximity of the distal femoral physis to the MPFL origin can be problematic in skeletally immature patients owing to the complex physeal anatomy. 21 This has led to several studies investigating the relationship between the MPFL origin on the distal femur and the distal femoral physis. However, these studies are limited by small sample sizes and heterogeneous methods of measurement. The purpose of this systematic review was to determine the distance from the MPFL central origin on the distal femur to the medial distal femoral physis in skeletally immature patients. We hypothesized that the distance from the MPFL origin on the distal femur to the distal femoral physis would vary by method of measurement and by type of specimen.
Methods
This systematic review was registered with PROSPERO on August 11, 2019. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed. 22 We conducted separate searches of the following medical databases: PubMed, SCOPUS, and Cochrane Central Register of Controlled Trials. The searches were performed on August 11, 2019, by a single orthopaedic surgery sports medicine fellow (K.R.S.) and confirmed by the senior author (S.L.S.). The search terms used were “medial,”“patellofemoral,”“ligament,” and “physis” (medial[All Fields] AND patellofemoral[All Fields] AND (“ligaments”[MeSH Terms] OR “ligaments” ([All Fields] OR “ligament”[All Fields]) AND (“growth plate”[MeSH Terms] OR (“growth”[All Fields] AND “plate”[All Fields]) OR “growth plate”[All Fields] OR “physis”[All Fields])).
Eligible studies consisted of studies published in the English language that measured the proximal-distal distance of the MPFL origin on the distal femur to the distal femoral physis in skeletally immature participants. Clinical studies, review articles, book chapters, and technique papers were excluded. In the event of different studies with duplicate (or overlapping) populations, the study with greatest sample size or greatest clarity of methods and results was included if the participants could not be separated. All references within included studies were cross-referenced for inclusion if missed by the initial search. The search results were reviewed for duplicates, and the inclusion criteria to determine the articles that were included in the final analysis (Figure 1).
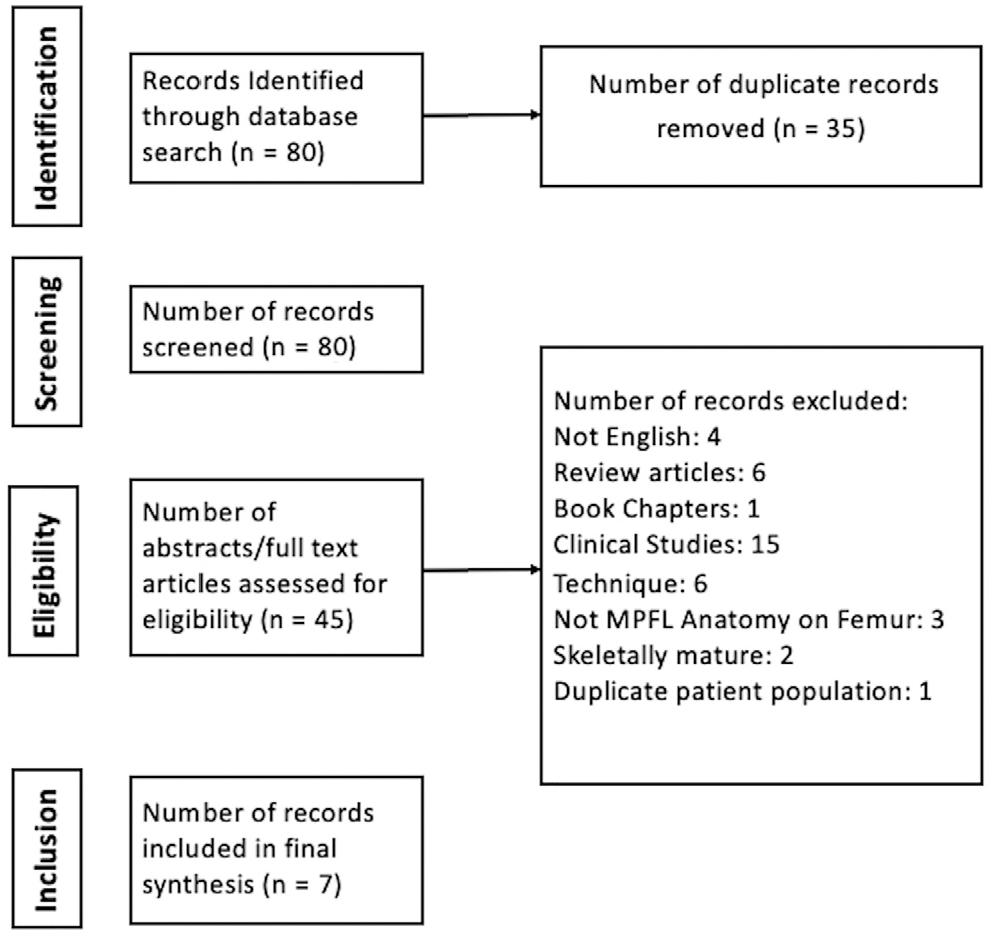
PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) flow diagram summarizing the literature search, screening, and review. MPFL, medial patellofemoral ligament.
Articles were reviewed, and data were extracted from the included studies with the methodology recommended by Harris et al. 12 All study, participant, and measurement parameters were recorded. Study and participant characteristics analyzed included year of publication, number of participants, number of femurs, age, sex, and laterality. Cadaveric and radiologic methods of measurement were recorded.
Study methodological quality was analyzed with the Anatomical Quality Assessment tool, with studies categorized as low risk, high risk, or unclear risk of bias. 15 Study heterogeneity precluded meta-analysis. Continuous variable data were reported as mean ± standard deviation. Categorical variable data were reported as frequency with percentage.
Results
Seven articles were analyzed (Table 1).2,9,11,23,30-32 According to the Anatomical Quality Assessment tool, all articles had low risk of bias. The number of femurs per study ranged from 6 to 159, for a total of 298 femurs. Three11,31,32 of 7 studies included more male than female patients (14% to 81% male). The mean ages ranged from 5.2 to 14.3 years (11.7 ± 3.4 years).
Study Characteristics a
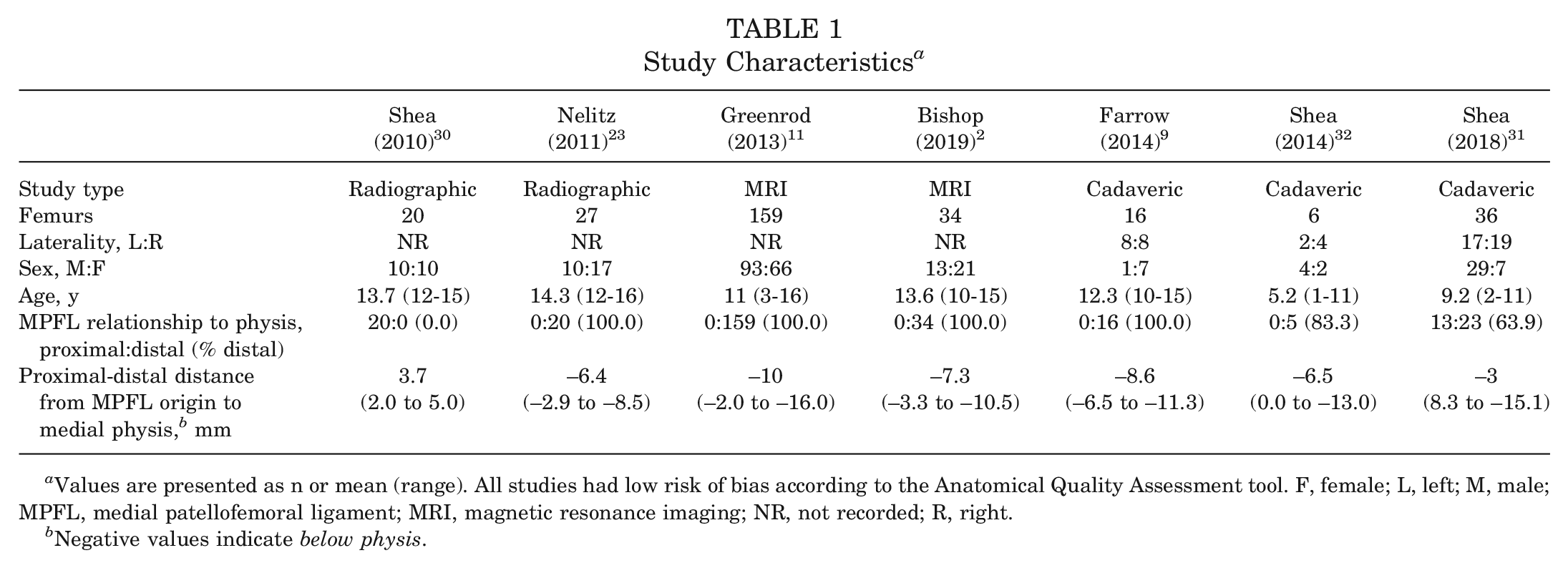
Values are presented as n or mean (range). All studies had low risk of bias according to the Anatomical Quality Assessment tool. F, female; L, left; M, male; MPFL, medial patellofemoral ligament; MRI, magnetic resonance imaging; NR, not recorded; R, right.
Negative values indicate below physis.
Two studies used digital radiographs of the knee to measure the distance from a point as described by Schӧttle et al 29 to the distal femoral physis. Shea et al 30 studied only lateral radiographs, while Nelitz et al 23 utilized lateral and anteroposterior (AP) radiographs of the knee to control for the undulating nature of the distal femoral physis. Two studies reviewed magnetic resonance imaging (MRI) of the knee to determine the origin of the MPFL. Greenrod et al 11 identified the MPFL origin on axial imaging and then cross-referenced this axial position with coronal images to measure the distance to the medial distal femoral physis. Bishop et al 2 identified the Schӧttle point on sagittal imaging of the notch and then extrapolated this point to the most medial sagittal slice on MRI showing the medial distal femoral physis.
One study utilized preserved cadaveric specimens of the distal femur for determining the distance from the MPFL origin to the distal femoral physis. In this study, Farrow et al 9 identified the MPFL origin in the sulcus between the adductor tubercle and medial epicondyle and used digital calipers to measure the distance to the medial distal femoral physis. In 2 studies by Shea et al,31,32 the MPFL origin was identified through cadaveric dissection of skeletally immature specimens. The specimens then underwent computed tomography scans to determine the distance from the midpoint of the MPFL origin to the medial distal femoral physis on coronal imaging.
The distance from the MPFL origin to the distal femoral physis ranged from 3.7 mm proximal to the physis to 10.0 mm distal to the physis in individual studies (Figure 2). Six of 7 studies reported that the MPFL origin on the distal femur lies distal to the medial distal femoral physis in the majority of specimens (range, 63.9%-100%) (Table 1).2,9,11,23,31,32 Overall, in these studies, the MPFL originated distal to the medial distal femoral physis in 92.8% of participants at a mean distance of 6.9 ± 2.4 mm.
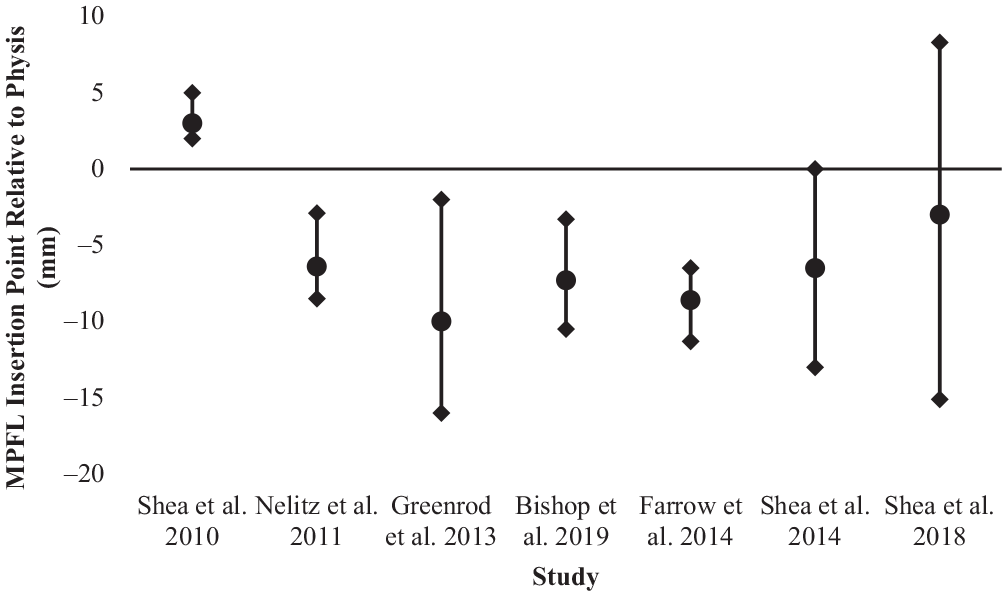
Medial patellofemoral ligament (MPFL) origin on the femur in relation to the distal femoral physis. Horizontal line represents the level of the physis. Below axis is distal to physis. Values are presented as mean ± SD.
The study by Farrow et al 9 investigated the mediolateral distance between the MPFL origin on the distal femoral cortex and the point where the distal femoral physis becomes distal to the MPFL origin. This study found that the distal femoral physis becomes distal to the MPFL origin at a point 10.5 mm lateral to the MPFL origin on the distal femoral cortex.
Four studies investigated the relationship between age and the MPFL origin on the distal femur.2,11,31,32 In 2 studies, Shea et al31,32 found that the origin of the MPFL was more proximal and closer to the physis as the patient ages. In contrast, Greenrod et al 11 found that the MPFL origin was more distal and farther from the physis as patients aged. Using a multivariable regression model, Bishop et al 2 demonstrated that age was not an independent predictor of the distance between the physis and MPFL origin. However, the MPFL origin was closer to the physis in female patients, with the entire sample still maintaining an MPFL origin that was distal to the physis.
Discussion
This systematic review summarizes anatomic descriptions of the MPFL origin on the distal femur and its relationship to the medial distal femoral physis. It was determined that the MPFL originates distal to the medial distal femoral physis in 92.8% of participants at a mean distance of 6.9 ± 2.4 mm. This study partially confirmed our hypotheses.
In terms of the modality for measuring the distance from the MPFL origin to the distal femoral physis, 4 studies2,11,23,30 utilized only imaging; 2 studies31,32 used cadaveric dissection and imaging; and 1 study 9 used only cadaveric specimens. Despite the varied methods of measurement, 6 of 7 studies found that the MPFL originated distal to the medial distal femoral physis in the majority of participants (92.8%).2,9,11,23,31,32 Shea et al 30 determined that the MPFL origin was proximal to the physis in 100% of their participants based on the method of Schӧttle et al 29 on lateral radiograph. Shea et al 30 correctly identified the Schӧttle point on the lateral radiograph. However, they were unable to account for the complex anatomy of the distal femoral physis in their measurements as the lateral radiograph shows only the central portion of the physis and not the convex medial aspect of the physis nearest the MPFL origin. 21 Had Shea et al also utilized an AP radiograph, they would have identified the MPFL origin distal to the distal femoral physis. This illustrates the importance of assessing the femoral MPFL tunnel starting point in the AP and lateral radiographic views during anatomic MPFL reconstruction to avoid physeal injury.
Huston et al 16 evaluated the method of Schӧttle et al 29 in pediatric patients and found it to be reproducible, with a small intraobserver variance. Although reliable in determining the MPFL origin intraoperatively, it is not a reliable method of measurement to determine the distance of the MPFL origin to the physis and should be used with caution in skeletally immature patients. Nelitz et al 23 were able to correct and control for the undulating nature of the distal femoral physis using a combination of lateral and AP radiographs of the knee. This allowed for a more accurate measurement and better understanding of the 3-dimensional nature of the distal femoral physis.
By excluding the study by Shea et al, 30 the mean distance from the medial distal femoral physis to the MPFL origin was 6.9 ± 2.4 mm distal. Despite the variations in methods of measurement (cadaveric, radiographic, MRI), these 6 studies all had similar distances from the physis.2,9,11,23,31,32 Additionally, Shea et al31-33 have since published several studies in support of the MPFL origin located distal to the medial distal femoral physis using a combination of computed tomography and cadaveric dissection. As such, it is our opinion that when an anatomic MPFL reconstruction is performed, the starting point for the femoral tunnel should lie distal to the physis.
Farrow et al 9 were only ones to investigate the mediolateral distance between the MPFL origin on the distal femoral cortex and the point where the distal femoral physis becomes distal to the MPFL origin. They found that the distal femoral physis becomes distal to the MPFL origin at a point 10.5 mm lateral to the MPFL origin on the distal femoral cortex. This also has important surgical implications when the femoral tunnel is drilled, as a direct lateral tunnel >10 mm would likely result in physeal injury. Greenrod et al 11 found similar results, with 64% of the patients sustaining physeal injuries if a 20 mm–length tunnel was drilled directly lateral starting at the MPFL origin on the distal femur. By starting the tunnel at the MPFL origin and directing it distally and anterior, one would be able to avoid physeal injury in most patients. This was confirmed by Greenrod et al, with only a 2% incidence of physeal injury when the tunnel was directed distally at 45° using a 20 mm–length tunnel. It is important to note, however, that this should be done with fluoroscopy, as the angulation and maximum tunnel length will vary by age and overall size of the epiphysis in each patient.
Several studies have investigated the relationship between age and the MPFL origin on the distal femur, with varied results.2,11,31,32 Two cadaveric dissection studies included in the review demonstrated that the origin of the MPFL was more proximal and closer to the physis as the patient ages.31,32 In contrast, Greenrod et al 11 found that the MPFL origin was more distal and farther from the physis as patients aged, and Bishop et al 2 found no relationship between age and MPFL origin. Unfortunately, neither cadaveric dissection nor imaging-based measurements have been shown to be superior, with both techniques having advantages and disadvantages over the other. As such, this should be a topic of future anatomic research.
Other studies, not included in the review owing to the inclusion of skeletally mature participants, had similar conflicting results. A retrospective review of pediatric patients using MRI by Edmonds et al 7 found that children >7 years old had an MPFL origin that was at or above the level of distal femoral physis. A later study by the same author compared the MRI of patients with and without patellar instability and found there to be no association between age and MPFL origin. 6 However, the authors did demonstrate that those with patellar instability had a more proximal MPFL origin, leading them to conclude that placement of the femoral tunnel distal to the physis may lead to a more stable MPFL reconstruction than proximally based reconstructions. This leads us to conclude that the varied measurements reported in the literature are likely due to individual anatomic differences as opposed to measurement technique.
Thorough understanding of the distal femoral anatomy in skeletally immature patients is necessary to avoid physeal injury during MPFL reconstruction. Intraoperatively, a combination of surface anatomy, ligament isometry, and radiographic views are used to determine the anatomic location of the femoral MPFL tunnel starting point. The anatomic MPFL origin is found through palpation of the sulcus between the adductor tubercle and medial epicondyle or through identification of the patulous native MPFL as it inserts on the femur. The lateral radiograph then allows for confirmation of this location as the Schӧttle point, and an AP view verifies that the starting point and tunnel trajectory remain distal to the physis. 24
Before femoral tunnel drilling, isometry of the MPFL can be used as a final check to ensure anatomic reconstruction of the MPFL. Isometry is perhaps one of the most important biomechanical features of the MPFL. An inaccurate femoral starting point would likely result in a graft that becomes too tight in flexion with resultant decreased knee range of motion. Additionally, as the patient ages, the MPFL origin may move proximally or distally, resulting in further loss of isometry. In consideration of this, it is generally accepted that with anatomic MPFL reconstructions, the MPFL is tighter in 0° to 30° of knee flexion and then relaxes in greater flexion angles to not overconstrain the patella in the trochlea. However, this has not been adequately studied in pediatric populations.
It is worth noting that there are other, nonanatomic techniques for MPFL reconstruction that are physeal sparing. Several techniques have been described where the MPFL is reconstructed with a soft tissue pulley around the medial collateral ligament or adductor magnus tendon.4,18,20 These studies reported a relatively high rate of recurrent patellar instability, with 11 of 35 patients (31.4%) reporting subluxation or dislocation after surgery at short-term follow-up. This is compared with the studies by Nelitz et al,24,25 where there were no cases of recurrent instability (0 of 46; 0.0%) or physeal injury from anatomic MPFL reconstructions. As such, it is our recommendation that anatomic physeal-sparing MPFL reconstruction be performed. However, in cases where physeal injury cannot be avoided, then nonanatomic reconstructions should be considered an alternative fixation strategy.
There are limitations noted among the studies included in this review. The design resulted in analysis of relatively few studies (7 studies) with a limited number of subjects (298 femurs). There was heterogeneity among the participants and methods for measuring the distance from the MPFL origin to the distal femoral physis. This prevented a meta-analysis and limits the strength of the conclusions. The methodological quality of studies as assessed by the Anatomical Quality Assessment tool demonstrated low risk for bias; however, the risk was not zero. We minimized this as much as possible with strict study eligibility and inclusion criteria. However, these limitations reflect the underlying limitations of the literature on this topic. Additionally, clinical studies were excluded, limiting this review to only anatomic studies without analysis of the clinical implications of nonanatomic versus anatomic MPFL reconstruction. Another possible limitation of this review is that other relevant studies on this topic could have been excluded, despite conducting a systematic search.
In conclusion, the MPFL originates distal to the medial distal femoral physis in the majority of participants at a mean proximal-to-distal distance of 7 mm distal to the physis. However, this is variable in the literature owing to study design and patient age and sex.
Footnotes
Submitted September 17, 2019; accepted December 12, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.G.S. has received education and hospitality payments from Arthrex, grants from Sanofi-Aventis, and speaker fees from DePuy Orthopaedics. M.R.S. has received intellectual property royalties from DJ Orthopaedics, Smith & Nephew, and Stryker; has received consulting fees from Medacta, Anika Therapeutics, Smith & Nephew, and Linvatec; has received speaking fees from Medacta, Smith & Nephew, and Linvatec; has received education payments from Biomet Sports Medicine; and holds stock or stock options from Biomimedica. G.D.A. has received consulting fees from Cytonics Inc, Fidia Pharma, RobiconMD, and Sideline Sports Doc; has received other financial and material support from Arthrex Inc and Stryker; and holds stock or stock options from Cytonics Inc. J.D. holds stock or stock options in Stabilynx. S.L.S. has received consulting fees and research support from Arthrex Inc; is a paid consultant for Ceterix Orthopaedics, CONMED Linvatec, Flexion Therapeutics, GLG Consulting, JRF Ortho, Moximed, Olympus, Vericel, Linvatec, and RTI Surgical; has received hospitality payments from Linvatec and Smith & Nephew; and has received a grant (indirect) from DJO. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.