
Abstract
Background:
Anterior cruciate ligament (ACL) repair has once again become a focus of research because of the development of new techniques.
Purpose/Hypothesis:
The purpose was to compare the functional results and recurrent instability rates in patients undergoing ACL repair with dynamic intraligamentary stabilization (DIS) versus primary ACL reconstruction (ACLR) for acute isolated ACL tears. The hypothesis was that functional results and knee joint stability after ACL repair with DIS would be comparable with that after ACLR.
Study Design:
Randomized clinical trial; Level of evidence, 1.
Methods:
A total of 85 patients with acute ACL tears were randomized to undergo either ACL repair with DIS or primary ACLR. The preinjury activity level and function were recorded. Follow-up examinations were performed at 6 weeks and 6, 12, and 24 months postoperatively. Anterior tibial translation (ATT) was evaluated using Rolimeter testing. The Tegner activity scale, International Knee Documentation Committee (IKDC) subjective form, and Lysholm knee scoring scale scores were obtained. Clinical failure was defined as ΔATT >3 mm in combination with subjective instability. Recurrent instability and other complications were recorded.
Results:
There were 83 patients (97.6%) who were successfully followed until 2 years. ATT was significantly increased in the DIS group compared with the ACLR group (ΔATT, 1.9 vs 0.9 mm, respectively; P = .0086). A total of 7 patients (16.3%) in the DIS group had clinical failure and underwent single-stage revision. In the ACLR group, 5 patients (12.5%) had failure of the reconstruction procedure; 4 of these patients required 2-stage revision. The difference in the failure rate was not significant (P = .432). There were 4 patients (3 in the DIS group and 1 in the ACLR group) who showed increased laxity (ΔATT >3 mm) without subjective instability and did not require revision. Recurrent instability was associated with young age (<25 years) and high Tegner scores (>6) in both groups. No significant differences between ACL repair with DIS and ACLR were found for the Tegner, IKDC, and Lysholm scores at any time.
Conclusion:
Whereas ATT measured by Rolimeter testing was significantly increased after ACL repair with DIS, clinical failure was similar to that after ACLR. In addition, functional results after ACL repair with DIS for acute tears were comparable with those after ACLR. The current study supports the use of ACL repair with DIS as an option to treat acute ACL tears.
Registration:
DRKS00015466 (German Clinical Trials Register)
Keywords
Since the early history of the surgical treatment of anterior cruciate ligament (ACL) tears, many efforts have been made to restore knee joint kinematics with ACL repair. However, the results of early repair techniques were not convincing. 28 In 1976, Feagin and Curl 12 reported unsatisfying results after ACL repair. Of 64 patients (all cadets at the United States Military Academy), 32 could be re-evaluated in a 5-year follow-up study. Only 22 of them could return to unrestricted duty, and more than 90% reported persistent subjective instability at the final follow-up. These poor results led to a paradigm change toward ACL reconstruction (ACLR), which is now considered the “gold standard” for treating ACL tears. However, with the recent development of new techniques, ACL repair has once again become a focus for both experimental and clinical research.1,7,9,17,22,38 In addition to ACL repair using suture anchors and the more rigid ligament bracing method, dynamic intraligamentary stabilization (DIS) has been introduced as a new technique to repair a torn ACL and restore knee joint kinematics after an acute ACL tear. 9 Similar to older techniques, the ACL is reattached to the femoral insertion site. In addition, an ultrastrong nonresorbable cord is placed along the ACL and attached to a dynamic spring fixed in the proximal tibia. With this mechanism, the tibia is maintained in a posterior drawer position through full range of motion, allowing the torn ACL to heal. A recent review comprising all studies published on the DIS technique to date demonstrated promising results with sufficient healing of the ACL. 2 Other techniques that can be used to repair a torn ACL (ie, anchor fixation with or without ligament bracing) have been described recently in small case series and nonrandomized studies.1,7,20 However, prospective comparative studies with ACLR are lacking, and the level of evidence to support the use of these new ACL repair techniques is still low.
The purpose of the present study was to compare the functional results and recurrent instability rates in patients undergoing ACL repair with DIS versus primary ACLR for acute isolated ACL tears. We hypothesized that the (1) functional results and (2) knee joint stability after ACL repair with DIS would be comparable with those after ACLR.
Methods
Between April 2014 and December 2015, there were 102 patients who were screened for eligibility to participate in the study. Patients with concomitant lesions that would alter the postoperative rehabilitation program (ie, meniscal tears that required repair and collateral ligament injuries) were excluded. Similarly, patients with previous knee injuries on either the affected or contralateral knee were excluded. Finally, a total of 85 patients (mean age, 28 years [range, 18-46 years]) with an acute (<3 weeks) isolated ACL tear were included in this study (Figure 1).
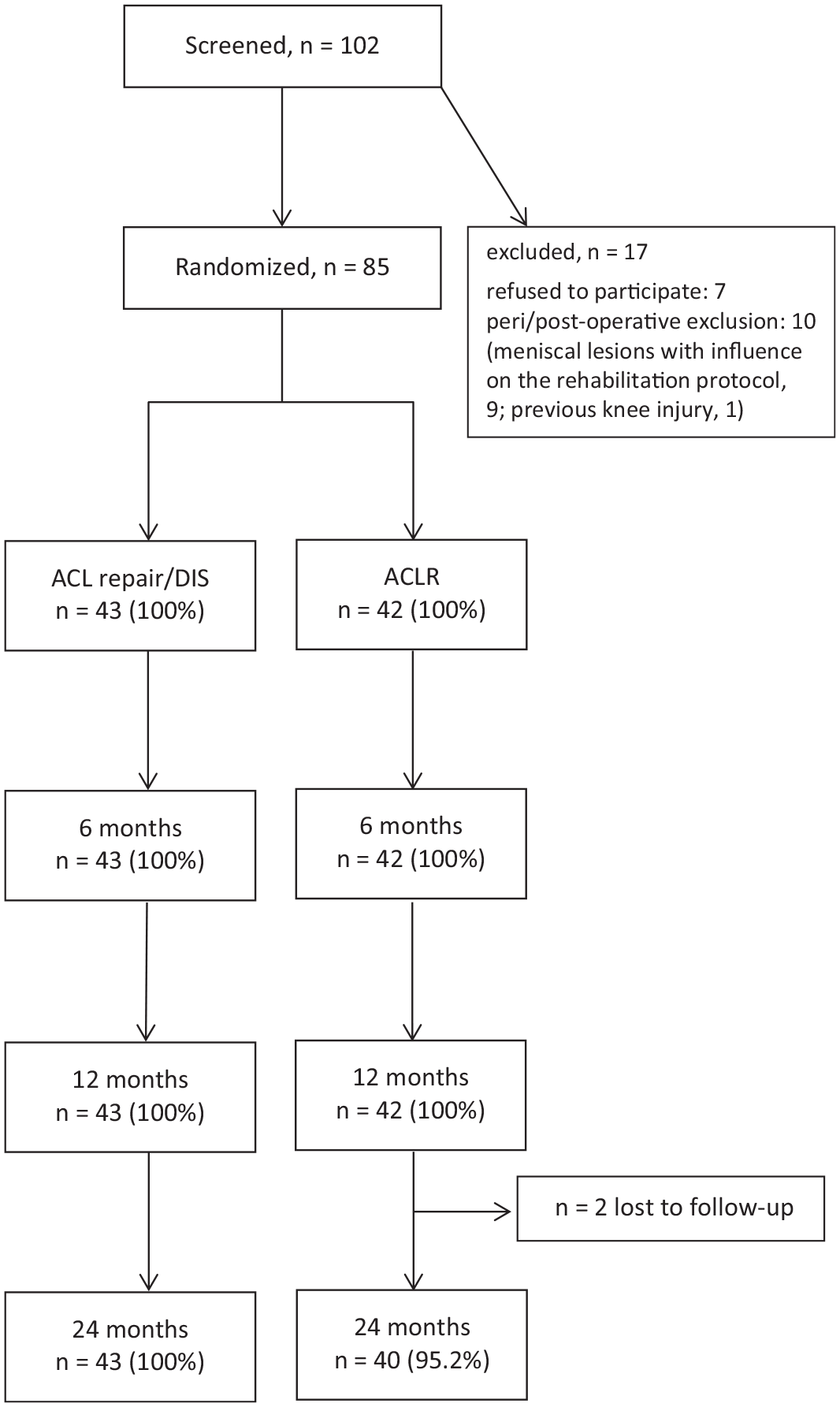
Diagram of grouping and patient flow. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; DIS, dynamic intraligamentary stabilization.
A block randomization (n = 4 per block) protocol was used to assign patients to undergo either DIS (Ligamys; Mathys Medical) (n = 43) or ACLR with a semitendinosus tendon autograft (n = 42). Table 1 shows the descriptive data for the 2 groups. In the operating theater, an assistant who was not involved in the study opened a sealed envelope immediately before surgery that contained the treatment group allocation for that patient.
Descriptive Data a
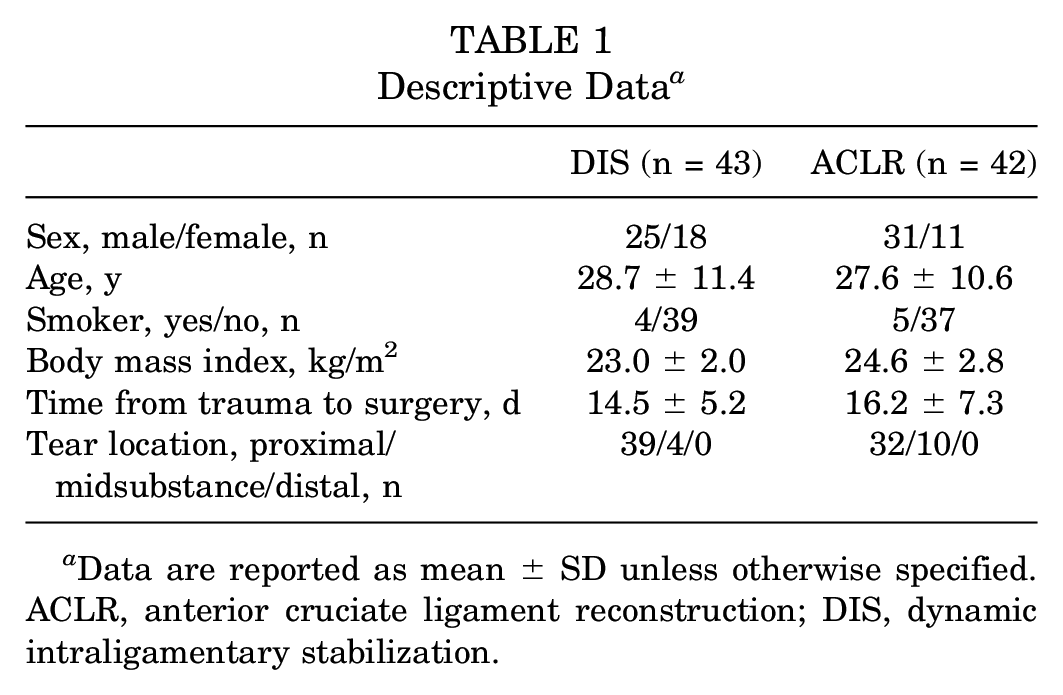
Data are reported as mean ± SD unless otherwise specified. ACLR, anterior cruciate ligament reconstruction; DIS, dynamic intraligamentary stabilization.
Surgical Technique and Rehabilitation
The operative procedures were performed at a single orthopaedic center by 4 of the study authors (C.K., M.H., M.J.R., B.S.), who were all experienced in ACLR. DIS was performed according to the technique described by Kӧsters et al. 24 Standard lateral and anteromedial portals were used. First, the ACL stump was evaluated for suitability of repair. In this cohort, all ACL tears were found to be repairable. A total of four 2.0 polyester sutures were then passed through the stump. Subsequently, with a standard 60° tibial aiming device, a K-wire was placed just at the posterior edge of the tibial footprint. The wire was overdrilled, and the tibial monobloc was implanted. Care was taken to preserve 2 cm of bone between the joint line and implant. The sutures of the ACL stump were shuttled through a 2.3-mm drill hole at the femoral insertion side. A braided cord containing the femoral button was then shuttled through the joint in a retrograde fashion and fixed to the tibial monobloc with a pretension of 80 N close to full knee extension. The joint was evaluated from extension to flexion to verify proper motion of the spring that was integrated in the monobloc. All but 4 tears were located proximal, close to the femoral insertion side, whereas 4 tears were located in the midsubstance. However, the stumps were closely adapted after repair, so the decision was made to perform DIS anyway. Figure 2 illustrates the DIS procedure.
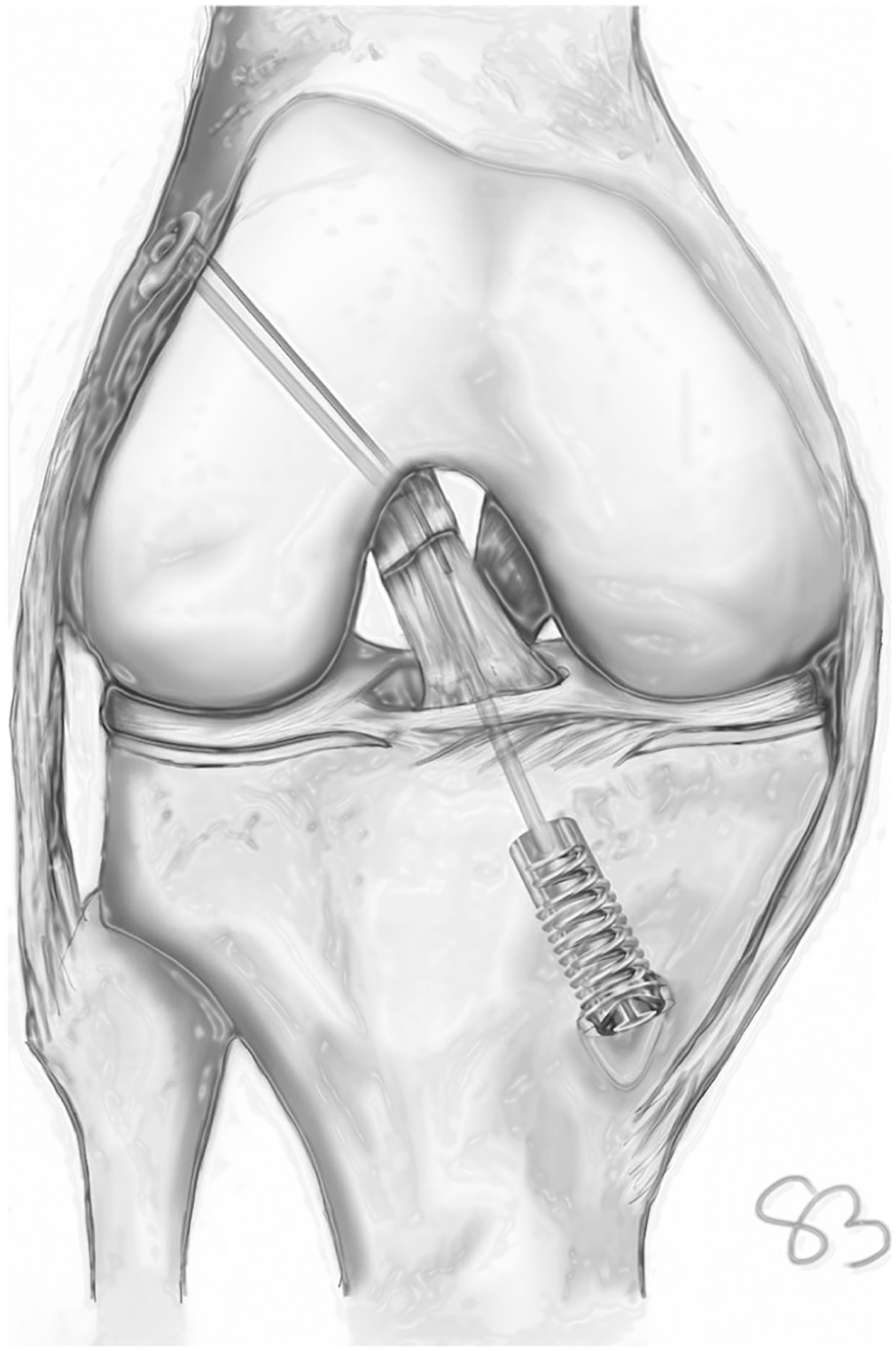
Schematic drawing of the dynamic intraligamentary stabilization procedure. Modified according to Schliemann B, Lenschow S, Domnick C, et al. 38
Anatomic single-bundle ACLR was performed using a 4-stranded semitendinosus tendon autograft. 35 The torn ACL was removed with only 2 to 3 mm of remnant tissue left on the tibial insertion side for orientation during tibial drilling. The graft diameter varied between 7.5 and 9.5 mm depending on the patient’s constitution. Debridement or partial resection of small meniscal lesions was performed in 12 patients in the DIS group and 6 patients in the ACLR group. Because these lesions did not alter the postoperative rehabilitation program, those patients were not excluded. No intraoperative complications were encountered in either group.
To exclude an outcome bias, the rehabilitation protocol was equal in both groups. For 5 days after either intervention, the affected knee was immobilized in a brace in extension, then a brace-free rehabilitation program was initiated. Full weightbearing was allowed after a 2-week period of partial weightbearing with 20 kg if the patient was pain-free. No restriction was placed on knee range of motion. Quadriceps and hamstring strength training was started with closed kinetic chain knee exercises. Proprioceptive exercises were introduced 4 weeks after surgery. Pivoting and competitive sports were allowed after a minimum of 6 months, but the decision was made individually in every patient.
Follow-up Examinations
A blinded observer (J.G.) conducted the follow-up examinations at 6 weeks and 6, 12, and 24 months after the procedure. Validated measurement tools were used to assess objective and subjective outcomes. At every follow-up examination, range of motion was assessed with a goniometer. The Tegner activity scale (range, 0 [low activity level] to 10 [very high activity level]), International Knee Documentation Committee (IKDC) subjective form (range, 0 [worst] to 100 [best]), and Lysholm knee scoring scale (range, 0 [worst] to 100 [best]) scores were obtained.
Rolimeter (Aircast) testing was performed with the knee in 30° of flexion to assess anterior tibial translation (ATT) at 6, 12, and 24 months.
Adverse events during the follow-up period were recorded. Clinical failure was defined as ΔATT of >3 mm (when comparing the affected knee with the contralateral side) in combination with a subjective feeling of instability (“giving way”). Patients with recurrent instability were excluded from further follow-up examinations.
Approval was obtained before the study from the local institutional review board (2013-414-f-S), and the study was registered on the WHO International Clinical Trials Registry Platform (DRKS 15466).
Statistical Analysis
A power analysis performed before the study resulted in the necessity of enrolling 28 patients per group based on an expected mean difference in ATT of 3 mm (regarded as clinically significant), a standard deviation of 2 mm, and an estimated loss to follow-up of 15% (α = .05; β = 0.8). The difference in ATT measured with the Lachman/Rolimeter test was chosen for the power analysis because of its high sensitivity and diagnostic accuracy.26,31
Differences in results between the different follow-up examinations within 1 group were analyzed with the Friedman test. The Mann-Whitney U test was used to evaluate differences between the 2 intervention groups. In the event of multiple testing, the Bonferroni correction was used to adjust the level of significance.
Results
Of the 85 patients who were initially randomized, 83 were successfully observed for 2 years. There were 2 patients in the ACLR group who were lost to follow-up between 12 and 24 months and could not be reached either by mail or telephone. Thus, the overall follow-up rate was 97.6%.
Anterior Tibial Translation
The mean difference in ATT between the injured and contralateral knees (ΔATT) was 6.7 ± 3.8 mm in the DIS group and 8.0 ± 1.7 mm in the ACLR group before the intervention. At the 24-month follow-up, this difference decreased to 1.9 ± 1.5 mm in the DIS group and 0.9 ± 1.1 mm in the ACLR group. A statistically significant difference in ΔATT was found between the DIS and ACLR groups (P = .0086) in favor of the ACLR group. All patients without recurrent instability had a negative pivot-shift test finding.
Functional Results
The mean Tegner score before the injury was 6 (range, 4-10) in both groups, indicating similar baseline activity. The Tegner, Lysholm, and IKDC scores over the follow-up period are illustrated in Figures 3 to 5. Compared with preinjury values, a significant drop occurred at the 6-week follow-up (DIS: Tegner, not significant; Lysholm, P≤ .0001; IKDC, P < .0001) (ACLR: Tegner, P = .0113; Lysholm, P < .0001; IKDC, P < .0001). Knee function recovered continuously until 24 months postoperatively. In both groups, all scores at the 24-month follow-up were still significantly worse than the preinjury values, indicating that normal knee function was not restored with either DIS or ACLR. However, no significant differences were found between the groups at any time during the follow-up period (24-month follow-up: Tegner, P = .8815; IKDC, P = .3783; Lysholm, P = .1459).
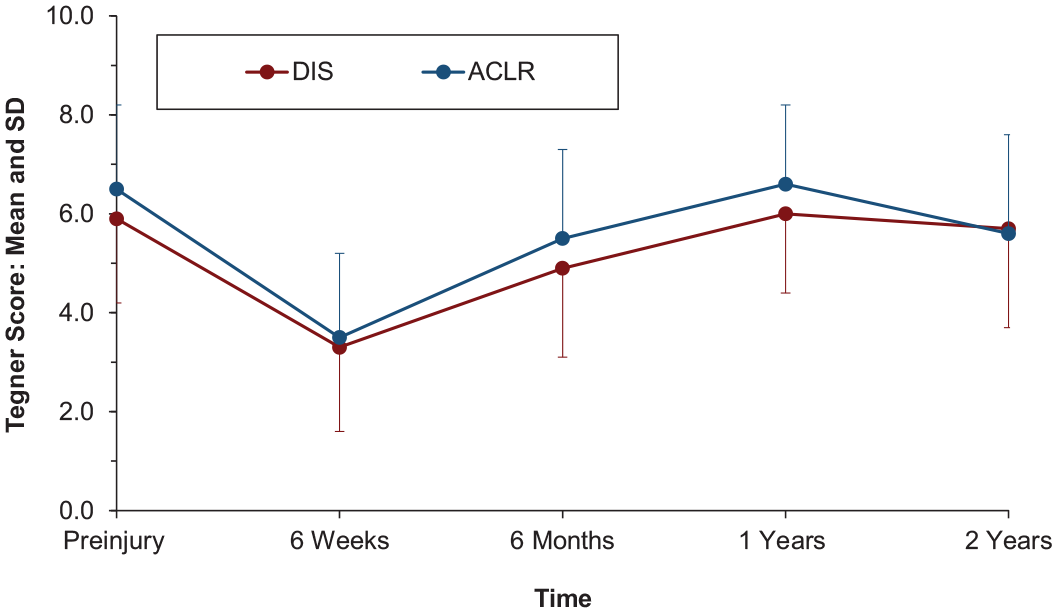
Tegner scores at the different follow-up examinations. ACLR, anterior cruciate ligament reconstruction; DIS, dynamic intraligamentary stabilization.
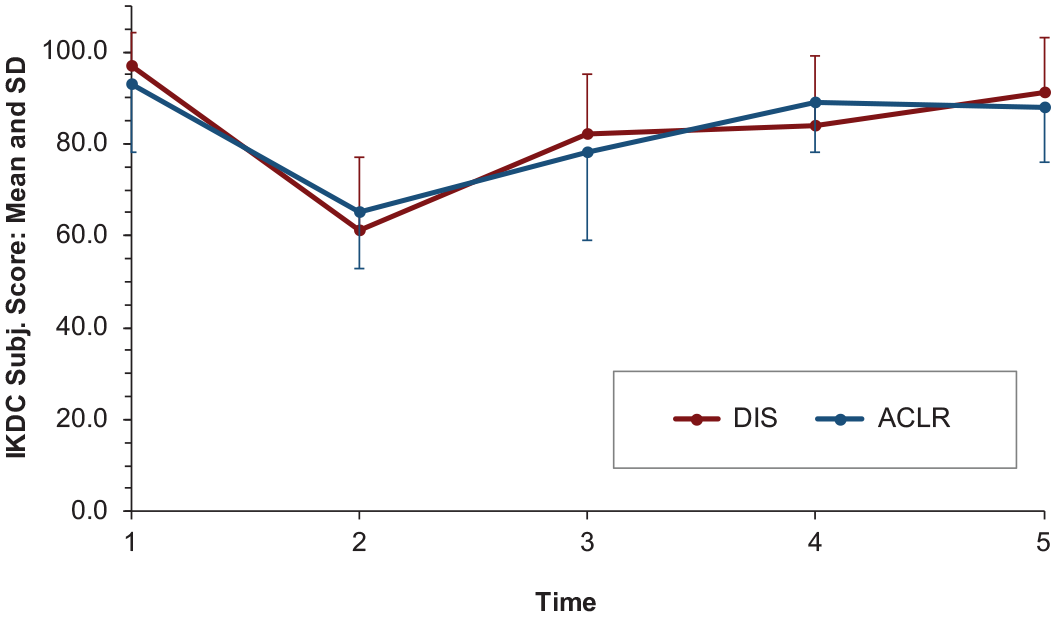
International Knee Documentation Committee Subjective (IKDC Subj.) scores at the different follow-up examinations.
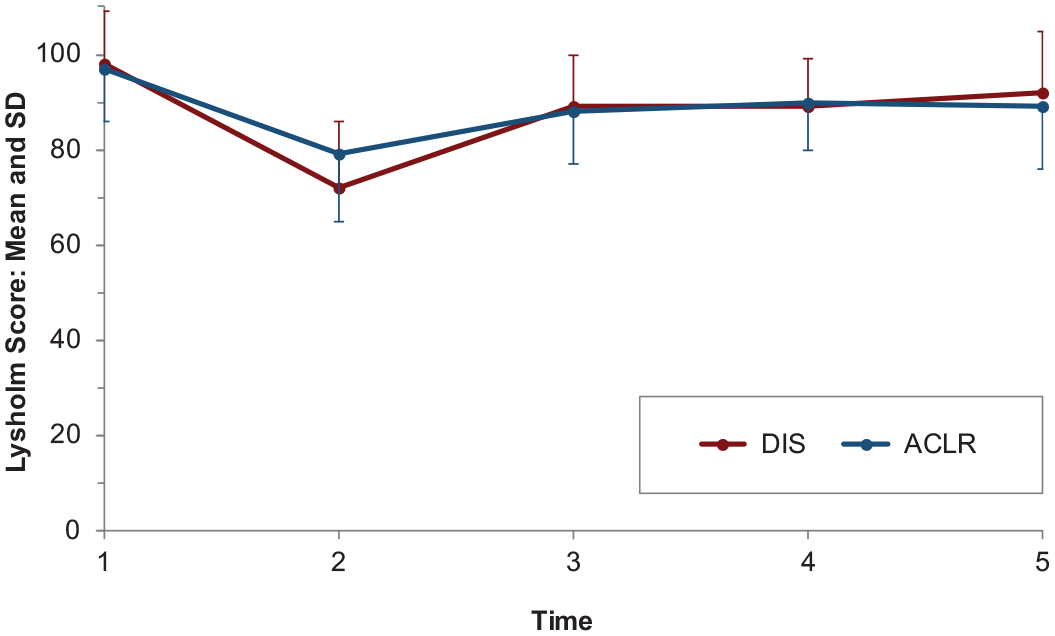
Lysholm scores at the different follow-up examinations.
Mean patient satisfaction at the final follow-up was 8.8 ± 1.4 of 10 in the DIS group and 8.4 ± 1.5 of 10 in the ACLR group (P = .1083).
Complications and Revision
Failure (ΔATT of >3 mm in combination with a subjective feeling of instability) was found in 7 of 43 patients (16.3%; 5 male/2 female) in the DIS group and 5 of 40 patients (12.5%; 3 male/2 female) (P = .432) in the ACLR group. All patients with failure had a second trauma after returning to their previous activity level. The mean time from the index procedure to failure was 17.0 ± 5.9 months (range, 11-26 months) in the DIS group and 12.6 ± 3.9 months (range, 9-20 months) in the ACLR group. In addition, another 3 patients in the DIS group had laxity with ΔATT >3 mm but had no subjective instability at the 24-month follow-up. No revision was performed (2 copers and 1 adapter). In the ACLR group, 1 patient had ΔATT >3 mm but without subjective instability (coper; preoperative and postoperative Tegner score, 6).
A total of 5 of 7 (71.4%) patients with recurrent instability in the DIS group had a preinjury Tegner score >6 and were younger than 25 years at the time of the injury. This trend was similar in the ACLR group (4/5 [80.0%] patients with a Tegner score >6 and age <25 years).
All revision procedures in the DIS group could be performed as single-stage interventions with removal of the tibial monobloc and ACLR with an autologous hamstring tendon graft (Figure 6). In contrast, 4 of 5 revision procedures in the ACLR group had to be performed as 2-stage procedures because of tibial tunnel widening. According to our in-house standard, the contralateral hamstring tendon was the graft of choice in revision ACLR. Because we assumed a graft diameter (semitendinosus and gracilis tendons combined) of a maximum of 10.5 mm, we performed 2-stage procedures in tunnels with a diameter >11 mm. Table 2 describes the revision ACLR cases of both groups.
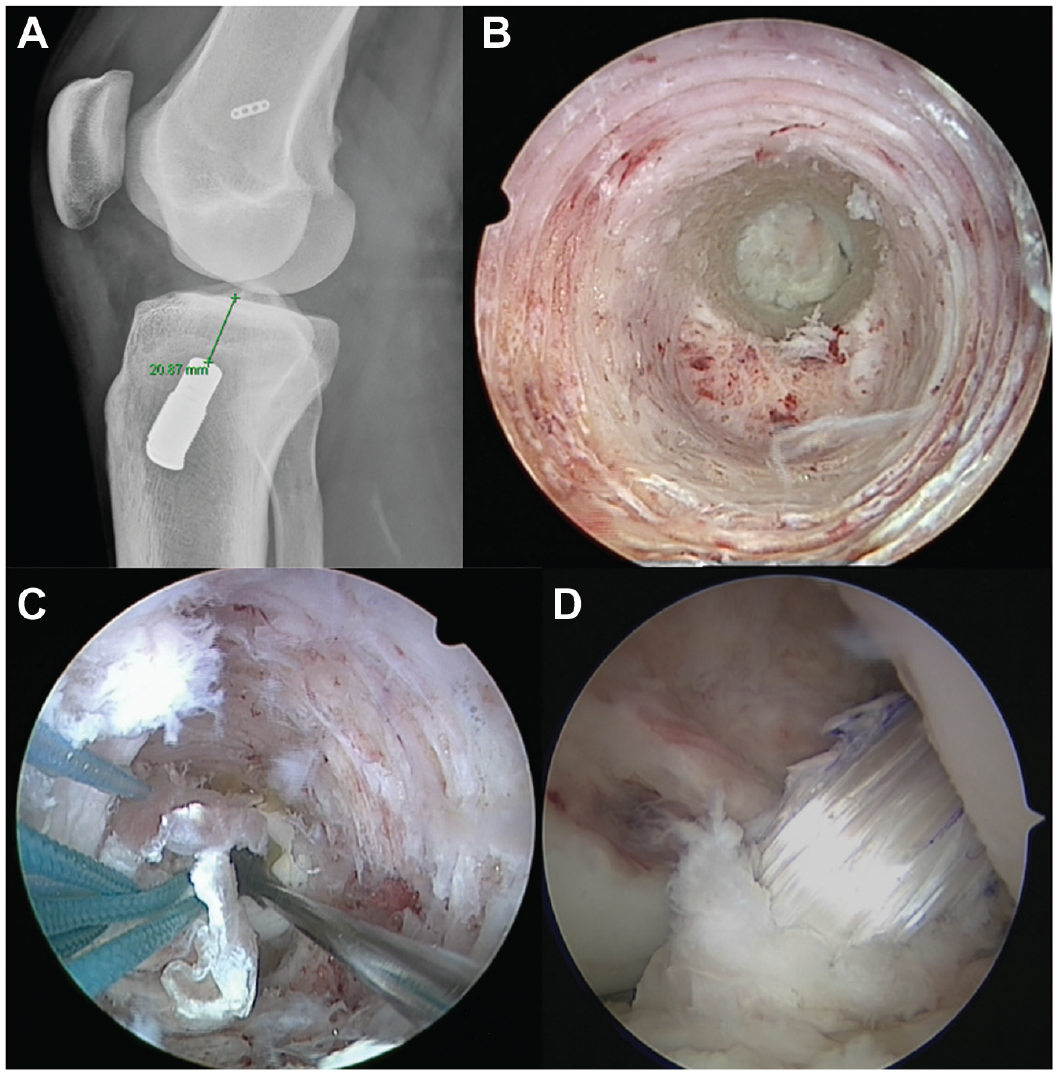
Single-stage revision for recurrent instability after dynamic intraligamentary stabilization. (A) Radiograph before revision demonstrating a 2-cm distance between the monobloc and joint line. (B) Tibial tunnel after removal of the monobloc. (C) Interference screw fixation of the autograft within the newly drilled 2-cm bone tunnel. (D) Intra-articular graft.
Revision ACLR a
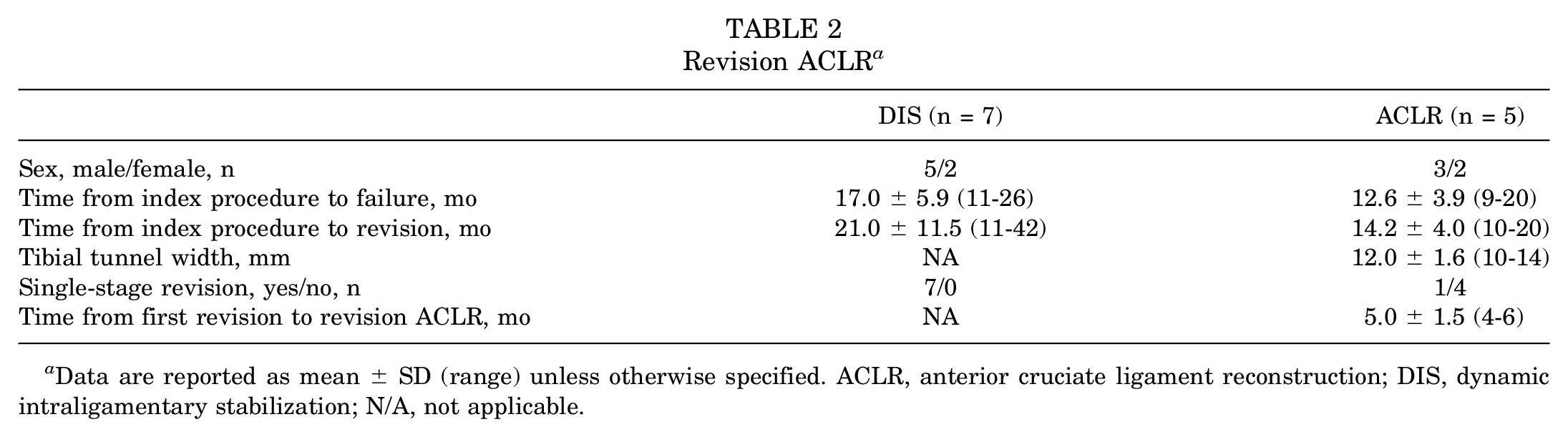
Data are reported as mean ± SD (range) unless otherwise specified. ACLR, anterior cruciate ligament reconstruction; DIS, dynamic intraligamentary stabilization; N/A, not applicable.
Furthermore, deficits in knee extension (3 DIS; 1 ACLR) and secondary meniscal lesions (1 DIS; 3 ACLR) led to reinterventions, resulting in an overall revision rate of 25.6% in the DIS group and 22.5% in the ACLR group. After these revision procedures, the follow-up was uneventful, and all patients returned to their previous activity levels. All reasons for revision are displayed in Table 3.
Reasons for Revision a
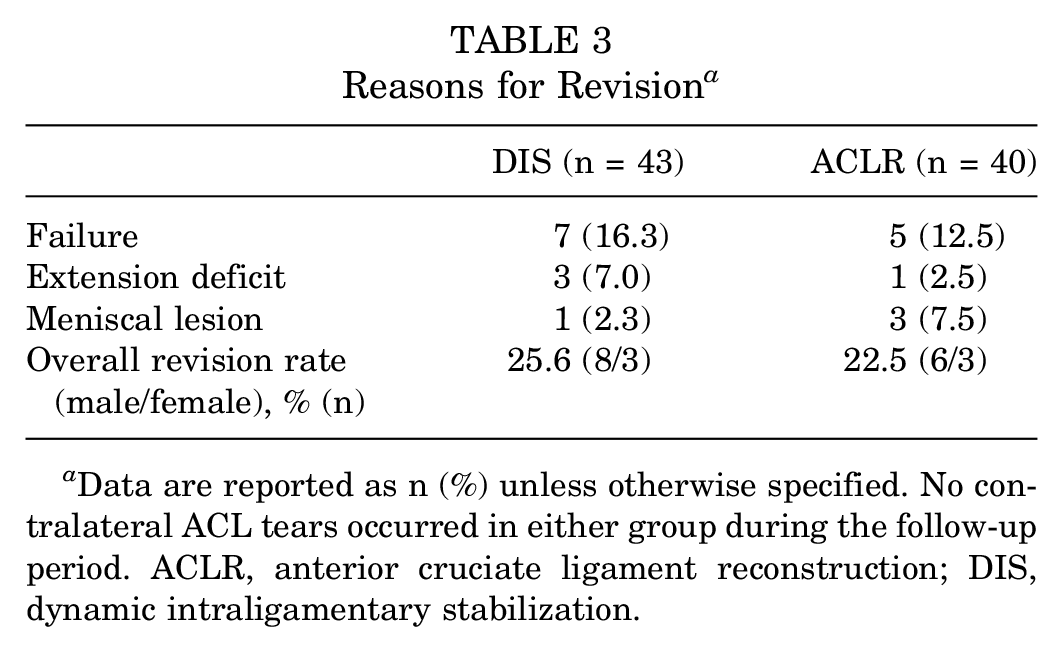
Data are reported as n (%) unless otherwise specified. No contralateral ACL tears occurred in either group during the follow-up period. ACLR, anterior cruciate ligament reconstruction; DIS, dynamic intraligamentary stabilization.
Discussion
In the present study, the failure and overall revision rates after ACL repair with DIS (Table 2) were comparable with those after ACLR. A total of 7 patients (16.3%) had failure in the DIS group compared with 5 patients (12.5%) in the ACLR group (P = .432). However, ATT was significantly greater in the DIS group compared with the ACLR group (ΔATT, 1.9 vs 0.9 mm, respectively; P = .0086). The clinical results of ACL repair with DIS were comparable with those of ACLR after the 24-month follow-up period. No significant differences were found between the 2 groups for any of the Tegner, IKDC, or Lysholm scores at any time point during the follow-up period.
The functional results are in accordance with those of Hoogeslag et al, 18 who performed a similar study with 48 patients undergoing either ACL repair or ACLR with the IKDC score as the primary outcome parameter. After 2 years, no significant differences between the 2 groups could be found for the IKDC score and the secondary outcome parameters (ie, Knee injury and Osteoarthritis Outcome Score, Tegner score, Rolimeter testing). Interestingly, failure was found in only 2 patients (8.7%) in the ACL repair group and 4 patients (19%) in the ACLR group. However, because of the small sample size, this difference was not significant. The rate of reinterventions other than revision was higher in the ACL repair group, which is again consistent with the finding of our study.
Previously, short-term results of the first 30 patients per group enrolled in this study were published. 37 All patients were furnished with an accelerometric step counter and underwent 3-dimensional gait analysis 6 weeks and 6 months after surgery. Although there was a trend for increased early postoperative activity after DIS (significant at weeks 2 and 3; P = .024 and .022, respectively), neither knee kinematic and kinetic parameters nor the functional scores showed any significant differences between DIS and ACLR. The increased early postoperative activity of patients undergoing ACL repair compares with the results of Hoogeslag et al, 18 who found 58.3% of the patients in the ACL repair group to have returned to their preinjury activity level after 1 year (42.9% in the ACLR group). However, this difference diminished after 2 years.
ACL repair was widely performed in the 1970s and 1980s with open techniques to restore knee joint kinematics after an ACL tear. In 1976, Feagin and Curl 12 reported on a cohort of 64 cadets at the United States Military Academy who underwent open repair of isolated ACL tears. A total of 32 patients could be re-evaluated, of whom 17 had a significant reinjury and 71% reported persistent pain. Taylor et al 41 published long-term results for the same cohort of patients with an average follow-up of 32 years. The revision rate at this time was 28%, but at least 53% of the patients rated their knee function as normal or nearly normal. Other studies have reported similar results with high revision rates, persistent symptoms, and an unacceptably low rate of return to preinjury activity levels.8,10,32,40,44
With the increasing popularity of ACLR using autografts and allografts, ACL repair has become less utilized and is only rarely performed. However, the potential drawbacks of ACLR (ie, higher failure rate than the native ACL, donor site morbidity, and loss of proprioception) and the development of modern arthroscopic techniques have led to a resurgence of the idea of repairing the torn ACL.
Anchor fixation, ligament bracing, and DIS are the main techniques currently used for ACL repair. To date, sufficient data are available only for DIS, with more than 1000 cases published in the literature.1,13,15,16,20,30,33,42
Several previous studies have demonstrated good outcomes after ACL repair with DIS. Since the first clinical report on this new technique by Eggli et al 9 in 2014, this technique has been comprehensively evaluated in experimental and clinical studies.4,14,15,17,19,23,24,38 From a biomechanical perspective, DIS can provide knee joint kinematics comparable with those of the ACL-intact knee.14,38 In the clinical setting, functional results are very promising after short-term and midterm follow-up, with failure rates that are slightly higher than those after ACLR.4,5,17,24,25 In the most recent and largest case series, Häberli et al 13 reported on 455 patients who underwent DIS for an acute ACL tear. In more than 90% of the cases, the native ACL could be preserved. The revision rate with secondary ACLR for failed repair was 8.7%. However, other authors have found higher failure rates in their case series.30,33 For example, Osti et al 33 revealed recurrent instability (retear or nonhealing) in 10 patients (17.5%) from their cohort of 57 patients (37 male/20 female) treated with DIS for an acute ACL tear. These rates of recurrent or persistent instability are higher than those published for ACLR.3,11,45 Andernord et al 3 found a 2-year revision rate of 1.8% in a cohort of 16,930 patients (57.7% male; data from the Swedish National Knee Ligament Register). Similarly, Faltstrom et al 11 reported a 4.3% revision rate within 5 years after the index procedure, indicating an increase in the recurrence rate with longer follow-up periods. No contralateral ACL tear occurred after DIS, indicating a potentially positive effect on proprioception by restoration of the native ACL. Bourke et al 6 reported a failure rate of 11% and contralateral ACL tears in 14% after 15 years in patients who underwent ACLR, indicating a graft survival rate of 89% and a survival rate of the contralateral ACL of 86%.
Another concept involving additional augmentation of ACL repair is ligament bracing (Arthrex). This technique is similar to that described by Paessler et al 34 in 1992, who augmented the sutured ACL with a synthetic cord. In comparison with DIS, ligament bracing comprises more rigid augmentation and, therefore, may not take the length change of the ACL during flexion-extension into account. 27 To date, only 1 report in the literature has presented the results of ligament bracing for augmentation of repaired ACL tears: Jonkergouw et al 20 reported on a series of 56 consecutive patients (58.9% male) undergoing ACL repair, of whom 27 had additional augmentation of the repaired ACL with ligament bracing. The functional results were satisfying with and without bracing, but the failure rates differed remarkably (7.4% with vs 13.8% without bracing). In spite of those rates, this difference was not statistically significant because the number of patients was too small to provide sufficient power.
Achtnich et al 1 published a comparative study of ACL repair using anchor fixation and ACLR. A total of 20 patients per group were followed for an average of 28 months. Although the functional results were comparable, again, the failure rate was significantly higher after anchor fixation than ACLR (15% vs 0%, respectively). Similarly, DiFelice et al 7 found a Lysholm score of 93 and ATT <3 mm in 7 of 11 patients undergoing anchor refixation of the torn ACL.
The failure rate after ACL repair (ie, 16.3% in the present study) may be attributed to the age and activity level of the patients who sustained a retear. The high number of patients treated with DIS to date allows the performance of a multivariate regression analysis. Thus, a young age (<25 years) and a high preinjury Tegner score (>5 in the study by Henle et al 15 and >7 in the study by Krismer et al 25 ), together with midsubstance tears, were identified as the main risk factors for failure of ACL repair. Conversely, a proximal tear in combination with a preinjury Tegner score <7 was associated with a recurrence rate of only 3.9%, which was in the range of those reported for ACLR.3,11,25,45 Analyzing the patients with failure in the present study revealed that a young age (<25 years) and an increased activity level (Tegner score >6 in 5/7 patients with failure after DIS) were also the main risk factors for revision. Interestingly, this was not only the case for the DIS group but also for the ACLR group (failure rate, 12.5%). All but 2 patients with clinical failure were younger than 25 years and had a preinjury Tegner score >6 in the DIS group. This is in accordance with the results of Schlumberger et al, 39 who found that age <25 years was a main risk factor for recurrence after both primary and revision ACLR.
All patients with failure after ACL repair underwent single-stage revision. In contrast, 4 of 5 patients in the ACLR group underwent 2-stage procedures because of tibial tunnel widening. Indications and measurement techniques regarding 1- or 2-stage revision are still not ideally defined. In the current literature, 2-stage revision is always recommended for tunnels measuring >16 mm in diameter. 36 Tunnels between 10- and 16-mm in diameter may need tunnel grafting depending on their morphology, planned graft choice, and location. In the present study, all patients with tunnel diameters >11 mm had 2-stage revision according to our revision standard using the contralateral hamstring tendon for revision ACLR. However, when assuming a threshold >15 mm, all of our revision procedures would have been single-staged. In 1 case with a tibial tunnel diameter of 10 mm, the placement of the tunnel was nonanatomic, and therefore, 2-stage revision had to be performed.
In addition, the progressive rehabilitation program with only a 5-day period of immobilization, immediate range of motion training, and early full weightbearing may have influenced the recurrence risk. However, the rehabilitation protocol was in accordance with current guidelines for rehabilitation after ACL repair. 43 Brace-free rehabilitation and early weightbearing do not seem to have a negative effect on knee laxity and functional outcomes.29,43
There were several limitations to this study. First, there was no control group with patients treated nonoperatively for their ACL tears. However, young and active patients with ACL tears usually will be recommended for ACLR to restore knee joint stability and prevent the development of secondary intra-articular lesions and early osteoarthritis. Therefore, initially, we elected to proceed without a nonoperative control group. Second, patients with proximal and midsubstance tears were included. Current studies have shown that ACL repair seems to be more successful in proximal-third tears.2,15,25,42 However, an influence of the tear pattern on the recurrence rate was not identified in this study. Third, 4 different surgeons performed the operative procedures in both groups. However, all of these surgeons were experienced with arthroscopic ACLR and trained at the same center. Furthermore, all surgeons had performed the DIS procedure before the initiation of the study. No influence of the surgeon on the final outcome was observed. This finding is in accordance with other studies. 15 Fourth, the study was only powered for differences in ATT. Therefore, we cannot definitely state that the functional results and patient-reported outcomes were equal in both groups. For the latter, the study might be underpowered and will be continued with a larger cohort of patients. Finally, the results cannot thoroughly be transferred to a high-risk population of patients younger than 20 years because the mean age of the cohort in this study was 28 years. Kaeding et al 21 demonstrated that the risk of failure decreases with every yearly increase of age. Regardless, at least age <25 years could be identified as a risk factor for recurrence in this study and others that have reported the results of both ACL repair and ACLR.15,25,39,46
Conclusion
After 2 years, the failure rate after ACL repair with DIS was comparable with that after ACLR (16.3% vs 12.5%, respectively; P = .432). While ATT measured by Rolimeter testing in the DIS group was increased, functional results after ACL repair with DIS did not differ from those after ACLR. Young age and a high activity level were the main risk factors for failure after both ACL repair with DIS and ACLR. Thus, ACL repair with DIS may be an option to treat patients with acute isolated ACL tears.
Footnotes
Acknowledgements
Submitted March 14, 2019; accepted January 2, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.S., M.H., and C.K. are consultants for Mathys Medical. M.H. is a consultant for Medacta, Conmed Linvatec, Olympus, and DJO. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.