
Abstract
Background:
There is no consensus on technique of choice for repair of bucket-handle meniscal tears (BHMTs).
Purpose:
To determine factors that affect patient outcomes and failure rates in patients undergoing all-inside repairs of BHMTs.
Study Design:
Systematic review.
Methods:
A systematic review of 3 databases using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines was performed. All English-language literature from 1993 to 2019 describing clinical outcomes for patients undergoing all-inside BHMT repair with ≥12-month follow-up was reviewed by 2 independent reviewers. Patient characteristics (patient sex, age), intraoperative factors (laterality, concomitant procedures, surgical technique, implants utilized), and postoperative outcomes (failure rates) were analyzed. Study quality was evaluated with the Modified Coleman Methodology Score (MCMS).
Results:
Fifteen studies (1 level 1, 4 level 3, 10 level 4) with 763 total patients (64% male; average age, 26.4 years [range, 9-58 years]; average follow-up, 39.8 months [range, 12-120 months]) including 396 all-inside BHMT repairs were included. Six devices were used for repair including the Meniscal Repair System, FasT-Fix, Meniscus Arrow, Biofix Arrow, RapidLoc device, and PDS II suture, with failure rates of 13.5%, 22.4%, 27.1%, 42.9%, 45.2%, and 0%, respectively. The overall repair failure rate was 29.3% at an average of 13.0 months (range, 5.0-32.4 months), but 19.0% for devices still in use. The RapidLoc and Biofix Arrow had higher failure rates than other devices (P = .0003). Women (31%) were less likely to experience a failure than were men (69%) (P = .03). Longer follow-up duration resulted in higher failure rates (>30 months, 34.4%; <30 months, 23.4%; P = .016). In 4 studies reporting on both all-inside and inside-out repairs, no significant differences in failure rates were observed. No significant differences in failure rates were found between medial and lateral repairs nor repair with and without concurrent anterior cruciate ligament reconstruction (P > .05 for all). The overall average MCMS was 54.4 ± 12.
Conclusion:
The overall failure rate after all-inside repair of BHMTs is 29.3% at an average of 13.0 months, with no difference in failure rates between medial and lateral meniscal repairs. The variables shown to negatively affect the failure rates were the RapidLoc and Biofix Arrow, male sex, and longer follow-up duration.
The fibrocartilaginous lateral and medial menisci serve as proprioceptors, stabilizers, and pressure distributers in the tibiofemoral joint.18,44,45 Meniscal injuries can result from trauma, degeneration, or congenital malformation, 7 and they are one of the most common types of surgically repaired knee injury in the United States. 1 From 1883 4 to the 1970s, the mainstay of meniscal injury management was partial or complete meniscectomy. 9 That began to change as new evidence arose demonstrating worse clinical outcomes, degenerative knee changes, and increased pressure loads as compared with newer meniscal preservation and repair techniques,6,18,28 and meniscal repair is now attempted whenever possible. Within the past 25 years, meniscal repair has evolved from open procedures to arthroscopic procedures, with arthroscopic procedures coming into greater favor because of their quicker recovery and rehabilitation times and fewer complications.26,43 The 3 arthroscopic techniques used today are the inside-out repair, outside-in repair, and all-inside repair. Although the inside-out repair remains the gold standard of meniscal repairs because of its proven success in a variety of meniscal zones,14,15,38 the outside-in technique can be useful for anterior tears that are hard to reach through arthroscopic portals, 21 and the all-inside technique has become increasingly popular since the introduction of the Meniscus Arrow (Bionx Implants Inc) in 1993. 3 The all-inside technique has shown reduced operative times, quicker patient recovery, and fewer potential neurovascular complications, especially with tears of the posterior horn.3,5,19,25
Although tear location is a large determining factor in choosing which technique to use, tear type also plays a role. Bucket-handle meniscal tears (BHMTs), defined as vertical longitudinal tears that can be displaced toward the intercondylar notch, often present with a locked knee and pose a particular challenge for surgeons. Data suggest that BHMTs demonstrate worse clinical outcomes than smaller vertical longitudinal tears after meniscal repair.32,33 As such, using the optimal repair technique for BHMTs is critically important. Because of the lack of definitive clinical data regarding the best technique to use for these tears, however, technique choice is largely determined by surgeon preference. Because the all-inside technique necessitates 1 fewer incision and assistant compared with the inside-out technique, 35 it might be the preferred choice if clinical outcomes are comparable. So far, the clinical outcomes data for the all-inside repair of BHMTs have been mixed. While tear vascularity, chronicity, and size all factor into the likelihood of a successful repair, 11 our goal was to review the current literature addressing clinical outcomes and prognostic factors regarding the all-inside repair of BHMTs.
Methods
Literature Search
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines using a PRISMA checklist. 27 Two independent reviewers (C.A.A., D.W.M.) conducted a search using PubMed, EMBASE, and the Cochrane Library up to May 15, 2019. The following search terms were used: “all inside meniscus repair,”“all-inside meniscus repair,”“all inside meniscal repair,”“all-inside meniscal repair,” and “bucket-handle.” A total of 1661 studies were reviewed by title and/or abstract to determine study eligibility based on inclusion criteria. In the event of disagreement, the final decision was made by a third reviewer (D.A.H.). Inclusion criteria were English-language studies from 1993 to 2019 that reported clinical outcomes for all-inside repairs of BHMTs with no less than 12 months of average follow-up. Exclusion criteria included review articles, presentation abstracts, biomechanical studies, and editorials. Studies were also excluded if data involving additional repair methods or tear types were inseparable from the all-inside repairs of BHMTs specifically. The corresponding authors of many of those papers were contacted, and includable data from 1 of them 34 was obtained and included. Fifteen studies § were included in the final review (Figure 1).
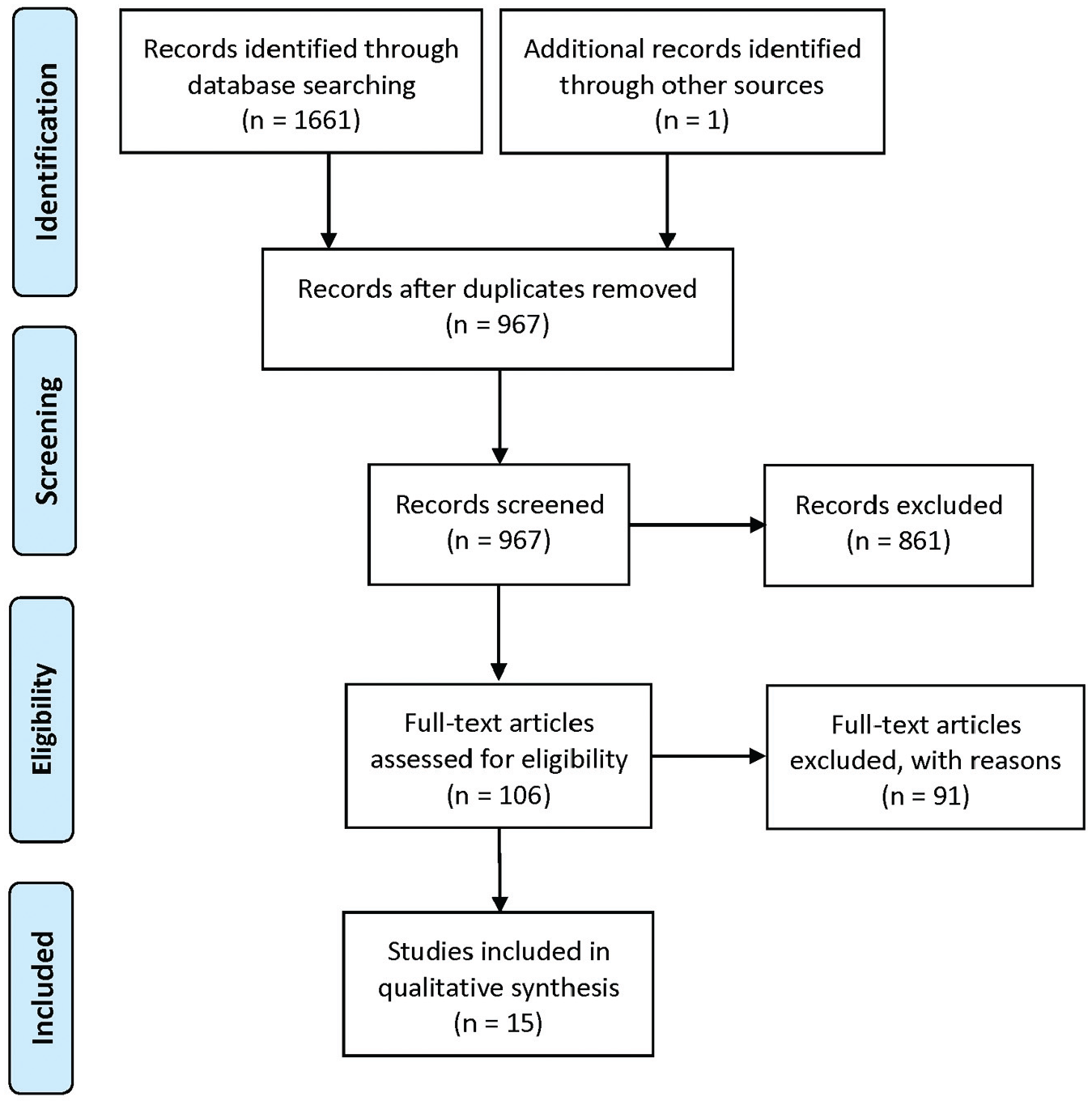
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Data Extraction
Data on patient characteristics, follow-up duration, devices and techniques utilized, meniscal tear location, concurrent surgeries, and failure rates were compiled and consolidated.
Study Methodology Assessment
Study methodological quality was evaluated with the Modified Coleman Methodology Score (MCMS). 13 MCMS is a quality assessment tool with output scores ranging from 0 to 100, with a score of 100 indicating that the study largely avoids chance, biases, and other confounding factors. Scores of 85 to 100 are considered excellent, 70 to 84 are good, 55 to 69 are fair, and less than 55 are poor.
Statistical Analysis
Analyses were done by chi-square test to compare categorical variables and linear regression to characterize the relationship between follow-up duration and failure rate. Statistical significance was set at α = .05.
Results
Study Characteristics
Fifteen studies § including 396 all-inside repairs for the treatment of BHMTs were included (Table 1). Saltzman et al. 34 was included in the results because its original 2018 publication met inclusion criteria for the search. Patient age ranged from 9 37 to 58 42 years with an average of 26.4 years across the 15 included studies, and 64% of the patients were men. The average patient follow-up ranged between 12 24 and 120 39 months within the studies, with an overall average follow-up of 39.8 months.
Study Characteristics of the 15 Studies Included in the Review a
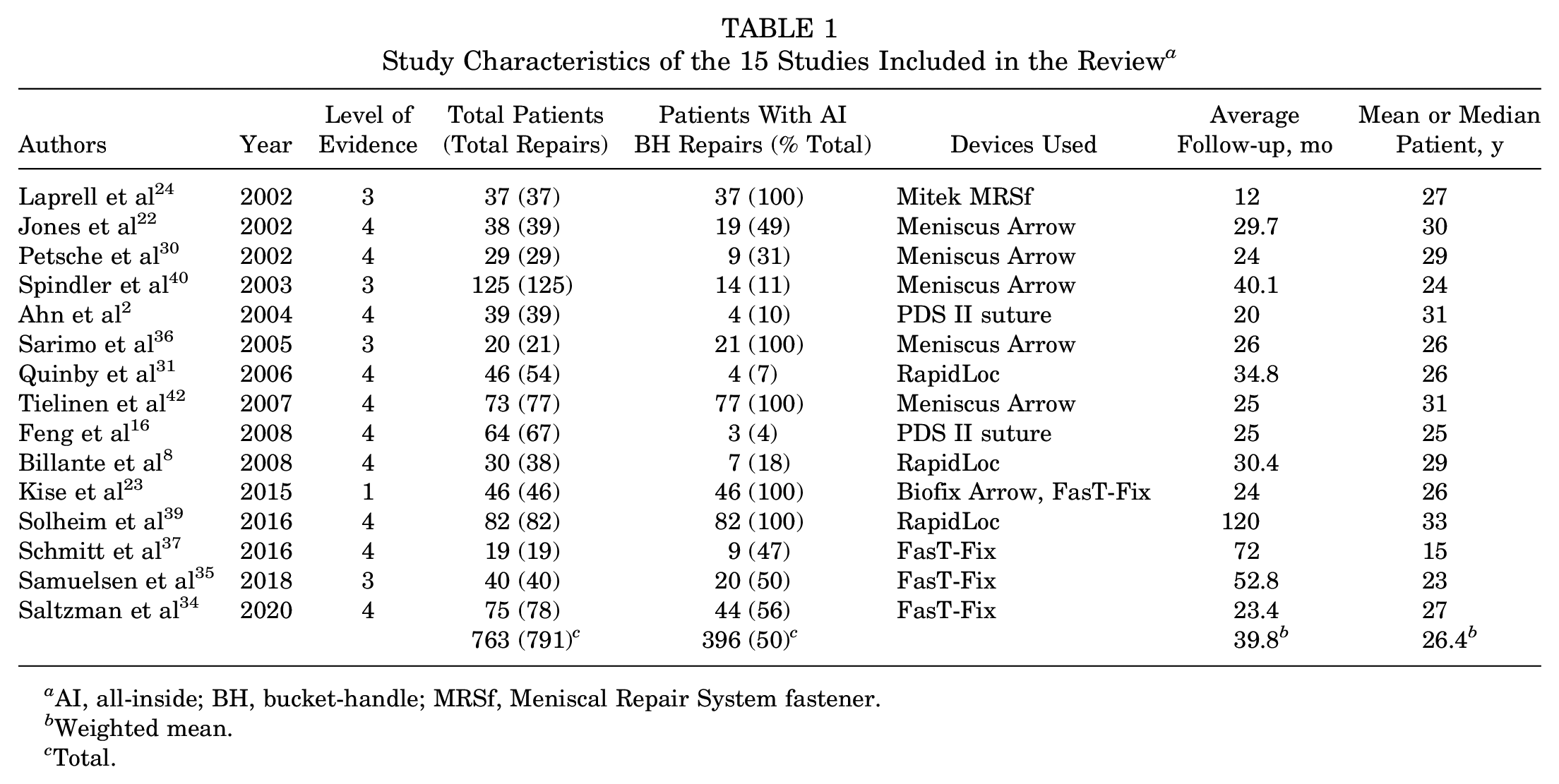
AI, all-inside; BH, bucket-handle; MRSf, Meniscal Repair System fastener.
Weighted mean.
Total.
Study Quality
Most of the studies included in this review were retrospective or prospective case series. Specifically, 1 study 23 was level 1 evidence, 4 studies24,35,36,40 were level 3, and 10 studies ∥ were level 4. The MCMS average was 54.4 ± 12 (range, 39-78), with the majority falling in the “fair” range (Table 2).
Study Quality and Failure Definition a
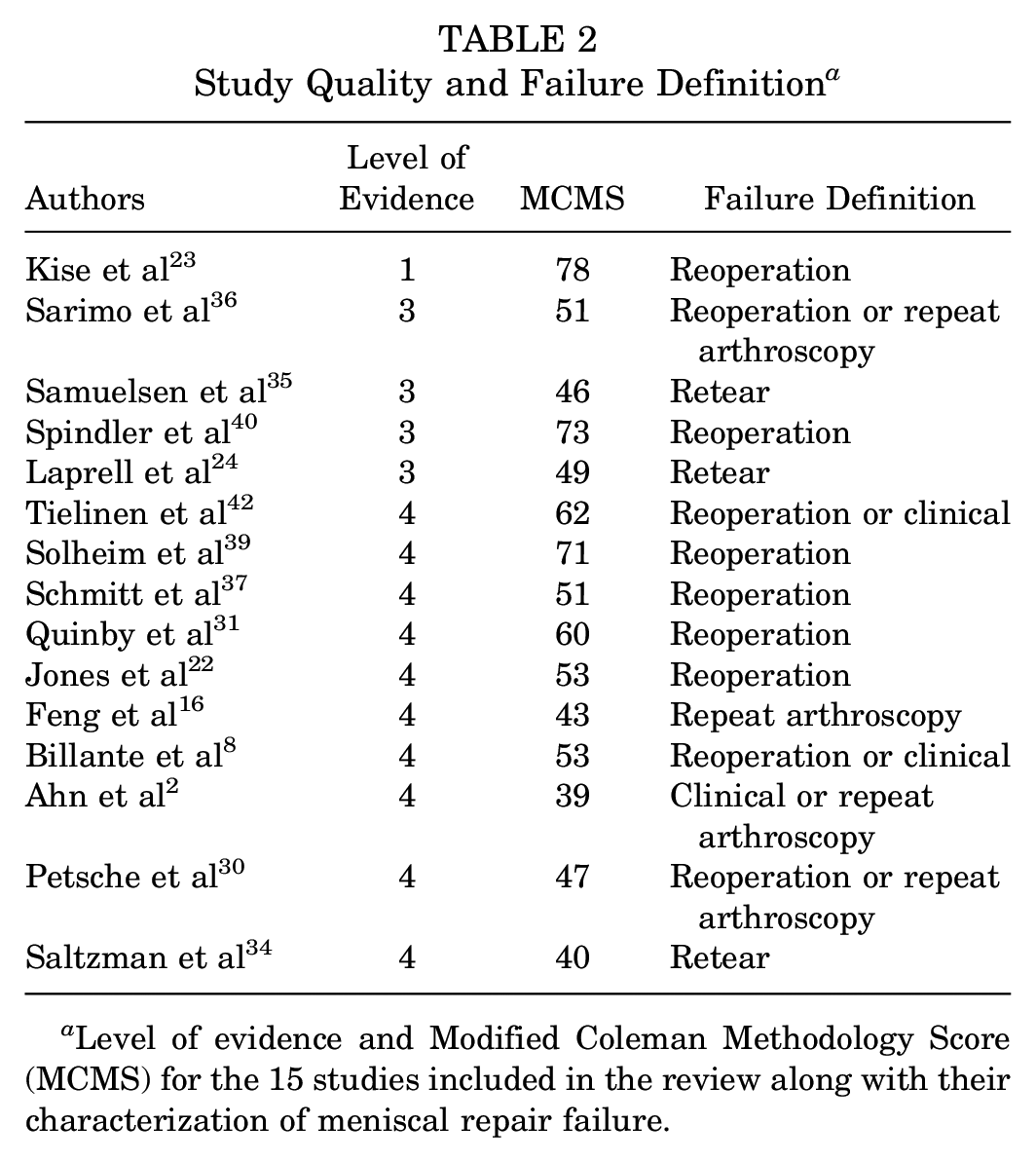
Level of evidence and Modified Coleman Methodology Score (MCMS) for the 15 studies included in the review along with their characterization of meniscal repair failure.
Repair Devices
The devices used for all-inside repairs varied from study to study. Six different devices were used in these studies; the Meniscal Repair System fastener (MRSf) (Mitek Products) was used in 1 study, 24 as was the Biofix Arrow 23 (Bionx Implants Ltd). PDS II (polydioxanone) sutures (Ethicon) were used in 2 studies,2,16 the RapidLoc device (DePuy Mitek) was used in 3 studies,8,31,39 a FasT-Fix device (Smith & Nephew) was used in 4 studies,23,34,35,37 and Meniscus Arrows were used in 5 studies22,30,36,40,42 (Table 1). Both first and second generations of the FasT-Fix device and Meniscus Arrow were utilized in the studies. Since there was no significant difference between failure rates between the 2 generations, the 2 generations were combined in the failure rate analysis because of ambiguity regarding which generation was used in at least 1 study. 42
Failure Rates
Differences in failure rates were compared for variables including patient sex, devices used, medial versus lateral meniscal repair, status of concurrent anterior cruciate ligament (ACL) reconstruction, and follow-up duration. Failures were similarly defined between the studies, with reoperation considered a failure in all cases. However, some studies distinguished clinical failure from retear or reoperation, ¶ while others2,8,42 did not (Table 2). Whenever it was possible to separate clinical failure from retear or reoperation, only the latter were considered failures. Both definitions of failure were combined for an overall failure rate of 29.3% at an average of 13.0 months for the all-inside repair of BHMTs in these studies (Table 3).
Failure Rates and Time to Failure a
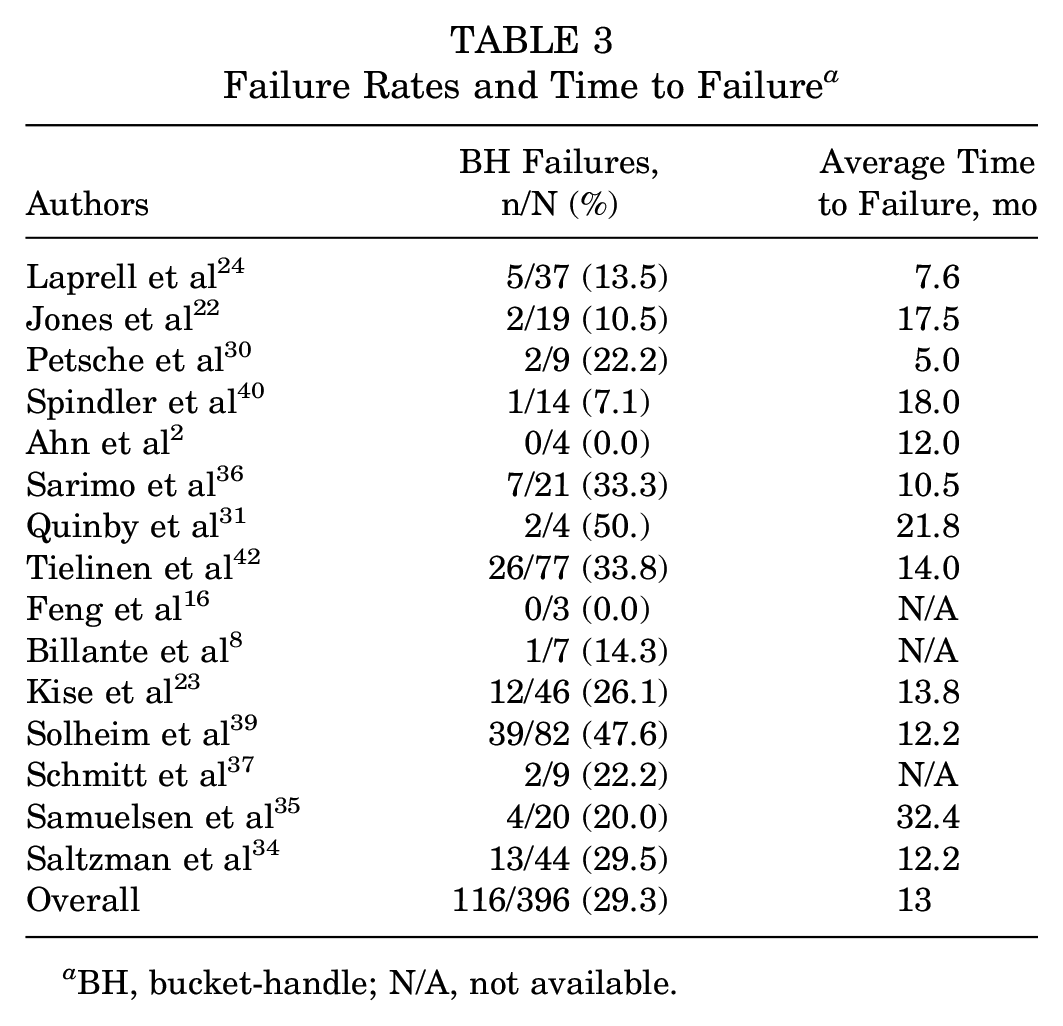
BH, bucket-handle; N/A, not available.
Device
The device-specific failure rates were 0% for the PDS II suture, 13.5% for the Mitek MRSf, 22.4% for the FasT-Fix meniscal repair system, 27.1% for the Meniscus Arrow, 42.9% for the Biofix Arrow, and 45.2% for the RapidLoc meniscal repair device. There was a significant difference in the failure rates for the different devices (P = .0003), with the RapidLoc device and the Biofix Arrow performing significantly worse than the others (Table 4, Figure 2). The devices currently in use or with subsequent generations still in use are the FasT-Fix, PDS II suture, and Mitek MRSf, which have a combined failure rate of 19.0% (n = 142).
Failure Rates of All-Inside Devices a
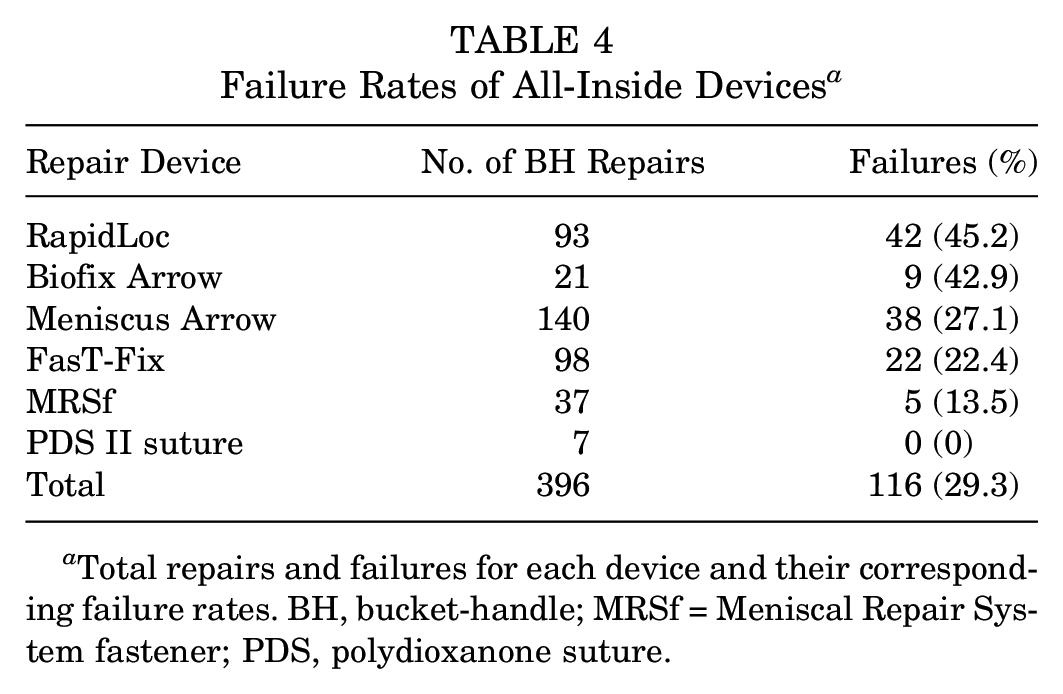
Total repairs and failures for each device and their corresponding failure rates. BH, bucket-handle; MRSf = Meniscal Repair System fastener; PDS, polydioxanone suture.
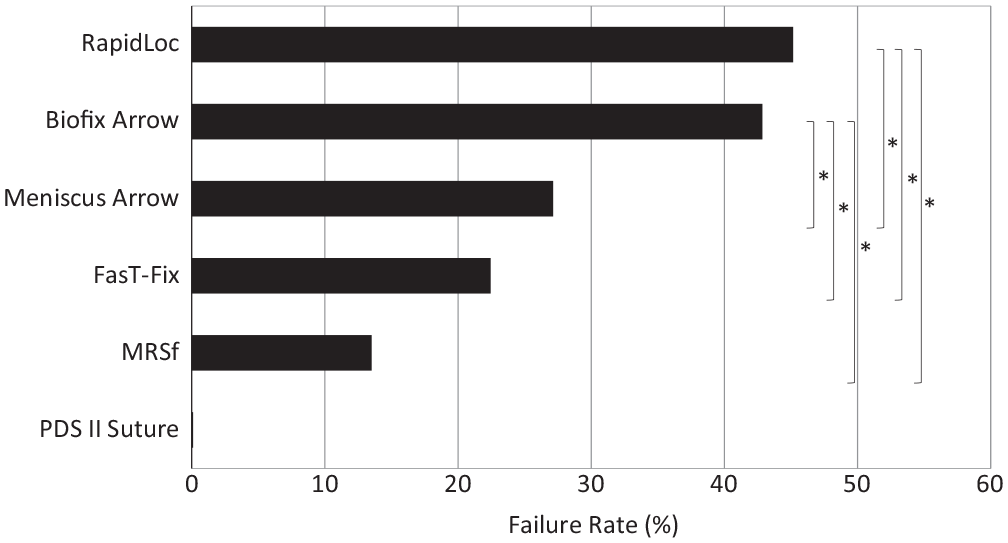
Failure rates of the 6 all-inside devices used for meniscal repair. An asterisk denotes statistical significance (P < .05). MRSf, Meniscal Repair System fastener; PDS, polydioxanone suture.
Sex
Although every study but one 42 reported overall sex ratios, only 2 studies34,39 reported specific statistics for BHMTs. In these studies, women (31%; n = 40) had a failure rate of 25.7% and were significantly less likely to experience a failure than were men (69%; n = 90) (P = .03), whose failure rate was 47.8% (Table 5, Figure 3).
Failure Rates by Sex, Follow-up, ACL Status, and Laterality a
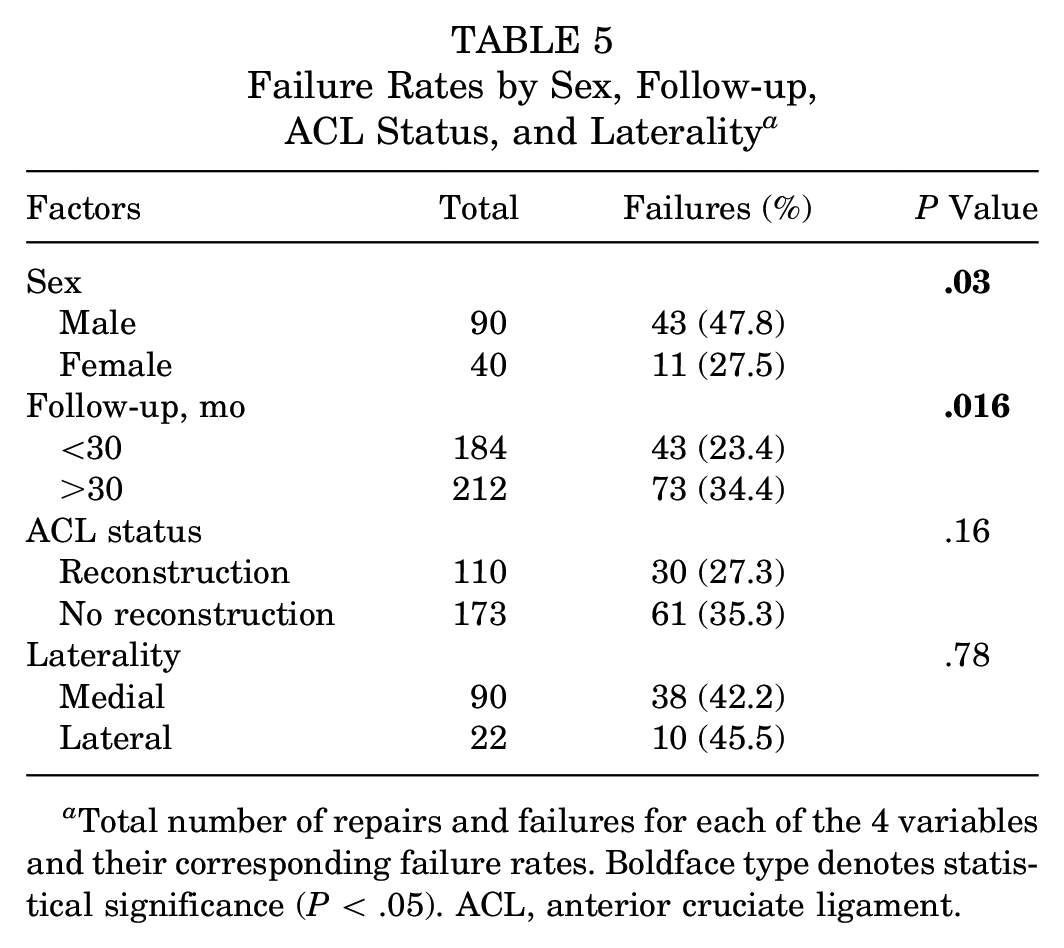
Total number of repairs and failures for each of the 4 variables and their corresponding failure rates. Boldface type denotes statistical significance (P < .05). ACL, anterior cruciate ligament.
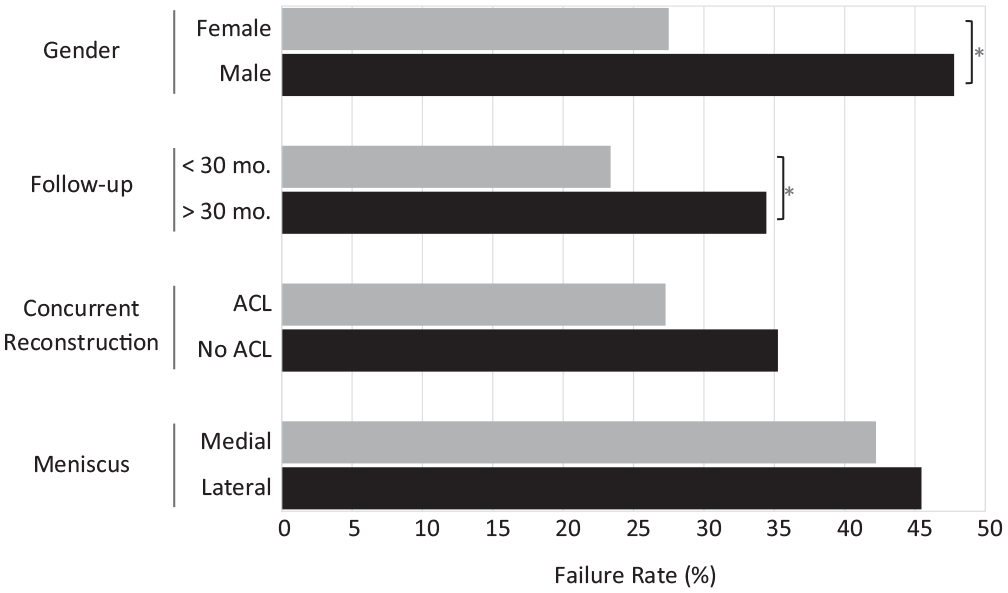
Factors affecting failure rates. An asterisk denotes statistical significance (P < .05).
Laterality
Nine studies reported laterality failure statistics, but just 4 studies2,36,37,39 had separable BHMT statistics (Table 5). In these studies, there was no significant difference between failure rates of medial (42.4%; n = 38) and lateral (45.5%; n = 10) meniscal repairs (P > .05) (Figure 3).
Concurrent Surgeries
Eight studies2,24,31,34,36,39,40,42 reported statistics for ACL injuries and reconstructions, which were all used in our analysis (Table 5). In all but 1 study, 24 ACL reconstructions were done concurrently with the meniscal repairs. Laprell et al 24 performed ACL reconstructions 6 to 8 weeks after the initial meniscal repairs. There was no significant difference in failure rates between those who had an isolated meniscal repair (35.3%; n = 61) and those who underwent concurrent ACL reconstruction (27.3%; n = 30) (P > .05) (Figure 3).
Follow-up
All 15 studies # reported study-wide average or median follow-up duration (Table 5). Linear regression was used to detect the relationship between follow-up duration and failure rate (Figure 4). The studies were subsequently split in half to determine significance by chi-square. Studies2,16,22,24,30,36,40,42 with an average or median follow-up duration of <30 months (53%; n = 8) had significantly lower rates of failure than studies8,23,31,34,35,37,39 with an average or median follow-up duration of >30 months (47%; n = 7) (P = .016) (Table 5).
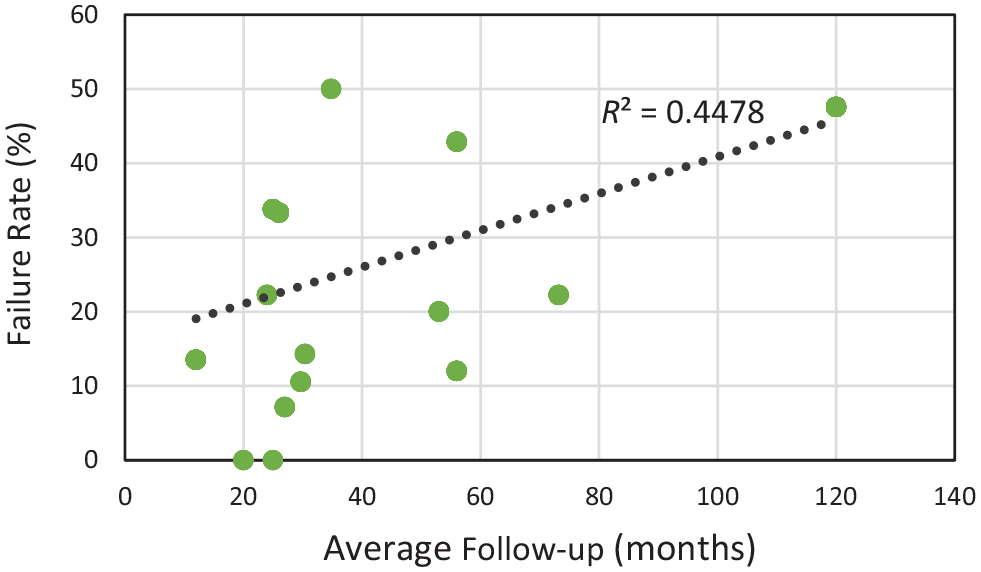
Relationship between studies’ average follow-up duration and meniscal repair failure rate via linear regression.
Inside-Out Repair Comparison
Four studies16,34,35,40 reported on both inside-out and all-inside repairs of BHMTs. All-inside repairs had a failure rate of 17.1% with 13 out of 76 repairs failing, while inside-out repairs had a failure rate of 17.2% with 15 of 87 repairs failing. There was no significant difference in failure rates between the techniques in these studies (P = .98).
Discussion
We found that the overall failure rate after all-inside repair of BHMTs was 29.3% at an average of 13.0 months with no difference in failure rates between medial and lateral meniscal repairs. The variables shown to negatively affect the failure rates were the RapidLoc device and the Biofix Arrow, male sex, and longer follow-up duration. This may suggest that failure rates are underestimated in studies with <30 months follow-up and, thus, would be higher with longer-term follow-up.
One area in which we found no difference, but that has historically been found to affect failure rates in short-term studies, is ACL reconstruction status. Several studies have demonstrated better outcomes when meniscal repair is done concurrently with ACL reconstruction,12,20,38,41 but these studies have short follow-up durations. The benefit of concurrent ACL reconstruction has been believed to be due in part to the increased blood accumulation from the surgically induced trauma. 12 A more recent systematic review by Nepple et al 29 looking at factors affecting meniscal repair failure rates at greater than 5 years of follow-up found no difference in failure rates between those with isolated meniscal repairs and those undergoing concurrent ACL reconstruction. Considering that our current review includes studies with an average follow-up of more than 3 years, it might be worthwhile to look further into the role that time plays in the relationship between meniscal repair and concurrent ACL reconstruction.
With an overall failure rate of 29.3%, our findings suggest that the outcomes of all-inside repair might be less favorable than those of the inside-out repair when used for BHMTs. A systematic review by Grant et al 19 in 2012 found a 17% failure rate in 8 studies reporting on inside-out repairs for isolated BHMTs. The authors restricted their analysis to repairs in the red-red or red-white zones and only required 3 months of follow-up, which may have resulted in a more favorable failure rate compared with the results of our study. This is because highly vascular regions of the meniscus allow for better healing and short follow-up durations do not catch failures that occur later, as our current study suggests. To enable accurate comparisons of failure rates between studies, future studies should ensure sufficient follow-up duration. Saltzman et al 34 used a Kaplan-Meier curve to conduct survival analysis in their 2018 study, concluding that failure rates steadily increase until 15 months. 34 As such, this time point should be considered the minimum necessary follow-up duration.
Although we found that the overall failure rate for BHMTs is higher for all-inside repairs than inside-out repairs, we also found that all-inside repair outcomes vary by device, and the devices associated with better outcomes had failure rates commensurate with those of inside-out repairs. 19 Our findings corroborate previous biomechanical studies demonstrating better durability of sutures than other methods. 10 Furthermore, some of the older devices that performed poorly in our analysis are no longer commonly used in practice. The combined failure rate for the devices still in use or with subsequent generations still in use is 19.0%, which supports the notion that the all-inside repair is a reasonable alternative to the inside-out repair for BHMTs. A 2017 study by Fillingham et al 17 looking at all-inside versus inside-out repairs for all types of meniscal tears found no difference in failure rates between the techniques, with clinical and anatomic failures of 10% and 16% for all-inside repairs, and 11% and 13% for inside-out repairs, respectively. Four of the studies included in our review had data for both inside-out and all-inside repairs, which allowed for a more direct comparison of the 2 techniques for BHMTs. Importantly, the failure rates of the techniques were almost identical, demonstrating that the all-inside repair seems to perform equally well within studies. Combined with the lower incidence of complications with the all-inside repair, this technique appears to be a good choice for BHMT repair when using a suitable device.
Limitations
It is important to keep in mind that the MCMS of the studies included in this review limit our ability to draw definitive conclusions. While 396 patients undergoing all-inside repair for the treatment of BHMTs were included in this systematic review, the meniscal repair devices varied from study to study, and sample sizes were therefore limited for particular outcomes. Since data were not presented in such a way to allow logistic regression analysis, our findings are purely correlative. Furthermore, data for sex and laterality were extractable from only 2 and 4 studies, respectively. Although the Meniscus Arrow went through at least 2 generations, we were unable to stratify based on generation because of the ambiguity of generation used in at least 1 of the studies. 42 While there were not significant differences between the device generations with the numbers in the studies we assessed, second-generation devices have been found collectively to be stronger than first-generation devices. 10 Additionally, because of the wide variation in the reporting of complications, we were unable to determine overall complication rates, which should always be a significant consideration for determining which surgical technique to use for meniscal repair. Finally, the definition of clinical failure was not consistently distinguished from retear or reoperation, which ultimately limits the ability to determine the healing rate without secondary imaging or second-look arthroscopy.
Conclusion
The overall failure rate after all-inside meniscal repair of BHMTs is 29.3% at an average of 13.0 months, with no difference in failure rates between medial and lateral meniscal repairs. The repair failure rate for devices still in use is 19.0%. The variables shown to negatively affect the failure rates were the RapidLoc device and the Biofix Arrow, male sex, and longer follow-up duration.
Footnotes
Submitted October 11, 2019; accepted December 12, 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.M.F. has received speaking fees from Arthrex Inc and publishing royalties and financial or material support from Elsevier. A.F.V. has received other financial or material support and consulting fees from Smith & Nephew and Stryker; education payments and compensation for services other than consulting from Arthrex; and hospitality payments from Steris Corp. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
An online CME course associated with this article is available for 1 AMA PRA Category 1 Credit™ at ![]() . In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.
. In accordance with the standards of the Accreditation Council for Continuing Medical Education (ACCME), it is the policy of The American Orthopaedic Society for Sports Medicine that authors, editors, and planners disclose to the learners all financial relationships during the past 12 months with any commercial interest (A ‘commercial interest’ is any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients). Any and all disclosures are provided in the online journal CME area which is provided to all participants before they actually take the CME activity. In accordance with AOSSM policy, authors, editors, and planners’ participation in this educational activity will be predicated upon timely submission and review of AOSSM disclosure. Noncompliance will result in an author/editor or planner to be stricken from participating in this CME activity.