
Abstract
Background:
Femoral tunnels that are not anatomically placed within the native anterior cruciate ligament (ACL) footprint during ACL reconstruction are associated with residual instability, graft rupture, and poor clinical outcomes. Although surgeons may intend to place their femoral tunnels within the native ACL attachment, this is not always achieved. This study assesses the variation between intended and achieved femoral tunnel positions in a large cohort of experienced ACL surgeons.
Hypothesis:
The accuracy with which experienced ACL surgeons achieve their intended femoral tunnel position is dependent on viewing portal, localization strategy, and drilling technique.
Study Design:
Controlled laboratory study.
Methods:
A total of 221 surgeons indicated their intended femoral tunnel location on a true lateral radiograph of a cadaveric knee specimen and a scaled photograph. Each surgeon then arthroscopically demonstrated the femoral tunnel on the specimen. The position was captured using fluoroscopy. The Euclidean distance (the straight-line distance between 2 points) between the intended and achieved tunnel positions, referenced to a grid applied to the lateral femoral condyle, was compared. Data were analyzed according to surgeons’ viewing portal (anteromedial [AM] or anterolateral [AL]), tunnel localization strategy (offset aimer, estimation from landmarks, ACL ruler, or C-arm fluoroscopy), and stated drilling technique (transtibial, AM portal, or outside-in).
Results:
Surgeons who viewed the lateral intercondylar notch wall through the AM portal were closer (mean distance, 9.5) to their intended position than those who viewed through the AL portal (mean distance, 15.1; P < .0001). By localization strategy, the mean distance between achieved and intended tunnel positions was greater for surgeons who used an offset aimer (14.5) and estimated the femoral tunnel position (12.9) than for those using a malleable ACL ruler (8.1; P < .0001) and fluoroscopy (4.3; P < .0001). Surgeons’ preferred drilling technique (AM portal, transtibial, or outside-in) had no effect on distance between intended and achieved positions. However, the mean achieved position was higher in the intercondylar notch for those using transtibial drilling (P < .042).
Conclusion:
Surgeons using the AM portal to view the femoral attachment site were closer to their intended tunnel position than those who viewed it with the arthroscope in the AL portal. Surgeons who used fluoroscopy to localize femoral tunnel position were the closest to their intended position. Those who used estimation or an offset aimer had the farthest distance between achieved and intended tunnel positions.
Clinical Relevance:
Although accurate tunnel placement can be achieved using any method, given the disparity between intended and achieved tunnel positions, it may be advisable, even for high-volume surgeons, to verify the placement of their tunnels using either fluoroscopy or a malleable ACL ruler to ensure that they achieve their intended position. Fluoroscopy may be particularly useful for cases where the native femoral stump is no longer visible and for revisions. Viewing through the AM portal is recommended to aid accuracy of tunnel placement.
Anatomic femoral tunnel placement such that the anterior cruciate ligament (ACL) reconstruction graft lies within the native ACL femoral attachment site has been shown to better restore anterior tibial translation, rotational stability, and normal knee kinematics.33,34,43 Graft tunnels placed outside the native femoral attachment site may result in loss of stability, 36 abnormal graft fiber–tensioning patterns, 61 and graft impingement with the roof of the intercondylar notch 28 or the posterior cruciate ligament. 32 Clinical studies have demonstrated that the most common technical error resulting in instability or graft failure after ACL reconstruction is nonanatomic graft placement28,35,59 and that nonanatomic femoral tunnel position is closely correlated with poorer clinical outcome scores. 8 It is also thought that the routine accurate placement of ACL grafts within the native ACL attachment sites may reduce the long-term incidence of osteoarthritis.
In cases of chronic ACL rupture, remnants of the femoral attachment may be difficult to visualize, making location of the femoral tunnel challenging. Positioning may be estimated using a number of methods. Use of a “clock face” method, describing the relationship of the femoral attachment site to a particular “o’clock” position, is well-established.5,21,41,49 However, this method depends on the correct orientation of the clock face and does not take into account the proximal-distal distance (“shallow-deep” in arthroscopic terms) of the tunnel along the intercondylar notch wall.5,21,23 The native ACL attachment site may also be located by its relationships to osseous landmarks, the intercondylar and bifurcate ridges, located on the posterior aspect of the lateral intercondylar notch wall of the lateral femoral condyle. 22 It has been reported that these ridges can be used to guide the position of the femoral tunnel. These anatomic landmarks, particularly the bifurcate ridge, are variable, can be challenging to reliably visualize through the arthroscope, and may not always be easily identifiable.10,22,46,56-58
The view of the intercondylar notch and the ACL femoral attachment site changes significantly depending on the arthroscopic portal used. 12 ACL reconstruction has traditionally been performed using 2 arthroscopic portals: anterolateral (AL) and anteromedial (AM). The AL portal is used as the arthroscopic viewing portal, and the ACL femoral tunnel is drilled through the AM portal. However, the lateral intercondylar notch wall and ACL femoral attachment site is viewed tangentially, with the arthroscope placed through the AL portal, potentially compromising the surgeon’s ability to accurately place the ACL femoral tunnel. 11 The intercondylar notch is viewed more orthogonally, with the arthroscope placed through the AM portal, and it has been reported that anatomic ACL reconstruction is facilitated by using 3 arthroscopic portals,4,12,18 allowing the surgeon to view the intercondylar notch wall more orthogonally through the AM portal while an accessory AM (AAM) portal is used as a working portal for instrumentation.
The use of surgical instruments to aid femoral tunnel placement during surgery is well-established. The transtibial ACL reconstruction technique that evolved in the 1990s popularized the use of a femoral offset aimer. The tip of the aimer is positioned in the “over the top” position and is used to drill a guide pin a fixed number of millimeters from this position. The size of the offset (in millimeters) from the over-the-top position is selected by the surgeon to achieve the desired femoral tunnel position and has been recommended as a reproducible method for transtibial 49 and AM portal 16 ACL reconstruction. Offset guide size selection may be based on the size of the knee, the size of the graft, and the morphology of the lateral femoral intercondylar notch wall.
An arthroscopic ruler may also be used to assist femoral tunnel placement. 12 The ruler is held parallel to the axis of the femur with the knee at 90° of flexion to locate the position of the tunnel at a measured distance from the proximal border of the articular cartilage on the lateral intercondylar notch wall. This technique has been suggested to be advantageous in that the position of the tunnel is related to the percentage distance along the ruler and is thus independent of the size of the knee. 10
Intraoperative fluoroscopy has been described as an accurate method to guide ACL femoral tunnel placement.2,31,40,44 The tip of a microfracture awl may be used to indicate the ACL femoral tunnel position on a true lateral fluoroscopic image of the knee obtained using a C-arm image intensifier. 12 The potential tunnel position may be referenced using the grid system described by Bernard et al. 9 This method has been stated to be reproducible and independent of different knee morphology.1,31
The purpose of this study was to compare the accuracy of different tunnel-positioning techniques, and it was hypothesized that accuracy of femoral tunnel localization might vary dependent on (1) strategy for viewing and localizing the femoral attachment site and (2) stated drilling techniques. The current study presents the first large study assessing the variation between intended and achieved femoral tunnel positions in a cohort of international high-volume ACL surgeons.
Methods
Surgeon Participants
A total of 221 surgeons from 23 countries each performing a minimum of 40 ACL reconstructions per year (range, 40-500), were included in the study. Inclusion took place over the course of 8 cadaveric workshops held at Bioskills laboratories. There were representatives from the United States, Europe, Australia, Africa, the Indian subcontinent, and the Middle East. Of the participants, 62 were members of the International ACL Study Group.
Experimental Setup
At each Bioskills laboratory session, a right-side human fresh-frozen cadaveric knee specimen was used. Each specimen was from a white donor: 6 female and 2 male; mean age, 61.4 years (range, 53-71 years). The knees were mounted in a standard Bioskills laboratory leg holder with the femur clamped and the tibia free to allow flexion/extension. AL, AM, and AAM viewing portals were made, and a routine arthroscopic examination was performed to ensure that there was no evidence of internal derangement to the menisci, articular cartilage, or ACL. A digital C-arm image intensifier (General Electric) was then used to obtain a true lateral image of the femur (Figure 1). Care was taken to ensure that the region of the femoral ACL attachment was centered in the beam and that the posterior condyles of the femur precisely overlapped. Once satisfactory positioning of the specimen was achieved, the position of the C-arm was locked.
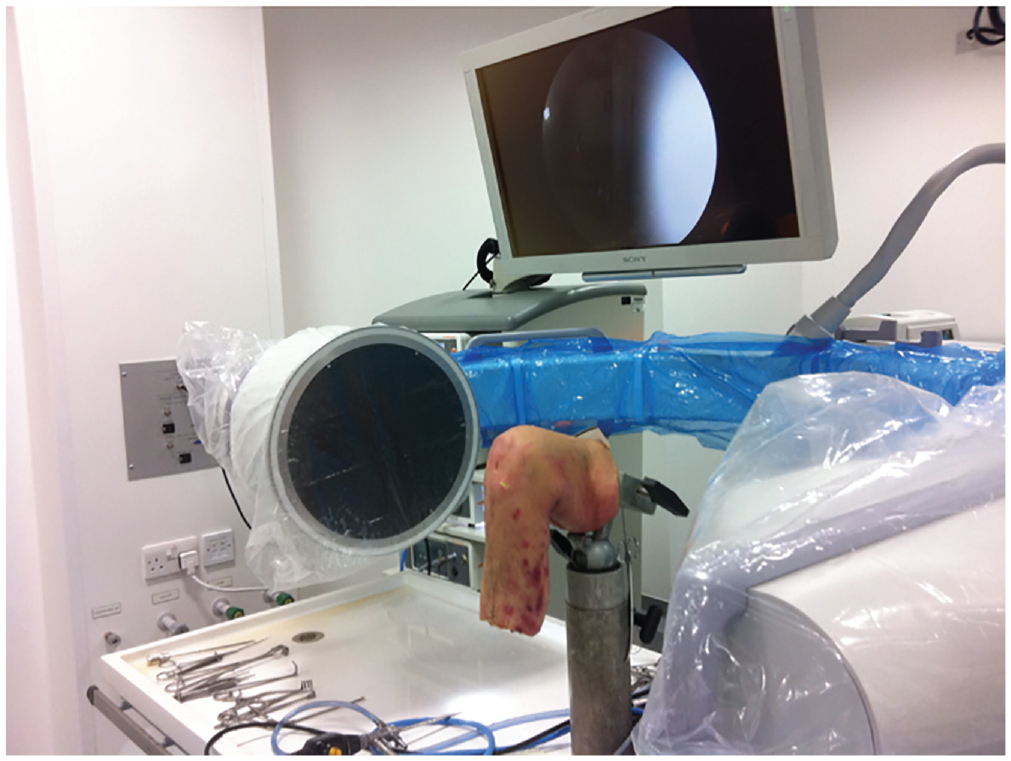
Experimental setup shows the C-arm positioned to obtain a true lateral image of the knee and the femur clamped securely in the Bioskills laboratory leg holder.
The native ACL was carefully divided midsubstance using an arthroscopic duckbill punch, and the ligament fibers were resected back to the femoral and tibial attachment sites with an arthroscopic shaver (Incisor Plus Elite; Smith & Nephew). Great care was taken not to damage the femoral attachment sites. To register the position of the femoral attachment site in each specimen, a 45° microfracture awl was introduced through the AAM portal, and with great care to not make any indentation in the bone, the tip of the microfracture awl was placed at 10 to 15 points (minimum, 10) around the periphery of the femoral attachment site. At each position, a true lateral fluoroscopic image was captured, thus creating a trace around the periphery of the ACL femoral attachment site (Figure 2). This process was repeated 3 times, and any outlying points were removed. After registration of the femoral ACL attachment, the C-arm of the image intensifier was locked in position to maintain the same true lateral radiograph throughout testing.
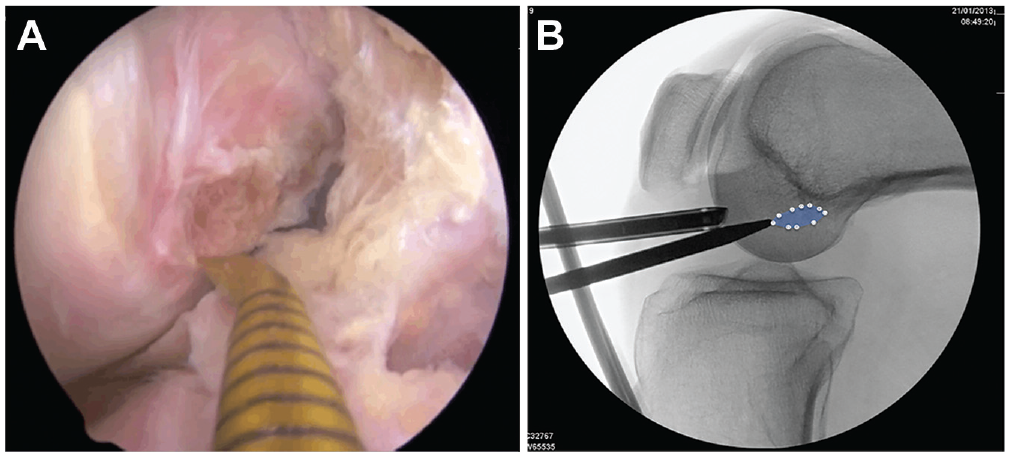
(A) A 45° microfracture awl placed through the accessory anteromedial portal was used to trace 10 to 15 points around the periphery of the native anterior cruciate ligament femoral attachment. (B) Each position was captured using the C-arm, allowing registration of the femoral attachment site.
To simulate a situation where soft tissue remnants at the femoral ACL attachment site were not clearly visible, 12 as with a chronic ACL rupture or a revision case, all of the soft tissues in the region of the native femoral ACL attachment on the lateral intercondylar notch wall were removed using a radiofrequency ablation wand (Super Turbovac 90; Smith & Nephew). Care was taken to preserve any underlying osseous landmarks and the cartilage border.
Intended Tunnel Position Questionnaire
Each participating surgeon was asked to complete a questionnaire to determine the nature of their ACL surgical practice, tunnel placement strategy, and use of viewing portals during the arthroscopy. To ascertain their intended femoral tunnel position, the questionnaire included a picture of the lateral fluoroscopic image of the knee specimen used for that laboratory session, showing the registered ACL femoral attachment footprint. In addition, a precisely scaled photograph of a lateral intercondylar notch wall was shown alongside the fluoroscopic image, with the identical ACL footprint precisely superimposed on it (Figure 3). The surgeons were then asked to mark with an X their intended position for the center of their femoral tunnel on the diagrams (intended position).
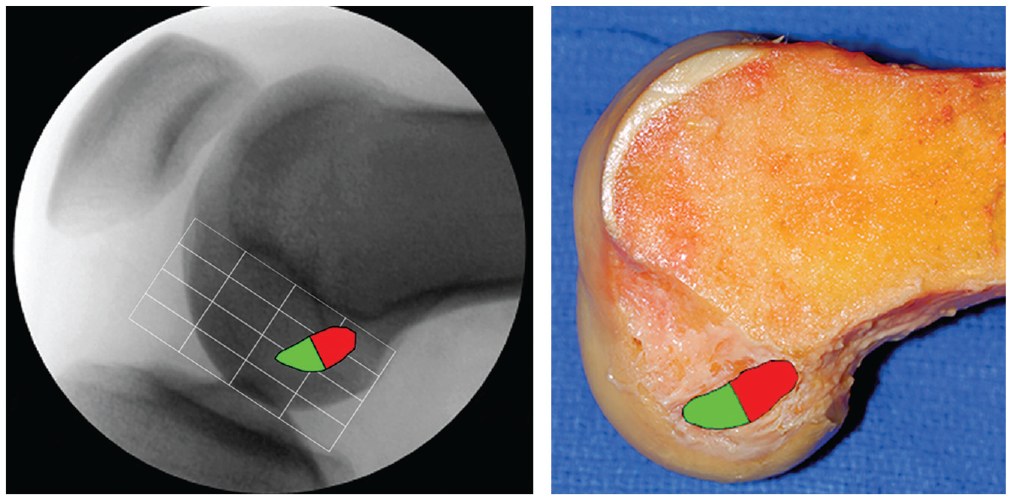
Each surgeon was asked to place an X on the diagrams to demonstrate the intended center of their femoral tunnel. The shaded areas indicate the anteromedial and posterolateral parts of the native ACL footprint
Assessment of Achieved Tunnel Position
After collection of the questionnaires, each participating surgeon was brought into the Bioskills laboratory and asked to arthroscopically demonstrate his or her selected ACL femoral tunnel position on the specimen. Surgeons were given several minutes to perform an initial arthroscopic inspection of the knee, allowing use of either the AM or AL portal. After surgeons were satisfactorily oriented, they proceeded to use the ACL tunnel placement strategy stated in their questionnaire. Participants were provided with any instrumentation that they required to assist with finding their desired tunnel location: offset aimer, ACL ruler, outside-in aimer, and so on. The position of the center of their proposed femoral ACL reconstruction tunnel was indicated by resting the 45° microfracture awl against the lateral intercondylar notch wall. The image intensifier was used to capture this location. For those surgeons who used an offset aimer, a guide wire was placed through the aimer and held against the bone instead of the microfracture awl. Offset aimers (Accufex Endofemoral Aimer; Smith & Nephew) were available from 4 to 7 mm and were selected by the surgeon. Great care was taken not to indent the bone and mark the specimen to ensure that each participant was blinded from the selected position of others. The tunnel localization strategy was recorded as follows:
Image intensifier: surgeons who used the C-arm to assist with tunnel placement
ACL ruler technique: surgeons who used a malleable ruler placed along the lateral intercondylar notch wall (Figure 4)
Offset aimer: surgeons who used an offset aimer
Estimator: surgeons who localized their tunnel without instrumentation by using, for example, a “clock face” technique or referencing from bony ridges
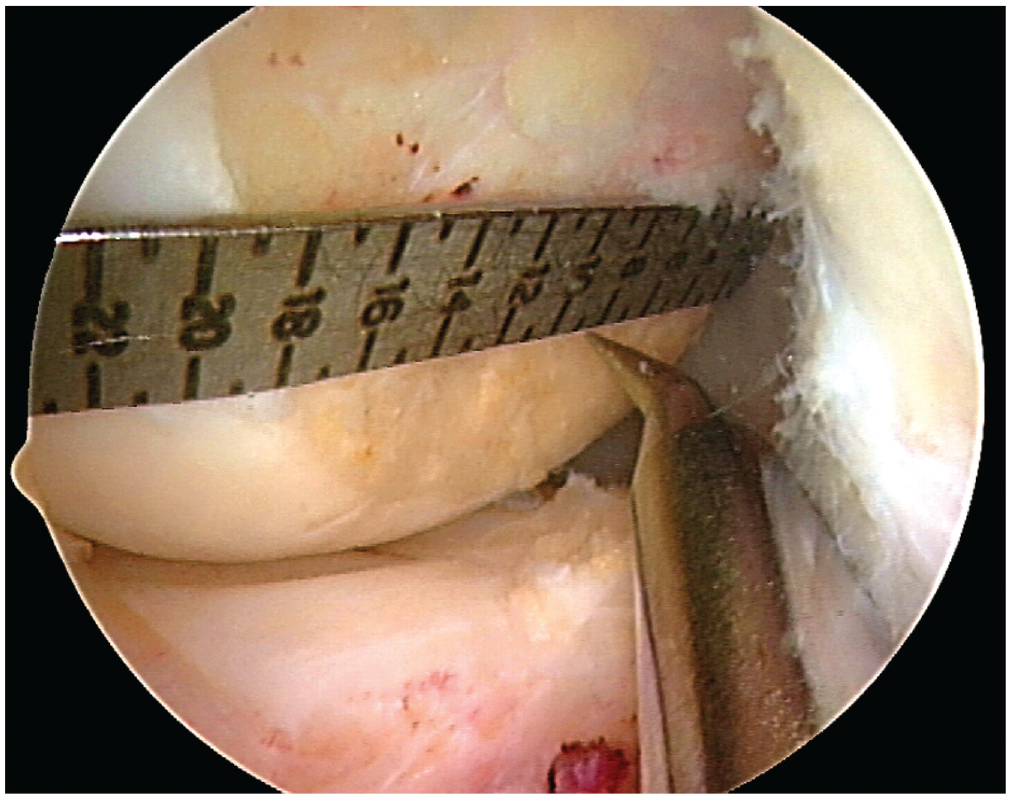
The ACL ruler is positioned on the lateral wall of the notch, with the end at the proximal border of the articular margin deep in the notch. The center of the native ACL femoral attachment has been described as being 50% of the distance from the proximal-to-distal (deep-to-shallow) cartilage borders. 10 Femoral tunnel position may then be referenced along the ruler. ACL, anterior cruciate ligament.
Some surgeons stated that in their routine ACL practice, they used a 2-portal ACL reconstruction technique and that they drilled through the AM portal, outside-in, or transtibially while viewing through the AL portal. However, for placement of the ACL femoral tunnel, they verified their selected position by viewing through the AM portal. This was similarly performed in the Bioskills laboratory. The surgeon initially located a position while viewing through the AL portal, with the microfracture awl placed thorough the AAM portal. The awl was held by the observer, and then the arthroscope was switched to the AM portal to verify the position. Participants using this technique were allowed to view through AL and AM portals until they were satisfied with their position and a fluoroscopic image was acquired. For analysis, these surgeons were included as “AM viewers,” as were surgeons who used a 3-portal ACL reconstruction technique.
After the awl was positioned to the surgeon’s satisfaction, a fluoroscopic image was taken: the achieved position. Surgeons were blinded from seeing the fluoroscopic image of their achieved tunnel position unless they stated that they used fluoroscopy as their tunnel placement strategy.
For those surgeons who used an offset aimer, a guide wire was placed through the aimer and held against the bone instead of the microfracture awl. The position of the tip of the guide wire was captured on a fluoroscopic image.
Data Analyses
To eliminate the effect of different-sized femurs on our investigation, the distance between the intended and achieved femoral ACL tunnels was modeled in 2 dimensions. The grid method of Bernard et al,9,55 as applied to the fluoroscopic true lateral images, allowed each intended and achieved tunnel position to be defined as a percentage ratio of the sagittal diameter of the whole lateral condyle measured along the Blumensaat line (X axis) and as a percentage of the maximum width of the femoral condyle perpendicular to the Blumensaat line (Y axis) (Figure 5). The achieved and intended tunnel positions were measured by an independent observer (J.R.) who was blinded to the names of the surgeons, their tunnel localization strategy, and their viewing portal used.

Each surgeon’s intended and achieved femoral tunnel position was referenced using the grid method of Bernard et al,
9
and the Euclidean distance between points was calculated with the formula ΔXY =
With this model, the difference between the intended and achieved femoral ACL tunnel positions were expressed as a vector (Euclidean distance). The magnitude of this vector was calculated using the Pythagorean theorem, which gives a value for the distance between the points, with 0 for a perfect match. The Euclidean distance between the intended and achieved tunnel positions was calculated using the following formula:

The positions of the native ACL AM and posterolateral bundle centers have been shown to lie a mean 8.2 mm apart at X = 24.6%, Y = 25.3% (AM) and at X = 32.3%, Y = 47.6% (posterolateral) using the grid method of Bernard et al 9 (vector magnitude, 23.1). Thus, a vector magnitude of 5 is approximately 1.8 mm in the average knee.
Statistical Analysis
A power calculation was performed assuming an alpha of .05 with the aim of achieving 90% power; significance was defined as P < .05. The minimum difference was based on a vector magnitude of 5 using the grid method of Bernard et al, 9 and it produced a minimum sample size calculation requirement of 200 surgeons. Raw data were imported into Microsoft Excel (Version 16, Microsoft Corp) for analysis. A 2-tailed Student t test for unpaired data was used to compare the Euclidean distance between the intended and achieved femoral tunnel positions for the different tunnel-positioning strategies, viewing portal techniques, and stated femoral drilling techniques.
Results
Data from the questionnaires showed that all surgeons intended to place the center of their femoral ACL reconstruction tunnel within the native ACL femoral attachment site (Figure 6), with a mean intended location at 27.0% (range, 18%-39%; SD, 3.5%) along the Blumensaat line (X) and 31.4% (range, 18%-49%; SD, 5.5%) of the width of the femoral condyle (Y). The mean achieved position was at X = 24.7% (range, 0%-40%; SD, 6.3%) and Y = 32.1% (range 0%-62%; SD, 12.0%). A total of 181 surgeons achieved a femoral tunnel within the native ACL footprint, while 40 surgeons achieved a position outside the native ACL attachment site of the specimen.
The (A) intended and (B) achieved femoral tunnel positions for all participating surgeons are shown on a true lateral radiograph of the knee relative to the grid of Bernard et al. 9 A sample femoral attachment site (specimen 3) is shown.
Viewing Strategy
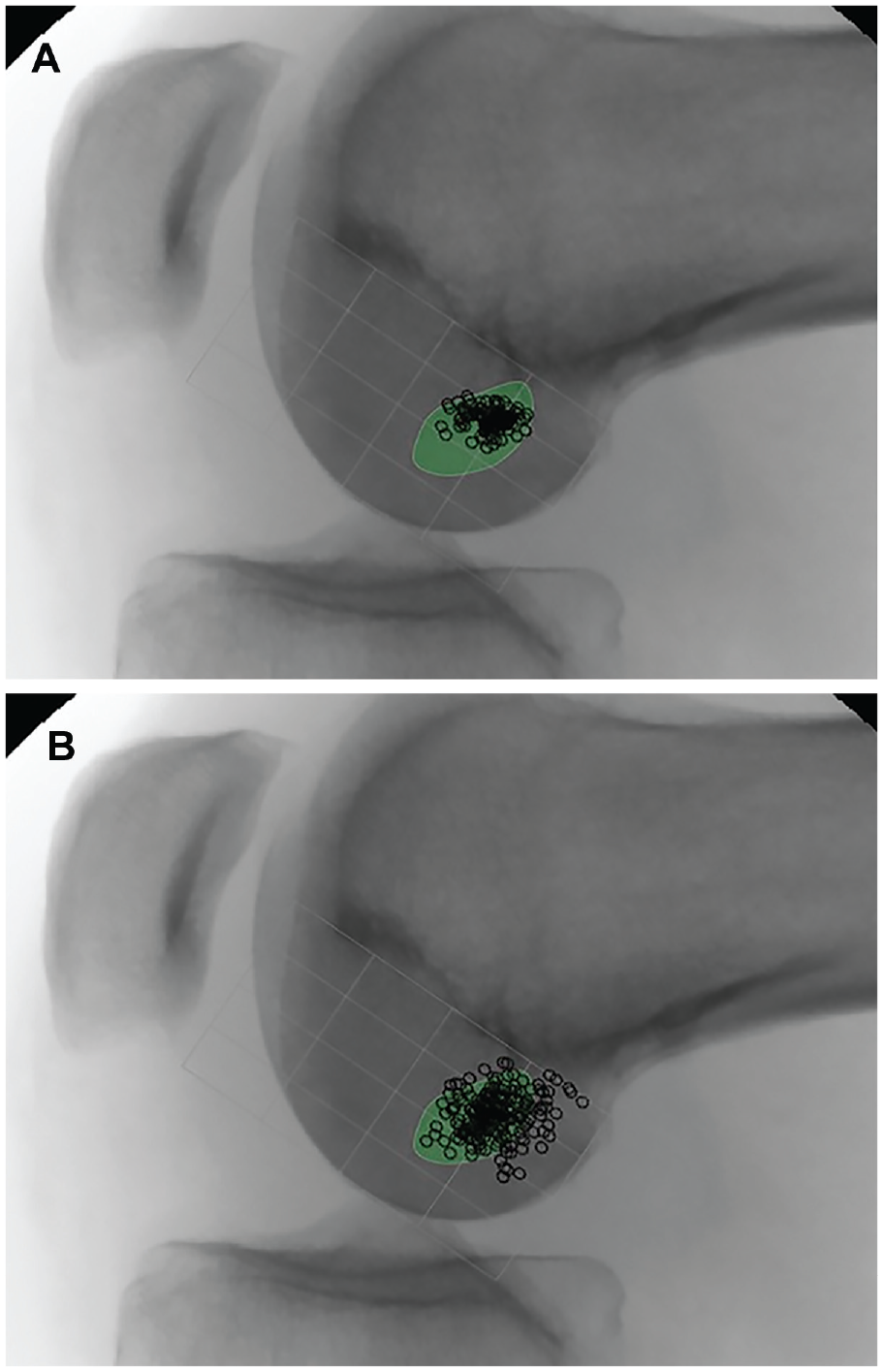
A total of 134 participants viewed the ACL femoral attachment site with the arthroscope in the AM portal (Figure 7) when positioning their tunnel; 87 chose the AL portal (Figure 8).
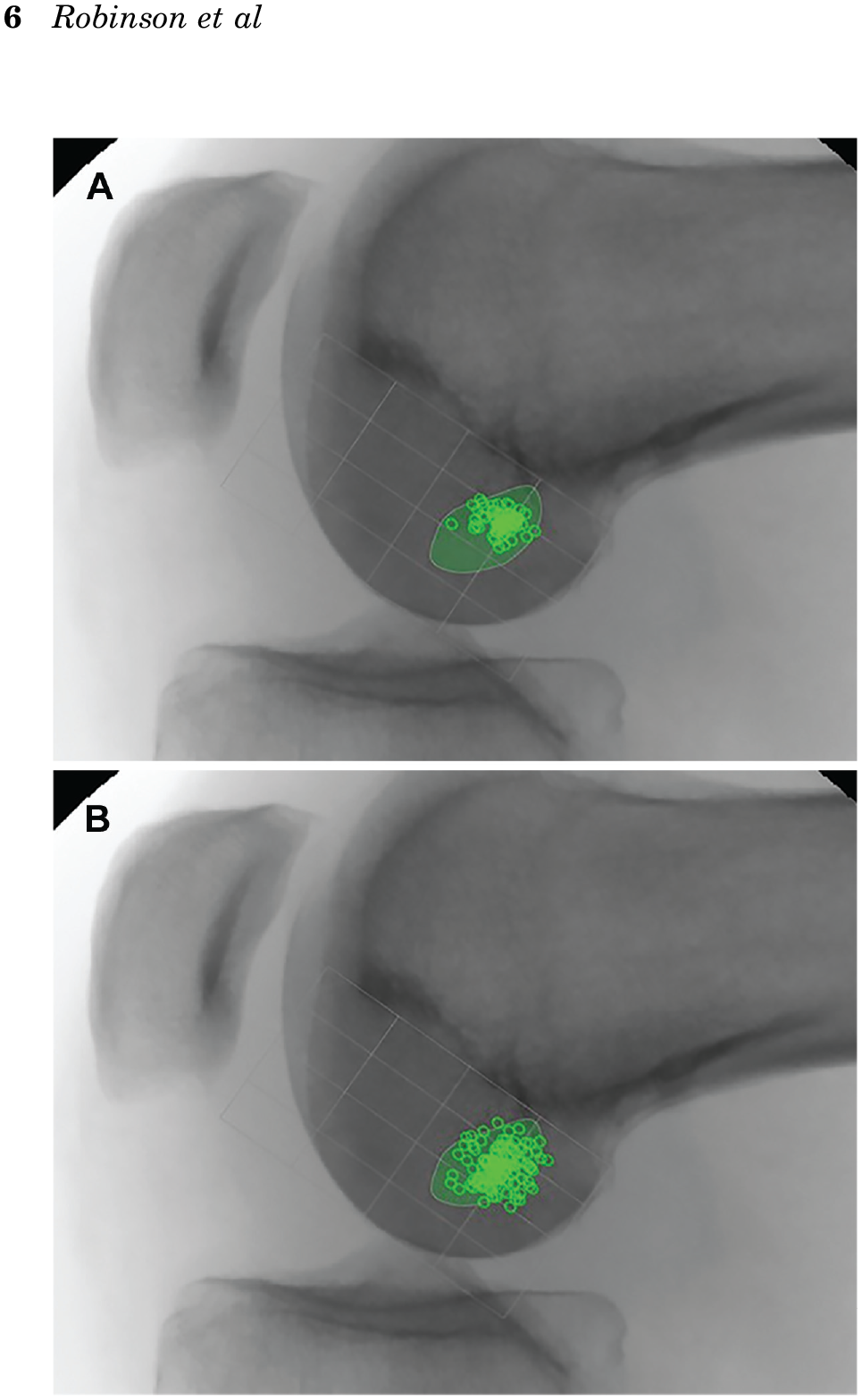
The (A) intended and (B) achieved ACL femoral tunnel positions for surgeons who viewed the lateral ACL femoral attachment site through the anteromedial portal. ACL, anterior cruciate ligament.
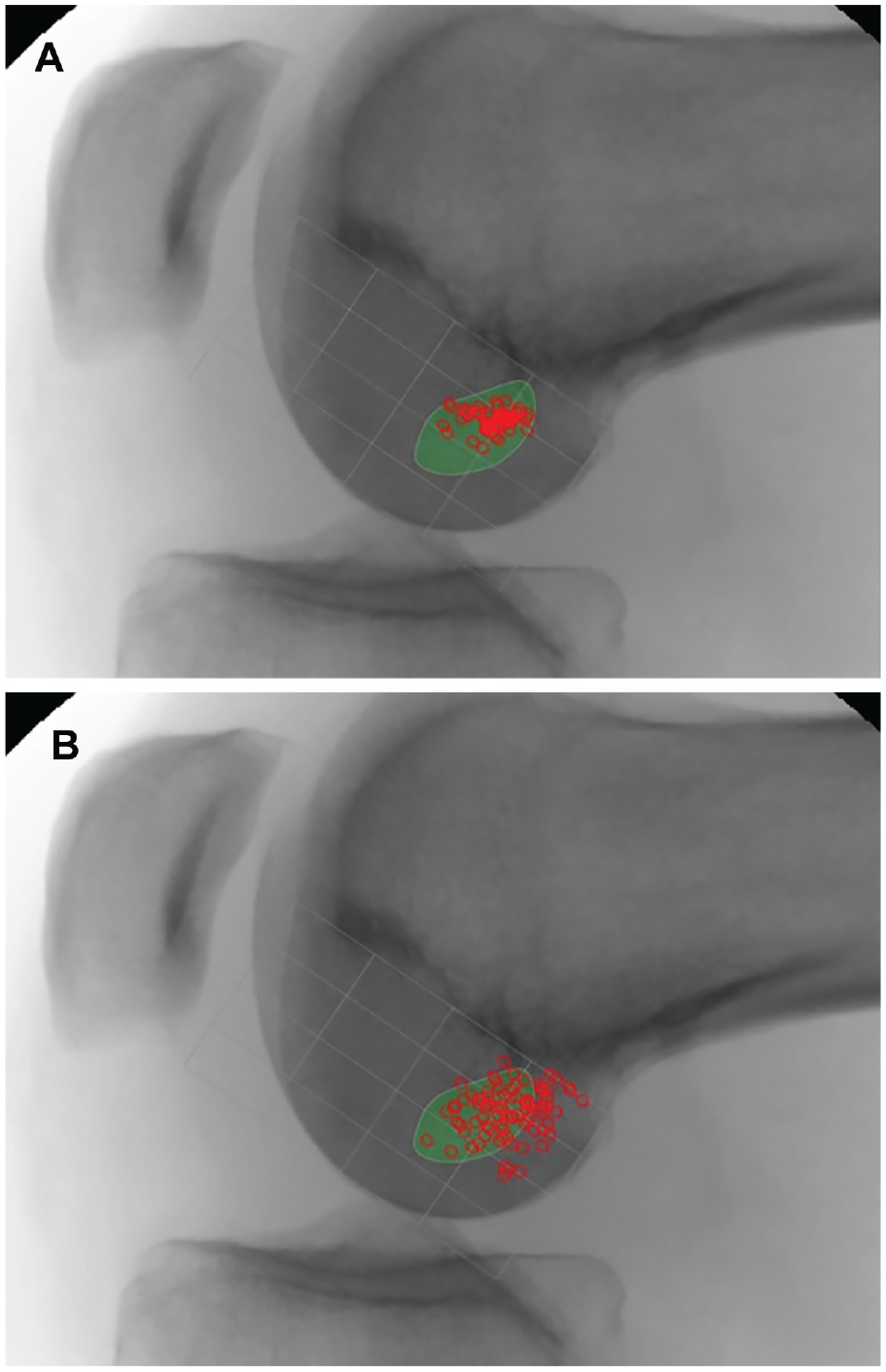
The (A) intended and (B) achieved ACL femoral tunnel positions for surgeons who viewed the lateral ACL femoral attachment site through the anterolateral portal. ACL, anterior cruciate ligament.
The mean intended position for AM viewers and AL viewers was similar. AM viewers were more likely to achieve a femoral tunnel position closer to their intended tunnel position than those who viewed through the AL portal (P < .0001) (Table 1). A total of 31 (36%) AL viewers achieved a tunnel position with the center of the tunnel located outside the native ACL femoral attachment site, as compared with 10 (7%) surgeons who viewed through the AM portal. The mean achieved position for AL viewers was higher and deeper in the intercondylar notch.
Differences Between Intended and Achieved Femoral Tunnel Positions for Different Viewing Portals a
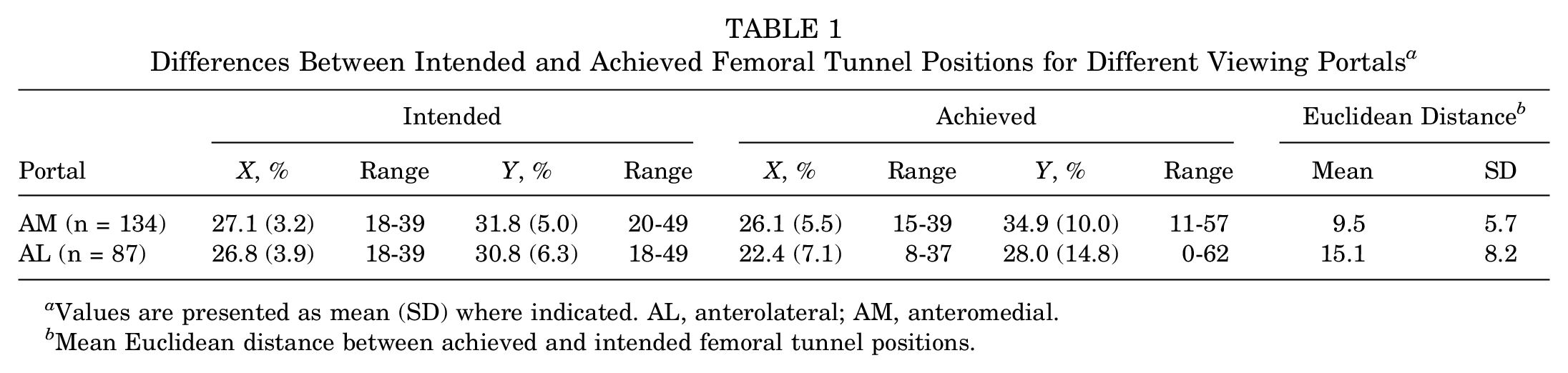
Values are presented as mean (SD) where indicated. AL, anterolateral; AM, anteromedial.
Mean Euclidean distance between achieved and intended femoral tunnel positions.
Localization Technique
The intended and achieved tunnel positions for the different femoral tunnel localization strategies is shown in Table 2. Surgeons using an offset aimer had the largest mean distance (14.5) between achieved and intended tunnel positions (Figure 9). This was not significantly different from surgeons who used estimation (ridges, clock face, etc) (Figure 10). Surgeons who used a malleable ACL ruler (Figure 11) achieved tunnel positions closer to their intended positions; however, the most accurate surgeons were those using fluoroscopy (Figure 12). In this group, all achieved tunnel positions fell within the native ACL footprint. Three surgeons who used a malleable ACL ruler (8%) decided on tunnel positions where the center of the tunnel was outside the native ACL footprint, as compared with 8 (25%) who used an offset aimer and 30 (22%) who used estimation. The mean achieved femoral tunnel position for surgeons using an offset femoral aimer was higher in the intercondylar notch (Y = 24.1%; P < .001) than it was for surgeons using the other localization techniques.
Differences Between Achieved and Intended ACL Femoral Tunnel Positions for Different Localization Strategies a
Values are presented as mean (SD) where indicated. ACL, anterior cruciate ligament.
Mean Euclidean distance between achieved and intended femoral tunnel positions.
Greater mean distance between achieved and intended femoral tunnel positions vs group C (P = .0002) and group D (P < .0001) but not group B (not significant).
Greater mean distance between achieved and intended femoral tunnel positions vs group C (P < .0001) and group D (P < .0001).
Greater mean distance between achieved and intended femoral tunnel positions vs group D (P = .002).
The (A) intended and (B) achieved anterior cruciate ligament femoral tunnel positions for surgeons who used an offset aimer.
The (A) intended and (B) achieved anterior cruciate ligament femoral tunnel positions for surgeons who estimated their femoral tunnel position.
The (A) intended and (B) achieved ACL femoral tunnel positions for surgeons who used an ACL malleable ruler. ACL, anterior cruciate ligament.
The (A) intended and (B) achieved anterior cruciate ligament femoral tunnel positions for surgeons who used fluoroscopy to position their femoral tunnel.
Drilling Technique
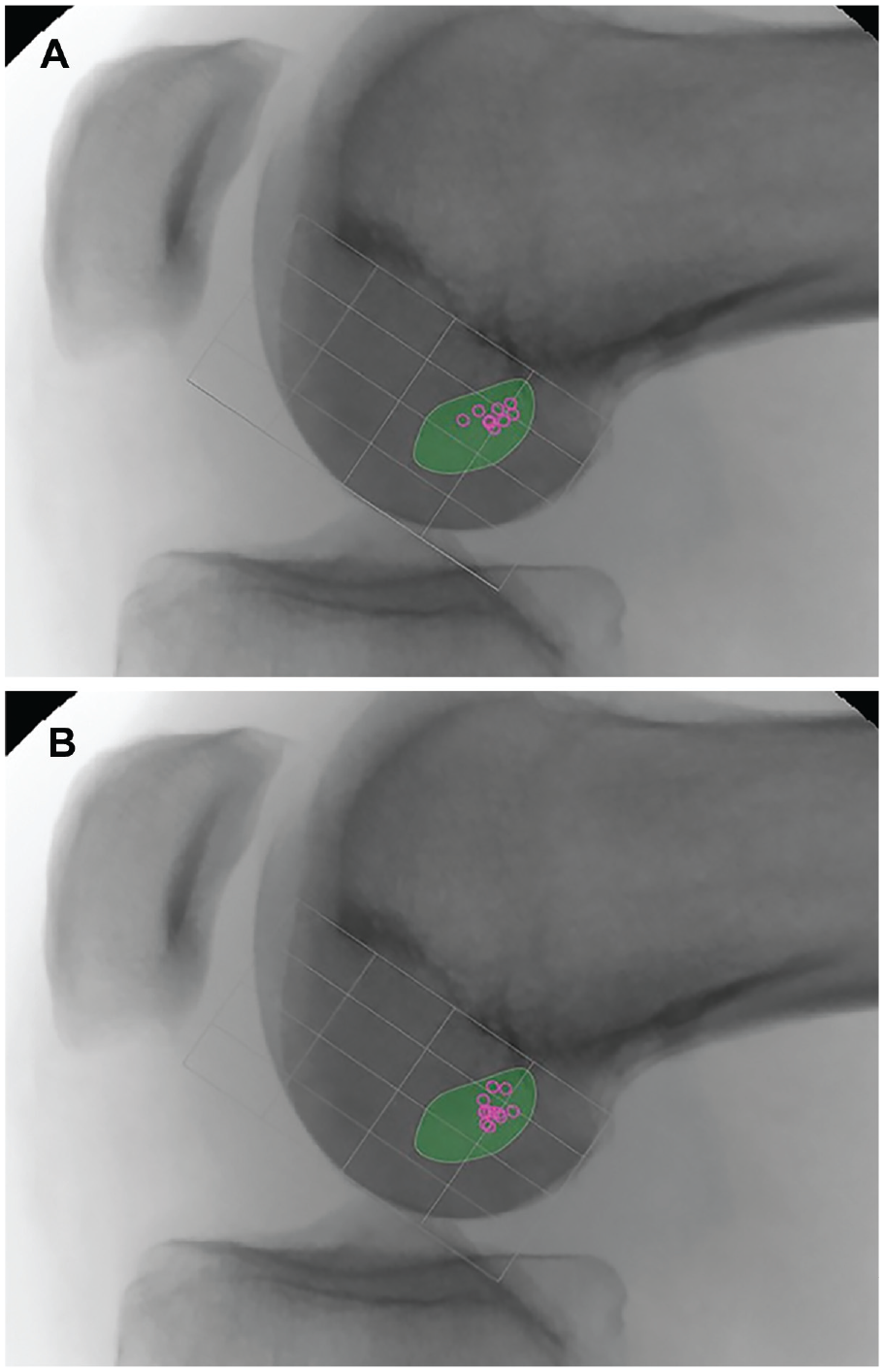
The mean achieved tunnel positions for the stated drilling technique are shown in Table 3. There were no significant differences in accuracy among the 3 drilling techniques. However, the average achieved femoral tunnel position was higher in the intercondylar notch for those using a transtibial technique as compared with those using the AM portal technique (P = .025), with no difference between those using an AM portal technique and those using outside-in drilling.
Differences Between Achieved and Intended ACL Femoral Tunnel Positions Dependent of Drilling Strategies a
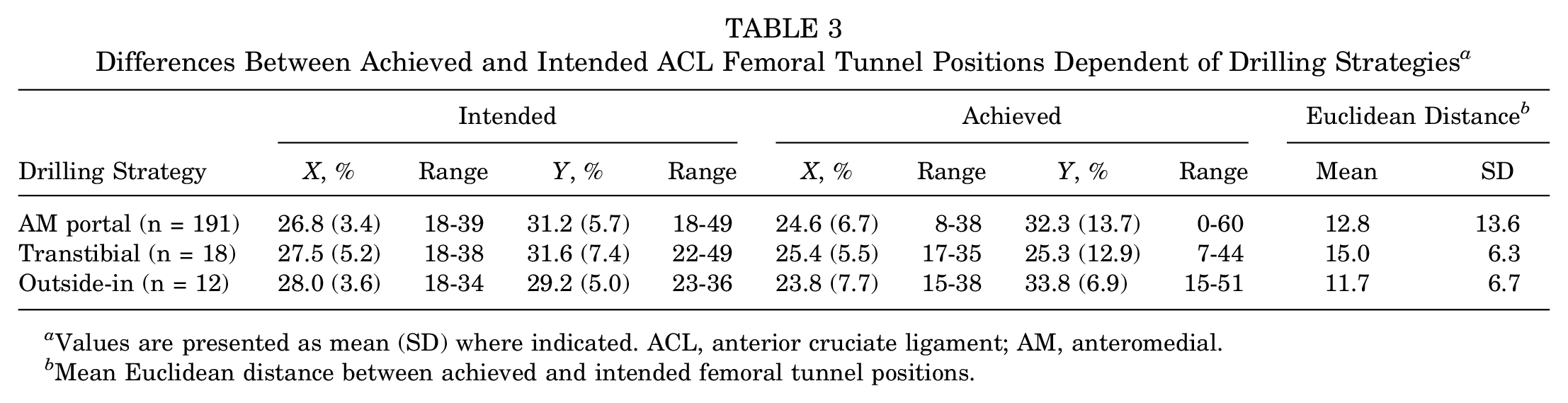
Values are presented as mean (SD) where indicated. ACL, anterior cruciate ligament; AM, anteromedial.
Mean Euclidean distance between achieved and intended femoral tunnel positions.
Discussion
The current study is the first to assess the accuracy with which a large cohort of experienced ACL surgeons from around the world locate their intended femoral tunnel position for ACL reconstruction. Our key findings were that accuracy appeared to differ according to viewing technique and tunnel localization strategy.
The restoration of native anatomy is a fundamental principle in orthopaedics. A femoral tunnel location within the native ACL footprint was desired by all surgeons in a survey of >800 by Budny et al. 14 Similarly, a tunnel position within the native femoral footprint was intended by all surgeons in our study. However, this was not always achieved according to our data. Previous studies have assessed the achieved tunnel positions in analyses of clinical practice8,31 but have not accounted for variation in intended tunnel position. Inderhaug et al 30 compared analyzed tunnel positions by performing postoperative 3-dimensional computed tomography scans. The achieved positions were compared with the center of the native ACL (X = 27%; Y = 34%) based on the data from a number of cadaveric studies. 10 Moloney et al, 42 in a laboratory study of 20 surgeons, investigated accuracy as compared with the “anatomic center” of the ACL footprint (X = 29%; Y = 37%). The data from our survey showed that although some surgeons intended a center position in the ACL footprint, many did not, representing different reconstruction philosophies. Some surgeons aimed for a position consistent with the center of the AM bundle; others opted for a position higher (more anterior) and deeper (more proximal) in the notch, consistent with an isometric graft location; and others chose a higher, more shallow position, consistent with an attempt to restore the direct fibers lying close to the lateral intercondylar ridge.19,26,27,43,51,52,61
No significant differences were found for the distance between intended and achieved tunnel positions for the 3 stated drilling techniques (outside-in, AM portal, or transtibial drilling). However, the achieved tunnel position for transtibial drillers was found to be higher in the intercondylar notch than for the other drilling techniques (P < .042). This difference should be interpreted with care, as surgeons who stated use of the transtibial technique marked their tunnel position in the specimen without a tibial tunnel being created. However, as suggested by previous literature, the transtibial technique tends to place the femoral tunnel higher in the intercondylar notch when compared with other techniques, and the tunnel is more vertical and may be located outside the native ACL footprint, owing to the restriction of drilling through the tibial tunnel.20,37,54 These limitations led to a move toward independent drilling techniques, categorized as “anatomic,” such as medial portal and outside-in drilling.25,37,53 However, in an analysis of the Danish ligament registry by Rahr-Wagner et al, 47 higher rates of revision were shown for ACL reconstruction using AM portal drilling. It was suggested that this finding might be due to a learning curve in the adoption of a new technique. We also found that surgeons using a transtibial drilling technique achieve a position higher in the intercondylar notch than do surgeons using AM portal drilling. (There was also a tendency for the tunnel to be higher in the notch as compared with outside-in drilling. This did not reach significance, perhaps because of the relatively low number of surgeons in the transtibial and outside-in groups.) Nevertheless, drilling through the AM portal did not confer superior accuracy with regard to a surgeon’s achieving an intended tunnel position. Drilling using the AM portal resulted in the most disparate tunnel positions of the 3 drilling techniques. Our study’s finding that drilling through the AM portal alone does not ensure accurate anatomic femoral tunnel placement may perhaps offer an explanation for the findings of Rahr-Wagner et al. Transtibial drilling may lead to higher femoral tunnel positions and vertical ACL grafts, which are known to be subject to lower in situ graft forces.3,50 Lower ACL graft forces may theoretically reduce the risk of graft rerupture.3,45
The surgeons who viewed through the AM portal were closer to their intended femoral tunnel positions than were those who viewed the femoral attachment area through the AL portal. With the arthroscope in the AL portal, the 30° arthroscope produces a tangential view of the lateral wall of the intercondylar notch, potentially compromising the surgeon’s ability to accurately place the ACL femoral tunnel. Placing the arthroscope in the AM portal provides a more orthogonal view of the lateral intercondylar notch 12 and thus may facilitate assessment of the ACL femoral tunnel position in the shallow-deep and high-low direction. Our study suggests that surgeons who used an AM viewing portal technique were more likely to be closer to their intended femoral position and there was less dispersion. Viewing the lateral wall of the intercondylar notch through the AM portal also eliminates the need to perform a notchplasty for visualization purposes. 11 It has been reported that the use of a 70° arthroscope may provide a similar orthogonal view of the femoral footprint location when used through the AL portal.7,13 However, this requires switching between arthroscopes during the procedure. The advantage of a 3-portal ACL reconstruction technique is that the surgeon can continue to visualize the lateral wall through the AM portal while working through the AAM portal.10-13 Surgeons using a 2-portal ACL reconstruction technique could initially mark their tunnel position using a microfracture awl and then verify this by switching to the AM portal.
The use of an offset femoral aimer was associated with the poorest accuracy in locating an intended femoral tunnel position. Previous authors have also described inaccuracies with the technique,6,15 and some have described that there can be a tendency for the femoral offset aiming guide to slide, leading to a more vertical tunnel. 15 In our study, the mean femoral tunnel position achieved by surgeons using this technique was higher in the intercondylar notch. A potential source of error in the use of an offset aimer is that the surgeon selects the size of the offset based on the size of the graft and the size of the femur. A weakness of our study is that tunnel positioning may have been more challenging for those using offset aimers, as the specimens were amputated midfemur and midtibia, thus making the selection of an appropriate-size offset more difficult than had the whole lower limb or patient been visible to the surgeon. However, ACL femoral footprint morphology does vary 19 among individuals, and it has been recommended that use of a ruler or fluoroscopy is advantageous, as each method is independent of the size of the knee.10,31
Estimation—whether through anatomic ridge identification, distance from the cartilage borders, the clock-face method, or frequently a combination of all these references— was the localization strategy most often used by surgeons in our study. Although the clock-face reference is typically used to specify the location of the ACL femoral tunnel, this method has several limitations: it ignores the depth of the intercondylar notch, there is no universally agreed reference position for the 3- and 9-o’clock locations, and the clock-face reference does not rely on any known anatomic ACL landmarks.23,24,60 The native ACL attachment site may also be located by its relationships to osseous landmarks, the intercondylar and bifurcate ridges, 22 and their use to reference accurate location of the femoral ACL tunnel have been described. 48 However, these anatomic landmarks, particularly the bifurcate ridge, may not always be easily identifiable and may be variable.10,22,46,56-58
There has been some debate as to the presence of the ridges in cases of chronic ACL rupture; however, in a case-control study, van Eck et al 58 found that there was no difference in the presence of the ridge landmarks in acute and chronic ACL rupture cases, with the lateral intercondylar ridge being identified in 88% of the patients with acute and chronic rupture. Additionally, the mean age of the cadaveric specimens in our study was 61.4 years. This may have been a potential weakness, as ACL reconstructions are usually performed in younger patients and it is unclear how the visibility of ridges may change with age.
A weakness of our study is that, particularly in more acute ACL reconstructions, there are remnant fibers of the native ACL present and these can be used to locate the position of the center of the femoral tunnel attachment site. Our experimental method removed the femoral attachment site fibers so they could not be used as a reference, thereby simulating the challenges faced by the surgeon when remnant fibers of the native ACL are absent, as is often the case in chronic ACL tears and in revision cases. None of the surgeon participants believed that this was unrepresentative of clinical practice.
Previous in vivo31,44 and laboratory 2 studies have found that the use of fluoroscopy for ACL reconstruction improves accuracy of tunnel placement. Our study similarly found that the surgeons who used fluoroscopy for ACL femoral tunnel placement were closest to their intended tunnel positions. Fluoroscopy is readily available in most orthopaedic departments. Although the technique is reliant on obtaining a true lateral image of the knee (with condyles overlapping), 9 radiation exposure to surgeon and patient is low,17,39 and there is a minimal increase in operative time.29,38 Its routine clinical use has been shown to improve accuracy in tunnel placement, 31 yet it was the least frequently used tunnel localization strategy in our study. The use of fluoroscopy may be particularly useful in revision cases, where arthroscopic landmarks may be distorted, and for surgeons adopting a new ACL reconstruction technique.
Whereas there might be concerns about the technical difficulty, added time, and radiation exposure with the use of intraoperative fluoroscopy, our study suggests that using a malleable ACL ruler improved the accuracy of achieving a desired femoral tunnel position over estimation or the use of an offset aiming device. The ACL ruler is inserted into the intercondylar notch to lie flat against the lower third of the lateral wall of the notch. The center of the ACL (corresponding to the position 24% along the length of the Blumensaat line and 37% of the width of the femoral condyle on a true lateral radiograph using the quadrant method of Bernard et al 9 ) has been confirmed to be at 50% of the distance from the proximal-to-distal articular margins on the lateral wall of the intercondylar notch as visualized arthroscopically. 10 Choosing a tunnel location that is <50% of the measured femoral footprint length will position the femoral tunnel deeper into the ACL femoral attachment site, resulting in a tunnel that covers more of the AM part of the femoral attachment site. Choosing a tunnel location that is >50% of the measured femoral footprint length will position the tunnel shallower in the notch, resulting in more coverage of the posterolateral part of the attachment site. 11
Conclusion
This study has shown that even high-volume surgeons may not achieve their intended femoral tunnel position. Although surgeons using any of the viewing portals, drilling techniques, and localization strategies described could achieve anatomic tunnel placement, accuracy in achieving the intended femoral tunnel position was best for those viewing through the AM portal and utilizing a malleable ACL ruler or using fluoroscopy. It may be useful for surgeons to verify their femoral tunnel position using these techniques, particularly if their regular practice is to use estimation or an offset aimer and localize the femoral tunnel viewing through the AL portal.
Footnotes
Acknowledgements
The authors acknowledge Linda Chilton, Dan Kidd, Kane Smith, and Shawn Markee for their help with laboratory setup and data collection and Nick Howells for his assistance with the statistics.
Submitted June 18, 2019; accepted January 2, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: The study was undertaken in Bioskills Laboratories sponsored by Smith & Nephew. All of the authors have received fees for speaking or for organizing an educational program with Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.